
Abstract
Purpose
This study addressed the need for a psychometrically validated independent living skills measure for care-experienced young people. Existing instruments lack adequate validation and do not reflect the diverse developmental and contextual realities of out-of-home care.
Method
An initial pool of 193 items was refined to 42 through expert review and pilot testing with young people aged 14 to 25 years. The measure was administered to 122 care-experienced participants in Western Australia. Psychometric evaluation followed the consensus-based standards for the selection of health measurement outcomes (COSMIN) framework and included exploratory and confirmatory factor analyses, internal consistency reliability, hypothesis testing for construct validity, and interpretability.
Results
The final instrument comprised 28 items across eight domains and demonstrated good structural validity, acceptable model fit, and strong internal consistency. Hypothesis testing supported construct validity, while interpretability analyses revealed ceiling effects for two domains.
Discussion
The measure provides a psychometrically sound tool to guide targeted transition planning and support for care-experienced young people.
Care-experienced young people transitioning from care require a comprehensive set of skills to support them as they enter adulthood. Care-experienced persons are individuals who have been in out-of-home state care (i.e., care-leavers) and are the preferred term among self-advocates and others with lived experience of out-of-home care (OHC) in Anglo-Saxon and other Western countries. The development of independent living skills (ILS) is fundamental to fostering confidence in both practical management and psychological resilience. These skills are cultivated throughout an individual's life through inherent abilities derived from direct observation and experience, as well as through explicit instruction, thereby facilitating independent living and smooth life transitions (Alexander, 2014; Starr et al., 2024b). Generally, ILS are categorized into eight interrelated and overarching domains: (1) Financial Management; (2) Knowledge of Accessing Available Supports; (3) Managing Housing; (4) Education Planning; (5) Job Seeking; (6) Health Risk Management; (7) Domestic and Self-help Tasks; and (8) Managing Relationships. Within these domains, both tangible skills and intangible competencies are encompassed, offering a comprehensive view of ILS (Nollan et al., 2000). The acquisition of ILS is essential for adolescents to mature and successfully transition into adulthood, typically developing over an extended period through staged processes aligned with individual developmental readiness (Mendes et al., 2023). Accordingly, ILS development is neither a prescriptive nor linear process; it is a lifelong and dynamic process. For children and young adults who have experienced OHC, the effective and supported acquisition of ILS has a significant influence on personal outcomes as they enter adulthood.
Care-experienced young people have spent time away from their families, living in state-provided OHC. A clearly delineated and vulnerable population with diverse backgrounds and life experiences, care-experienced young people faces poorer life outcomes and greater barriers to developing ILS compared to noncare-experienced peers (Organisation for Economic Co-operation and Development [OECD], 2022). Proficiency in carrying out daily ILS in emerging adulthood directly impacts an individual's “functional independence,” or ability to self-manage life (Nguyen et al., 2020; Starr et al., 2024a). Research has demonstrated that individuals transitioning from OHC (or “care-leavers”) are at increased risk of adverse outcomes, including social exclusion, homelessness, diminished educational engagement, higher likelihood of unemployment or underemployment, involvement with the criminal justice system, substance abuse, and poor mental health (Atkinson & Hyde, 2019; Mendes et al., 2023; Reid, 2007; Stein, 2006).
For care-leavers, the transition from dependence to independent living tends to be sudden, intricate, and nonlinear, attributable to the abrupt cessation of supported living and care services (Baker, 2017; Mendes et al., 2013; Stubbs et al., 2023). The swift transition into adulthood may be exacerbated by welfare policies that emphasize independence over interdependence, thereby neglecting systemic barriers. Although policies differ by country and, in some cases, by state regarding the timing of the transition from OHC to independent living, it predominantly occurs during the critical developmental stage of emerging adulthood, generally between the ages of 18 and 25 years (Arnett, 2000; McGhee & Deeley, 2022). Furthermore, evidence suggests that the structure of OHC, particularly residential care, can hinder the development of ILS, as it offers limited opportunities for observation and experiential learning, which are essential for acquiring vital life skills.
The characteristics of personality can also influence the acquisition of ILS, as can an individual's sense of self-determination—the ability to make self-directed choices and decisions in life—and sense of self, which encompasses awareness and understanding of oneself. These factors directly affect confidence in exercising autonomy and independence (Powers et al., 2012; Starr et al., 2025). A robust sense of self and self-determination are essential for youth to successfully navigate the transition from OHC, as they foster emotional readiness and resilience capacity (McGhee & Deeley, 2022; Starr et al., 2024b). Furthermore, a sense of belonging facilitates ILS through interdependence, as an individual's social connections, supportive relationships, and community involvement can contribute significantly to the development of ILS and engagement in related activities. Additionally, a strong sense of belonging and psychological safety underpin the establishment of enduring relational, practical, and psychological support systems necessary for managing life transitions (Mendes et al., 2023; Reid, 2007). This interdependence is fundamental to successful transitions and challenges narrow notions of self-sufficiency. The development of ILS is pivotal for an individual's effective participation in society and their long-term well-being. Consequently, prioritizing the acquisition of ILS by youth with care experience prior to their departure from care is considered best practice, as it facilitates the cultivation of interdependence within a supportive environment before achieving full independence (Reid, 2007).
In general populations, young people often acquire and develop ILS through a process characterized by trial and error. These individuals may benefit from a sense of security, such as a safety net, or may simply acquire skills as needed, evolving over time (Mendes et al., 2023). In numerous countries, young people reside with their parents well into their 20s, providing them with time and security to develop ILS; however, such familial advantages are not always accessible to care-experienced young people (Cruz et al., 2025; Eurostat, 2025). Their personal, social, and environmental experiences influence their capacity to develop and sustain ILS. Achieving the comprehensive range of ILS necessary for managing and coping with independent living is often unfeasible for care-experienced young people prior to reaching the age threshold and transitioning out of the OHC system (Cruz et al., 2025). Consequently, it is essential to assess the acquisition of life skills to identify specific areas that require targeted support and improvement during care.
Given the interconnected and nonlinear nature of ILS acquisition, traditional checklist-based measures can fail to capture important relational aspects and dimensions of ILS. A scoping review of 24 studies (Cruz et al., 2025) found that life skills are often developed in a structured classroom setting, while Whitley-Gronborg et al. (2025) identified that inclusive and holistic support helps facilitate the acquisition of ILS. Although many studies have developed theories and explored factors influencing care-leavers’ acquisition of ILS, few psychometrically validated measures of ILS exist (García-Alba et al., 2022; Starr et al., 2024a). The interconnected nature of ILS domains is not reflected in existing measures, which tend to be context-specific or programmatic checklists instead of psychometrically validated tools (Starr et al., 2024a). Furthermore, the need for flexibility in measures—due to ILS acquisition occurring throughout childhood and beyond—is often overlooked, or as Nollan et al. (2002) state, “Readiness to live on one's own is a life-long process.” Psychometrically validated measures of ILS are essential in planning to inform decisions about the autonomous development, or “readiness,” of young people in OHC and those soon to leave care (Nollan et al., 2000). They can pinpoint both the strengths and areas needing improvement in acquired skills, as well as emphasize where focused learning and assistance might be required while care is ongoing and as young people near the end of state-supported care (García-Alba et al., 2022).
In many OHC interventions, the development of ILS is frequently identified as a necessary component or objective of the intervention (Cruz et al., 2025). Nonetheless, detailed pragmatic guidance on how to effectively promote and facilitate the development and acquisition of ILS within these interventions remains scarce. Cruz et al.’s (2025) scoping review indicated that only three of the 24 primary studies utilized an ILS evaluation measure. Specifically, two studies employed the Ansel–Casey Life Skills Assessment I–V (ACLSA I–V; Nollan et al., 2002), while one used a custom, study-specific assessment measure (Greeson & Thompson, 2017; Jones, 2011; Schwartz-Tayri & Spiro, 2017). The ACLSA I-V is a psychometrically validated instrument segmented by age groups (ACLSA I–IV), with an additional fifth screening measure encompassing a broader age range (ACLSA I–V). However, the authors note that this list is not exhaustive of all living skills (Nollan et al., 2002). The Daniel Memorial Independent Living Assessment (DMILA; Alexander, 2014) has been widely employed in the United States and Canada since the 1980s; however, its validity remains uncertain, and evaluations of internal consistency have revealed poor reliability (Georgiades, 2005). Additional measures have been developed for adult populations (Zorzi et al., 2023), alongside instruments such as the Independent Living Skills Evaluation (ILSE; Johnson et al., 1981, 2008) and the National Independent Living Skills Assessment Instruments (NILS; Dunlap & Sands, 1987), which are intended for both adults and young individuals. Nonetheless, these assessments have been specifically evaluated for populations with developmental or intellectual disabilities and are therefore not validated or normed for young people in OHC. Furthermore, DMILA, ILSE, and NILS predate contemporary social policy frameworks that endorse extended transitions for care-leavers, tailored training programs, and structural supports during and following placement in OHC (McDaniel et al., 2014; Mendes & Rogers, 2020). More recently, Garcia-Alba et al. (2021) developed and validated the PLANEA Independent Life Skills Scale; however, its application is limited to the context of Spanish residential care. Existing measures lack a shared, standardized definition or approach to ILS (Starr et al., 2024b). Additionally, there exists a significant need for an ILS assessment tool that accounts for the diversity of experiences within OHC and the social and contextual factors influencing ILS acquisition.
There is a need for a more nuanced and comprehensive ILS measure because there remains ambiguity about how to define ILS in research and policy, despite critiques of ILS as a poorly conceptualized construct. Some studies (Mendes & Moslehuddin, 2006) note that ILS is often defined merely as a generic checklist of competencies (e.g., cooking and budgeting). This list lacks theoretical grounding and fails to account for the developmental and relational needs of care-experienced young people.
Definitions must acknowledge how ILS are nuanced based on individual characteristics and demographics (Starr et al., 2024b). Such contextual factors are important as the acquisition of ILS requires systems to adopt individualized approaches (Starr et al., 2025).
A checklist approach treats ILS as a binary concept (you either have ILS or you do not), which can position young people as incompetent. Research by Mann-Feder and Goyette (2019) emphasizes that without relational scaffolding, ILS often break down under stress, yet definitions rarely incorporate this interdependence mindset.
The lack of an agreed international definition of ILS for care-experienced young people (Starr et al., 2024a) highlights the need for a nuanced, valid, and sensitive multiinformant measure (García-Alba et al., 2021). Relying on self-reports alone may not provide a full assessment and analysis of need. As Courtney et al. (2018) found in longitudinal studies, care-leavers often overestimate their readiness. A nuanced measurement approach would be multidimensional (confidence scores, practical opportunities to test ILS, conversational and reflective, and reviews of outputs or ILS integration).
ILS need to be material or practical/functional (Starr et al., 2025), such as knowing how to do something like paying a bill, and inter- and intrapersonal or transformative (Hiles et al., 2013), such as critical thinking to navigate complex systems, and accessing support as and when needed. These factors contribute to a richer definition of ILS and conceptual clarity.
Adopting a life-course perspective (Elder Jr., 2008; Elder Jr. et al., 2003) that encompasses the nuanced and lifelong journey of ILS, along with the influence of personal and social contexts on its development, underscores the dynamic nature of ILS acquisition. From a longitudinal standpoint, extending from birth to old age, life course theory posits that individuals’ developmental pathways are shaped by the interconnected and evolving aspects of life stages, socioemotional factors, environmental influences, and historical contexts (Elder Jr., 2008). Numerous studies have employed life course theory to emphasize how the skills, pathways, and trajectories of care-experienced young people upon leaving care are molded by contextual factors (Brady & Gilligan, 2019; Horrocks, 2010; Kelly et al., 2023; Oterholm & Höjer, 2023). Furthermore, the development of ILS for care-experienced young people necessitates social capital or interdependence. When these concepts are considered within developmental and ecological frameworks, where they are viewed as homogeneous yet interconnected variables within and across influencing domains (Damon & Lerner, 2008), the aim of leaving care shifts from an emphasis on “independence” to one of interdependence. Therefore, the development and evaluation of an ILS measure grounded in a life course perspective are warranted.
This study addresses the necessity for the development of a more nuanced and comprehensive ILS measure, which has been psychometrically evaluated for application with care-experienced young people. Therefore, the purpose of this research is to ascertain the psychometric properties of the developed ILS measure, thereby enhancing the evidence base.
Method
This study was embedded within a larger project, Navigating Through Life (NTL; Parsons et al., 2020). NTL is a mixed-methods longitudinal study examining young people's transitions from OHC in Western Australia (WA). One component of NTL's protocol involved repeated measurement of young people's ILS across five data collection waves. Consequently, a psychometrically sound measure of ILS suitable for the local socio-cultural context was necessary. A measure was developed and piloted, and its structural reliability, internal consistency, construct validity, and interpretability were assessed using data from wave one of NTL. The development and psychometric evaluation methods were guided by the consensus-based standards for the selection of health measurement outcomes (COSMIN) taxonomy of measurement properties and definitions for health-related outcomes (Mokkink et al., 2010).
Instrument Development
Item generation for the instrument began by assembling a bank of 193 items, drawing on items from the Ansell-Casey Life Skills Assessment for 16–19 year olds (ACLSA-III; Nollan et al., 2002), now known as the Casey Life Skills Assessment (Casey Family Programs, 2022), and the New South Wales (NSW) ILS Checklist for Young People in Care (NSW Government Department of Communities and Justice, 2019). The latter draws from the Life Skills Inventory (Washington State Department of Social and Health Services, 2000) and the Casey Family program domains (2022). These two tools were chosen because the ACLSA-III was the only previously validated ILS measure identified that was developed for the intended population and age group, while the latter accounts for the Australian socio-cultural context. The initial bank of items was grouped according to the eight domains of the NSW Government ILS checklist: Money, Housing, Education and Training, Employment, Health and Wellbeing, Daily Living Skills, Personal and Social Development, and Legal Rights and Responsibilities. Items outside these domains were initially removed from the item bank.
Three members of the research team then began assessing the remaining item bank to ensure content validity. Items were reviewed for redundancy, with the aim of removing overlapping items. When two or more items were judged to ask the same question, the most comprehensible one—based on simpler syntax and vocabulary—was kept. Items related to services, payments, or systems that were only present in NSW were either adapted for the WA context or removed if no equivalent existed. For example, references to Homes NSW (social housing provider in NSW) were replaced with the Department of Housing (social housing provider in WA). Additionally, items were excluded if they were conceptually aligned with other constructs being measured within the broader NTL study (Parsons et al., 2024). For instance, social inclusion was measured separately within NTL, and items within the Personal and Social Development domain that related more to a sense of belonging or connectedness (such as staying in touch with friends) were excluded from the developed ILS measure. Conversely, items related to social skills and understanding (such as identifying and avoiding dangerous relationships) were retained. Furthermore, items initially removed from the item bank for not aligning with the domains of Money, Housing, Education and Training, Employment, Health and Wellbeing, Daily Living Skills, Personal and Social Development, or Legal Rights and Responsibilities were reviewed again to determine whether any additional conceptual domains were represented. This review led to the creation of a ninth domain—Safety—as several of the removed items aligned with personal and online safety.
Next, the remaining items were reviewed for relevance. Items that all three research team members rated as most relevant were kept, while those all three considered least relevant were removed. The draft measure was then assessed for comprehensiveness, and the items were checked and edited for clarity to ensure complex phrasing or vocabulary was avoided. Afterwards, the items were refined through a process of expert review, pilot testing, and cognitive interviewing. Members of the research team who had not been involved previously, along with the project's two advisory groups—one comprising peak organizations, service providers, advocacy groups, and associations in OHC, young people, and community services sectors, and the other involving Aboriginal expertise in OHC, advocacy, young people and community services—reviewed the measure for relevance, comprehensiveness, and clarity. Experts provided written feedback on relevance, comprehensibility, and comprehensiveness that was reviewed by the research team and feedback was incorporated before piloting with care-experienced young people aged 14–25 years who have lived experience of OHC in WA. A total of 42 statements were presented for participants to rate on a five-point Likert scale. The instrument was administered on an iPad using REDCap (Harris et al., 2009, 2019). Following this, a cognitive interview process was conducted, during which young people were asked about the relevance, clarity, and comprehensiveness of the items. Researchers conducting the interviews made written notes, and feedback was compiled and reviewed by the team to determine necessary changes to the instrument. The outcome of this development and content validity process is presented in the Results section.
Participants
To determine the psychometric properties of the ILS measure, data from participants during Wave 1 of NTL were analyzed. Participants were recruited via the WA Government Department of Communities, specialist OHC service providers, young people and transitional support organizations, and word of mouth between May 2019 and October 2021. Eligibility required participants to be aged 14–25 years and to have lived in, or been previously placed in, OHC in WA for at least six months. Participation was voluntary, and informed consent was obtained from all. The broader project received ethical approval from the Curtin University Human Research Ethics Committee (HREC; Approval number: HRE2018–0170). Participants completed the ILS measure, a demographics survey, and six outcome measures, followed by a qualitative interview focused on transitioning from OHC and postcare experiences.
Statistical Analysis
The measurement properties of the ILS measure were assessed based on the COSMIN taxonomy of psychometric properties and definitions for health-related outcomes (Mokkink et al., 2010). Participant data were used to evaluate structural validity, internal consistency, and hypothesis testing for construct validity. Since no gold standard assessments exist (i.e., an external criterion for the phenomenon being measured), criterion validity could not be determined, and because the current dataset comes from a single measurement point, responsiveness was outside the scope of this study. However, although interpretability is not classified as a psychometric property according to the COSMIN taxonomy, it was included in the analyses as an important characteristic of a measure, allowing for the assignment of qualitative meaning to quantitative data (Mokkink et al., 2010).
Structural Validity
Both exploratory and confirmatory factor analyses were performed to determine structural validity (i.e., the degree to which scores reflect the underlying dimensionality of the construct being measured). Missing data were replaced with the variable means, and sample size adequacy was assessed using the Kaiser–Meyer–Olkin (KMO) test and Bartlett's test of sphericity (Williams et al., 2010). Factor analyses were performed using IBM SPSS 26 and AMOS 24 (Collier, 2020).
For interpretative best-fit model purposes, a cutoff of 0.4 for the factor loading was used (Pituch & Stevens, 2016). As there is no definitive cutoff for the application of model fit indices, the COSMIN good fit indices criteria were employed (i.e., comparative fit index [CFI], Tucker–Lewis index, or comparable measure >0.95, or the root mean square error of approximation [RMSEA] < 0.06, or the standard root mean square of the residual [SRMR] < 0.08; Pituch & Stevens, 2016; Prinsen et al., 2018).
Internal Consistency
Internal consistency indicates the level of relatedness among items in a measure. It is advised that confirmatory factor analysis (CFA) findings be supported by internal consistency reliability indices. Depending on the stage of factor analysis, Cronbach's α, composite reliability (CR), and McDonald's omega (ω) were calculated in this study for each subscale to verify the internal consistency reliabilities of the domains.
Cronbach's α is the most widely used measure of internal consistency, but it assumes equal item loadings (tau-equivalence) and may over- or underestimate reliability if this assumption is violated. CR, derived from CFA, utilizes factor loadings and error variances to offer an estimate consistent with the measurement model. McDonald's omega (ω) is another factor-based reliability coefficient that estimates the proportion of total variance explained by a common factor and can accommodate unequal item loadings, making it generally more accurate than α. Therefore, this study reports three indices: α for comparison with previous research, CR to reflect CFA-based reliability, and ω as a more robust, model-based estimate. Reliability values between 0.70–0.79 are considered acceptable, 0.80–0.89 good, and ≥0.90 as excellent, with values above 0.95 indicating potential item redundancy. The same criteria were applied to α, CR, and ω, with a preference for ω when item loadings differ (Cohen, 2013; Hayes & Coutts, 2020). The strength of inter-item correlations was interpreted based on Cohen's classification: 0.10 as weak, 0.30 as moderate, and 0.50 as strong in terms of magnitude (Pituch & Stevens, 2016; Streiner et al., 2014).
Hypothesis Testing for Construct Validity
Hypothesis testing for construct validity assesses how well scores on a measure align with hypotheses, such as internal relationships, correlations with other measures, or differences between relevant groups, assuming the measure accurately captures the construct being studied (Mokkink et al., 2010). The following hypotheses were tested: (1) no significant differences are expected in ILS between genders (independent samples t-test); (2) age is positively associated with ILS (analysis of variance); and (3) Young people who left care, compared to those who remained in care, have higher ILS (analysis of variance).
Interpretability
Interpretability refers to the extent to which one can assign qualitative meaning to quantitative scores or changes in those scores (Mokkink et al., 2010). The interpretability of the ILS measure was assessed by examining the floor and ceiling effects of raw scores (quantitative scores). Floor and ceiling effects are deemed to be present if more than 15% of all participants reach the lowest or highest possible scores, respectively (Terwee et al., 2007), which indicates that extreme items at the lower or upper ends of the scale are absent, thereby negatively affecting content validity and reliability (Terwee et al., 2018).
Results
Instrument Development: Content Validity
The initial item bank was reduced to 63 items adapted for the WA context, aligning with the requirements of the NTL study, and covering the domains of Money, Housing, Education and Training, Employment, Health and Wellbeing, Daily Living Skills, Personal and Social Development, Legal Rights and Responsibilities, and Safety. After review of all three content aspects (i.e., relevance, comprehensibility, and comprehensiveness) by six experts (four members of the research team and two members of the project's advisory groups), 42 items remained in the draft measure, phrased as statements, each with a five-point Likert-like response scale from 1 (strongly disagree) to 5 (strongly agree).
The draft measure was piloted with seven young people aged 14–25 who have lived experience of OHC. No additional items were added after the cognitive interviews, and only a few were minimally rephrased based on participant feedback to improve comprehensibility. By reporting on all three aspects of content validity with sufficient numbers of professionals and participants with OHC experience (qualitative studies: n ≥ 7), the COSMIN criteria for instrument development and content validity were satisfied (Terwee et al., 2018).
Participants
A total of 122 participants were recruited: 59.0% (72 out of 122) young men, 40.2% (49 out of 122) young women, and 0.8% (1 out of 122) nonbinary. Participants (nmissing values = 2) ranged in age from 14 to 25 years (mean = 18.75 years; standard deviation [SD] = 2.45): 25.4% (31 out of 120) were 14–16 years old, 44.3% (54 out of 120) were 17–20 years old, and 28.7% (35 out of 120) were 21–25 years old. Overall, participants (nmissing values = 4) spent most of their placements in foster care (32.0%, 9 out of 118) or kinship care (32.0%, 39 out of 118). Others remained longer in residential care (19.5%; 23 out of 118), unendorsed placements (7.6%, 9 out of 118), independent care (2.5%, 3 out of 118), or other types of care (4.2%, 5 out of 118). A total of 54.1% (66 out of 122) of all participants had left care, while the remaining still lived in an OHC placement. Additionally, 32.8% (40 out of 122) identified as Aboriginal or Torres Strait Islander.
Structural Validity
Exploratory Factor Analysis (EFA)
The ILS measure consists of 42 items across nine domains. Table 1 provides an overview of the original 42 items and how they were coded for the statistical analyses. Data were complete for 10 items (n = 122), while missing data for the remaining 32 items were identified and replaced with the mean group score for each item. The percentage of missing data per item ranged from 1.67% (30 items: <2 out of 122) to 13.33% (2 items: <16 out of 122). The mean item score was 4.14 (SD = 0.42). More details on descriptive statistics for each item are provided in Table 2.
ILS Items Per Domain.
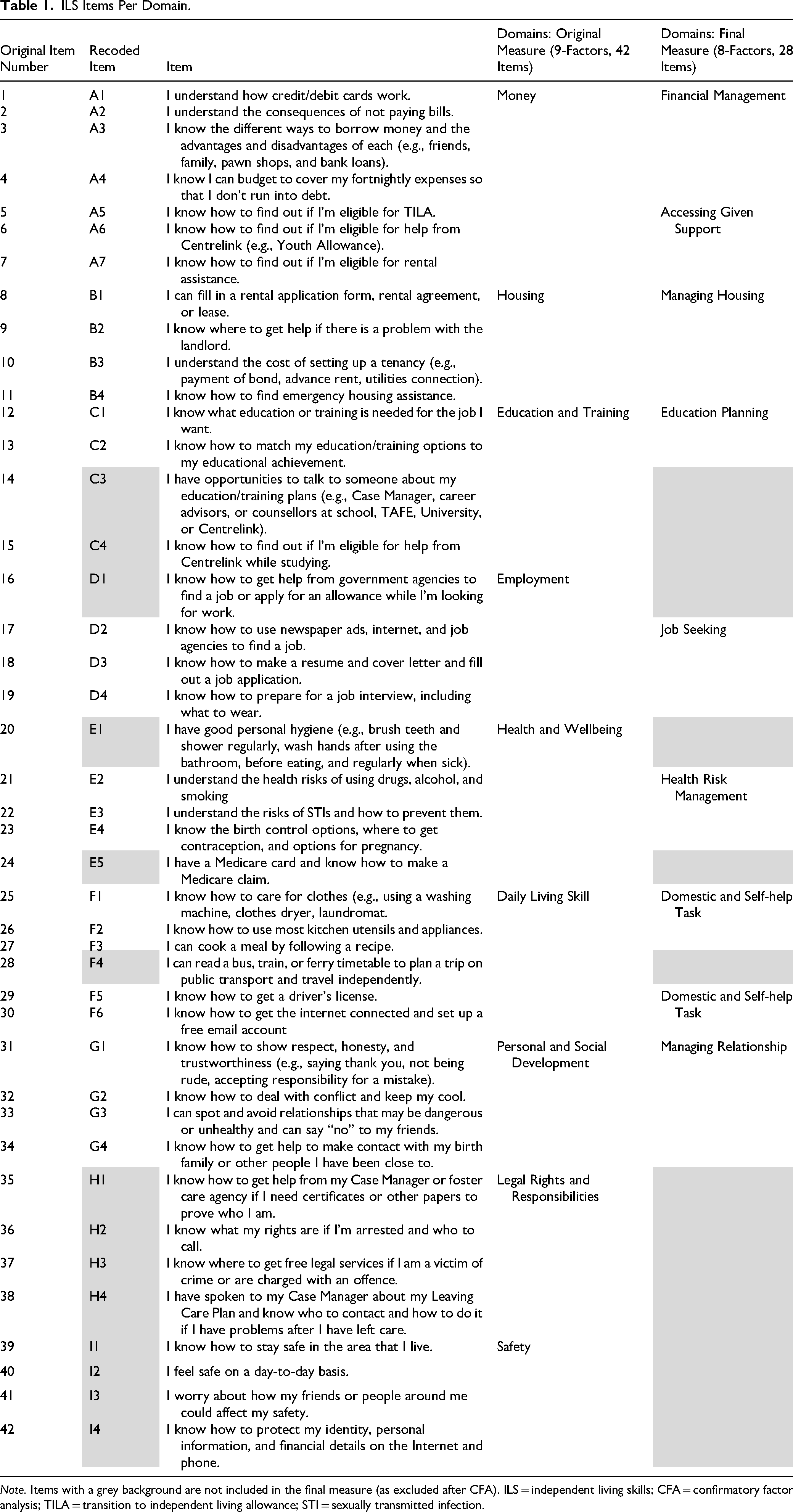
Note. Items with a grey background are not included in the final measure (as excluded after CFA). ILS = independent living skills; CFA = confirmatory factor analysis; TILA = transition to independent living allowance; STI = sexually transmitted infection.
Descriptive Statistics for Item Scores of the Original ILS Measure (n = 42 Items).
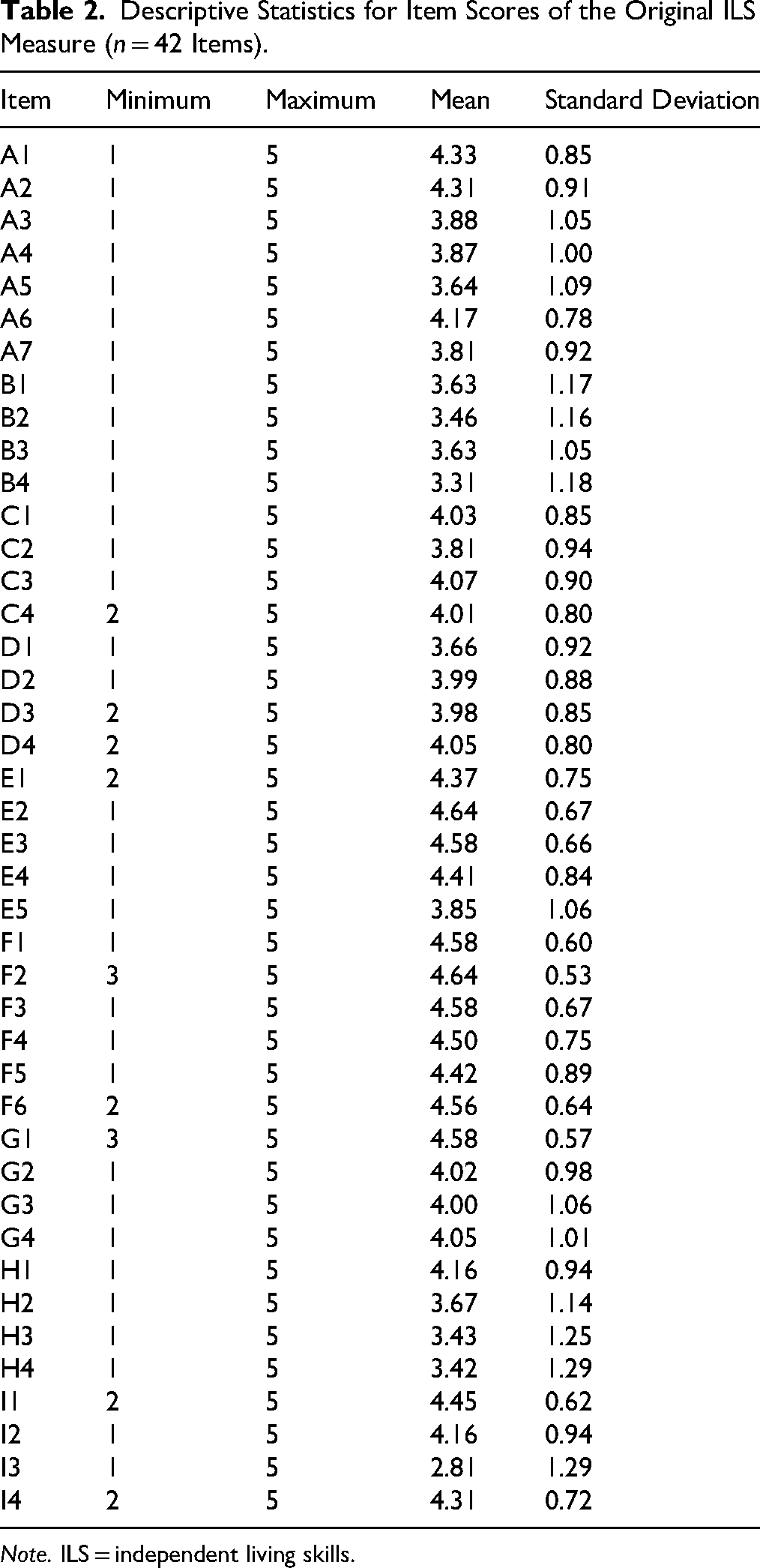
Note. ILS = independent living skills.
Although the sample size for the dataset did not meet the recommended 5:1 ratio of respondents to tested items specified by the COSMIN criteria (Terwee et al., 2018), sampling adequacy confirmed through the KMO index (with a cutoff value of 0.8) and the dataset's appropriateness for factor analysis, as indicated by Bartlett's test of sphericity (p < 0.001; Thompson, 2004), suggests that the current sample size complies with the COSMIN guidelines.
The mean item communality after EFA was 0.61 (SD = 0.17), with one item displaying low communality (factor loading <0.32; Tabachnick & Fidell, 2019). An EFA on all 42 items (using maximum likelihood extraction with varimax rotation and an eigenvalue cutoff >1) initially yielded 11 factors explaining 70.41% of the total variance. However, several factors were weakly defined; examination of the scree plot and theoretical considerations indicated that a nine-factor structure would be a more coherent and interpretable representation of the data. To improve interpretability and align with the theoretical framework of the original ILS, a nine-domain model was tested.
The resulting nine-factor solution (see Table 3) explained 65.37% of the total variance, with clearer factor loadings that better reflected the intended construct domains. Most items showed strong loadings (≥.40) on their respective factors, and the overall pattern aligned well with the intended domains. However, two domains (A and C) exhibited substantial cross-loadings across multiple factors, indicating a lack of conceptual clarity and a suboptimal structural fit. Despite this, the pattern of loadings supported the original ILS's theoretical framework and provided a solid empirical basis for subsequent model testing. Therefore, the nine-domain model was retained for the CFA initial model. Total explained variance per factor, based on a cutoff eigenvalue fixed to a nine-factor solution for 42 items, is reported in Table 4. Importantly, no items were removed at the EFA stage; all refinements occurred during theory-guided CFA.
Factor Loadings for EFA (Maximum Likelihood and Varimax Rotation): Eigenvalue is Fixed to 9 Factors.
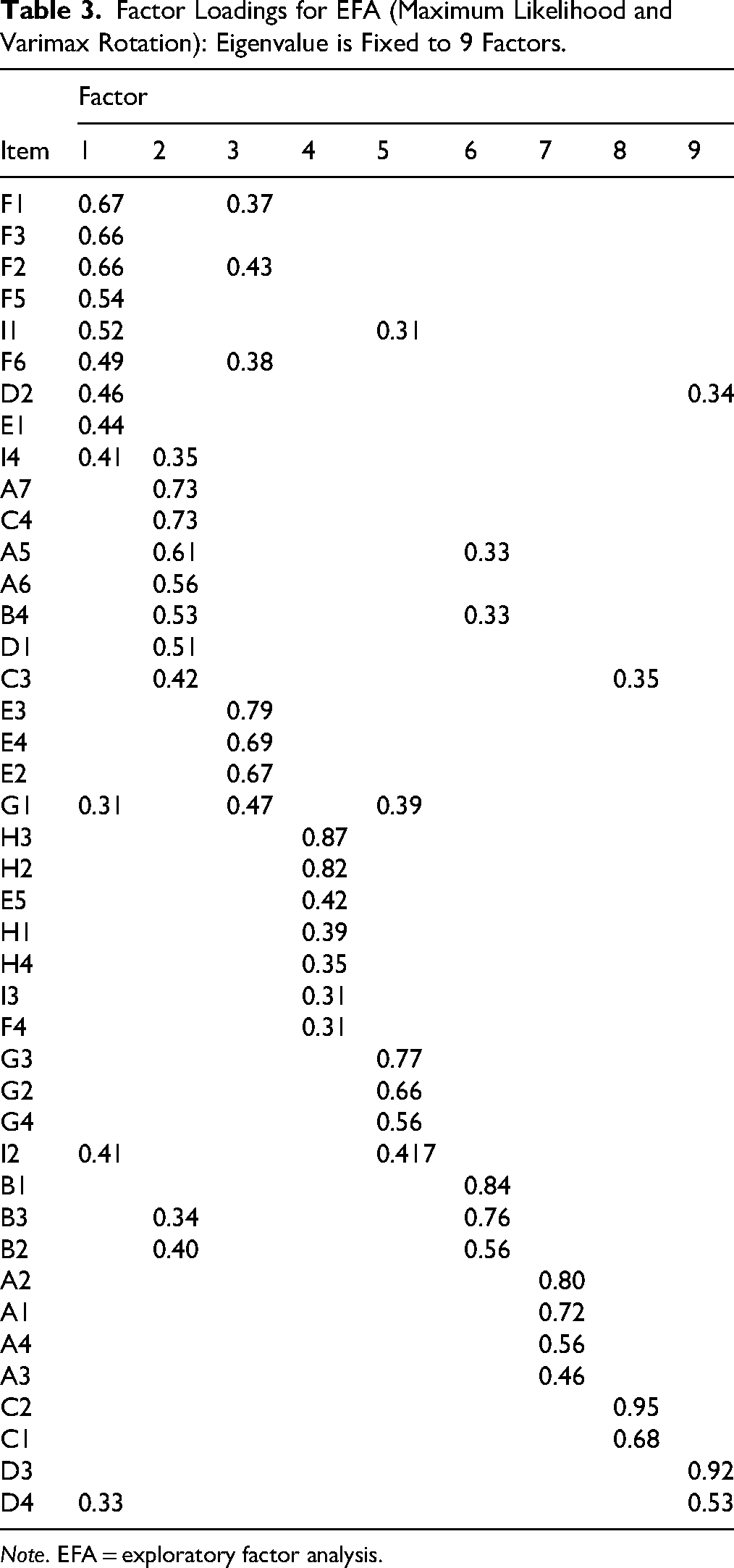
Note. EFA = exploratory factor analysis.
Total Explained Variance for EFA Fixed to a Nine-Factor Solution for 42 Items.
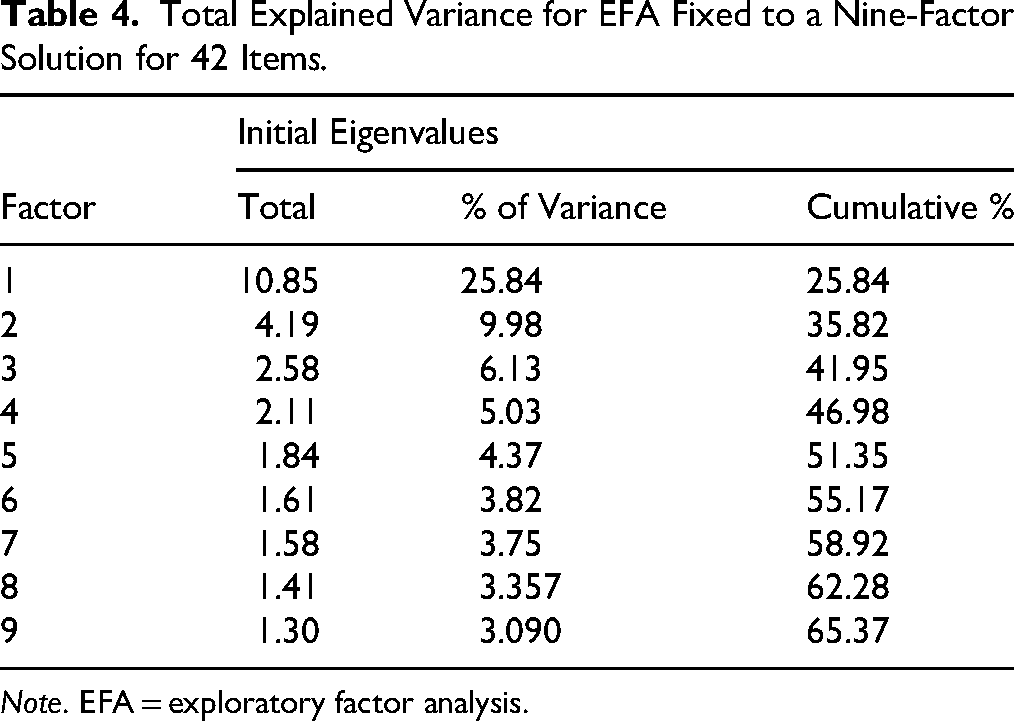
Note. EFA = exploratory factor analysis.
Reliability testing using the original ILS structure showed higher Cronbach's αs for three domains after removing a single item (see Table 5), with Cronbach's α per subscale ranging from 0.68 to 0.84. All subscales except one (Factor I: Cronbach's α = 0.68) demonstrated good internal consistency (Cronbach's α ≥ 0.70).
Cronbach's α per Domain and Item–Total Statistics (Reliability Tests) Based on EFA Fixed to Nine-Factor Solution for 42 Items.
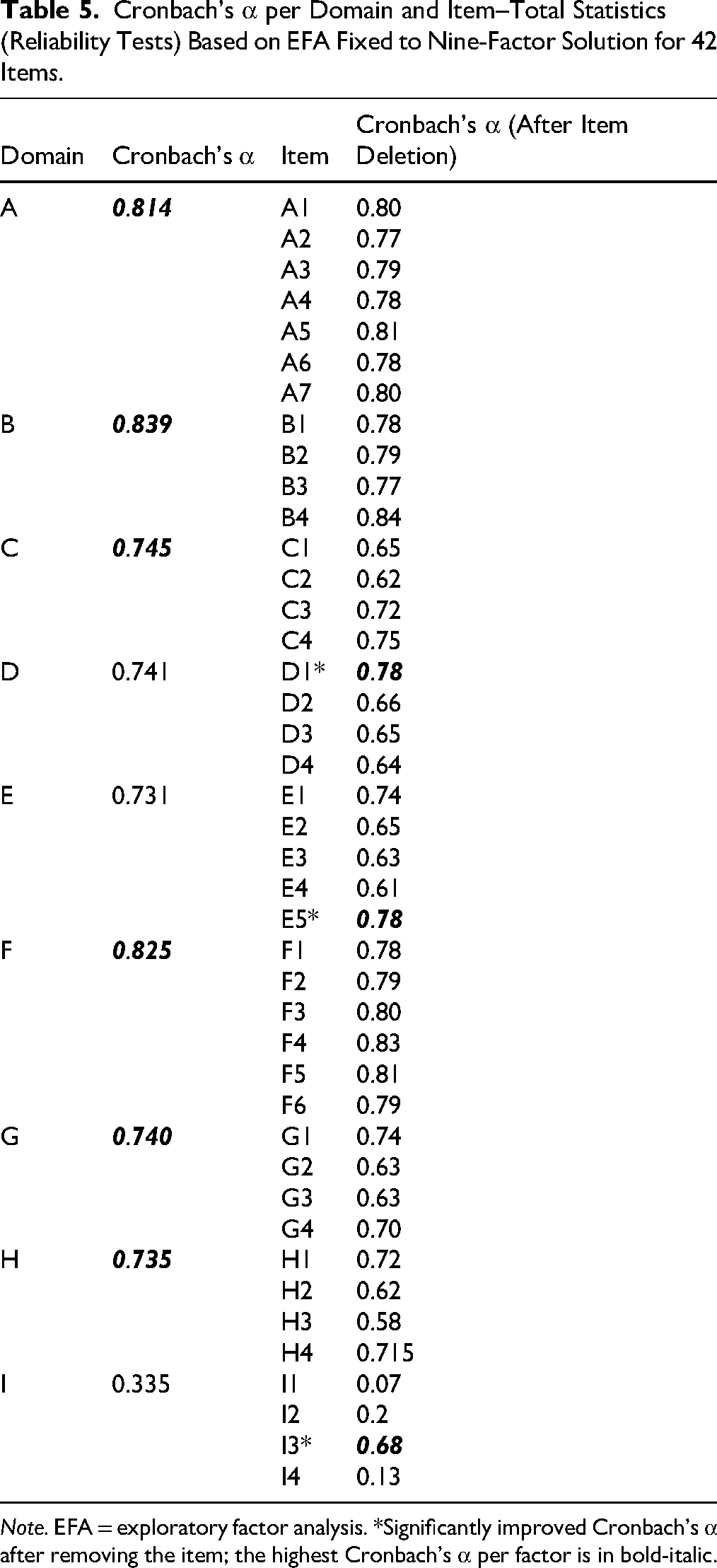
Note. EFA = exploratory factor analysis. *Significantly improved Cronbach's α after removing the item; the highest Cronbach's α per factor is in bold-italic.
CFA
Although EFA supported the original nine-domain structure of the ILS instrument, the initial CFA (the original structure of the ILS measure) modelling results demonstrated a poor fit as indicated by the CFI = 0.666, SRMR = 0.112, and RMSEA = 0.095. These indices indicated structural misspecification, necessitating model refinement. Construct-level evidence was mixed and highlighted notable weaknesses, particularly for Factor I, which failed to meet recommended reliability standards (CR = 0.62; Hair, 2021). Convergent validity was also only marginally acceptable, with average variance extracted (AVE) exceeding 0.50 for only one factor and remaining at the lower acceptable threshold (AVE > 0.40) for the other eight factors (Hair & Alamer, 2022). Taken together, these construct-level results did not compensate for the poor global fit, indicating that although some individual domains demonstrated acceptable internal properties, the overall factorial structure required systematic refinement. Accordingly, a theory-constrained, stepwise CFA refinement process was undertaken, as detailed below.
The Money domain demonstrated multidimensionality, with previous EFA consistently separating budgeting and credit-related items from welfare eligibility items, and CFA showing differential standardized loadings (0.57–0.78 vs. 0.49–0.63). These findings, together with theoretical distinctions between financial skills and system navigation, supported splitting this domain into Financial Management and Accessing Given Support. Two domains, Safety (Domain I) and Legal Rights and Responsibilities (Domain H), were removed due to weak psychometric performance and model instability. The Safety domain showed poor reliability (α = 0.335; AVE = 0.367) and nonsignificant CFA loadings, while the Legal Rights and Responsibilities domain generated substantial modification indices without theoretical justification and exhibited redundancy with support-related constructs. Removal of these domains resulted in marked improvements in model fit and construct validity.
Items were removed only when they demonstrated a combination of (a) weak standardized loadings (<.50), (b) low corrected item–total correlations (<.40), and (c) large modification indices (>20) indicative of cross-domain associations that could not be theoretically justified. Six individual items were also excluded during CFA because they did not meet the stated criteria. In particular, items such as D1 (seeking help from government agencies for employment), C3 and C4 (education-related support and eligibility), and E5 (Medicare access) were empirically and conceptually aligned with service navigation and entitlement literacy rather than with job seeking, education planning, or health competence, and became statistically redundant with the Accessing Given Support factor. These items demonstrated weak loadings on their intended constructs (0.399–0.489), low item–total correlations (0.332–0.487), and large modification indices (e.g., MI = 24.07–28.44), indicating substantial shared unexplained variance with entitlement-related indicators. Retaining these items suppressed convergent validity, with AVE values remaining below preferred thresholds (0.40–0.46) and multistage vector (MSV) approaching or exceeding AVE, reflecting inflated cross-factor covariance. Their removal resolved this redundancy, resulting in AVE ≥ 0.43, MSV consistently lower than AVE, reduced interfactor correlations, and improved discriminant validity.
Similarly, items E1 (personal hygiene) and F4 (public transport use) demonstrated weak standardized loadings on their respective constructs (0.448 and 0.487), substantially lower than other indicators within the Health Risk Management domain (0.750–0.833) and the Domestic and Self-Help Task domain (0.695–0.780), indicating limited shared variance with the intended latent constructs. Removal of E1 improved internal consistency of the health domain (Cronbach's α increased from 0.731 to 0.777), while F4 showed consistently low factor representation (0.330), indicating limited shared variance with domestic self-help skills. These statistical patterns support the interpretation that E1 reflects habitual self-care behavior and F4 represents context-dependent mobility skills, both theoretically distinct from the targeted latent constructs.
The final CFA model resulted in an eight-factor structure comprising 28 items, yielding a good model fit (CMIN = 611.72; CMIN/df = 1.87 [excellent]). Significant improvements were achieved in SRMR (0.079: excellent) and RMSEA (0.079: acceptable). The initial and final CFA factorial structures are shown in Figures 1A and 1B, respectively. Table 1 provides an overview of the eight domains, including the 28 items. The final CFA results confirm good structural validity, meeting the COSMIN criteria for sound measurement properties (RMSEA < 0.08; Terwee et al., 2018).
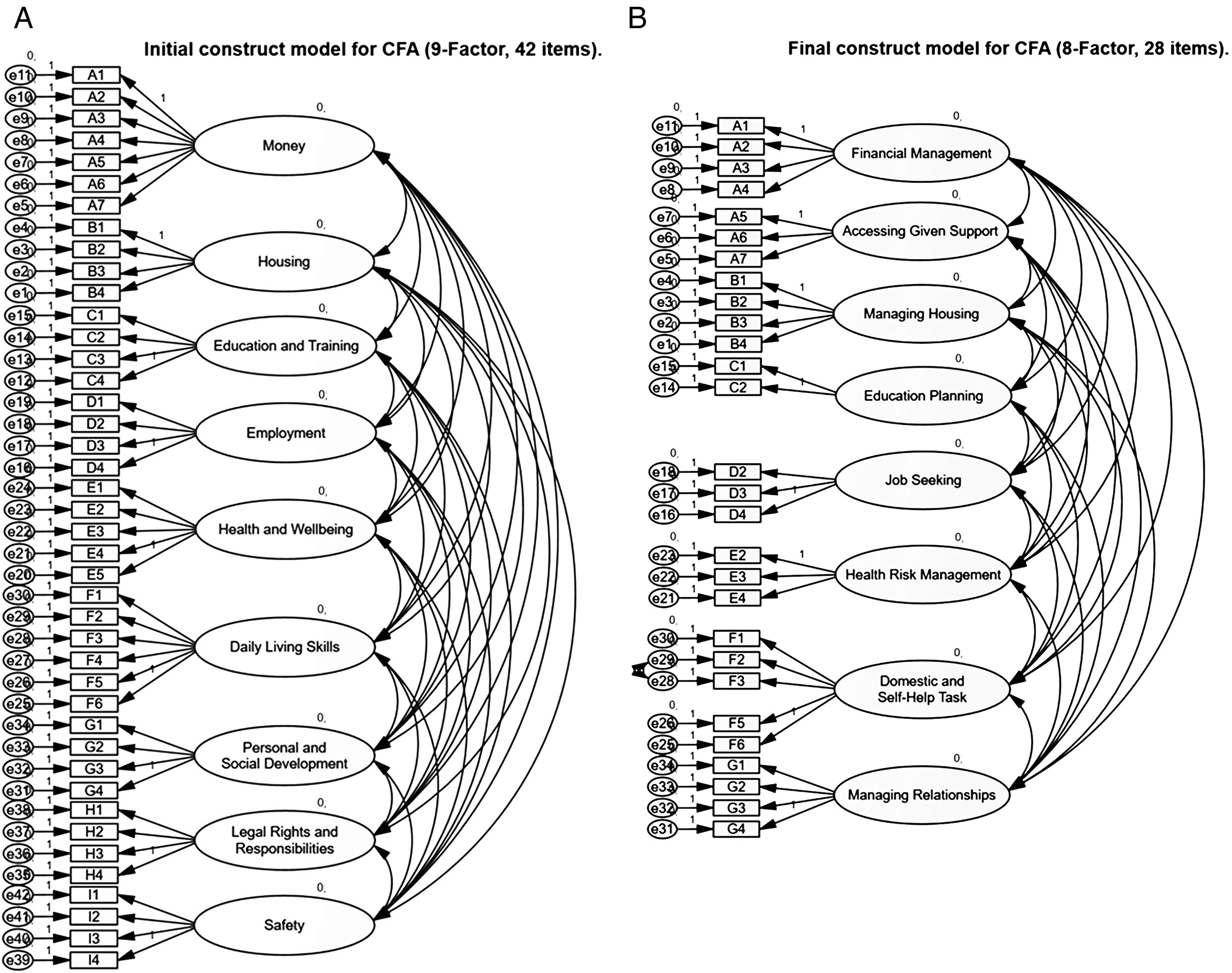
(A) Initial construct model for CFA (nine-factor solution for 42 items). (B) Final construct model for CFA (eight-factor solution for 28 items).
Internal Consistency Reliability
Indices derived from the CFA model were used to evaluate both internal consistency (CR, α, ω) and convergent validity (AVE). The data were normally distributed; as such, parametric correlations were calculated (Pearson). Inter-item correlations within each ILS domain ranged from 0.43 to 0.72, indicating moderate to strong correlations (see Table 6). Inter-item correlation for the ILS total score was 0.26, suggesting a weak correlation. This points to item heterogeneity suitable for a multidimensional construct. All factors showed satisfactory CR values (0.77–0.85), surpassing the 0.70 threshold and reflecting good model-based internal consistency. AVE values ranged from 0.44 to 0.73, with seven domains exceeding 0.50, indicating that most items (7 out of 8 domains) had more than half of their variance explained by their respective latent constructs, demonstrating good convergent validity in line with COSMIN criteria (Terwee et al., 2018).
Cronbach's α, McDonald’s ω, and AVE for the ILS Measure (Eight-Factor Solution for 28 Items).
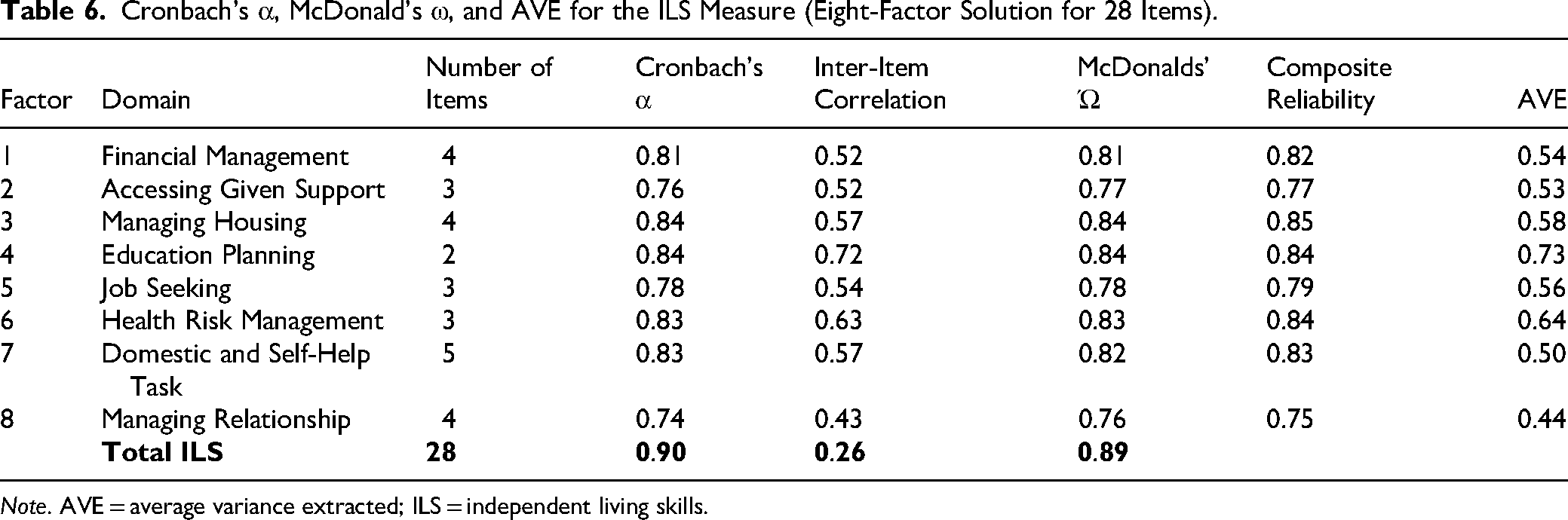
Note. AVE = average variance extracted; ILS = independent living skills.
Cronbach's α ranged from 0.74 to 0.84 across domains (total α = 0.90), indicating good to excellent internal consistency without item redundancy. McDonald's ω values (0.76–0.84 across domains; total ω = 0.89) closely mirrored α and CR, supporting reliability estimates while accounting for unequal item loadings. The consistency across α, ω, and CR demonstrates that the ILS measure has stable and robust internal consistency, and the close correspondence among these coefficients suggests that the assumption of tau-equivalence is reasonably met.
Hypothesis Testing for Construct Validity
Since data were normally distributed (skewness = −0.08; kurtosis = −0.32), parametric statistical analyses were employed to evaluate hypothesis testing for construct validity. Placement characteristics by placement type are shown in Table 7. The following three hypotheses were assessed using the ILS total scores:
Participant Characteristics by Placement Type.
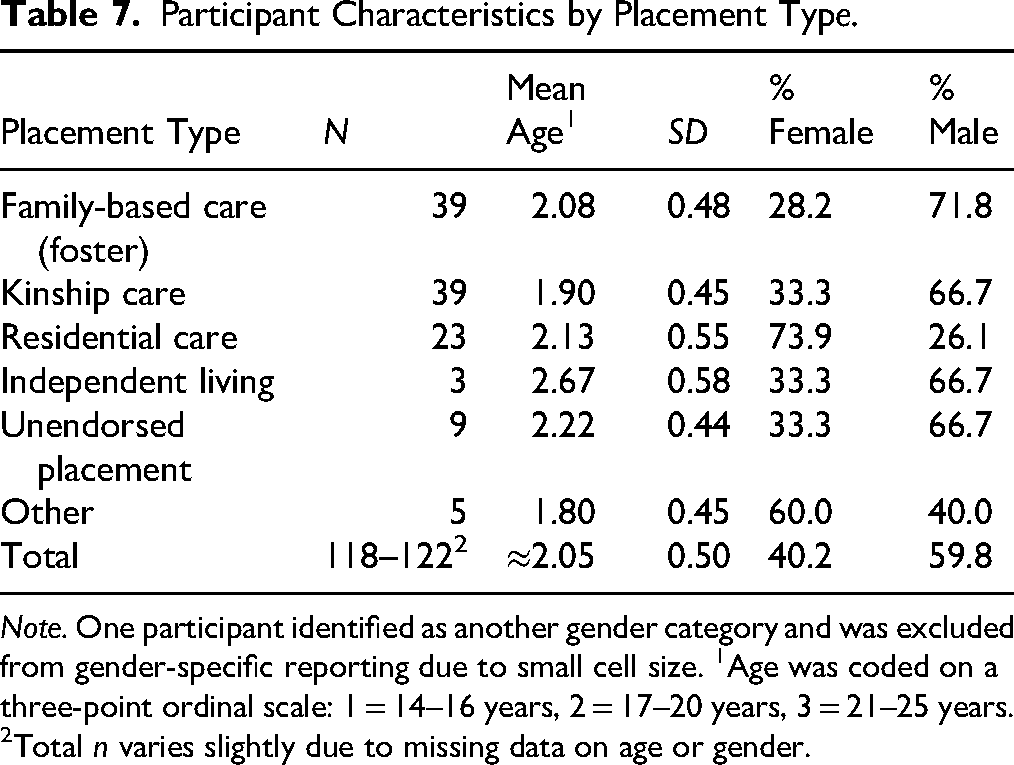
Note. One participant identified as another gender category and was excluded from gender-specific reporting due to small cell size. 1Age was coded on a three-point ordinal scale: 1 = 14–16 years, 2 = 17–20 years, 3 = 21–25 years. 2Total n varies slightly due to missing data on age or gender.
(H1) The hypothesis that there were no significant differences in ILS between genders was confirmed using an independent samples t-test: MeanMale = 114.7 (SD = 13.49), MeanFemale = 115.3 (SD = 12.75), F(1, 119) = 0.34, p = 0.79, and two-tailed. Analyses were conducted for male and female genders only (other gender: n = 1).
(H2) An analysis of variance confirmed the hypothesis that age was positively associated with independent living (i.e., older participants had higher ILS scores). Three age groups were created: 14–16 years (n = 31; mean = 109.0 [SD = 14.41]), 17–20 years (n = 54; mean = 116.0 [SD = 12.30]), and 21–25 years (n = 35; mean = 118.77 [SD = 11.90]). Statistically significant differences between groups were identified: F(2, 117) = 5.08 and p = 0.008. Post hoc tests revealed significant differences between the youngest and oldest groups (mean difference = 9.75 [standard error = 3.15], confidence interval −3.52 to −15.98, and p = 0.02), but not for other group comparisons.
(H3) The hypothesis that young people who left care (n = 68), compared to those who remained in care (n = 54), have higher ILS was partially supported. The mean ILS total score for young people who left care was higher (116.9, SD = 12.10), compared to those who were in care (112.6, SD = 14.00), approaching significance, F(1, 120) = 3.270, p = 0.07, and two-tailed.
If 75% of the a priori formulated hypotheses for the construct validity of a measure have been confirmed, the COSMIN criteria for good psychometric quality are considered met. Based on the combined results for all three hypotheses, the COSMIN grading confirmed adequate hypothesis testing for the construct validity of the ILS measure.
Interpretability
Means and standard deviations for the ILS total score and subscales were calculated. Next, floor and ceiling effects were assessed by calculating the percentage of participants who reached the lowest or highest possible scores (see Table 8). No floor effects were identified. Very few participants scored at the lowest end: two or fewer per domain (≤1.6%). Significant ceiling effects were observed in Health risk management (48.5% left care and 53.7% in care) and Domestic and self-help tasks (45.5% and 40.7%, respectively), indicating reduced sensitivity in detecting improvements among higher-functioning individuals. Floor effects across domains were minimal, with the highest at 6.1% in Education planning (left care). Overall, at the total scale level, floor and ceiling effects were negligible (≤3.7%), indicating the ILS adequately captures a wide range of functioning across both groups. When comparing young people in care with those who have left care, ceiling effects persist in both groups, but are more pronounced among those who have left care. These results suggest that several domains could benefit from items involving more complex ILS tasks.
Evaluation of Floor and Ceiling Effects for the ILS Measure (N = 122).
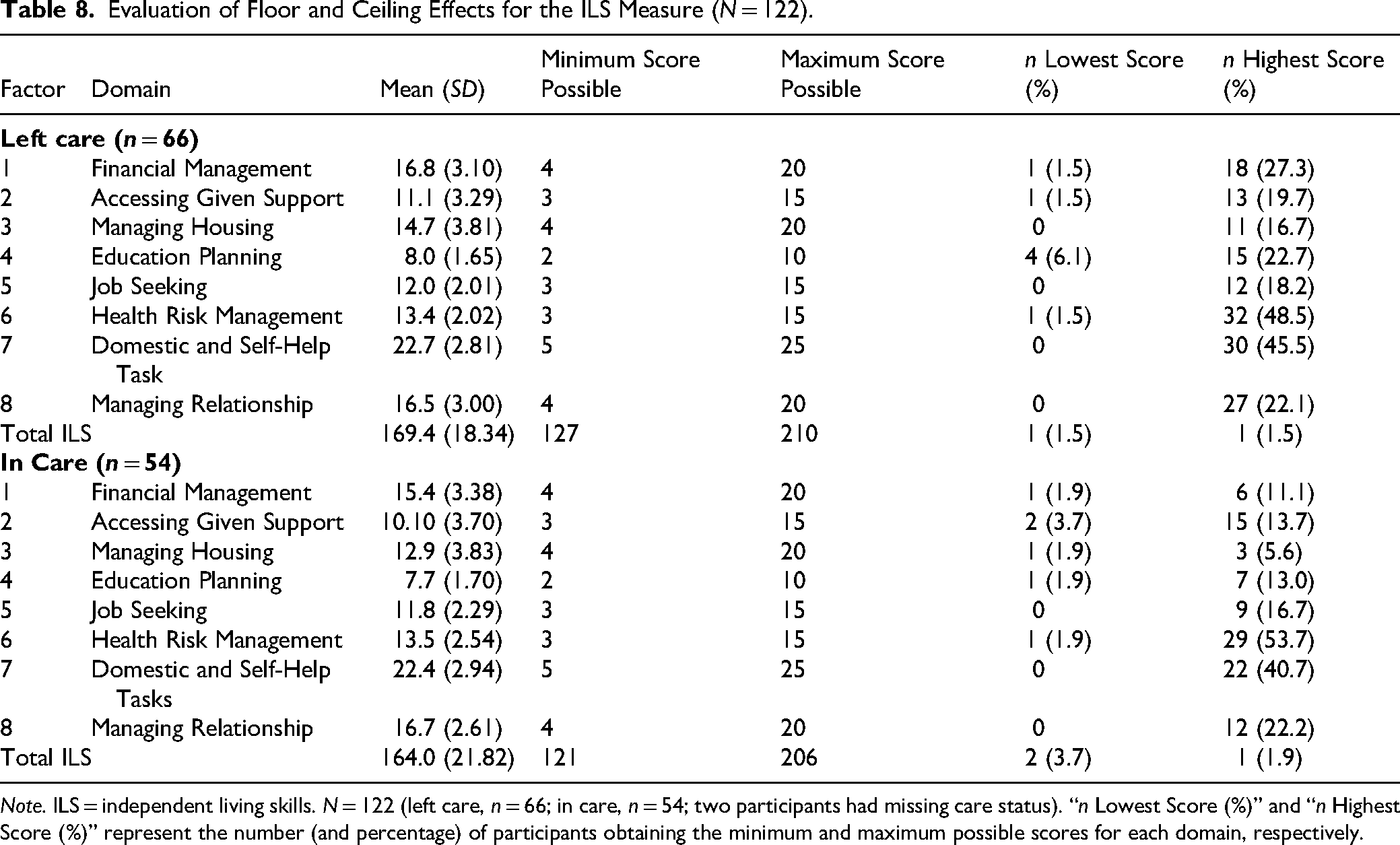
Note. ILS = independent living skills. N = 122 (left care, n = 66; in care, n = 54; two participants had missing care status). “n Lowest Score (%)” and “n Highest Score (%)” represent the number (and percentage) of participants obtaining the minimum and maximum possible scores for each domain, respectively.
Discussion
Using the COSMIN taxonomy, this study demonstrated that the ILS measure exhibits good internal consistency and structural validity following item and domain refinement, as well as acceptable hypothesis testing for construct validity and interpretability. A ceiling effect was observed for care-leavers. Assessing the ILS measure at a single time point has prevented evaluation of its responsiveness.
This study addressed the scarcity of validated ILS measures for care-experienced young people and the need for a more nuanced, interconnected understanding of ILS. It validates a constructed measure designed to capture the holistic, interrelated nature of skill acquisition for care-experienced young people. Assessing the development of ILS in young people in OHC is essential to ensure timely support and intervention in skill development, particularly before they leave care and transition into independence in adulthood. Since these skills are often cultivated through family support and opportunities, young people in OHC are likely to miss out on or not be exposed to experiences that allow them to take on independent responsibilities, where they can develop these skills (Cruz et al., 2025; Mendes et al., 2023; Starr et al., 2024b). Due to the fragmented and routine-focused nature of OHC, care-experienced young people are at risk of not acquiring essential ILS. Therefore, care and social support workers must measure the progress and development of ILS among young people in OHC. However, existing measures of ILS do not adequately capture the lifelong, interconnected nature of skill acquisition and the integration of various domains and constructs (Starr et al., 2024a). Often, such measures concentrate on specific domains or set specific life-outcome goals, or “life-aspirations.”
The initial development of the ILS measure involved 42 items across nine domains. Ambiguity or content overlap, indicated by cross-loadings during cross-factor analysis, was identified in two domains, prompting refinement of the ILS measure. Items were removed, combined, or reworded, resulting in a 28-item measure across eight domains. The revised ILS measure, with fewer domains and items, demonstrated good structural validity. The heterogeneity of care-experienced young people from diverse backgrounds may explain initial results (Organisation for Economic Co-operation and Development [OECD], 2022; Starr et al., 2025), which can challenge the standard validity of measures. Additionally, the acquisition of ILS by care-experienced young people may be influenced by the OHC environment and the opportunities available for developing or learning skills through observation (Cruz et al., 2025; Mendes et al., 2023; Starr et al., 2024b).
The measure demonstrated acceptable interpretability for young people in care and those transitioning out of care. This is a promising result, as it indicates that the skills constructs and domains included are valid for care-experienced young people who are still in OHC or in the process of leaving care. No significant differences were observed between genders; however, as hypothesized, age is positively associated with ILS. Younger people in OHC had lower ILS levels, whereas older age groups showed increases. The positive link between age and ILS may also relate to the trend toward significance in the difference between care statuses (in care or care leaver). A ceiling effect was observed for those who have left care. Care-leavers’ acquisition of ILS is often slower compared to their noncare-experienced peers (Organisation for Economic Co-operation and Development [OECD], 2022); however, the ceiling effect and the association of ILS level with age and care status (in care or care leaver) suggest that these skills continue to develop. Over time, young people who have experienced OHC may have ILS levels similar to those of peers raised in traditional family settings. This suggests that age-related maturation explains much of the initial differences observed between groups. However, chronological age is likely an imperfect proxy for time processes relevant to ILS; time since leaving care and care history (e.g., duration in care, placement stability, and transitions) may shape trajectories and help clarify the patterns seen, including ceiling effects. We therefore plan to examine these in future analyses (and, where appropriate, model age nonlinearly). Future research could examine pre- and postmeasurements, as well as longitudinal data, to better understand how ILS acquisition advances throughout OHC and care-leaving, and its relationship to age-based development.
Practical Implications
The ILS domain scores may be most useful when interpreted as a profile of relative strengths and support needs, rather than as a stand-alone indicator that further support is unnecessary. This profile can support transition planning and aftercare by helping practitioners and young people identify priorities, particularly in domains with greater variation and clearer scope for change. For domains with marked ceiling effects (Health risk management; Domestic and Self-help tasks), high scores should be interpreted cautiously, as they may reflect mastery of basic tasks rather than offering meaningful discrimination among higher-functioning individuals. Ceiling effects indicate that these domains may be less suitable for tracking incremental change among higher-functioning young people. In these domains, scores may function best as a prompt for brief, real-world follow-up discussion about how skills are applied in more complex situations, rather than as a stand-alone signal that support is no longer needed.
Strengths and Limitations
The strengths of this study showcase the robustness of the developed ILS measure, which is underpinned by validated constructs and a thorough psychometric evaluation grounded in the COSMIN taxonomy. Specifically designed for care-experienced young people, the measure accurately captures the development and acquisition of life skills within OHC settings. The innovative co-design and piloting process has significantly enhanced the content validity of the items and the overall measure. Although the lack of repeated measurements prevented testing responsiveness, ongoing longitudinal studies are essential to demonstrate how the measure performs across the life course, particularly for care-leavers. Notably, ceiling effects observed among care-leavers suggest that incorporating more complex or extended constructs could better reflect the skills acquisition of those who have been out of care for some time and have developed ILS outside of OHC. Recognizing these factors is crucial, as current limitations may affect the interpretation of results for care-leavers outside the immediate transition period. Accordingly, researchers using the current version of the ILS in future studies should interpret changes over time with caution in domains affected by ceiling effects.
Several limitations should also be considered. The sample size (N = 122) was modest relative to the initial 42-item instrument and did not meet commonly cited respondent-to-item heuristics for factor analysis, potentially affecting the stability of the factor structure despite subsequent model refinement. In addition, the demographic composition of the sample, including a relatively high proportion of participants identifying as Aboriginal or Torres Strait Islander (32.8%), reflects the service context from which the sample was drawn and may limit the generalizability of the findings to other populations and settings. Replication in larger and more demographically diverse samples, including formal testing of measurement invariance, is therefore recommended.
Future Research
While the ILS measure shows promise, further research is required to establish its responsiveness, diagnostic performance, and measurement invariance across different populations and socio-cultural contexts. There is a need for future studies with larger samples to further validate and strengthen the psychometric properties of the ILS measure, ensure test–retest reliability, and enable analyses using Item Response Theory (IRT) and differential item functioning. These approaches will also allow more in-depth examination of measurement invariance across various subgroups (e.g., gender, cultural background, or care type). Future research involving comparison groups of participants who are not care-experienced, along with convergent validation against other measures, will help build the evidence base. Currently, the measure aligns specifically with the care-experienced population. Validating it against the noncare-experienced peers could demonstrate its wider applicability for future use. Cross-cultural validation in translated and adapted versions of the measure would also increase its generalizability.
As this study was conducted within a longitudinal project, the number of measures administered was limited to minimize participant burden. Consequently, comparisons between the ILS and other measures targeting similar or related constructs, such as self-determination or transition readiness, to establish convergent validity, remain to be addressed. Beyond known-groups hypotheses, future research could further enhance construct validity by examining external convergent and discriminant evidence. For example, expecting moderate positive correlations with transition readiness/self-management (transition readiness assessment questionnaire; Wood et al., 2014) and low or near-zero correlations with theoretically distinct constructs, such as life aspirations or general attitudes and values. When external correlations are based on models, bootstrap confidence intervals can be employed to assess discriminant validity.
Additionally, IRT analyses can be applied to examine item difficulty hierarchies and more precisely identify ceiling effects within the ILS measure. This would inform the development of additional, more challenging items in domains where current items may not adequately capture advanced ILS. Such refinements would enhance the sensitivity of the ILS to both individual differences and changes in skills among care-leavers over time.
Conclusion
This study examined the development and psychometric properties of a new measure of ILS for care-experienced young people, including its structural validity, internal consistency, and hypothesis testing. The ILS measure showed promise in identifying skills that need development in young people both during and after leaving care, providing a tool that OHC providers and stakeholders can use to better measure, manage, and develop targeted ILS programs. Further research is needed to determine the ILS measure's responsiveness, diagnostic performance, and measurement invariance across different populations.
Footnotes
Acknowledgments
The authors would like to acknowledge the contributions of the SIDR partner agencies, as custodians of the data analyzed in this study, and all Western Australian young people whose data contributed to the findings. Before accessing the data, approval was obtained from all relevant data custodians, including the Curtin University HREC (Approval number: HRE2018–0170), the Department of Health HREC, and the Western Australian Aboriginal Health Ethics Committee. The authors do not have permission to share data.
ORCID iDs
Authors Note
This research was conducted while Dr. Michael Starr was at Bath & North East Somerset Council. Dr. Starr is now at Post 16 Service, Bristol City Council.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Australian Research Council (LP170100044), in conjunction with the Government of WA Department of Communities and Wanslea, and the Research Council of Norway (324475).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.