
Abstract
Objectives:
Social workers frequently face verbal aggression. While most studies have focused on long-term consequences of these encounters, this study examined how verbal aggression influences perceived acute stress and behavioral performance in social workers during these situations.
Method:
Twenty-seven participants engaged in scenarios with a trained actor portraying service user under either low or high verbal aggression conditions. Psychophysiological responses were measured during and following each scenario. Behavioral performance was evaluated by two experienced raters using a standardized checklist.
Results:
High verbal aggression elicited significantly higher cognitive and somatic anxiety, greater mental effort, increased heart rate, and reduced self-confidence compared to low aggression. Performance quality, including empathy and active listening, declined under high aggression.
Conclusions:
Exposure to verbal aggression heightens acute stress and impairs social workers’ performance. Current training may be insufficient to mitigate these effects, as the trained skills degrade under pressure.
Social work is a profession in which practitioners often find themselves in emotionally charged and high-stakes situations. Such situations may include informing a homeless individual that they can no longer stay in the shelter or telling an ex-convict that their court obligations are not being met, risking a return to prison. These situations highlight the crucial and impactful role social workers play in contact with service users during challenging moments (Munobwa et al., 2023; Robson et al., 2014; Videl-Marti & Ruiz Bueno, 2024). Therefore, the nature of social work can be intense, making social workers targets of frustration, hostility, or aggression (i.e., behaviors intended to cause physical or psychological harm; Thirer, 1993). Aggression can manifest as verbal abuse, threats, intimidation, or physical assault, which may threaten the well-being of social workers and compromise professional relationships and service delivery. In the Netherlands, for example, 67% of social workers report experiencing aggression in the workplace, predominantly from service users (Ipsos, 2021).
So far, research has focused predominantly on the long-term consequences of aggression in social workers. For example, encountering aggression during work leads to emotional distress, anxiety, reduced job satisfaction, and increased turnover intentions (Dowling & Banka, 2020; Lamothe et al., 2018; Schablon et al., 2018). Also, after being confronted with aggression, social workers may respond by trivializing or rationalizing such situations, and in some cases by denying them altogether (Enosh et al., 2012; Lamothe et al., 2018; Newhill, 2003). Others rely on avoidance-oriented responses, such as lowering expectations of service users progress or shifting responsibility, which may provide temporary relief but ultimately foster negative long-term consequences (Astvik et al., 2014; Shin, 2011). Such coping patterns lead to diminished professional effectiveness and a higher risk of stress-related absenteeism (Tuck, 2013). Given the high prevalence and substantial impact of aggression, strategies to mitigate its risks and support practitioners in their roles are desirable (Dowling & Banka, 2020; Dulatkyzy, 2023; Enosh & Tzafrir, 2015; Virkki, 2008a, 2008b; Vogus et al., 2016). In order to improve such strategies, it is useful to analyze the behavioral patterns in such (social work) situations. Helping practitioners perform well in the moment, rather than only cope afterwards, can significantly shape the immediate course of social worker–service user interactions.
Social workers are expected to maintain professional conduct under conditions of aggression and intense emotions (Lamothe et al., 2018). They must remain composed, assertive, and communicative, working to de-escalate conflict and safeguard all involved (Øien & Lillevik, 2014). Evidence indicates, however, that the effectiveness of de-escalation skills may be compromised when social workers experience heightened stress or emotional strain (Keesman & Weenink, 2020). Acute stress can impair performance not only through heightened emotional arousal but particularly in tasks that are predominantly cognitive, such as verbally setting limits by indicating that the service user must stop threatening the social worker. Under acute stress, cognitive functions that are essential for these tasks—including attention, working memory, impulse control, and perspective-taking—deteriorate and increase the risk of errors and ineffective interactions (Nieuwenhuys & Oudejans, 2017).
A central factor in these acute stress responses is anxiety, which often emerges as the dominant emotional reaction in high-stakes social work interactions (Robinson, 1990). Following the integrated model of anxiety and perceptual–motor performance (Nieuwenhuys & Oudejans, 2012, 2017), attentional focus may shift away from task-relevant stimuli to threat-related stimuli when anxiety is experienced. Consequently, a social worker may be more distracted by the aggressive behaviors of the service user rather than focusing on what steps to take to de-escalate the situation, such as verbal boundary setting or emotional self-regulation. Research in other performance contexts, such as sports and police work, has repeatedly shown the negative effects of acute anxiety on performance (Andersen et al., 2016; Giessing et al., 2019; Oudejans, 2008; Sandel et al., 2024; Taverniers et al., 2011). To further understand these effects, researchers have examined how exposure to realistic and controlled scenarios influences anxiety levels and task performance. Such experimental designs provide valuable insights into how acute stress impacts professionals’ cognitive and behavioral functioning (Di Nota & Huhta, 2019). These findings are particularly relevant to police work, where officers are also required to maintain composure, communicate effectively, and make rapid decisions under pressure (Anderson et al., 2019; Renden et al., 2017).
Similar stress-related mechanisms are likely to operate in other high-demand professions, such as social work. If verbal aggression significantly increases perceived stress and impairs performance in social workers, targeted interventions could mitigate these effects, improving both practitioner well-being and service quality. Therefore, this study examines how verbal aggression affects social workers in realistic simulated scenarios. We assess acute stress responses and concurrent task performance during service-user interactions enacted by a professional training actor under low and high verbal aggression conditions. We hypothesize that higher levels of verbal aggression, compared to lower levels, will lead to: H1) higher cognitive anxiety, greater mental effort, higher physiological arousal, and lower self-confidence; H2) lower performance on task performance, defined as the use of de-escalation skills such as verbal limit-setting, maintaining composure, and communication with service users.
Method
Participants Recruitment
Participants were recruited through professional networks, social work organizations, and educational programs. In addition, a recruitment call was posted on LinkedIn, accompanied by a short informational video in which the first author explained the purpose and procedure of the study. Interested individuals could register directly in response to this call. Participation was voluntary and unpaid. All participants provided written informed consent. The study was approved by the institutional ethics committee of the first author.
Design
The study employed a one-group pretest-posttest repeated measures design. All participants completed scenarios in three conditions: low verbal aggression (LVA), high verbal aggression (HVA), and cooperative interaction (CI). The CI condition served as a neutral comparison to reduce expectation effects and was not included in the analyses. Each participant completed two scenarios per condition, resulting in six scenarios in total. To introduce some contextual variation, half of the scenarios took place in a simulated living room and half in a simulated consultation room, with one scenario per condition in each setting. Photographic examples of the simulated consultation room and living room settings are presented in Figures 1 and 2.
Photographic example of the consultation room.

Photographic example of the living room.
Participants interacted with a professional training actor (male, 65 years old) who portrayed a service user. The actor displayed scripted behavior corresponding to each condition. In the LVA condition, the actor expressed mild irritation without overt hostility. In the HVA condition, the actor raised his voice, interrupted the participant, and prevented them from finishing their sentences. No physical aggression occurred, although indirect aggressive behaviors toward objects (e.g., slamming a chair or hitting a table) were included. In the CI condition, the actor responded in a calm and cooperative manner. An overview of the scenario manipulation per verbal aggression condition is presented in Table 1. Standardized scenario scripts were used to ensure consistency across conditions and are available from the corresponding author upon reasonable request.
Overview of Scenario Manipulation Per Verbal Aggression Condition.
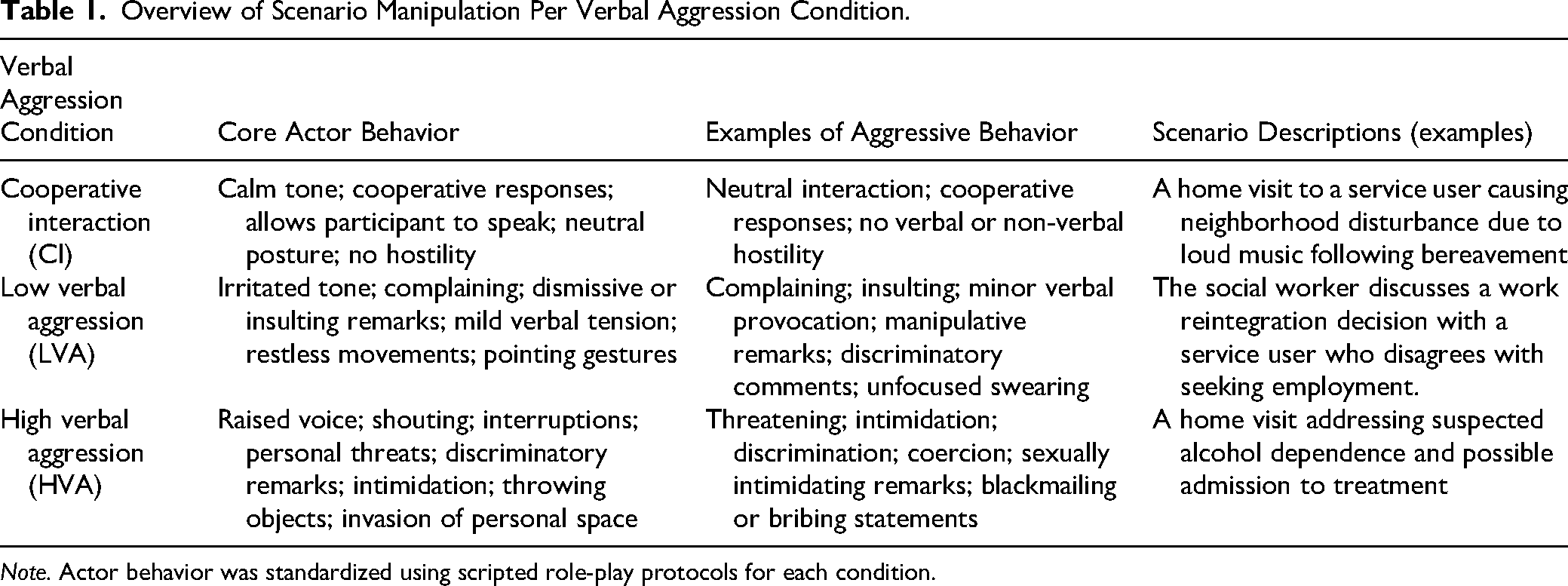
Note. Actor behavior was standardized using scripted role-play protocols for each condition.
Measures
Trait Anxiety
To account for baseline variations in anxiety that may influence responses to threatening situations (Nieuwenhuys & Oudejans, 2012, 2017), trait anxiety was assessed using the Dutch version of the Trait scale of the State–Trait Anxiety Inventory (STAI-DY2; Spielberger et al., 1983; van der Ploeg et al., 1981). The questionnaire consists of 20 statements (e.g., “I feel safe,” “I feel rested”) rated on a 4-point Likert scale ranging from almost never to almost always. Previous research has demonstrated high internal consistency for the Trait scale, with Cronbach's α typically above .90 (Spielberger et al., 1983; van der Ploeg et al., 1981). This assessment was included to confirm that participants’ trait anxiety scores fell within the normative range for adults, ensuring that anxiety levels reported during the study were primarily the result of the verbal aggression manipulation rather than dispositional tendencies to respond with elevated anxiety.
Psychological Responses
To assess whether the LVA and HVA conditions led to increased perceived stress responses, various questionnaires and measurements were administered. Participants’ cognitive anxiety, somatic anxiety, and self-confidence were measured using a Dutch translation of the Mental Readiness Form-Likert (MRF-L) by Krane (1994). This instrument is a simplified version of the CSAI-2 questionnaire (Martens et al., 1990), and assesses each construct with a single item, allowing rapid assessment immediately after each scenario. Participants rated three 11-point Likert scales: cognitive anxiety (“My thoughts are… not worried—worried”), somatic anxiety (“My body is… not tense—tense”), and self-confidence (“I feel… not confident—confident”). Prior research has demonstrated adequate validity of the MRF-L, with correlations of r = .76 for cognitive anxiety, r = .69 for somatic anxiety, and r = –.68 for self-confidence with the CSAI-2 (Krane, 1994).
Additionally, as an indirect measure of stress and anxiety, participants completed the Rating Scale Mental Effort (RSME; Zijlstra, 1993), a single-item visual analogue scale that measures the amount of mental effort required to complete a task. The scale ranges from 0 (no effort at all) to 150 (extreme effort), with verbal anchors provided at intermediate points (30 = a little effort, 65 = some effort, 100 = much effort, 115 = very much effort). The RSME has demonstrated good test–retest reliability (0.78 in work environments and 0.88 in laboratory settings; Zijlstra, 1993) and has been applied in multiple previous studies on effects of stress and anxiety of performance (police officers; e.g., Nieuwenhuys et al., 2009; Renden et al., 2014, 2017).
Physiological Responses
As heart rate tends to increase in stressful situations due to activation of the autonomic nervous system (Anderson et al., 2002), participants’ average and peak heart rates were recorded, using the POLAR H10 heart rate sensor sampling at 1 Hz. Heart rate was measured in beats per minute during the entire duration of each scenario.
Performance
Participants’ performance was assessed based on video recordings of the scenarios. Videos were captured from multiple angles using two GoPro HERO 7 Black cameras manually operated by the researchers. Following the experiment, the videos were uploaded to a custom-designed evaluation tool built within the Qualtrics XM platform (Qualtrics, Provo, UT) to provide online access for the independent raters. The interface of this Qualtrics-based performance assessment tool is shown in Figure 3.The performance evaluations were conducted by two independent raters—a lecturer in Mental Health Nursing and a senior care manager at a mental health organization, both with over 10 years of experience in social work. The inter-rater reliability was adequate, with Kendall's coefficient of concordance w = 0.62, p = .039, indicating satisfactory agreement between the two assessors (van Rossum & Gagné, 1994). Intra-rater reliability was also good: the primary assessor re-evaluated the LVA and HVA conditions of four participants (16 videos total), with linear weighted Cohen's Kappa yielding w = 0.58, p < .001.
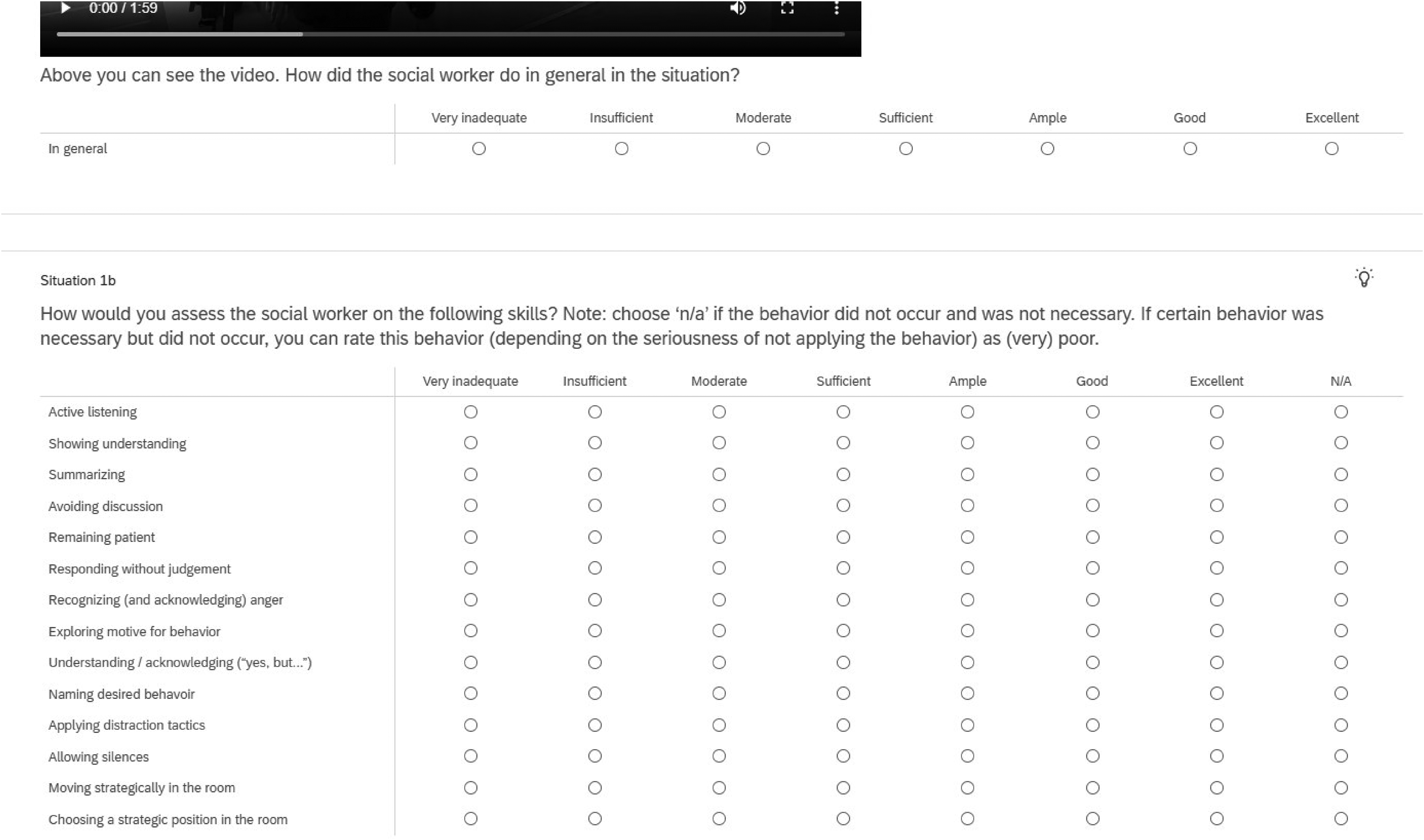
Screenshot of the Qualtrics-based assessment tool used to rate social workers’ de-escalation performance in simulated scenarios.
Task performance was assessed by the application of de-escalation skills commonly trained among social workers in the Netherlands. Participants were expected to apply these professional de-escalation skills during the scenarios, as operationalized in the performance indicators presented in Table 2. An initial pool of behavioral performance indicators was derived from a review of core competencies emphasized in Dutch aggression management training programs and refined through expert consultations with experienced aggression de-escalation trainers. From this pool, a final set of 15 performance indicators was distilled and operationalized to constitute the performance assessment tool.
Initial Pool of De-Escalation Performance Indicators.
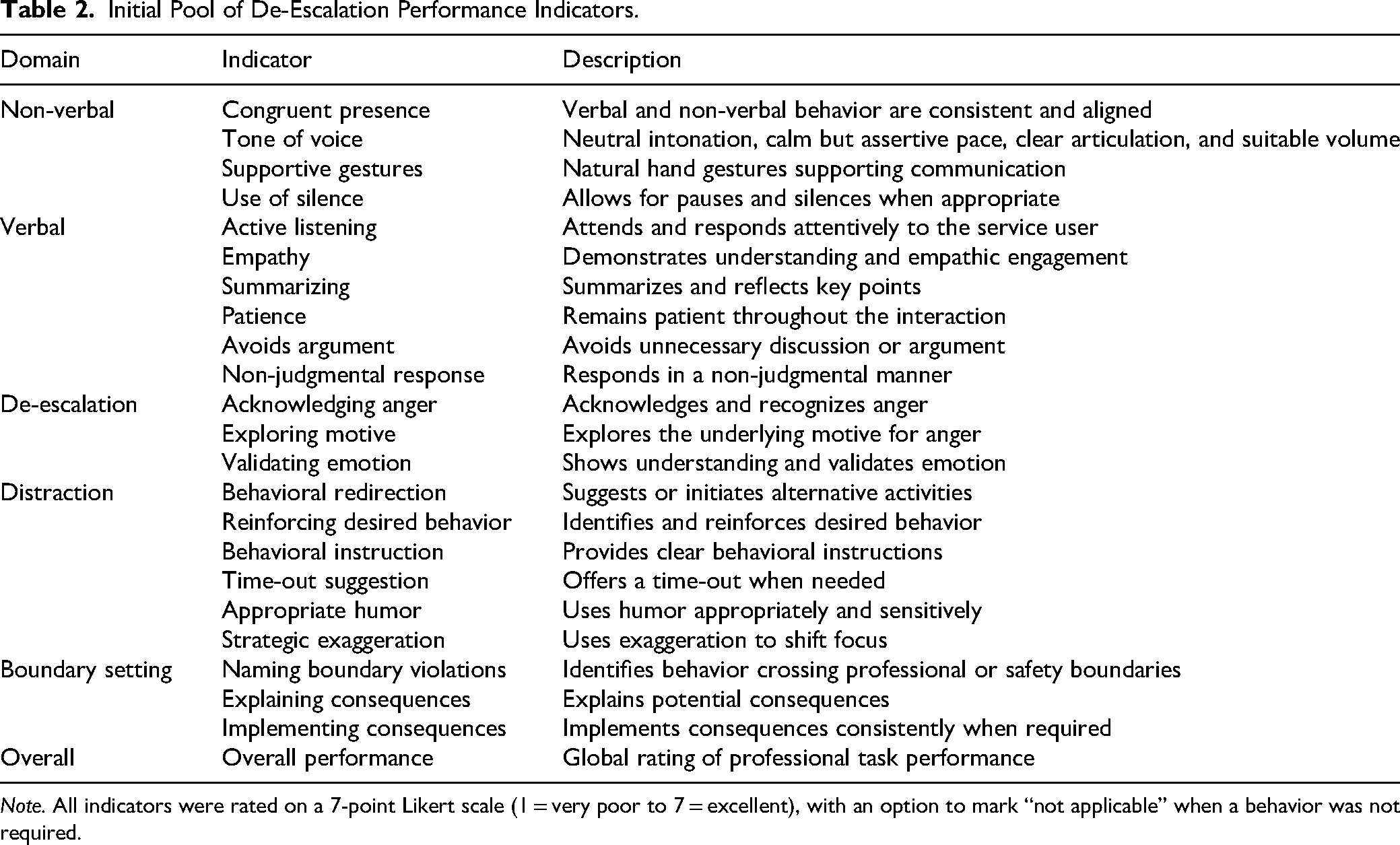
Note. All indicators were rated on a 7-point Likert scale (1 = very poor to 7 = excellent), with an option to mark “not applicable” when a behavior was not required.
Participants’ performance was rated on these 15 specific indicators and one overall performance indicator using a 7-point Likert scale ranging from very poor to excellent, with the option to mark “not applicable” if a skill was unnecessary. Scores below 4 indicated insufficient skill mastery. The assessors rated the first participant together to reach consensus. Inter- and intra-rater reliability were evaluated using Kendall's coefficient of concordance and linear weighted Cohen's Kappa, respectively. For Cohen's Kappa, values around 0.40 are considered to indicate moderate agreement, while values above 0.75 reflect excellent agreement (Brashear et al., 2002). In the present study, the intra-rater reliability was kw = 0.58, p < .001, indicating good agreement.
Experience Questionnaire
To evaluate the realism of the scenarios, participants’ perceptions of their performance, and usefulness of such scenarios for potential training interventions, a seven-item experience questionnaire was administered at the end of the last scenario. The questionnaire included items, for example, that asked participants about how realistic the scenarios were (i.e., The scenarios were realistic for what I experience in the field, I would like to receive training in which realistic scenarios like the one in this experiment are practiced), and how they perceived their performance in each scenario. All items were rated using a 5-point Likert scale (1 = “strongly disagree,” 5 = “strongly agree”).
Procedure
The experiment was conducted in a simulated living room and a simulated consultation room at the first author's institution. Upon arrival, participants received instructions, completed consent forms and questionnaires (Trait Anxiety, Demographic, MRF-L) and were fitted with heart rate. Next the participants performed the six scenarios. A safety coach (lead researcher) monitored the sessions, and either party could call “break” to pause (break was used twice when participants found the scenarios emotionally challenging). After each scenario, participants reported stress levels and mental effort and confirmed comfort before proceeding. Upon completion, they filled out a feedback questionnaire about their experience (see Figure 4 for a schematic overview of the procedure).
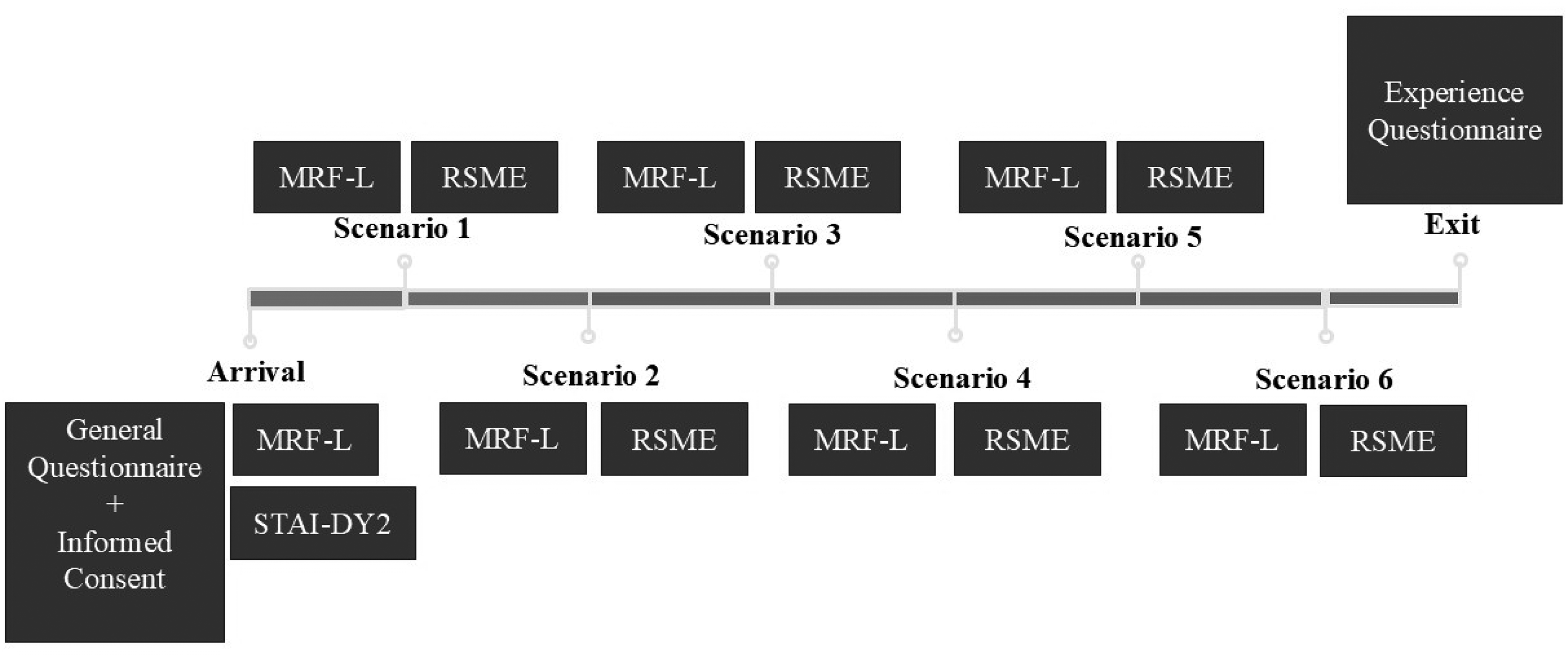
Scheme procedure experiment.
Data Analysis
Descriptive statistics (means, standard deviations, and ranges) were computed for the Trait scale of the State–Trait Anxiety Inventory (STAI) to verify comparability with normative data (van der Ploeg et al., 1981). This step was taken to ensure that observed stress responses during the task could not be attributed to dispositional characteristics of the participants.
To evaluate the study hypotheses, paired-samples t-tests were conducted comparing LVA and HVA conditions on cognitive anxiety, somatic anxiety, self-confidence, mental effort, and both mean and peak heart rate. Additional paired-samples t-tests were performed to examine differences in task performance between the LVA and HVA conditions, including the overall performance score and the specific behavioral indicators (see Table 4). For all paired comparisons, cases with missing data on either score of a pair were excluded from the relevant analysis using pairwise deletion. Two behavioral indicators (“Summarizing” and “Allowing Silences”) could not be analyzed due to an insufficient number of complete observations; results for these variables are therefore not reported and should be interpreted with caution.
Assumptions underlying the paired-samples t-tests, including normality and the presence of outliers, were assessed prior to analysis. Effect sizes were calculated using Cohen's d for dependent samples (Cohen, 1988; Lakens, 2013), with values of 0.20, 0.50, and 0.80 interpreted as small, medium, and large effects, respectively. Finally, data from the experience questionnaire was analyzed using descriptive statistics to provide additional insight into participants’ subjective experiences during the task.
Results
Participants Characteristics
Twenty-eight social workers were recruited; however, data from one participant were excluded because the participant did not complete the procedure, leaving a final sample of 27 participants (13 men and 14 women, mean age = 35.7 years, SD = 5.98). Most participants held a bachelor's degree in social work (n = 16), with others having completed a vocational degree in Social Work (n = 3), a master's in Social Work (n = 3), a bachelor's/master's in Pedagogy (n = 3), a degree in Drama Therapy (n = 1), or a master's in Psychology (n = 1). Fourteen participants were actively working in the field, while 13 were employed as educators (former social workers with experience in handling aggression situations). The average work experience was 9.6 years (SD = 5.9).
Preliminary Analyses
Descriptive statistics indicated a mean Trait Anxiety score of M = 32.11 (SD = 4.79), with a 95% confidence interval ranging from 30.22 to 34.01. This mean was lower than the Dutch normative value (M = 37.3; van der Ploeg et al., 1981), indicating relatively low baseline anxiety levels in the sample. No participants showed clinically elevated trait anxiety, and all 27 participants were therefore included in the analysis.
Psychophysiological Responses
Hypothesis 1 predicted higher cognitive and somatic anxiety, greater mental effort and physiological arousal, and lower self-confidence under HVA compared to LVA. The paired t-tests showed significant differences in mean scores between conditions for cognitive anxiety, somatic anxiety, self-confidence, mental effort, average heart rate, and peak heart rate (ps ≤ .046, see Table 3). All effects were in the expected direction. A small effect was found for cognitive anxiety (d = −0.48), and peak hearth rate (d = −0.40). Large effects were observed for somatic anxiety, self-confidence, and mental effort (ds ≥ −0.92). Together, these results confirm the hypothesis that higher levels of aggression lead to higher levels of acute stress.
Stress Variables Under Low Verbal and High Verbal Aggression Conditions (n = 27).
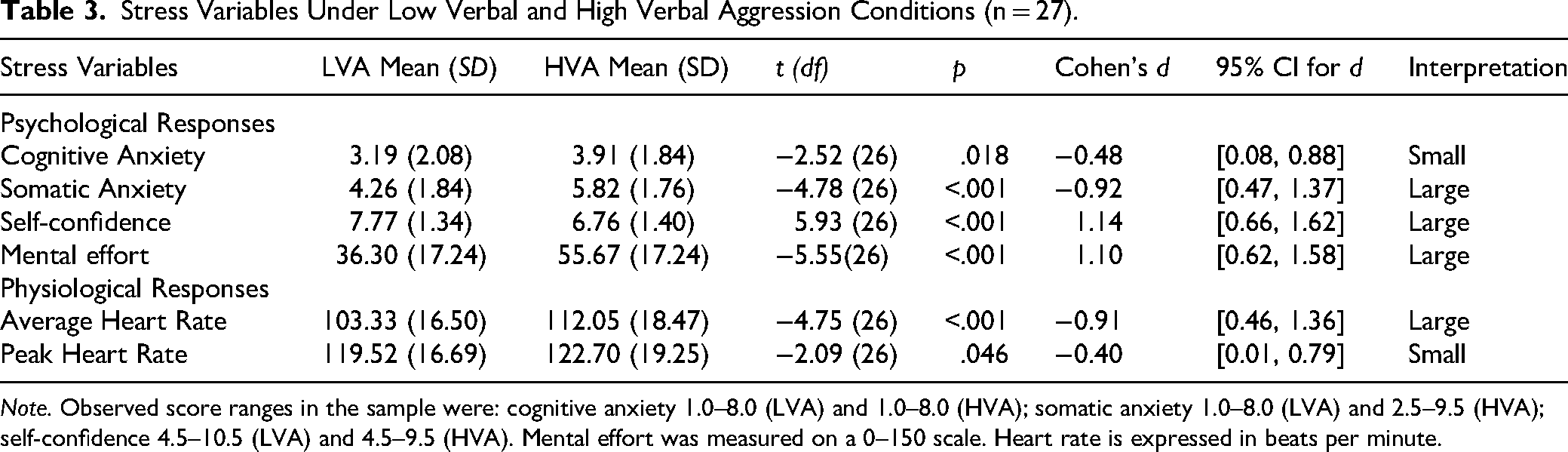
Note. Observed score ranges in the sample were: cognitive anxiety 1.0–8.0 (LVA) and 1.0–8.0 (HVA); somatic anxiety 1.0–8.0 (LVA) and 2.5–9.5 (HVA); self-confidence 4.5–10.5 (LVA) and 4.5–9.5 (HVA). Mental effort was measured on a 0–150 scale. Heart rate is expressed in beats per minute.
Performance
Hypothesis 2 predicted lower professional task performance under HVA compared to LVA. The paired samples t-tests showed that, as predicted, the overall performance scores were lower in the HVA compared to the LVA condition. This decline in performance was statistically significant with a large effect size (p < .001, d = 1.63, see Table 4). Furthermore, in the HVA condition, participants consistently showed lower scores on nearly all performance indicators compared to the LVA condition. For instance, active listening was significantly reduced under HVA aggression relative to the LVA condition, indicating a large effect (t(26) = 10.63, p < .001, d = 2.05).
Performance Indicators Under Low Verbal and High Verbal Aggression Conditions (n = 27).
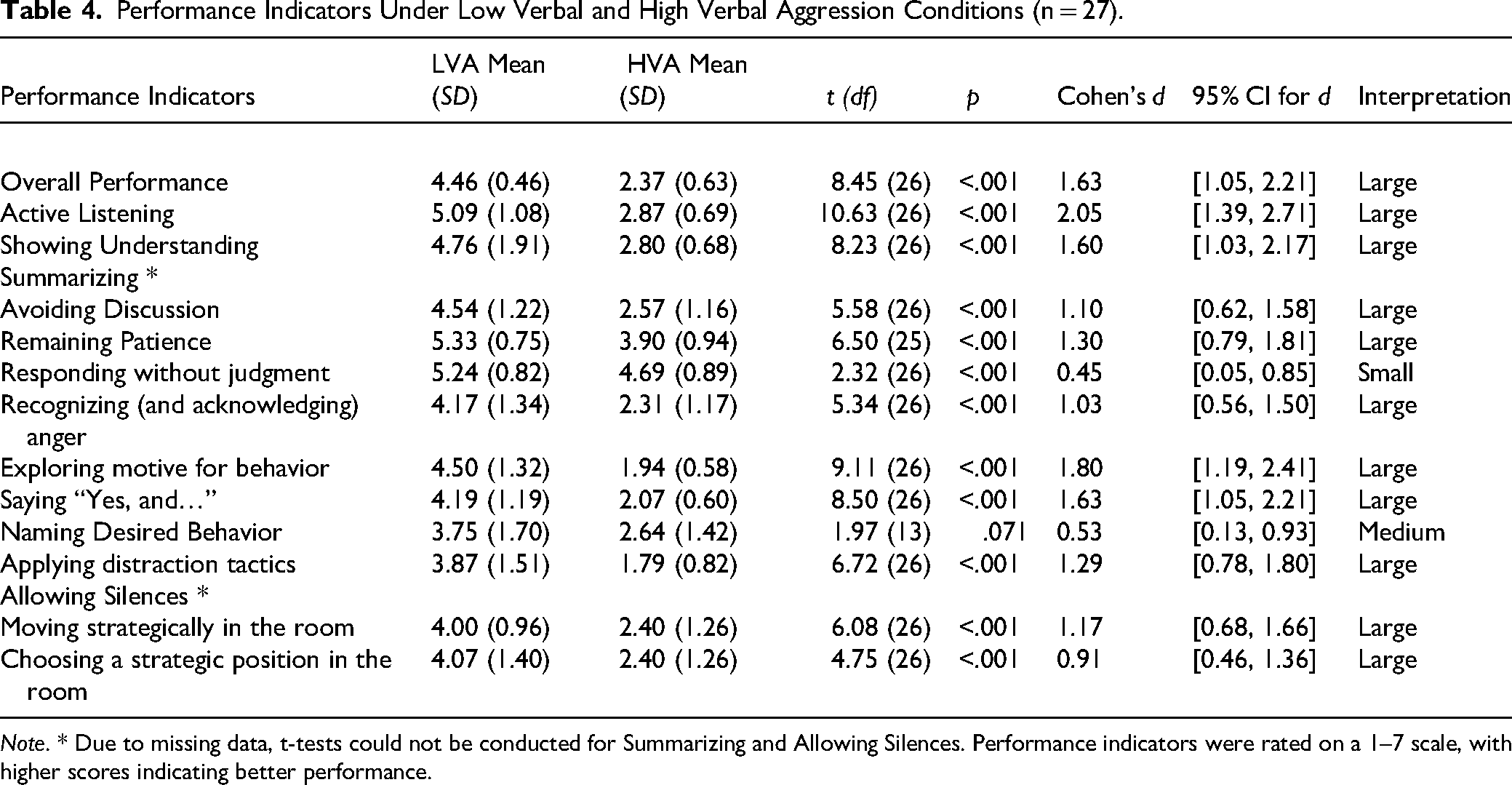
Note. * Due to missing data, t-tests could not be conducted for Summarizing and Allowing Silences. Performance indicators were rated on a 1–7 scale, with higher scores indicating better performance.
Similar patterns were observed for showing understanding, avoiding discussion, remaining patient, recognizing anger, exploring motives for behavior, applying “Yes, and…,” using distraction tactics, and moving or positioning strategically in the room, all accompanied by large effect sizes (ds > 0.90). Responding without judgment also scored significantly lower under high aggression (p < .001) but with a small effect size (d = 0.45). Naming desired behavior showed a medium-sized but non-significant effect due to the relatively small sample size (p = .071, d = 0.53). Given that the vast majority of tests indicate large effect sizes, we refrained from implementing corrections for multiple tests to the p-values as we did not see grounds for Type-I error inflation. Overall, our hypothesis that acute stress reduces performance was confirmed.
Experience Questionnaire
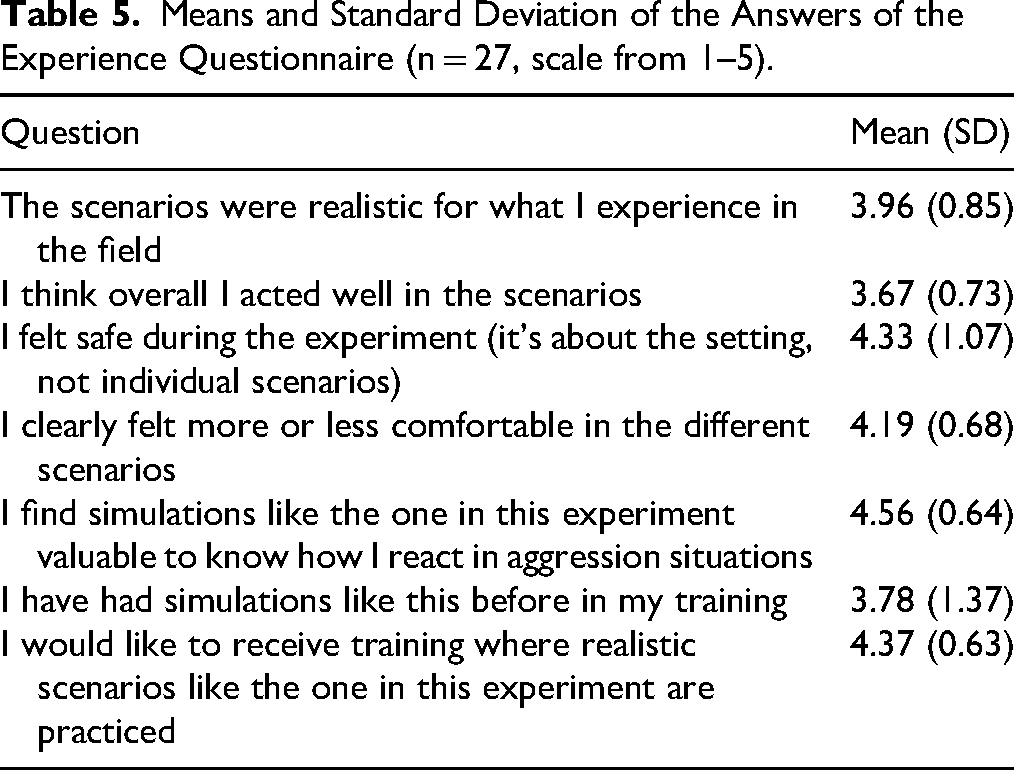
The most striking result from the experience questionnaire was that participants perceived the scenarios as realistic (see Table 5). In contrast to the behavioral observation, which showed impaired performance under HVA, participants evaluated their own performance as reasonably good. Furthermore, participants indicated that they would like to train more with realistic scenarios.
Means and Standard Deviation of the Answers of the Experience Questionnaire (n = 27, scale from 1–5).
Discussion and Application to Practice
Social workers frequently encounter interactions that involve verbal aggression, which can compromise their well-being and impair professional performance (Munobwa et al., 2023). Despite the high prevalence of such incidents, few experimental studies have systematically explored the immediate impact of verbal aggression on social workers’ stress responses and task effectiveness (Robson et al., 2014; Videl-Marti & Ruiz Bueno, 2024). Therefore, in the present study we investigated whether verbal aggression induces acute stress responses in social workers, and whether these stress responses are accompanied by concurrent decrements in task performance. By examining both stress indicators and behavioral performance within the same simulated interactions, the study provides an integrated account of how aggression affects social workers in the moment. Building on research in other high-demand professions, we hypothesized that higher levels of verbal aggression would result in (a) increased anxiety, mental effort, and physiological arousal, accompanied by reduced self-confidence, and (b) consequently lower performance on professional tasks, compared to exposure to LVA.
In line with these hypotheses, our results confirm that social workers responded with acute stress to high levels of verbal aggression, which impaired their ability to effectively apply their professional skills. In other words, with HVA, stress responses were higher than with LVA and accompanied by lower levels of task performance. This is consistent with previous research, across domains such as law enforcement and healthcare, which shows that elevated stress can hinder performance in demanding interpersonal situations (Dijkstra et al., 2024; Renden et al., 2017). Social workers’ professional skills also seem vulnerable to stress. In line with the integrated model of anxiety and perceptual-motor performance (Nieuwenhuys & Oudejans, 2012, 2017), acute stress may lead to a shift from goal-directed attention to stimulus-driven attention with more attention toward task-irrelevant cues, consequently disrupting the cognitive and emotional regulation processes required for professional functioning.
Interestingly, there seemed to be a discrepancy between perceived and actual performance. While the social workers rated their own performance as satisfactory, a decline was observed by the raters under HVA. Similar patterns have also been observed in other high-stress training contexts. For example, in immersive mass casualty incident training using virtual reality, self-reported performance did not correlate with objective performance indicators, suggesting that individuals may struggle to accurately access their competence in the absence of social or temporal benchmarks (Baetzner et al., 2025). From a psychological perspective, this misalignment can be interpreted as a form of cognitive dissonance, in which individuals maintain a positive self-concept despite evidence to the contrary (Cooper, 2007; Festinger, 1957; Harmon-Jones & Mills, 2019). In the context of social work, professionals may perceive themselves as coping effectively under verbal aggression, even when objective measures reveal impairments in critical interpersonal skills.
Altogether, the current findings suggest that targeted training interventions may be needed to prevent declines in de-escalation performance when social workers are confronted with aggression. What those trainings would look like is an open question. Exposure to elevated levels of stress in controlled training situations appears crucial for preparing professionals to function effectively under comparable real-world conditions, a finding that aligns with evidence from sports and law enforcement, where pressure training has similarly been shown to enhance performance under pressure (Kegelaers & Oudejans, 2022; Nieuwenhuys & Oudejans, 2011; Renden et al., 2017). Such training enables individuals to experience physiological and cognitive stress responses in a safe environment, helping them to recognize their own stress reactions and practice their professional skills under pressure (Dijkstra et al., 2025; Hill et al., 2024). Given that participants attached a high degree of realism to the scenarios developed for this study, they may provide an empirically grounded starting point for future training under pressure. Educational social work programs should consider integrating such training into their curricula when they educate social workers that are going to work in the field (see Dijkstra et al. (2025) for examples in healthcare). Future research is needed to evaluate the effectiveness of pressure training interventions in the domain of social work.
The procedure used in this study may also be applicable in other social work contexts in which professionals regularly encounter aggression or emotionally charged confrontational interactions. In the present study, the scenario scripts were developed based on situations commonly addressed in Dutch social work education and training, thereby enhancing ecological validity and ensuring that scenarios were recognizable to participants. Potential settings for future studies include child protection services, community mental health teams, domestic violence response services, debt counseling, and municipal front-office services. For example, in child protection services, a realistic scenario might involve a social worker discussing concerns about suspected child abuse with a parent. Replication in other contexts or countries therefore requires adapting the scenarios to context-specific service user concerns, professional roles, and training practices. In addition, the use of professionally trained actors, clear safety protocols, and ethical procedures for managing potential participant distress are essential when implementing realistic aggression simulations (Andersen et al., 2016; Baetzner et al., 2025). Researchers and training developers seeking to replicate this approach should carefully tailor scenarios to the target practice context while ensuring adequate safeguards for participant well-being.
The present study has two limitations that should be acknowledged. First, the performance of the social workers was scored based on video footage by raters. The inter- and intrarater reliability were acceptable (W = 0.62 and kw = 0.58, respectively). The score was established after a single consensus meeting, which could potentially be improved through a more consensus-oriented procedure involving multiple rater meetings. Second, although actor-based simulations provided controlled and ecologically valid scenarios, they cannot fully capture the complexity and unpredictability of real-world service users’ interactions. Future research could explore longitudinal effects of repeated exposure to verbal aggression, examine coping strategies that mitigate stress and performance decline, and investigate diverse social work populations and settings.
To conclude, social workers in HVA situations experienced more stress, which was accompanied by lower performance levels of de-escalation skills. These findings align with research in related professional fields, such as law enforcement. The results indicated that practicing with realistic scenarios may help maintain de-escalation skills in high stress conditions, which can help prevent or reduce performance decline in aggression situations.
Footnotes
Acknowledgments
We gratefully acknowledge Arjan Doolaar, information specialist at the HAN Library, HAN University of Applied Sciences, for his extensive support in reviewing and improving the manuscript's adherence to APA guidelines and reference formatting.
Ethical Considerations
This study involved human participants and was approved by the ethics committee of the HAN University of Applied Sciences. No specific permissions were required for corresponding locations. The employers of all authors had no influence on this manuscript. The study was approved by the ethical committee of the HAN University of Applied Sciences.
Consent for Publication
All authors confirm that written informed consent for publication was obtained from all relevant participants. The written consent forms are held by the authors and will be made available to the journal upon request. All authors have reviewed and approved the final manuscript and consent to its publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.