
Abstract
Keywords
Young People Experiencing Homelessness are Particularly Vulnerable
Young people experiencing homelessness are among the most vulnerable populations, often having experienced significant adversity such as abuse, neglect, and persistent family conflict or instability (Hyde, 2005; Tyler & Schmitz, 2013). Those with experience in out-of-home care— particularly young people who are transitioning to independence—as well as young people involved in the juvenile justice system, face substantially higher risks of homelessness (Fowler et al., 2017; Kushel et al., 2007; Shah et al., 2017). This risk increases further for those involved in both systems (Narendorf et al., 2020). Certain demographic groups—particularly First Nations youth, gender and sexual minorities, and young people with disabilities—are overrepresented amongst those experiencing homelessness (Collins et al., 2018; Grattan et al., 2022; McCann & Brown, 2019). Many young people experiencing homelessness also exhibit high levels of psychological distress, and may have diagnosed or undiagnosed mental health conditions and/or substance use issues (Davies & Allen, 2017).
Homelessness can have a profound impact on young people's physical and mental health and wellbeing (Boivin et al., 2005; Kidd et al., 2016; Toolis & Hammack, 2015). As homelessness persists, young people often rely more on emergency services and become increasingly estranged from family, support networks, and mainstream support services—further compromising their mental and physical health (Mayock et al., 2013). Extended periods of homelessness heighten exposure to violence, exploitation or risky behaviors (Barman-Adhikari et al., 2016; Heerde et al., 2015), and without adequate support, many face persistent housing instability into adulthood (Parpouchi et al., 2021).
Existing Approaches to Supporting Homeless Youth
A range of service models have been developed to prevent and respond to youth homelessness, reflecting its multiple and intersecting causes. Young people experiencing homelessness face distinct developmental, social, and legal challenges that require tailored solutions different from those used with adults (Gaetz, 2014). Current interventions include: (a) homelessness prevention programs that identify and support at-risk young people before they become homeless; (b) family-strengthening interventions that improve relationships between young people and their families; (c) transitional, supportive, and subsidized housing programs that provide temporary or permanent housing with varying levels of support; (d) counseling and treatment addressing health-related or therapeutic needs; (e) non-housing case management and individualized supports to help young people navigate systems and services; (f) economic and employment interventions that build skills, job-readiness, and provide employment placements; and (g) outreach and service-connection efforts that engage young people experiencing homelessness and link them with available resources. These interventions may be provided individually or in combination (Morton et al., 2020).
Housing First approaches—models that prioritize rapid access to permanent housing without preconditions such as treatment compliance or abstinence, with optional and flexible support services—have demonstrated improved housing (Woodhall-Melnik & Dunn, 2016), health (Baxter et al., 2019), and criminal justice (Leclair et al., 2019) outcomes among adults, and show a positive return on investment (Jacob et al., 2022). However, evidence of their effectiveness for young people—and the adaptations required for successful implementation with this population—remain limited.
Mechanisms of Housing and Support Interventions
Neither housing nor support services alone can typically meet the complex needs of young people experiencing homelessness (Morton et al., 2020). Addressing youth homelessness effectively requires combining both elements to provide a stable foundation from which young people can address other aspects of their lives.
Housing interventions range from temporary or transitional housing to permanent supported housing (PSH). The primary goal is to provide safe, affordable, and appropriate accommodation that considers the youth's age, developmental stage, needs, and abilities (Gaetz, 2017). PSH offers ongoing housing with no set time limits, aiming for sustained tenancies (Baxter et al., 2019; Semborski et al., 2021). This stability allows young people to focus on their health, relationships, personal development, education, and employment without the immediate stress of housing insecurity (Carnemolla & Skinner, 2021).
Support services address needs beyond accommodation, whether provided alongside housing or independently. These services typically include case management, counseling, mental health or psychological assistance, independent living or life skills development, transportation assistance, employment skills training and coaching, educational support, and personalized advice or mentoring (Gaetz, 2014, 2017; Gaetz et al., 2021; Kozloff, Adair, Palma Lazgare, et al., 2016). These services aim to promote social and community integration, support mental health and substance use issues, and enhance overall well-being. By addressing these various aspects, support services help develop the independent living skills necessary for long-term stability (Alves & Roggenbuck, 2021; Parsell et al., 2015).
Interventions that combine housing and support services models vary in their underlying philosophies. Some adopt conditional approaches, requiring participation in mental health, substance use treatment or employment services as a precondition for housing. Others, such as Housing First, are grounded in a rights-based philosophy that provides housing without preconditions, emphasizing immediate access and individual choice (Gaetz, 2014; Kozloff, Adair, Palma Lazgare, et al., 2016). The Positive Youth Development approach reflects a strengths-based philosophy that focuses on identifying and nurturing positive factors in young people's lives and environments to promote resilience, competence, and autonomy (Semborski et al., 2021). Rights- and strengths-based frameworks are not mutually exclusive, with interventions commonly drawing on one or both.
Considering Intervention Components and Their Implementation
Housing and support interventions for homeless youth are complex social interventions, comprising multiple interacting components that work together within dynamic service systems (Macnaughton et al., 2015). They are often place-based and adapted to local contexts, reflecting differences in housing markets, service infrastructure, and population needs (Aubry et al., 2015). This complexity can pose challenges for both replication and scaling (Greenwood et al., 2013; Nelson et al., 2013). Identifying which components are common to effective programs can clarify the elements most critical for achieving positive outcomes and inform the design of adaptable, evidence-informed service models (Barth et al., 2012; Chorpita et al., 2005).
Implementing complex housing and support interventions requires consideration of factors beyond the relative effectiveness of different models. The complexity of this population's needs, combined with the resource-intensive nature of providing both housing and support services, creates substantial implementation hurdles (Shelton et al., 2018). Implementation barriers can manifest at various levels—both internal and external to the organization providing the service—and may vary between different contexts (Aarons et al., 2011). Understanding factors that help or hinder implementation is crucial, as even the most promising intervention will fail to achieve its intended outcomes if not implemented effectively (Fixsen et al., 2005).
Why It Is Important To Do This Review
Several reviews have examined the effectiveness of interventions for young people experiencing homelessness (Altena et al., 2010; Carnemolla & Skinner, 2021; Morton et al., 2020; Munthe-Kaas et al., 2018; Wang et al., 2019). However, each of these reviews has important limitations. All examined housing programs and support services as broad, separate groups rather than assessing the effectiveness of models that combine them. Some also included youth alongside older adult populations (Munthe-Kaas et al., 2018). As a result, prior reviews provide little basis for assessing whether approaches that combine housing with other supports are likely to improve outcomes for young people.
Additionally, methodological limitations in some reviews reduce confidence in their findings, including failure to distinguish methods suitable for inferring causality (Altena et al., 2010; Carnemolla & Skinner, 2021; Morton et al., 2020) or assess threats to internal validity through risk of bias assessment (Altena et al., 2010; Morton et al., 2020). No previous reviews have examined either the impact of combined housing and support services or the specific components that constitute these interventions. Our review addresses these gaps by applying stricter methodological criteria and by identifying the core components of included interventions.
In addition, we examine barriers and facilitators to implementation among included interventions. Understanding these factors is important as they can inform assessments of feasibility or appropriateness, support the selection and tailoring of implementation strategies, promote fidelity and sustainability, and guide the development of scalable, evidence-informed service models (Shelton et al., 2018).
Objectives
This review was undertaken to inform the implementation and evaluation of a housing and support services intervention for young people experiencing homelessness, developed by Melbourne City Mission—a community organization in Victoria, Australia, that provides housing, education, and support services to people experiencing disadvantage.
The primary objective was to identify evidence on the effectiveness of interventions that combine housing with other support services in improving housing stability, health and well-being, social connectedness, independence, and economic outcomes among homeless youth. The secondary objectives were to identify: (a) the core components of included interventions; (b) barriers and facilitators to their implementation; and (c) instruments used to measure participant outcomes.
The review was guided by four research questions:
Among young people experiencing homelessness, what housing and support interventions are effective in improving housing stability, health and well-being, social connectedness, independence, and economic outcomes compared to services as usual? What are the components of housing and support interventions for homeless youth? What are the barriers and enablers to implementing housing and support interventions for homeless youth? What instruments are used to measure housing stability, health and well-being, social connectedness, independence, and economic outcomes in studies of housing and support interventions for homeless youth?
Method
Our methods were pre-specified in a protocol registered on OSF (Taylor, Bruce, et al., 2023). Key elements of our methodology are included in this section, with additional detail provided in the supplementary material—including a PRISMA 2020 (Table S1) and SWiM (Table S2) checklist (Taylor et al., 2025).
Selection Criteria
Inclusion and exclusion criteria, organized by Population, Intervention, Comparison, Outcomes, Study design, and Setting (PICOSS) domains, are provided in Table 1.
Inclusion and Exclusion Criteria by PICOSS Domain.
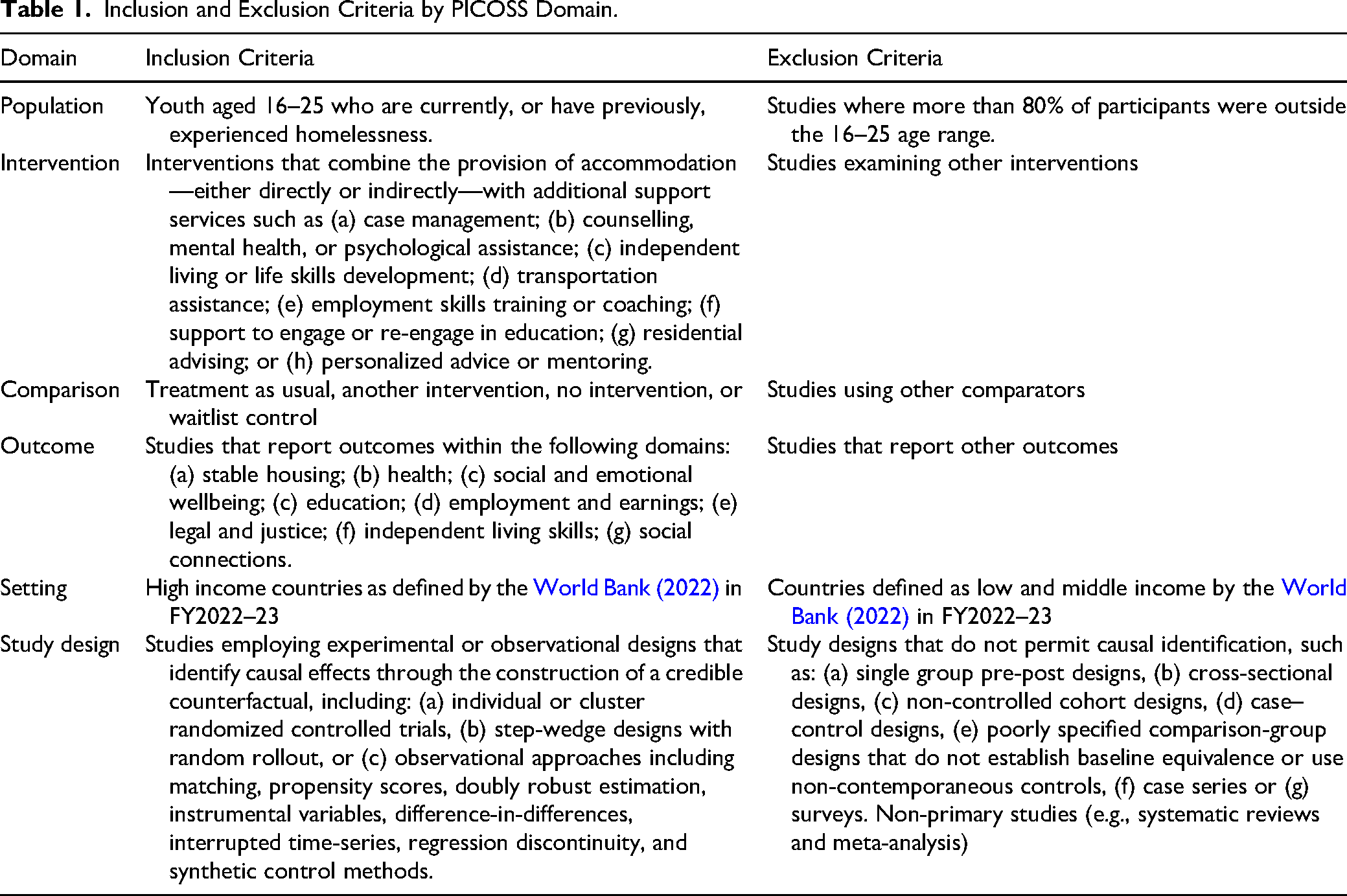
The population of interest was youth aged 16–25 years (inclusive) who are currently or were previously homeless. The age range was selected to align with: (a) the eligibility criteria for MCM's housing and support intervention, and (b) the developmental period of emerging adulthood (Arnett, 2000), during which homelessness can significantly disrupt critical developmental milestones (McDonald et al., 2024).
Eligible interventions combined accommodation provision (directly or indirectly) with additional support services such as case management, coaching or mentoring, counselling, independent living or life skills development and assistance with transportation, employment, or education. Studies could compare interventions with usual services, alternative or no interventions or a waitlist.
Primary outcomes included housing stability, health, social and emotional wellbeing, education, employment and earnings, with secondary outcomes including legal and justice involvement, independent living skills, and social connections. We included both randomized and non-randomized studies that used a counterfactual approach to assess the impact of the intervention.
Search Methods
We searched the following 10 electronic databases with no year of publication or language restrictions: Cochrane CENTRAL Register of Controlled Trials via Ovid (1996 to 7 June 2023); CINAHL via EBSCO (1937 to 7 June 2023); Criminal Justice Abstracts via EBSCO (2010 to 8 June 2023); EMBASE via Ovid (1974 to 8 June 2023); ERIC via ProQuest (1966 to 8 June 2023); APA PsycINFO via Ovid (1806 to 8 June 2023); Ovid MEDLINE (1946 to 8 June 2023); Sociological Abstracts via ProQuest (1952 to 7 June 2023); Social Services Abstracts via ProQuest (1980 to 8 June 2023); Violence and Abuse Abstracts via EBSCO (1995 to 8 June 2023). Search terms and the number of return records for each database are provided in the supplementary material (Table S3).
Gray literature was sourced by reviewing Australian and International clearinghouses, government agencies and organizations known to be undertaking or consolidating research in this area (Australian Housing and Urban Research Institute, Analysis and Policy Observatory database, Australian Criminology Database, Australian Family and Society Abstracts database, Chapin Hall at the University of Chicago and Washington State Institute for Public Policy). Details of the search process for each of these sources is included in the supplementary material (Table S4).
Studies included in reviews by Altena et al. (2010), Wang et al. (2019) and Morton et al. (2020) were also considered for inclusion.
Barriers and enablers to implementation are not typically reported at length in the results of published RCTs or NRSs. We expanded our search to review additional reports of included studies to identify them. These included: study protocols, conference presentations, technical reports, and process/implementation evaluations. Additional reports of included studies were identified by reviewing: (a) reference lists of included studies, (b) trial registries associated with the registration identifier cited in the published article, and (c) other publications by authors of included studies (we examined Google Scholar profiles and university websites).
Data Collection and Extraction
Two reviewers (DT and SV) independently screened each title/abstract identified by the search strategy, with a third reviewer resolving any disagreements (AS and SB). Studies deemed potentially relevant during title/abstract screening underwent full-text assessment by two independent reviewers (DT and SV) using the inclusion and exclusion criteria outlined in the protocol (Taylor, Bruce, et al., 2023). Discrepancies were resolved through discussion with an additional reviewer (SB and AS). Covidence (Veritas Health Innovation, n.d.) and Zotero (Corporation for Digital Scholarship, 2022) were used for deduplication, literature screening, and library storage/referencing, respectively.
The same reviewer pairs (DT and SV) conducted data extraction, with one reviewer extracting data and the second independently verifying all entries. Discrepancies were resolved through discussion. From each paper, we extracted study characteristics, data necessary to convert outcomes to a common effect size for each time point that it was available, details of outcome measurement instruments and information on potential implementation barriers and facilitators. All extracted data were organized and stored in a shared data extraction spreadsheet on Google Sheets. Data extraction templates are provided in the supplementary material (Tables S5 and S6).
Data Analysis and Synthesis
Measures of Treatment Effect
To enable cross-study comparison, reported results were converted to standardized mean difference (SMD) using Borenstein et al.'s (2009) formulas. Hedges’ (1981) correction (g) was applied to account for small-sample bias in Cohen's d. The R code we used for these transformations is available in the supplementary material.
Synthesis of Results
The diversity of outcome measures, assessment timepoints and study designs prevented us from undertaking quantitative synthesis in the form of meta-analysis or regression. Following the SWiM (Synthesis Without Meta-analysis) reporting guideline (Campbell et al., 2020), results were grouped by outcome domain. For each included study, every relevant result at every reported time point was extracted and converted to a standardized effect size (g) and reported in tables. Because studies reported outcomes at different follow-up periods, all available time points were included to capture potential variation in intervention effects over time and avoid presenting a partial picture of results. Results were then narratively synthesized within each domain, describing the outcome constructs assessed, timing, study design, effect size and 95% confidence interval (CI), and the direction of effect. For constructs with a clear normative direction, we indicated whether findings favored the intervention or comparison group; outcomes without an inherent direction (e.g., service costs or utilization) were treated as not directionally interpretable.
We intentionally avoided describing results in terms of statistical significance due to its known limitations in systematic reviews. Consistent with current Cochrane guidance (Higgins et al., 2023), we interpreted findings based on effect sizes and their 95% CIs to convey both magnitude and uncertainty. To aid interpretation, we applied Cohen's (1988) benchmarks—small (g = 0.2), medium (g = 0.5), or large (g = 0.8).
Risk of Bias Assessment
Risk of bias (ROB) in included studies was assessed using the Revised Cochrane Risk of Bias tool for randomized trials (RoB2) (Sterne et al., 2019) or the Risk of Bias In Non-randomized Studies of Interventions (ROBINS-I) (Sterne et al., 2016) for non-randomized studies. A single reviewer (DT or SV) completed each assessment, and a second reviewer independently verified all judgements. Discrepancies were resolved through discussion.
Implementation Analysis
We used the exploration, preparation, implementation, sustainment (EPIS) framework—a conceptual model for implementing evidence-informed practices and interventions—to identify and interpret barriers and enablers to the implementation of included interventions (Aarons et al., 2011; Moullin et al., 2019). EPIS comprises four phases: (1) exploration—identifying needs and assessing interventions; (2) preparation—planning, building capacity, and adapting interventions to context; (3) implementation—operationalizing the intervention with attention to fidelity and local context; and (4) sustainment—integrating the intervention into standard practice and maintaining effectiveness (Aarons et al., 2011; Moullin et al., 2019). A key feature of EPIS is its consideration of both the inner (organizational) and outer (system) contexts at each phase. The outer context includes factors such as service environment, policy, funding, and inter-organizational networks, while the inner context encompasses organizational structures, leadership, and characteristics of the individuals involved (Aarons et al., 2011).
We reviewed all included studies, including any associated publications, to identify author-reported barriers and enablers to implementation. Each barrier and enabler was coded by a single reviewer (SV) according to (a) the EPIS phase to which it most strongly related, (b) whether it pertained to the inner (organizational) or outer (system) context, and (c) whether it concerned housing or support service components, or both. Coding was independently reviewed by two additional reviewers (DT and AS) to ensure accuracy and consistency. A thematic analysis was then conducted to identify cross-cutting themes, grouping similar barriers and enablers within and across EPIS phases.
Assessing Housing First Components of Included Interventions
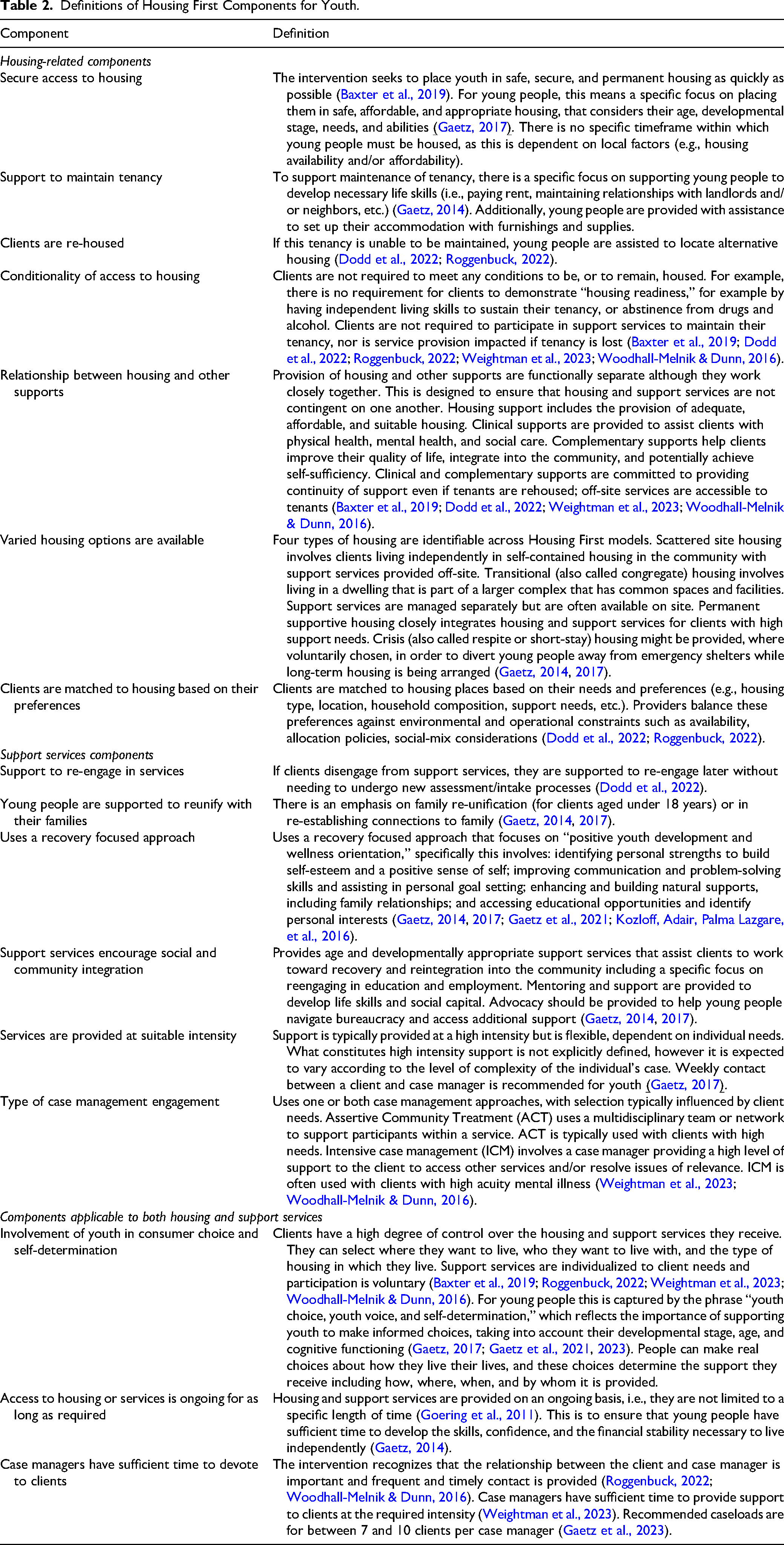
To examine the core Housing First components of included interventions—that is, the essential features or active ingredients theorized to be necessary for achieving desired outcomes (Blase & Fixsen, 2013; Ogden, 2022)—we reviewed all included studies and any associated publications to identify information on the specific housing and support service components delivered within each intervention. Each intervention was then mapped against our Housing First component definitions (Table 2) to determine which components were present. Coding was completed by one reviewer (SV) and reviewed for accuracy by a second reviewer (DT).
Definitions of Housing First Components for Youth.
Documenting Outcome Measures Used in Included Studies
We identified and documented all survey instruments used to measure participant outcomes in the included studies. This process aimed to catalogue instruments previously employed with homeless youth to support future program evaluation and to inform researchers seeking to adopt consistent measures that enable cross-study comparison and future evidence synthesis. A single reviewer (SV) extracted details for each instrument, located the primary reference, and assessed whether the instrument was (a) publicly available, (b) supported by evidence of validation, (c) validated in populations with complex needs, (d) validated among homeless youth, and (e) free to use. This was reviewed for accuracy by two additional reviewers (DT and AS).
Deviations from the Protocol
We initially planned to search the Social Care Online database; however, it was no longer accessible when searches were conducted in October 2023. The protocol also specified that included populations must have substantial socio-emotional needs requiring support beyond housing, such as (a) current or prior mental health issues (self-reported or diagnosed), (b) prior involvement with the child protection or out-of-home care system, (c) prior involvement with the juvenile or adult justice system, (d) a history of family violence (as victims or perpetrators), (e) current or prior substance use issues (self-reported or diagnosed), (f) a physical or intellectual disability, (g) receipt of public assistance payments, and/or (h) membership of a demographic group known to face additional barriers (e.g., adolescent parents, First Nations youth, or LGBTIQ + young people). While participants in included studies likely met these criteria, demographic and clinical characteristics were rarely reported in sufficient detail to apply them consistently. Finally, we did not pre-specify that we would explore barriers and facilitators encountered during the implementation of included interventions. This decision was made during the review when the limited number of eligible studies precluded quantitative synthesis.
Results
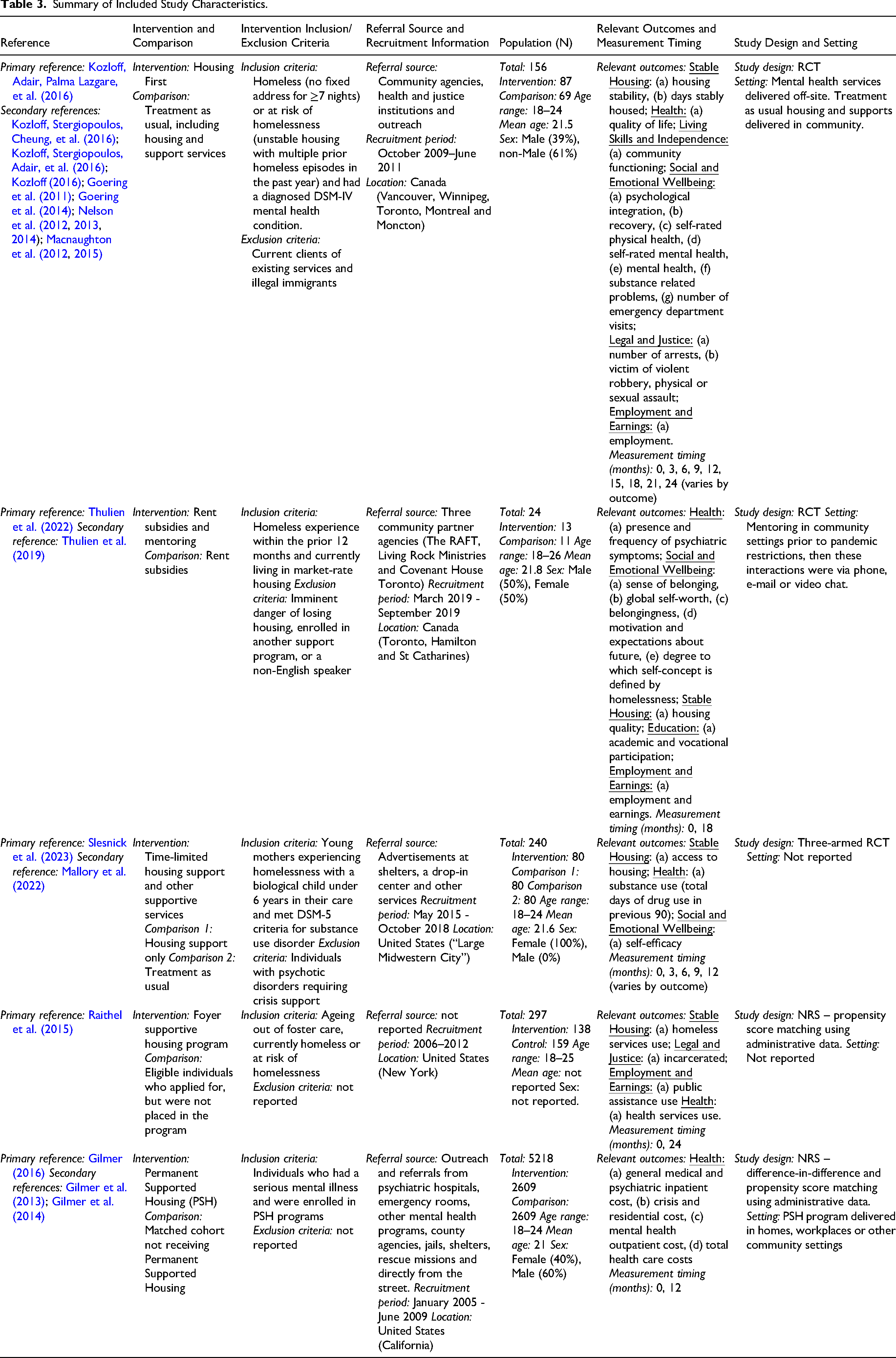
The PRISMA 2020 flowchart (Figure 1) (Haddaway et al., 2022) summarizes the results of our sourcing and screening process. Our electronic database search yielded 4,232 records, of which 2,638 were unique and screened for inclusion. Another 1,678 records from gray literature sources were also screened. From this, five studies—reported across 19 papers, including protocols, implementation evaluations, and conference reports—met our inclusion criteria and were included in this review (see Table 3). Two study protocols were identified that described ongoing studies that would likely meet our inclusion criteria. Three studies were randomized controlled trials (RCT), while the remaining two were non-randomized studies (NRS). Included studies reported results that encompassed seven out of eight outcomes of interest to this review—no studies reported social connections outcomes. All studies were conducted in North America, with three from the United States and two from Canada. Across the four studies reporting age, mean participant age at commencement ranged from 21.1 to 21.8 years. One study examined the impact of an intervention funded at the state level and implemented locally (Gilmer, 2016), while the remaining four tested novel interventions implemented only at the local level (Raithel et al., 2015)—some across multiple sites (Slesnick et al., 2023). Of those, one was a subgroup analysis of a service initially designed for adults (Kozloff, Adair, Palma Lazgare, et al., 2016), while the explicit aim of another was to pilot or test the feasibility of novel interventions (Thulien et al., 2022).
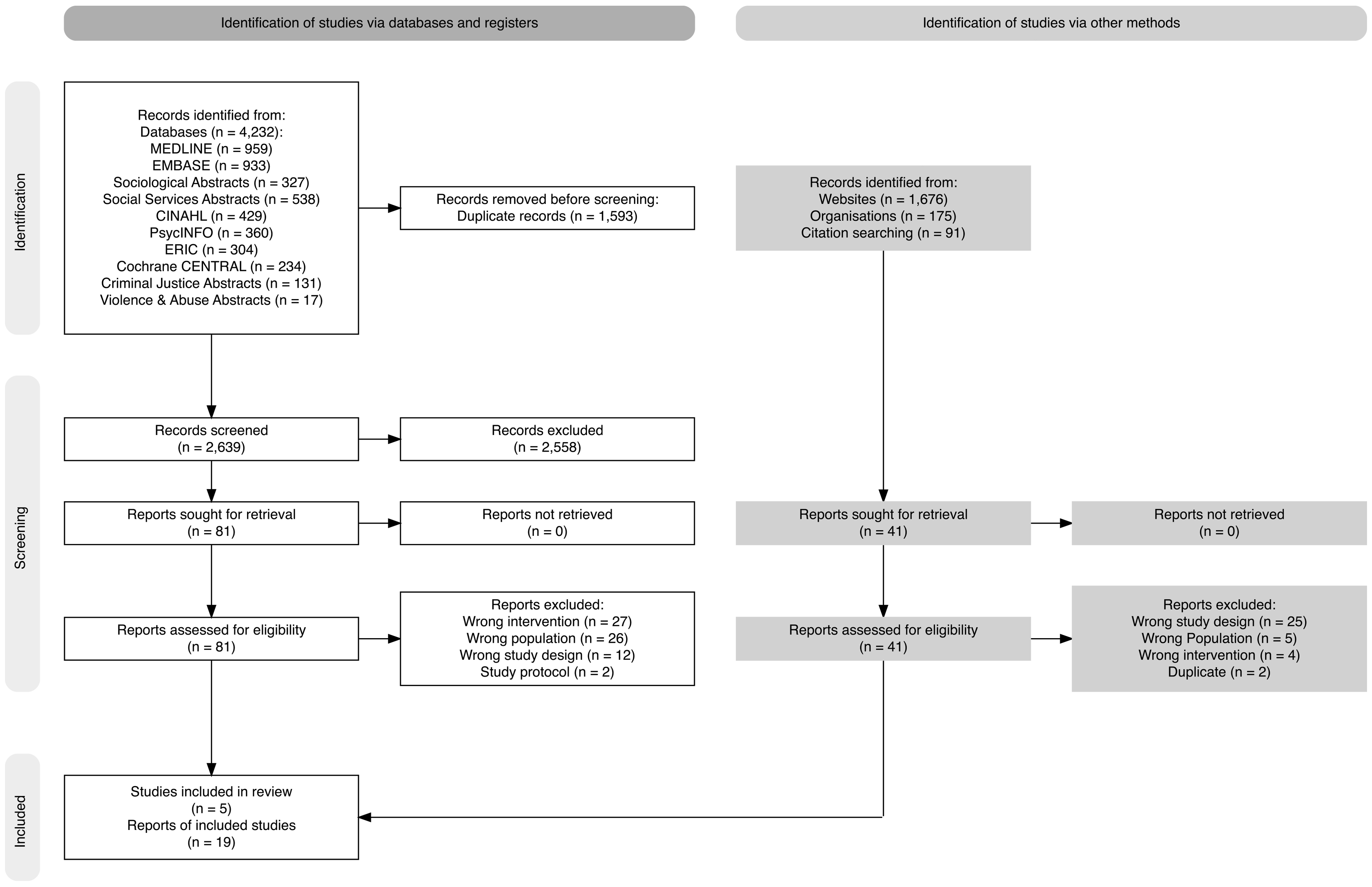
PRISMA 2020 flowchart.
Summary of Included Study Characteristics.
Risk of Bias Within Studies
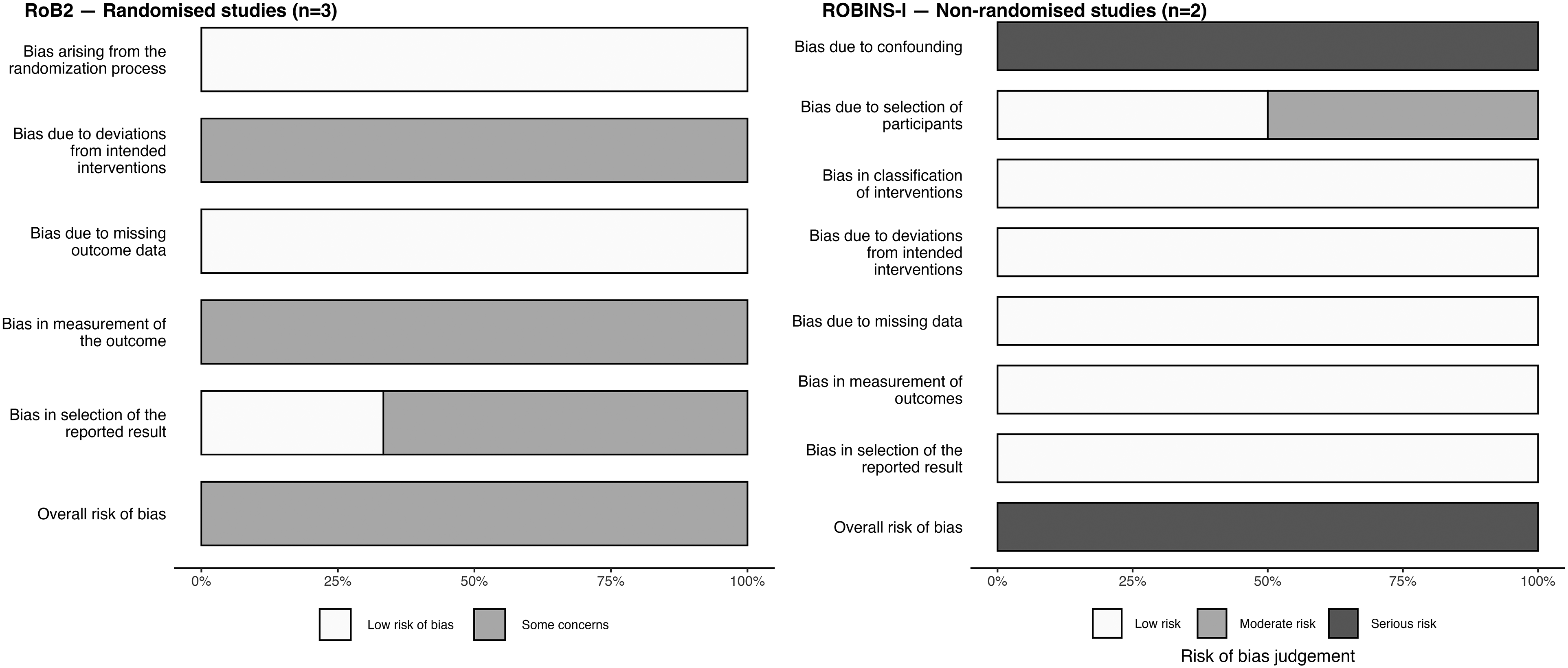
We had some concerns surrounding the ROB in all three RCTs and serious concerns about both NRSs (Figures 2 and 3). In the RCTs, sources of bias included: (a) deviations from intended interventions due to non-blinding; (b) outcome measurement bias from non-blinded interviewers and self-reported measures; and (c) selective reporting, with two studies lacking pre-specified analysis plans. While these limitations warrant consideration, they reflect inherent challenges in social welfare research where double-blinding is often impractical and resource constraints often preclude external outcome assessment. The serious potential for confounding for both NRSs arose from the absence of a justification that the authors matching strategy satisfied the conditional independence assumption. Detailed ROB assessments are included in the supplementary material (Tables S10 and S11).
Summary of risk of bias assessments for included studies.
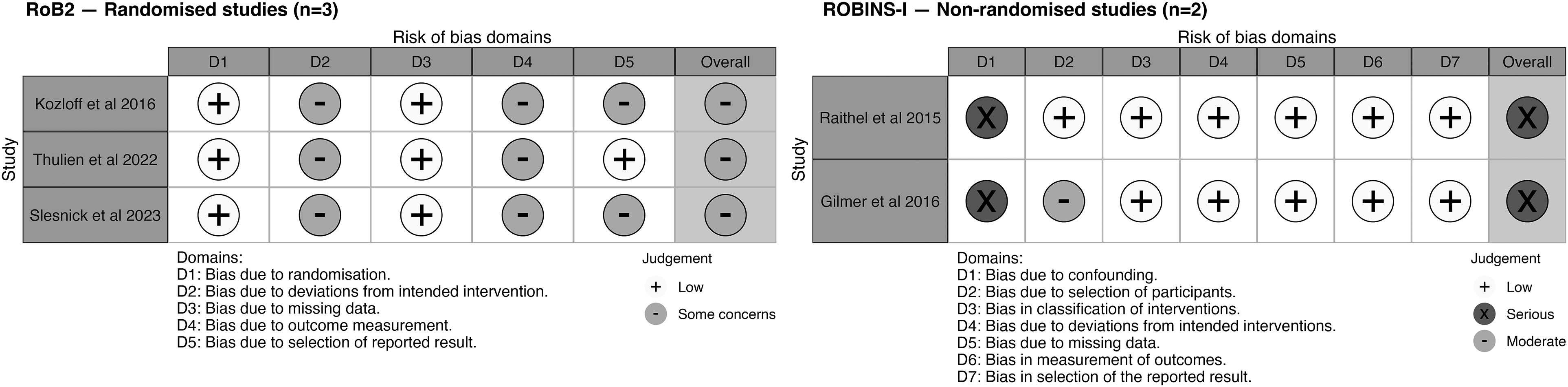
Breakdown of risk of bias assessments for included studies by domain.
Impact of Included Interventions
Stable Housing Outcomes
Four included studies reported five measures of four housing-related outcome constructs, including: if youth were housed at a point in time (at 6, 9, and 12 months), the number of days they were housed (at 3, 6, 9, 12, 15, 18, and 24 months), the quality of their housing (at 18 months) or if they used homeless shelters (at 24 months) (Kozloff, Adair, Palma Lazgare, et al., 2016; Raithel et al., 2015; Slesnick et al., 2023; Thulien et al., 2022). Reported results encompassed 13 unique effect sizes, of which eight had CIs excluding the null in favor of the intervention (see Table 4).
Stable Housing Outcomes.
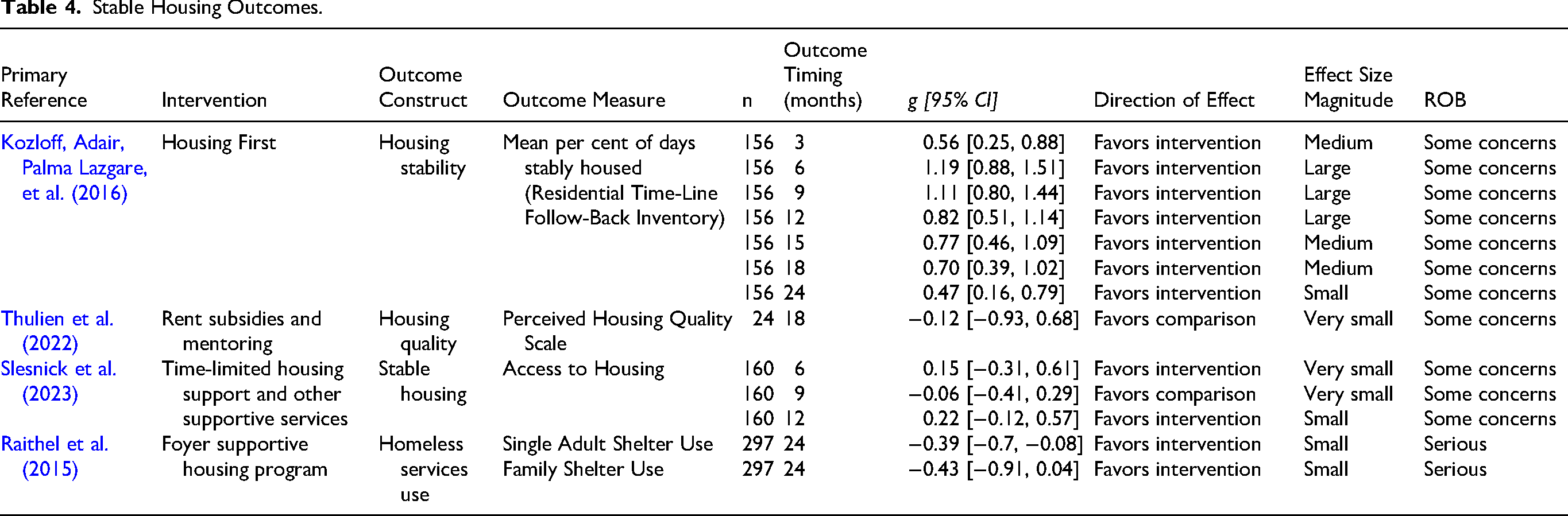
Although estimates changed over time, a Housing First RCT in Canada reported effects favoring the intervention at every quarterly follow up from 3 to 24 months for the length of time participants were stably housed. The effect was medium in size at 3 months (g = 0.56, 95% CI: [0.25, 0.88]) and largest at 6 months (g = 1.19, 95% CI: [0.88, 1.51]), before diminishing over time. At 24 months the effect remained positive but had reduced to a small magnitude (g = 0.47, 95% CI: [0.16, 0.79]) (Kozloff, Adair, Palma Lazgare, et al., 2016).
An NRS of a foyer program in New York found a small reduction in the use of homeless shelters by single adults at 24 months (g = −0.39, 95% CI: [−0.7, −0.08]) (Raithel et al., 2015). For all other reported housing outcomes—including access to housing, perceived housing quality, and family homeless shelter use—the CIs included the null value, indicating that the intervention had no impact on these outcomes as measured in these studies.
Health Outcomes
All five included studies reported at least one health-related outcome, and these included measures of: physical health (at 12 and 24 months), mental health (at 6, 12, 18, and 24 months), psychiatric symptoms (at 6, 12, 18, and 24 months), substance use (at 3, 6, 12, 18, and 24 months), quality of life (at 6, 12, 18, and 24 months), emergency department visits (at 6, 12, 18, and 24 months), health services use (at 6, 12, 18, and 24 months) and health care expenditure (at 12 months). In total, reported outcomes included 15 measures of 20 outcome constructs. These results were transformed into 59 unique effect sizes, of which 11 had CIs excluding the null. Among these, four favored the intervention, one favored the comparison and six related to outcomes that were not directionally interpretable (see Table 5).
Health Outcomes.
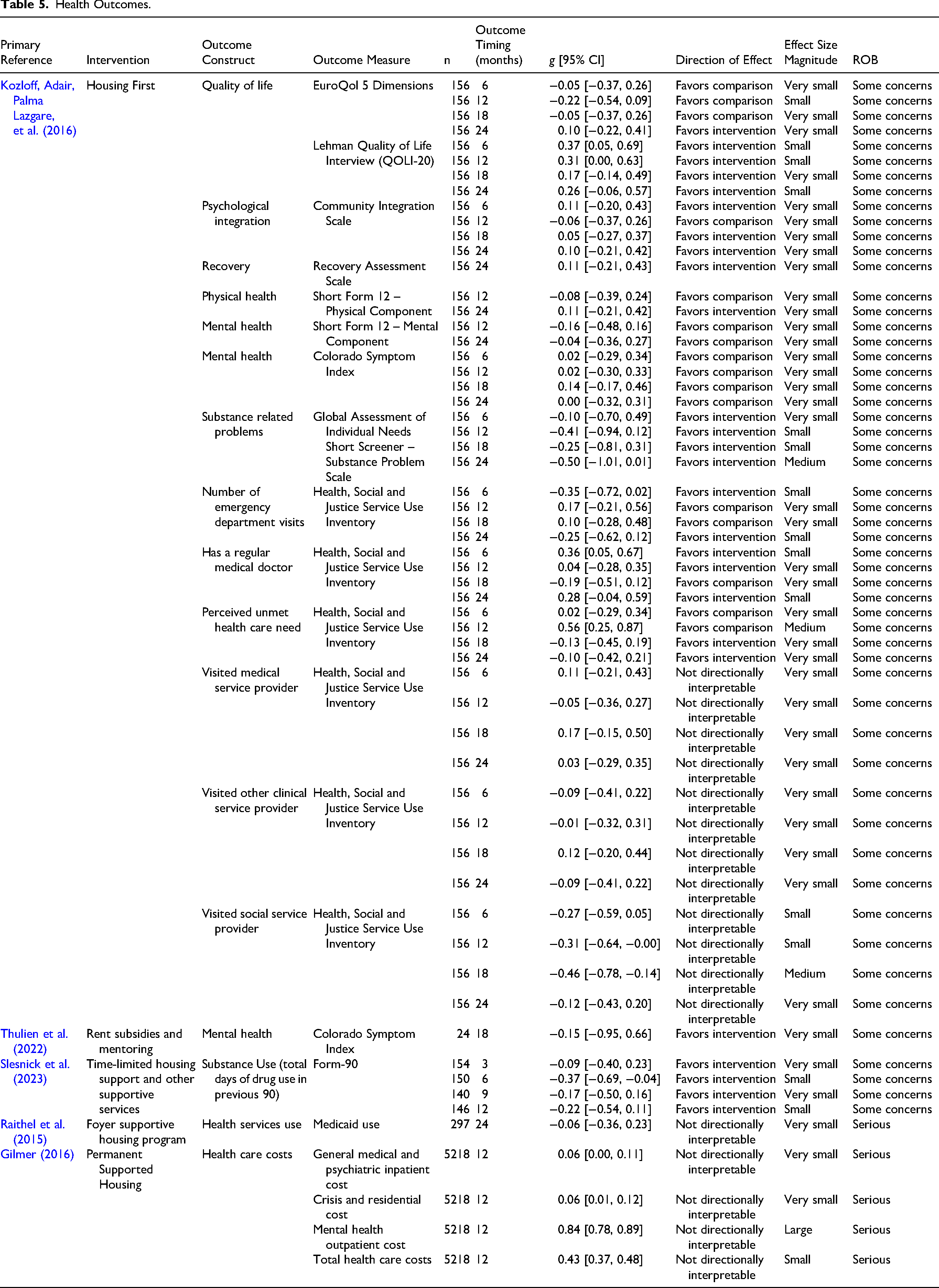
A Housing First RCT in Canada reported small improvements favoring the intervention in quality of life at 6 months (g = 0.37, 95% CI: [0.05, 0.69]) and 12 months (g = 0.31, 95% CI: [0.00, 0.63]); however, the difference between the intervention and comparison disappeared by 18 and 24 months. Another small effect favoring the intervention was observed at 6 months (g = 0.36, 95% CI: [0.05, 0.67]) for “has a regular doctor,” however this was not sustained at 12, 18, or 24 months. Those receiving the intervention were less likely to visit a social services provider at 12 (g = −0.31, 95% CI: [−0.64, −0.00]) and 18 months (g = −0.46, 95% CI: [−0.78, −0.14]), however these are not directionally interpretable. Small or very small reductions in substance use were observed at every time point, however, CIs included the null (Kozloff, Adair, Palma Lazgare, et al., 2016).
An RCT of a time-limited intervention that provides housing and support services in Canada reported a small reduction in substance use (g = −0.37, 95% CI: [−0.69, −0.04]), as measured by the Form-90, at 6 months. However, there was no difference in substance use at other time points (3, 9, or 12 months) where this outcome was assessed (Slesnick et al., 2023).
An NRS examining the impact of Californian permanent supportive housing programs reported higher health care expenditure for the intervention group across all categories assessed by the study at 12 months, although these outcomes are not directionally interpretable. A large difference was observed for mental health outpatient costs (g = 0.84, 95% CI: [0.78, 0.89]). A small difference was observed for total health care costs (g = 0.43, 95% CI: [0.37, 0.48]), and differences for general medical and psychiatric inpatient costs (g = 0.06, 95% CI: [0.00, 0.11]) and crisis and residential costs (g = 0.06, 95% CI: [0.01, 0.12]) were very small (Gilmer, 2016). The single effect sizes from an RCT of rent subsidies and mentoring (Thulien et al., 2022) and NRS of a foyer program (Raithel et al., 2015) both had CIs that included the null.
Social and Emotional Wellbeing Outcomes
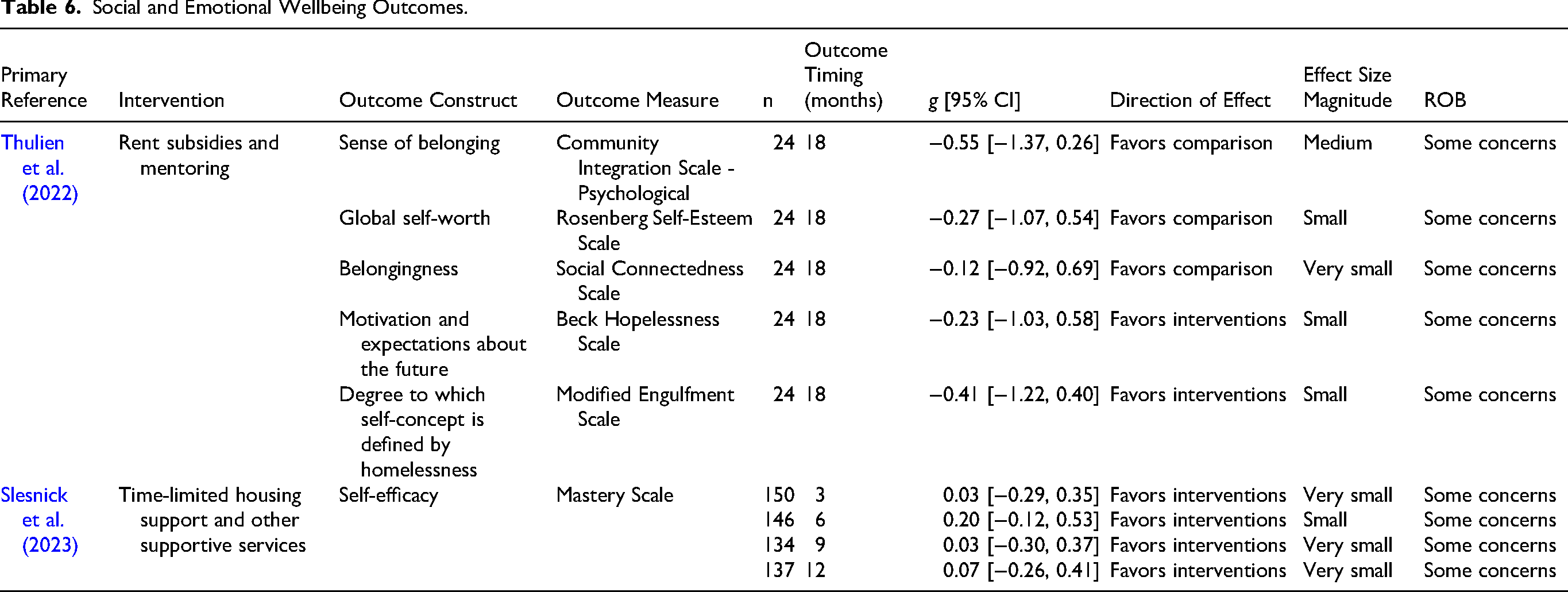
Two included studies reported six measures of six outcome constructs that fell within the social and emotional wellbeing domain (Slesnick et al., 2023; Thulien et al., 2022). Reported outcomes included: self-efficacy (3, 6, 9, and 12 months), sense of belonging (at 6 and 18 months) and motivation and self-worth (both at 18 months). Reported results were transformed into nine effect sizes, all bar one—which was medium-sized—were small or very small, six favored the intervention, the remaining three favored the comparison. All results had CIs that included the null (see Table 6).
Social and Emotional Wellbeing Outcomes.
Education Outcomes
A single RCT of an intervention that provided rent subsidies and mentoring in Canada was the only included study to report an education outcome (Thulien et al., 2022). It reported a single outcome measure assessing if participants were engaged in academic or vocational education or training 18 months following commencement. The small effect size favoring the comparison included the null (see Table 7).
Education Outcomes.

Employment and Earnings Outcomes
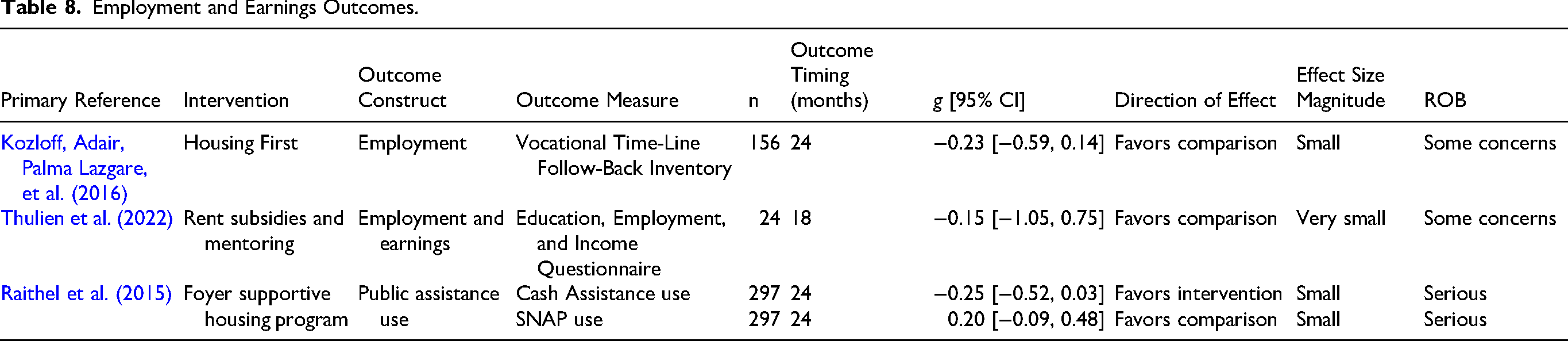
Three studies reported four different measures of three employment and earnings-related outcome constructs. These included: employment status (at 18 and 24 months), employment and earnings (18 months), and use of Supplemental Nutrition Assistance Program (SNAP), i.e., “food stamps” or receipt of cash welfare payments (both at 24 months) (Kozloff, Adair, Palma Lazgare, et al., 2016; Raithel et al., 2015; Thulien et al., 2022). These results were transformed into four effect sizes, all of which were very small or small and had CIs that included the null (see Table 8).
Employment and Earnings Outcomes.
Legal and Justice Outcomes
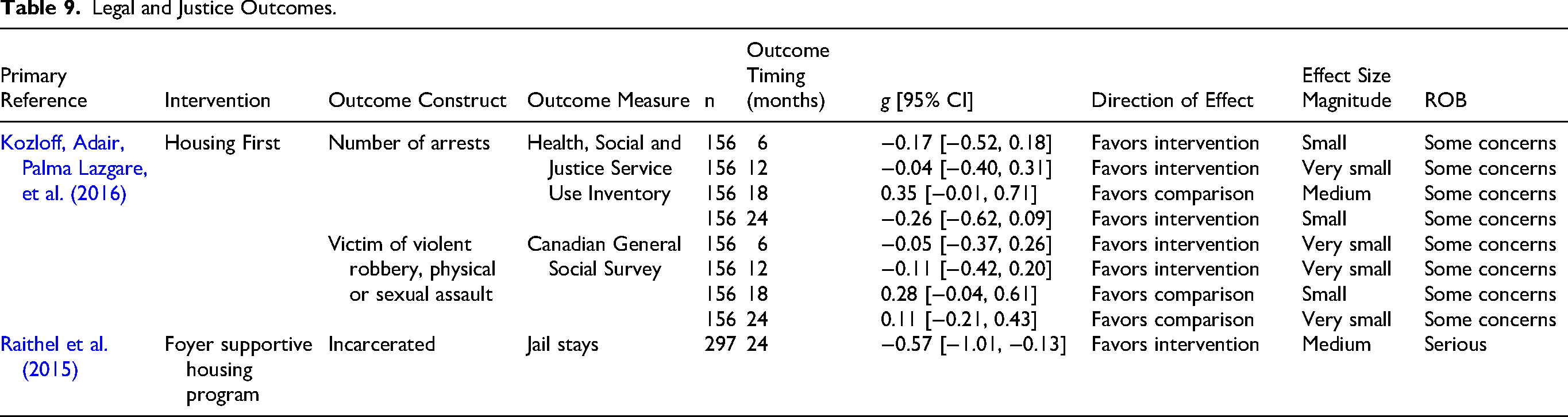
Two included studies reported three different legal and justice outcome constructs measured using three different measures (Kozloff, Adair, Palma Lazgare, et al., 2016; Raithel et al., 2015). Two measures examined perpetration: jail stay (at 24 months) and number of arrests (at 6, 12, 18, and 24 months). A single victimization measure assessed whether a participant was a victim of violent robbery, physical or sexual assault (at 6, 12, 18, and 24 months). Reported results were transformed into nine effect sizes, only one of which had a CI that excluded the null and favored the intervention.
An NRS of a foyer program in New York reported a medium-sized (g = −0.57, 95% CI: [−1.01, −0.13]) reduction in the proportion of participants who spent time in jail at 24 months (Raithel et al., 2015).
The remaining two legal and justice outcomes, both of which came from an RCT of Housing First, varied in whether they favored the intervention or comparison (Kozloff, Adair, Palma Lazgare, et al., 2016). However, all reported CIs that included the null, suggesting that Housing First may not have an impact on these outcomes (see Table 9).
Legal and Justice Outcomes.
Living Skills and Independence Outcomes
One RCT from Canada reported a single outcome measure that assessed an individual's living skills and independence—community functioning (at 6, 12, 18, and 24 months) (Kozloff, Adair, Palma Lazgare, et al., 2016). Reported results were transformed into four effect sizes for each follow-up period, three of which favored the intervention. However, they were all very small and had CIs that included the null (see Table 10).
Living Skills and Independence Outcomes.

Components of Included Interventions
The distribution of these components across included interventions is summarized in Table 11—additional detail is provided in the supplementary material (Table S8). We did not identify sufficient studies to undertake any quantitative analysis that would allow us to determine the impact of any individual component of included interventions, such as meta-regression (Petropoulou et al., 2021) or component network meta-analysis (Taylor, Featherston, et al., 2023). Accordingly, we are unable to assess the effectiveness of any of these components with an acceptable level of certainty. We can only report their presence or absence.
Distribution of Housing First Components Across Included Studies.
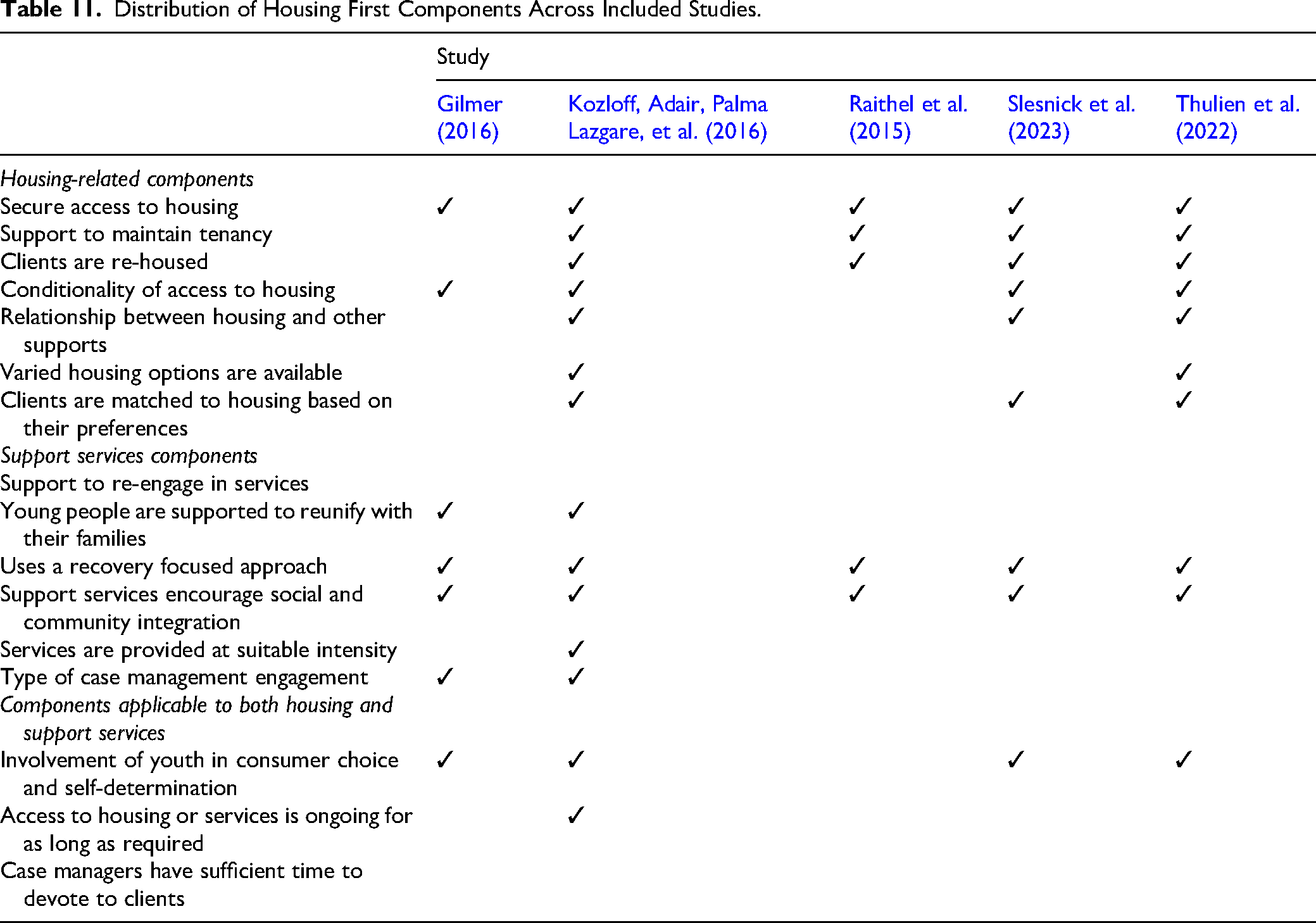
Across the included studies, securing access to housing for participants was a universal priority. Four interventions facilitated this through the direct provision of housing (Gilmer, 2016; Kozloff, Adair, Palma Lazgare, et al., 2016; Raithel et al., 2015; Slesnick et al., 2023), with the remaining one providing rental subsidies (Thulien et al., 2022). All studies, bar Gilmer (2016), provided support to maintain a tenancy through various means such as subsidies for utilities, case management, peer support, and life skills development. Most studies did not require participants to meet specific conditions to access housing, and the relationship between housing and other supports was generally not contingent on one another, allowing for flexible service delivery. Four interventions specifically re-housed clients when necessary (Kozloff, Adair, Palma Lazgare, et al., 2016; Raithel et al., 2015; Slesnick et al., 2023; Thulien et al., 2022). Two included studies incorporated both varied housing options and preference-based matching, promoting client choice and autonomy.
All included studies provided intervention components that included a range of support services to participants. All five studies employed a recovery-focused approach, emphasizing personal strengths, mental-health support, peer support and strengthening social and family relationships. All five interventions also included components aimed at social and community integration, focusing on participation in education and employment, life-skills training and broader community engagement. Kozloff, Adair, Palma Lazgare, et al. (2016) and Gilmer (2016) specifically supported young people to reunify with their families when desired. One intervention specifically adjusted the intensity of services based upon participants’ needs and preferences (Kozloff, Adair, Palma Lazgare, et al., 2016). The type of case management engagement varied, with Kozloff, Adair, Palma Lazgare, et al. (2016) using Assertive Community Treatment and Intensive Case Management (ICM), while Gilmer (2016) used ICM and a multidisciplinary treatment team model.
Four of the five interventions actively involved youth in consumer choice and self-determination, empowering them to make decisions about the services they received (Gilmer, 2016; Kozloff, Adair, Palma Lazgare, et al., 2016; Slesnick et al., 2023; Thulien et al., 2022). The duration of access to housing and services was only expressly unlimited in one case, with Kozloff, Adair, Palma Lazgare, et al. (2016) providing ongoing access for as long as required.
Barriers and Enablers to Program Implementation
Detailed barriers and enablers identified at all stages of the EPIS framework are available in the supplementary material (Table S12). This section provides a summary.
Implementation Barriers
During exploration, a single outer-context barrier concerned legal status and informed consent requirements, which limited the ability to implement housing components of Housing First to young people aged under 18 (Kozloff, Adair, Palma Lazgare, et al., 2016).
In the preparation stage, several outer-context issues affected the ability of some sites to deliver housing and support components of Housing First. These included: (a) limited local housing and homelessness services infrastructure, (b) insufficient service capacity, (c) human resources constraints, and (d) insufficient time to build relationships with existing community services (Nelson et al., 2013). Inner-context barriers included: (a) limited engagement of staff with lived experience, and insufficient cultural and linguistic competence (particularly for work with First Nations and culturally and linguistically diverse youth) and (b) limited communication about the scope for local adaptation, which reduced staff buy-in (Nelson et al., 2012, 2013, 2014).
During implementation, inner-context barriers to providing housing and support services included insufficiently developed program protocols, which constrained teams’ ability to manage intake, secure housing, and concurrently support existing tenants (Nelson et al., 2012, 2014). Housing availability was a major outer-context issue for implementing housing components, due to both limited affordable housing stock and a reluctance among some housing providers and/or landlords to house clients with complex needs such as mental health issues or substance use disorders (Macnaughton et al., 2012, 2015; Nelson et al., 2012, 2014). For support services, inner-context barriers included: (a) crisis management diverting staff from supporting clients to develop long-term goals and take proactive steps toward achieving them (Macnaughton et al., 2015), and (b) competing operational demands that affected service quality and left little time for staff to engage in further training and development (Nelson et al., 2012, 2014). Inner-context barriers to implementing both housing and support services included: (a) limited opportunities for informal communication between teams, including across sites, which hindered collaboration, and (b) high staff turnover, which negatively affected service delivery (Macnaughton et al., 2015; Nelson et al., 2012, 2014).
In the sustainment phase, inner-context barriers affected both housing and support services. These included: (a) the time-limited nature of the project funding, which made landlords reluctant to sign extended leases (Macnaughton et al., 2015) and (b) the high cost of providing the program, which was identified as a barrier to sustainability (Nelson et al., 2012).
Implementation Enablers
In the preparation phase, inner-context enablers for housing and support services included strong leadership with the technical, interpersonal, and decision-making capacity needed to guide implementation, alongside flexibility to tailor the program to local and cultural needs at each site (Macnaughton et al., 2015; Nelson et al., 2012, 2013, 2014). Outer-context enablers included strong collaboration between the program and existing community services and early alignment between program values and local stakeholders, both of which supported recruitment and helped build initial momentum for implementation (Nelson et al., 2012, 2013).
During implementation, outer-context enablers for housing components centered on strong partnerships with landlords and property managers to secure and sustain quality housing, and this collaboration facilitated early intervention in tenancy problems, reducing escalation to police involvement or eviction (Macnaughton et al., 2015; Nelson et al., 2012, 2014). For support services, inner-context enablers included partnerships with consumers, which facilitated peer-led activities and improved communication between clients and staff (Nelson et al., 2012, 2014). Across both housing and support services, outer-context enablers included strong partnerships with government agencies, which supported access to housing, mental health and homelessness services, and income support payments, and engagement with local partners, who facilitated the integration of the program into the community's existing support and services (Nelson et al., 2012, 2014). Inner-context enablers included a strong organizational culture, and governance structure that supported clear roles, collaboration, and effective communication (Nelson et al., 2012, 2014). Diverse and stable teams with relevant expertise strengthened service delivery, and shared values aligned with Housing First principles reinforced fidelity and consistent practice (Macnaughton et al., 2015; Nelson et al., 2012, 2014).
In the sustainment phase, outer-context enablers included relationships with community stakeholders and agencies across the wider service system, which supported implementing agencies to take ownership of the program and contributed to its long-term sustainability (Macnaughton et al., 2015). Across both housing and support services, inner-context enablers included the sustained commitment of staff to the program and its values, despite the challenging nature of the work (Macnaughton et al., 2015).
Use of Measures
Beyond administrative data, included studies used 20 distinct survey instruments. Using information cited in included studies, we were able to identify evidence that 16 (80%) of these measures had been validated among any population. We found evidence that eight (40%) had been validated amongst a population with complex needs, but no evidence that any had been validated amongst homeless youth. Of the 20 instruments, 16 (80%) were publicly available. Overall, seven were free to use, four were paid, and nine had unclear cost status. A complete list of measures used in included studies is provided in the supplementary material (Table S9).
Discussion and Applications to Practice
This systematic review examined interventions that combine housing with other supports for youth experiencing homelessness in high-income countries, addressing four questions: their effectiveness across key outcome domains; the core components that comprise such interventions, the barriers and enablers influencing implementation, and the instruments used to measure outcomes. Together, these questions provide a framework for interpreting the current evidence base and identifying priorities for future research and practice.
In relation to the first research question—effectiveness across key outcome domains—the available evidence remains limited. Only five studies (reported across 19 papers) met the prespecified inclusion criteria, all of which were conducted in North America. These studies exhibited substantial heterogeneity, particularly in the type, measures, and timepoints of reported outcomes, preventing any planned quantitative synthesis. While some interventions showed promising short-term impacts in housing stability, the effects often diminished over time. For example, one study observed that a large improvement on housing stability at six months decreased to a small one by 24 months (Kozloff, Adair, Palma Lazgare, et al., 2016), reflecting both reduced housing stability among intervention participants and improvements amongst those who received treatment as usual. While Housing First appears to accelerate the path to stable housing, its advantage over treatment as usual diminishes over time. Health-related outcomes demonstrated mixed results, with modest improvements in quality of life and substance use in some studies, but increased healthcare costs in others. Effect sizes for social, emotional, educational, and employment outcomes were mostly imprecise, suggesting that the included interventions did not have a consistent impact in these domains. Overall, the scope, strength, and quality of existing evidence is insufficient to draw firm conclusions about the effectiveness of existing interventions. However, it is promising that all included studies were published within the last decade, suggesting growing research interest in this field and that additional evidence will emerge in the future.
Regarding the second research question—identifying the core components of included interventions—the housing components of the included studies ranged from Housing First approaches to transportable rent subsidies, each of which incorporated various supporting components such as case management, mental health services, and life skills training. Across studies, securing access to housing was a universal priority, typically accompanied by flexible, recovery-oriented support services. However, the small number of studies precluded any quantitative analysis of the impact of individual component effects.
For the third research question—barriers and enablers to implementation—the review identified challenges across multiple domains, including housing procurement, service integration, and workforce capacity. These findings underscore the challenges of delivering complex interventions with youth experiencing homelessness and highlight the need for more robust, long-term studies that can determine the specific components and implementation strategies most effective in supporting this vulnerable population.
Addressing the fourth research question—outcome measurement approaches—included studies used 20 distinct instruments, some of which were nearly half a century old. Many of these instruments have not been validated among populations with complex needs, which raises questions about their suitability.
Taken together, these findings indicate that, although the review cannot definitively point to the merits of a particular model, several practical lessons emerge for researchers, policymakers, and practitioners interested in developing, implementing, or evaluating similar interventions—particularly regarding intervention intensity, duration, and implementation.
For the first research question, these findings suggest several implications for how future effectiveness research should be designed and interpreted. The scarcity of available evidence severely limits the ability to draw substantive conclusions about which interventions are most effective. The concentration of included studies in North America (United States and Canada) may further constrain generalizability to other high-income settings. However, even within North America, the studies varied substantially in their geographic, social, and economic contexts; the availability of local services; and the demographic characteristics of participating youth. This heterogeneity highlights the importance of understanding how context and population characteristics shape intervention effects, rather than assuming that findings will or will not be replicable elsewhere.
Advancing understanding of “what works for whom” will require routine reporting of key participant characteristics and more systematic examination of subgroup effects. Groups disproportionately represented among youth experiencing homelessness—including First Nations young people, gender and sexual minority youth, and young people living with disability—may respond differently to specific combinations of housing and support. Yet the small number of studies and limited demographic reporting precluded any meaningful exploration of heterogeneity in outcomes across these populations. Other variables that may warrant stratification, such as baseline substance use, mental health status, or implementation fidelity, were similarly under-reported.
Finally, the limited duration and scope of follow-up in existing studies restrict understanding of long-term outcomes. Short-term improvements in housing stability were often not sustained, underscoring the need for studies that track outcomes over extended periods and capture theorized transitions into education, employment, improved health, and increased safety. Studies using linked administrative data have particular advantages in this regard, given their ability to follow young people across multiple systems over time.
The second research question, on intervention components, has important implications for both reporting standards and program design. Given the likely continued heterogeneity of interventions providing housing and support services, future studies must provide clear and detailed descriptions of what the intervention comprises. Policymakers and practitioners need this level of specificity to assess its feasibility, cost, and scalability. Two programs may both be described as providing “permanent supported housing,” yet differ markedly in case management intensity, workforce composition, eligibility criteria, or the scope or integration of additional support services. Detailed reporting is not only essential for replication but also for enabling component-level quantitative synthesis.
In this review, we framed components based on the core elements of a Housing First approach. This structure provides one possible component taxonomy and could serve as a potential reporting standard for both future primary studies and systematic reviews, although it is not the only option. The development and adoption of a shared component taxonomy would help ensure that studies consistently identify which housing and support services are offered, the intensity and duration of those elements, and any staffing, service delivery, and context-specific adaptations. Such consistency would also support more informative component-level analyses, including the identification of core intervention components—an important step in understanding, replicating, and scaling complex interventions.
The implementation analysis highlights several conditions that must be in place if such interventions are to be delivered and sustained in practice, particularly around intervention fidelity, partnerships, funding stability, and scalability. Implementing interventions for youth experiencing homelessness is inherently challenging, and clear reporting of implementation processes is essential to guide program developers and service providers. Measuring and reporting fidelity is feasible using existing tools (Gilmer et al., 2013), although further development or adaptation of these measures for youth-focused interventions would strengthen future research and practice.
A consistent finding across included studies was the centrality of strong partnerships—both between housing providers and between support services already engaged with young people. Effective collaboration helps maintain beneficial service relationships as young people transition into stable accommodation. However, establishing and sustaining these partnerships depends heavily on program stability and longevity.
The substantial costs of providing long-term housing while young people address trauma and its impacts represent a fundamental implementation barrier. This creates a dual challenge: securing adequate funding to deliver the intervention itself and demonstrating financial sustainability to maintain the confidence of essential partners. Service providers require assurance of continued funding to invest in workforce capability and maintain consistent staffing. Housing providers and landlords likewise need confidence in the longevity of programs before committing properties or entering into longer-term arrangements.
Scalability also emerges as a crucial consideration. Smaller programs may feasibly build or adapt dedicated housing stock, but this becomes increasingly difficult for initiatives seeking to operate at scale. Portable rent subsidies offer greater scalability but require young people—many with complex needs—to navigate the private rental market, which can be challenging and inequitable. The choice between these strategies should be informed by well-estimated levels of demand and careful consideration of the needs and capabilities of the target population. Given the heterogeneity within this population and the diverse contexts in which these interventions are delivered, a mixed approach may be optimal. Combining dedicated housing for higher-risk individuals with rental subsidies for those requiring less intensive support may enable both scalability and responsiveness. Future research should explore the feasibility, acceptability, and effectiveness of these approaches when stratified by risk.
The fourth research question, on outcome measurement, points to opportunities to strengthen both comparability and the policy relevance of future studies. The use of heterogeneous outcome measures limits the ability to assess outcomes across studies. When multiple measures are administered concurrently, they often capture overlapping constructs and employ different scales, increasing respondent burden without adding clarity. Future research would benefit from the use of consistent, validated instruments that are psychometrically sound and easy to complete.
One potential avenue is the use of PROMIS (Patient-Reported Outcomes Measurement Information System) measures (Cella et al., 2010). These person-centered instruments cover multiple domains of physical, mental, and social health; apply consistent scaling; use item response theory to reduce respondent burden; are free to use; and can be administrated across diverse survey administration platforms and languages. They also offer scope for extending measurement into other domains relevant to youth homelessness.
More broadly, research in this field often reflects public health or social welfare priorities, which shapes the outcomes that are typically assessed. While many of these short- and medium-term outcomes are important, a perspective framed by human capital development provides a coherent scope for a core outcome set that includes longer-term outcomes such as skill development, qualification attainment, and stable employment, whose effects can accumulate and generate downstream benefits over a lifetime. This approach recognizes that stable housing, physical and mental health, and supportive relationships are necessary intermediate steps in accumulating education, skills, and employment that form human capital (Wulczyn et al., 2021). Such a framework also facilitates downstream economic evaluations, as established approaches exist to quantify their benefits over time (Lee & Aos, 2011).
Finally, consideration should be given to the development of a core outcome set for youth homelessness interventions—an agreed minimum set of outcomes to be measured and reported across studies. Guidance from the COMET Initiative provides a methodological framework for developing and reporting such sets (Williamson et al., 2017).
The provision of stable housing should be understood as a prerequisite for addressing the complex issues faced by homeless youth. Changing trajectories for these vulnerable young people is a complex process with no quick fixes. While support services are crucial, they are unlikely to have a sustained impact if not coupled with stable housing. Housing provides the foundation from which young people can engage more effectively with support services, address health concerns, pursue education or employment opportunities, and develop the skills needed for independent living. Policymakers and practitioners should recognize that stable accommodation is not just an end goal, but a necessary starting point.
Homeless youth present with unique needs compared to their adult counterparts, necessitating interventions that reflect the developmental stages of youth and emerging adulthood. Although the evidence identified in this review is insufficient to recommend a particular approach conclusively, Housing First principles appear promising and warrant further investigation. The heterogeneity of youth experiencing homelessness underscores the need for interventions that can adapt to varied population characteristics and local contexts. Future impact evaluations should consider analyses that allow us to identify what works for whom, thereby informing more targeted and effective interventions. Component-level analysis also has the potential to clarify the essential elements of successful programs—an important consideration for complex, multicomponent interventions. Recognizing the challenges of conducting research with this population, well-executed non-randomized studies should be considered when randomized designs are not feasible.
Supplemental Material
sj-docx-1-rsw-10.1177_10497315251415139 - Supplemental material for Housing and Support Interventions for Homeless Youth in High-Income Countries: A Systematic Review
Supplemental material, sj-docx-1-rsw-10.1177_10497315251415139 for Housing and Support Interventions for Homeless Youth in High-Income Countries: A Systematic Review by David Taylor, Stephanie Vecchio, Susan Baidawi and Aron Shlonsky in Research on Social Work Practice
Footnotes
Acknowledgments
The authors wish to acknowledge the support and assistance of staff from Melbourne City Mission.
Author Contributions
DT led the investigation (literature screening, risk of bias assessment), data curation (data extraction), and formal analysis (effect size transformation), he was also responsible for methodology (search strategy), and writing—original draft. SV conducted the investigation (literature screening, risk of bias assessment), data curation (data extraction), and contributed to writing—original draft. SB participated in investigation (literature screening), writing—review and editing. AS led the conceptualization, methodology (search strategy), funding acquisition and contributed to writing—review and editing, and writing—original draft.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was funded by Melbourne City Mission.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data and materials necessary to reproduce the analyses presented in this systematic review are available on GitHub at https://github.com/davetayl-r/youth-homelessness-review. The repository includes all data and code required to facilitate replication.
Supplemental Material
Supplemental material for this article is available at https://davetayl-r.github.io/youth-homelessness-review and archived at or ![]()