
Abstract
Cultural Adaptation of Parenting Interventions: Formative Evaluation in Thailand
Evidence-based parenting programs are considered a key strategy for eliminating violence against children (World Health Organization [WHO], 2018). A recent WHO guideline review on parenting programs identified over 430 randomized controlled trials (RCTs) of these interventions, with more than 150 in low- and middle-income countries (LMICs; Backhaus et al., 2023; WHO, 2023). However, despite the growing number of studies in LMICs and the solid evidence in support of these interventions (Backhaus et al., 2023; Chen & Chan, 2016; Knerr et al., 2013; McCoy et al., 2020), few parenting programs are implemented routinely and at the scale needed to tackle violence against children effectively.
Barriers to sustained implementation include expensive licensing fees and program costs for many evidence-based and “brand name” programs, which often render them out of reach for many LMICs (Mikton, 2012). In response, an international initiative led by the Universities of Oxford and Bangor (United Kingdom), Cape Town and Stellenbosch (South Africa), WHO, and the United Nations Children’s Fund (UNICEF) prompted the development of Parenting for Lifelong Health for Young Children (PLH-YC), a freely available, evidence-based parenting program (Ward et al., 2014). This intervention, which targets parents of children aged 2–9 years, has demonstrated reduced violent discipline in RCTs, including in South Africa (N = 296) and the Philippines (N = 120) (Lachman et al., 2021; Ward et al., 2020).
A similar endeavor has transported PLH-YC to Thailand, through a partnership between the Universities of Oxford and Cape Town, the nongovernmental organization (NGO) Clowns Without Borders South Africa, UNICEF, and the Thai Ministry of Public Health (MOPH). This effort responded to high rates of parent-perpetrated violence in childhood and the desire to test program delivery through the public health system. A Thai national survey of 34,540 households found that 54% of adults reported using psychological or physical punishment against children during the past month (National Statistical Office of Thailand, 2023).
This formative evaluation aimed to assess the extent to which PLH-YC required cultural and contextual adaptation before delivery to low-income families within the public health system in the Udon Thani province of Thailand. This qualitative study followed United Kingdom Medical Research Council guidelines on developing and evaluating complex interventions (Craig et al., 2008) and was situated within a larger, collaborative research project to inform a subsequent feasibility pilot, RCT, and wider dissemination within routine service delivery. We posed two main research questions: (1) What is the cultural and contextual relevance of the key program themes, process, structure, schedule, and logistics of PLH-YC that can inform adaptation? (2) What are the potential barriers and opportunities for scaling up an adapted version of PLH-YC within the public health system in Thailand? In this study, parents include biological parents, relatives, and other nonbiological primary caregivers of a child.
Research Approach and Accompanying Theoretical Frameworks
We adapted two complementary theoretical frameworks to inform our approach to this qualitative study: the five-stage cultural adaptation framework proposed by Barrera et al. (2013) and the RE-AIM (reach, effectiveness, adoption, implementation, and maintenance) framework for evaluating the public health impact of interventions in routine delivery systems and at scale (Glasgow et al., 1999). Barrera et al. (2013) posited that information gathering is a vital first stage of cultural adaptation, which includes formative studies to determine how well an intervention might suit the needs and views of a particular cultural group and assess the community's capacity for intervention implementation. This first stage is then followed by the preliminary adaptation design, testing (such as through pilot studies), adaptation refinement, and the trial of the adapted intervention (Barrera et al., 2013). According to several meta-analyses, cultural adaptation can strengthen an intervention's appeal, effectiveness, and sustainability for a target group (Baumann et al., 2015; Griner & Smith, 2006; Huey & Polo, 2008). In addition to cultural factors, contextual adaptations may also include modifications to delivery strategies, intervention deliverers and other agents, and settings (Evans et al., 2019).
The RE-AIM framework includes five evaluative dimensions: reach, effectiveness, adoption, implementation, and maintenance. We considered the potential reach of the intervention (factors relating to the characteristics of participants and barriers to enrolment and attendance), opportunities and impediments to adoption and implementation by the community and government institutions, and the potential for maintenance of the intervention over time through institutionalization and enforcement (Glasgow et al., 1999). We reconfigured these two frameworks to be understood as nested dimensions, with cultural adaptation operating within a broader implementation context that includes the public health system and relevant organizations, services, and actors (see Figure 1).
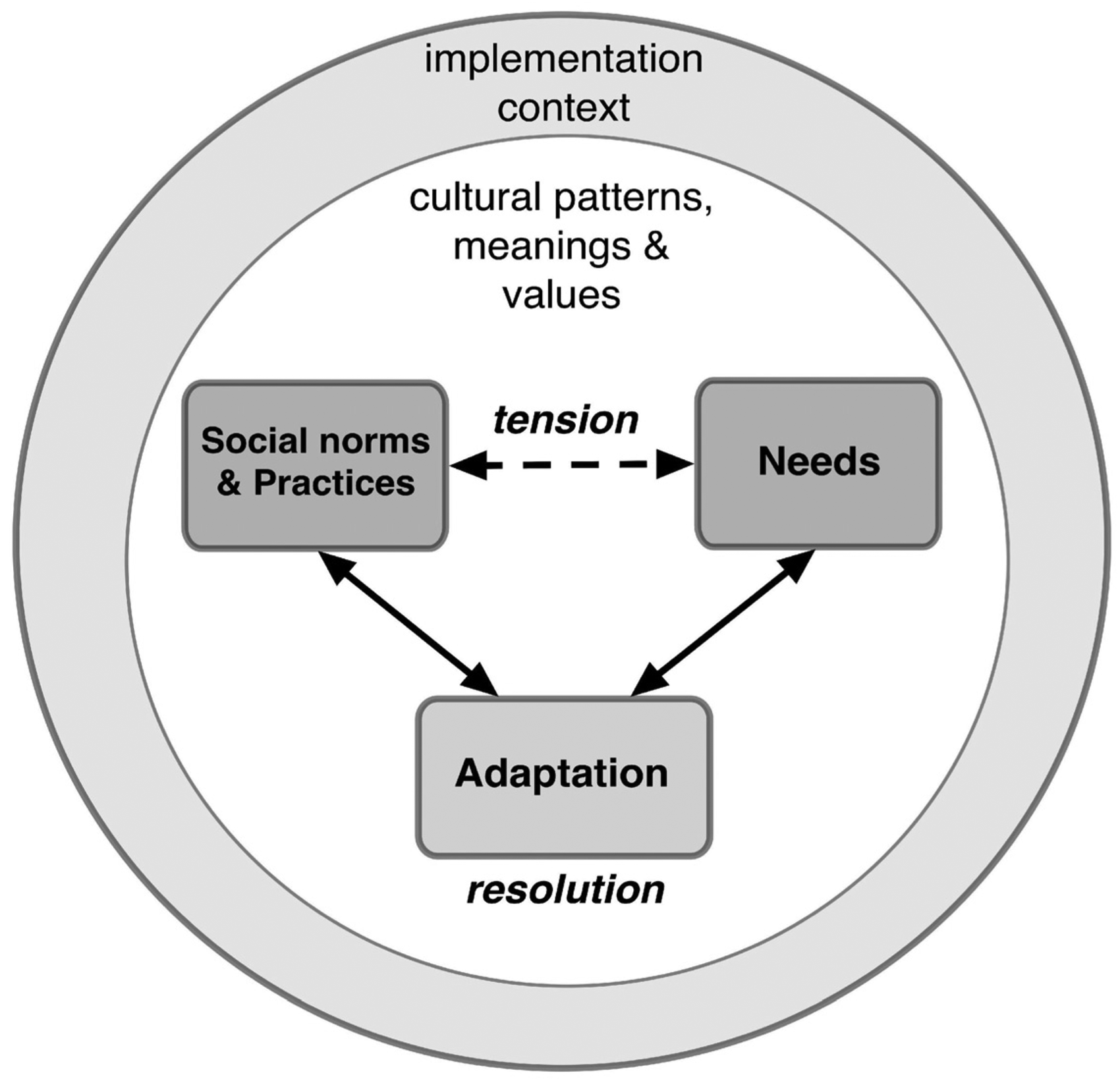
Nested Conceptual Model of Cultural and Contextual Adaptations as Resolutions of Tensions Between Perceived Needs, Norms, and Practices.
Intervention Description
PLH-YC is a group-based, nondidactic, and collaborative parenting program originally developed in South Africa for low-income Xhosa families (Lachman et al., 2016). It is based on social learning principles derived from over 50 years of research on parenting programs that emphasize the importance of establishing positive parent–child relationships before addressing difficult child behaviors and learning nonviolent limit-setting and discipline techniques (Kaehler et al., 2016). Program content includes many of the common components found in evidence-based programs from high-income country contexts (Kaminski et al., 2008; Leijten et al., 2019). The program uses a model of “Building a House of Support for You and Your Child,” in which parents learn and practice new parenting skills over 12 sessions organized into three main categories (see Figure 2). The first category involves three sessions focused on building positive parent–child relationships, including spending individual time with children and using child-led play and descriptions of actions and emotions (Eyberg, 2005; Kaehler et al., 2016). The second category, positive reinforcement, consists of four sessions on labeled and immediate praise, simple and free rewards, and limit setting through positive instructions and consistent rules and routines. Positive discipline, the final category, comprises nonviolent behavior management techniques, including redirecting and ignoring negative behaviors, ignoring negative attention-seeking and demanding behaviors, using appropriate consequences to support compliance, and using time-out as a consequence for aggressive or destructive behaviors. The last session includes brief content on involving children in resolving conflicts and provides parents with an opportunity to reflect and discuss continued skills application.
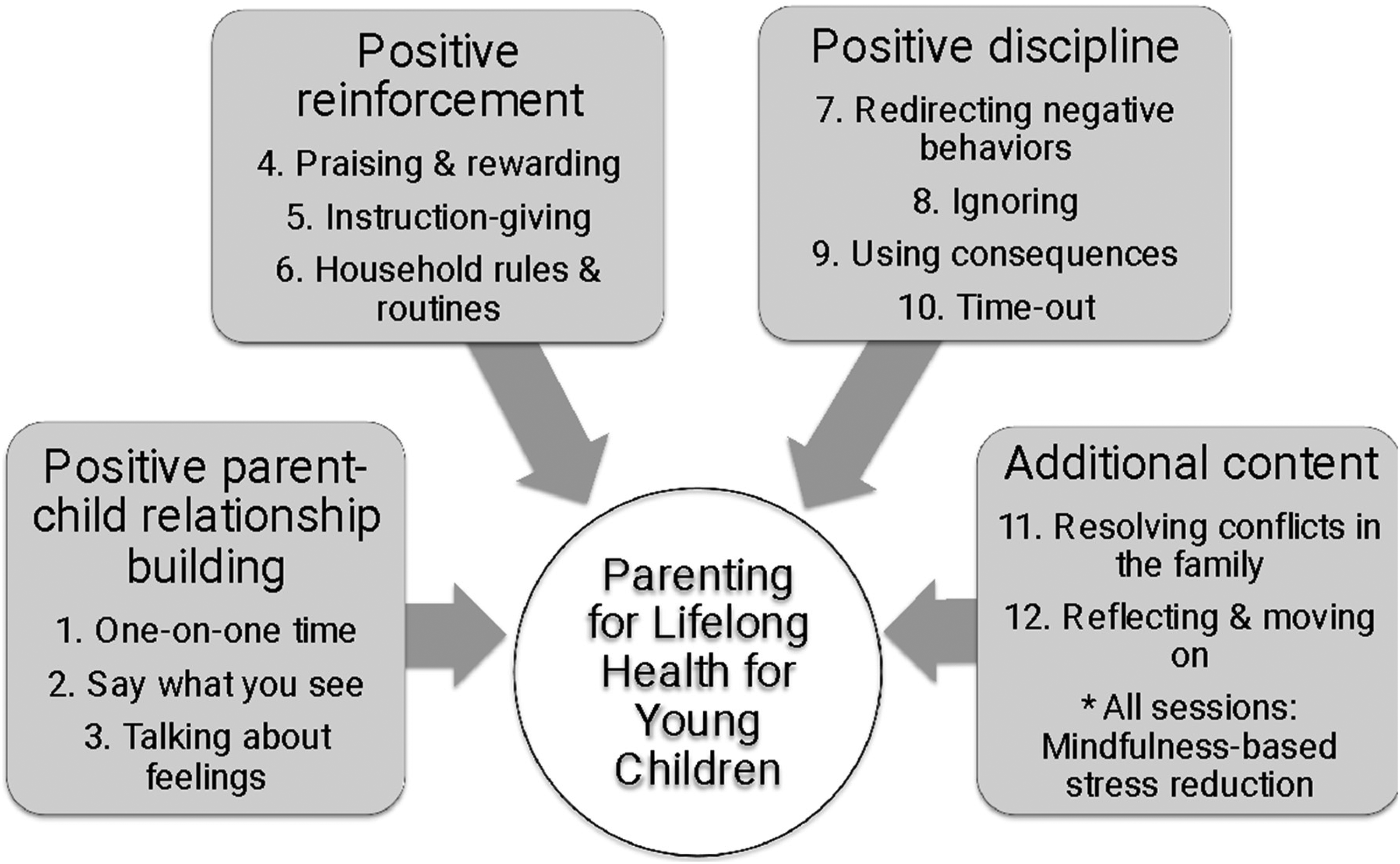
PLH-YC Original Program Session Themes. PLH-YC = Parenting for Lifelong Health for Young Children.
PLH-YC is designed to be delivered by two trained facilitators to groups of 12–15 parents who meet weekly or fortnightly. During each session, facilitators (a) lead participants through mindfulness-based stress reduction techniques; (b) refer to illustrated stories to help parents identify specific parenting techniques; (c) provide coaching support while parents practice these techniques in role-plays; and (d) assign home practice activities. At the beginning of the following session, parents report on home practice experiences, and facilitators help them identify solutions to challenges. The facilitators also conduct individual consultations in participants’ homes to introduce PLH-YC and if parents miss a session or require additional support. Parent handbooks summarizing core parenting skills serve as a resource during home practice or following program completion. Parents also receive personalized weekly phone calls and text message “boosters” to encourage skills practice at home. Lunch, transportation, and childcare are provided to overcome potential attendance barriers (Heinrichs et al., 2005).
Method
Setting
This study was conducted in Udon Thani province after consultation with the MOPH and UNICEF to bolster ongoing local efforts to prevent violence through the public health system and community-based networks. Udon Thani is one of the 20 provinces in Northeastern Thailand, the country's largest region and where the highest number of those living in poverty reside (Office of the National Economic and Social Development Council, 2025). Most of the population speaks the Isan language at home, although Central Thai is widely understood. Several participants from Bangkok and Chiang Mai were also interviewed to provide a broader perspective, given that MOPH wished to explore the potential for national dissemination.
Participants
Study participants (N = 26) were recruited via phone and email through purposive sampling from multiple sectors to strengthen the validity of narrative accounts (Creswell & Miller, 2000). Fifteen interview participants were identified via referrals from the Provincial Public Health Office, five from key informant lists in two UNICEF reports (McCoy & Supaporn, 2016b, 2016c), four through snowball sampling, one as a self-recommended replacement for an absent key informant, and one as a key informant from UNICEF. To participate in individual interviews, respondents had to belong to one of three groups: policymakers (i.e., district-, provincial-, and national-level officials; n = 8); practitioners (i.e., frontline health, social welfare, or education providers; n = 9); and professionals in public health, child protection, and early childhood education (n = 4). Six respondents were also invited to join a Thai Parenting Experts Working Group to advise on the study. Inclusion criteria for working group membership required participants to be involved in researching, advising, and/or providing services to families with young children. No persons refused to participate or dropped out of the study.
Data Collection Procedures
All data collection instruments were translated into Thai. Individual interviews and focus group discussions (FGDs) were conducted in parallel. After providing written informed consent, participants completed a short demographic survey. Seventeen interviews were conducted in Thai and Isan by the lead author and a research assistant, and three in English by the lead author. Three FGDs with the Thai Parenting Experts Working Group were conducted in English and Thai, depending on the topic. Interviews lasted 60–120 min, while FGDs lasted 3–5 h. Interviews and FGDs were audio-recorded, and FGDs videotaped. These were transcribed verbatim, with Thai dialogue translated into English. The lead author and research assistant also took written notes of key points and emerging themes. No compensation was provided to interview participants, while FGD participants were offered lunch and travel subsidies. Ethical approval was obtained from the relevant institutional review boards, and participants provided written informed consent prior to participation.
Interviews were semistructured and included five broad themes: (1) the respondent's role in services for parents of young children; (2) key issues relevant to adapting PLH-YC; (3) potential program delivery structures and schedules; (4) program logistics, including deliverers, setting, recruitment, attendance, and engagement; and (5) potential for scale-up and embedding within the public health system. All respondents received a two-page project brief before the interviews. After each interview, written transcripts and interviewer notes were examined for additional emergent themes, which informed probing questions in later interviews.
The FGDs were also semistructured, with participants receiving a copy of the PLH-YC facilitator manual before the first meeting (Lachman et al., 2018). Moderators during the first FGD included two PLH-YC developers, who determined a priori that the original 12-session program should be reformulated into a shorter eight-session version so that it would be more feasible to deliver given local resource constraints. This discussion explored each of the original 12 program themes, with moderators probing the feasibility and cultural relevance for the Thai context, including whether components should be altered, excluded, or combined (Wainberg et al., 2007). The second discussion centered on a proposed restructuring of the program and the review of illustrated stories. Before the third discussion, a draft manual featuring adapted illustrations by a Thai artist was shared, incorporating participant inputs and aiming to balance fidelity and fit to the target population. In this final meeting, the moderators probed the content, structure, and flow of each of the eight sessions. Transcripts and summaries of FGDs were shared with working group members for comment and correction.
Data Analysis
We used thematic analysis to examine all qualitative data (Braun & Clarke, 2006). We took a hybrid approach, combining deductive methods driven by the theoretical underpinnings of parenting research with an inductive approach (Crabtree & Miller, 1999). First, the lead author, as lead coder, and A.S., who was not involved in data collection, agreed on a Cohen's kappa coefficient interrater reliability threshold of k = 0.70, which indicates substantial agreement (Landis & Koch, 1977). Next, the lead coder developed an initial coding framework and preliminary manual based on the semistructured interview questions and emergent patterns and themes (Patton, 2015). Using NVivo 12 Pro, coders applied the coding frame to each transcript, revising the frame after each iteration. A high agreement was ultimately achieved across all codes (mean k = 0.81). The lead coder then coded the remaining transcripts and reexamined them for patterned responses, broader meanings and implications, and divergent viewpoints.
Results
Most interview respondents were female (see Table 1). Many were frontline workers in the health, social work, or education (42%) and possessed 11 or more years of experience (65%) and graduate degrees (73%).
Participant Characteristics (N = 26).
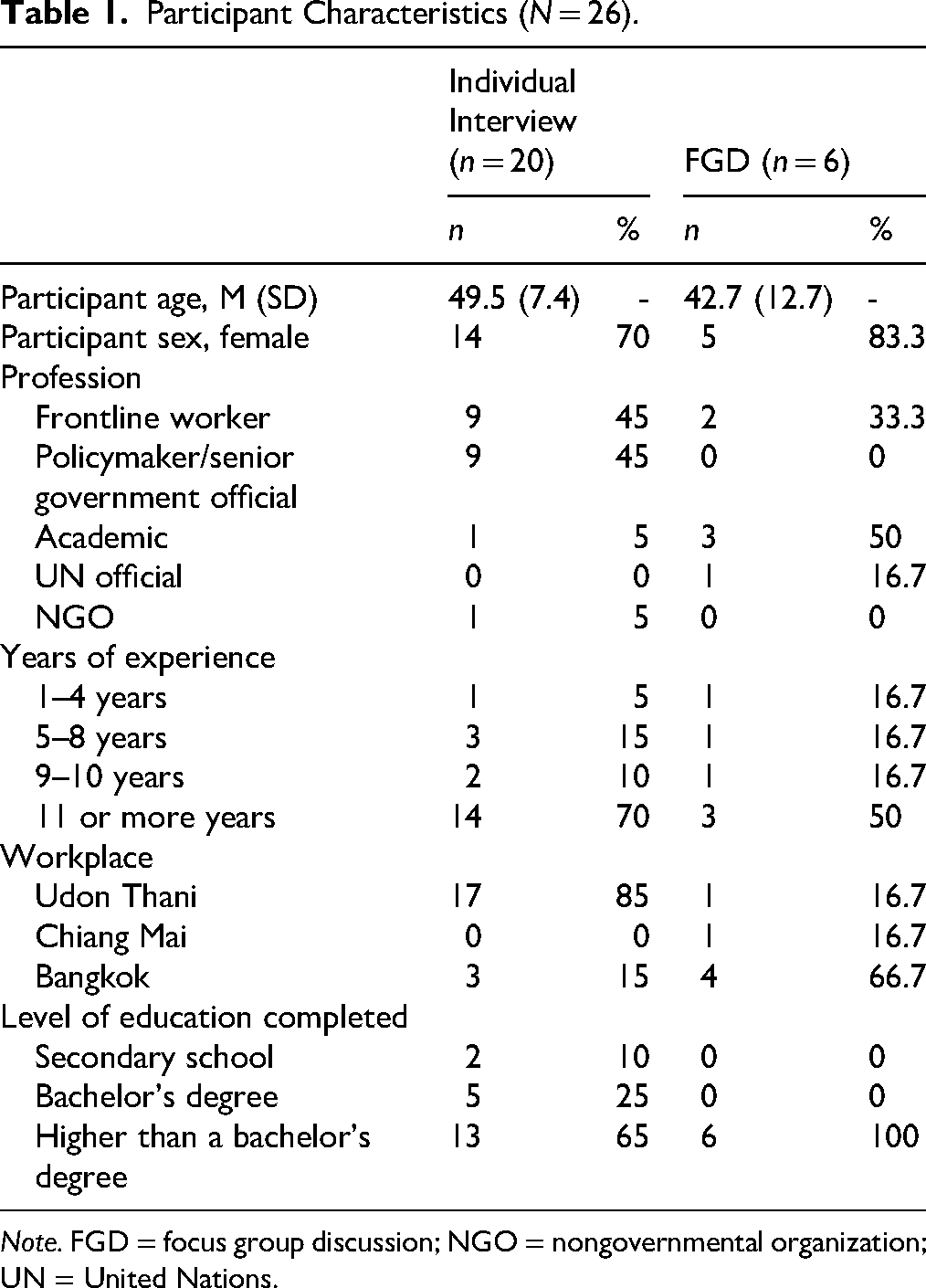
Note. FGD = focus group discussion; NGO = nongovernmental organization; UN = United Nations.
Cultural Focus
A key emergent issue was whether and to what extent the content and materials should be based on the local Isan language, social norms, and material culture in Udon Thani, as opposed to a pan-Thai orientation. Participants agreed that it would be appropriate for materials to be in the Central Thai language, given the similarities of many customs across geographic regions, as well as for practical reasons. A nurse based in Udon Thani (ID#15, interview), who had completed the PLH-YC facilitator training, explained: “I think this one can be used all over the country, not only the people in Isan because of the nature of the Thai people—the matter of tradition is not different.”
Many participants, however, also recognized the value of delivering the program in Isan and incorporating aspects of localization. One reason was due to the potential for forging closer ties with participants. A provincial-level policymaker (ID#3, interview) expressed: “The local language insinuates friendliness, familiarity, siblings … easy to talk and to understand.” Another policymaker (ID#10, interview) insisted that facilitators should be capable of translating the content into Isan during spoken delivery. References were made to strategies used by other parenting programs transported to Thailand, with one NGO worker (ID#1, interview) noting that space could be provided within the manual for facilitators to write their own notes in the local language to guide session facilitation.
Several references were made to the potential infusion of religious practices into program content. One Chiang Mai-based psychologist (ID#22, FGD) advised that although the taking a pause exercise used throughout the program for stress management could be linked to Buddhist mindfulness and meditation, it would be best to avoid the incorporation of religious terms when PLH-YC is being delivered in diverse communities: “… there might be some Muslims, some Christians … [so] maybe not appropriate.” For instance, two respondents cautioned that the program materials would need to be tailored for the Southern Thailand region, given the strong influence of Islam, with one NGO worker (ID#1, interview) flagging: “Thinking of parents in … the deep South … it's completely different … If anything contradicts their religious teachings, how would you explain that? … Because they thought that this is what the religion says [and] you have to follow [it].”
Finally, several experts suggested surface-level adaptations of the illustrated stories. Given that many children in Northeast Thailand are looked after by their grandparents, the Thai Parenting Experts Working Group members agreed that story characters should include grandparents. Adaptations to story scenes depicting play were also suggested, in order to portray toys used by children in low-income families. In reference to one story where a child is playing with building blocks, one local academic (ID#27, FGD) proposed an alteration: “They [children in Udon Thani] play with rocks … with leaves, things that you pull off a tree ….” Modifications to the presentation of local food and household items were also suggested, with the latter including the illustration of earthen jars instead of sinks, and the removal of beds and tables given rural customs to sleep on bedrolls and to sit on the floor during mealtimes.
Program Themes
Respondents had specific views regarding the cultural relevance of program content and the core themes. Except for time-out, the original themes were widely regarded as appropriate and important to maintain in the Thai program. A social worker from Udon Thani (ID#19, interview) remarked: “I think that it [the content] is all included and relevant. It aims to improve the quality of life of children … it covers everything.”
Within the overarching function of positive parent–child relationship building, which encompasses the first three program themes, participants underscored the strong linkages between these themes and the potential for condensation. Participants also emphasized the importance of the theme of dedicated one-on-one time, given the perceived lack of parental devotion to relationship building and the prioritization of work and income generation. According to one village health volunteer (i.e., community health worker) (ID#16, interview): “Most of them just don’t have enough time for their kids … this is the main issue.” A few pointed out that parents either lacked skills in engaging in play or did not want to play with their children. One local academic (ID#27, FGD) was particularly emphatic in stating: “They do not know how to play.” Clinician respondents also strongly embraced the value of strengthening communication about emotions, especially given the tendency to avoid such topics in Thai culture. Furthermore, according to a Bangkok academic (ID#23, FGD), emotional self-regulation is a widespread cultural challenge for Thai people: “It's not normal in Thailand to teach [children] how to manage their own feelings … We’re not taught to be responsible for our emotions.”
Under the second overarching function of positive reinforcement, specific and constructive praise was regarded by two Bangkok-based experts as one of the most valuable program components. They remarked that their research showed that parents used only two particular skills after completing their parenting program: praising and emotional validation (ID#23, FGD). However, participants reported that many Thai parents believed that praising was harmful, as it was perceived to fuel narcissism. A social worker in Udon Thani (ID#19, interview) explained: “That's why not many people use it with their child. It shouldn’t be like that. It would be good for parents to try and compliment their child in a positive way ….” Respondents who had previously delivered parenting programs also contended that praising was “unnatural,” as Thai parents had never been parented that way themselves. One academic in Bangkok (ID#24, FGD) pointed out: “… they never use it … they never experienced it.”
Regarding instruction giving, two Bangkok-based academics suggested building in flexibility, using timers during transition warnings, and emphasizing the importance of understanding the child's perspective, noting that they had seen successes with these techniques with Thai parents. Several experts also advocated that child participation in decision-making should be integrated into household rules and routines. One Bangkok-based psychologist (ID#26, FGD) advised that it could be incorporated in moderation alongside parental authoritarian tendencies, stating: “… because of how Thai culture is and everything, it's good to be directive, but maybe we could ask them to be part of at least one rule, where they have an agreement with the child.” One policymaker in Udon Thani (ID#7, interview) was strongly in favor of making household rules and routines an integral part of the program. He asserted: “I want this program to emphasize parents setting a good example and how to do it.”
The final overarching element in PLH-YC—positive discipline—is manifested through redirecting, ignoring, giving consequences, and using time-out. Parenting experts stressed the interlinkages between these themes, with redirecting and ignoring constituting forms of consequences for unwanted or difficult child behaviors. Bangkok-based respondents also advised offering children choices of potential consequences for negative behavior, with one participant (ID#24, FGD) stating: “… the consequences will work very well when the kids know that this is the consequence from their own choice.” However, a Bangkok psychologist (ID#26, FGD) pointed out that this tactic may not be acceptable to Thai parents “… because they might feel like they’re relinquishing the control over to the children.”
Participants widely regarded time-out as prone to misuse and potentially harmful to children. Several experts underscored that two imported parenting programs they had delivered to Thai families did not include time-out. A Chiang Mai-based psychologist (ID#22, FGD) mentioned: “[It's] not encouraged … because there's a risk of using it in a punitive manner.” A Bangkok-based practitioner (ID#23, FGD) stated that time-out was not representative of positive discipline and that a preferential method—which she had used successfully at her child development center—would be to encourage children to enter an untimed and self-imposed break to regain emotional control.
The final themes—resolving conflicts in the family and reflecting and moving on—were perceived as not essential. The necessity of parent–child collaboration in this conflict resolution approach and parental instinctiveness to explain and settle problems for children rather than with them were cited as reasons to potentially deprioritize this theme. One Bangkok-based psychologist (ID#26, FGD) explained: “Maybe parents would feel like it's instinctive for them to solve the problem for the child, instead of just asking for the child's solution.”
Delivery and Structure
Participants shared their views regarding the appropriateness of nondidactic, participatory problem-solving-based methods used during PLH-YC delivery. All participants extolled the benefits of group discussion and the fostering of exchange and mutual support: “Doing a group workshop is a good thing … It's about being an example in the group … so they can learn by exchanging stories, and that makes it easier to remember” (ID#9, interview). Two participants asserted that in-session practice and homework could help fuel this collaborative process, including a local public health officer (ID#17, interview) who commented: “I think they’ll pay attention when you engage them and let them practice … But if you just lecture them and ask them to practice at home, it's likely they wouldn’t be able to do it.”
Several Bangkok-based academics who have facilitated parenting interventions also shared that, in their experience, providing “scripts” to parents was an effective method. They remarked that parents often had trouble communicating positively with their children, particularly regarding their emotions. They recommended using words to initiate the conversation, such as mae kaojai nu sao (“Mother understands that you feel sad …”) and mae dai yin wa nu yaak dai (“Mother understands that you really want this …”). They also commented that templates for praise worked well with Thai parents: “We said you can praise but you have to have the three keywords—the word for praising, then specific behaviors, and the last one is very important—like, the adjective” (ID#23, FGD).
Participants were asked to share their thoughts on the group-based format of PLH-YC in comparison with one-on-one modalities. Most participants expressed that group formats were preferable and that individualized sessions were more “problematic” and better reserved for those with particular needs. Resource constraints were also cited as justification for group formats, with one education sector policymaker in Udon Thani (ID#5, interview) asking: “Group-based workshops are beneficial in a sense that we don’t have to use that many facilitators, time, or resources, right?”
Respondents saw the value of combining group-based sessions with individualized home visits. One village health volunteer (ID#16, interview) pointed out that both formats were beneficial and could coexist, with one-on-one visits providing an opportunity for in-depth learning about parents’ needs and circumstances. Participants further explained that a home visit would allow facilitators to observe the “truth” concerning how the child and family interact with each other. One Bangkok-based child psychiatrist (ID#2, interview) remarked: “I think for home visits … you can see how they speak and how they talk to the child.” Several participants also pointed out that home visits were already part of regular service delivery by nurses, teachers, and village health volunteers. Finally, participants underscored the importance of having a friendly demeanor during such visits, and that visitors should aim to establish close ties. One local social worker (ID#19, interview) advised: “… we would visit them like we visit our relatives and care about them.”
Several challenges regarding home visits were raised. Some participants cautioned that these visits needed to be conducted in a sensitive manner, particularly given the program's primary aim of preventing violence against children. One nurse in Udon Thani (ID#20, interview) shared: “People in the community know that there is a project in their community … I don’t know if it will be risky …? Will they be seen as a family that abuses children?” Further, two respondents were concerned about the potential burden on facilitators, especially nurses. One public health officer (ID#17, interview) noted: “Even if their job is to do visits … not many do it, and most don’t want to.”
Respondents were also prompted to advise on the timing of parenting sessions for low-income families in Udon Thani. Sundays and mornings were recommended as the most convenient for working parents, although several noted that many grandparents may be available at any time as they were less likely to work. However, the lack of facilitator availability during weekends was cited as an obstacle to this. One local teacher (ID#4, interview) remarked: “If there's going to be a problem it will be with the facilitators, because it's also their day off.” In contrast, some respondents noted that weekend scheduling would be preferable. According to one local policymaker in the public health sector (ID#11, interview): “It would be convenient for the staff … [as] sometimes they have shift work.”
Recruitment, Attendance, and Engagement
Respondents shared various strategies they thought would be effective for program recruitment. Many strongly emphasized the importance of identifying and contacting eligible parents through collaboration with local community actors and institutions. Village health volunteers were widely mentioned as the most relevant and effective partners. One local public health officer (ID#17, interview) stated: “If the village health volunteers get through to them then they’ll come, because they trust (them) … even more than the doctors. They see them as relatives from the same family.” Several respondents from the education sector pointed out that teachers at Early Childhood Development Centers and primary schools could also play a key role in recruitment. Announcements through village heads, village public address sound systems, and brochures were also cited as potential recruitment strategies.
Regarding the target population, many participants emphasized that most young children in Udon Thani were cared for by their grandparents, who often did not provide quality care and were difficult to reach and influence. A provincial-level policymaker (ID#9, interview) shared: “… parents are at work and only the grandparents are left … They’re old so sometimes they get it, sometimes they don’t.” Increased risk of abuse was one such problem perceived by a senior-level policymaker in Bangkok (ID#10, interview), who noted: “The children who stay with their grandparents have more risk of violence, compared to staying with their own parents.”
Although some saw the value of recruiting families with known cases of abuse, several participants expressed that this would be counterproductive and that more supportive approaches were appropriate. One provincial social welfare policymaker (ID#6, interview) stated: “When we invite them, we can’t say ‘high-risk families’ or ‘families who use violence.’ Don’t say it like that … They won’t come. Invite them and say this family should join this activity so we can learn as a group.”
Most respondents believed it would be appropriate to provide low-income families with incentives such as monetary compensation or services to encourage recruitment and attendance. In line with the original design of PLH-YC, suggested services included childcare during parenting sessions and transporting attendees with vehicles belonging to health promotion hospitals—government health centers located at the subdistrict level. One provincial-level policymaker (ID#3, interview) stated: “If a meal is readily provided—free food—and you can bring your children … They’ll be more than happy to come because then they have nothing to lose.”
Respondents also shared their views regarding the types of professions that would be most appropriate to deliver PLH-YC within a public health setting: nurses, village health volunteers, public health officers, or social workers. Several participants explained that parents perceived and trusted these professions in a hierarchical manner according to perceived professional prestige. One nursing academic (ID#14, interview) stated: “… Doctors would be most believed followed by nurses, public health officers, social workers, and village health volunteers.” Others emphasized that the personal characteristics and skills of the facilitators were more important than the profession, with desirable attributes including being friendly, playful, sensitive, observant, passionate, and able to communicate simply and effectively. According to one local social worker (ID#19, interview): “First of all, their heart should be in it before it starts.”
Nurses—who are colloquially referred to as maw, the same Thai term for doctors—were frequently described as competent, trusted, and familiar with families in the areas in which they work. One local social worker (ID#19, interview) noted: “People believe in our society that if the doctor/nurse said it's good, then it must be.” Further, a provincial-level education sector official (ID#5, interview) claimed: “They’ll be happy that they get to receive knowledge from the doctors/nurses. Health promotion hospitals are really important to them.” However, nurses were also perceived as not ideal facilitators due to their busy schedules and tendency to use scolding: “But you do have to choose the nurses that … are sociable, and have great relationships in the village. Not the kind of nurses that would just scold patients” (local education sector official, ID#5, interview).
Most participants described village health volunteers in a very positive light, indicating that they had the potential to become program facilitators as they were often regarded as close to families in the community, frequently conducted home visits, and were already important local actors in monitoring child development. One provincial social welfare official (ID#6, interview) explained that “villagers would have high regard for them because they take care of them in sickness and all,” while a local teacher (ID#4, interview) explained: “I see the benefits of village health volunteers … They have a closer relationship than us.” However, several persons pointed out that their capacities were variable. A local education sector official (ID#5, interview) noted that some fulfilled their roles well, while others lacked effective communication and dissemination skills.
While respondents expressed that social workers had skills and expertise in dealing directly with issues of violence, many admitted that they had little contact with them and were unfamiliar with their work. Most of those who understood the role of social workers, however, spoke positively about their involvement: “If they meet children that have family problems … if violence occurs, they will be able to help out in this case” (nurse in Udon Thani, ID#15, interview). Alternatively, a subdistrict social welfare official (ID#18, interview) was wary that the involvement of social workers could raise suspicions: “Hypothetically, if public health officers or nurses plan to visit a client one-on-one it would be normal … But if the social workers go in, they’ll ask, ‘where did you come from?’”
The involvement of public health officers was widely perceived as appropriate, as they already collaborate with nurses at health promotion hospital Parent Schools and tended to be skilled at working with community members: “I think they would be a good group of facilitators and would be better (than nurses). Nurses work mostly in … treatment, but if it's community-based then it would be the officers that go into the village” (local hospital director, ID#8, interview).
Finally, teachers were described as possible program facilitators by several participants, who noted they were accustomed to conducting home visits and were more familiar with the behaviors of children in the community. One local public health officer (ID#17, interview) explained: “It's like they’re another parent … I think they’re better than doctors/nurses.” However, one Bangkok-based respondent (ID#23, FGD) posited that the content of PLH-YC may be in conflict with local teaching practices: “The reason they [parents] don’t like teachers is because … they use negative discipline, so when they say something that contrast to their behaviors, it's hard for human [parents] to understand and believe it.”
Setting for Program Delivery
Participants were asked for their views regarding the proposed hospital setting for the program, as well as their suggestions for other appropriate venues. Many participants underscored that health promotion hospitals were village based and accessible, well equipped, open during weekends, operate shuttles for picking up participants, and already host Parent Schools. According to one local nurse (ID#20, interview), “It is more convenient because, actually, the health promotion hospital is like a hub of the community.” It was also perceived as less stigmatizing: “But if we make an appointment at the health promotion hospital, then it seems like we’re prioritizing health and wellness … People wouldn’t think that a child in this house has a problem, that's why they’re going to the workshop” (local social worker, ID#19, interview). However, one local mental health official (ID#21, interview) saw the setting as potentially stigmatizing: “Sometimes if we call them to the health promotion hospital, it's like they are in a problem group … There is some stigma to a certain extent.”
Respondents also mentioned primary schools, child development centers, nurseries, subdistrict administrative offices, village pavilions, and temples as other possible venues. However, several people expressed doubts about the appropriateness of such places, with one local education official (ID#5, interview) noting that “the village sala [pavilion] is too hot, too loud … and it's disorganized.”
Potential for Scaling Up
Participants were prompted to share their views regarding any potential opportunities or obstacles regarding the scaling up of PLH-YC, with an emphasis on prospects for integration within the public health system. Overall, interviewees were optimistic that such a program could become a regular health service, provided that certain strategies were followed. Several participants advised that a key strategy was to work through top-down channels, such as by embedding the program within a ministerial policy. One local nurse (ID#20, interview) noted: “If we bring anything that is not in the policy, it will … not get support … but when it's executive level policy, it will be successful or will be used as a key performance indicator of the ministry ….” A provincial-level social worker (ID#19, interview) added that research supporting the program's effectiveness would assist in promoting such a policy:
If research supports it, then we can see its feasibility and request for it to be included in the ministerial-level service plan. In terms of the multidisciplinary team on the front lines … it could be included in their manual of job responsibilities … [and] the coursework for nursing colleges or at the department of social work.
Many participants commented on the suitability of situating the program within the public health system. Some indicated that officials sometimes questioned whether it was appropriate for the MOPH to tackle violence prevention, as this was perceived to fall within the remit of the Ministry of Social Development and Human Security. However, there was an acknowledgement that the latter did not have sufficient local-level reach to address violence prevention: “I now think that it would really work best at the Ministry of Public Health, even though family issues actually fall under the role of the Ministry of Social Development and Human Security. But this ministry does not have local connections … They don’t have the resources” (provincial-level public health officer, ID#9, interview). Several participants pointed out that implementation through the public health system would work well, as they were already delivering parenting programs through health promotion hospitals, which were part of a broader organizational network linked to the provincial and district public health offices.
Many participants also highlighted the value of developing partnerships between the health promotion hospitals and the Tambon Administrative Offices. One municipal-level official (ID#3, interview) stated that these offices were well resourced: “Reason number one … They have all the 4 M's … Men, Money, Management, Materials.” One subdistrict level official (ID#18, interview) underscored that sustainability was possible if working in cooperation with these offices: “It would be sustainable if they [the Tambon Administrative Offices] worked together with the hospital and created a memorandum of understanding.”
Several others perceived that it would be better to involve schools. A local mental health policymaker (ID#21, interview) noted: “If we can organize it in … nursery and primary school, … the public health staff can assist the ‘hardcore’ [parents who use violence] group. It would be better, more sustainable, and right. It shouldn’t be in hospitals.” However, one local academic (ID#14, interview) cautioned that this may not be appropriate as violence was also perpetrated in schools: “Schools have problems with violence too … I think there is already a policy [against violence], but in practice it's different.”
Several participants also suggested undertaking a “model” approach, with a particular subdistrict demonstrating how PLH-YC could be implemented through various departments and professionals in practice, which then serves as a learning center for other subdistricts prior to expansion. One senior policymaker (ID#7, interview) advised: “We can … make that sub-district a model. A model that collaborates with public health officers and local authorities related to education and health centers … You could collaborate with … the heads of villages, community leaders, and village health volunteers.”
Despite the myriad possibilities, some participants suggested that scaling up PLH-YC would be met with challenges at the senior management level due to the divisions that persist between and within ministries, departments, and administrative geographic regions, as well as due to the overburdening of frontline workers. One provincial-level public health officer (ID#9, interview) noted: “If you only do it in Udon Thani … would they [MOPH] accept that? You have to increase the area to different regions for them to believe in the program, that it works, and it is possible.” A mental health sector policymaker (ID#21, interview) suggested that a plethora of programs and approaches already existed without sufficient time and training for implementation: “There are many instruments in Thailand … It takes too much time … and the new one is coming … Is there a new instrument? I haven’t used the old one to the fullest extent yet. This is an obstacle.”
One subdistrict-level official (ID#18, interview) underscored that the current workload of members on his team would prevent them from fully implementing the program in practice: “We’ll take what's suitable for us to use. But we’re not going to count from one to 10, we’re not going to do weekly home visits, and how many hours per week. We can’t really do it, can we?” Finally, one mental health policymaker (ID#21, interview) divulged that challenges with cross-sectoral collaboration would hamper scale-up efforts, therefore requiring careful selection of sites:
It isn’t only the responsibility of the MOPH … It requires cooperation amongst many sectors, such as the local area, civil society, and community members … Is cooperation smooth in Thailand? It isn’t. They still work separately. It will affect expansion. That's why you should work in the areas that are ready … then it will work.
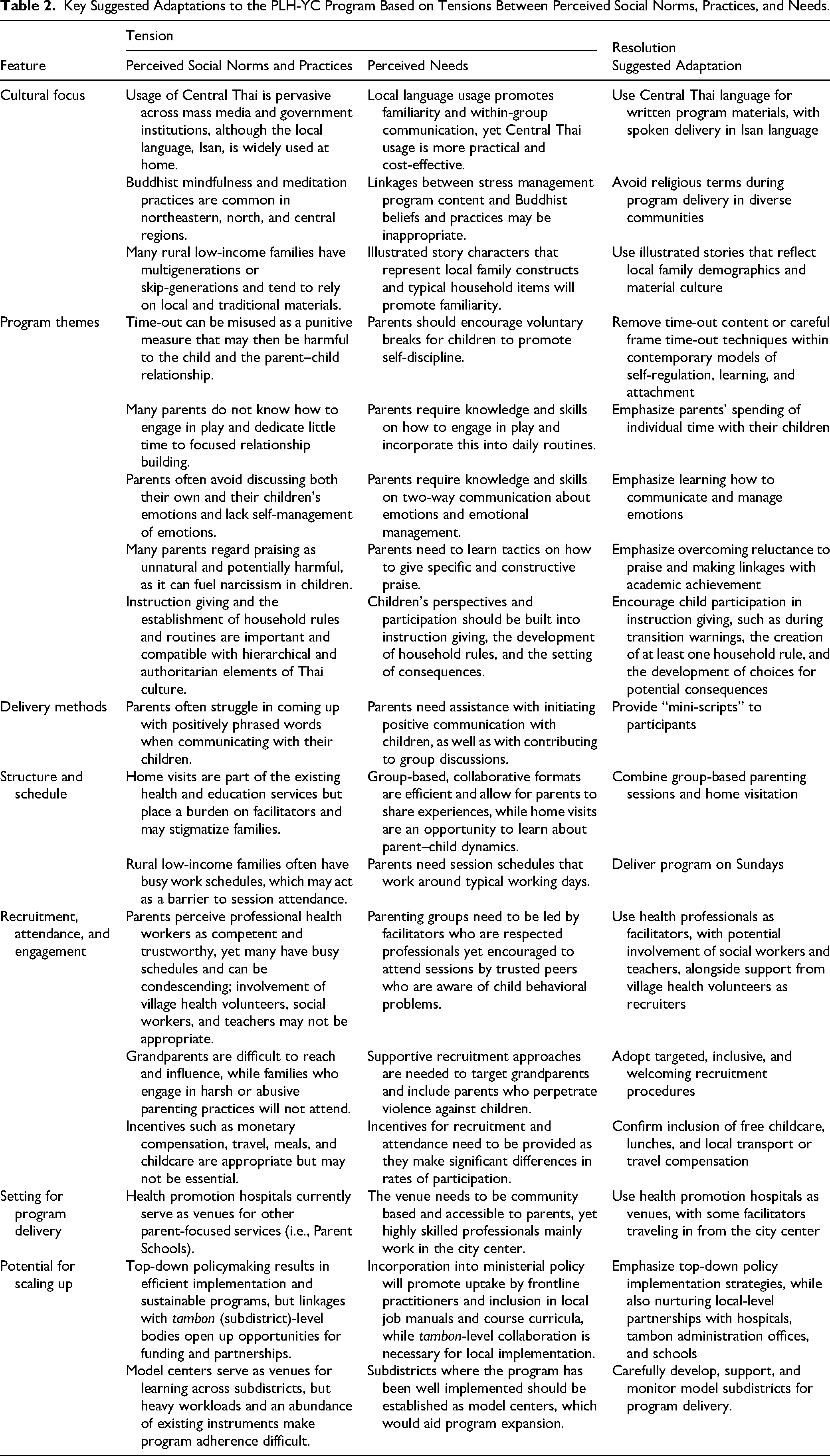
Table 2 summarizes the emergent themes regarding perceived social norms, practices, and needs, along with the adaptations suggested by respondents.
Key Suggested Adaptations to the PLH-YC Program Based on Tensions Between Perceived Social Norms, Practices, and Needs.
Discussion and Applications to Practice
This study aimed to understand the cultural and contextual relevance of the key program themes, process, structure, schedule, and logistics of PLH-YC and explore potential barriers and opportunities for scaling up an adapted version of the program. Emergent themes regarding tensions between existing social norms, practices, and needs, as well as proposed resolutions, provide a useful foundation for program adaptation. To our knowledge, it is the first formative evaluation for a parenting program that aims to reduce violence against children in Thailand and one among few such evaluations conducted in LMICs, including Panama (Mejia et al., 2014, 2015), South Africa (Lachman et al., 2016), and Uganda (Siu et al., 2017). It is also the only formative evaluation that has specifically targeted integration within the public health system in an LMIC.
Study results suggest that most of the original PLH-YC program themes were culturally relevant for practitioners and families in Thailand. However, respondents regarded time-out (in the traditional sense of time-out from positive reinforcement, i.e., as a punishment) as potentially harmful, although the reasons cited did not draw from experiences in implementing this technique in a Thai context. These views reflect the ongoing debate in the field on the use of time-out as a strategy (Dadds & Tully, 2019) and conflict with evidence that it is associated with larger parenting program effects (Kaminski et al., 2008; Leijten et al., 2019). The consistent disapproval of time-out by respondents suggests that it should not be included in the Thai version of PLH-YC; alternatively, it could be carefully framed within contemporary models of self-regulation, learning, and attachment and used as a “cool down” before discussing bad behavior with a child to help ameliorate tendencies to use this technique punitively (Dadds & Tully, 2019). An emphasis on the broader goal of developing children's ability to self-regulate their emotions, which is consistent with Buddhist concepts of sati (careful awareness of one's thoughts and feelings), as well as the use of meditation to attain calm (Kelly, 2008), may also make this skill more appealing to Thai parents and practitioners. However, while such an approach may be well embraced in most communities in Udon Thani, where 99.5% identify as Theravada Buddhist (Community Development Department, Ministry of Interior, 2017), its explicit incorporation into a common, national version of PLH-YC may be perceived as culturally inappropriate in Muslim-majority populations in the South. This tension between evidence on the effectiveness of time-out and local cultural preferences points to the need for additional consultations and multi-arm research with other religious communities in Thailand, with potential testing of versions including and excluding time-out content.
Respondents expressed varying degrees of concern that parents would struggle to apply certain skills and dedicate little time to do so, particularly those that focus on positive parent–child relationship building. This may be related to parents’ poor understanding as to how such play is conducive to warm and positive parent–child relationships and supports healthy child development. These findings correspond with other qualitative research with parents and health workers in central Thailand (N = 25), which found that caregivers had difficulties managing time for child development activities and had limited knowledge of how play benefited child development (Morrison et al., 2018). Parents’ lack of time is backed up by data showing that Thailand is one of few countries with weekly work schedules often exceeding 48 h (Lee et al., 2007). Given the recommendations to include a child development education component in the program, as well as ethnographic research findings from Eastern Thailand (N = 22 families), which suggest that caregivers who were aware of the benefits of early child development were more likely to effectively interact with their children (Chivanon & Wacharasin, 2012), it would be important to incorporate this topic. Finally, the perception that communicating about emotions would be challenging for Thai families given the cultural avoidance of socio-emotional communication is reflected in ethnographic research with nurses and nurse educators (N = 14) in Thailand. This study found that not expressing strong feelings might relate to the Buddhist principle of non-attachment to people and objects (Burnard & Naiyapatana, 2004). Thai social norms tend to value emotional neutrality and distance, which must conform to one's “status, power, rank, and seniority” in relation to someone in a more exalted position, such as a parent (Klausner, 1993, p. 381; Weisz et al., 1987). Suggested adaptations for overcoming this tension thus included emphasizing socioemotional communication and self-management of emotions.
Several respondents perceived that Thai parents would struggle to involve children in conflict resolution, which requires child participation in problem-solving. This contrasted with suggestions by Bangkok-based parenting experts that the program should help parents engage children in establishing and enforcing household rules and routines. This approach may be more feasible with middle-class, university-educated urban parents, but perhaps overly aspirational for rural families who may be more likely to embrace a traditional emphasis on hierarchical family relationships and on teaching people to obey according to their level of seniority (Auemaneekul, 2013). Moreover, a multicountry cross-sectional survey including Thai Buddhist participants (N = 232) found that Thais were more likely to use indirect, ambiguous, and nonconfrontational strategies when faced with conflict; this preference is common to high-context cultures, or cultures where individuals are prone to using implicit rather than direct communication codes (Croucher et al., 2012). Such roles and preferences may thus translate to reluctance to involve children in conflict management within Thai families and within the style of program delivery. Nonetheless, the view by several participants that the adapted program should somehow address interpartner and intrafamilial conflict, and even include partners and extended family members as program enrollees, underlines that the issues of conflict resolution and synergistic parenting are critical.
Finally, respondents made several practical propositions regarding PLH-YC materials. Although the shared view was that the facilitator manual should be written in the Central Thai language, the delivery of the program in Udon Thani should be in Isan; providing space within the manual for facilitators to note down concepts and examples in Isan may thus be a simple yet useful modification.
Findings also demonstrate that respondents regarded the program's process, structure, and schedule as relevant and suitable to the local context. Regular skills practice and homework, the group-based format, the inclusion of home visitation, and the timing of weekly sessions over 8 weeks were perceived by most as appropriate and feasible. However, while the participatory discussion methods were broadly embraced by participants in both Bangkok and Udon Thani, this stood in juxtaposition with existing practices for the top-down teaching of parents within the public health system. The lack of sufficient precedent in utilizing such methods, the cultural deference toward doctors and nurses, and the value placed on emotional distance between those of differing status may present challenges for health professionals in undertaking a facilitator role that relies on open exchange and the sharing of personal challenges. Health professionals may thus require focused facilitator training and additional coaching on how to adopt collaborative methods and avoid gravitation toward didactic instruction.
Most respondents spoke affirmatively regarding involving nurses as facilitators, referring to the significant trust and respect they command from villagers. Nurses are fundamental to the Thai health system given their qualifications, geographic distribution, and numbers (180,000 in 2016), with each health promotion hospital typically staffed by three to five nurses who serve a subdistrict population of 3,000–5,000 people (Tangcharoensathien et al., 2018). The predominant perception that nurses would be the most suitable service providers is corroborated by qualitative research with parents and caregivers in Bangkok, Chiang Mai, and Trang, which found that parents indicated that they would trust health professionals over all others for the provision of useful parenting information (McCoy & Supaporn, 2016a). Moreover, a comparative study on doctor–patient communications in several Asian countries, including Thailand, highlighted the great esteem that these professions are afforded within Thai institutions, based on the general sentiment that they are persons of high status who impart important information to patients—who are in a subordinate position (Matusitz & Spear, 2015). The potential for condescension in such a dynamic may have reinforced the perception that nurses known for “scolding” should not be selected as program deliverers, given that they may not exhibit the friendliness, passion, and sensitivity some participants expressed as vital characteristics of all facilitators.
Findings regarding the potential strengths and challenges of utilizing village health volunteers are reinforced by other qualitative research in central Thailand. Such studies have found that although most (61%) have only a primary level of education, village health volunteers are able to readily address health problems from the strength of existing, trusted relationships and that their collaboration with health professionals enhances their credibility within communities (Kowitt et al., 2015; WHO, 2007). This rapport and local presence mirror the potential of utilizing community health workers to promote early childhood health and development in other LMICs (Rotheram-Borus et al., 2014; Yousafzai et al., 2014). The favorable reputation of village health volunteers in Thailand has been cultivated since their establishment in the 1960s; in 2010, there were over 800,000 active volunteers, providing coverage to 12 million households (Kowitt et al., 2015; WHO, 2007). The functions, capacities, and social perceptions of village health volunteers thus merit proper consideration as facilitators who could be paired with nurses for parenting program delivery.
An important logistical factor was related to the program setting. Access to parenting programs has been identified as a crucial factor for the successful engagement of low-income families (Axford et al., 2012); at the same time, the employment of nurses, village health volunteers, and social workers as facilitators would need to address their access barriers as well, to encourage their involvement. This is particularly critical given the limited numbers of social workers, as well as the noted workload that nurses face. Subdistrict health promotion hospitals were mentioned by most participants as convenient, fully equipped, and community-based locations where nurses, public health officers, and village health volunteers were already based.
Finally, another logistics-related factor that will require contextual adaptation concerns the recruitment, attendance, and engagement of participants. Interviewees often mentioned that the target population would include many grandparents who are likely to reside in multigenerational or skip-generation households. The latter household type is prevalent across Thailand, where one in five children live without either biological parent—the highest such ratio out of 40 surveyed LMICs (UNICEF, 2012). Some participants expressed concerns that grandparents engaged in poor caregiving practices, opinions supported by a cross-sectional study (N = 320) in Northern Thailand, which found that children reared by grandparents were twice as likely to have delayed development compared to those raised by their parents (Nanthamongkolchai et al., 2009). In addition, the fact that 87% of over 60s in Thailand attended only primary education (Knodel et al., 2015) and that many participants in our study noted that grandparents often have mobility, hearing, and vision impairments presents accessibility considerations. Transportation arrangements, facilitation styles, recruitment and program materials, group activities, home visitation, and between-session communication methods will all need to be attuned to these challenges.
Findings also revealed several key opportunities and barriers to scaling up PLH-YC, corresponding with dimensions of the RE-AIM model (Glasgow et al., 1999). The assumption of a top-down policy implementation approach with delivery at community-based health promotion hospitals may enable intervention reach by target families, encourage adoption by local health offices and frontline practitioners, and bolster prospects for long-term maintenance. The creation of a ministerial-level policy, accompanied by requisite budgets and performance monitoring indicators, was stressed by several respondents as necessary for program expansion and institutionalization. There is an opportunity to build on the current policy emphasis by the MOPH to boost lagging developmental milestones in the northeast (Sookatup et al., 2018). This top-level political prioritization of early childhood development initiatives may constitute a promising base for further policy advocacy and for integrating parenting programs within a service package that promotes nurturing care and protection. However, the concerns of several respondents that local-level senior management may not recognize the value of parenting programs, despite national-level emphasis, demonstrate that both top-down and bottom-up policy advocacies are necessary. This is likely to require messaging that draws from the high-quality parenting intervention science literature, as well as community empowerment and user demand approaches, which parents, local officials, and service providers may find more compelling.
Another opportunity lies in the significant trust placed by communities in health workers. This reliance, combined with the nationwide reach of health promotion hospitals (Pagaiya & Noree, 2009), opens the prospect of embedding parenting within primary care units. Health services are often regarded as ideal starting points for scaling up early childhood development interventions, including parenting programs (Richter et al., 2017). Moreover, there are many examples of parenting programs that have demonstrated positive results when delivered via health sector platforms in LMICs, including Iran (Oveisi et al., 2010), Jamaica (Walker et al., 2018), Pakistan (Yousafzai et al., 2014), and Peru (Oré et al., 2011). As mentioned by some respondents, it may be acceptable to involve social workers and teachers as cofacilitators; however, the latter may first require that they complete a positive teaching program and be assessed on their ability to apply such techniques in their classrooms.
Finally, results suggest that establishing a model subdistrict, whereby local officials, practitioners, and community-based networks across sectors work in synergy to implement PLH-YC, may also be a promising scale-up strategy. Such an approach may allow for the systematic integration of an intervention within a scalable unit's existing services, followed by further testing, refinement, and evaluation prior to expansion. Local institutions would need to be sufficiently strengthened to ensure that program staff have adequate levels of competency and supervision to deliver a high-quality program alongside strong community demand for such a service (Richter et al., 2017). It would be important to carefully monitor whether PLH-YC can be sustained in such a model, particularly given participant feedback that heavy workloads and existing demands may weaken program adherence. Research on key barriers to scale-up found that diminished implementation fidelity is a common threat, which may be attributable to misjudging the readiness of an intervention to go to scale, as well as significant differences in conditions between feasibility pilot and scaled-up contexts (Yamey, 2012).
This study has several limitations. First, we used a small and purposive sample, with 14 persons identified from a list of government-recommended officials, experts, and practitioners. Thus, there was potential sampling bias due to the overrepresentation of government-approved stakeholders and those working in the health sector. Second, we did not directly interview parents or children; instead, we drew on findings from recent qualitative research with families in Thailand. This decision was made on the basis that parents would be better positioned to provide substantive feedback after directly experiencing the program during subsequent piloting. Indeed, in-depth interviews were conducted with 11 parents who had varying levels of program participation during the pilot to explore perceived changes in parent–child relationships and interactions (McCoy et al., 2021). Third, in-depth feedback on program themes could not be obtained from most respondents, except for the Parenting Experts Working Group and three practitioners who were interviewed after they participated in facilitator training. While the interviewers provided a description of PLH-YC content through a verbal overview and a program brochure, such approaches cannot compensate for a lack of full exposure to the program. Finally, participants were not sampled from the Muslim-majority south, given the study's focus on the cultural and contextual adaptation of a program for families in the Buddhist-majority northeast, which limits the generalizability of findings at the national level.
Despite these drawbacks, this study makes a useful contribution to the existing research base on cultural and contextual adaptation of evidence-based parenting programs. The findings informed the subsequent adaptation of the program (reflecting resolutions listed in Table 2), which was tested in the feasibility pilot (N = 60) from December 2018 to April 2019, demonstrating good feasibility as well as preliminary effectiveness in reducing child maltreatment and 22 out of 24 secondary outcomes (McCoy et al., 2021). These results were used to develop a slightly more refined version, which was evaluated in an RCT (N = 120) from May 2019 to January 2020 and found to be effective in improving positive parenting and reducing harsh, violent parenting (Gardner et al., 2025).
Other parenting interventions being transported to LMICs, or indeed any new contexts and systems, may also benefit from modeling this systematic approach, given that tested interventions often fail after scale-up when developers have not undertaken crucial formative work to ensure they fit the delivery system (Banerjee et al., 2017). Conducting thorough formative evaluations at the outset to guide careful cultural and contextual adaptation is an essential part of this process. There remains a need for further research in this area, including studies using factorial experiments, to examine core components of intervention delivery and scale-up (Lachman et al., 2019), draw upon mixed-method approaches, and carefully assess cultural and contextual readiness for feasibility piloting, intervention effectiveness, and long-term intervention scale-up and sustainability.
Footnotes
Author Note
Since the completion of the study, several authors have had new or additional affiliations. AM is now based at the Chiang Mai University, Department of Family Medicine and the Peace Culture Foundation, Thailand. JML is no longer affiliated with the University of Glasgow and is now also affiliated with the Centre for Social Science Research (CSSR) at the University of Cape Town, South Africa, and Parenting for Lifelong Health, UK. AS is now with the Department of Psychiatry and Behavioural Neurosciences and the Offord Centre for Child Studies at McMaster University, Canada.
Acknowledgments
We are grateful to the respondents who took the time to share their views with us. In particular, we would like to thank Dr. Chanvit Tharathep at the MOPH and the officials at the Udon Thani Provincial Public Health Office. We thank Tassawan Poomchaichote for her hard work in coordination and translating and transcribing interviews, Dr. Phaik Yeong Cheah at the Mahidol-Oxford Tropical Medicine Research Unit (MORU) for her crucial support for this project, and Dr. Inge Vallance for assistance with manuscript preparation. We thank the funders, primarily UNICEF Thailand as well as MORU (funded by the Wellcome Trust, UK) and the Department of Social Policy and Intervention at the University of Oxford, for their support.
Ethical Considerations
Ethical approval was granted by the Universities of Oxford (OXTREC Ref# 522-17), Cape Town (Ref# PSY2017-007), the MOPH (Ref# 10/2561), and the Udon Thani Provincial Hospital (Ref# 0032.1/11102).
Consent to Participate
All participants provided written informed consent prior to study participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: UNICEF Thailand, Grant PCA/THLC/2017/002 to Prof Gardner, University of Oxford; UK Medical Research Council and Scotland's Chief Scientist Office's Social and Public Health Sciences Unit through Complexity in Health Programme (MC_UU_12017/14) and Relationships and Health Programme (MC_UU_12017/11).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study was part of a multiphase project funded by UNICEF Thailand. As per the agreement between the University of Oxford and UNICEF, the manuscript was submitted to UNICEF for review before journal submission. UNICEF requested no changes. All authors were engaged as consultants or university staff under the project. The Parenting for Lifelong Health for Young Children (PLH-YC) program was developed by the PLH partnership, now a registered UK charity (![]() ). JML, CLW, and FG are PLH co-founders and developers; JML serves as the charity's CEO. None of the authors derive any royalties or other funds from use of the program, although JML has on occasion received fees for training. Our universities receive research grants for studies of PLH, and this does benefit our careers.
). JML, CLW, and FG are PLH co-founders and developers; JML serves as the charity's CEO. None of the authors derive any royalties or other funds from use of the program, although JML has on occasion received fees for training. Our universities receive research grants for studies of PLH, and this does benefit our careers.
Data Availability Statement
Deidentified qualitative data from this study, including coding frames, can be accessed by contacting the first author.