
Abstract
Introduction
Adolenscence is marked by dramatic neurological, hormonal, social, cognitive, emotional, and behavioral changes (Brandt, 1977; Vijayakumar et al., 2018). Adolescents in search of their identity often rebel against their parents, exposing themselves to imminent risks. This can make parents feel powerless and hopeless, and, consequently, parents may unsuccessfully attempt to engage their children in therapy. Additionally, as argued by Lieneman et al. (2017), parents who successfully motivate adolescents to enter therapy often report the adolescents’ lack of willingness to embrace the therapeutic process. In fact, treatment discontinuation is a widespread phenomenon in child and adolescent mental health services, with 28%–75% of young clients quiting treatment prematurely (Desrosiers et al., 2020; Swift & Greenberg, 2012). Forcing youth into therapy via lawful actions such as detention has also been tried and found to be ineffective (Parhar et al., 2008).
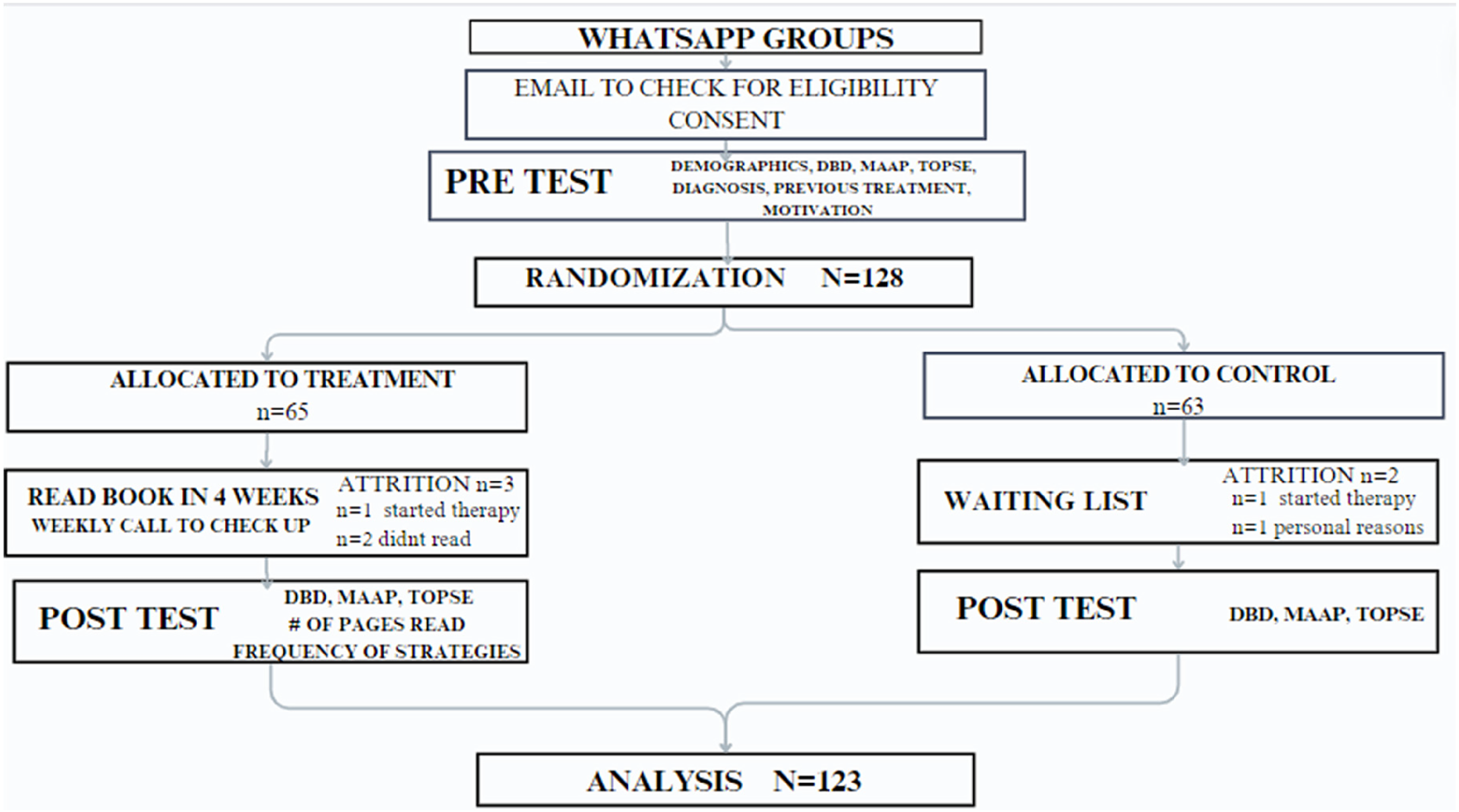
CONSORT diagram.
Lebowitz et al. (2014) offer another approach. Rather than forcing children to enter therapy, these researchers recommend providing therapeutic tools to parents, who can then apply them with their children in their home environment. Each parent becomes a therapy agent who has the potential to produce changes in the life of the child and the family. This form of intervention has been found to effectively reduce anxiety symptoms and behavioral issues among children in the K-12 age group and to provide parents with a sense of empowerment (Lebowitz et al., 2014). Therefore, parent-directed interventions may provide adequate therapeutic intervention without bringing the adolescent into the therapy room.
The act of transforming parents into therapy agents and providing them with a structured model of action that includes tools and strategies for behavioral management is a new and underexamined approach for parents of adolescents. Employing a randomized controlled design, the present study tested the efficacy of a self-help book for parents in terms of reduced parent-reported adolescent child's behavioral symptoms and their own increased sense of competency in responding to child's behavioral symptoms compared to those parents in a control group.
Background and Significance
In most of the literature on therapy for adolescents, the starting point is that therapy must be voluntary (Olson et al., 2008). Indeed, a fundamental condition for the success of therapy with adolescents is initial motivation. Adolescents are very sensitive to attempts at manipulation, such as small lies and temptation through rewards. Therefore, attempts to elicit their participation in therapy must be direct, honest, and devoid of issues other than the best interests of the adolescent. When the adolescent has no initial motivation, therapists are stymied and the only option they have is to persuade the adolescent to engage in therapy (Choate, 2007).
Traditional psychotherapeutic approaches with young people frequently do not work for a large portion of this population (Keen, 2005). Some alternatives to overcome the motivation barriers to treatment include using backpacking as a therapeutic process for troubled adolescent women participating in wilderness therapy (Caulkins et al., 2006), using music as a therapy tool (Keen, 2005), art therapy (Huang et al., 2021), and family therapy (Fishman, 2017; Maya et al., 2020). Yet, challenges in promoting constructive interactions with adolescents that will serve as a motivator for change are still notable.
Parent Training
Studies suggest that coercive parent–child interactions, inconsistent discipline, and poor parental monitoring place youth at risk for the development of antisocial behavior symptoms (Compton et al., 2003; Paterson et al., 2016). Nevertheless, it has long been established that the relationship between child behavior symptoms and parenting is bidirectional (Belsky et al., 2000; Sameroff & Mackenzie, 2003). In this respect, parent and child behaviors might reinforce each other in a loop; e.g., dysfunctional parenting behaviors produce child behavior symptoms, which in turn results in more dysfunctional parenting (Serbin et al., 2015).
Given this parent/child feedback loop and the acknowledgment that parents, not just highly trained therapists, can act as change agents of child's behavior (Bandura, 1974; Khanna et al., 2017). Consequently, parenting programs have proliferated, which emphasize a diversity of content and skills such as interaction, communication, and limit setting (Kaminski et al., 2008). Parent training involves teaching parents how to address and intervene with their child's behaviors, with programs sharing common targets such as improving the quality of parent-child interactions, increasing reliance on positive reinforcement, and using effective alternatives to physical discipline (McCart et al., 2006; Weisenmuller & Hilton, 2021). Research on these diversity of parent training programs and methods for intervening with their child's behavioral problems has found positive outcomes for both parents’ and children's behaviors across a variety of populations and problems (Long et al., 2017).
Self-Guided Parent Training
Contextual and systemic factors have been identified that frame and constrain access to parental training programs (Weisenmuller & Hilton, 2021). Barriers include cost of services/insufficient insurance coverage, time or location of services, lack of trained practitioners, and concerns regarding stigma (Baumel & Faber, 2018). One way to overcome these barriers is through self-help parenting programs, which exist along a continuum from entirely self-administered to those that include brief therapist assistance, usually via the telephone. Such programming is defined as any therapeutic intervention designed to be implemented by the parent(s), presented either in written (bibliotherapy) or multimedia format (O'Brien & Daley, 2011).
A systematic review of bibliotherapy, which refers to written materials in the form of an instruction manual and multimedia self-help parent programs, concluded that there is good evidence supporting the efficacy in improving child behaviors with resulting outcomes comparable to those achieved with more intensive therapist input. Furthermore, the review found that including minimum levels of therapist support in addition to self-help materials enhanced child and parent outcomes (Montgomery & Maunders, 2015). Sanders et al. (2014) report on a randomized trial design that compared the efficacy of two self-help variants of the Triple P-Positive Parenting Program: an online version and a self-help workbook. The results found that both interventions were associated with significant and clinically meaningful declines from pre- to post-intervention in levels of disruptive child behavior, dysfunctional parenting styles, risk of child maltreatment, and interparental conflict in both mother and father report measures. Intervention effects were maintained at 6-month follow-up. Khanna et al. (2017) conducted a random trial in which participants were assigned to (a) parent training provided through Child Anxiety Tales (CAT), (b) parent training provided via bibliotherapy (BIB), or (c) a waitlist control (WLC). The results demonstrated that parents’ knowledge about how to manage a youth with anxiety improved significantly after BIB and CAT, and both parent-training approaches were considerably better in outcomes than WLC. The investigators further determined that these gains were maintained at 3-month follow-up.
Study Hypotheses
While significant advances have been made in the identification and treatment of children and adolescents’ mental and behavioral health, the supply of mental health professionals trained to provide evidence-based treatments along with other barriers to these treatments as previously noted persist. Consequently, there is a need to expand the evidence base of alternative treatment formats. To fill this gap, the following study of a self-help book designed to help parents respond to their child's problem behaviors was conducted to examine the following hypotheses:
H1: Parents who read the self-help book will experience a greater reduction in reported child's behavioral symptoms than those in the control group. H2: Parents who report applying strategies from the self-help book will experience a greater reduction in their children's behavioral symptoms than those who only read the book without applying strategies. H3: Parents who read the self-help book will experience a greater increase in parental sense of competency than those in the control group. H4: Parents who read the self-help book will experience a greater increase in parental self-efficacy than those in the control group. H5: Parents who report applying strategies from the self-help book will experience a greater increase in parental sense of competency than those who only read the book without applying strategies. H6: Parents who report applying strategies from the self-help book will experience a greater increase in parental self-efficacy than those who only read the book without applying strategies.
Methods
The present study used an experimental design to examine the efficacy of a parental intervention on parents’ perceived sense of competency in responding to their child's problem behaviors and the degree of their reported child's behavioral symptoms. Self-help intervention is defined for purposes of the current study as using similar parameters as bibliotherapy, with parents reading the material on their own. All participants were provided with contact information should they experience harm or discomfort. No reports were made. Approval for the study was provided by Ono Academic College Institutional Review Board in Israel. The study protocol was not preregistered in a clinical trials registry.
Sample Criteria
Parents in Israel who reported struggling with parenting their adolescent children were recruited for the study. To be eligible parents had to meet the following inclusion criteria. They needed to have an adolescent child(ren) between the ages of 10 and 17 with at least one behavioral symptom that concerned them and for whom they reported difficulty parenting. All participants were required to have Internet access and be proficient in Hebrew. Participants voluntarily consented to participate in the study and confirmed that they were not currently seeking individual or group support or intervention for parenting skills. Participants also ensured that their child was not currently undergoing therapy and self-reported that they had not already read the book used for the intervention. Finally, participants were required to be willing to finish reading the book within 4 weeks.
Power Analysis
The calculations were based on the recommended power of 0.80, an alpha of 0.05, and a medium effect size of 0.30, determined from two previous studies (Lebowitz et al., 2014; Omer et al., 2013) with two conditions. Using Cohen's (1992) power table, n = 60 per group for a total N = 120 participants was identified as the necessary sample size. To protect from loss of power due to attrition, an additional 10 participants were planned per group, resulting in N = 140.
Recruitment
To acquire a sample of participants, recruitment procedures relied on the use of snowball procedures, with the researcher initially reaching out to parent groups on the platform WhatsApp. Thirty-four adolescent parenting groups were identified. The groups’ permission was sought from their administrators to post recruitment materials on their relevant WhatsApp group. Of these groups, 28 provided permission to use their WhatsApp group as a venue for study recruitment, leading to a pool of 28,000 potential participants.
Upon receiving permission for recruitment from administrators, the researcher posted a brief description of the study and what participation entailed and inclusion criteria for the study. The post also indicated that study participation was voluntary and provided the phone and email contact information for the researcher. Parents were asked to use the researcher's contact information provided in the post to furnish their email address if they were interested in participating in the study. Members of the WhatsApp group members were asked to share the recruitment post with other parents who may be interested in participating in the study. The researcher collected email addresses from those who responded. Recruitment continued until N = 128 eligible participants had been assigned to either a control or treatment group.
Randomization
After generating study ID numbers that would be used, the researcher divided ID numbers into blocks of 10. The researcher then used the “Random Between” function in Excel to randomly select a value of either 1, representing the treatment group, or 2, the control group for each block of 10 ID numbers. This process enabled the researcher to ensure a relative level of balance between groups as participants entered the study on a rolling basis. The researcher then assigned ID numbers to participants in the order in which informed consent forms were obtained.
Data Collection Procedures
Upon receiving an interested parent's email address, the researcher sent an email listing study inclusion criteria and providing the consent form. The consent form included a brief description of the study, as well as a discussion of the potential risks and steps to be taken to reduce risks as well as procedures for protection of confidentiality. The potential participants were asked to review the information, and if they felt they met the inclusion criteria to sign the consent form and email it to the researcher.
Upon receiving completed informed consent forms, a member of the research team scheduled a time to complete the pretest survey over the phone. Phone surveys were employed due to the lack of suitability of Qualtrics for use in the Hebrew language and variability in particpant access to reliable internet access. Participants were called the day after they completed the pretest survey, which lasted 30–45 min, to inform them as to the group they were assigned.
Each participant completed pretests, posttests, and intervention activities (treatment group) in their location of choice, typically their homes or workplaces, ensuring their comfort and privacy. Participants were located across Israel with data collection taking place between January and April 2024. Two assistants aided the researcher in conducting the initial pretest surveys with an additional assistant for the posttest 4 weeks later. Participants received no incentives to participate.
Control Condition
Members of the control group received no materials during the intervention period, but they were informed that the research team would be in contact with them to schedule a posttest survey in 4 weeks. They were offered a copy of the book once they completed the posttest.
Experimental Intervention
Individuals assigned to the treatment group were asked whether they preferred receiving a digital or physical copy of book, Where has my Cute Kid Gone? A Survival Guide for Parents of Adolescents (Leeman, 2021), written by the first author. As this information was conveyed to the researcher (first author), each treatment group participant was provided with a copy of the experimental treatment text. Once receipt of the book was confirmed, the 4-week clock for a participant's experimental intervention began. Throughout each participant's 4-week intervention period, a member of the research team called to inquire as to how far they were in the book. At the end of each participants’ 4-week intervention period, they were contacted by a member of the research team to schedule a posttest phone survey.
The self-help book used as the intervention contains 253 pages and is divided into five main sections. The first section explains how to use the book and how the book is constructed. The second describes the adolescence stage of development and the struggles parents face during these years. The third discusses the importance of setting parenting goals and offers communication strategies for parents and ways to solve tensions between the parent and adolescent. Included in this section are 10 tools for assistance with parenting adolescents. The fourth part discusses several issues and struggles common to adolescents and a model to help parents deal with them: struggles at school, loss of parental authority, substance abuse, social struggles, and sexuality issues. The book is built in a way that encourages parents to apply the content to their daily parenting routines and offers case studies and includes diagrams, symbols for each strategy, and illustrations.
The book is designed to be user-friendly in several ways. First, the book sections are color coded, and each page number has a corresponding color, making it easy for parents to refer to specific sections. Second, every strategy is represented by an icon, which helps parents learn new terms and familiarize themselves with the content. Third, examples from the author's clinical experience, disguised to maintain confidentiality, are provided. Fourth, all terms use catchy Hebrew names. Lastly, in Chapters 8–11, a list of strategies is provided at the bottom of each page with an index indicating where each strategy can be found in the book.
Section 1: Introduction
Chapter 1 provides a reassuring message to parents, assuring them that the adolescent stage will end. Chapter 2 provides a personal introduction where the author shares his story of adolescence and how he eventually became a therapist and developed the therapy method offered in the book. Chapter 3 provides an explanation of how to use the book. Chapter 4 discusses the benefits and reasoning behind parent-guided therapy versus individual therapy.
Section 2: The Parent Conception of Parenting Adolescents
Chapter 5 presents different styles of parenting and describes the pros and cons of each style and helps parents identify which style of parenting they are using and if its effective. Chapter 6 provides seven fundamental principles for parenting adolescents. Each concept is divided into an explanation, bullet points of what's in it for me (the parent), and what's in it for their child. Additionally, there are questions to help parents assess whether they have successfully applied each concept in their parenting. The seven concepts are called “the parents guiding stars” and have acronyms in Hebrew to help parents remember the basic concepts.
Section 3: Applying Parent-Guided Strategies
Chapter 7 emphasizes that setting parenting goals is crucial. It serves as a reminder for parents to act accordingly and helps them gauge the effectiveness of their actions in achieving their objectives. There is a clear distinction made between short-term and long-term goals. The chapter ends with an activity designed to assist parents in setting their own parenting objectives. Chapter 8 highlights ineffective communication methods commonly used by parents and provides alternative solutions based on the communication concepts explained in the chapter. Chapter 9 shows the parent's toolbox for parenting adolescents including concrete descriptions of strategies such as walk your talk (being a positive role model is the most important tool parents have); sharing is caring (parents often feel the need to shield their children from the harsh realities of life but failing to expose children to reality may not effectively prepare them for the real world); reality check (this tool suggests that parents should approach their child's experiences as if they were happening in the real world); and setting boundaries (this tool assists parents in identifying the boundaries they wish to establish and offers guidance on how to respond appropriately if a boundary is breached).
Section 4: Interventions for Times of SOS
Chapter 10 is designed to give parents a reliable model to follow during times of crisis. The model provides clear stages and directions to assist parents in navigating through difficult situations. It is important to have a plan in place to ensure the safety and well-being of everyone involved. By following this model, parents can feel confident that they are taking the necessary steps to handle the crisis effectively. Remember to stay calm, communicate clearly, and prioritize the safety of your family above all else. Chapter 11 discusses the application of the model to five common areas of crisis experienced during adolescence. These include crises at home, school, and socially as well as issues related to substance abuse, sex, and sexuality. The chapter provides valuable tips that are tailored to these specific crises, along with guidance on how to adapt the tools presented in the previous chapter to address these challenges effectively.
Section 5: Takeaways
Chapter 12 provides 33 practical tips for parents to enhance their bond with their adolescent. These tips cover a range of activities and conversation topics to improve their relationship. Chapter 13 provides six significant statements that parents should communicate to their adolescents. These include “I love you,” “no,” “sorry, I made a mistake,” “I forgive you,” “I'm proud of you and believe in you,” and “just listen.” Each sentence is accompanied by an explanation as to why they are crucial. Chapter 14 explores the statements that teenagers make which parents dislike hearing and what these statements might actually signify. Chapter 15 assists parents in preparing for the next developmental stage of young adulthood. It acknowledges the end of adolescence and encourages the continued use of strategies offered in the book for the future.
Measures
The study employed three scales to measure the depenendent variables. Group assignment (treatment or control) was used as a measure of intervention condition, and the number of times each of the 16 strategies was used (0–40) as a measure of treatment application.
Self-Efficacy: Me as a Parent Scale(MaaPS)
The 16 item MaaPS includes questions such as follows: I have confidence in myself as a parent, I know I am doing a good job as a parent; and I have all the skills necessary to be a good parent to my child. Questions are answered on a 5-point Likert scale ranging from strongly disagree to strongly agree. The scale has adequate internal consistency (0.62–0.84), satisfactory convergent validity, reasonable test–retest reliability, and Cronbach’s alphas 0.84 (Črnčec et al., 2010). The Cronbach alpha for this sample was excellent (0.92).
Tool to Measure Parenting Self-Efficacy
The tool to measure parenting self-efficacy (TOPSE) consists of eight subscales of six items each. Six TOPSE subscales were identified as relevant to the study: empathy, control, discipline, self-acceptance, learning, and emotion. Participants responded to statements by selecting from a Likert scale of 0–10, where 0 means completely disagree and 10 means completely agree. Examples of items include “Setting limits and boundaries is easy for me” and “I can find ways to avoid conflict.” Internal consistency reliability for the TOPSE total score was identified as α = 0.89 while the Cronbach alphas of six subscales used for the study ranged from 0.81 to 0.91 (Kendall & Bloomfield, 2005). The Cronbach alpha for this sample ranged between 0.88 and 0.97.
DBD Rating Scale
Disruptive Behavior Disorder (DBD) rating scale is a 45-item assessment tool completed by parents or teachers, who rate the extent to which each item reflects the child's behavior using a 4-point scale ranging from “not at all” to “very much” or “don’t know” (Pelham et al., 1992). Examples of items include the following: “Exhibits inattention to details, resulting in careless errors in academic tasks”; “Frequently exhibits loss of temper”; and “Exhibits cruelty towards animals.” The scale demonstrates good internal consistency, with Cronbach's alpha coefficients ranging from 0.80 to 0.95, and strong construct, concurrent, and discriminant validity across different demographic groups, including various age ranges, genders, and ethnic backgrounds (Pelham et al., 1992). The Cronbach alpha for this sample was 0.95, which is considered excellent.
Strategies Measure
Participants in the treatment group were asked: Since reading the self-help parental guidance book as part of this study, how many times have you used each of the strategies? (in Hebrew, there was a synopsis of each strategy) rated on a scale from 0 to 40 times. Strategies were as follows: authentic and emotional communication, using first-person grammar, validation, stopping ping-pong conversations, exiting the boxing arena, shooting from the hip, walking your talk, sharing is caring, reality checking, setting boundaries, disarming parent's triggers/soft spots, consequences-payment timing, overprotecting, separating zones, all aboard, and motivating.
Descriptive Variables
Age, gender, number of children in the parents’ household, marital status of parents, employment status, residence location, religion, monthly income, gender of child, and age of child were collected. Child mental health diagnosis and prior mental health treatment, prior parental support training for child's behaviors, and prior participation in therapy were obtained.
Analyses
Participants who began therapy during the intervention period or failed to complete the posttest were removed from the dataset (n = 5). All other observations were included in analysis. Given the small attrition rate (4%) equally distributed between groups (n = 3 in treatment, n = 2 in control) leaving a sample size large enough to detect an effect, missing data were addressed through pairwise deletion rather than using an intent-to-treat approach (refer to Figure 1). Initial equivalency of groups was examined. Descriptive statistics for all study variables were generated. Means, standard deviations, minimums, and maximums were calculated for continuous variables and frequencies were calculated for all categorical variables. Hypotheses were tested with a series of models using multiple regression analyses.
Equivalency Between Groups at Pretest
Equivalence between treatment and control groups was conducted using independent t-tests for continuous variables and χ2 tests of independence for categorical variables. The two groups were significantly different on child's age and each of the dependent variables at pretest. Children in the treatment group were older than children in the control group, and the treatment group had higher behavioral symptom scores and lower parent self-confidency scores on the MaaPS and TOPSE subscales (see Table 1). To account for these differences, child's age and each pretest score were included as control variables in hypothesis testing. No categorical variables were significantly different between the two groups at pretest including parent or child gender, child mental health, or prior parent or child treatment.
Equivalency Between Treatment and Control Groups at Pretest.
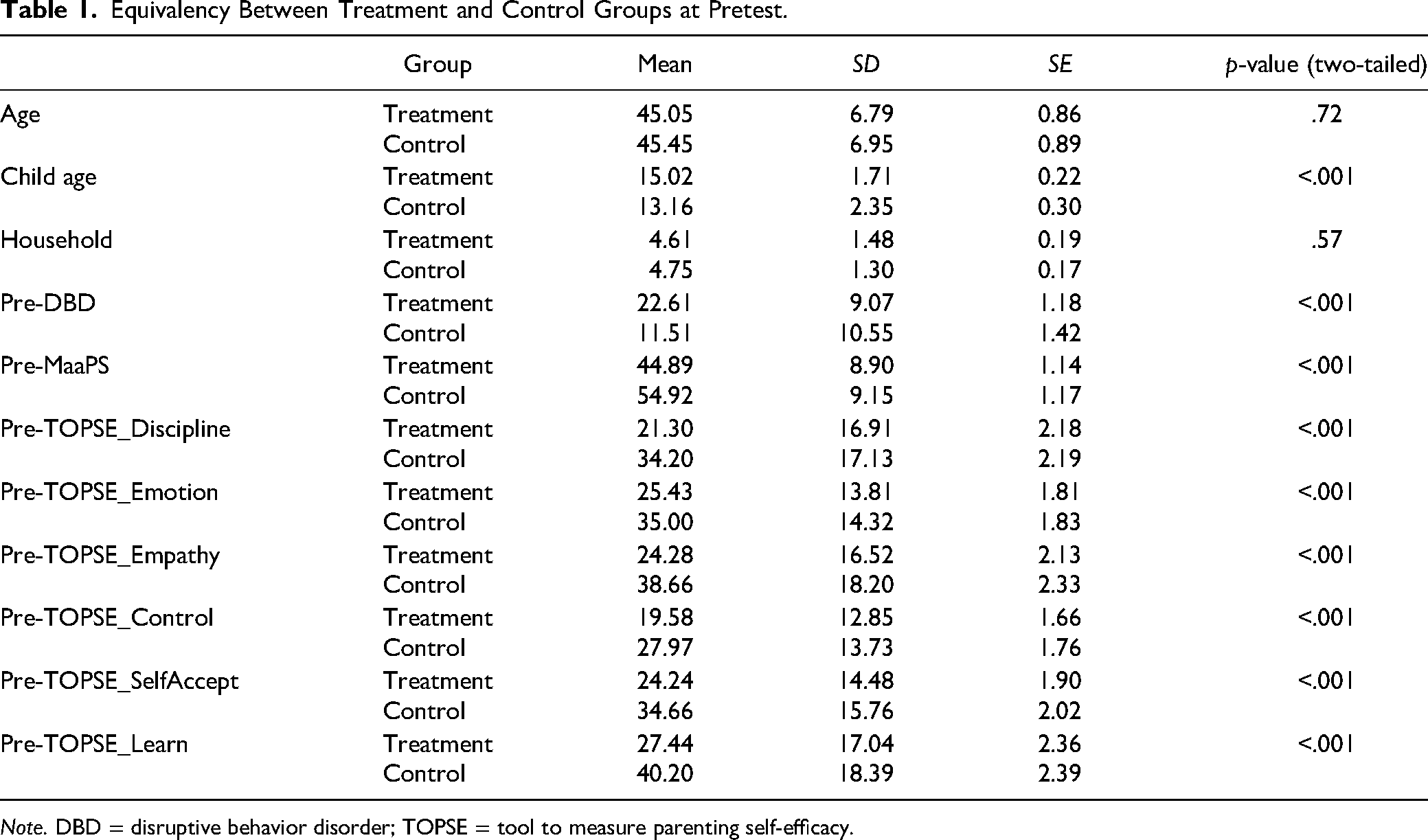
Note. DBD = disruptive behavior disorder; TOPSE = tool to measure parenting self-efficacy.
Data Preparation for Hypothesis Testing
Prior to hypothesis testing, 10 new variables were created including eight change scores for each DV. Two application variables were also created: (a) number of strategies, calculated by creating binary variables for each of the 16 strategies (0 = no application or 1 = application 1 + times) and summing them, and (b) frequency of application, calculated by summing the number of times parents reported applying each strategy across the 16 strategies.
Assumptions of normality for continuous variables were tested using skew and kurtosis statistics. DBD change in the control group was found to be skewed with high kurtosis due to an outlier, which was Winsorized. This brought skew and kurtosis to acceptable levels. TOPSE empathy and self-acceptance change, which both had kurtosis statistics above the acceptable range in the control group due to values clustered at 0, were removed from analysis.
Hypothesis Testing
Hypothesis 1 was examined using multiple regression with DBD change as the DV, group assignment as the IV, and the pretest scores and age of child as control variables. Because there were no parents in the treatment group who applied no strategies, the IV planned for Hypothesis 2 was adjusted from a binary (strategies yes or no) to the number of times across strategies and the number of strategies used. The following multiple regression model was used to test Hypothesis 2: DBD change as the DV, number of times strategies used, number of strategies, and number of pages read as the IVs and the pretest scores and age of child as control variables.
Hypothesis 3 was tested employing one multiple regression model with parental sense of competency as the DV (MaaPS change), group assignment as the IV, and the pretest scores and age of child as control variables.
Hypothesis 4 was tested using four multiple regression models, one for each of four measures of parental self-efficacy as the DV (TOPSE discipline change, TOPSE control change, TOPSE emotion change, and TOPSE learning change), group assignment as the IV, and the pretest scores and age of child as control variables. A Bonferroni correction was used to protect against Type 1 error given the multiple models testing different measures of the same construct (parent competency). The cutoff under which differences between groups were identified as significant was calculated as p < .05/4 (the number of models) = 0.01.
Because there were no parents in the treatment group who applied no strategies, the IV planned for Hypothesis 5 was adjusted from a binary (strategies yes or no) to the number of times across strategies and the number of different strategies used. The following multiple regression model was used to test Hypothesis 5: parental sense of competency change as the DV (MaaPS change), number of times strategies used, number of different strategies employed, and number of pages read as the IVs and the pretest scores and age of child as control variables.
Hypothesis 6 was tested using multiple regression models, each with a different parental self-efficacy variable as the DV (TOPSE discipline change, TOPSE control change, TOPSE emotion change, and TOPSE learning change), number of times strategies used, number of different strategies employed, and number of pages read as the IVs and the pretest scores and age of child as control variables. A Bonferroni correction was again used with the cutoff under which changes were identified as significant was calculated as p < .05/4 (the number of models) = 0.01.
Results
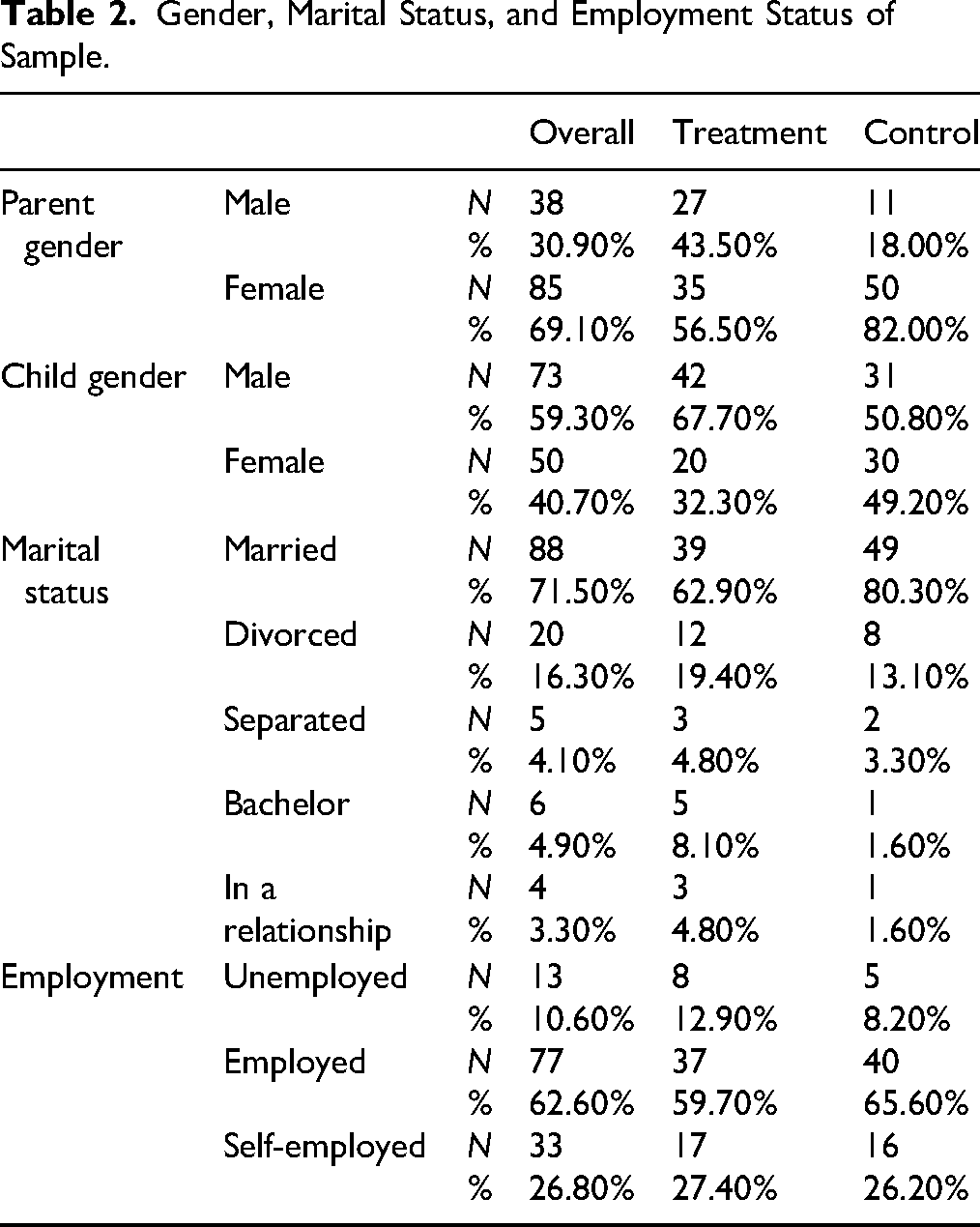
A total of N = 123: n = 61 in control and n = 62 in treatment group were included in analyses. Over two-thirds of the parents in the sample were female (69%), most were married (72%), and over half were employed (63%). The sample was equally split by child gender, with 51% male and 49% female. See Table 2 for details.
Gender, Marital Status, and Employment Status of Sample.
Parents ranged in age from 32 to 65 (M = 45 years, SD = 6.17) and children ranged in age from 8 to 18 (M = 14, SD = 2.25). Participants reported an average of five people (SD = 1) living in their household. See Table 1 for additional detail by group.
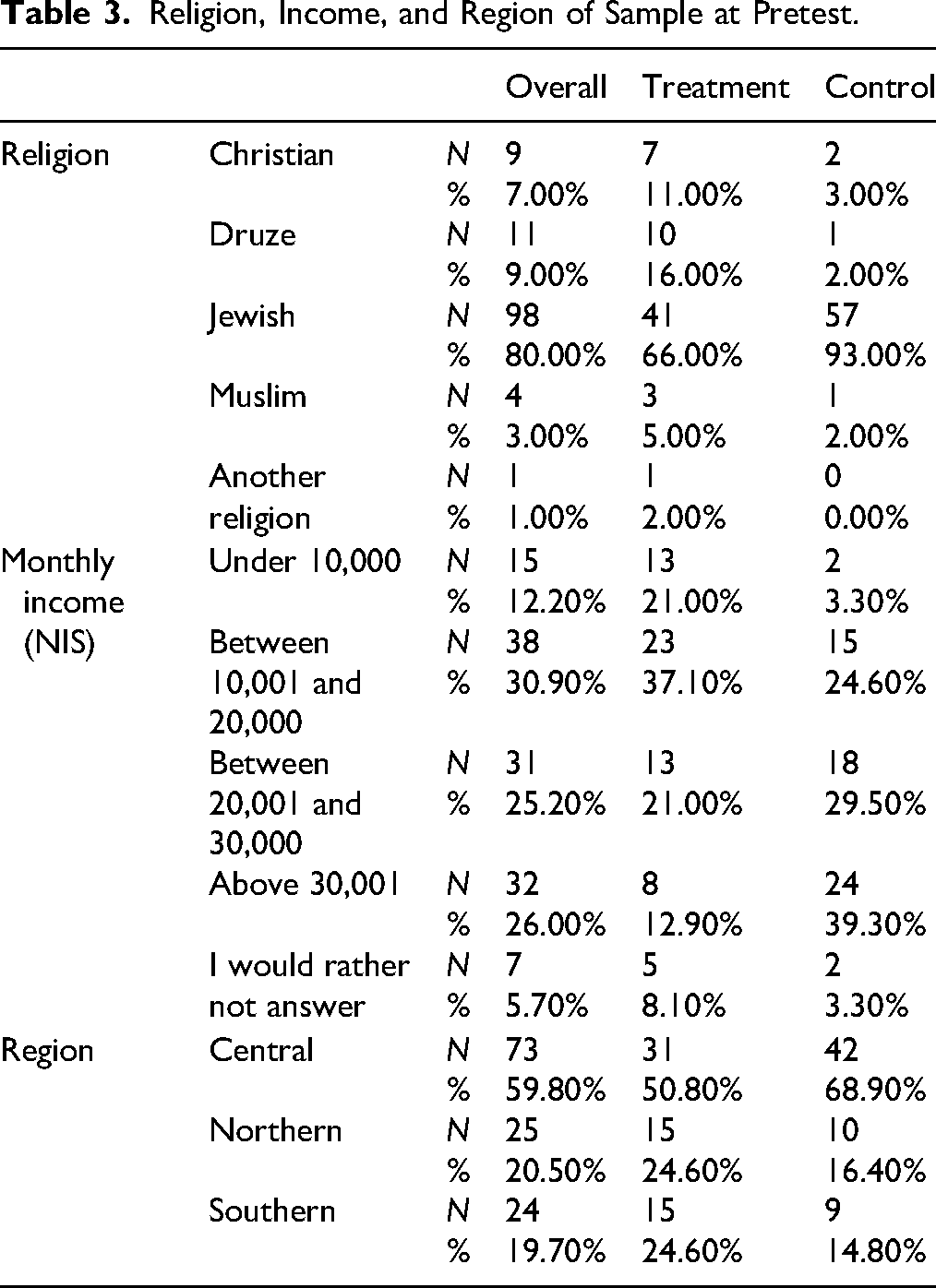
As shown in Table 3, 80% of participants identified as Jewish, 9% as Druze, 7% as Christian, and 1% another religion. Participants primarily resided in Central Israel (60%). with 20% each in Northern and Southern Israel. Given the evacuation due to the ongoing war, it is uncertain whether the reported locations reflect the participants’ current or permanent residence.
Religion, Income, and Region of Sample at Pretest.
The average number of pages read by the treatment group was 194 (SD = 50.07), ranging from 42 to 234. Parents, on average, utilized the strategies a total of 233 times across the 4-week period (SD = 154.90) ranging from 8 to 640 times, and utilized an average of 12 of the 16 strategies (SD = 3.71). The most commonly used strategies included setting boundaries (n = 59 participants, 95%), validation (n = 57, 92%), and consequences (n = 53, 87%). Every strategy was utilized at least once by over 50% of participants.
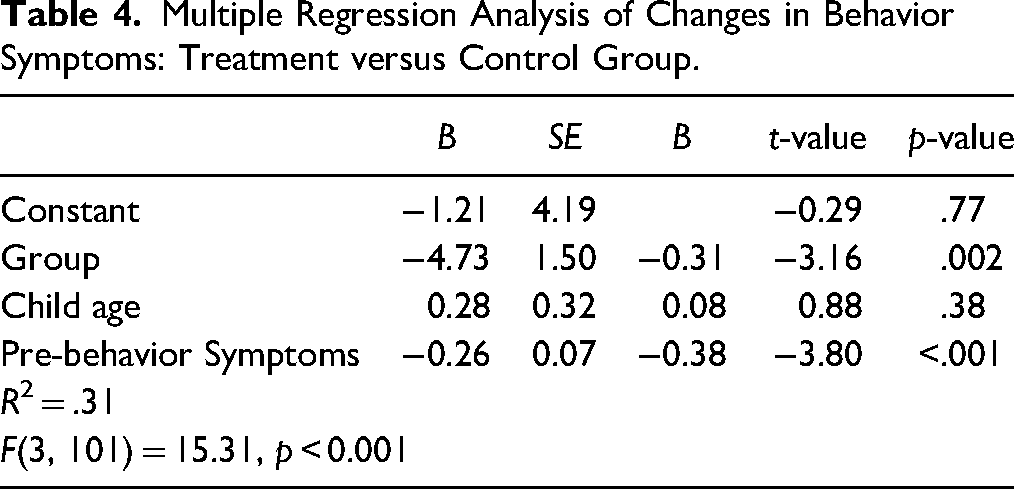
Hypothesis 1: Parents Who Read the Self-Help Book Will Experience a Greater Reduction in Reported Child's Behavioral Symptoms Than Those in the Control Group
Hypothesis 1 was examined using multiple regression analysis to test a model with change in behavioral symptoms included as the DV, group assignment as the IV, and the pretest scores and age of child included as control variables. As shown in Table 4, the combination of variables explained 31% of the variance in behavioral symptom change scores, R2 = .31, F(3, 101) = 15.31, p < .001, suggesting that 31% of the differences among children's change in behavioral symptoms could be predicted by the combination of variables. The treatment group had significantly greater reductions in behavioral symptoms between pretest and posttest compared to the control group when controlling for child's age and pretest scores (B = −4.73, p < .01). This indicates that, on average, the treatment group had ∼5-point greater reduction in behavior symptoms between pretest and posttest compared to the control group, which equates to a large (Cohen’s d = −3.15), clinically important and meaningful difference with practical implications. This supports the first hypothesis that the intervention would reduce behavioral symptoms in children whose parents were in the treatment group relative to those in the control group.
Multiple Regression Analysis of Changes in Behavior Symptoms: Treatment versus Control Group.
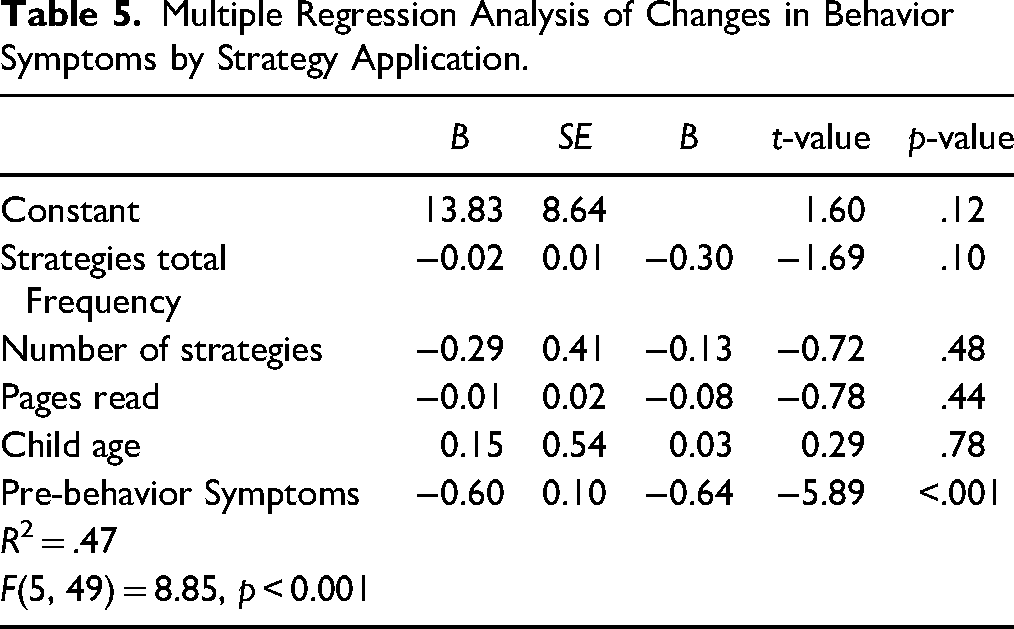
Hypothesis 2: Parents Who Report Applying Strategies from the Self-Help Book Will Experience a Greater Reduction in Their Children's Behavioral Symptoms Than Those Who Only Read the Book Without Applying Strategies
Hypothesis 2 was analyzed with treatment group data only, using multiple regression analysis to test a model with change in behavioral symptoms included as the DV, number of pages read as an IV, and the pretest scores and age of child included as control variables. Because there were no parents in the treatment group who applied n = 0 strategies, an IV planned for Hypotheses 2 was adjusted from one binary (strategies yes or no) to two continuous IVs: the number of times across strategies and the number of different strategies used.
As shown in Table 5, the combination of variables explained 47% of the variance in the change in behavioral symptoms, R2 = .47, F(5, 49) = 8.85, p < .001, suggesting that almost half of the differences among children in their behavior symptoms could be predicted by the combination of variables. Neither the total number of times the 16 strategies were used nor the total number of different strategies used predicted significant difference in behavioral symptoms between pretest and posttest, suggesting that the change in behavior symptoms was not greater among parents who used strategies more frequently than those who used them less frequently. It also suggests that the change in behavior symptoms was not greater among parents who used more of the 16 strategies than those who used fewer. This does not support the second hypothesis that increased application of strategies will be associated with greater reductions in behavioral symptoms.
Multiple Regression Analysis of Changes in Behavior Symptoms by Strategy Application.
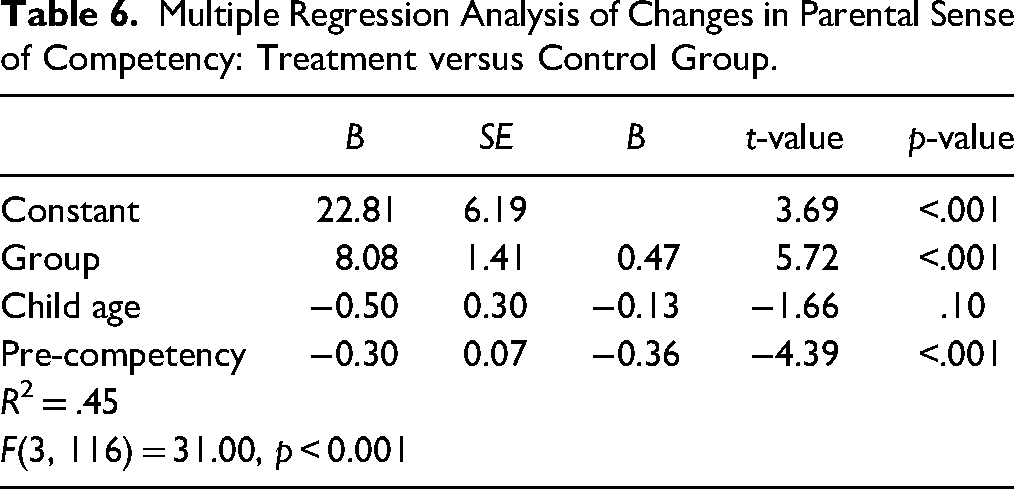
Hypothesis 3: Parents Who Read the Self-Help Book Will Experience a Greater Increase in Parental Sense of Competency Than Those in the Control Group
Hypothesis 3 was examined using multiple regression analysis to test a model with change in parental sense of competency (MaaPS) included as the DV, group assignment as the IV, and the pretest scores and age of child included as control variables. As shown in Table 6, the combination of variables explained 45% of the variance in changes in parent sense of competency, R2= .45, F(3, 116) = 31.00, p < .001, suggesting that 45% of the differences among parent's change in confidence could be predicted by the combination of variables. The treatment group had significantly greater increases in parent competency between pretest and posttest compared to the control group as assessed by the MaaPS when controlling for child's age and pretest scores (B = 8.08, p < .01). This indicates that, on average, the treatment group had an 8-point greater increase in parental competency between pretest and posttest compared to the control group, which equates to a large (Cohen’s d = 5.70), clinically important and meaningful difference with practical implications. This supports the third hypothesis that the intervention would increase parental confidence in parents who were in the treatment group relative to those in the control group.
Multiple Regression Analysis of Changes in Parental Sense of Competency: Treatment versus Control Group.
Hypothesis 4: Parents Who Read the Self-Help Book Will Experience a Greater Increase in Parental Self-Efficacy Than Those in the Control Group
Hypothesis 4 was analyzed using four multiple regression models, each with a different parent self-efficacy variable included as the DV (TOPSE discipline change, TOPSE emotion change, TOPSE control change and TOPSE learning change), group assignment as the IV, and the pretest scores and age of child included as control variables. As shown in Table 7, the combination of variables in Model 1 explained 41% of the variance in changes in parental self-efficacy, R2= .41, F(3, 116) = 27.24, p < .001, suggesting that 41% of the differences among parents’ change in self-efficacy regarding disciplining their child could be predicted by the combination of variables. The treatment group had significantly greater increases in self-efficacy regarding disciplining their child between pretest and posttest compared to the control group when controlling for child's age and pretest scores (B = 10.68, p < .01). This indicates that, on average, the treatment group had ∼11-point greater increases in parental self-efficacy between pretest and posttest compared to the control group, which equates to a large (Cohen’s d = 5.42), clinically important and meaningful difference with practical implications. This supports the fourth hypothesis that the intervention would increase parental self-efficacy in parents in the treatment group relative to those in the control group when parental self-efficacy is defined as the ability to discipline their child.
Multiple Regression Analysis of Changes in Parental Self-Efficacy: Treatment versus Control Group.
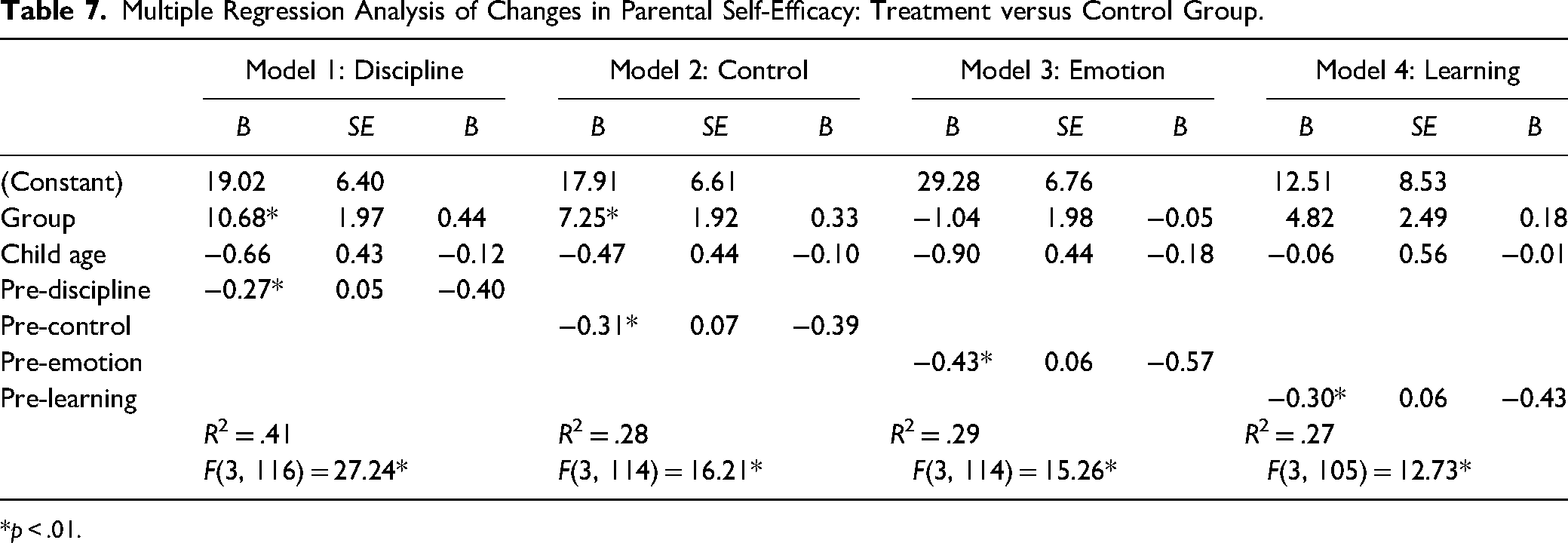
*p < .01.
The combination of variables in Model 2 explained 28% of the variance in changes in parental self-efficacy, R2 = .28, F(3, 114) = 16.21, p < .001, suggesting that 28% of the differences among parents’ change in self-efficacy regarding controlling their child's behavior could be predicted by the combination of variables. The treatment group had significantly greater increases in parents’ change in self-efficacy regarding controlling their child's behavior between pretest and posttest compared to the control group when controlling for child's age and pretest scores (B = 7.25, p < .01). This indicates that, on average, the treatment group had 7-point greater increases in parental self-efficacy between pretest and posttest compared to the control group, which equates to a large (Cohen’s d = 3.77), clinically important and meaningful difference with practical implications. This supports the fourth hypothesis that the intervention would increase parental self-efficacy in parents in the treatment group relative to those in the control group when parental self-efficacy is defined as the ability to control their child.
The combination of variables in Model 3 explained 29% of the variance in changes in parental self-efficacy, R2 = .29, F(3, 114) = 15.26, p < .001, suggesting that 29% of the differences among parents’ change in self-efficacy regarding emotional connection with their child could be predicted by the combination of variables. There was no significant difference between treatment and control groups in changes in parental emotional self-efficacy between pretest and posttest. This does not support the fourth hypothesis that the intervention would increase parental self-efficacy in parents in the treatment group relative to those in the control group when parental self-efficacy is defined as having an emotional connection to their child.
The combination of variables in Model 4 explained 27% of the variance in changes in parental self-efficacy, R2 = .27, F(3, 105) = 12.73, p < .00, suggesting that 27% of the differences among parents’ change in self-efficacy regarding learning to adjust to their child's changing needs could be predicted by the combination of variables. There was no significant difference between treatment and control groups in changes in parental self-efficacy regarding learning to adjust to their child between pretest and posttest. This does not support the fourth hypothesis that the intervention would increase parental self-efficacy in parents in the treatment group relative to those in the control group when parental self-efficacy is defined as learning to adjust to their child's changing needs.
Hypothesis 5: Parents Who Report Applying Strategies from the Self-Help Book Will Experience a Greater Increase in Parental Sense of Competency Than Those Who Only Read the Book Without Applying Strategies
Hypothesis 5 was analyzed with treatment group data only, using multiple regression analysis to test a model with change in parental sense of competency included as the DV, number of pages read as an IV, and the pretest scores and age of child included as control variables. Because there were no parents in the treatment group who applied n = 0 strategies, an IV planned for Hypotheses 5 was adjusted from one binary (strategies yes or no) to two continuous IVs: the number of times across strategies and the number of strategies used.
As shown in Table 8, the combination of variables in Model 1 explained 63% of the variance in changes in parental sense of competency, R2 = .63, F(5, 53) = 20.91, p < .001, suggesting that 63% of the differences among parents’ change in competency could be predicted by the combination of variables. The number of times the strategies were used between pretest and posttest predicted significant increases in parent sense competency when controlling for number of pages read, child's age, and pretest scores (B = 0.02, p < .01). This indicates that with every additional use of a strategy, parental competency between pretest and posttest increased by 0.02 of a point, which equates to a medium effect (β = 0.43; Cohen, 1992) with some practical and clinical implications. This supports the fifth hypothesis that increased application of strategies will be associated with greater increases in parent sense of competency.
Multiple Regression Analysis of Changes in Parental Sense Competency by Strategy Application.
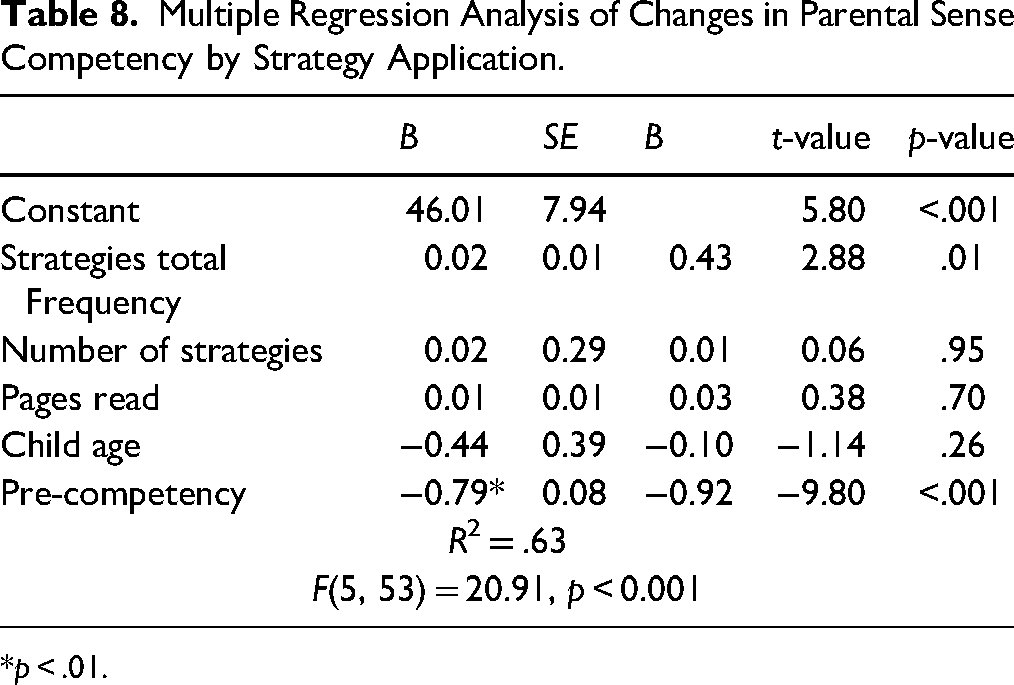
*p < .01.
Hypothesis 6: Parents Who Report Applying Strategies from the Self-Help Book Will Experience a Greater Increase in Parental Self-Efficacy Than Those Who Only Read the Book Without Applying Strategies
Hypothesis 6 was examined with treatment group data only, using two multiple regression models to test changes in parental self-efficacy, one each with discipline and control as the DV, number of pages read as an IV, and the pretest scores and age of child included as control variables. Because there were no parents in the treatment group who applied n = 0 strategies, an IV planned for Hypotheses 6 was adjusted from one binary (strategies yes or no) to two continuous IVs: the number of times across strategies and the number of different strategies used. Only those measures of self-efficacy that were found to be significantly different between the treatment and control group (discipline and control) were used to test this hypothesis.
As shown in Table 9, the combination of variables in Model 1 explained 62% of the variance in changes in parent self-efficacy, R2 = .62, F(5, 53) = 17.74, p < .001, suggesting that 62% of the differences among parents’ change in self-efficacy in disciplining their child could be predicted by the combination of variables. The number of times the strategies were used between pretest and posttest predicted significant increases in parental self-efficacy in disciplining when controlling for number of pages read, child's age, and pretest scores (B = 0.04, p < .01). This indicates that with every additional use of the strategies, parental self-efficacy regarding discipline between pretest and posttest increased by 0.04 of a point, which equates to a large (β = 0.53), clinically important and meaningful difference with practical implications. This supports the sixth hypothesis that increased application of strategies will be associated with greater increases in parental self-efficacy when it is defined as the ability to disciple their child.
Multiple Regression Analysis of Changes in Parental Self-Efficacy by Strategy Application.
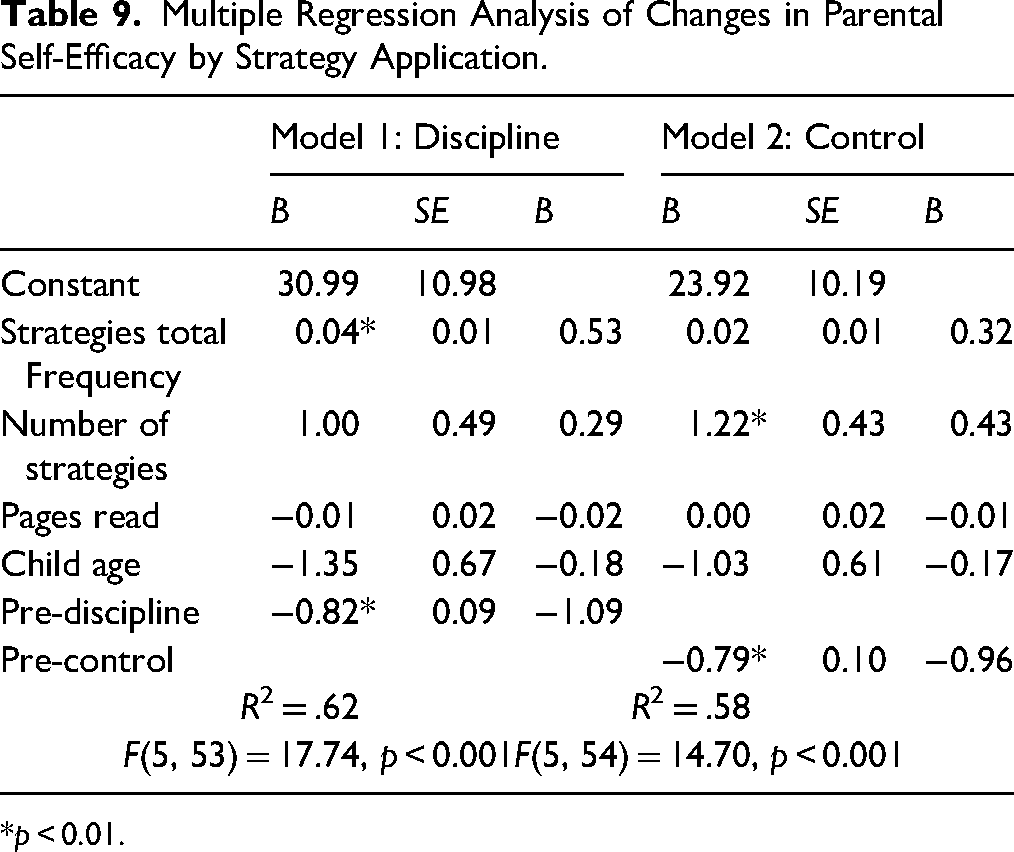
*p < 0.01.
The combination of variables in Model 2 explained 58% of the variance in parental self-efficacy change scores, R2 = .58, F(5, 54) = 14.70, p < .001, suggesting that 58% of the differences among parents’ change in self-efficacy in controlling their child's behavior could be predicted by the combination of variables. The number of strategies used between pretest and posttest predicted significant increases in parent self-efficacy to control their child's behavior as assessed when controlling for number of pages read, child's age, and pretest scores (B = 1.22, p < .01). This indicates that with every additional strategy used, parental competency between pretest and posttest increased by over 1 point, which equates to a medium effect (β = 0.43), with some practical and clinical implications. This supports the sixth hypothesis that increased application of strategies will be associated with greater increases in parental self-efficacy when it is defined as the ability to control their child's behavior.
Discussion
The purpose of this study was to assess the effectiveness of reading a self-help book aimed at elevating parents’ sense of competency and reducing parents’ assessed behavior problems of their adolescents. Overall, results suggest that both reading the book and implementing the strategies articulated in it had a positive effect on the behavior of adolescents as assessed by the parents and on parents’ own sense of competency.
The first hypothesis, that parents who read the self-help book would report a greater reduction in their child's problem behaviors than those in the control group, was supported. This is consistent with previous research, stating how parents respond to adolescents’ problem behaviors is crucial to enhancing or changing that behavior (Belsky et al., 2000; Sameroff & Mackenzie, 2003; Serbin et al., 2015). By implementing new strategies and changing how they interact with their children, parents can reduce their assessed problem behaviors. This is also consistent with previous research suggesting that parents can have a vital influence on their children's behavior without the active involvement of a trained therapist (Bandura, 1974; Khanna et al., 2017).
The second hypothesis, that parents who report applying strategies from the self-help book would experience a greater reduction in their child's assessed problem behaviors than those who only read the book without applying strategies, was adjusted by necessity to comparisons of the number and frequency of strategies applied, as none of the parents in the intervention group reported not applying any of the strategies offered in the book. This adjusted hypothesis was not supported, with neither the amount nor the frequency of different strategies implemented being associated with greater reduction of children's problem behaviors as reported by the parent. Friedson (2016) explores parents’ complex roles in managing their children's behavior symptoms, emphasizing that different strategies may be effective depending on the context and specific behavior issues. Taking this into account, it is likely that being adaptive in choosing single or sets of strategies, as well as implementing them at appropriate times, is the key to improving problematic behavior rather than using as many strategies as often as possible. This implies that the book was able to give not only strategies but also the understanding of how to implement them wisely. Additionally, the fact that all readers reported applying some of the strategies articulated in the book might suggest that it offers strategies that are both acceptable and feasible to its readers. In the analysis of the intervention's effectiveness, the positive outcomes observed in the treatment group occurred irrespective of the number or frequency of different strategies used by the parents. This might indicate that the intervention, as facilitated by the self-help parental guidance book, was effective across all levels of engagement, suggesting that it is not the number strategies that lead to reductions in child problem behaviors, but their appropriate application.
Hypothesis 3, that parents who read the self-help book would experience a greater increase in parental sense of competency than those on waitlist, was supported. Hypothesis 4, that parents who read the self-help book would experience a greater increase in parental self-efficacy than those on waitlist, was also supported. Specifically, results indicated a greater increase in general sense of competency and a sense of self-efficacy specifically related to control and discipline in the treatment group relative to the control group. It should be noted that these two specific types of self-efficacies reflect two of the top three most used strategies—setting boundaries (control) and consequences (disciplining). It is plausible that parents experienced more incidents of success in these specific areas and thus increased their sense of self-efficacy related to them. This enhanced sense of control and discipline is particularly relevant in the context of adolescent therapy refusal given that empowering parents effectively addresses this challenge by providing them with practical tools to manage behavior without direct therapeutic intervention.
Hypothesis 5, that parents who report applying strategies from the self-help book would experience a greater increase in a sense of parental competency than those who only read the book without applying strategies, and Hypothesis 6, that parents who report applying strategies from the self-help book would experience a greater increase in self-efficacy than those who only read the book without applying strategies, were also both adjusted to reflect that all parents used at least one strategy. Hypothesis 5 was supported, with results indicating a greater increase in a general sense of competency among those using strategies more frequently. Hypothesis 6 was also supported, with results indicating greater self-efficacy related to discipline for those using strategies more frequently, and having a greater sense of control for those employing more strategies. Gaining a sense of competence and self-efficacy is tied to experiencing success in completing tasks related to the area in question (Glatz et al., 2024). Thus, reading the book and implementing the strategies articulated in it may have provided parents with opportunities to experience success in their parenting tasks, and as a result, an increase in their general sense of competency. In fact, it is likely to assume that the greater the variety and frequency of employing strategies, the more opportunities emerged to experience a sense of competency.
Regarding the differential impact of control and the number of strategies applied by parents, variations in the effectiveness of different numbers and types of strategies can arise from a diversity of factors. Each child is unique, and their responses to parental strategies can vary significantly based on their temperament, previous experiences, and current circumstances. Some children may respond better to a limited set of consistent strategies, while others might need a broader array of approaches to address diverse behavioral challenges. Several studies and parenting programs advocate for a “toolbox” approach, which encourages parents to experiment with different strategies and techniques to find what works best for their unique family dynamics and their child's individual needs (Kazdin, 2017). This approach promotes the idea that parents can benefit from having a repertoire of strategies at their disposal, allowing them to tailor their responses based on the specific circumstances and their child's unique characteristics.
Implication for Social Work
The findings of this study have profound implications for social work practice, especially in how self-help resources can revolutionize support for parents dealing with adolescent behavior problems. As demonstrated, self-help books offer a cost-effective, accessible, and flexible method to enhance parental competency and empower parents to actively shape their children's developmental trajectories. These resources not only reduce costs but also allow parents to engage at their own pace and time, making them particularly valuable in settings where traditional therapeutic resources are limited or inaccessible. By leveraging such approaches, social workers can extend their reach to parents in remote or underserved areas, effectively overcoming barriers related to transportation, time constraints, costs, and stigma, thus facilitating easier access to necessary support for managing adolescent challenges.
Relevance of these results becomes even more pronounced when considering the widespread issue of adolescent resistance to therapy—a challenge often compounded by stigma, denial, or a simple reluctance to seek professional help (Kazdin & Blase, 2011). In such scenarios, empowering parents through self-help materials provides a vital alternative approach. Such books equip parents with practical strategies that are foundational cognitive–behavioral techniques adapted for home use. Study outcomes underscore that the application of these strategies by parents has the potential to lead to significant perceived improvements in adolescent behavior, confirming research that adapting effective parenting skills can achieve substantial positive outcomes without direct involvement of adolescents in therapy sessions (Forehand et al., 2013).
While serving as a primary support tool for parents, such books can also act as a catalyst for initial change, even in cases where professional intervention is ultimately necessary. These resources can lay the groundwork for constructive dialog within the family and can pave the way for adolescents to eventually engage with therapy, serving as a bridge between initial resistance and eventual acceptance of professional help. This gradual progression underscores the adaptive nature of self-help materials, which can provide immediate relief, while also facilitating a pathway to more intensive therapeutic interventions when needed.
Strengths and Limitations
The strengths of this study are highlighted by its significant sample size. A diverse sample of 128 parents from various regions of Israel participated, thus, increasing the generalizability and utility of the findings. Importantly, while the extent of engagement varied, with some parents applying the strategies more frequently than others, every participant engaged with the intervention to some degree, demonstrating the material's practicality and appeal.
The adaptation of data collection to telephone surveys due to the ongoing war and limited internet access turned out to be a significant strength of this study. A key factor in the success of this method was the human contact provided to participants through one-to-one telephone interactions with the research assistants. This personal touch likely played a crucial role in maintaining participant engagement and commitment to the study. Unlike digital surveys, where participants can easily abandon the survey midway without any personal interaction, telephone surveys involve a real-time connection with another person, which can encourage participants to complete the process. Moreover, the weekly check-ins with participants in the treatment group to monitor their reading progress could have further encouraged participants to read the book. These regular touchpoints helped ensure that participants remained actively involved in the study. These methodological strengths underscore the importance of flexibility and adaptability in research design, particularly in contexts marked by instability and limited resources. They also highlight the potential for telephone-based interventions to serve as a viable alternative in scenarios where traditional methods are impractical or unsafe, leveraging human interaction to foster higher completion rates. However, it is important to note that using telephone surveys is resource intensive, requiring significant time and cost of hiring research assistants.
Also, measures of child behaviors were self-administered and from the perspective of the parent. Therefore, they have the biases and limitations of these types of measures. Furthermore, while there were changes in participant perceptions of their child's behavior, which is certainly important, it is unknown to what extent these measures represent actual behavior change.
Study participants’ demographic composition may limit the findings’ generalizability to the broader Israeli population. The sample closely mirrored the general Jewish population of Israel, with 79.68% of participants identifying as Jewish. However, there were notable discrepancies in the representation of other religious and ethnic groups, such as Christians and Druze, which may be attributed, in part, to the fact that the book was in Hebrew. This language barrier limits the accessibility of the intervention for non-Hebrew-speaking populations. This limitation is particularly relevant in Israel, where the population is linguistically diverse, with many Arab and other non-Hebrew-speaking communities. As a result, the findings of the study may not fully capture the experiences and responses of these populations to the intervention. Future studies should consider translating intervention material into multiple languages to ensure its accessibility and relevance to a wider range of participants.
The study lacked a long-term follow-up period to assess any possible sustained effects of the self-help book. Long-term follow-up is esssential to determine if observed effects are short-lived or have lasting impacts on outcomes (Sanders et al., 2014). However, this research model could easily be adopted as a long-term study. The intervention equips parents with strategies and techniques that they can continue to use and implement over an extended period. Unlike interventions that require ongoing professional guidance or support, the self-help book empowers parents to independently apply the learned techniques in their day-to-day parenting practices as circumstances change and their child develops. This aspect of the intervention makes it feasible for researchers to track its effects longitudinally without the need for sustained direct involvement from professionals.
Future Research
To truly understand the long-term effects of self-help parental guidance books, longitudinal studies are essential. These studies should track changes in parental competency and child behavior over extended periods, beyond the initial post-intervention assessments. Such studies will help ascertain whether the improvements observed are transient or if they translate into long-term benefits for families.
It is also vital to position the self-help book within the broader spectrum of parental guidance interventions. Comparing its effectiveness against other approaches, such as group workshops or individual counseling, could identify the most beneficial delivery methods for different types of parents or issues. In addition, offering some professional support to parents as they read the book may also be important to assess. Such comparative studies could focus on various outcomes, including cost, ease of implementation, and the depth of impact on child and parental outcomes. Integrating the self-help book with other interventions could potentially amplify its benefits. For instance, combining the book's guidance with school-based programs or community services might provide a more holistic approach to addressing child behavior problems and enhancing parental competencies.
Future research should also consider incorporating assessments that include both children's self-reports and parents’ perceptions of behavioral symptoms. This approach would allow for a comparative analysis of how children perceive changes in their behavior versus how their behavior is observed and reported by their parents. Such studies could uncover discrepancies or confirmations between self-perceptions and external observations, offering deeper insights into the effectiveness of the self-help interventions from a dual perspective.
Conclusion
The findings of this study suggest that a self-help parental guidance book can be an effective tool for improving parental sense of competency and reducing parent-reported child behavior problems. These findings highlight the potential benefits of self-help resources in supporting families given that the book format removes common barriers such as location constraints, limited resources, and the scarcity of available professionals, which are particularly pressing issues in war-torn Israel where there is a notable shortage of therapists. Additionally, the use of a self-help book addresses the common resistance among adolescents to engage in traditional therapy, offering parents a viable and less confrontational alternative to support their children's needs. This approach not only broadens the reach of therapeutic guidance but also empowers parents by providing them with the tools necessary to effect change independently, making it an invaluable resource in the landscape of child and adolescent mental health support and development.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.