
Abstract
Keywords
Introduction
This systematic narrative review (Grant & Booth, 2009; Popay et al., 2006; Snilstveit et al., 2012) synthesizes evidence from original research studies and previous relevant reviews on allied topics about the outcomes from couple-based interventions for relational approaches to working with interpersonal violence (IPV) within established heterosexual adult couple relationships at secondary and tertiary prevention levels. This can be measured by the participants’ experiences and opinions, including issues of desistance and of safety for both participants, with particular attention being paid to issues regarding the seriousness of the IPV. This review used explicit methods for study identification and quality appraisal, followed by a narrative approach to synthesizing a range of types of research findings (Popay et al., 2006). The systematic narrative review approach was employed, as it allows for a broad approach/scope to what is being searched for, and this area of efficacy of couple-based treatments for IPV with a focus on safety is underresearched. One example of such a review in a related area of family violence is that of McKay and Bennett (2023).
This topic is important because of the extent, nature, and effects of IPV in such couple relationships, and the possibility of strengthening families and society through relationship-based approaches to this problem. Although this article focuses on established heterosexual couple relationships, IPV is neither uncommon nor confined to people from specific educational, ethnic, LGBTQ+, and religious or cultural groups regardless of employment status or disability (Muster, 2021; National Institute for Health and Care Excellence, 2014, 2018; Spratt et al., 2022; Tsantefski et al., 2018). This review focuses on heterosexual relationships, as the evidence of high frequency and impact on each of the partners in such relationships may be different from the dynamics involved in, for example, LGBTQ + relationships, with same-sex IPV being sufficiently different to warrant a separate review, being a specialist subpopulation that merits separate analysis.
A World Health Organization (2022) examination of IPV globally estimated that 26% of women around the world have been physically and/or sexually assaulted at least once by a male partner or husband, affecting some 641 million women (World Health Organization, 2022). The majority of reported domestic violence incidents involve men as perpetrators and women as victims, and also have negative effects on the experiences of mothers and children (Littlechild, 2021; Muster, 2021). However, men also experience IPV (National Institute for Health and Care Excellence, 2014, 2018; Straus, 2012), with a small number of studies finding similar prevalence as for women (Desmarais et al., 2012a, 2012b). Public policy guidance is generally based on the premise that women in established heterosexual relationships are more likely than men to experience repeated partner abuse, abuse over a longer period of time, and more severe abuse, and are generally regarded as at risk of more severe and repeated physical violence, more coercive control, and to have more fear (National Institute for Health and Care Excellence, 2014; 2018).
This review uses the World Health Organization (2022) definition of IPV: Intimate partner violence refers to behaviour within an intimate relationship that causes physical, sexual or psychological harm, including acts of physical aggression, sexual coercion, psychological abuse and controlling behaviours. This definition covers violence by both current and former spouses and partners. (p.1)
Within such a definition, the literature can variously conceptualize/refer to different types of IPV processes within relationships—unidirectional; characterological; and asymmetrical—and as can be seen at the other end of a spectrum of such types of IPV, bidirectional, symmetrical, and situational. The latter three types are where, while the perpetrator is violent, they are not coercive and controlling, which has been seen to generally result from stressors and conflicts within intimate relationships (Crasta et al., 2022).
The review reported here looked at the evidence of the effectiveness of couple-based approaches to preventing IPV in heterosexual relationships. This topic is important because of the extent, nature, and effects of IPV in such couple relationships, and the possibility of strengthening families and society through relationship-based approaches to this problem.
Characterological IPV is where there is violence from one partner to another in terms of coercive and controlling behavior, which is mostly unidirectional, meaning that a particular program (e.g., couple-based) might be unsafe for one of the partners, a particular issue which arose within some of the research findings examined in this article. Such characterological IPV can be seen as commensurate with Duluth gender-based programs, which deal with male to female violence, related to patriarchal ideas, and issues of men's dominance over women partners, rather than where there is a greater degree of bidirectional IPV (Gondolf, 2015).
Bennett et al. (2020) conceptualize two general typologies of IPV: (1) characterological violence, where severe physical, psychological, and sexual IPV is used to dominate and control a partner; and (2) situational (or bidirectional) couple violence where couple conflicts escalate into IPV. The latter tends to be more symmetrical and reciprocal, often followed by remorse from both partners, and not involving a context of control or fear to the same extent. There is evidence for substantial bidirectional IPV within relationships (Langhinrichsen-Rohling et al., 2012; Moffitt et al., 2001; Spratt et al., 2022; Straus, 2008, 2009).
Regardless of the precise comparative prevalence of different forms of directionality of IPV among men and women and the proportion that is bidirectional, evidence suggests that most couples stay together at least for some time after IPV starts, with it often escalating over time. The couple partners often do not separate, with partners finding it difficult to leave for a number of reasons, including economic issues, children, and fear of increased violence from the other partner after such separations (National Institute for Health and Care Excellence, 2014, 2018; Psych Central, 2021). People experiencing IPV often fear disclosing the abuse at any point in time, from when it starts to escalate, including possibly while in treatment, and indeed afterwards. This highlights how safety and protection need to be considered across the range of couple-based treatments (National Institute for Health and Care Excellence, 2014, 2018; Psych Central, 2021).
One of the aims of this review was to examine the prevention of likely IPV or further IPV through relationship-based approaches. Prevention as referred to in this article relates to where assessments have been made about couples assessed at risk of IPV to prevent it happening, or where it has occurred already, to prevent reoccurrence. This review thus focuses on the prevention at secondary and tertiary levels within single agency and interprofessional agency work.
One of the first definitions of primary, secondary, and tertiary health care classified these as follows:
Interventions to prevent a problem from occurring as primary Interventions at a stage before problem is manifested as secondary. Remediation to reverse manifestations of problem as tertiary (Starfield, 1996).
The American Academy of Family Physicians (AAFP) states that primary care is provided by physicians specially trained for and skilled in comprehensive first contact and continuing care for people with undiagnosed signs or symptoms and includes health promotion, disease prevention, and health maintenance in a variety of settings (AAFP, 2024). Primary levels of prevention–relating to efforts such as public education programs and education in schools, aimed at a general population—were beyond the scope of this review. It was also beyond the scope of this review to consider risk factors for IPV in general (Spencer et al., 2020) or access to services (Baikady et al., 2023).
The UK's National Institute for Health and Care Excellence (NICE) defined primary health care as that which delivers outside of hospitals, whereas secondary care is to be provided in formal settings, for example, clinics/ hospitals. Tertiary care is defined as care that requires complex treatments in specialized settings (National Institute for Health and Care Excellence, 2018).
In this context, this review has excluded primary care as it involves generalized preventive work; this review was concerned with treatment for couples where the IPV was already acknowledged and requires specialist treatment. Building on the above context, in relation to established heterosexual couple IPV, the questions for this review were:
What types of relational approaches exist to support relationships so as to prevent and treat IPV at secondary and tertiary prevention levels? What does research tell us about the effectiveness of various types of relationship supports and programs in addressing IPV? What pointers to good practice in relationship-support programs to address IPV can be gained, including in relation to safety issues?
Method
The study team sought to use effective and transparent methods for this review of the literature (Campbell et al., 2018). This review used explicit methods for study identification and quality appraisal, followed by a systematic narrative approach to synthesizing a range of types of research findings (Popay et al., 2006). The systematic narrative review approach was employed, as it allows for a broad approach/scope to what is being searched for, and this area of efficacy of couple-based treatments for IPV, and with a particular focus on safety, is underresearched (see e.g., McKay & Bennett, 2023). Such an approach has an explicit, justifiable, and robust methodology for the searching and quality appraisal stages, followed by a narrative synthesis. Popay et al. (2006) set out the value of narrative systematic reviews, and examples of such reviews that allow for a broad search while maintaining methodological rigor and providing valuable evidence for practice are those of McKay and Bennett (2023) and Campbell et al. (2018). The value of systematic narrative reviews is set out by Sukhera (2022) as “a narrative review can include a wide variety of studies and provide an overall summary, with interpretation and critique. Examples of narrative review types include state of the art, critical, and integrative reviews, among many others…They allow review authors to advance new ideas while describing and interpreting literature in the field” (Sukhera, 2022, p. 414) (see Figure 1).
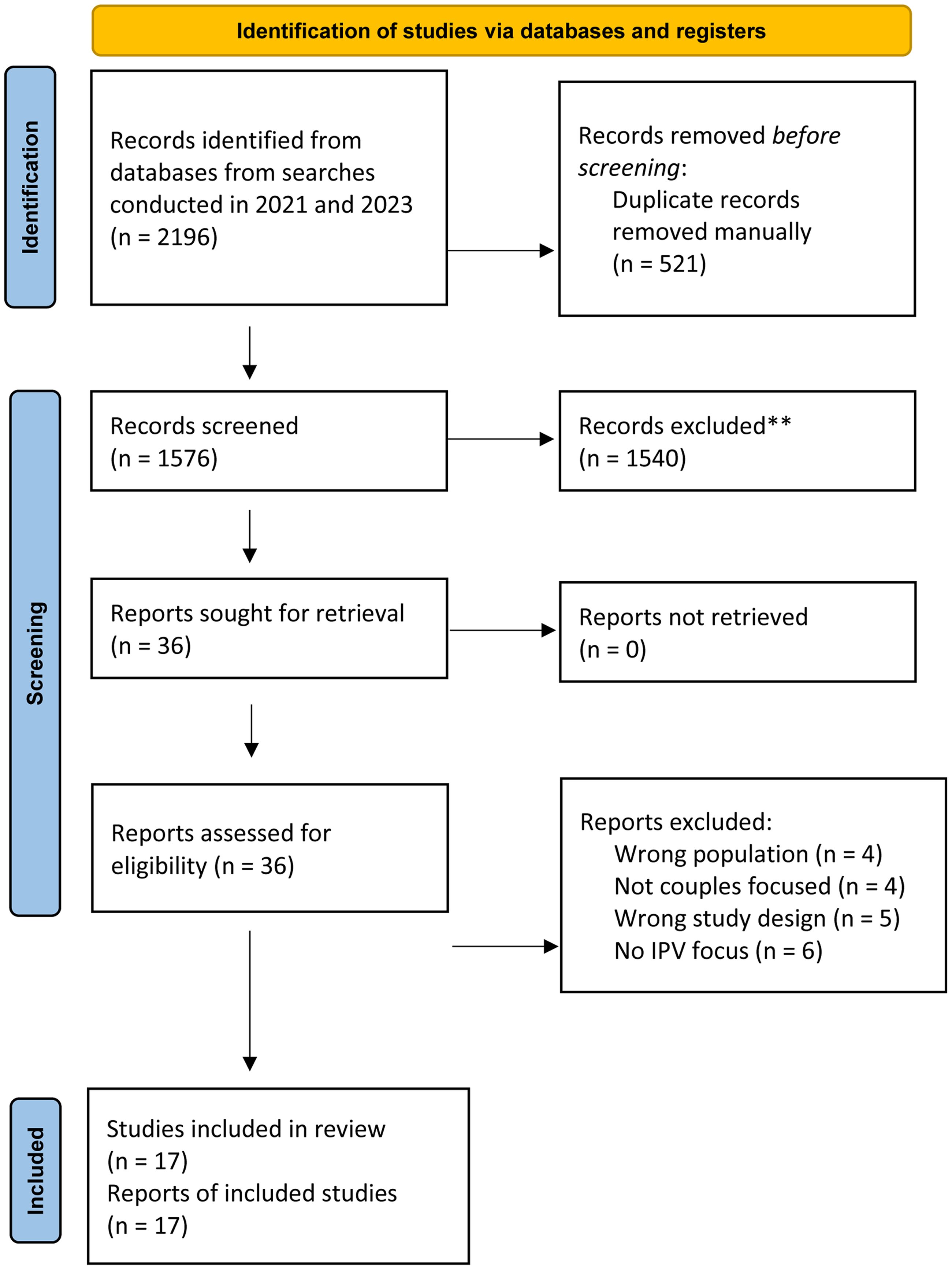
PRISMA diagram.
Identification of Included Studies
Three members of the research team worked together on the development of search terms for study identification (Booth et al., 2022) and to agree inclusion and exclusion criteria. There were no exclusions in relation to the countries in which the research was carried out.
The following terms were searched free text in the title or abstract: (Domestic OR partner OR marri* OR marital OR couple* OR relational OR relationship OR wives OR wife* OR husband*) N3 (violence OR abus* OR homicide OR maltreatment OR aggress* OR conflict OR assault*) AND (intervention OR service) AND (evaluation OR effectiveness). In addition, each concept was mapped to thesaurus subject headings across the different databases. For example, “Domestic Violence” AND “Psychosocial Intervention” AND “Program evaluation” (Table 1).
Inclusion and Exclusion Criteria.
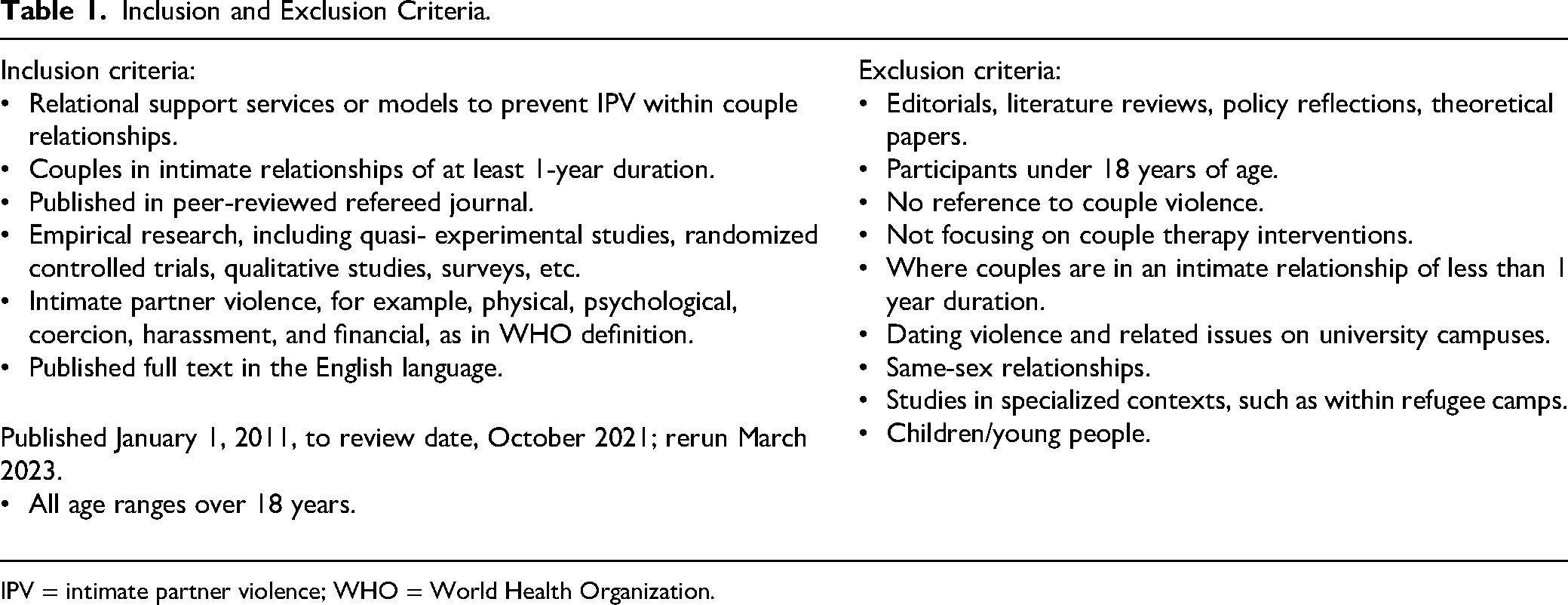
IPV = intimate partner violence; WHO = World Health Organization.
The development of the search strategy was informed by the research team's subject expertise, a scoping literature search, and published methodology on social work literature searching (Bates et al., 2017; Best et al., 2014), including specifically in relation to IPV (McGinn et al., 2016). The search was structured using three concept groups: IPV; relational programs and interventions; and evaluation of effectiveness. Five bibliographic databases were searched for publications in the English language, on the October 6 and 7, 2021: Medline, CINAHL Plus, Psychinfo, Social Care Online, and Scopus. Date limits were set for January 1, 2011, to the date of review. Full details of the search strategy can be obtained from the corresponding author. In all, 1,860 citations were retrieved from across the five databases. Duplicates were removed using Rayyan Qatar Computing Research Institute (QCRI) systematic review software (Ouzzani et al., 2016) giving, at that stage, a total of 14 articles for inclusion in the review.
An additional search was carried out to update the results and make them more contemporary (Rethlefsen & Page, 2021). The same software was used to carry out the same search again in March 2023. There were at this latter stage two methodological matters to consider. Changes in database access precluded the ability to rerun the search in PsychInfo. In addition, Social Care Online had been decommissioned but still searchable in March 2023, with updates having ceased in December 2022. In the updated searches in 2023 to capture the most recent publications, Medline, CINAHL Plus, Scopus, and Social Care Online gave a total, after removal of duplicates, of 237 articles. Overall, this gave a total of 1,576 articles for inclusion. Applying the inclusion criteria to these rerun searches, we added three original research articles to the analysis, making a final total of 17 articles for inclusion in the review.
Two members of the team independently reviewed articles for inclusion. Within a high level of agreement, areas of difference were discussed and resolved with three team members working together. The team used the populations, interventions, comparisons, outcomes, time, and settings (PICOTS) approach (Samson & Schoelles, 2012). The database searching was complemented by hand search of the included studies in the review articles retrieved; citation searching of the reference lists of included studies; and articles identified through previous work of the research team. Assessed against the inclusion criteria (see Table 1), these processes added one more article beyond those retrieved by the database search, giving a final inclusion of 17 studies.
In addition to the original research articles, we have included what we refer to as “relevant systematic reviews,” which focus on our particular review questions and aims, and provide valuable contextual findings in relation to lessons for social work (and other professional) assessments and interventions in this area. The search process retrieved six such relevant systematic literature reviews. The findings from these, and their relevance to the issues addressed in the currently reported review, are included in the Relevant systematic reviews section.
Method of Appraisal and Synthesis
The quality threshold for inclusion was that studies were published in a journal with a masked (“blinded”) refereeing process, thereby utilizing the expertise of appropriately selected peer reviewers (Taylor et al., 2007). The narrative synthesis used an adapted form of Thomas and Harden's (2008) thematic synthesis of qualitative research data as a means of completing both inductive and deductive analysis, to allow a rich and detailed account of the data, examining patterns to identify key themes within datasets, and to interpret the meaning behind the presence of those patterns and themes in context (Bengtsson et al., 2020). The approach involved reading and rereading the data in the original article, developing descriptive themes, and subsequently generating analytical themes.
Synthesis of Results
Overview of Included Research Articles
Of the 17 included studies there were 7 randomized controlled trials; 2 quasiexperimental studies; 5 qualitative studies; 1 study using secondary analysis of data on couples in treatment; 1 survey of couples; and 1 single-case nonconcurrent multiple-baseline design. Studies retrieved were from seven countries: USA (9), Iran (3), Colombia (1), Finland (1), Nigeria (1), Rwanda (1), and the UK (1). The total number of couples across all studies was 3,357. In addition to couple participants, several studies included also professionals or community members involved in the program (n = 37). In Stern et al.'s (2018) research on a couple-based intervention contained within a wider community-based program in Rwanda, one element of the intervention was the provision of “safe spaces,” and the views of the safe-space users (n = 7) and the safe-space facilitators (n = 3) were included, thus providing their perspectives of the value of these spaces as part of the intervention. In addition, this study included more general stakeholder views: the National Women's Council (n = 3); religious leaders (n = 3); and program staff (n = 3). In Ripoll-Núñez et al.'s (2012) study, family therapists (n = 3) and referring judges (n = 2) took part. In Raymond et al. (2016), clergy (n = 5) were interviewed, both the Christian (n = 1) and Muslim (n = 4) faiths. In McConnell's research, interviews with practitioners (n = 6) and team managers (n = 3) were included. The range of numbers of couples in each of the 17 studies varied from 1 to 1,080.
The themes developed for the final analysis were: (1) the effectiveness of programs, how this was judged, and for which groups of people; (2) the levels and nature of IPV relevant for couple-based therapy; (3) safety protocols (4) whether the program was state or court ordered or had voluntary attendance; (5) whether group- or couple-based delivery; and (6) attrition and completion rates (Tables 2 and 3).
Overview of Included Studies.
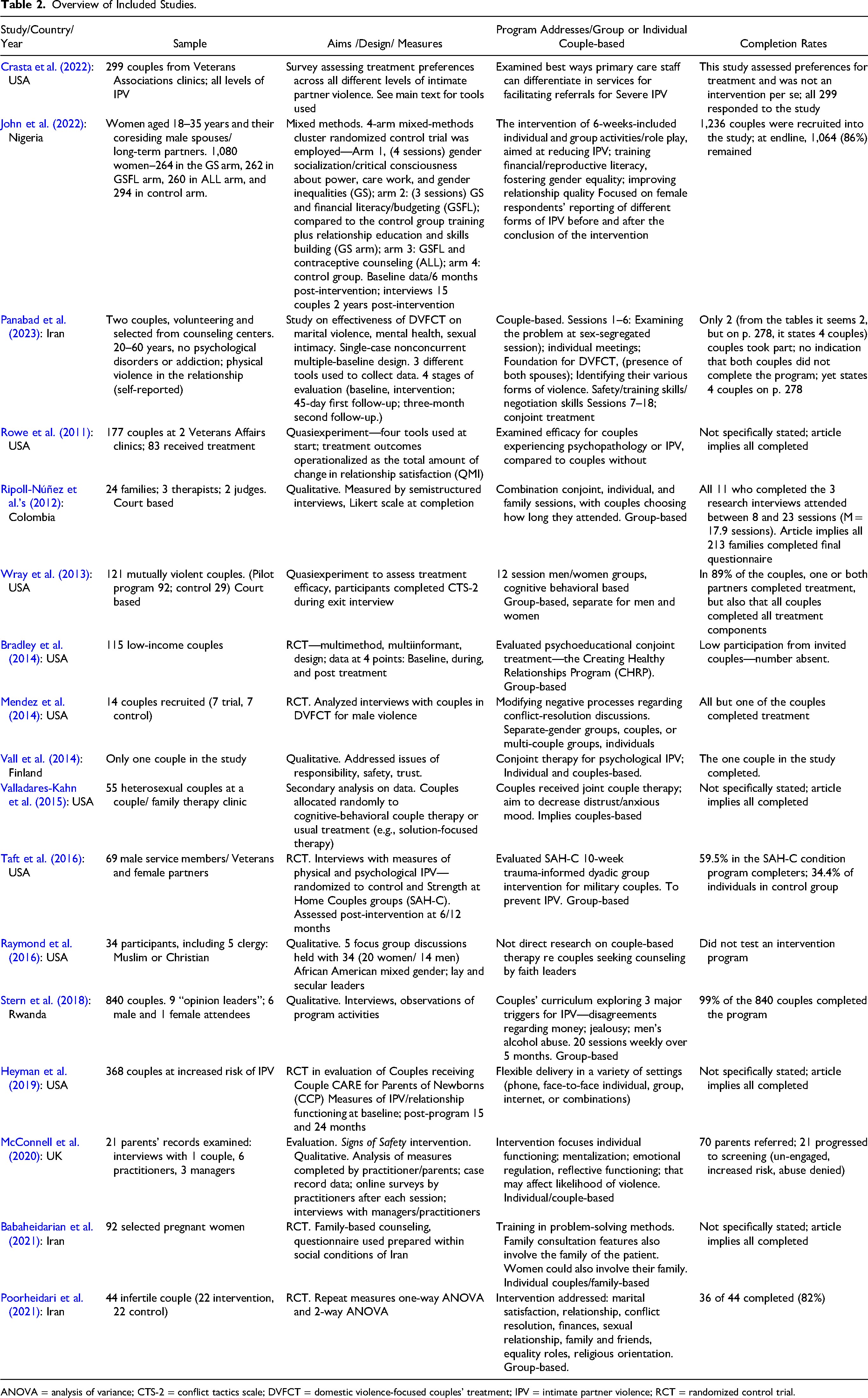
ANOVA = analysis of variance; CTS-2 = conflict tactics scale; DVFCT = domestic violence-focused couples’ treatment; IPV = intimate partner violence; RCT = randomized control trial.
Key Elements of Included Articles.
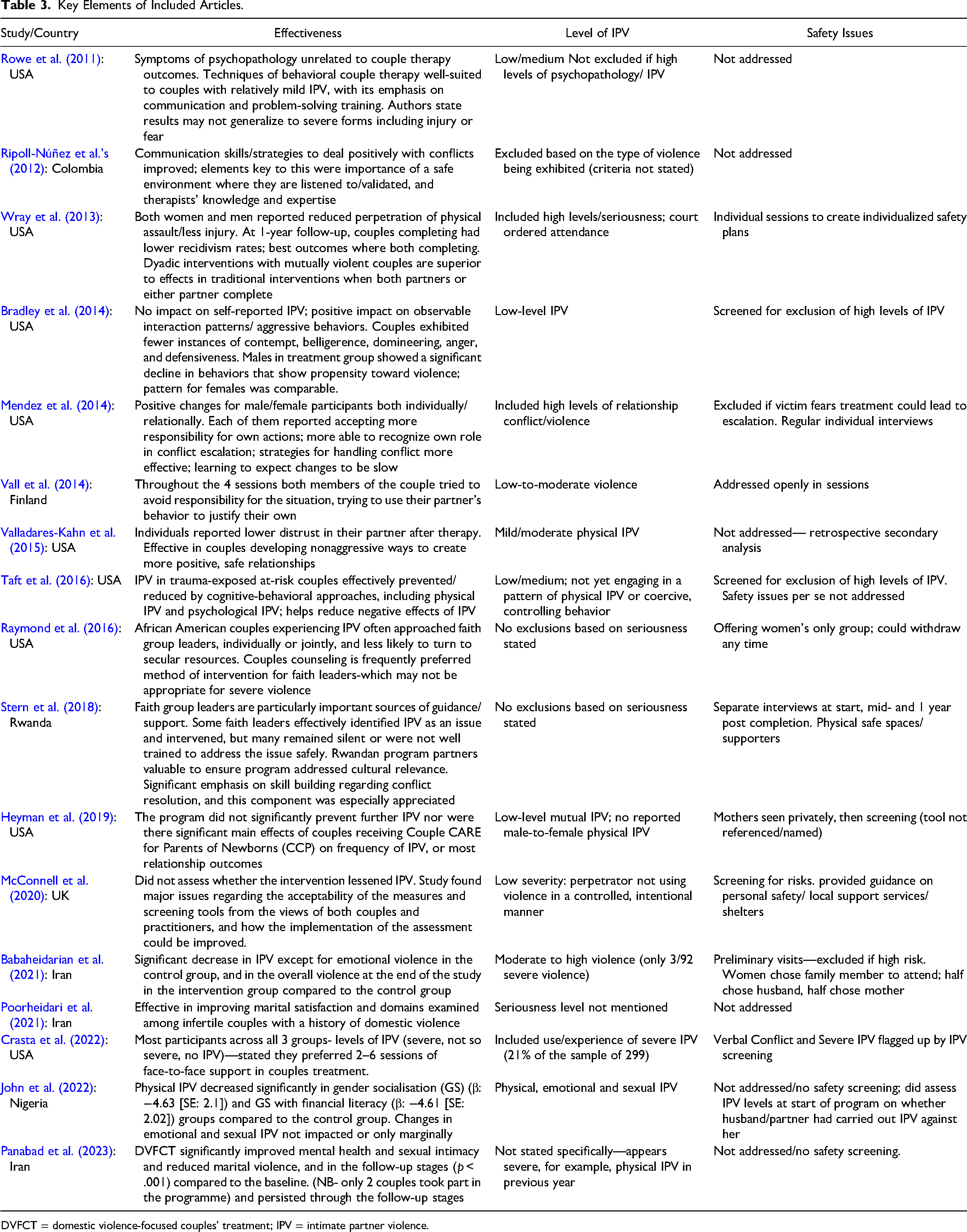
DVFCT = domestic violence-focused couples’ treatment; IPV = intimate partner violence.
Court-Ordered and Voluntary Programs
Eleven of the programs set out to assess and work with low to medium levels of IPV, and most studies examined programs which were voluntary rather than court ordered. A number of studies point out that one of the issues to consider within this is where there are court-based interventions, the motivations for the partners are likely to be different from that for a program in which participation is voluntary. The former may be more appropriate where there are issues of power and control, whereas voluntary programs might be more suitable where there is mutual aggression.
Group-Based or Couple-Based Interventions
Although most studies did not attempt to evaluate whether group-based treatment might be better than for couples alone, the main findings of those that did were group-based programs can be safe and effective where safety protocols are properly put in place, with Crasta et al. (2022) reporting that most partners preferred couple-based treatment, even where the IPV was the most serious.
Measures Used to Assess IPV Risk and Outcomes From Interventions
A range of tools was used in the articles included in the review to measure the risk of IPV and outcomes from interventions. There was varying use of tools at the beginning, during, or post-completion of treatment. Many studies used self-reported interviews or focus groups with couples; some used these with service providers also. The revised conflict tactics scale (CTS-2) (Straus et al., 1996) was the most frequently used scale; others are identified below. Bradley et al. (2014) observed interaction patterns and aggressive behaviors while couples tackled areas of disagreement. The specific affect coding system (SPAFF) was used in Gottman and Krokoff (1989) to analyze patterns of feelings and communication exhibited during discussions. Stern et al. (2018) used observational methods, also. Participants’ views about the value of various elements of the program were also a feature in seven studies.
Panabad et al. (2023) utilized the Symptom Checklist-90-Revised, the couples’ sexual intimacy questionnaire, and the violence against women questionnaire to collect data. Crasta et al.'s (2022) study assessing treatment preferences across different levels of IPV, including severe IPV, used the brief version of the revised CTS-2; patient health questionnaire; PTSD checklist; alcohol use disorder identification test; couples satisfaction index (CSI); danger assessment; women's experience of battering scale; and screener for clinically significant IPV. The verbal conflict and the severe IPV groups in this study were both flagged by IPV screening. The authors recommend the use of the women's experience of battering scale, as this explores the psychological experience of power and fear, relating to the safety issues we particularly address in this article.
In John et al.'s (2022) study, IPV was measured by way of a series of questions to the woman to assess if a husband/partner had been physically abusive. In-depth interviews with 15 couples (spouses interviewed separately) two-years post intervention were also carried out. Taft et al. (2016) used the six-item Quality of Marriage Index (Norton, 1983) to assess levels of IPV and risk. Other cut-off points were scoring below 101 on the dyadic adjustment scale (DAS) (Spanier, 1976) or psychological IPV above the 75th percentile on the revised CTS-2. The psychological aggression subscale elements of dominance/intimidation on the multidimensional measure of emotional abuse was also used for assessment purposes (Murphy & Hoover, 1999). The validated 32-item DAS; the depression and anxiety subscales of the 53-item brief symptom inventory; and the 2-item physical aggression subscale of the revised CTS-2S were used in Rowe et al.'s study, which also used the quality of marriage index to assess treatment outcome.
The secondary analysis by Valladares-Kahn et al. (2015) used the revised CTS-2 (Straus et al., 1996), and the positive and negative affect schedule (PANAS) (Watson et al., 1988). Individuals’ overall trust in their partner was measured with the eight-item dyadic trust scale (DTS) (Larzelere & Huston, 1980). Heyman, as well as questionnaires completed after each session by participants, program coaches, supervisors, and participants on the intervention process, also used the revised CTS, the CSI (Funk & Rogge, 2007); the relationship attribution measure (RAM) (Fincham & Bradbury, 1992); the behavioral self-regulation for effective relationship scale (SRS) (Wilson et al., 2005); and the conflicts and problem-solving scale (CPS) (Kerig, 1996).
In the Iranian study by Poorheidari et al. (2021), cultural issues were of specific note. Tools used were the standard CTS-2 and the ENRICH marital satisfaction scale. The standard Straus et al.'s questionnaire of domestic violence as modified in 1990 and 1996 was used, with revisions by Kazhal et al. (2008) for use in Iran, where three questions related to sexual violence were omitted because of cultural conflicts, and the phrase “sexual partner” was replaced by “spouse.”
In Panabad et al.'s (2023) study in Iran, the Symptom Checklist-90-Revised, couples’ sexual intimacy questionnaire, and the violence against women questionnaire were used. McConnell et al.'s (2020) study included the analysis of measures completed by participants during the assessment; case record data; practitioner surveys after each appointment; and qualitative interviews with managers and practitioners. The study found problems for both participants and practitioners with the tools used. The number of measures, the difficulty in explaining some of the language, and the unfamiliar measures, meant that practitioners had to decide whether to hold long sessions or additional sessions to complete the assessment. The complexity delayed scoring and made explanation to participants difficult.
Self-report was often used as a measure of change. However, there may be reasons why one of the partners might not report the extent or seriousness of IPV, and this is a key issue for safety during intervention (Heron et al., 2022; McConnell et al., 2020; National Institute for Health and Care Excellence, 2014, 2018). This is particularly relevant where there is characterological violence, with fear and control of the abused partner within the relationship dynamics. A number of the programs had separate meetings with each partner individually at the beginning and during the program to assess and manage safety risks.
The Efficacy of Couple-Based Programs
Various methods and tools were used within the research studies examined to assess progress and outcomes, as set out in the previous section. The overall results suggest where there were interventions, it resulted in positive evidence of effectiveness to some extent in most of the studies examined, whereas some were more mixed in the types of outcomes that can be seen as beneficial, often dependent upon the type and level of seriousness of IPV. The three exceptions to largely positive outcomes were:
Heyman et al.'s study (2019), with no significant prevention of further IPV or most relationship outcomes; it is notable that Heyman et al.'s study was with new parents in maternity units, and so had a rather specialist population. Bradley et al.'s (2014) study that showed limited efficacy, with no impact on self-reported IPV, though there were positive impacts on observable interaction patterns and aggressive behaviors, with couples exhibiting fewer instances of contempt, belligerence, domineering, anger, and defensiveness. Some studies did not address specifically if the intervention lessened IPV, for example, McConnell et al. (2020).
The strongest positive evidence was in relation to low, and sometimes low/medium levels of IPV. Evidence from programs addressing the more serious forms of IPV was from five, possibly six studies (as one did not state specifically severity in their sample). The studies clearly addressing the more serious forms of IPV were: Babaheidarian et al. (2021) (though only 3 of the 92 couples in this study were of a high level of seriousness), Crasta et al. (2022), Mendez et al. (2014), Rowe et al. (2011), and Wray et al. (2013). Panabad et al. (2023) did not specifically state severity in their sample, but inclusion criteria included physical IPV in the previous year, so probably would be viewed as severe. However, only two couples took part in the program, so this could be seen to limit the value of this study's findings, as may also be the case with Babaheidarian et al. (2021). Some studies did not state the level of seriousness in their sample: Stern et al. (2018); Raymond et al. (2016); Ripoll-Núñez et al.'s (2012); and Poorheidari et al. (2021).
There were inconclusive findings on the appropriateness and effectiveness of working with couples where one or both exhibited serious mental health disorders (e.g., schizophrenia or bipolar disorder) or severe substance abuse disorders. Some studies specifically excluded couples where there were issues of mental health problems or drug/alcohol misuse. These were excluded in Valladares-Kahn et al.'s study (2015)
Most studies, apart from Heyman et al. (2019) and Bradley et al. (2014), found a decrease in physical and psychological aggression. Other areas of improvement found across studies included: increased respect; better communication; improved feelings of well-being; increased trust; more positive mood; and reduced anxiety. Therapeutic solution-focused work on improving communication and conflict management were also valued. Partners could better recognize their own role in the escalation of conflict by gaining insight into the impact of their own behavior. They learned strategies for handling conflict more effectively and learned to expect change to be slow. In the Iranian study by Poorheidari et al. (2021), improvements in marital satisfaction, personal characteristics, relationship, conflict resolution, financial management, leisure activities, sexual relationship, family and friends, equality roles, and religious orientation were reported.
John et al.'s 2022 study discusses the potential utility of gender-transformative interventions for improving physical IPV outcomes. Physical IPV decreased significantly in the gender socialization (GS) (β: −4.63 (SE: 2.12)) and GS and financial literacy (β: −4.61 (SE: 2.02)) groups compared to the control group. Changes in emotional and sexual IPV were marginally significant or insignificant, respectively, suggesting that the intervention had little impact on nonphysical forms of IPV. At the same time, in in-depth interviews, couples reported improved communication and trust, and enhanced conflict management skills. They concluded that structural interventions may not be sufficient in the short term to shift the underlying gender-power dynamic and oppressive gender norms that promote IPV. However, the gender socialization component of the intervention, which focused on critical reflection, skill building, and relationship strengthening to foster egalitarian spousal relationships, may have been a crucial mechanism for reducing IPV in this population, and fostering women's empowerment within the household by targeting couples and addressing gender norms and strengthening relationship.
Safety Protocols
A key area mentioned by participants in studies was the need for feeling safe, and thus the need for safety protocols. Eleven of the studies mentioned this, with six not doing so (John et al., 2022; Panabad et al., 2023; Poorheidari et al., 2021; Rowe et al., 2011; Taft et al., 2016; Valladares-Kahn et al., 2015). There was a variety of levels and approaches taken, for example, unstructured or more structured guidance for therapists in the ways clinical assessment of risk should and could take place. Seven studies had specific protocols or tools which they used to specifically address this. In four of the studies which did address safety, it was unclear if a specific protocol or tool had been used. There was wide variation among programs in explicit assessment at the beginning and during the program, in relation to how safe each of the partners was feeling. There was variation in whether individual discussions and safe spaces were provided for each person in the couple to be able to share concerns, and a variety of ways in which this was addressed, from clinical judgment (with therapists advised to be aware of risks, and screen on this basis) through to the use of protocols or tools.
Only two studies referred to specific safety assessment tools. Crasta et al. (2022) recommend the use of the women's experience of battering scale, which explores the psychological experience of power and fear, as their study suggests the importance of evaluating fear/control issues and injury potential at the point of referral. In addition, Bradley et al. (2014) proposes the use of Friend et al.'s model (2011) regarding safety issues related to the type and severity of IPV, and addressing relationship dynamics that may provide insight into the severity and frequency of IPV, even if partners are not able or willing when asked directly about this. The screening procedure used in Bradley et al. (2014), the revised CTS-2 (Straus et al., 1996), was found to be helpful in assessing indirect information about violence in the relationship, such as motivation for violence and beliefs regarding the impact of violence on a person's partner.
In Ripoll-Núñez et al.'s study (Ripoll-Núñez et al., 2012), the clinicians checked safety issues with clients regularly throughout the intervention. Where high levels of potentially injurious or controlling violence were suspected, facilitators spoke with partners individually, to identify couples who were not appropriate for this type of conjoint treatment based on the type of violence being exhibited. McConnell et al. (2020) concluded that couple-based interventions require assessment processes that clarify risk and needs, and which screen out unsuitable couples. However, Crasta et al.'s (2022) findings were that each of the partners within the couple, even if there may be concerns regarding, for example, characterological/asymmetrical/unidirectional IPV, would tend to still prefer couple-based treatments even if their IPV is at a serious level; so perhaps the key issue is if each partner really is feeling safe in any treatment that is about to or is taking place. McConnell et al. (2020) note the complexity of balancing safe, comprehensive assessment and couple engagement within this context, and how it is inherently difficult to predict safety; as risk is dynamic and inherently contextual, practitioners need to be aware that participant accounts may not be reliable. They highlight several risk assessment tools for domestic abuse used in the UK that may be of value: the domestic abuse, stalking and honor-based violence (DASH) risk model used by police services, the spousal assault risk assessment (SARA) (Kropp et al., 1999), and the danger assessment scale (Campbell et al., 2009). The appreciation of the effects of such behavior in engendering of fear in victims—on the reporting of abuse, and the fear of the reactions from the abuser if they do—can be seen to be key to the development of partners’ responses to such domestic violence, and their feelings of ability to be able to report this in protecting themselves.
Religious and Faith-Based Issues
Faith group leaders were found to be particularly important sources of guidance and support by Stern et al. (2018) in Rwanda. Raymond et al. (2016) found that African American couples in the USA experiencing IPV often approached faith group leaders, either individually or jointly, and are less likely to turn to secular supports. They found that when a couple experiences severe violence, there may be problematic issues to address regarding safety, as couple counseling is frequently the preferred method of intervention from faith leaders, which may not be appropriate for serious IPV where there are characterological situations. Issues of cultural understanding were raised by two of the studies. In such situations, faith leaders are placed in the difficult position of balancing divergent interests in maintaining family integrity, protecting the victim, and counseling the perpetrator. Stern et al. (2018) note how involvement of Rwandan program partners as codesigners and facilitators ensured the program was culturally relevant. In Babaheidarian et al.'s work (2021), data were collected using a questionnaire which was amended to be more culturally sensitive to the social culture of Iran.
Accepting Individual Responsibility for Behaviors
In contrast to the findings of Vall et al. (2014) on the limitations of intervention on this, Mendez et al. (2014) found that couples in their programs talked about both themselves and their partners accepting more responsibility for their own actions after the intervention. Some female participants who reported becoming empowered said they were less likely to tolerate unacceptable behavior from their partner following treatment. Mechanisms of survivor validation in which perpetrators are held to account have been found to be central to the change process (McGinn et al., 2015). Panabad et al. (2023) also mentioned this as part of the process although it is worthy of note the authors’ viewed couples having “serious problems in accepting responsibility for their actions, especially the female victim who holds her husband responsible for beating her” (p. 278).
Attrition Rates
There was wide variation in the rates of attrition. Attrition was high in the 22-week program evaluated by Bradley et al. (2014), and work by Hawkins et al. (2012) shows shorter relationship-education programs with 9–20 hours of content may be more effective, as attending once a week for the full 22 weeks the program was too challenging for some participants, resulting in lack of intervention completion. This might be addressed by shortening the program, and improving the incentives, for example, providing childcare support, light snacks, meals, or transport to decrease attrition. In McConnell et al.'s (2020) study, only 21 of 70 parents referred progressed to screening and assessment. John et al. (2022) had a 14% attrition in the program they examined, and in Panabad et al.'s (2023) research, there were two couples both sets completing the program.
Relevant Systematic Reviews
Armenti and Babcock's (2016) review outlines U.S. court- and state-mandated treatments for male-perpetrated IPV, recommending conjoint treatment may better address IPV not motivated by power or control, and concluded that the programs may not meet the needs of couples experiencing bilateral or situational violence, or where a woman is the primary aggressor.
The review by Carr (2014) presented evidence from meta-analyses, systematic literature reviews, and controlled trials for the effectiveness of couple and family therapy for adults with various relationship and mental health problems. There was evidence for couple therapy (typically involving 20 sessions over 6 months) being effective for many couples, whereas most traditional programs for male perpetrators at that time were judged to have small effects on IPV reduction
Stith et al. (2022) state that IPV is common among couples seeking relationship education or therapy. Their review examined research findings for both IPV and child maltreatment from 2010 to 2019 that targeted couple or family relationship interactions or processes that addressed IPV treatment, which included conjoint interventions. They determined that, including studies before 2010 that they examined, relationship education programs (including IPV between couples) are “probably efficacious,” while programs based on cognitive behavioral couple therapy are “possibly efficacious” (Stith et al., 2022, p.247).
Karakurt et al. (2016) concluded from their review of six articles that couples suffering from situational violence may benefit from couple therapy, but professionals are cautious to risk the possibility of further IPV between the partners during and after treatment. They concluded that benefits varied across couples, and advised those providing interventions to consider their patients’ cultural background before determining whether couple therapy is an appropriate intervention. They stressed that their findings were only applicable to instances of mild to moderate situational couple violence.
A systematic narrative review of studies of survivor perspectives of IPV perpetrator interventions found that survivors identified some positive changes in their male partner due to his taking part in a program although the sustainability of this change was unclear (McGinn et al., 2015). Changes were perceived in their partners’ behavior and beliefs, and also in the respondents’ feelings of safety. Key barriers to perpetrator change from the survivors’ perspectives included alcohol dependency, mental health challenges, and relationship dynamics. Survivors perceived changes in perpetrator behavior through the use of conflict interruption techniques and new communication skills. Changes in belief systems were viewed as needed for complete desistance from violence, but more difficult to effect. Mechanisms of survivor validation, in which perpetrators are held to account, were viewed as central to the change process.
Spencer et al.'s (2019) meta-analysis provides an overview of risk indicators for IPV victimization, examining 391 studies in analyzing 50 risk indicators for IPV victimization for women and 28 risk indicators for men. The study calculated the overall strength of each risk indicators for both men and women, to find which were most strongly correlated with IPV victimization across gender. Five of the 28 risk markers differed significantly between men and women; namely alcohol use, depression, older age, child abuse in family of origin, sexual IPV victimization; findings which may aid in assessment of risk and safety for treatments.
Limitations of the Review
The inclusion criteria for this review of evidence for the effectiveness of couple-based interventions where there is IPV within relationships referred only to heterosexual couples. Reviewing studies in relation to, for example, those within lesbian, gay, bisexual, or transsexual relationships (see e.g., Harden et al., 2022) was beyond the scope of this review. This review did not set out to study equality and diversity issues, such as ethnic background, although studies from a range of countries and cultures are available (see e.g., Sokoloff & Dupont, 2005). The perspectives of perpetrators might also add a richness to the understanding of the effectiveness of IPV interventions (McGinn et al., 2020).
Discussion and Applications to Practice
This systematic narrative review addresses evidence from original research studies, and previous relevant reviews in allied areas, about the outcomes from couple-based relational interventions for working with interpersonal violence in the form of IPV within established couple relationships at secondary and tertiary prevention levels. The studies provided evidence—as measured by the participants’ experiences and opinions, and a variety of tools and instruments—in relation to improvement in aspects of relationships, desistance from future IPV, and safety for both participants. Overall, the studies reviewed contribute to conceptualizing the effectiveness of relationship interventions for IPV in relation to the level of seriousness of the IPV, and its nature.
The review found that overall, in 15 of the 17 articles included, couple-based approaches utilizing various mixes of individual and group-based therapy can effectively reduce the likelihood of IPV. Attrition was low for the majority of couple-based relational programs (see Summary Table 2). There was wide variation in rates of attrition, with little clear evidence of whether longer programs had higher attrition rates although this is suggested to be the case by Bradley et al. (2014), and from this they suggested that work by Hawkins et al. (2012) shows shorter relationship-education programs with 9–20 hours of content may be more effective and have higher program completion rates. The strongest evidence of the effectiveness in the programs studied was in relation to low and sometimes low/medium levels of IPV, with less evidence of programs attempting to include more serious characterological violence, with associated elements of coercive control.
In relation to studies where measures of change were used and positive changes were recorded, and dependent upon the particular aims and context of the intervention, positive changes were found in reduced rates of IPV; development of communication skills, conflict resolution skills and strategies to deal positively with situations that cause IPV; feelings of safety for both partners; level of trust and longer term change in themselves and their partners; and in an Iranian study, financial management, leisure activities, sexual relationships, relationships with family and friends, equality roles, and religious orientation.
One measurement of change often used is that of self-reported violence although the validity of this has been questioned, as one of the partners might not report IPV either at assessment or later. This may be due to the fear of repercussions if a partner using coercive control came to know of their partner's reports of this to agencies, and thus there would appear to a need for this to an essential feature in assessment and interventions to be planned for and minimized. There can be concerns among agencies and practitioners that couple-based approaches can minimize abusers’ feelings of personal responsibility and accountability for their part in the violence. Evidence of partners accepting personal responsibility as a result of interventions was weak but most did not attempt to examine this.
The nature and levels of seriousness of IPV in a presenting couple, and screening for this, was a key feature in several studies. Methods for assessing applicability of the program to certain couples were examined, and the results of examination of assessments for programs based on, for example, where there is mutual aggression, or where it may be on another end of the spectrum, where there was violence from one partner to another in terms of controlling behavior. This latter configuration can mean that a particular program (e.g., couple-based) might be unsafe for one of the partners. Most programs studied set out to assess and work with couples:
Who were experiencing mutual aggression rather than characterological IPV between themselves; In whom there was a low to medium level of physical, psychological or emotional abuse; and In programs that could be state or court ordered, or voluntary, without any such level of compulsion.
There were few, inconclusive, findings on the appropriateness and effectiveness of working with couples where one or both exhibited serious mental health disorders or severe substance abuse disorders although Rowe et al. (2011) found that symptoms of psychopathology (e.g., depression, anxiety) were unrelated to couple therapy outcomes, and Panabad et al. (2023) found that DVFCT had generally improved mental health amongst participants in their study.
The literature has variously conceptualized different types of IPV processes within relationships as situational; symmetrical; bidirectional; unidirectional; characterological; and asymmetrical. In general, there is evidence for positive outcomes from relationship-based approaches to IPV in low to medium severity cases. However, programs need to have safety protocols and risk-assessment tools for acceptance onto the program and during ongoing treatment. The severity and nature of the IPV should, from the results of this review, be regarded not as an either/or for assessment of whether an individual situation is one of characterological coercive control or one of mutual violence and aggression but as a continuum, with a decision reached with each partner re safety.
Safety of both participants within relationship-based approaches to IPV was found to be a key feature. The evidence from this review would be that although safety issues (and effective assessment of these) are important, couple-based interventions can often be acceptable to, and even welcomed by, both partners (Crasta et al., 2022) where the program facilitates them to feel safe. Examples are given in this review, including approaches and tools for doing this. A key finding is that of Stern et al. (2018), who conclude that the provision of “safe spaces” was an important element in the program.
These review findings can be valuable for social workers and other professionals in understanding how they might most effectively provide safe relationship-based interventions for couples where there is a medium to high risk of IPV. The strongest positive evidence was in relation to low and sometimes low/medium levels of IPV. The article has set out main areas of improvements, by what means, that couple-based interventions can bring, and why. The evidence that various forms of both individual and group-based interventions for couples at risk of IPV or where it is occurring can safely reduce the likelihood of IPV, most reliably in relation to mutual low or medium levels of IPV, with maybe less validity for more serious, characterological forms of IPV. However, in relation to one of the concerns raised by some, that such couple-based work can put individual partners at risk of further IPV, particularly where there are signs of control by one partner over the other, it seems clear from our knowledge that careful assessment and screening are needed with regard to possible negative effects within the applicability and safety of couple-based relational programs. Thus, proactive assessment and ongoing monitoring of the safety of both partners, considering potential coercive control within characterological forms of IPV within the couple's relationship becomes important. This then leads to consideration of methods and tools to aid identification of safety issues for both partners. Articles reviewed recommend, for example, Friend et al.'s model (2011), and obtaining direct information regarding perpetration and victimization of violence via the CTS (Straus et al., 1996), as mentioned within this article.
Regarding treatment planning, length of programs and the complexity and number of tools used within them are issues to be considered, as addressed by McConnell et al. (2020) and Bradley et al. (2014), with the latter referring to work by Hawkins et al. (2012) that suggested that relationship-education programs with 9–20 hours of content had the strongest effects. In terms of measuring the effectiveness of such interventions, Bradley et al. (2014) highlight the importance of including observational methods to detect program effects, as well as self-report before commencement of, and during, the intervention. The currently reported review highlighted how in certain cultures and faith groups, faith group leaders are an important source of information and support for couples exhibiting IPV, with individuals and couples in those groups less likely to seek other forms of help.
Specific issues for assessment and involvement in couple-based treatment have been highlighted, particularly in relation to the safety of both partners and mechanisms to ensure this. Although good evidence was found in the review of the benefits of couple-based therapy, the findings tended to be in relation to low or medium levels of IPV, and where there was mutual violence and aggression rather than coercive (characterological) control by one partner. Mechanisms for assessing and managing safety during programs have been considered in depth. Features identified by clients as being key within the interventions included the importance of a safe environment where they are listened to and validated, and therapists’ knowledge and expertise. There may be a spectrum of types of IPV which might, with further research, be classified and then assessed and considered in applying safety assessment within effective relational interventions for specific types of IPV.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Norwegian Financial Mechanism 2014–2021 grant for the operational program: Justice, through the Institute of Justice, Warsaw, Poland. This support is gratefully acknowledged.