
Abstract
Until recently, little attention has been given to the experiences of lesbian, gay, bisexual, transgender, and queer or questioning (LGBTQ+) young people in the social care system, or the needs of social workers supporting this population. A systematic scoping review of the international evidence demonstrates that LGBTQ+ young people are disproportionately overrepresented in social care, and experience poorer health, mental health, and well-being outcomes compared to their cisgender and heterosexual counterparts in care (Schaub, Stander, et al., 2022). It is estimated that between 15.5% and 30.4% of young people in care identify as LGBTQ+, and this overrepresentation is far greater for those from racial or ethnic minority backgrounds (Fish et al., 2019; Schaub, Stander, et al., 2022). While LGBTQ+ young people enter care for the same reasons as their peers (e.g., abuse, neglect), they often experience rejection, marginalization, and discrimination related to their sexual orientation, gender identity, and expression (SOGIE) in different phases of contact with the care system, from initial referral through to aging out or leaving care (Kaasbøll et al., 2021; Schaub, Stander, et al., 2022). This includes increased placement instability or breakdown, longer duration of time spent in care, and an overreliance on restrictive group home placements for LGBTQ+ youth (McCormick et al., 2017; Schaub, Stander, et al., 2022), which have been found to have an adverse effect on mental health outcomes (Evans et al., 2017; Ford et al., 2007). Although fewer data are available regarding the experiences of transgender and gender-diverse young people, the literature suggests heightened challenges among this group from peers, birth families, and social care professionals (Mountz et al., 2018; Schaub, Stander, et al., 2022). Overall, LGBTQ+ young people are less satisfied with their out-of-home care experiences than non-LGBTQ+ youth and have specific social care needs that often go unmet or ignored due to prevailing hetero- and cisnormative societal values or biases (McCormick et al., 2017; Schaub, Stander, et al., 2022).
One of the most significant challenges in supporting LGBTQ+ young people is limited knowledge and training in this area for social workers. Social work students and practitioners report a lack of knowledge and an absence of adequate training to meet the needs of LGBTQ+ young people, and trans and gender-diverse people especially (Craig et al., 2016; Inch, 2017; Schaub, Stander, et al., 2022). In addition to this, social workers and social work students may also have neutral or even negative and homo/bi/trans-phobic attitudes toward LGBTQ+ young people, and do not believe that care systems are particularly protective or supportive of this population (Greeno et al., 2022; Weeks et al., 2018). Indeed, LGBTQ+ young people report cis/heteronormative care environments, delaying disclosure of their SOGIE in fear of negative reactions, and harmful encounters with professionals who characterized their SOGIE as pathological, predatory, and circumstantial (Kaasbøll et al., 2021; Schaub, Stander, et al., 2022; Schaub et al., 2023). Affirming relationships with social workers is particularly important to the resilience of this population and an openness and willingness to discuss SOGIE-related issues are strongly associated with positive outcomes (Álvarez et al., 2022; Paul, 2020; Ryan et al., 2009; Schaub et al., 2023). Training can thus have a significant positive impact on the experiences of LGBTQ+ young people; however, there is a dearth of research in this regard.
Several studies have investigated the efficacy of ongoing professional development and training in improving knowledge, attitudes, and beliefs of helping professionals toward LGBTQ+ individuals, and the results are promising. Recent systematic reviews exploring the effectiveness of LGBTQ-related training interventions among medical, nursing, and mental healthcare students and providers found that educational programs can be effective at improving self-reported knowledge and promoting more tolerant attitudes about the LGBTQ+ community and LGBTQ-related healthcare (Bettergarcia et al., 2021; Yu et al., 2023). Similarly, studies found that professional development training programs on LGBTQ+ issues had significant positive effects on teachers’ and educators’ beliefs and attitudes toward LGBTQ+ young people (Greytak et al., 2013; Szalacha, 2003). Nevertheless, there is a paucity of research regarding the training of social workers. A recent non-randomized pre- and post-test study evaluating an LGBTQ+ competency training intervention (comprising of two 3-hr in-person sessions) with child welfare practitioners (i.e., social workers, clinicians, and group home staff) indicate that practitioners significantly improved their knowledge of LGBTQ+-related issues and competencies post-training (Weeks et al., 2018). Much of this work, however, originates from the USA with an absence of international research and no large, robust studies, such as randomized controlled trials (RCT), to date evaluating the effectiveness of such training for social care professionals for supporting LGBTQ+ young people (Hunt et al., 2019; Schaub, Stander, et al., 2022).
The use of e-learning modules can be an effective strategy to provide ongoing professional development and enhancement of professionals’ knowledge in working with marginalized populations. This method has several advantages over traditional face-to-face training. First, e-learning training programs provide flexibility and easy access to learning materials from any location from which the learner has access to the Internet (Akhter et al., 2021; Gad, 2023). E-learning training modules may be an attractive option for social workers who struggle with high workloads and caseloads. Second, this type of training can be developed and maintained with limited resources and as a result can be offered at a low price (Akhter et al., 2021). This may be particularly relevant in contexts where there are ongoing developments in the policy and legal landscape concerning LGBTQ+ rights.
To the best of the authors’ knowledge, this study is the first RCT evaluating the effectiveness of e-learning training module for improving the knowledge and attitudes of social workers about LGBTQ+ young people. We also examined possible factors that might account for differences in primary outcomes. The literature suggests several factors that may facilitate or inhibit the effectiveness of LGBTQ+ knowledge programs including age, gender, religiosity, and a connection to the LGBTQ+ community. Previous studies highlight the impact of intergenerational differences in understanding SOGIE among helping professionals, with younger generations correlated with more positive attitudes toward LGBTQ+ communities (Gandy-Guedes, 2018). It has also been well established that women display more favorable attitudes than men toward LGBTQ+ people (Dotti Sani & Quaranta, 2020; Herek, 2002), and there is a close connection between religious affiliation, or religiosity, and negative attitudes among social workers toward LGBTQ+ people (Westwood, 2022). Finally, having a close friend or family member who identifies as LGBTQ+ has been linked to greater LGBTQ+ knowledge and the potential to engage in supportive behaviors in a recent survey with care professionals in the USA (Greeno et al., 2022).
The current study tested the effectiveness of an e-learning training module for children's social workers in England to support LGBTQ+ young people, compared to “business as usual.” We evaluated the impact of the training on LGBTQ+ knowledge and heteronormative attitudes and beliefs. Based on previous literature, we developed the following hypotheses:
Intervention group participants will increase their LGBTQ+ knowledge, in comparison to the control group. It is expected that the score on the LGBTQ+ Knowledge Scale (KNWL) will increase between the pre- and post-test for the intervention group, and remain similar for the comparison group. Intervention group participants will decrease in heteronormative attitudes and beliefs, in comparison to the control group. It is expected that the score on the Heteronormative Attitudes and Beliefs Scale (HABS) will decrease between the pre- and post-test for the intervention group and will remain similar for the control group or decrease to a lesser extent.
Moderators taken from previous literature (described above) including age, gender identity, religiosity, connection to the LGBTQ+ community, and previous training, are included as covariates. We recognize that the study is underpowered to detect such effects with statistical significance, so these tests will be indicative only.
Method
Design
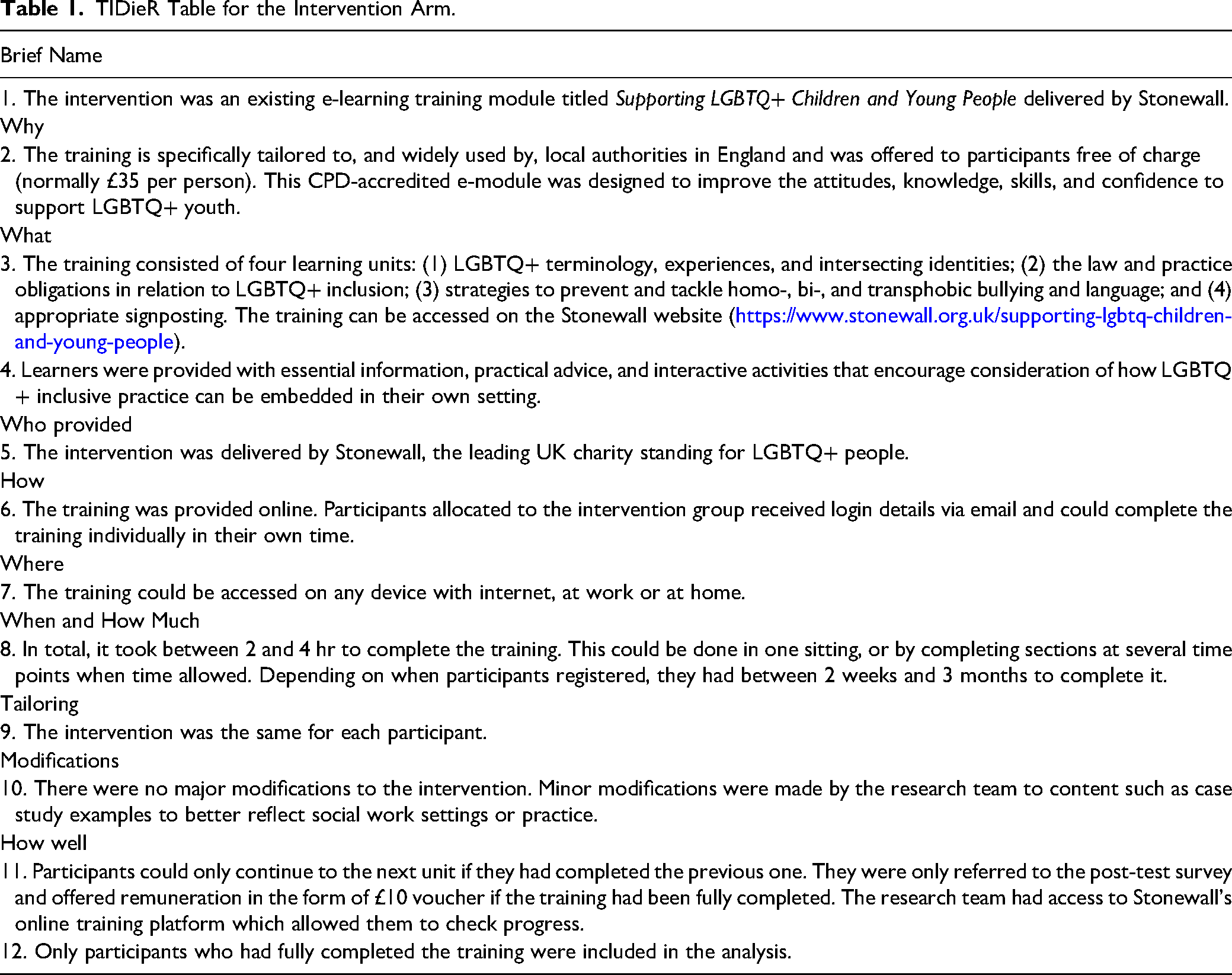
This study has a two-armed, pre- and post-test, pragmatic pRCT design combined with a census-style process evaluation. PRCTs measure the effectiveness of an intervention in “the real word,” more specifically, under usual conditions of care (Zwarenstein et al., 2008). Participants were individually randomized to either the intervention or control group. Intervention participants were provided access to the Stonewall e-learning module, and the control group followed a “business as usual” model (further details provided in Table 1). A pRCT design was appropriate for this study for three key reasons: (1) The e-learning intervention is already in wide use, making it important to test its effectiveness; (2) a number of cohort trials of education programs suggest this is a promising way of informing social workers about sexuality and gender (Inch, 2017; Schaub et al., 2017); and (3) there was sufficient recruitment power to conduct a pRCT that would provide meaningful results.
TIDieR Table for the Intervention Arm.
The census-style process evaluation was conducted in accordance with key Medical Research Council (MRC) guidance (Moore et al., 2015). It was designed to assess the intervention delivery to understand and explain any identified intervention effects (or lack thereof; see Schaub, Montgomery, et al., 2022 for further details on design and conduct). Additionally, it aims to understand the extent to which participants were satisfied with different aspects of the training program and identify any suggested changes for improvement.
This trial was analyzed and reported in line with the Consolidated Standards of Reporting Trials for Social and Psychological Interventions (CONSORT-SPI) reporting guidance (Montgomery et al., 2018) and a checklist is available by writing the corresponding author. This study followed a published protocol (Schaub, Montgomery, et al., 2022) and utilized co-production techniques involving a range of stakeholders, including social care professionals and a group of LGBTQ+ young people (16–24) with lived experiences of social care. Study design included feedback from stakeholders at different stages of development, implementation, and evaluation. We also solicited stakeholder perspectives on drafted practice and policy recommendations. The trial was registered on the Open Science Framework (OSF; https://osf.io/25d8z).
Participants and Procedures
Participant recruitment was designed in response to the dispersed nature of the social care sector and the scale of the study. Participants were recruited using a number of complementary sampling strategies. First, the research team drew on existing connections with social work networks and connections to disseminate the recruitment call. Second, we undertook a social media campaign advertising the study on Twitter, LinkedIn and Facebook. Third, we approached individuals based on their specific position and knowledge (critical case sampling). Lastly, we used chain sampling, asking participants to forward the recruitment call to other potential participants (Onwuegbuzie & Collins, 2007). A separate paper provides recommendations for the recruitment and retention of social workers as research participants (Keemink et al., forthcoming).
The recruitment advert provided potential participants with a registration link to a Qualtrics (2020) page where eligibility was checked. Individuals were eligible to participate if they met all four inclusion criteria: (1) employed by a local authority in England, (2) work in children's social care services, (3) registered with Social Work England, and (4) not have previously completed a Stonewall e-learning module. If criteria were met, they were sent a Qualtrics link to the pre-test survey including a consent form following which they were randomized at the individual level. Participants in the intervention group were automatically given access to the post-intervention test on completion of the e-learning module. Participants in the comparison group were sent a link to the post-intervention test a month before completion of the study (November 2022). From November 2022, participants received weekly text and email reminders to complete the post-test. After completion of the post-test, participants received a thank-you email including a £10 e-voucher. Upon conclusion of the trial, participants in the comparison group were allowed to access the training, but this incurred a cost to their organization.
Conditions
Intervention Arm: Stonewall E-Learning Module
We describe the intervention in Table 1 following the Template for Intervention Description and Replication (TIDieR, Hoffman et al., 2014).
Control Arm: Business as Usual
Participants in the control group received an email informing them that they would undergo business-as-usual (BAU) training conditions as provided by their employer (e.g., general Equality and Diversity training which is mandatory in the UK), and that they would be contacted in November 2022 to capture such training and complete the post-test. There was no further contact between the control group and the research team. While this posed a risk for attrition, this approach reflects the pragmatic nature of this trial and approximates the real-world context. We recognize that there would be considerable heterogeneity within this group as BAU is likely to vary across social work departments across the country. However, this variability forms a sound, pragmatic basis from which to compare the intervention. It may also be the case that some participants may have accessed the intervention (contamination).
Measures
Measures were administered between June and November 2022. The primary outcome measures for this study were heteronormative attitudes and beliefs and perceived LGBTQ+ knowledge. The pre- and post-tests aim to detect changes in the two outcome measures before and after randomization.
Outcome Measure 1: Heteronormative Attitudes and Beliefs
Heteronormative attitudes and beliefs are measured with the 16-item HABS (Habarth, 2015), which assesses participants’ heteronormative attitudes, as well as including elements of gender identity. Questions are answered on a 7-point Likert scale, ranging from strongly disagree to strongly agree. The HABS produces an overall score with excellent internal reliability (α = .91) and consists of two subscales, Essential Sex and Gender, which has excellent reliability (α = .92), and Normative Behavior, which has acceptable reliability (α = .78). Items 1, 4, 9, 11, 12, 15 and 16 are reverse coded, and the maximum score is 112. Higher scores indicate stronger heteronormative attitudes and beliefs. This scale has successfully been used in previous research with UK social workers (Schaub et al., 2017).
Outcome Measure 2: Perceived LGBTQ+ Knowledge
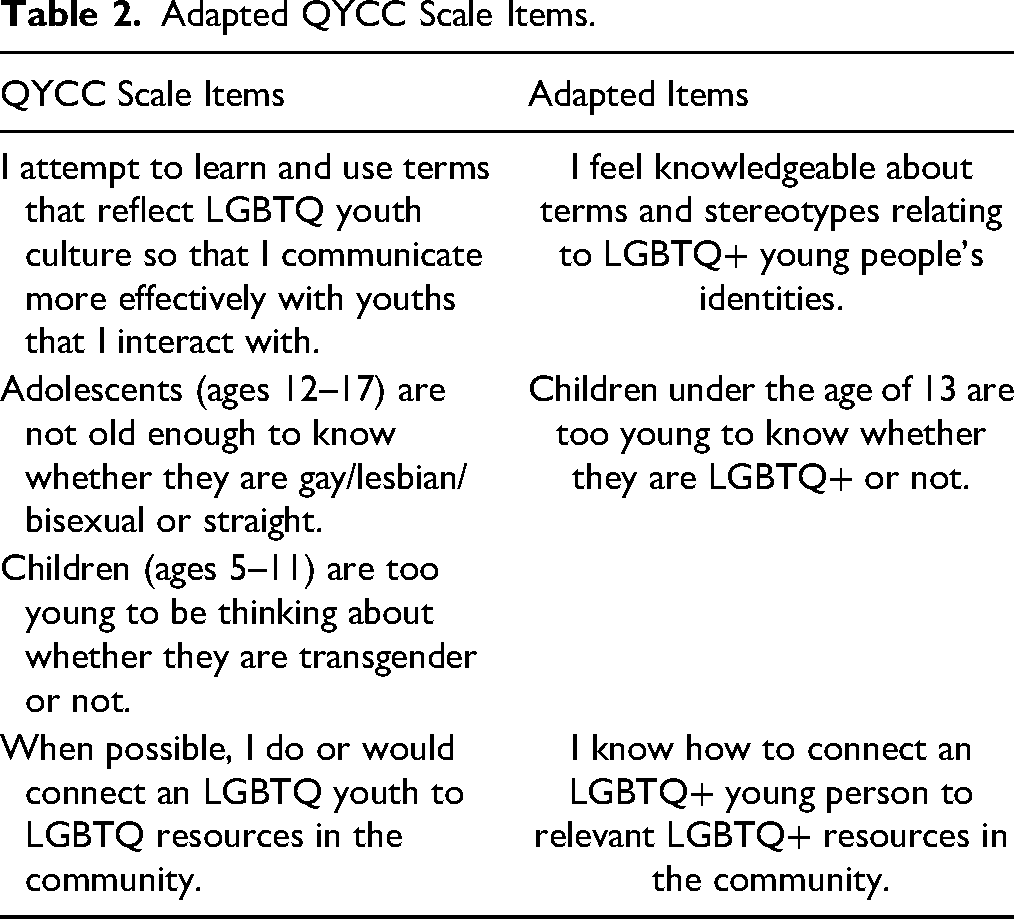
To assess social workers’ perceived LGBTQ+ knowledge of social workers in working with LGBTQ+ populations, we used an adapted version of a Queer Youth Cultural Competency Scale (QYCC) aimed at people engaging with LGBTQ+ young people (Gandy-Guedes, 2018). This scale has excellent internal reliability (α = .94). Our version is a five-item measure adapted according to the core components of the intervention and our theory of change model (see Schaub, Montgomery, et al., 2022), and questions are answered on a 5-point Likert scale, ranging from strongly agree to strongly disagree. The full scale was shortened to five items to limit the time burden on participants. Although it was based on an existing, reliable scale, our adapted scale was not validated; arguably, this has consequences for its reliability. However, in similar studies, LGBTQ+ knowledge is commonly assessed using non-standardized measures specifically designed by research teams for their training programs (Morris et al., 2019). A few examples of adapted items can be found in Table 2. For our version, Items 3 and 4 are reverse scored, and the maximum score is 25. Higher scores indicate greater knowledge about the LGBTQ+ community.
Adapted QYCC Scale Items.
During the pre-test, we also collected data on age, gender identity, sexual orientation, years of working experience, ethnicity, and previous LGBTQ+ training. Additionally, data on religiosity and connection to the LGBTQ+ community were gathered with the following measures.
Religiosity
Religiosity was measured with the seven-item Interreligious Centrality of Religiosity Scale (CRSi-7; Huber & Huber, 2012), which measures five core dimensions of religiosity (intellect, ideology, public practice, private practice, and experience) and is suitable for both Abrahamic and non-Abrahamic religions. There are very high correlations between the measure and self-reports of religious identity (r = .83). Responses are recorded with five-point Likert style items focussed either on frequency (very often, often, occasionally, rarely, never) or level of importance (very much so, quite a bit, moderately, not very much, not at all).
Connection to the LGBTQ+ Community
Participants were asked if they have any close friends or family who identify as LGBTQ+. The response options included yes, no, or prefer not to say.
Process Evaluation
In addition to the outcome data collected to analyze the effect of the intervention on heteronormative attitudes and LGBTQ+ knowledge, the post-test for the intervention group included process evaluation questions to assess the training program's acceptability, implementation, mechanism, and context. The process evaluation included both open and multiple-choice questions.
Randomization
Participants who had provided consent and completed the pre-test were randomly assigned to the intervention group or control group using web-based allocation. Participants were individually randomized and occurred continuously throughout the trial. The research team undertook six weekly balance check to ensure stratification and identify any imbalances. The research team was not blind to participant grouping but was unaware of allocation at the start of the trial due to the web-based allocation. This was necessary to support intervention participants with any challenges with accessing the training. Recommendations for trials where blinding is not appropriate include blinded outcome assessment and robust outcomes (Kahan et al., 2014); Both of these were included here. Furthermore, while participants were aware of their allocation (given the pragmatic nature of the intervention), they were unaware of other participants’ allocation.
Data Analysis
Quantitative data were analyzed using IBM SPSS Statistics Version 28 (IBM Corp, 2021). Demographic data are presented using descriptive statistics. Effectiveness of the training and exploration of moderators are analyzed using inferential statistics (analysis of covariance [ANCOVA], repeated measures ANOVA). We have taken an intention-to-treat approach (ITT) for the primary outcome measures (HABS and KNWL). This approach includes all participants who were randomized, irrespective of group allocation and missing outcome data. This is a conservative approach, ensuring unbiased conclusions about intervention effectiveness (McCoy, 2017). Findings will be reported and compared for two approaches to missing data imputation: Baseline Observation Carried Forward and imputation of group means. Additionally, data will be analyzed following a per-protocol approach to compare findings. These results can be found on OSF.
Qualitative data from implementation and process evaluation were analyzed using conventional content analysis (Hsieh & Shannon, 2005). Coding was completed concurrently and supported by QSR NVivo software. Relevant factors were identified relating to implementation outcomes and suggestions for quality improvement/practice change. These were discussed with the advisory groups to ensure alignment with sector applicability.
Power Analyses
A paucity of similar studies in the literature meant that we were unable to carry out a priori power analyses with suitable certainty. Nevertheless, a meta-analysis of anti-bias, multicultural, and moral education training programs aimed at reducing prejudice, concludes that a small to medium effect of d = .23 is common for large-scale samples (Paluck et al., 2021). Based on this effect size, it was estimated that we required 298 participants in each trial arm (for 80% power, 0.05 significance level).
Ethical Considerations
Ethical approval was obtained from the University's Ethics Committee in April 2022. All participants provided electronic informed consent (on Qualtrics) before participating in the study and were free to withdraw at any point before the conclusion of the study.
Results
Participant Flow
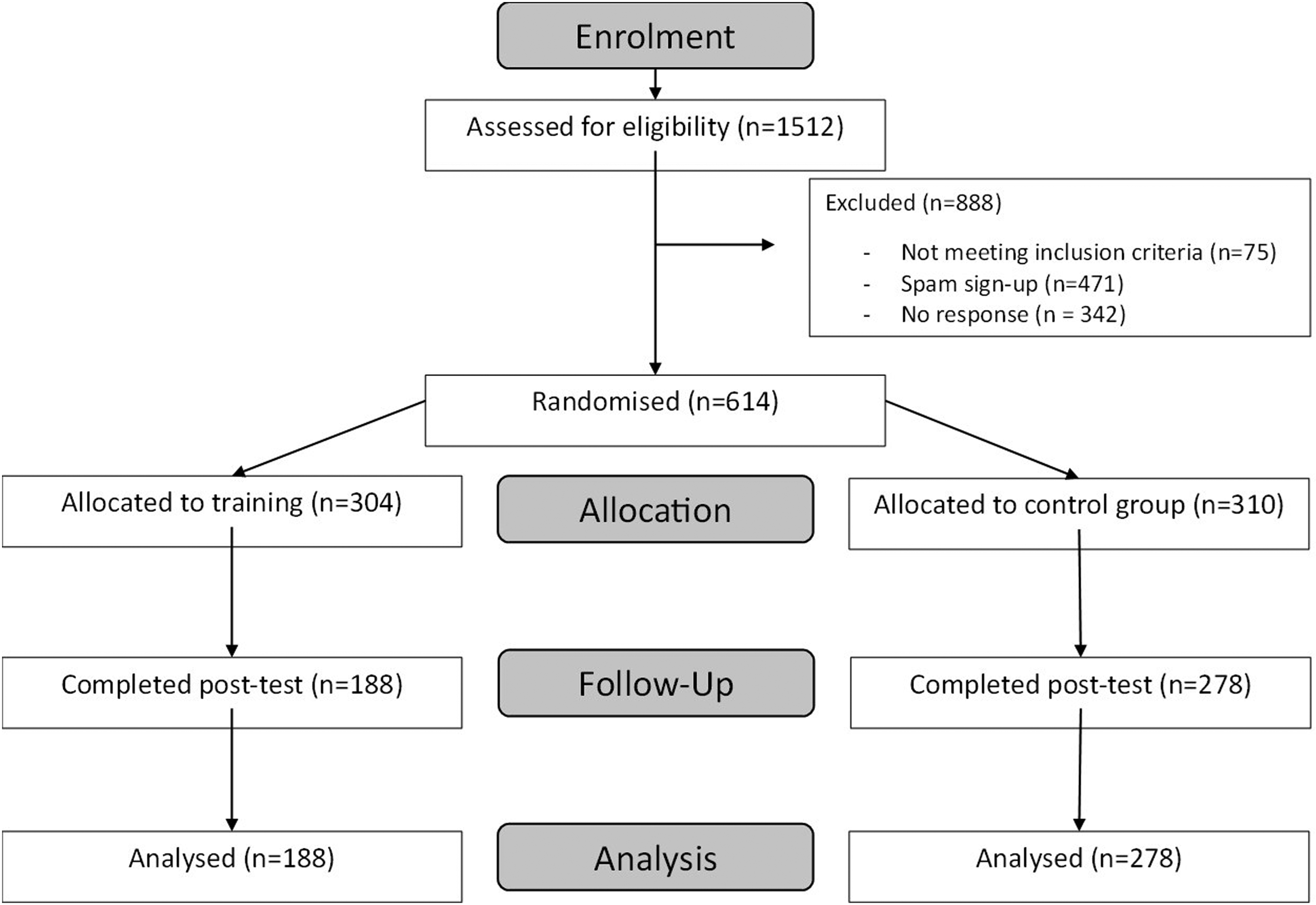
In total, 1,512 people registered for the study, of which 927 were eligible to participate (see Figure 1). Exclusion occurred due to not meeting the pre-specified inclusion criteria, spam sign-ups, and non-response after invitation to pre-test. Six hundred fourteen people completed the pre-test and were randomized, with 304 participants in the intervention group and 310 participants in the control group. The post-test was completed by 188 participants in the intervention group and 278 participants in the control group, making the final sample for analysis 466.
Trial flowchart.
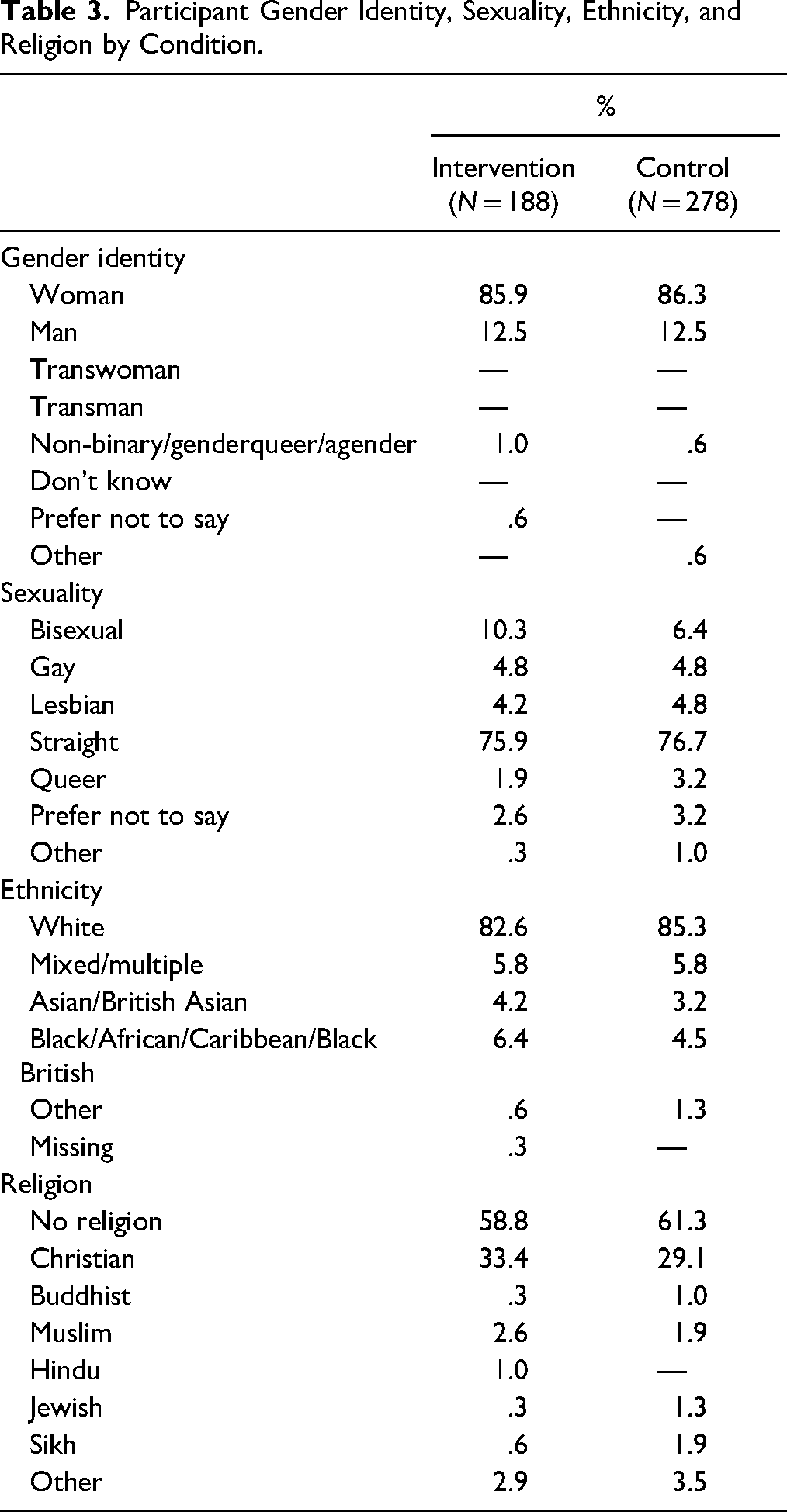
Tables 3 and 4 present the participant characteristics for both conditions in terms of gender identity, sexual orientation, religion, age, and years of experience as a social worker. The average age of our sample was approximately 40 years (41.18 in the intervention group, 39.27 in the control group), which broadly aligns with the general population (GOV.UK, 2022).
Participant Gender Identity, Sexuality, Ethnicity, and Religion by Condition.
Participant Age and Years of Experience by Condition.

Data Checks
Before running the main analyses, data were visually inspected and checked to meet assumptions of normality, homogeneity, and linearity.
Effectiveness of the Intervention
At pre-test, the intervention condition scored slightly higher on the HABS scale (Intervention, M = 40.12; Control, M = 38.98), and slightly lower on the KNWL (Intervention, M = 19.84; Control, M = 21.09). No other baseline differences were found between groups, except that an independent samples t-test indicated that there was only a significant difference between condition on the KNWL scale (Intervention M = 19.84, Control M = 21.09) on the pre-test, t(622) = −4.356, p < .001. Table 5 presents the means and standard deviations for the main outcome scales on the pre- and post-test for each condition.
Means and Standard Deviations on the HABS and KNWL Scale per Condition.

Missing Data
Analysis of patterns of missing data indicated that two variables had more than 1% missing data: HABS post-test (25.3%) and KNWL post-test (26.0%) as is typical in trials such as this one (Crutzen et al., 2015). Split by condition, it became evident that the intervention condition had 39.5% missing data for both post-tests. Unusually, the control condition had only 11.2% missing data for the HABS post-test, and 12.5% missing data for the KNWL post-test. The analyses suggested that data were missing at random. Taken together, this means that the intervention group had an attrition rate of 38.2% and the control group had an attrition rate of 10.3%. Differential attrition rates can be problematic for the internal validity of studies, and we have considered this in the interpretation of our findings.
The following results are presented using two different imputation approaches. First, we describe analyses using the last observation carried forward (LOCF) approach, in which missing data are imputed based on a participant's last observed score on the dependent variable(s). In this case, at baseline, we only have a pre- and post-test measure. This means that the participants for which we would impute outcome data based on their baseline observations automatically do not present any change between pre- and post-test (regardless of condition). Therefore, this is a very conservative approach to missing data. Additionally, we undertook and report here the analyses using the post-test mean for each condition as imputation, which is a more positive approach to missing data. Each missing value on the post-test will be replaced by the mean of the available data for that condition.
ANCOVAs
These analyses test the following hypotheses:
Compared to control group participants, intervention group participants will increase their LGBTQ+ knowledge. It is expected that the score on the LGBTQ+ KNWL will increase between the pre- and post-test for the intervention group and will remain similar for the control group. Compared to the control group, intervention group participants will decrease in heteronormative attitudes and beliefs. It is expected that the score on the HABS will decrease between the pre- and post-test for the intervention group and will remain similar for the control group or decrease to a lesser extent.
For the following analyses, we used a LOCF imputation method.
Heteronormative Attitudes and Beliefs Scale
There was no difference between conditions on the HABS post-test score, F(1, 615) = 1.335, p = .248, η p 2 = .002, but LGBT connection and HABS pre-test score were significant predictors of HABS post-test score, F(1, 615) = 4.255, p = .040, η p 2 = .007; F(1, 615) = 72.454, p < .001, η p 2 = .105.
Perceived LGBTQ+ Knowledge Scale
An ANCOVA with the KNWL post-test score as dependent variable, condition as independent variable, and age, gender identity, LGBTQ+ connection, religiosity, previous LGBTQ+ training, and KNWL pre-test score as covariates revealed a significant effect of condition, F(1, 615) = 15.756, p < .001, η p 2 = .025. Participants in the intervention condition scored higher on the post-test KNWL scale (M = 22.64) than participants in the control condition (M = 21.52) when controlled for the covariates. There was also a significant covariate for KNWL pre-test score, F(1, 615) = 46.727, p < .001, η p 2 = .071, indicating there was a significant effect of condition while controlling for the KNWL pre-test score.
For the following analyses, we used a mean imputation method.
Heteronormative Attitudes and Beliefs Scale
The intervention decreased heteronormative attitudes and beliefs since participants in the intervention condition scored lower on the post-test HABS scale (M = 35.68) than participants in the control condition (M = 37.78). An ANCOVA with the HABS post-test score as dependent variable, condition as independent variable, and age, gender identity, LGBTQ+ connection, religiosity, previous LGBTQ+ training, and HABS pre-test score as covariates revealed a significant effect of condition, F(1, 615) = 9.606, p = .002, η p 2 = .015.
Perceived LGBTQ+ Knowledge Scale
The intervention increased perceived LGBTQ+ knowledge as participants in the intervention condition scored higher on the post-test KNWL scale (M = 24.11) than participants in the control condition (M = 21.79). An ANCOVA with the KNWL post-test score as dependent variable, condition as independent variable, and age, gender identity, LGBTQ+ connection, religiosity, previous LGBTQ+ training, and KNWL pre-test score as covariates revealed a significant effect of condition, F(1, 615) = 116.006, p < .001, η p 2 = .159.
Per protocol analyses revealed significant effects of Condition for both outcome measures, see OSF for more details.
Table 6 provides an overview of the F, p, and η p 2 values for the different data analysis approaches (ITT vs. Per protocol) and different imputation methods (LOCF and mean imputation).
F, p, and η p 2 Values of the ANCOVA Main Effect for Condition for the Different Analysis and Imputation Approaches.
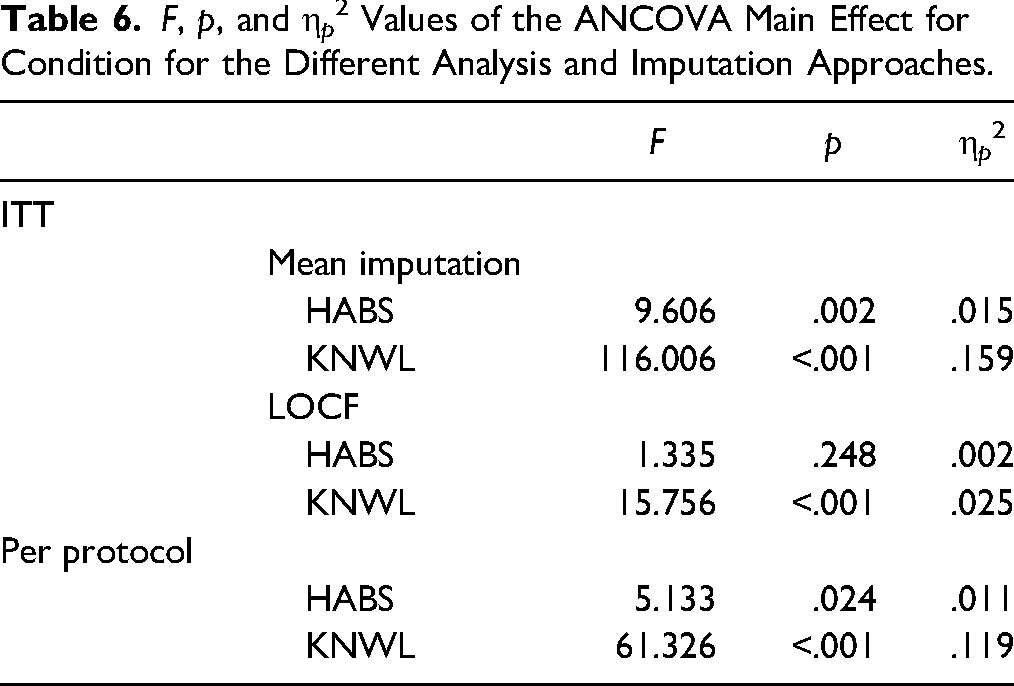
The ANCOVAs confirmed both of our hypotheses. Intervention condition participants scored higher on the post-test KNWL scale and lower on the post-test HABS scale, compared to control condition participants. The only exception was the result on the post-test HABS scale with the LOCF imputation. All effect sizes for main effects could be considered large (Richardson, 2011). However, the effect sizes for the difference on the KNWL scale were larger than the effect sizes for the HABS scale. This difference is reflected in the Discussion section.
Repeated Measures ANOVAs
We conducted a series of repeated measures ANOVAs to examine whether the difference between pre- and post-test measures differed between the intervention and control condition.
For the following analyses, we used a LOCF imputation method.
Heteronormative Attitudes and Beliefs Scale
There was a difference between the pre- and post-test on the HABS. A repeated measures ANOVA with pre- and post-test scores on the HABS as within-subject factors, and condition as between-subject factor only yielded a significant main effect of the HABS (pre vs. post), F(1, 622) = 11.712, p < .001, η p 2 = .018.
Perceived LGBTQ+ Knowledge Scale
There was a difference between the pre- and post-test on the KNWL scale, and this difference was larger for the Intervention condition. A repeated measures ANOVA with pre- and post-test scores on the KNWL scale as within-subject factors, and condition as between-subject factor yielded a significant main effect of the KNWL scale (pre vs. post), F(1, 622) = 88.261, p < .001, η p 2 = .124, and a significant interaction effect of the KNWL × Condition, F(1, 622) = 34.747, p < .001, η p 2 = .053.
For the following analyses, we used a mean imputation method.
Heteronormative Attitudes and Beliefs Scale
There was a difference between the pre- and post-test on the HABS, and this difference was larger for the Intervention condition. A repeated measures ANOVA with pre- and post-test scores on the HABS as within-subject factors, and condition as between-subject factor yielded a significant main effect of the HABS (pre vs. post), F(1, 622) = 28.023, p < .001, η p 2 = .043, and a significant interaction effect of the HABS × Condition, F(1, 622) = 8.909, p = .003, η p 2 = .014.
Perceived LGBTQ+ Knowledge Scale
There was a difference between the pre- and post-test on the KNWL scale, and this difference was larger for the Intervention condition. A repeated measures ANOVA with pre- and post-test scores on the KNWL scale as within-subject factors, and condition as between-subject factor yielded a significant main effect of the KNWL scale (pre vs. post), F(1, 622) = 191.756, p < .001, η p 2 = .236, and a significant interaction effect of the KNWL × Condition, F(1, 622) = 98.956, p < .001, η p 2 = .137.
The significant main effects found in these analyses further confirm our two hypotheses. Additionally, the significant interaction effects demonstrate the difference between pre- and post-test measures was greater for the intervention condition than for the control condition, strengthening the evidence for the effectiveness of the e-learning module. Again, all effect sizes for the main effects could be considered large (Richardson, 2011). Effect sizes were higher for the difference on the KNWL scale for both imputation methods. This difference is examined in the Discussion section.
Split Group Analyses
For the following analyses, we used the data set where missing values were imputed using mean imputation. We explored whether the intervention was more effective for specific subgroups based on previous research (see above). For the perceived LGBTQ+ knowledge measure, no subgroup differences were identified. However, analyses for the HABS revealed several subgroup effects. A significant effect of condition was identified for participants:
with 0–10 years of experience, F(1, 426) = 6.226, p = .013, η
p
2 = .014. who identified as straight, F(1, 474) = 10.667, p = .001, η
p
2 = .022. who identified as a woman, F(1, 535) = 8.379, p = .004, η
p
2 = .015. who were over 35, F(1, 260) = 7.074, p = .008, η
p
2 = .026. who had a connection to the LGBTQ+ community, F(1, 494) = 9.277, p = .002, η
p
2 = .018.
These groups scored lower on the HABS post-test than participants in the control condition compared to other subgroups, suggesting the training could be most effective for these subgroups. The effect sizes of these analyses can be considered large, suggesting practical significance.
Implementation and Process Evaluation
In the post-test survey, participants (N = 188) in the intervention condition were asked several questions about the process of undergoing the e-learning module. Both quantitative and qualitative data were collected. Analysis of quantitative data revealed that participants were positive about the e-learning module. More than 90% of participants reported being very satisfied or satisfied with each of the four units of the training module and found it easy to enroll in the course. Having completed the course, 99.5% of participants think they are better able to support LGBTQ+ young people. Qualitative data indicated participants felt their skills and confidence were improved about working with LGBTQ+ young people. They described the value of tailored resources; research and case study guidance; practical recommendations/strategies to address SOGIE-related challenges; and applications of professional's legal and professional responsibilities as per the Equality Act 2010.
When asked about areas requiring better explanation, only 15.7% answered yes. From this small minority of responses, analysis showed that participants would prefer greater focus on social work context (e.g., inspection criteria, local authority requirements for social care), and more information about young people that are transgender, gender diverse, or with asexual or pansexual identities. Additionally, social workers wanted more content about two topics: working with families of origin about challenges accepting SOGIE, and what supports would be effective in improving the poor mental health of LGBTQ+ young people in care.
Discussion and Applications to Practice
This study was the first RCT testing the effectiveness of an LGBTQ+ knowledge e-learning training module for children's social workers. We evaluated the impact of the training on social worker's LGBTQ+ knowledge and heteronormative attitudes and beliefs compared to a control group experiencing “business as usual.” Following a review of the literature, we included age, gender identity, religiosity, connection to the LGBTQ+ community, and previous training as potential covariates.
Our findings show the training was effective at increasing LGBTQ+ knowledge and reducing heteronormative attitudes and beliefs of children's social workers, when tested in the real world. We examined the effectiveness using best practice analysis approaches and found an effect of the training for all approaches, except on the HABS using an ITT analysis and LOCF imputation method. In all analyses, the perceived LGBTQ+ KNWL yielded an effect of the intervention. We also found significant interaction effects for the two main outcome scales and condition. These effects demonstrate the difference between pre- and post-test measures was greater for the intervention condition than for the control condition, further strengthening the evidence for the effectiveness of the e-learning module. Furthermore, the implementation and process evaluation suggested participants were very positive about training access and content. Most importantly for this study and the population under inspection, participants felt confident that their LGBTQ+ knowledge had increased as a result of the training.
Although the change in both knowledge and attitudes was significant, the effects on knowledge were larger. This discrepancy seems intuitive, as the main theory of change of the training was to increase participant's knowledge about LGBTQ+ young people and their support. An increase in knowledge by learning facts and concepts is likely to be easier to achieve than a change in attitudes, which would involve developing new viewpoints; this change often includes an emotional factor and might require contact with the marginalized group (Steck & Perry, 2017). A contrasting supposition is the difference in effect size could be attributed to the difference in scales used. The scale for perceived LGBTQ+ knowledge included five answer options, whereas the HABS scale provided seven answer options. Indeed, the number of Likert scale response options may affect response style (Weijters et al., 2010).
With respect to the covariate analyses, we only found significant effects in the ITT analyses in which we used an LOCF imputation method. For the HABS, a connection to the LGBTQ+ community and the HABS pre-test were found to be significant. For the perceived LGBTQ+ KNWL, the pre-test was a significant covariate. Overall, these findings demonstrate that the moderators that we included are not strong predictors of intervention success, suggesting that the intervention is relatively robust in its effectiveness.
Subgroup analyses only revealed differences in the HABS measure and suggested that the training might, perhaps, be more effective in reducing heteronormative attitudes and beliefs for certain groups than others. More specifically, stronger effects on heteronormative attitudes and beliefs were found for children's social workers who: (1) have 0–10 years of experience, (2) identify as straight, (3) identify as a woman, (4) have a connection to the LGBTQ+ community, or (5) are over 35 years old. However, these findings should be interpreted with caution, as the subgroups were unequal in size and some subgroups were potentially too small to reach sufficient power. A lack of an effect in some of the subgroups can be explained by further exploring the pre-test scores. For example, we did not find an effect of condition on the HABS post-test scores for those who identify as LGBTQ+, which can perhaps be attributed to the assumption that LGBTQ+ participants are more likely to have fewer heteronormative attitudes and beliefs to start with regardless of condition.
Overall, our analyses provide substantial evidence about the effectiveness of the e-learning training module. We opted for the use of several analysis approaches and missing data imputation methods to explore the robustness of the results. We found effects for almost every analysis and imputation method used. Our findings echo consistent calls within the literature for SOGIE training and the experiences of LGBTQ+ young people in care (Schaub, Stander, et al., 2022). This study supports and expands on previous research related to training among helping professions and demonstrates the effectiveness of e-learning training in improving the knowledge and attitudes of social workers regarding LGBTQ+ young people with a brief but comprehensive intervention. This information is important as it can increase the accessibility of education and training specific to this group in highly accessible and relatively cost-effective ways among the wider social care workforce. These findings are also relevant to those engaged in a range of educational and training settings in other helping or public sector professions, and have implications beyond social work practice, education, and research.
A notable strength of this study is that was the first of its kind within the UK social work context succeeding in the recruitment of a large sample of children's social workers. Rigorous RCTs remain scarce in social care and social work research (Dixon et al., 2013; Moody et al., 2020). We utilized co-production techniques involving a range of stakeholders, including social care professionals and a group of LGBTQ+ young people (16–24) with lived experiences of social care.
Another strength is that we were able to recruit a sample that broadly reflected the English social worker population. In September 2021, there were 32,500 full-time children and family social workers in England (GOV.UK, 2022), so our sample represents approximately 2%. The sample predominantly identified as female (∼86%), which corresponds with the English national children's social work workforce (87%; GOV.UK, 2022). This also aligns with the international workforce, for example, the USA, where 84.4% of the workforce identified as female (Data USA, 2020). In our sample, 17.4% of participants were of ethnic minorities, which is slightly lower than the proportion in the national workforce (23%; GOV.UK, 2022). Not only was our sample similar to the population, but it was also of a healthy size, especially considering recruitment challenges reported in previous research (Acquivita et al., 2009; Canda et al., 2004) and the lack of research capacity in social workers (Harvey et al., 2013; Wakefield et al., 2022).
There were also some limitations to the present study. First, the sample was self-selecting, which may have led to an overrepresentation of certain groups. We had a greater representation of LGBTQ+ people than is found in the general population, suggesting a greater interest from this population. However, we did find evidence suggesting that the training was similarly effective for participants who had and did not have a connection to the LGBTQ+ community, suggesting that levels of connection did not impact the intervention effectiveness. With regards to our methods, firstly, it could be noted that the time between the pre- and the post-test was not equal across the sample. However, this was a pragmatic RCT, allowing us to test the effectiveness of the intervention under real-world conditions. Second, to assess perceived LGBTQ+ knowledge, we constructed our own scale. Although it was adapted from an existing scale (Gandy-Guedes, 2018) with excellent internal reliability (α = .94), our scale was not validated. The decision for a shorter, unvalidated measure was made to reduce burden on participants. In similar research, LGBTQ+ knowledge gains among helping professionals are typically assessed using non-standardized measures designed by researchers specifically for their training programs that employ multiple-choice, Likert scale, or true–false formats, according to a systematic review (Morris et al., 2019). Lastly, we experienced differential attrition rates across conditions, which could potentially bias the results. Previous research demonstrates that a higher attrition rate in the intervention condition is common (Crutzen et al., 2015), and this does not automatically bias the results (Hewitt et al., 2010). However, it is important to view these findings as initial positive evidence for the effectiveness of the training that should be further solidified in future trials.
This study offers an important building block for future research and provides initial evidence of the effectiveness of the e-learning training module to increase perceived LGBTQ+ knowledge and decrease heteronormative attitudes and beliefs in children's social workers. Our findings follow several recommendations for future research. First, future studies should address the longitudinal effect of the training by administering follow-up measures at several intervals after the post-test has taken place. Second, data could be collected on the impact of the training on social workers’ practice. This could for instance be measured by follow-up interviews or surveys inquiring about changes made to practice as a result of the training. Third, future studies could explore how the training could be optimized for children's social workers. Participants expressed a need for more social work-specific content, which could be co-produced with stakeholders in future work. Fourth, in the following studies, it could be explored how effects of this training extend to other healthcare and educational professions to ensure that LGBTQ+ young people are supported in all environments they encounter. We suggest that such tailoring is likely to improve the effects of these interventions. Finally, we strongly advocate for the increased use of RCTs in social work and social care research. Although adaptions might be required, this study demonstrates it is feasible and contributes to a robust evidence base.
This study's findings show that LGBTQ+ training is an essential first step for improving the knowledge and challenging dominant cis-heteronormative views in children's social care (Schaub, Stander, et al., 2022). As a result, we recommend mandatory and comprehensive training for all social workers in England about the experiences and needs of LGBTQ+ young people, including for pre- and post-qualifying social work programs.
Conclusion
We can conclude that the Stonewall e-learning training module Supporting LGBTQ+ Children and Young People is effective at increasing perceived LGBTQ+ knowledge and decreasing heteronormative stereotypes in children's social workers in England. This study offers an important foundation for the development of effective social workforce training on LGBTQ+ issues. Future research should test the longitudinal replication of these results, as well as optimize the training to make it optimally suitable for children's social workers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Our work was funded by What Works for Children's Social Care. The views expressed here are those of the authors and not necessarily those of What Works for Children's Social Care or the Department for Education (England; grant number 1001929). We are most grateful to all the social workers who participated in this study, as well as our young advisor's committee and stakeholders for their input and feedback.