
Abstract
Solution-focused brief therapy (SFBT) is a strengths-based, collaborative, and future-oriented, clinical intervention that evolved out of the systemic family approaches to therapy in the early 1980s (de Shazer, 1985; de Shazer et al., 1986). SFBT was developed in a community-based, family services clinic, the brief family therapy center (BFTC) in Milwaukee by two social workers, Steve de Shazer and Insoo Kim Berg, and an interdisciplinary group of clinicians and researchers (Lipchik et al., 2012). The BFTC served as a routine practice setting and a training clinic and was on a public bus line providing access for families who were involved in social services systems. Consistent with its origins, SFBT has continued to be practiced across different types of community- based services. While community-based services can be defined in different ways this article defines community-based services as practice settings within a geographical or catchment area that offers a network of non-profit and public, clinical and social services (McLeroy et al., 2003). Clinical services in community-based settings refer to activities undertaken in the community, rather than in institutional settings, to promote mental health (e.g., children and family services agencies, community mental health clinics, probation offices, and educational settings, American Psychological Association [APA], 2015). Community-based services provide clinical interventions to several different types of underserved populations with varying problems and the same was the case for the BFTC where SFBT was first practiced. Children, adolescents, adult clients, and families with different presenting problems such as, family and couple conflicts, child behavioral problems, depression, and substance use were among the cases from the BFTC (de Shazer & Berg, 2002).
The practice and research literature on SFBT offers several examples demonstrating how SFBT was practiced in community-based services. Berg and De Jong (1996), for example, showed how SFBT can be practiced with mandated clients who were involuntary and sent to social workers in family services. Berg (1994) provided instructions on how to practice SFBT in family preservation services delivered in homes with clients from the child protective services. Pichot and Dolan (2014) presented case studies and life lessons for how SFBT can be practiced in the clinical and administrative practices of a community agency serving clients with substance use and behavioral health problems. In a systematic review, Gingerich and Peterson (2013) noted that SFBT is widely used by social workers and other human services professionals because it focuses on strengths instead of problems and is brief as it is usually delivered in six or fewer sessions. In a review of 251 outcome studies, Neipp and Mark Beyebach (2022) analyzed the practice of SFBT in schools and community services and found that over 20% of the studies they reviewed were in some type of community-based setting. Kim et al. (2019b) further summarized the results from eight meta-analyses on SFBT and discussed specific examples of how SFBT was practiced in community-based services. Practice literature and the three independent reviews mentioned here show the feasible use of SFBT as an effective, brief intervention in community-based services. Studies have also concluded that there is a need to study the outcomes of SFBT when practiced within community-based services (Neipp & Mark Beyebach, 2022).
SFBT Practice
SFBT is now practiced globally within psychotherapy, social services, schools, child welfare, and communities-based organizations (Beyebach et al., 2021). According to Abdulla and Woods (2021), the lack of study of SFBT practice techniques in relation to outcomes is a major shortcoming in the empirical studies of SFBT. We found no meta-analysis examining the efficacy of SFBT questions and techniques in community-based services. Studying the outcomes of different types of SFBT techniques has clinical implications, because it may be beneficial to know the numbers and types of SFBT techniques needed to achieve effective outcomes. The study of SFBT techniques also has important implications for how to achieve SFBT intervention fidelity and for the effective training of social workers within community-based services (Yates & Lee, 2021). Founders of SFBT, de Shazer and Berg (2002), argued that it was important to identify specific SFBT techniques so that practitioners and researchers could better understand SFBT and complete rigorous, clinically relevant, and comparative research studies. Four key techniques were identified by the developers of SFBT: (1) asking the miracle question; (2) asking scaling questions; (3) taking a break; and (4) offering the clients compliments followed by a homework task or experiments.
The SFBT treatment manual developed by the Solution-Focused Brief Therapy Association expands upon these techniques (Bavelas et al., 2013) discussing techniques such as, (1) pre-treatment change, (2) difference questions and amplifying differences, (3) relationship questions, (4) coping questions, and (5) exception questions. The manual also discusses the importance of the collaborative therapeutic alliance, the co-construction process—listening, selecting, and building questions and formulations (paraphrases and reflections) from the client's statements, and the focus on building a desired future (Bavelas et al., 2013, p 10).
Past Studies on SFBT Techniques
Past studies compared solution-focused questions to problem-focused questions and these studies found mixed results with some studies favoring SFBT techniques (e.g., Beyebach, 2014; Richmond et al., 2014) and other studies showing equivocal results between solution-focused questions and problem-focused questions (e.g., Neipp et al., 2021). Richmond et al. (2014) specifically found that SFBT improved scores on the outcome questionnaire at intake compared to problem-focused questions. Beyebach (2014) found that SFBT techniques, pre-treatment change, scaling, and negotiating goals had a positive impact on therapeutic outcomes such as goals, expectations, and self-efficacy. Neipp et al. (2021) study found positive results for SFBT questions but also for problem-focused questions. Specific to the SFBT techniques studied, the miracle and exception questions were more effective than problem-focused questions in decreasing negative affects, while scaling questions produced more action steps.
To better understand the SFBT techniques and process, Franklin et al. (2016) performed a meta-summary of 33 SFBT process studies to investigate what techniques are used to achieve outcomes in SFBT. For the purpose of comparisons, these researchers grouped SFBT techniques and processes into four categories to evaluate which techniques had the most empirical support across studies: (1) linguistic and collaborative language; (2) therapeutic relationship and style; (3) strengths and resources, and (4) future-oriented techniques. The most empirical support was found for the language techniques (co-construction process) and the strengths-oriented techniques. However, Franklin et al. (2016) study did not examine SFBT techniques in relation to specific outcomes (e.g., depression, family functioning), which would strengthen existing reviews and current practice literature.
Specific Problems, Populations and Outcomes
Problems and populations have been examined in past meta-analyses and systematic reviews, but previous meta-analyses did not examine the effects of various techniques of SFBT. In a review of 43 outcome studies, for example, Gingerich and Peterson (2013) reported the strongest evidence for SFBT was with adult clients with depressive symptoms where five separate studies used the Beck Depression Inventory to reliably measure outcomes. These authors also concluded that SFBT may be efficacious with adolescents. Reviews within schools show SFBT is effective for psychosocial and interpersonal outcomes where researchers found small to medium effects across different outcomes (Franklin et al., 2022). Health-related psychosocial outcomes have also been studied in medical settings across nine studies showing small effect sizes (Zhang et al., 2017). Other reviews have examined outcomes such as trauma, substance use, and family functioning (Eads & Lee 2019; Franklin & Hai, 2021; Kim et al., 2019a), reporting positive results when analyzing the results from quasi-experimental and experimental studies.
Meta-analyses on SFBT have repeatedly examined internalizing and externalizing behaviors as an outcome but with mixed results and without studying specific problems within those dimensions (e.g., depression, anxiety, substance use). Corcoran (2012), for example, found that SFBT was not effective for externalizing behaviors, but Bond et al. (2013) and Hsu et al. (2021) found statistical support for SFBT's effectiveness for externalizing behaviors, showing small to medium effect sizes, but no support for internalizing behaviors. Kim (2008) and Schmit et al. (2016) respective reviews showed SFBT achieved small effect sizes for internalizing symptoms and behaviors and the Kim study did not yield positive statistical results with externalizing behaviors. Previous reviews and meta-analyses included both experimental and quasi-experimental studies and authors have mentioned limitations for the interpretation of the positive results because of the weaknesses in research designs, small sample sizes, and the lack of precise enough measures to determine specific outcomes, such as grouping different measures together under broader categories (e.g., internalizing disorders). A meta-analysis of randomized controlled studies that includes an examination of SFBT techniques and specific outcomes, such as depression, anxiety, trauma, substance use, family functioning, health, and psychosocial outcomes, is especially clinically relevant and will build on previous reviews.
Study Aims
This study aimed to conduct a meta-analysis of randomized controlled trials (RCTs) on SFBT for adolescent and adult clients that received services in outpatient, community-based settings. Despite the prevalent use of SFBT in community-based services, no meta-analysis has specifically examined the effects of SFBT on outcomes in community-based services or examined the effectiveness of specific SFBT techniques on outcomes. We planned this study to analyze how effective the number and types of SFBT techniques for the outcomes studied. This meta-analysis will especially contribute to the practice literature by examining SFBT across RCT studies on clinically relevant outcomes, such as depression, anxiety, behavioral health, health and wellbeing, family functioning, and psychosocial outcomes. The results of this study will make a unique contribution by providing implications for the efficacious practice of SFBT in outpatient, community-based services.
Methods
Search Procedures
The Cochrane recommendations for searching RCTs were followed for the search process (Higgins et al., 2019), for example, articulating types of participants, intervention, comparison, outcomes (PICO framework), choosing effect measures and computing estimates of effect, and summarizing risk of bias and publication bias. Six electronic databases were searched: PsycINFO, SocINDEX, Medline, Education Resource Information Center (ERIC), Psychology and Behavioral Sciences Collection, and Dissertations and Theses Global. The following keywords and terms were used to search study title, abstract, and keywords: (Solution-Focused OR “Solution Focused” OR SFBT OR “Solution-Focused Brief Therapy” OR Solution-Oriented) AND (random* OR experiment*). In addition, forward and backward searches were conducted to identify potentially eligible studies that were cited by articles and reviews. The database search and the manual search of literature included studies published (for published studies) or completed (for unpublished studies) before October 2018, yielding a total of 2625 records. Due COVID-19 pandemic related delays, we conducted an updated search using the original search criteria for the time period 2018–2021, which yielded another 134 records. This study was registered with PROSPERO (study number: CRD42020163906).
Inclusion and Exclusion Criteria
This review included published and non-published studies from all countries as long as the study report was available in English. Studies in this review met the following preset criteria:
SFBT Intervention. Studies were focused on SFBT, which was identified by the individual studies’ authors by name and through further examination by the research team based on the SFBT therapeutic techniques identified in the studies. We included SFBT therapeutic techniques, such as focusing on strengths, scaling questions, exception questions, coping questions, the miracle question, and other techniques that were identified in the SFBTA treatment manual and that have been defined in previous studies (e.g., Gingerich & Peterson, 2013). Studies that combined SFBT techniques with other therapeutic approaches were included as long as the authors explicated the study's intention was to examine the outcomes of SFBT and described the techniques of SFBT that met the criteria for this review. Sample. Study participants were adolescents, adults, and/or families. This review specifically focused on adolescents and adult populations because other studies have suggested efficacy with these age groups (Franklin et al., 2022; Gingerich & Peterson, 2013). Studies with children 5–10 years old were excluded because the literature on SFBT indicated a need to creatively adapt SFBT techniques to meet the developmental needs of children of this age group (e.g., Berg & Steiner, 2003). Community-Based Services Settings. Studies were included if SFBT was studied in any outpatient setting in the community, such as hospital clinic, social services agency, university clinic, or mental health center. High schools and in-school mental health services were excluded because a recent meta-analysis has been conducted on those studies (Franklin et al., 2022). Research Designs. Only RCTs were included. Different types of comparators and controls were included, such as inactive controls (i.e., no treatment, waitlist control, treatment as usual) and active controls (i.e., using other interventions). Outcome Measures. Studies were included if they focused on any behavioral health, health, family functioning, or psychosocial outcomes. The following definitions were used in this review to categorize the outcomes: (a) Health and Wellbeing Outcomes included health status, adjustment to illness, and indications of wellbeing, such as personal strengths, positive emotion, and quality of life. (b) Anxiety Outcomes included anxiety symptoms and anxiety disorders. (c) Depression Outcomes included symptoms of depression and depressive disorders. (d) Behavioral Health Functioning Outcomes included trauma, substance use, and other general psychiatric symptoms, such as somatization and psychosis. (e) Family Functioning Outcomes included quality of couple and family relationships, communication, conflict resolution, parenting skills, coping, and problem-solving abilities within a family. (f) Psychosocial Adjustment Outcomes included functioning in social roles across different settings, such as health care, living situations, social and interpersonal relationships, and employment settings.
Data Extraction
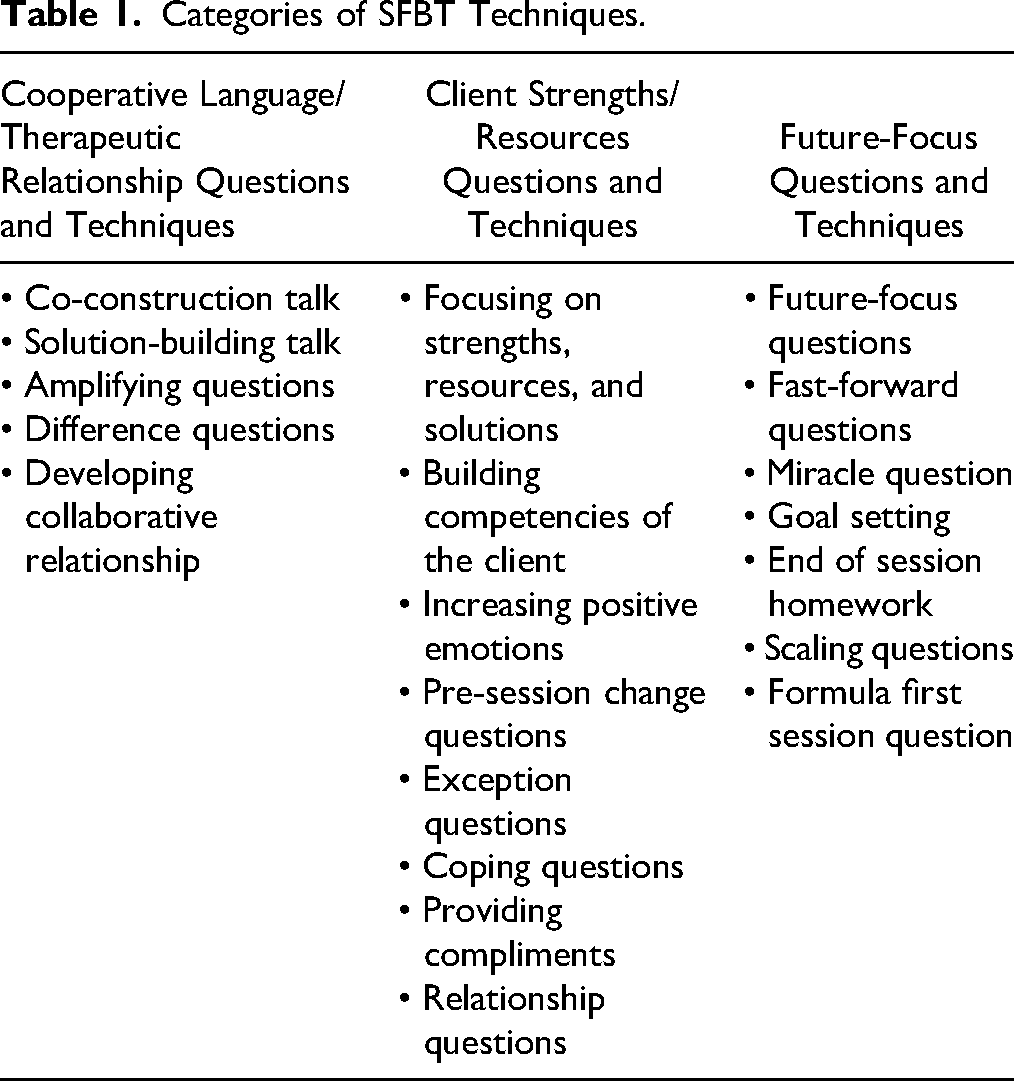
The research team consists of an experienced group of faculty members and doctoral students with expertise in meta-analysis and SFBT. The team developed a coding form based on Cochrane's recommendations (Higgins & Green, 2011) for data extraction and is available upon request. The data extraction form was used to collect information on research design, participant and setting descriptors, intervention descriptors, moderators (i.e., SFBT techniques) and effect size data. SFBT techniques were further categorized using a modified version of the categories used in the Franklin et al. (2017) study (see Table 1 for categories of SFBT techniques).
Categories of SFBT Techniques.
Five studies were originally coded with the form to pilot the coding categories before two coders proceeded with coding. Rayyan, a web and mobile app for systematic reviews (Ouzzani et al., 2016), was used in this review to help expedite the initial screening of titles, abstracts, and full-text articles. Two reviewers independently conducted title and abstract screening and full-text review. The inter-rater agreement rate was calculated by the number of studies with a consensus in a reviewer pair divided by the total number of studies screened and came out to be 97.5%. The two reviewers resolved disagreements through discussion, and if an agreement could not be reached, a third reviewer was consulted. Two coders coded the data independently and separately; hence no formal measures of inter-rater reliability were obtained. Two other coders checked all the data and specifically examined each measure and the SFBT techniques for accuracy in coding.
Risk of Bias Assessment
Two reviewers independently conducted risk of bias assessment using the Cochrane Collaboration's tool for assessing risk of bias in randomized trials (Higgins et al., 2019). Studies were rated with high, low, or unclear risk in seven domains: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, reporting bias, and other bias. Studies were rated as having low other bias (1) when baseline balance was achieved or (2) when baseline balance was not achieved but the imbalanced variables were adjusted in primary analyses. Baseline balance is achieved when participants in treatment and control groups do not differ significantly.
Statistical Analysis
Data analyses were conducted in R statistical software (version 3.5.3), including the metafor and robumeta packages to implement robust variance estimation (RVE) in meta-regression. Other than descriptive statistics of study characteristics, we first calculated standardized mean differences and small sample size corrected Hedges’ g as treatment effect sizes. We encountered a couple of odds ratio effect sizes and converted these into the same metric as Hedges’ g. Specifically for meta-analysis, we first calculated an overall treatment effect size across all outcome domains. Then, we estimated treatment effect sizes for each outcome domain separately (domain-specific subgroup analysis) for the following: health and wellbeing, anxiety, depression, behavioral health functioning, family functioning, and psychosocial adjustment. For moderator analysis, we evaluated “outcome domain” as a potential moderator to evaluate the between-domain treatment effect differences.
In addition, we considered the number of SFBT intervention techniques and categories of SFBT techniques for subgroup and moderator analysis in relation to SFBT's treatment effects. We also considered participants’ demographic and intervention characteristics as potential moderators. However, due to missing data in included studies, these analyses were not feasible.
We selected meta-regression with RVE (Tipton & Pustejovsky, 2015) as the primary analytical framework for a couple of important reasons. First, meta-regression with RVE enables us to include multiple effect sizes from the same study to promote statistical power while effectively accounting for the within-study dependence among effect size estimates. Second, meta-regression with RVE effectively models the variances associated with meta-regression coefficients (i.e., intercepts and coefficients) across fixed- versus random-effects models. As a result, meta-regression with RVE does not require an investigation of heterogeneity among studies (or effect sizes) to pre-determine a meta-analysis model, that is, between a fixed- versus and random-effects meta-analysis model.
Results
Thirty-three publications from 28 studies met study criteria and were detailed in the preferred reporting items for systematic reviews and meta-analyses (PRISMA) diagram (see Figure 1). For the meta-analysis, we combined those publications from the same study, resulting in a final meta-analytical sample of 28 studies. Sensitivity analysis comparing our decision to combine those studies and the alternative decision to separate those publications from the same study revealed very similar findings.
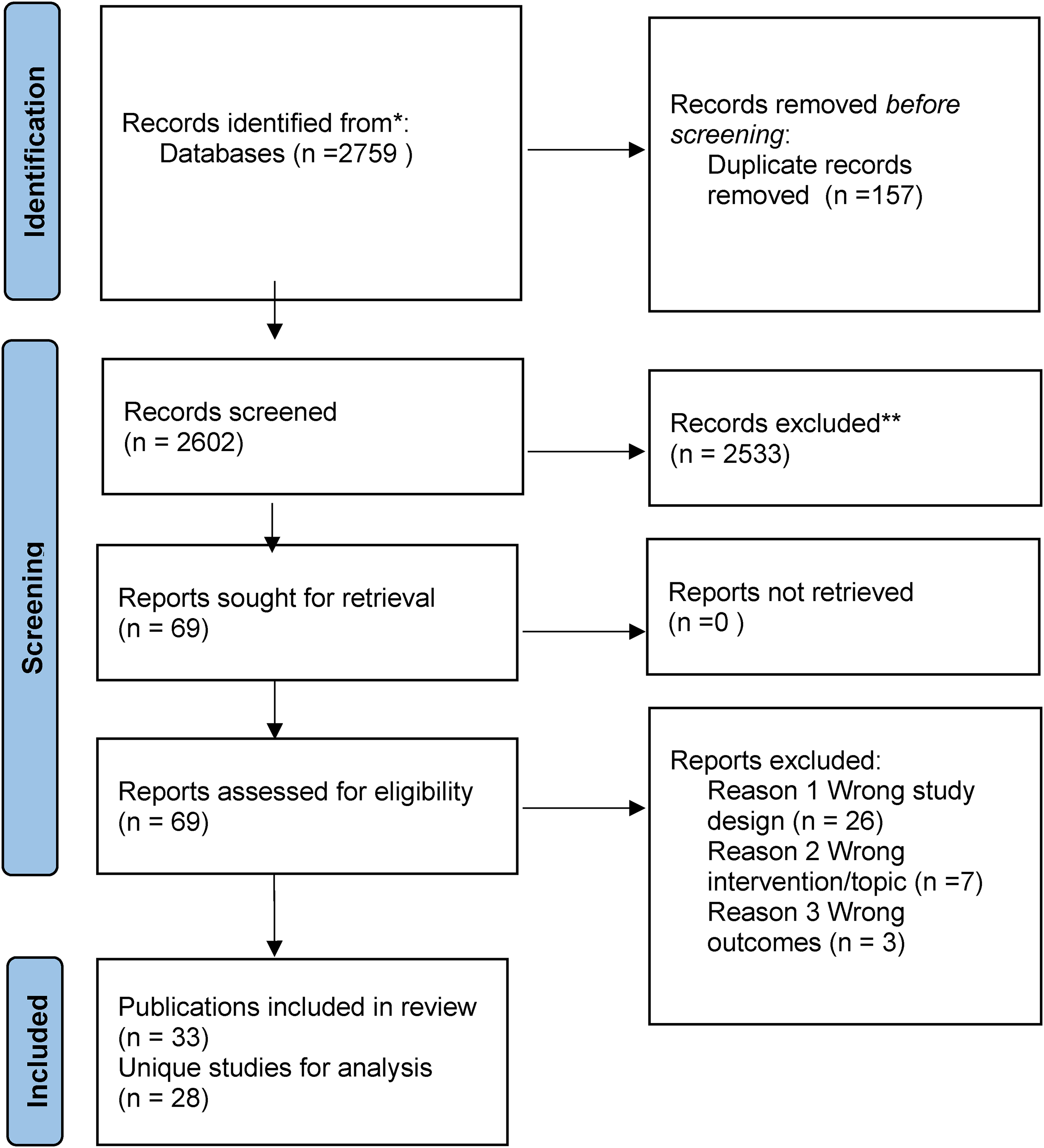
PRISMA diagram.
The average sample size across studies was 72. Across the 28 included studies, 26 reported on participants’ sex, and females accounted for the majority of the included sample (68.25%). Slightly more than half of the 28 studies reported information on participants’ race/ethnicity (n = 15, 53.57%). Of the studies that reported participants’ race/ethnicity, an average of 38.69% of participants were White, 19.12% were Asian, 11.12% were Black, 2.76% were Hispanic, and 28.31% were other races/ethnicities (e.g., American Indian/Alaskan Native, Native Hawaiian/Pacific Islander, mixed race, Iranian). In addition, six studies took place in community services agencies (21.43%), five studies in hospital clinics (17.86%), four studies in mental health centers (14.29%), three studies in university mental health clinics (10.71%), two in social security offices (7.14%), one study in a counseling center (3.57%), one in prison (3.57%), one in a residential program (3.57%), one in a call center (3.57%), one in a probation setting (3.57%), one online (3.57%), and two in unspecified outpatient settings (7.14%).
Risk of Bias and Publication Bias Assessment
Across 28 studies, 50% (n = 14) of the studies were rated as having a low risk of bias in random sequence generation; 35.71% (n = 10) were rated to have an unclear risk of bias; and 14.29% (n = 4) were rated as high risk of bias in random sequence generation. In terms of allocation concealment, 57.14% (n = 16) were identified as having an unclear bias, 28.57% (n = 8) had a low risk of bias, and 14.29% (n = 4) had a high risk of bias. For blinding of participants and personnel, most of the included studies (n = 17, 60.71%) were reported as having a high risk of bias, 21.43% of studies (n = 6), and 17.86% (n = 5) studies were unclear or low risk of bias, respectively. Similarly, most studies (n = 20, 71.43%) reported a high risk of bias in the blinding of outcome assessment; 7 studies (25%) reported a low risk of bias, and one study (3.57%) reported an unclear risk of bias. In terms of incomplete outcome data, 57.14% of studies (n = 16) were reported as having a low risk of bias, 28.57% (n = 8) studies had a high risk of bias, and 14.29% (n = 4) had an unclear risk of bias. Most studies were identified as having an unclear risk of bias in selective reporting (n = 22, 78.57%); 5 studies (17.86%) reported a low risk of bias, and 1 study (3.57%) reported a high risk of bias in selective reporting. Lastly, for other biases, 24 studies (85.71%) were identified as having a low risk of bias, 3 studies (10.71%) had unclear risk of bias, and 1 study (3.57%) had high risk of bias.
Publication bias was evaluated using visual inspection by plotting effect sizes against standard errors, and a reasonably symmetric funnel plot is evidence supporting the absence of publication bias. As shown in Figure 2, the funnel plot is reasonably symmetric, suggesting no strong concern of publication bias. The conclusion of the visual inspection was further supported by the Vevea and Woods sensitivity weight function model by comparing an observed treatment effect size and a theoretical effect size when the funnel plot is perfectly symmetric. The differences between the two effect sizes were not statistically significant, and the likelihood ratio test is statistically non-significant, confirming the visual conclusion that there's no major concern of publication bias.
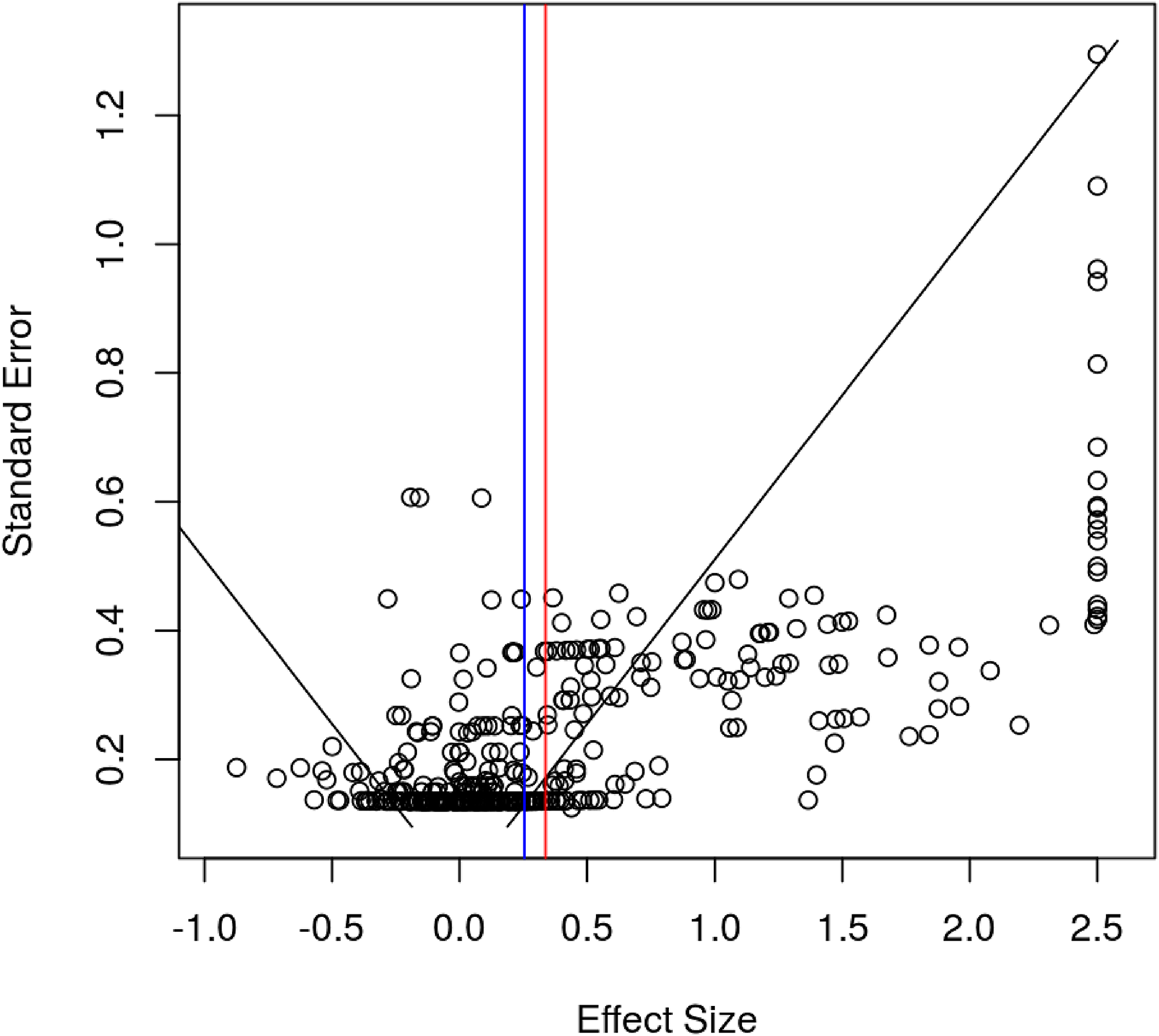
Funnel plot for publication bias.
Meta-Analysis and Subgroup Analysis
Across 28 studies and 340 effect sizes, meta-regression with RVE revealed an overall statistically significant and medium treatment effect size across outcome domains (i.e., depression, anxiety, behavioral health, health, family functioning, and psychosocial adjustment), g = 0.654, 95% CI: 0.386–0.922, p < 0.001. Across outcome domains, participants receiving SFBT on average are expected to have 0.654 standard deviations greater improvement than their counterparts in the control condition, and the difference was statistically significant (see Table 2).
Results of Meta-Analysis Across Outcomes and Within Outcome Domains.
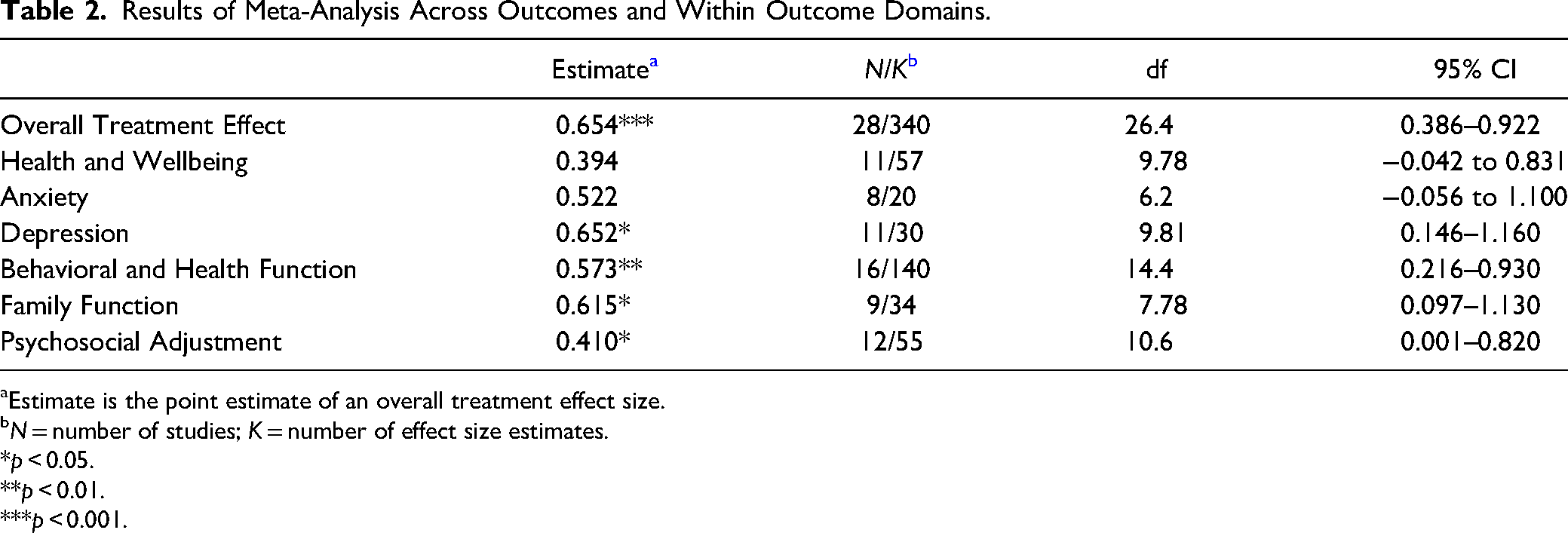
Estimate is the point estimate of an overall treatment effect size.
N = number of studies; K = number of effect size estimates.
*p < 0.05.
**p < 0.01.
***p < 0.001.
Subgroup analysis for specific outcome domains revealed that SFBT was statistically significant with medium treatment effects for depression outcomes, g = 0.652, 95% CI: 0.146–1.116, p = 0.017, behavioral health function, g = 0.573, 95% CI: 0.216–0.930, p < 0.01, family function, g = 0.615, 95% CI: 0.097–1.130, p = 0.026, and psychosocial adjustment, g = 0.410, 95% CI: 0.001–0.820, p = 0.049. In contrast, the overall treatment effect of SFBT was statistically non-significant for health and wellbeing outcomes g = 0.394, 95% CI: −0.042 to 0.831, p = 0.072, and anxiety outcomes g = 0.522, 95% CI: −0.056 to 1.100, p = 0.070.
Outcome Domain as a Moderator
Moderator analysis evaluating the between-domain treatment effect size differences was evaluated using meta-regression with effect size as a dependent variable and treatment category as an independent variable. Outcome domain was not a significant moderator, suggesting no significant differences in SFBT's treatment effect across outcome domains (results not shown in a table due to statistical non-significance).
Number and Category of SFBT Techniques for Subgroup and Moderator Analysis
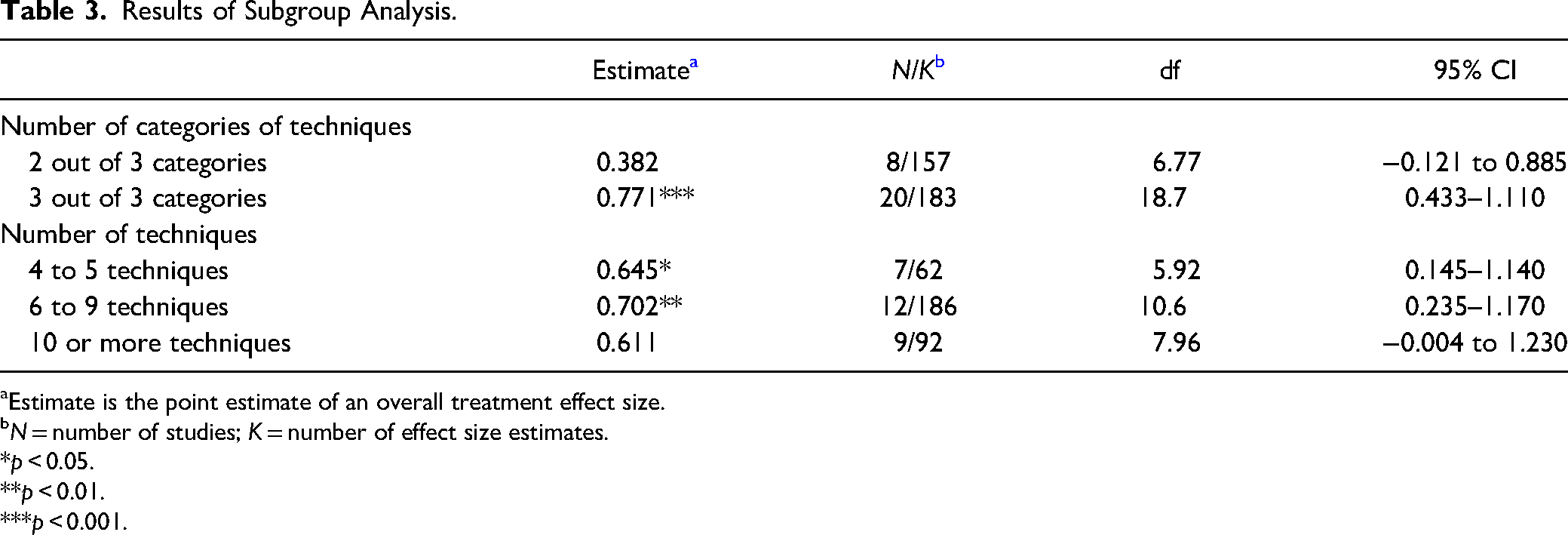
As shown in Table 3, the subgroup analysis findings of the SFBT techniques revealed that SFBT studies that used 2 out of 3 categories of SFBT techniques (see Table 1 for category descriptions) reported an overall statistically non-significant treatment effect g = 0.382, 95% CI: −0.121 to 0.885, p = 0.115, whereas SFBT studies that used all 3 categories of SFBT techniques reported an overall statistically significant and large treatment effect, g = 0.771, 95% CI: 0.433–1.110, p < 0.001. The difference between the two types of studies (i.e., those that used only 2 versus those that used all 3 categories of SFBT techniques) was statistically non-significant.
Results of Subgroup Analysis.
Estimate is the point estimate of an overall treatment effect size.
N = number of studies; K = number of effect size estimates.
*p < 0.05.
**p < 0.01.
***p < 0.001.
In terms of the number of SFBT techniques in relation to treatment effect, an overall statistically significant treatment effect was identified among SFBT studies that used 4 to 5 techniques, g = 0.645, 95% CI: 0.145–1.140, p = 0.019, and SFBT studies that used 6 to 9 techniques, g = 0.702, 95% CI: 0.235–1.170, p < 0.01. However, SFBT studies that used 10 or more techniques reported an overall statistically non-significant treatment effect, g = 0.611, 95% CI: −0.004 to 1.230, p = 0.051.When we evaluated the number of techniques used as a moderator, its moderation effect was not statistically significant.
Discussion
This study examined the outcomes of SFBT with adolescent and adult clients who received services in outpatient, community-based services, analyzing the results from 28 RCT studies across six different outcome domains. The overall results indicated that SFBT had a statistically significant and medium treatment effect size across outcome domains, g = 0.654, 95% CI: 0.386–0.922, p < 0.001 when compared to different types of comparators such as inactive controls (i.e., no treatment, waitlist control, treatment as usual) or active controls (i.e., other interventions). When compared to other interventions, SFBT was mostly compared to CBT and treatment as usual that used eclectic, non-specified interventions (60.71%) or nothing at all (39.29%).
Outcome Domains
An aim of this study was to evaluate specific outcomes so that we can see on what types of problems SFBT has an effect. The results showed that SFBT was effective in four of the six outcome domains, including depression outcomes (g = 0.652, p = 0.017), behavioral health functioning (g = 0.573, p < 0.01), family functioning (g = 0.615, p = 0.026), and psychosocial adjustment (g = 0.410, p = 0.049). The overall treatment effect of SFBT was statistically non-significant for health and wellbeing outcomes (g = 0.394, p = 0.072) and anxiety outcomes (g = 0.522, p = 0.070).
The statistically significant results for depression have been reported in other studies (Gingerich & Peterson 2013). Other meta-analysis studies have also shown small effects for internalizing behaviors that included depressive symptoms, such as Kim (2008) and Schmit et al. (2016). This study makes a contribution by specifically examining depression across the studies thus building on Gingerich and Peterson's review. Gingerich and Peterson (2013) reported the effectiveness of SFBT with adult clients with depressive symptoms in five separate studies and four of these studies found SFBT to be comparable to well-established alternative treatments for depression such as CBT. The effect size in this study approached a medium treatment effect for the depression outcome, adding more evidence for the effectiveness of SFBT. On the other hand, anxiety, another internalizing behavior that is strongly associated with depression and other mental health conditions, did not show a statistically significant treatment effect. This is an interesting finding because some past studies have shown that SFBT is effective with internalizing disorders (Kim, 2008; Schmit et al., 2016) which is presumed to include anxiety symptoms; however, other studies on internalizing disorders in children and adolescents did not show a statistically significant effects (Bond et al., 2013; Hsu et al., 2021). We speculate that the discrepancies across studies have to do with differences in study designs and types of measures and this warrants further investigation.
This study showed an effective treatment effect for the behavioral health outcome domain that included different measures to assess trauma, substance use, and general psychiatric symptoms. The findings of this study build upon other reviews that examined SFBT's behavioral health outcomes (e.g., Eads & Lee; 2019; Franklin & Hai, 2021) and make a contribution to rigor by only including RCT designs. The limitations of the different measurements and small sample sizes within the behavioral health studies reviewed did not allow us to assess specific outcomes (e.g., substance use) as we were able to do with the depression outcome, but the medium treatment effect found in this study shows that SFBT is a promising intervention for behavioral health conditions. The implication is that it may be a useful intervention for clinical work within community mental health settings and deserves further study with more specific measures of behavioral health outcomes.
The positive treatment effect of SFBT for family functioning is an important finding because there have only been a few research studies done on this outcome domain and the studies that have been reviewed have not shown statistical effectiveness for SFBT with couple and family problems (Kim, 2008; Neipp & Mark Beyebach 2022). In contrast to past studies, this study showed a positive treatment effect for the family functioning outcome domain and a medium treatment effect. While these are encouraging results for the potential applications of SFBT for family services, it is important to note that the majority of studies dealt with parenting and the behaviors of adolescents (e.g., Keating et al., 2016; Priebe et al., 2013). The findings from this study thus are consistent with past reviews that indicated that SFBT is a promising intervention with adolescents and families (Bond et al., 2013). At the same time, more research is warranted for other couple and family related problems (Davarniya et al., 2018) given the limited number of studies that have been done on SFBT in couple and family therapy.
The health and wellbeing outcome domain showed a statistically non-significant treatment effect, and this is in contrast to another meta-analysis. Zhang et al. (2017) found a small effect for SFBT in medical settings with health-related outcomes. Some differences between these studies were that the present study was in outpatient clinic settings only and fewer studies were included in the outcome analysis. The health-related constructs in the Zhang et al. (2017) study that found a small effect size also resembled depression and psychosocial outcomes measured in the current study. In the Zhang et al. (2017) study, for example, psychosocial outcomes included health-related depression along with psychosocial adjustment to illness. The health outcome and wellbeing domain in this study included positive emotion outcomes and other indicators of positive wellbeing that have been posited to be important to change in SFBT (Kim & Franklin, 2015). These measures deserve further study because of their significance to the change process and outcomes in SFBT (Neipp et al., 2021). In this study, psychosocial adjustment further showed a positive effect. This builds on other research (e.g., Gingerich & Peterson, 2013) that showed SFBT is an effective intervention in community-based services that involve adjustment to social roles, such as workers’ compensation, job placement, and rehabilitation settings.
SFBT Techniques
This study analyzed the numbers and types of SFBT techniques by grouping techniques into three categories which constitute a modified version of the four categories that were first used in a review of process studies by Franklin et al. (2017). An overall statistically significant treatment effect was identified among SFBT studies that used 4 to 5 techniques, g = 0.645, 95% CI: 0.145–1.140, p = 0.019, and SFBT studies that used 6 to 9 techniques, g = 0.702, 95% CI: 0.235–1.170, p < 0.01. This finding implies that the use of too few SFBT techniques (3 or less) may not be an efficacious way to practice SFBT. On the other hand, the use of ten or more techniques was statistically non-significant in this study. This means that the use of too many SFBT techniques in an intervention may be counterproductive to client change. SFBT has been discussed as being more than its techniques and is a style of therapeutic conversation that uses various techniques to co-construct a preferred future and facilitate client change (Franklin et al., 2017). The results of this study could possibly mean that practitioners who use too many SFBT techniques may be technique-driven without fully understanding how to use the various techniques to support the client's change. A similar finding has been discussed in studies on Motivational Interviewing, for example (Wilson et al., 2018, cited in Yates & Lee, 2021).
The current study indicates a dosage effect of 4–9 SFBT techniques to obtain intervention effectiveness. This finding is important for training, practice, and research because techniques in studies can vary considerably, and this variation has implications for fidelity and the conclusions that may be drawn about efficacy in studies. For example, Abdulla and Woods (2021) concluded that SFBT was not effective in an outcome study based on an intervention using one SFBT technique (i.e., success scaling technique). In the future, researchers need to give more attention to the numbers and types of techniques in the SFBT interventions within outcome studies. Future studies should include multiple SFBT techniques and apply techniques across different categories (i.e., cooperative language/therapeutic relationship questions & techniques; client strengths/resources questions & techniques; and future-focused questions & techniques) to improve the fidelity and effectiveness of SFBT. As indicated, in this meta-analysis, the studies that used all three categories of SFBT techniques reported an overall statistically significant and large treatment effect (g = 0.771, 95% CI: 0.433–1.110, p < 0.001), compared to studies that only used two categories of techniques and did not achieve an effect. This study builds upon Franklin et al. (2017) review of SFBT process studies that showed the significance of the strengths and resources’ techniques and the use of co-construction of meaning in conversations. Moreover, this study also shows that using techniques focusing on the future is essential to client change in SFBT. Future-oriented conversations are strongly emphasized by the SFBTA treatment manual and in past studies and have been identified as a necessary component for a therapy to be considered SFBT (e.g., Gingerich & Peterson, 2013; Kim, 2008).
Limitations of Study
There are several limitations to this review and meta-analysis. First, although the authors made every effort to conduct a thorough search, it is impossible to guarantee that every potentially eligible study was identified during the search process. Second, due to the time and human resources restrictions caused by the COVID-19 pandemic, not all data was double-coded; hence no formal measures of the coding inter-rater reliability were obtained. Third, while authors made best effort to ensure objectivity and rigor, there is always a chance that our findings are subject to human errors during screening and data extraction. Fourth, there is considerable missing data on descriptive information within studies (i.e., race/ethnicity) which limited further moderator analysis that could be completed. While we made considerable efforts to retrieve SFBT intervention technique information from study reports and contacting the authors, the missing data on this variable may have impacted the related subgroup analysis and findings. Finally, overall, the studies had small sample sizes, and there were limitations to fidelity and measurement. As indicated by the results of the risk of bias measure (described in the results section), several limitations to study designs limit the interpretation of positive findings with confidence. This means that the effective outcomes in this study need to be evaluated along with the overall quality of the primary studies. Despite these limitations, this meta-analysis is the first to investigate RCT studies in community-based services and builds on previous research that has shown the effectiveness of SFBT with clinically relevant outcomes.
Conclusion
This study found support for the effectiveness of SFBT when used in outpatient, community-based services with adolescent and adult clients and families. Results showed medium treatment effects for depression, behavioral health functioning, family functioning, and psychosocial functioning from available RCT studies. This study further showed that SFBT is most efficacious when four to nine SFBT techniques are used across three categories of SFBT techniques (i.e., cooperative language/therapeutic relationship questions & techniques; client strengths/resources questions & techniques; and future-focused questions & techniques). The use of three or fewer SFBT techniques or only two categories of techniques did not achieve a statistically significant treatment effect in this study. It is important to build on these findings with other studies with larger samples, better treatment fidelity, and more rigor in RCT study designs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.