
Abstract
Relevant studies demonstrate how an inadequate family background is connected to specific negative outcomes, from attention and behavioral problems to juvenile delinquency (Barylnik, 2003; Hurtig et al., 2005; Simões & Matos, 2008). A 2-year-long longitudinal effort from the US showed that families with high levels of conflict and low levels of positive family relations are linked to poor parental monitoring, an association of adolescents with deviant peers and further engagement in problem behavior (Ary et al., 1999). A recent Finnish longitudinal study found that parental strictness during children's upbringing can eventually lead to higher levels of emotional distress, anxiety, or depression symptoms in adulthood (Kiviniemi et al., 2020). In addition, early experiences of a negatively perceived childhood environment or lack of emotional support are connected to personality disorders such as borderline personality disorder (Vanwoerden et al., 2021).
Similarly, lower socioeconomic status of families and poverty affect children in various negative ways. Studies demonstrate that low socioeconomic status has an impact on the development of children, their literacy, school performance, reading skills, aggression, or internalizing behaviors (Dolean et al., 2019; Duncan & Magnuson, 2012; Letourneau et al., 2013; von Stumm et al., 2022). In particular, crowding of the home environment or high levels of disorganization in the home environment is associated with the overall cognitive and behavioral development (Evans, 2006; Ferguson et al., 2013; Liddell & Kruger, 1987, 1989; Wachs & Çorapçi, 2003). Long-term exposure to high levels of disorganization in the home environment is associated with less scholastic achievement, slower socioemotional development, internalizing problems, early depression, learned helplessness, and low self-regulation (Ackerman & Brown, 2010; Evans et al., 2005; Fiese & Winter, 2010). Children need a secure structure and predictable surroundings (Ferguson et al., 2013).
Importantly, as there is a moderating effect of socioeconomic risk on the link between chaotic home environment and parental executive functioning (Deater-Deckard et al., 2012), it is also clear that home environment and socioeconomic background hold important psychological influences on parents. We are convinced that it would be especially the factors regarding parents and their behavior that have important implications for an overall healthy development of children and that can prevent the growth of children's problem behavior (Eddy et al., 2014). Educated parents who engage in activities such as reading books and newspapers stimulate their 3- to 4-year-old children with more familial activities than their counterparts with less “cultural capital” (Becker, 2014). In particular, it would be specific parental activities such as reading to children, the use of complex language, care, and warm relationships represented in parent-child interactions, that facilitate healthy children's cognitive development (Bradley, 2002). As early cognitive development is linked to children's externalizing behaviors and their understanding of emotions (Guajardo et al., 2009), it appears that the development of children in cognition and behavior are closely related.
Early Childhood Interventions Through Parenting Programs
A UK longitudinal survey study of parents and children demonstrated that developmental and family risk factors emerging by three years of age can, to some extent, predict different trajectories of misconduct throughout childhood (Staff et al., 2015). We agree with the notion that conduct disorders or problematic behavior in children have important implications for both individuals and their well-being and society and associated costs (Baker, 2016, Welsh et al., 2008). Therefore, one of the main goals of training in parenting programs resides in the prevention of child behavior problems or delinquency, and at the same time, in promoting health and well-being in families (Cordova et al., 2014; Lachman et al., 2016, 2018; Piquero et al., 2008).
There is strong evidence of 50 years of research into behavioral family interventions mapping the long-term effectiveness of such programs for children with high levels of misconduct (Farrington & Welsh, 2007). The earlier the intervention is introduced, the higher probability that it will be effective (Allen, 2011; Farrington & Welsh, 2007). Scholarly research demonstrates that between the ages of three and ten, children's behavioral difficulties can be easily identified, attended and modified (Hutchings & Gardner, 2012). Thus, we would expect intervention programs focused on strengthening parental competencies and positive child-rearing practices in families with small children to be the most effective at reducing children's misconduct.
As studies have also demonstrated a link between the poor learning ability of children and a lack of parenting skills (Hutchings & Williams, 2019), we claim that early childhood development is preconditioned by the factors in the family environment, where child–parent communication and parenting style have a major influence. Positive parenting practices such as spending time with a child in joint activities, monitoring, structuring the child's time, and constructive discipline have been associated with a reduction in the child's misconduct despite other influencing factors (Forgatch & DeGarmo, 2002). Even small-scale interventions connecting parents with their children, and engaging them in mutual activities, can lead to improved child–parent relationships, promote desirable and reduce undesirable behaviors in children (Cluver et al., 2017; Lachman et al., 2016, 2018).
For some time already, parenting programs aimed at training parents in effective child-rearing methods have been developed (Forehand & Long, 1996; Patterson, 1982; Thomas & Zimmer-Gembeck, 2007; Webster-Stratton and Herbert, 1994). Patterson's program proved effective when reducing antisocial behavior over short periods in small-scale studies (Dishion et al., 1992; Patterson et al., 1982, 1992). Randomized control trials in Australia have provided evidence of the effectiveness of the Australian Triple P (positive parenting program) used in both individual and group settings (Thomas & Zimmer-Gembeck, 2007). However, it would be especially Incredible Years parenting program that proved effective in reducing disruptive child behavior and in increased use of incentives and praise for socioeconomically disadvantaged families in particular (Leijten et al., 2017).
In the Czech Republic, socially disadvantaged families are at least limitedly provided with certain services, such as financial or housing assistance. However, less attention is paid to strengthening the relationship between parents and children. As the negative outcomes of the development are often connected to disadvantaged family environments or low socioeconomic status, we think that the focus of parenting programs on disadvantaged families is instrumental. To strengthen the parenting competencies through an innovative form of support, we introduced professionally moderated parenting groups based on the collaboration of research institutions in the “Pooling Study of Parenting for Lifelong Health” and the methodology of “Parenting for Lifelong Health for Young Children program” (Hutchings & Williams, 2019).
Presented Evaluation
Hutchings and Williams (2019) summarized the key components of effective behavioral family interventions based on the long-term research of parenting programs: (1) New parenting skills must be actively rehearsed; (2) Parenting programs must teach principles rather than prescribe techniques; (3) Parents must practice new skills at home; (4) Programs should include nonviolent sanctions for misconduct as well as strategies to develop positive relationships through time together, play, and praise (Hutchings & Williams, 2019).
The above-described principles were incorporated into the Parenting for Lifelong Health for Young Children program manual referred to in the following chapter. Through the impact evaluation of the “Parenting Program for Disadvantaged Families,” we aimed to verify whether the intervention of an evidence-informed, locally adjusted parenting program based on the manual of Hutchings and Williams (2019) for socially disadvantaged families in the Czech Republic has been successfully translated into the anticipated and measurable results.
Research question was specifically aimed at determining whether the intervention provided with trained social workers, based on the theoretical and methodological approach given by “Parenting for Lifelong Health for Young Children,” was successful in increasing in the overall level of self-reported parenting skills, parent-reported children's behavior and in its exploratory part—curtailing the use of physical punishment. The quantitative impact evaluation employed a quasi-experimental design with two groups: a treatment and a control group.
Evaluation Design, Sample, and Program Description
Evaluation Design
The evaluation design aimed to be as close as possible to the experimental design with the possibility of comparing the treatment and control groups. The evaluation study was conducted alongside a small-scale controlled trial that examined the preliminary effectiveness of the intervention with socially disadvantaged families with children aged 3–9 years. Data from this study were used to expand the calibration sample of one of the psychometric models (see the “Method” section). The treatment itself was conducted by 13 social workers from partner organizations in two regions of the Czech Republic. Similarly, as in other countries involved in the pooling study, the social workers willing to participate underwent training in providing parental skills support to their clients and group facilitation. The training was attended by 3–5 member teams from each cooperating organization. In collaboration with social workers, families with children aged 3–9 years were invited to join the intervention. These are referred to as the treatment group of families.
Control group families include partner organizations’ clients that have been supported by other colleagues but were not involved in the treatment themselves. These social workers have not been trained or supervised to support their ability to aid with parental skills in client families. Thus, families in the control group are, by nature, similar to treatment families because they are clients of the same social services organizations but have not been included in a parenting treatment group. Participants were assigned at a 1:1 ratio to a treatment or control group, but not in a random manner, as the families were selected by social workers themselves. The control group received no active treatment during the trial.
Setting
This study was conducted from November 2020 to April 2022 in four localities (Vsetín, Zlín, Roudnice nad Labem, and Krupka) in two regions in the Czech Republic—Ústecký region and Zlínský region. These localities are considered socially excluded or at risk of social exclusion (Čada et al., 2015). Social exclusion is defined as the gradual and escalating exclusion from full participation in the social, material, and symbolic resources produced, shared and consumed by the general society to ensure welfare, the organization of social life, and participation in decision-making (Čada et al., 2015).
The share of people at risk of poverty or social exclusion in the Czech Republic is 14.6% (the aggregate indicator of social exclusion includes three items: the risk of income poverty rate, the material deprivation rate, and the low work intensity rate). Approximately 1.5 million people are at risk of poverty or social exclusion in the entire Czech Republic, including almost 100,000 children under the age of six (Čada et al., 2015). Moreover, comparative studies of education systems demonstrate that it is extremely difficult to escape poverty, even for those generations growing up in it. In addition, according to the Czech School Inspectorate, the Czech education system does not provide equal educational opportunities, and pupils’ outcomes are largely influenced by the social status of their parents (Česká školní inspekce, 2014).
Participants
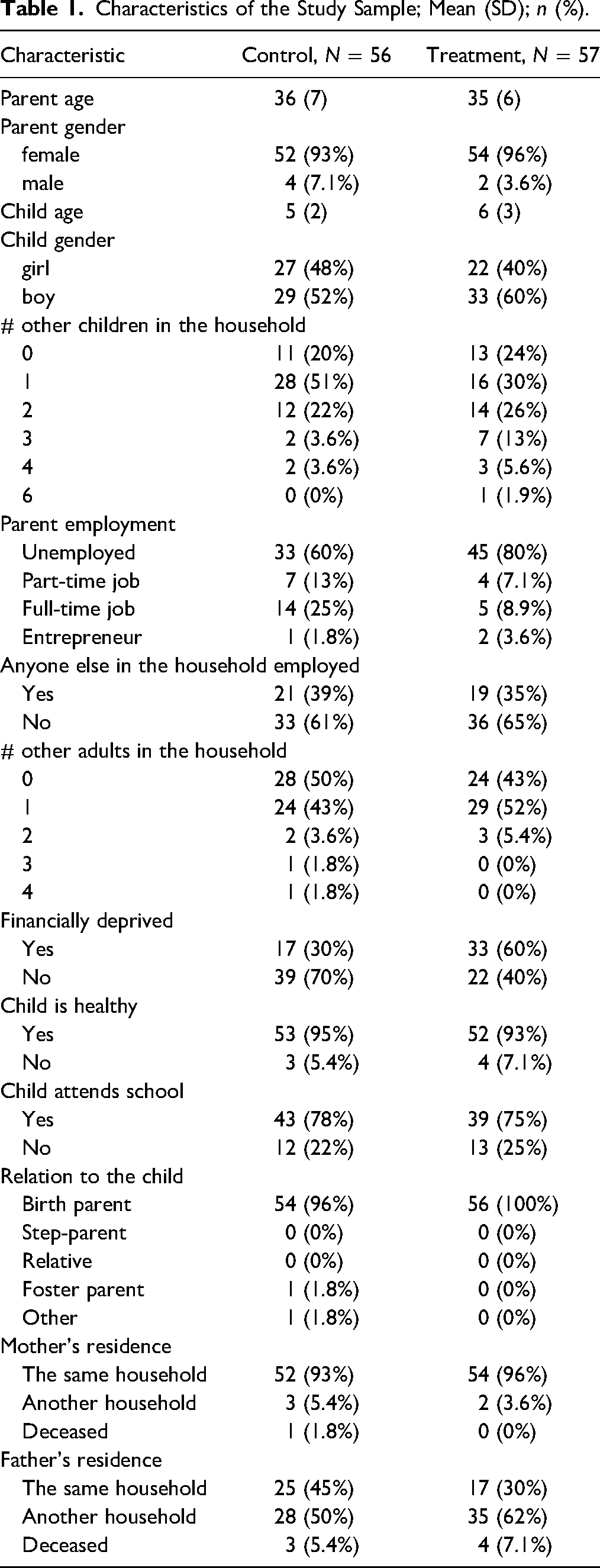
There were 56 parents in the treatment group and 57 parents in the control group recruited among the clients of social services of involved organizations as described above. Inclusion criteria required parents to be (a) living in socially excluded or at risk of social exclusion localities, (b) aged 18 or above, (c) the primary caregiver of a child between the ages 3 and 9, and (d) a resident in the same household as the child. Participating families were from highly vulnerable populations; most were recipients of social benefits living in unsatisfactory flats or shelters. See Table 1 for further details.
Characteristics of the Study Sample; Mean (SD); n (%).
Parenting for Lifelong Health for Young Children (PLH Kids) Program
The Parenting for Lifelong Health for Young Children (PLH Kids) Program is part of a larger initiative called Parenting for Lifelong Health (World Health Organization, 2022). Its objective is to develop and test a suite of effective, feasible, culturally relevant, and scalable parenting programs (Lachmann & Hutchings, 2018).
The PLH Kids referred to in this paper is a group-based parenting program for families with children aged 2 to 9. The program was initially tested in South Africa. PLH Kids and its adapted versions have also been implemented in the Democratic Republic of Congo, Kenya, Macedonia, Moldova, Montenegro, the Philippines, Romania, South Africa, South Sudan, Thailand, and Uganda. The current study is based on data from the pilot study of PLH Kids parenting group interventions with 57 families in three regions of the Czech Republic.
Program Content
The program promotes parenting practices and behaviors that build the skills of parents or caregivers to interact positively and provide adequate support and care to their children. It has been designed specifically for vulnerable families facing challenges with their children's behavior with the goal of promoting positive parenting to reduce the risk of child abuse and neglect in low-income communities (Lachmann & Hutchings, 2018). The main theme is “Building a Home of Support for Parents and Children” (Figure 1). Helping parents build a home of support for themselves and their children helps parents manage their children's behavior while promoting healthy parent–child relationships (Lachmann & Hutchings, 2018).
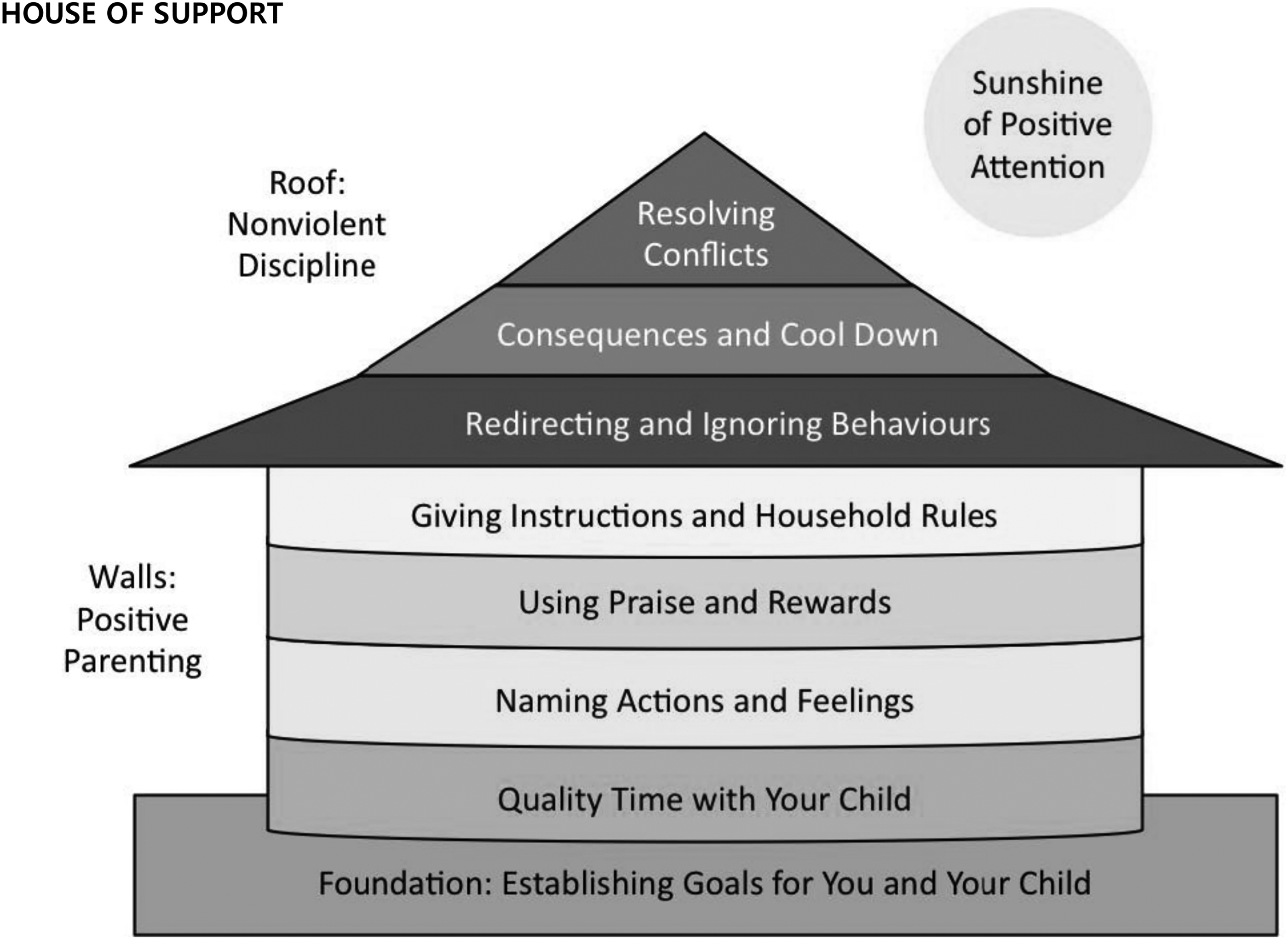
“Building a house of support” program model. Source: Lachmann and Hutchings, 2018. Parenting for Lifelong Health Program for Young Children–Facilitator Manual.
PLH Kids uses an analogy of home to demonstrate why it is important for parents to build a strong, positive relationship with their children. The foundation of the home is a symbol used for the definition of parents’ goals in communication with children and the improvement of parent–child relations. The parent's goal should be realistic, clear, and achievable. It should stem from the parents’ needs and hopes. The walls are the most important and constitute the strength of the house. They include positive parenting strategies such as spending dedicated time with children, building language skills, talking about feelings, praising and supporting good behavior and symbolize positive, and healthy parent–child interactions. The roof of the house symbolizes setting limits, establishing house rules, and dealing with difficult child behavior: “If the foundation and the walls of the house are strong, the roof is easier to maintain” (Lachmann & Hutchings, 2018). Finally, the house is enlightened by the “Sunshine of Positive Attention,” which symbolizes the importance of children receiving as much positive attention as possible from their parents.
Program Design
PLH Kids has the following components: (1) a pre-program home visit to identify the needs of parents and establish the goals the parents hope to achieve during the program; (2) 12 group sessions on parenting skills (ideally 12–15 participants per group, sessions delivered either weekly or every other week covering one or more of the 12 sessions); (3) individual in-home sessions for families requesting or needing additional support (when feasible); (4) a final celebration or graduation ceremony at the end of the program (Lachmann & Hutchings, 2018).
Each session has a similar structure in which a facilitator and co-facilitator guide parents through a series of activities along a core central theme. While the content might vary from week to week, the core activities remain the same. Sessions always start with welcoming activities and then move on to home practice discussions followed by introducing the new topic lesson on core parenting skills (e.g., say what you see). Then, parents are guided through illustrated stories or scenarios demonstrating parenting practices either correctly or incorrectly (Figure 2). Next, the parents practice these skills in role-play. Each session ends with a new home activity assignment for each parent, followed by the closing ritual (Lachmann & Hutchings, 2018).
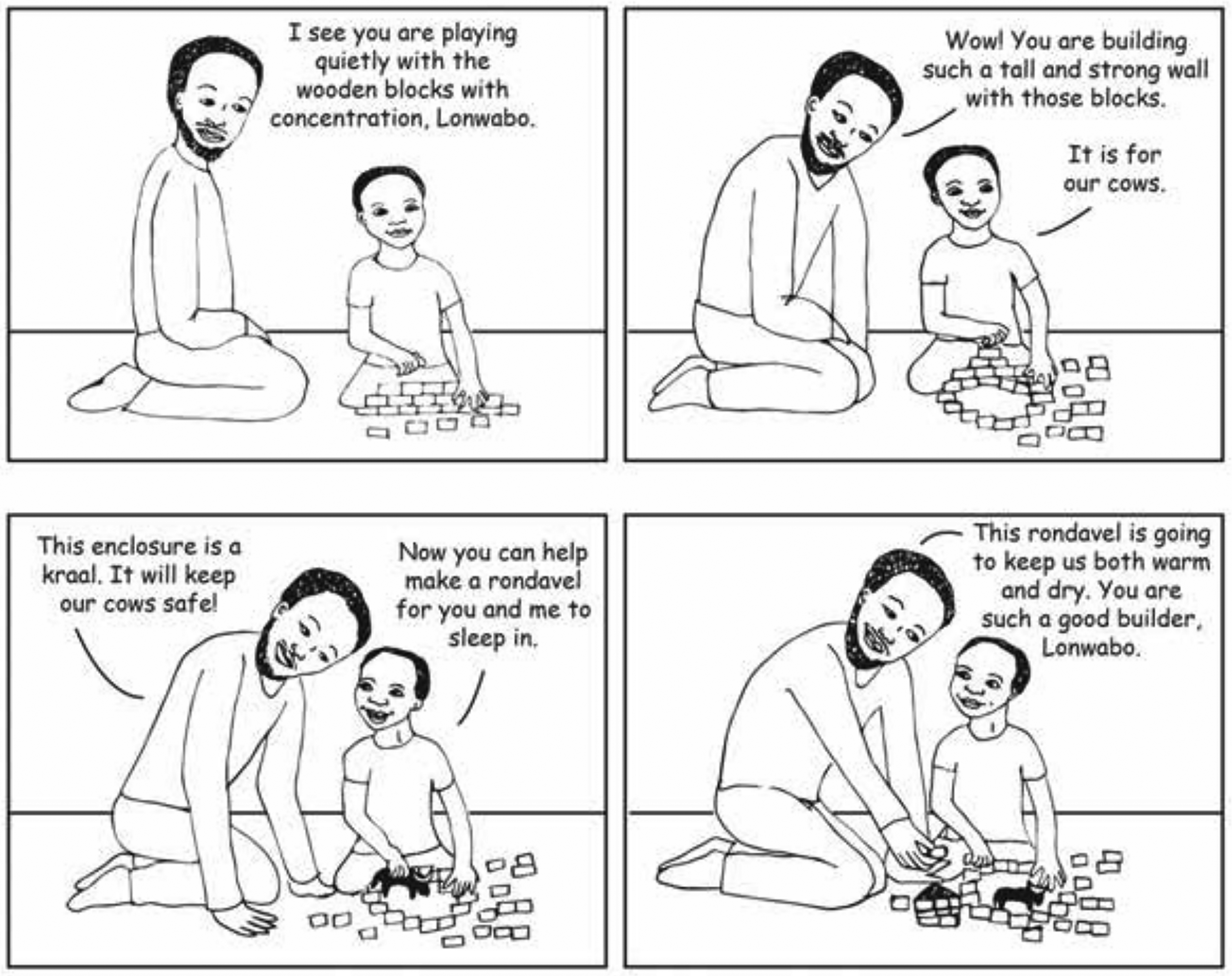
Example of an illustrated storyboard with Lonwabo's (boy's) father taking a more collaborative approach to Quality Time with his child. He allows Lonwabo to take the lead and “Says what he sees” by using words to describe the actions. Source: Lachmann and Hutchings, 2018. Parenting for Lifelong Health Program for Young Children–Facilitator Manual.
The facilitator of the program should ensure that parents practice the new skills and ways of doing things because evidence from similar parenting interventions has proven that the most important aspect of learning new methods and strategies is practicing them at home.
Program Delivery
The scalability of the program was ensured by the detailed facilitator manual providing guidance to the group leaders (social workers, therapists, and lecturers). Before the start of the program, group leaders had to attend intensive initial training (40 h) in program delivery and the supervision of the facilitation (4 × 2 h), both provided by the expert team of SCHOLA EMPIRICA, z. s. in close collaboration with one of the authors of the program manual—Prof. Judy Hutchings.
In addition, facilitators received training in establishing parenting goals around child behavioral outcomes (3 h) as well as practical training in group facilitation (6 h). Facilitators also participated in monthly intervention sessions that involved the identification of challenges experienced while delivering the program, problem-solving, and sharing good practices with the program delivery in different localities.
To support the implementation and motivation of participants, facilitators were provided with additional information enhancing their skills to engage parents in the behavior change process, e.g., weekly text messages that served as boosters to remind parents of home practice activities and encourage active participation during the sessions. Facilitators also carried out home visits or online consultations to support parents who were having difficulties joining some of the group sessions.
Method
The research questionnaire for the quantitative part of the evaluation was developed in collaboration with the PLH research consortium under the international pooling study that collects and analyses data from programs similar to the one evaluated in this report. The study is being led by Professor Lucie Cluver of the University of Oxford and Professor Cathy Ward of the University of Cape Town. Based on the cooperation and experience with previous evaluations, the following tools for impact evaluation were selected: (1) Parenting Young Children (PARYC; McEachern et al., 2012) questionnaire, which measures behavior in the parental role via self-report (two of the three subscales of this questionnaire were used); (2) Strengths and difficulties questionnaire (SDQ; Goodman, 1997), by which the parent assesses the child's behavior; (3) in addition to these two standardized instruments, items regarding child punishment, and several other were used to provide a general description of the households. Apart from the PARYC and SDQ, we also describe how the use of punishment changed in time and between the treatment group and the measurement wave. However, this part is considered exploratory.
Parenting Young Children (PARYC) Questionnaire
The original PARYC questionnaire contains 21 items that measure parental role performance in three dimensions (each measuring seven items): Supporting Positive Behavior, Setting Limits and Proactive Parenting. Based on the recommendation of the PLH research consortium, the items for the first two factors mentioned were used in this study. The factor-analytic reliability estimates
Strengths and Difficulties Questionnaire (SDQ)
The SDQ is a short screening questionnaire dedicated to 3- to 16-year-old children or adolescents. It is an informant-reported (usually by a parent or a teacher) instrument. We used the paper-based parent form of the SDQ with a body of 25 items measuring five behavioral dimensions. The first four dimensions (Emotional Symptoms, Conduct Problems, Hyperactivity/Inattention, and Peer Relationship Problems) are formulated as negative, which in practice means the lower the value, the better the behavior. The last dimension (Prosocial Behavior) is designed to be positive, so higher values are better.
Quantitative data were collected in two waves—the first wave took place before program delivery (baseline) during an individual meeting between a parent and a social worker, and the second at the end of the program after completing the 12th parenting group session. Parents from the control group were also interviewed at similar time points. The factor-analytic reliability estimates
Estimates of Latent Traits
To obtain estimates of children's socioemotional skills (SDQ) and parental behavior (PARYC), we followed the item response theory (IRT) paradigm. Since the responses were recorded using Likert scales, and both SDQ and PARYC comprise multiple dimensions, we opted for the multidimensional extension of the graded response model (MGRM; Muraki & Carlson, 1995) to estimate the factor scores of both children and parents. Models were estimated using the mirt package (Chalmers, 2012) in R (R Core Team, 2022). We applied the robust Metropolis-Hastings Robbins–Monro algorithm (Cai, 2010) with the dimensions allowed to covary. Regarding the estimation of the factor scores, we employed the maximum a posteriori estimator (MAP) using a quasi-Monte Carlo integration (because of the multidimensionality).
For SDQ, we fitted the MGRM to 2,603 response patterns obtained in our previous research. For 1,504 children, the age was known (M = 4.35; SD = 1.03), and of 2,574 children with the gender identified, 49.78% were girls. SDQ measures should be invariant in terms of gender, age, and development (Murray et al., 2021). The calibration sample was recruited from a general population without any regard to socioeconomic status of the children's families, so the estimated latent trait (factor score, theta) of zero refers to an “average” child. As usual, the standard deviation of all factor scores is 1.
For the PARYC, the MGRM was calibrated on data from this and one other similar study that we conducted. Responses from the first wave of both were used to calibrate the model (total N = 208; Mchild age = 5.43; SDchild age = 2.36; 40.49% girls; Mparent age = 34.91; SDparent age = 7.00; 97.07% female). In contrast to the SDQ, the calibration sample is not “average” by any means, and its sociodemographic properties follow those described in Table 1.
Testing the Intervention Effect
A linear mixed model (LMM) was used in the study, mainly to properly model the dependent observations “within” each family. Only random intercepts were estimated due to the sample size, accounting for the differences in the families. For the fixed effects, all dimensions of SDQ and PARYC (analyzed separately) were dependent variables in the model. The independent variables can be divided into two parts: (1) interaction between research group and measurement wave (to test the hypothesis whether the groups differ in the development of the selected latent traits); (2) confounding variables we want to control for, which are, for all models we fitted, the age of child in baseline wave, age of parent in baseline wave, sex of child, sex of parent, number of other children in household, number of other adults in household, job of parent, employment status of other persons in household, financial deprivation, health of child, school attendance and relationship to child. Despite the large number of covariates, multicollinearity was not a problem in any model. Concerning the other assumptions, residuals in all models were checked graphically and there was no deviation from normality, except at the very end of the tails.
Dealing with the omnipresent error affecting latent variables measurement, each observation was weighted by the normalized standard error of the latent trait estimate during LMM fit (Grimm et al., 2021; note that the conclusions are the same for unweighted data). To compute the p values, we used the Satterthwaite degrees-of-freedom approximation as implemented by the lmerTest package (Kuznetsova et al., 2017). The significance level was set to .05.
In terms of hypotheses, we test that the interaction term between the treatment group and measurement wave is different from zero, for all factor scores of PARYC and SDQ. In other words, we test whether there was a statistically significant difference in parental self-reported competencies and parent-reported children's behavior for the treatment group.
Results
Results from PARYC Measurement
Table 2 presents the descriptive statistics of the PARYC dimensions for both study groups per each of the two waves. For both dimensions, we tested the hypothesis that there is a non-zero interaction term of measurement wave and study group. In what follows, we present the coefficient being tested, the 95% CI, the test itself, and an approximation of the effect size: for Setting Limits b = 0.35, 95% CI [0.03, 0.68]; t(82.46) = 2.15, p = .034,
Descriptive Statistics of PARYC Dimensions per Study Group and Measurement Wave; Mean (SD).
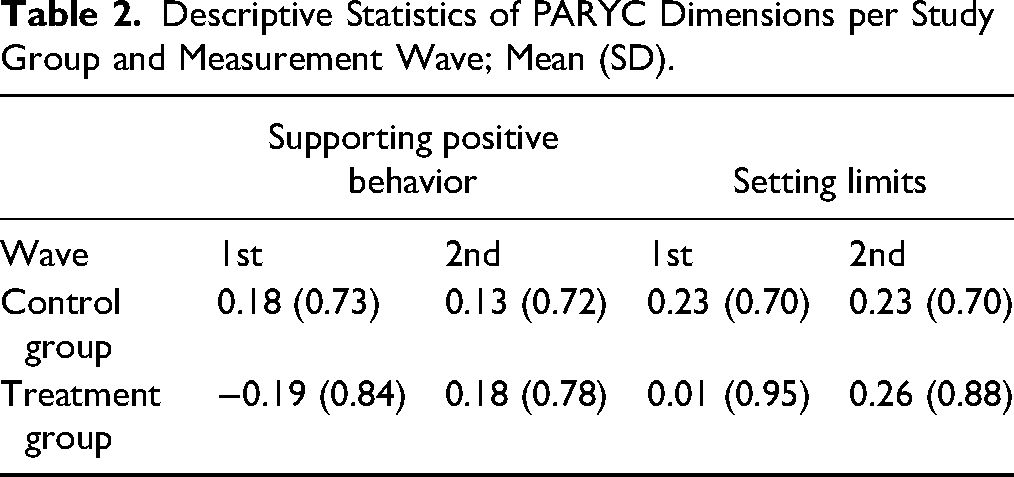
Regarding parenting behavior, in both areas, the treatment group experienced a significantly higher positive shift than the control group. While the values of the control group hardly changed over time, the treatment group evolved significantly toward positive values (Figure 3). A reader may note the different baseline positions of the intervention group, especially in Supporting Positive Behavior. However, our interest aimed specifically toward testing the difference in the development of the groups.
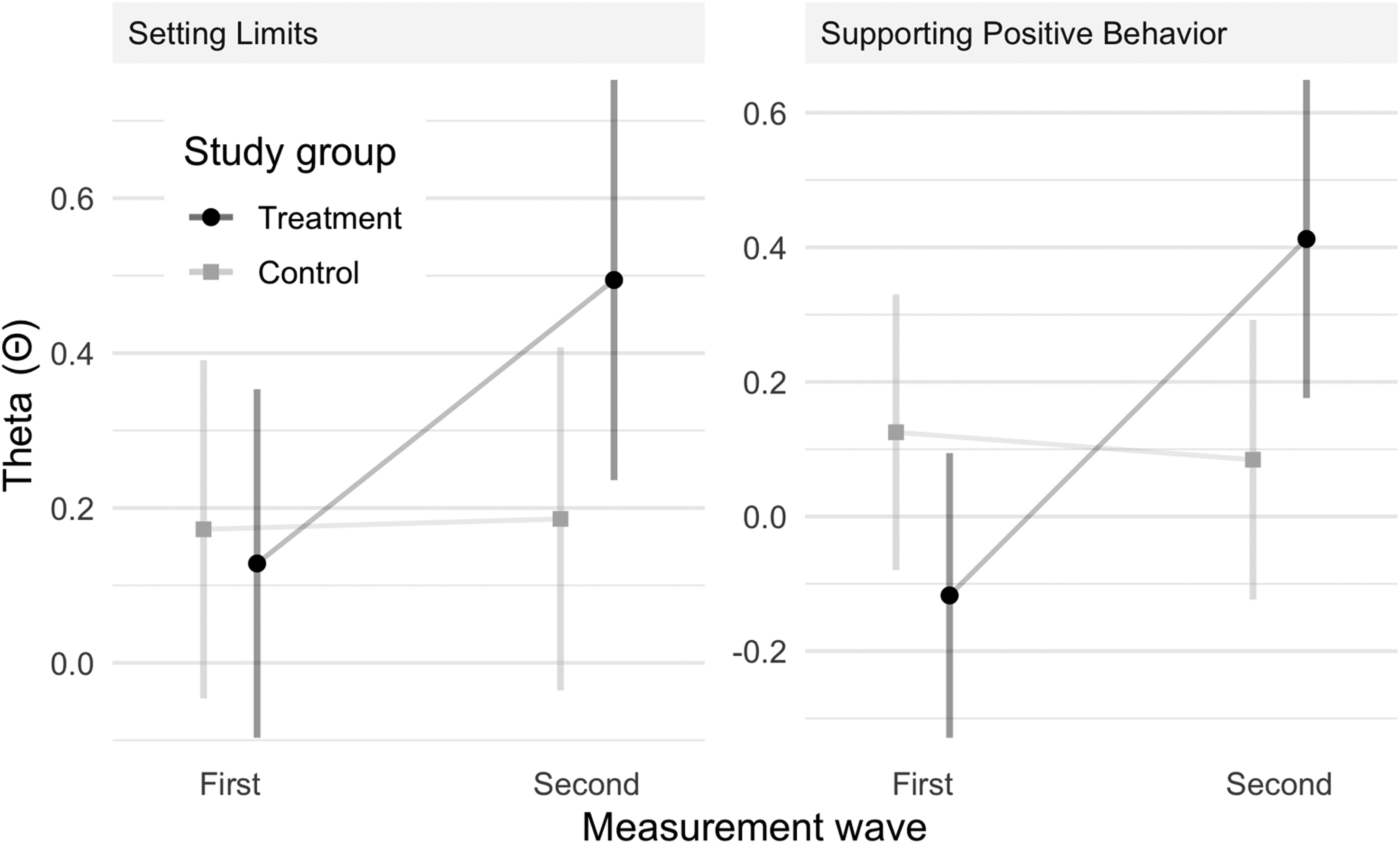
The development of PARYC factor scores in both groups between the measurement waves. The vertical bars refer to 95% CIs around the marginal means.
Results from SDQ Measurement
Table 3 presents the descriptive statistics of the SDQ dimensions for both study groups per each of the two waves. For all SDQ dimensions, we tested the hypothesis there is a non-zero interaction term of measurement wave and study group: for Emotional Symptoms b = −0.42, 95% CI [−0.67, −0.16]; t(79.34) = −3.27, p = .002,
Descriptive Statistics of SDQ Dimensions per Study Group and Measurement Wave; Mean (SD).

As with parental behavior, the socioemotional skills of the children from the treatment group themselves developed statistically significantly better in all areas than those of the children in the control group. Figure 4 shows the marginal means for both groups and both measurement waves. Even within the SDQ, we can see, similar to the results from PARYC, that the control group almost stagnates over time, while the treatment group decreases in the negative areas and increases in the positive area.
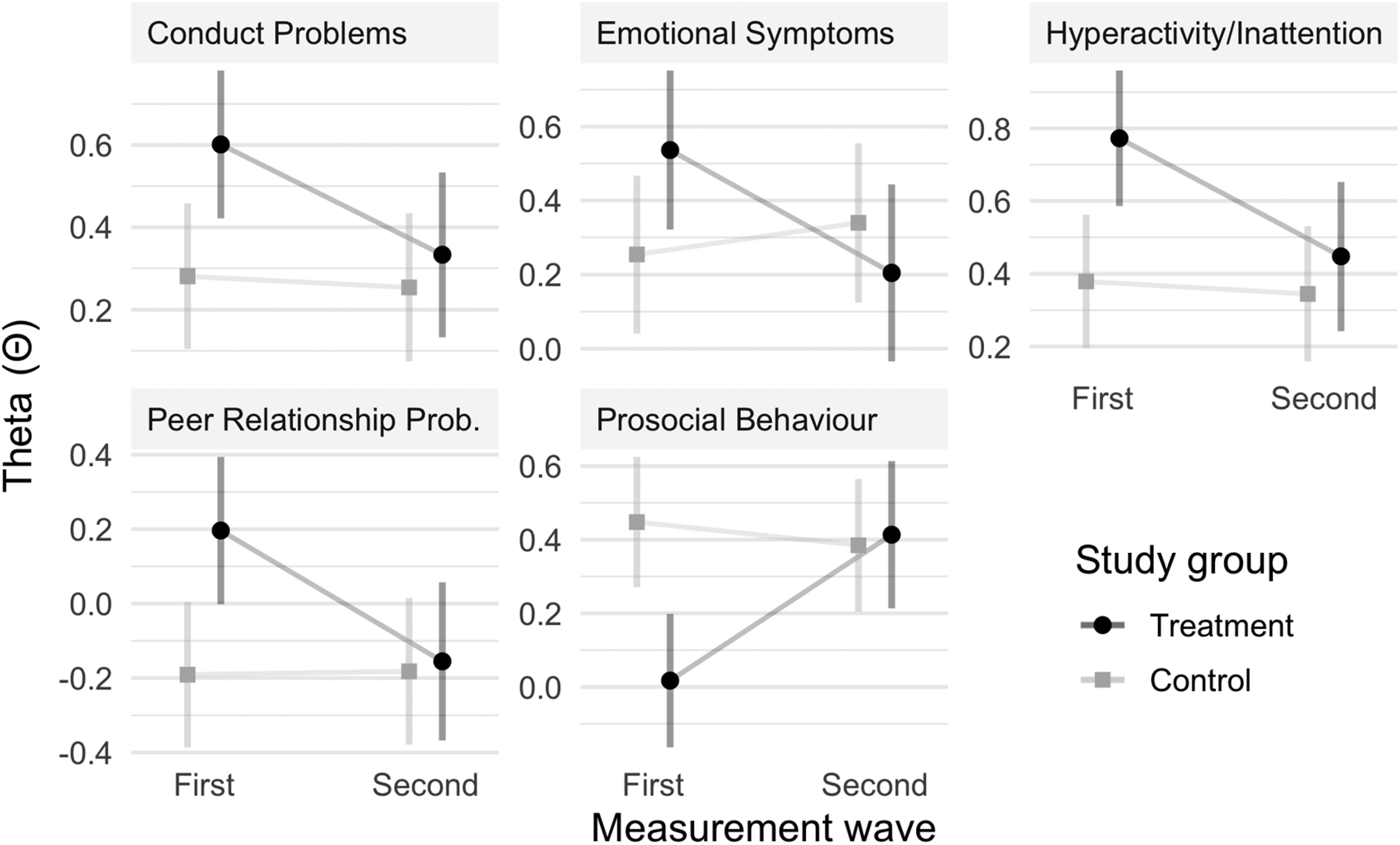
The development of SDQ factor scores in both groups between the measurement waves. The vertical bars refer to 95% CIs around the marginal means. Note that for the first four SDQ dimensions, the smaller the value is, the better.
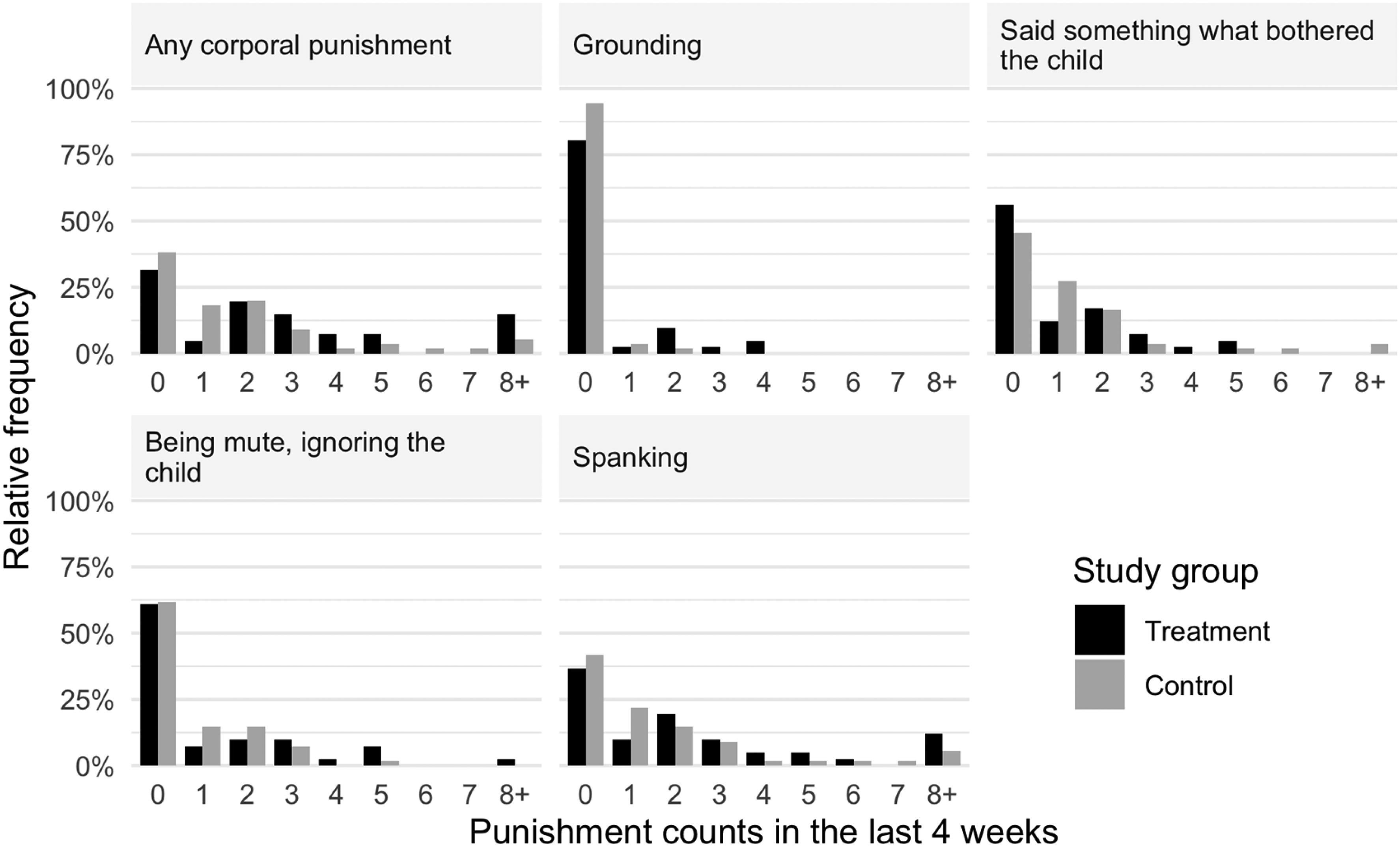
Utilization of different child punishment means at baseline.
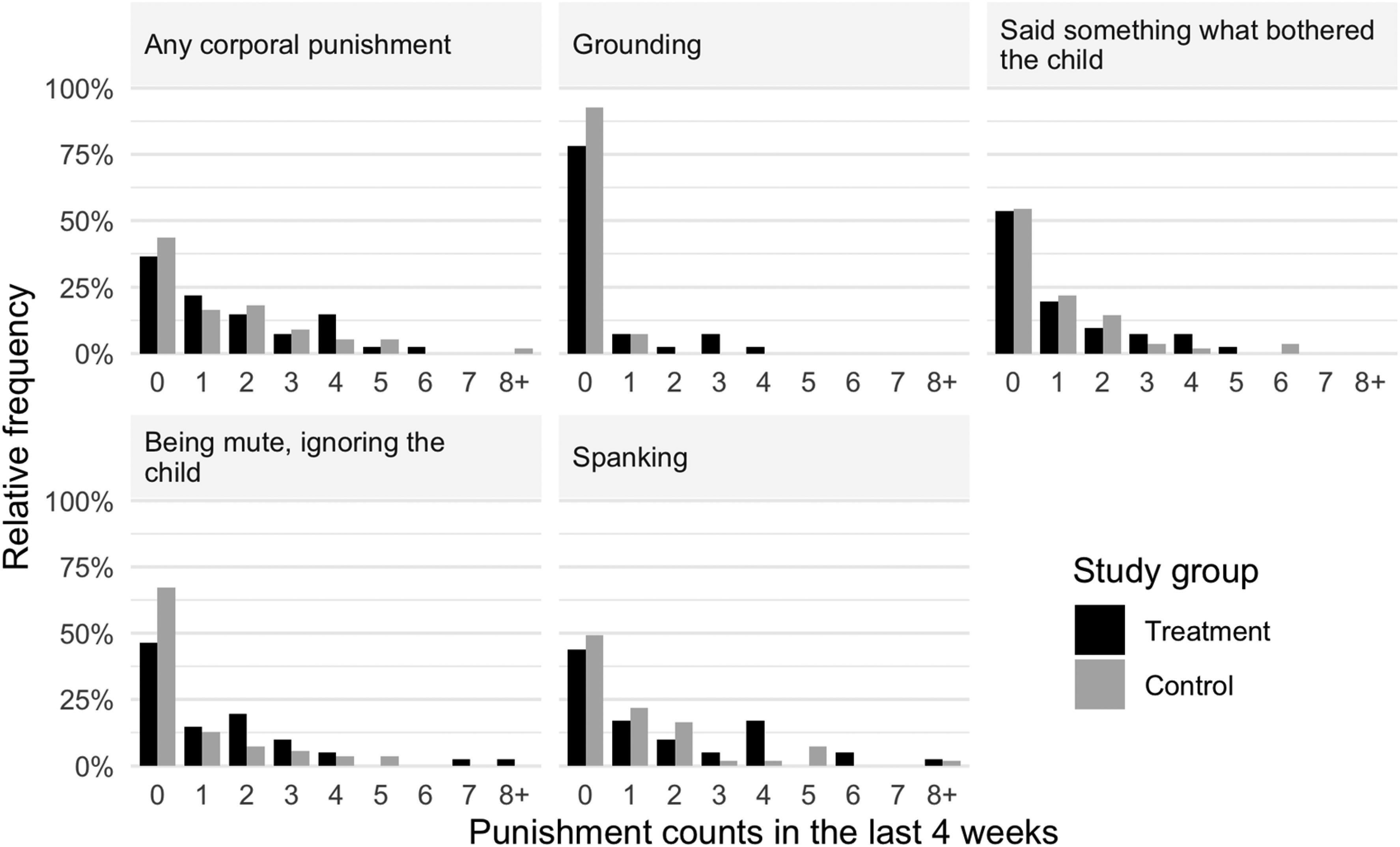
Utilization of different child punishment means in the second wave.
Discipline and Punishment
Throughout our analysis, we also briefly addressed the theme of discipline and punishment. Punishment items are an inherent part of any given scale and therefore are to be considered exploratory. Specifically, we measured whether the intervention itself led to a decrease in various undesirable forms of punishment. The seven items would include questions regarding harsher punishment, such as physical punishment or home confinement, to punishment such as ignoring or saying something troubling to the child involved.
The results indicate that in the first wave of measurement, harsher punishment such as physical punishment was used in at least 66.4% of the involved families (at least once in the four weeks prior to the measurement). Specifically, this would mean spanking in 59.3% of families or grounding used in 14.2%. Most of the punishments were present in the treatment group. The largest differences were apparent in the case of grounding, which was used 17.4 p.p. more often in the treatment group (Figure 5).
During the second wave of measurement, the proportion of punishment in both groups (treatment and control group) remained relatively unchanged; however, there was a decrease apparent in physical punishment (of 5 p.p.). On the other hand, there was a slight increase in punishment in the form of “being mute, ignoring the child” (Figure 6).
Moreover, there were differences between the two groups. In the treatment group, there was a substantial increase in punishment in the form of ignoring (14.7 p.p.) and a mild increase in verbal punishment (2.4 p.p.). We think that one of the possible reasons is that the methodical approach itself concentrates on limiting physical punishment; in the treatment group, there could be compensation apparent through other ways to punish. Moreover, ignoring the negative behavior of a child is an implicit part of the program introduced.
Considering the latter, it is, however, evident that at least in the case of attitudes toward physical punishment, there was a decrease. In the first wave of measurement, 24.7% of respondents in the treatment group approved of physical punishment as an implicit part of child upbringing (agreed or strongly agreed); in the second wave of measurement, 19.6% of treatment group respondents approved of physical punishment. Nevertheless, in the control group, the decrease was more substantial (from 30.4% to 20.0%). However, the differences in the development between the groups are rather negligible.
Discussion and Applications to Practice
This study provides evidence of the successful impact of a parenting program for disadvantaged families in the Czech Republic. We base our findings on the results of two distinct measurements. Using PARYC and SDQ measures, we first assessed both (1) self-reported competencies and (2) parent-reported changes in children's behavior. Both measures demonstrate a considerable difference between the treatment and the control group development. Intervention in the treatment group led to support for positive and proactive parenting or setting limits on the children's behavior. Similarly, there were significant beneficial effects on prosocial behavior and emotional/behavioral symptoms in children.
In terms of the exploratory part of the analysis, there is a visible decrease in physically related punishment. In the treatment group, there was a substantial increase in other-than-physical punishment. Specifically, it means that parents would more often ignore the child or punish the child verbally. We think there are two possible explanations for this. The first is methodological. Through the course of the program, parents were encouraged to deliberately ignore the negative behavior of their children. This could, in the end, lead to higher levels of overall reported ignoring as a secondary effect of the intervention. The second explanation is that the increase in ignoring and verbal punishment can, to some extent, compensate for the change in behavior of the parents, who would use such punishment as a substitute. Theoretical approaches such as the communication skills deficiency model would indicate that verbal and physical aggression are connected and that both forms of aggression substitute more constructive ways of communicating based on argumentation (Infante et al., 1990; Roberto et al., 2006).
With regard to specific links between verbal punishment and children's behavior, a recent study investigating parenting behaviors in 66 low- and middle-income countries showed that verbal punishment such as calling the child names or shouting are linked to children having higher odds of demonstrating aggressive behavior to a similar magnitude as specific physical punishment such as shaking or hitting the child (Ward et al., 2021, 2022). Some studies further demonstrate that verbal punishment can actually hold more substantial or consistent effects on children's delinquency or the increase in oppositional defiant symptoms than corporal punishment (Derella et al., 2020; Evans et al., 2012). We believe such findings show that various parental practices can hold unintuitive effects, implying that parental practices should be scrutinized and studied in a complex manner. For these reasons, and as physical abuse often co-occurs with psychological abuse or intimate partner violence, we see it as relevant to focus on complex interventions aimed at supporting parents in various ways (Leppäkoski et al., 2021).
Nevertheless, as there was not a clear decrease considering the parents’ approval of physical punishment, we cannot fully conclude that the parenting program was successful in encouraging parents to reflect on their initial attitudes toward corporal punishment. This is one of the certain limits in regard to our study, especially since recent examples demonstrate that bad practices in child rearing are connected to biased attitudes toward parenting and lower performance in implicit attitudes tasks (Camilo et al., 2022). Studies demonstrate that adolescents seem to mirror their parents’ beliefs toward specific forms of physical punishment such as spanking (Afifi et al., 2022). Therefore, we believe that even small changes in attitudes could be effectively reflected in the long term.
On a more practical note, we believe parenting group programs have important advantages. Based on peer support, they allow individuals to share common problems and solutions (Furlong & McGilloway (2012)). Moreover, Kleyn et al. (2021) demonstrated that through social media, those who attend parenting programs become more active within their caregiver networks. With their increased likelihood of speaking about parenting, they further positively influence other parents and their behavior toward children (Kleyn et al., 2021).
As an early intervention tool, parenting programs enable changes in the family environment that have a direct impact on children's cognitive development (Hutchings & Gardner, 2012). As a prevention tool, they minimize future costs related to child and adolescent delinquency (Baker, 2016; Piquero et al. 2008; Welsh et al., 2008). As recent research repeatedly negatively links children's development, their behaviors and cognitive development with lower socioeconomic status or poverty (Dolean et al., 2019; von Stumm et al., 2022), we think disadvantaged families would especially benefit from various ways of complex social work, including parenting programs.
The results of the meta-analysis on parent training effectiveness by Leijten et al. (2013), demonstrate that when measured one year after the end of treatment, disadvantaged families show less improvement when compared to nondisadvantaged families (Leijten et al., 2013). For the intervention in the socioeconomically disadvantaged families to be effective, it seems essential for social workers to provide complex, long-term interventions. Moreover, as the perception of the usefulness of parent training is one of the important factors in the intervention (Graf et al., 2014), it seems crucial for social workers to be able to provide training that is understandable for the parents and communicate the benefits. And indeed, programs aimed at increasing the quality of children's environment, focused on fostering the skills of parents, can have long-term benefits, such as the improvement of well-being of children in adulthood (Kiviniemi et al., 2020; Vanwoerden et al., 2021). For this reason, and in line with other authors’ work, we think it would be especially the role of practitioners, their competence, experience or training, that holds an important role in successful implementation of evidence-based parenting programs (Shapiro et al., 2015; Turner et al., 2011). Future scholarly efforts should refocus on the practitioners’ perspective in a more detailed way.
Regarding the limitations of our study, it is important to note that the outcome of the program is influenced not only by the content but also by the way the program is implemented. As there was a lack of independent observers in the process of data collection, it is difficult to assess the accuracy of the responses of the respondents and to what extent they were influenced by other factors. Another limitation is that although there is a detailed manual provided by the PLH research consortium, it is reasonable to assume that there were adaptations made to the delivery of the program, as evidence demonstrates that adaptations in evidence-based programs occur in almost half of the cases (Moore et al., 2013). A different limitation may be that despite the participants being sampled from the same population of clients of social service organizations, they could in fact differ in some regards, as the discrepancy at the baseline measurement might suggest. Even though we controlled for a number of confounding variables, and although the primary hypotheses all concerned the differences in the development—and not merely the differences in the second measurement wave—it is possible that families differed in other unobserved variables. Future research might consider more detailed matching techniques, such as propensity score matching or random assignment to the groups to bring more robust conclusions.
Conclusion
In the example of a Central and Eastern European country, this quantitative evaluation report demonstrates the outcomes of a “parenting program for disadvantaged families.” Quantitative data based on a total of 113 parents divided into treatment and control groups show increases in self-reported parenting skills or parent-reported children's behavior. Items aimed to measure parents’ attitudes toward physical punishment in particular demonstrate at least partial changes. Although the effects may be considered minor, we believe even those could further translate into factors connected to cognitive development, school achievements, or wider positive socioemotional changes.
We conclude that the program was successful in its aims and methods; however, there are some limitations to the evaluation process. It is worth noting that although our observed effects were all statistically and practically significant, the overall characteristics of the sample and its size do not allow us to draw broader claims generalizable to the entire population. Future research should further investigate the role of parenting programs on a wider range of participants, including participants with distinct socioeconomic status.
Footnotes
Author Note
The presented research output is a part of the project “Parenting groups as a tool for supporting parenting skills in families from socially disadvantaged and culturally different backgrounds” (reg. no. CZ.03.2.X/0.0/0.0/17_076/0011464), implemented under the “Support for innovative services for children and families at risk” (Call No. 03_17_076) of the Operational Programme Employment from the European Structural and Investment Funds and the state budget of the Ministry of Labour and Social Affairs of the Czech Republic.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Labour and Social Affairs of the Czech Republic and the European Social Fund (grant number CZ.03.2.X/0.0/0.0/17_076/0011464).