
Abstract
Experiences and Resource Use Related to a Family-Based Intervention for Parents with Substance Use
Children growing up in families with substance use disorders (SUD) is common worldwide. In Sweden, 5% of children live in a family where one or both parents have a problematic use of alcohol, drugs, or medicines (Raninen et al., 2016). Despite this, interventions targeting the entire family are lacking in Sweden. A brief family-based intervention, the Sofia model, was developed and tested in a medium-large Swedish municipality. The current paper describes parents’ experiences of the model as well as an economic assessment of the implementation and resource use.
The short- and long-term effects of growing up with parents with SUD are known to be detrimental for the children as well as for the family as a whole. In the short-term, children are at increased risk for maltreatment and neglect, as well as mental- and somatic ill-health (Dube et al., 2001; Finger et al., 2010; Laslett et al., 2012). In the longer term, children risk failing at school, developing addiction, and unemployment (Hawkins et al., 1992; Jääskeläinen et al., 2016; Kilpatrick et al., 2000; Mellentin et al., 2016).
In addition to the risk of negative consequences on children's health and well-being, the risks also contribute to a large economic burden for society. In a retrospective register-based study in Sweden, over 41,000 children growing up in families with mental health problems or SUD were followed until the age of 35 (Hovstadius et al., 2015). The study estimates that approximately 8% of children who grow up under these circumstances consume resources which amount to about a quarter of total societal costs related to mental ill-health and SUD. A majority of these costs are related to productivity losses due to the increased risk of unemployment (Hovstadius et al., 2015).
Co-parents are also known to be affected by the parent with SUD because of their increased risk of financial problems, health problems, exposure to violence, legal problems, high levels of psychological distress, and lower quality of life, (Benishek et al., 2011; Birkeland et al., 2018; Kahler et al., 2003; Lander et al., 2013). When aiming at improving outcomes for children in families where a parent has SUD, it is crucial to increase the protective factors, whereof several consider the co-parent (Gresko et al., 2022). The co-parent could serve as a dependable adult that, with a positive caring style, provide the child with a secure relationship (Park & Schepp, 2015; Velleman & Templeton, 2016). In order to do this the co-parent's own well-being and health needs to be acknowledged and supported in the context of a family-based intervention.
Interventions for the Family
Historically, interventions for adults with SUD have focused on individuals with the disorder, where the aim has been to lessen or terminate the abuse (Cassidy & Poon, 2019; Copello et al., 2005). The role of the family has changed from being a part of the problem to be a part of the solution, with family members increasingly being viewed and acknowledged as individuals who could benefit from interventions in their own right (Copello et al., 2005; Usher et al., 2015). There has been a shift in recent years toward the potential benefits of including a family perspective in substance abuse treatment (Baldwin et al., 2012). In line with the increased recognition of children's rights, this shift has also come to include children as their own agents with a right to interventions within the family context (Bröning et al., 2019).
There is a wide range of interventions focusing on family members affected by an adult with SUD (Hogue et al., 2022; Templeton et al., 2010). A recent review on family psychosocial interventions concluded that behavioral interventions with a family focus integrated with substance use treatment may have a beneficial effect on family functioning and reduce conflict (McGovern et al., 2021).
Family-Based Interventions in the Swedish Context
Scientifically evaluated family-focused interventions targeting families where one or both parents have SUD have been missing in the Swedish context (Socialstyrelsen [National Board of Health and Welfare], 2009), and few interventions focus on communication with the children about the parent's SUD (Pihkala et al., 2017). This might be due to the previous lack of attention to the family members in their own right, the social services being organized in different units targeting adults with addiction or the children, and the social worker's experience of lack of skills to work with children or adults with substance use (Huebner et al., 2017; Velleman & Templeton, 2007).
In 2014, a participation-based research project was initiated in a medium-large municipality in Sweden including families with substance abuse (children and parents) and social welfare personnel involved in the care of these families. In the first phase of the research project, interviews and research circles resulted in recommendations for what a family intervention should include in order to enhance protective factors and mitigate risk factors (Alexandersson & Näsman, 2015). The most important identified aspects were to provide children with adequate information about the parents’ substance abuse and to give them the possibility to pose questions and gain answers (Alexandersson & Näsman, 2015).
Other important aspects that were identified included children's need to express their worries and experiences, and enhancing the family's ability to communicate about the problems. In addition, aid and support to the parents, both in relation to their own or their partner's substance abuse problems and parenting, were emphasized as important. Based on these aspects, a team of social workers created the Sofia model.
The Sofia Model
The Sofia model is a cooperative model between child welfare social workers and social workers working with individuals with SUD. The target group for the model is families of children between 0 and 12 years of age who have one or more parents with SUD. The Sofia model aims to emphasize the children's situation in the family, pay attention to the children's needs, and help the families to communicate about issues related to substance use problems. The intention is that this will motivate parents to seek further help, for example, treatment for the substances use disorder, family support, or specific support for their children. To reduce the risk of negative secondary outcomes, the Sofia model aims to give support to the whole family and thereby reduce risk factors in the family and strengthen protective factors around the child.
The model consists of five meetings (Brosjö, 2019).
(Figure 1).

Meetings in the Sofia model.
It starts with a planning session for the social workers and a coordinator from the Sofia model staff. Thereafter, the whole family participates in three family meetings, and the children are offered two additional individual sessions with a child welfare social worker, social worker from the addiction unit, and the coordinator. During the family meetings, information regarding the parent's disorder and what support is available for the parent with SUD, the co-parent, and children, is provided. The individual child sessions aim to provide information to the child about the addiction, and the child is given the opportunity to express their experiences and needs.
The Sofia model was pilot tested in a medium-large municipality in Sweden from 2018 to 2021. The pilot was conducted in the context of the clinical setting with its opportunities and shortcomings in terms of, for example, fidelity to the model. The pilot was monitored by the municipality itself and half way, in 2019, a report was compiled. This report focused on the implementation of the model, including e.g., number of families reached, information/communication about the model to other services, and the development of procedures for social services units to work together (Andersson, 2019). There was, however, a need for a more thorough understanding of families’ experiences of the Sofia model as well as its cost implications. Thus, the current study aimed to explore parents’ experiences of the Sofia model and their perceptions of the model with regard to meeting the children's needs and improving family communication about substance use problems. In addition, the study aimed to assess the cost of setting up and running the intervention, and the parents’ and children's resource use in comparison to a reference population.
Method
Design, Participants, and Ethical Issues
The study consists of a qualitative part, comprising interviews with parents, and a cost assessment comprising estimations of intervention costs and resource use within substance abusing families.
Qualitative Part - Interviews with Parents
A qualitative methodology was used whereby parents who had participated in the Sofia model were interviewed. Both parents with SUD and co-parents have been interviewed. Participants could be partners or former partners, as all participants in the Sofia model were invited. In one interview, it was stated that the participant knew that his or her partner would participate.
Participants
A total of 14 parents were interviewed, of whom 10 were women and four were men. Based on the parent's descriptions, seven of the parents had or previously had a SUD and seven were co-parents to a parent with SUD. The parents had children aged 4 to 18. Three terms are used to represent the respondents: parent with SUD, co-parents, and parents, where the latter includes both parents with SUDs and co-parents. Furthermore, the term family is used when describing parents and children.
Recruitment
All parents who had participated in the Sofia model from 2019 to 2020 received an information letter about the study. A list of parents who had consented to participate in the study was provided by the project leader of the pilot study to the researchers (AF, KF). Thereafter the interviewer contacted the parents to give further information about the study and schedule an interview.
Design of Interview Guide
A semi-structured interview guide was developed by experienced qualitative researchers and revised in collaboration with the project leader of the pilot study. General open questions were combined with probing questions. The interview guide focused on three different areas: The parent's perception of the Sofia model; if the parents perceived that the child was involved and received support; the parent's perception of the family's ability to communicate regarding the addiction problem after having participated in the Sofia model.
The Interview Procedure
The semi-structured interviews were conducted by an interviewer who was a senior social worker with no previous contact with the families. The interviewer received a short training by one author (KF) before the interviews. The interviews were conducted by telephone and were audio recorded. Another author (AF) listened to the first audio recordings and provided feedback to the interviewer. All interviews took place during the period of March to May 2021.
Ethical Statement
The qualitative part of the study was approved by the Swedish ethical review board Dnr 2020-07251. The information letter sent to parents contained information regarding their potential participation in the study, that participation was voluntary, that the parent could end the interview at any point in time and that the interview was going to be recorded. Pronouns and dates in the quotes presented in the results section have been altered to ensure protection of the respondents’ identities.
Qualitative Analysis
The recorded interviews were transcribed and pseudonymized and information that could identify the respondents was excluded. The transcripts were analyzed through qualitative content analysis with an inductive approach (Elo & Kyngäs, 2008; Lindgren et al., 2020). The audio-recorded interviews were repeatedly listened to, transcribed and analyzed inductively using qualitative content analysis (Lindgren et al., 2020). The transcribed interviews were segmented into meaning units. The meaning units were inductively sorted and organized into codes, categories, and themes consecutively based on their differences and similarities. All parts of the analysis took place through collaboration between authors (AF, KF) and were repeated until both authors agreed that the categories and themes correctly reflected the participant's stories. The analysis was undertaken based on the Swedish transcriptions. The themes and quotes were translated into English during the process of writing the paper.
The material was analyzed from May to June 2021, with a focus on children, parents, and families. Meaningful units were identified in the transcribed material and then coded. The codes were divided into subcategories which were merged into categories. All parts of the analysis took place through collaboration between the authors and were repeated until agreement about whether the categories correctly reflected the parents’ descriptions.
Intervention Costs and Resource Use. Participants
A total of 40 families, consisting of 86 children and 76 parents, who received the Sofia model were included in the estimation of intervention costs and resource use consumed. In addition, 30 families with a total of 51 children and 59 parents were included as a reference population to estimate the resource use of families eligible for the Sofia model, but not remitted to the intervention. This reference population was not invited by the social services to participate in the intervention due to various reasons, including child-care disputes and violence in the families. According to social services, five of these 30 reference families received similar services offered by the Sofia model.
Recruitment
All families who were eligible within the social services to receive the Sofia model between 2018 and 2021 were included.
Design for Intervention Costs
A top-down approach was used to estimate intervention costs, with cost items identified based on information from financial monitoring of the project (Drummond, 2015). These items included time spent by project leaders, venue, materials, as well as training and supervision of social workers. The financial monitoring also included monetization of the cost items. All salary costs include social fees and vacation allowance paid by the employer. The time perspective was the whole implementation period, from September 2018 to June 2021, thus 2 years and 8 months. The costing perspective was the social services.
Design for Resource Use
A bottoms-up approach was employed whereby individual level data was used to estimate resource use (Drummond, 2015). Resource use was estimated for care provided by the social services, including treatment related to alcohol abuse. Resource use was estimated for families eligible for the Sofia model during the 2 years and 8 months of implementation. Families were enrolled at different stages, hence the length of time that resource use was estimated for varied between families. Information on the type of service, quantity used (number of hours per week and between which dates) and any additional information was gathered from the social service case records. Hourly, daily, or weekly average costs for each type of service used were estimated by the social services. These average unit costs were thereafter multiplied by the quantity used by each individual. All salary costs include social fees and vacation allowance paid by the employer.
Ethical Statement
The cost and resource use assessment was approved by the Swedish ethical review board Dnr 2020-07251. Consent from the participants was not necessary due to the regularly collected data from the social services being anonymized.
Quantitative Analysis
A descriptive analysis was carried out, illustrating the cost of the Sofia model for 40 families and resource used within social services for parents and children eligible for the Sofia model, including 40 families who received it and 30 families who serve as a reference population. Costs are presented per family, by type of resource used, and by children/parents. All costs are estimated in Swedish Krona (SEK) and recalculated into 2021 Euro (€) using a purchasing power parity of 9.95 SEK to €.
Results
Qualitative Part - Interviews with Parents
The respondents talked about how they came into contact with the Sofia model, how they perceived the model, their children's participation, and how they communicated about addiction in the family. Six categories emerged from the qualitative analysis: (1) The Road to the Sofia model, (2) The Sofia model – What is That?, (3) The Sofia model for Us, (4) Parental Support – for the Needs of the Child, (5) The Children in the Sofia model, and (6) The child Kept in the Dark. The categories are presented with illustrative quotes from the interviews.
The Road to the Sofia Model
In most instances, the families described that they gained access to the Sofia model through reports of concern to the social services. In many cases, several reports of concern were needed before the family received help. Both in cohabiting and separated families, co-parents had made reports of concern to the social services. “I made a report of concern, how my daughter is doing with her father. Well, there are actually two, we've been to social services twice. But that's the last time. The time before that, the police made a concern report” (Co-parent 3, mother).
According to the parents, the reports of concern were most often made by the health care services, primarily from personnel in the emergency department, after a parent's intoxication or suicide attempt. In several of these cases, it was the children who called the ambulance or contacted the co-parent to resolve the emergency situation. How we got in touch with Sofia. We finished the investigation, and then just about a week later, there was an incident at the children's father's home, where I had to call the police…And it was the children who contacted me so that I could come and help them (Co-parent 6, mother).
“I'm an alcoholic, and I made two suicide attempts last year. The hospital contacted the social services but I already had a caseworker before I attempted suicide and then the children got their caseworker.”
What kind of support had you received before then, before Sofia?
“I had sessions with an alcohol and drug therapist twice a week. But then that wasn't enough, and I got myself a caseworker, and was going to start outpatient care. There was nothing for the children. That came later” (Parent with SUD 8, mother).
Some also described long-term support from the social services regarding parenting or relationship issues. However, in these supportive contacts the substance use problems were never discussed. It was not until a report of concern was made that these parents got in touch with the addiction unit and the Sofia model.
Some co-parents described that it took time for the substance use problems to be discovered. One reason for this was when the parent with SUD did not fit the stereotype of a person with an addiction problem. Another reason was when the addiction was more unusual, for example, a parent was misusing sex and this was not recognized as an addiction by the social services.
The Sofia Model - What is That?
Many families received numerous interventions from the social services, often over long periods of time, and when describing these, they seldom named specific interventions. All contacts, support, and interventions were labeled “soc” [short for social services] and the parents seemed not care to distinguish between different interventions or work models. “I actually do not remember, for us, there have been an incredible number of meetings with soc, and they have probably been called different things, for different people, as well” (Co-parent 14, mother).
Other parents didn’t recognize having participated in the Sofia model at all. “But do we stand, do I stand as registered that I have somehow been part of this Sofia model in some way?” (Co-parent 3, mother).
Several parents explained that they lacked knowledge about the model due to being away for addiction treatment during their family's start of the Sofia model. Other parents with SUDs described their insufficient knowledge to be due to the fact that they did not live with their child. This applied both to families where the child was placed in foster care and when the child lived with the co-parent.
Some parents associated the Sofia model with the report of concern to the social services. When these reports had resulted in foster care placement, it affected the perception of the Sofia model. These parents described that the Sofia model had resulted in their children being placed in foster care or an escalation of their own addiction. “But it did not lead to anything getting better, my children were taken after that, so I would not say that it has” (Co-parent 9, mother).
The Sofia Model for Us
The families described having obtained a large variation in number of meetings and content of these in the Sofia model. Few parents described that they had received the entire model. The majority of parents had attended one or up to three meetings. In these meetings, the other parent, a social worker from the addiction unit, a child welfare social worker, and a social worker from the Sofia model, participated. These meetings were described as an opportunity to talk about the addiction, something which was appreciated. And that was a bit what I thought, just that of facilitating the conversation, that everyone can have a say… that you can say everything you want and need and feel and think, that there is no one who orchestrates the conversation, or directing the conversation. I thought that was good (Parent with SUD 13, father).
The parents described that the first meeting contained a lot of information, which was perceived as positive by some and negative by others. “I don't remember, well it was a lot of information with everything they went through” (Parent with SUD 7, mother).
The meetings were described as being focused on the parent with SUD and the future interventions for the addiction. To gain insight into these interventions and care was beneficial, according to the co-parents. In some instances, the co-parent had been unaware of the addiction problem. In these cases, there was a need for more information about SUD and how it can manifest itself.
Other situations that were perceived as difficult was when the addiction problems concerned other issues than alcohol or drugs. Parents described that the social workers appeared to lack knowledge about other forms of addiction, which made them minimize the impact of the addiction in relation to the children and to the parents’ abilities to parent. This had a very negative and even detrimental effect on the co-parent and the children. “They [the social workers] were ignorant about how addicts work, how duplicitous and, and… Yeah… [sigh] He, he can run a successful professional life” (Co-parent 14, mother).
The timing of the Sofia model varied according to the parents. Some parents described that it was a short contact and sometimes the Sofia model was experienced as rushed in time. This resulted in parents not having time to talk through what they needed at the meetings, nor did parents and/or children have time to participate in planned interventions outside the model before the last meeting in the Sofia model. On the other hand, some parents who perceived that the model provided the family with continuous support.
Parental Support – for the Needs of the Child
In families where the co-parent was co-living or shared custody with the parent with SUD, the co-parent expressed a need for support on their own behalf in their parenting role. This need was described partly in relation to their own feelings toward the parent with SUD and partly about the difficulties of co-parenting with a parent who was actively abusing alcohol or drugs. “I feel that we need tools to… be able to… manage our parenting” (Co-parent 2, mother).
The co-parents perception of the Sofia model meeting was that the focus was on the parent with SUD, much less attention was given to the co-parent. The overall experiences were that the co-parents’ needs and roles as parents were neglected in the meetings. “I do not really know what I did at those meetings, because they did not talk about me, like. Or did I [laugh a little] I was there, but it was not me it was about” (Co-parent 9, mother).
The co-parents described that they wished for more support and help within the Sofia model and that they wished that the support had existed over a longer period of time. Even the parents who say that they have received a lot of support and help via the Sofia model emphasized that even more support might be needed as the situation was very difficult and they had been under severe pressure. “I was actually completely paralyzed too” (Parent with SUD 7, mother).
The Children in the Sofia Model
Few parents could give a clear answer to the question of whether the children had attended meetings within the Sofia model. Most of the parents described that the children had not participated, while others were unsure whether their children had participated. No child seemed to have had their own child-meeting within the Sofia model.
According to the parents, younger children had not participated in the Sofia model at all. They did not attend meetings, their needs were not discussed among the adults, and due to their age, they did not receive any other support or interventions from the social services. This was despite the fact that the children were exposed to sudden separations between the child and the parent with SUD as the parents were hospitalized, taken into custody, or had to leave for addiction treatment. “My daughter was considered to be too young, because she was only four years old at the time” (Co-parent 3, mother).
On the other hand, there were descriptions of how the needs of older children emerged in connection with the Sofia model meetings. The meetings had provided information about what interventions were available for those children. However, there were no descriptions of how this information was provided during the meetings, nor if it was given to the parents or the children themselves.
One parent with SUD emphasized the importance of the children's voluntariness in the Sofia model and argued that the child's interests and will were allowed to guide participation. Most parents also described that their children did not want to go to more meetings, or meet more people and that the children expressed that they “didn't want to talk to anyone” (Parent with SUD 11, mother). This referred to the social services’ investigation and the Sofia model meetings. “They do not want to go there [laughs]. They think it's boring to be there, but I, I think it has been good that they have been there and talked, and they have had the opportunity to say what they want” (Parent with SUD 8, mother).
The parents described the meetings where children did participate as not being child-friendly and that the children became passive in the discussions. Children's experiences of the meetings ranged from boring to, in some cases, very negative and harmful, according to the parents. In the latter case, the children were forced to describe and talk about their parent's addiction in front of the parent with substance abuse. They were both forced to speak and stay in the meeting; even though they had been promised they could be silent and leave the meeting if they so wished. The Sofia model increased the stress and anxiety of these children, and they refused any further contact with the social services. “The meeting we had with the Sofia model. It was terrible, I really thought it, I thought it, it was terrible what the children were subjected to there, that it, it was so ruthless to their pain and anxiety” (Co-parent 14, mother).
Another aspect of the children in the Sofia model, as described by co-parents, was how the parents with SUD had difficulties taking their children's perspectives. It was not enough that the child welfare social worker tried to reach through to the parent, aiding them to take their children's perspective. I didn't think the dad fully understood the consequences his actions could have led to, and actually did lead to. I would have liked a little more support from the social workers in that. I thought the child social worker was trying to reach him. But maybe didn't get all the way through. The social worker from the addiction unit, I don't know, I thought she reached him better with what she said (Co-parent 6, mother).
The Child Kept in the Dark
In the interviews, after having answered questions about the Sofia model, the parents were asked if they could talk their children about SUD. Few parents described that they talked to their children about the SUD. Only one parent said that she always had been open with the children about her addiction. The parent described that she told her children that she was an alcoholic when seeking help for the addiction. “I told them that in the fall two years ago when I started, when it all started with me getting help for… alcoholism, like.” (Parent with SUD 8, mother).
In the other interviews, a more varied picture emerged. For example, some co-parents tried to protect their children by not talking to them about the addiction or the situation at home. The contact with the Sofia model made them understand that it was helpful and important for the children that the parent can talk about the addiction and aspects and experiences related to this, even difficult ones. And then I kind of tried to clean up after him, and keep the facade up for the kids, and… So that they would not understand anything, so that I think that behavior has hung on, in my own behavior since, that I have not talked with them, or with the eldest (Parent with SUD 11, mother).
Of the relatively few parents who described that they talked to their children about the addiction problem, some said that they talked more after having participated in the Sofia model or after receiving support from the family units at the social services. Parents with SUD described that they received support with how they could talk to their children about the dangers with alcohol and drugs and how intoxicated people can behave. One parent verbalized that “the social worker told me what to say to him [the child]” (Parent with SUD 5, father).
Most parents, however, described that they did not themselves take the initiative to talk to the children about the abuse. They also described it as challenging to listen and talk to the children about the parents’ use disorders, the parents’ and child's wellbeing, violence and other potential traumatic situations. Rather, they expected their children to ask questions if they needed to. However, based on what the parents said, there seem to be few children asking any questions.
Several parents expressed that it was particularly difficult to talk to their younger children as they lacked knowledge on how young children can react to parents’ addiction. They also described a wish to better understand signs that their children were in need of support and help. Several parents wanted more support with this within the framework of the Sofia model.
Intervention Costs and Resource Use
Table 1 shows the estimation of the cost of the Sofia model over 2 years and 8 months. In total, 40 families participated in the Sofia model. The largest cost could be attributed to the project leaders. In total, it cost €350,799 to deliver the intervention to 40 families, which averaged to €8,770 per family.
Cost of Implementing the Sofia Model Over 2 Years and 8 Months in Uppsala Municipality in Sweden. Costs Presented in 2021 Euro (€).
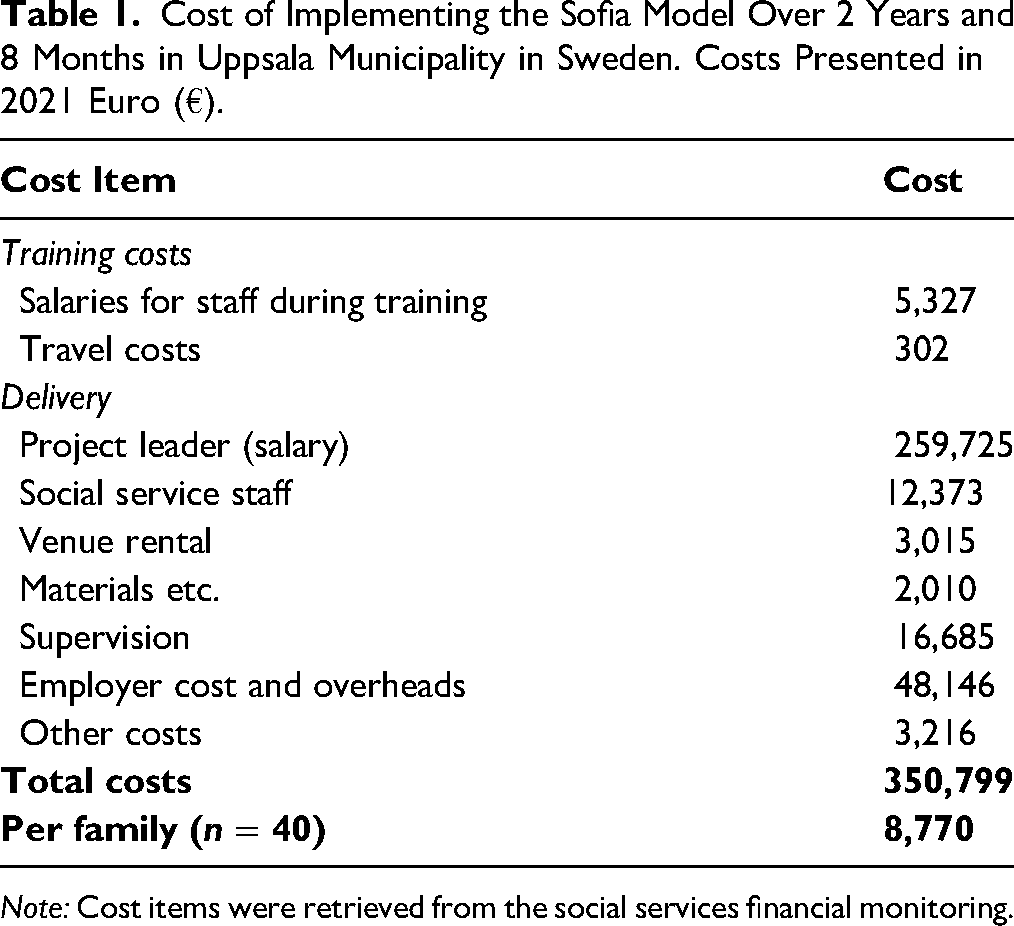
Note: Cost items were retrieved from the social services financial monitoring.
Table 2 shows the unit costs for all resources used by the families who received support from the social services, while Table 3 indicates the quantity of resources used, and the final cost of all resources used for families within the Sofia model and the reference population. As Table 3 shows, both parents and children consumed more resources within the Sofia model compared to the reference group. This can be seen both from the frequency of consumption, as well as the total costs. The major cost driver for both children and their parents was related to the use of different types of foster or residential care homes. For children within the Sofia model, about 13% were placed in foster care homes, while the corresponding frequency of children in the reference group amounted to 10%. Almost 18% of the adults in the Sofia model had been receiving care in residential care homes, and 5% in the reference group. Lower costs for children could be seen for services related to their parent's alcohol use disorder, such as specific group support which roughly 5% of the children in the Sofia model received, and 1% in the reference group. Treatment within the last 2 years and 8 months for SUD delivered by the social services was rather infrequent for parents. About 28% of families received family-directed treatment and support within the Sofia model, and 17% in the reference group. No individual support directed at the co-parent was provided. On average, the cost for all types of resource use per family was estimated at €22,960 within the Sofia model, and €18,855 in the reference group.
Unit Costs for Different Types of Care Provided by the Social Services. Costs are Presented in 2021 Euro (€).
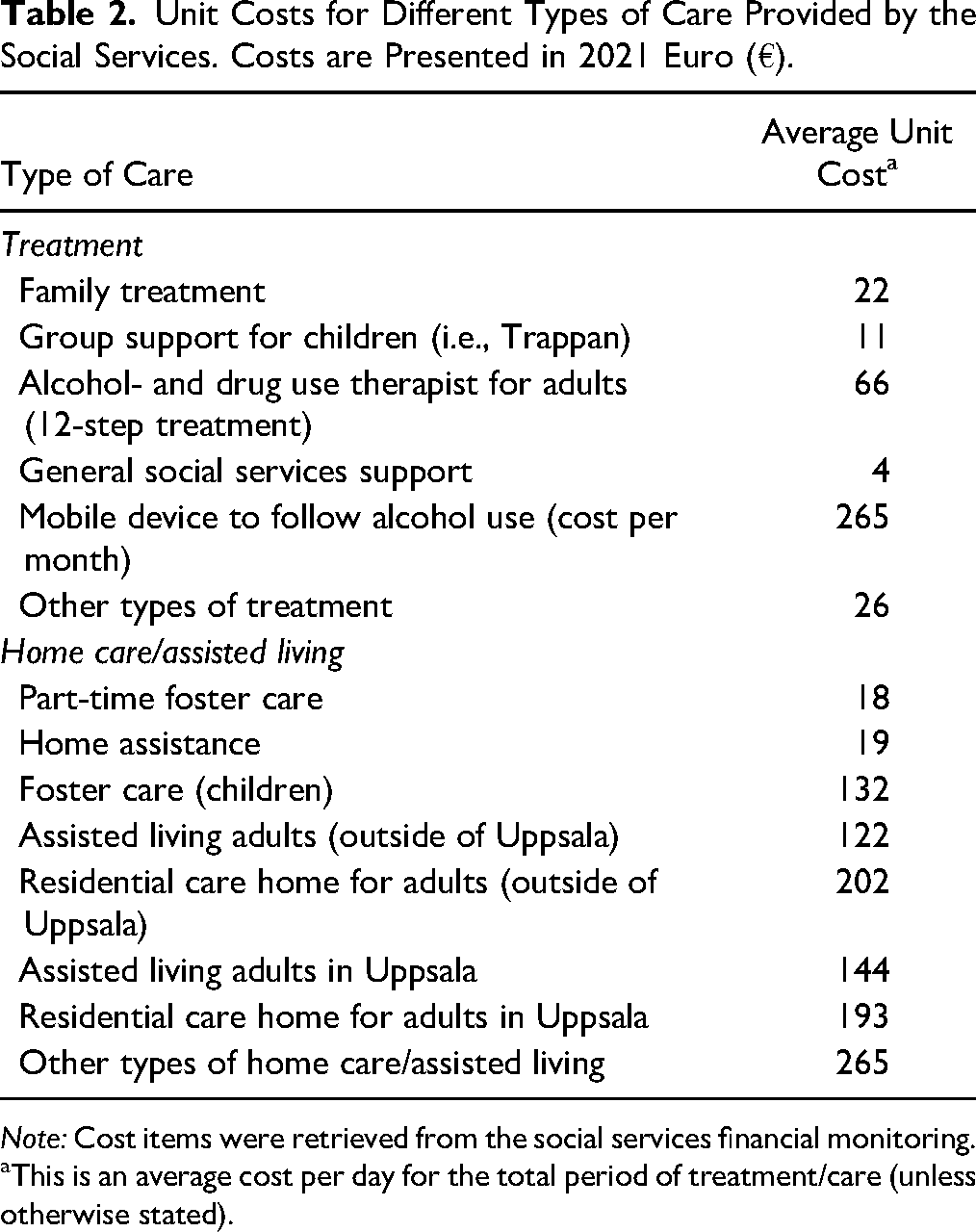
Note: Cost items were retrieved from the social services financial monitoring.
aThis is an average cost per day for the total period of treatment/care (unless otherwise stated).
Resource use and Related Costs of Families Receiving Interventions from the Social Services Over a Time Period of 2 Years and 8 Months. Costs are Presented in 2021 Euro (€).
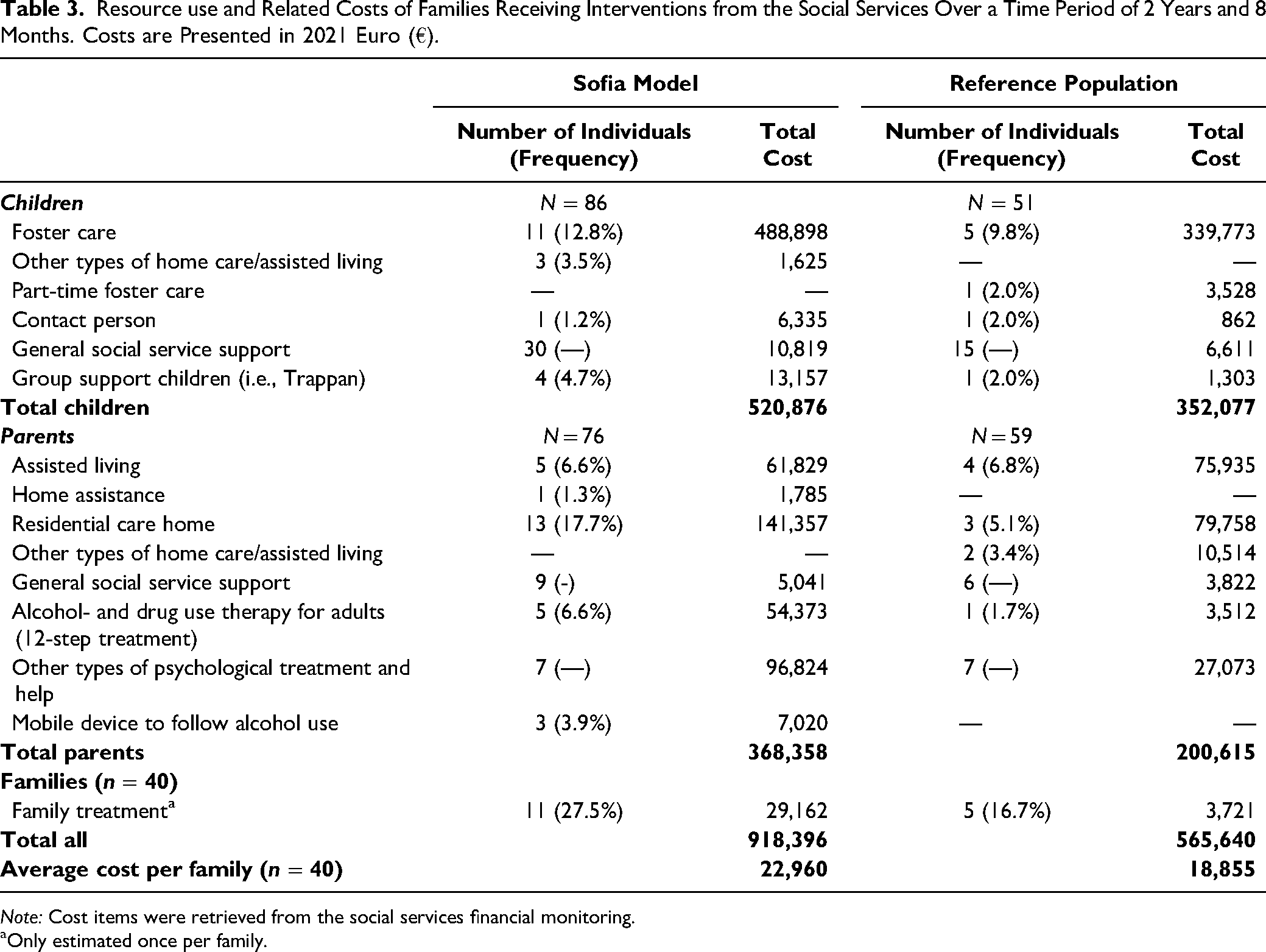
Note: Cost items were retrieved from the social services financial monitoring.
aOnly estimated once per family.
Discussion
In this study, 14 parents were interviewed regarding how they experienced the Sofia model and their perceptions of the model with regard to meeting the children's needs and improving family communication about substance use problems. Understanding parents’ experiences is important as it provides a basis for understanding whether the intervention is acceptable to them. Intervention costs and family resource use was assessed where the 40 families who received the Sofia model were compared to a reference population of 30 families. The findings will be discussed in relation to the goals of the Sofia model as well as previous research in the field.
A Rocky Road to Early Family Centered-Intervention
The parent's overall experiences of the Sofia model were that the road to the model was long and filled with very stressful events, especially for the children. The children had been negatively affected by the substance use problems in the family – both in terms of the child's well-being and the relationship with their parents. It is well known that children in families where one or both parents have SUD are at increased risk for maltreatment and mental ill-health (Finger et al., 2010; Laslett et al., 2012) and our results are in line with these findings. In addition, the interviews also contained descriptions of potentially traumatic events for the child in situations where the parent was intoxicated. Exposure to parental intoxication has been related to adverse health outcomes and early alcohol use for children (Haugland et al., 2020; Kerr et al., 2012).
The rocky road to the family-based intervention was also evident in the parents’ descriptions of how multiple reports of concern to the social services had been needed, before the family was offered the Sofia model. This was despite the fact that parents with SUD could have had a long contact with addiction treatment services. This is a serious concern as health care professionals in Sweden have a legal obligation to consider the needs of children, according to the Swedish Health and Medical Care Act (SFS 2017:30). Thus, all professionals who work with adults with addiction must take into account that there may be children with the adult and they are obliged to report to social services if they suspect child abuse. In this way, the Sofia model fails in offering early family centered support and intervention to these families. The importance of preventive and early interventions for children in families with parental SUD has been highlighted in several studies (Bröning et al., 2019; Cuijpers, 2005; Velleman & Templeton, 2016). Thus, it is necessary to investigate how families should be referred to an intervention, such as the Sofia model, to examine the organizational prerequisites and barriers, and to collaboratively work to overcome these. It is well known that individuals with problematic drinking and/or SUDs find it difficult to use traditional systems of care, especially when it concerns parenting. This is why staff in substance use treatments need to be extra attentive to these adults (Neger & Prinz, 2015; Niccols & Sword, 2005).
A Place to Talk About the Addiction
Another important overall experience of the Sofia model was that parents appreciated the opportunity to talk about the addiction together with professionals from the addiction unit, child social welfare unit, and the Sofia model coordinator. Previous studies have investigated the importance of moving toward an interdisciplinary practice, including professionals within child protection and substance abuse treatment professionals (Blakey, 2014). Parents also strongly valued being treated with respect and in a non-judgmental way, something which they considered important for the entire family. Living in a family with addiction problems is often shameful, including anxiety related to contacts with the social services (Battle, 2019). Therefore, the non-judgmental treatment families receive from the social services is important. In addition, this approach has been demonstrated to be an important part of building supportive relationships with staff as it reduced patients’ feelings of shame, something which could even act as a motivator to abstain from alcohol (McCallum et al., 2016) and help with recovery (Thompson, 2022). In addition to the social workers’ accepting attitude, parents thought the information about additional support available to them and their older children, was useful. In fact, families participating in the Sofia model used more care which is supported by the results from the resource use estimation of the Sofia model. These results demonstrate that the families participating in the Sofia model have received a larger proportion of interventions such as family treatment and housing assistance, compared to the families in the reference population. However, it is not possible to entail whether the larger use is due to the intervention, which a future evaluation would be able to ascertain.
Parental Needs in the Shadow of Substance Use Problems
The parents criticized the Sofia model, especially the predominant focus on the parent with SUD and the addiction, something which left little room for the needs of the co-parent and the family. Previous research has stressed the importance of support to the co-parent, as he or she can have a vital role in providing a secure relationship with the child (Park & Schepp, 2015; Velleman & Templeton, 2016) and even act as a protective factor when aiming at improving child outcomes in families with SUD (Gresko et al., 2022). The co-parents’ experiences of their needs for support being overlooked are also evident in the results of the resource use estimation as no co-parents received individual support.
Another criticism was that there was not enough attention paid to the parent with SUD as a parent, in particular their ability to take the children's perspectives and well-being into consideration. This is unfortunate, as helping the parent with SUD to improve their relationship with their children, learn parenting skills and gain insight into the intergenerational transmission of substance use and parenting is important for the parents themselves and for their children (Niccols et al., 2012; Sword et al., 2009).
Both these results were contrary to the purpose of the model, which is to pay attention to the entire family, i.e., the child or children, the co-parent, and the parent with SUD.
The Lack of a Focus on the Children
The main goal of the Sofia model was to pay attention to the children and their needs. Further, the goal was to provide the children with adequate information about the parent's addiction and to give them the possibility to pose questions and gain answers. In order to achieve this, the model includes specific meetings for the child and the family meetings were supposed to be child-focused. According to the parents, these goals have not been realized. Very few children were present at the family meetings and no children received specific child meetings. There were no clear answers in the interviews as to why the children did not participate to a larger extent in the family meetings. However, one explanation could be that they did not want to talk to unknown adults from the social services. Another reason could be that they rejected participation to avoid communicating about their parent´s substance use, perhaps based on years of encouragement not to talk about the abuse, or based on a lack of trust in the social services (Hill, 2015; Taylor & Kroll, 2004). Yet another barrier to children's participation could be that the parents acted as gatekeepers as they are used to, and want to, keep the SUD a secret (Barnard & Barlow, 2003).
When children did participate in the family meetings, they experienced these as boring and did not want to attend additional meetings, hindering their possibilities to have their rights respected. Some children experienced the meetings not only as boring but as increasing their stress and anxiety. There can be several complicating factors when adults want to talk to children about their parent's SUD. One of these can be the stigmatization of substance abuse in the society (Livingston et al., 2012) and another could be the lack of knowledge and experiences in talking to children about difficult topics (Velleman & Templeton, 2007), especially young children.
Some parents could describe that their older children did receive additional support from the social services, i.e., via support groups or psychotherapy. Though, it was not clear whether this was a result of the information they obtained at the Sofia model meetings. However, the results from the resource use estimation indicates that children in families that participated in the Sofia model received just a few additional interventions during and after the Sofia model than the children in the reference population during the same period of time. The youngest children seemed to have been completely invisible in the Sofia model. They did not participate at the family meetings, they were not offered their own child meetings, their parents did not receive information on how to talk to them about the addiction nor was there any additional support available to them. These children are exposed to numerous adverse life events and the described loss of contact with the parents for shorter and longer periods can result in attachment difficulties (Lander et al., 2013). The lack of attention on young children's needs and well-being is particularly problematic, both from a child's rights perspective (UN General Assembly, 1989) and when aiming at preventing children from adverse mental, somatic and educational development (Copello et al., 2005).
Communicating about Substance Use Problems with Children is Difficult
With regard to the children, the main goal of the Sofia model was to make the children's needs and voices heard
A second goal was to facilitate communication within the family regarding addiction and the parent's SUD. Neither this aim was achieved, as only a few parents described that they talked to their children about the substance use. Talking about substance use can be demanding for parents, and feelings of shame and guilt can arise (Pihkala et al., 2017). Instead, parents waited for their children to ask questions, albeit having learned the importance of talking to children about the addiction and difficult experiences related to this. A previous Swedish intervention, solely aiming at encouraging communication about a parents’ illness, resulted in openness about substance use within the families and an improved understanding of the children's needs (Pihkala et al., 2017). Thus, for the Sofia model to work as intended regarding the focus on children and communication about the addiction, much could be improved.
Limitations
One limitation of the study is the number of participating parents, and the predominance of mothers and co-parents as the experience of the parent with SUD may be lacking in the data collection. As few children attended the Sofia model meetings, children's experiences were not possible to collect, even though this is of utter importance. A limitation for the resource use estimation was the difference between the population receiving the Sofia model, and the reference population. To determine eligibility for participation in the intervention, an investigation by the social services was needed. Thereafter, families could enroll in the intervention. The time of enrollment was set as the starting point for estimating resource use. As the reference group had no starting point, resource use was calculated from the time of the investigation. There is thus a likely underestimation of resource use for the intervention group. In addition, due to the selection bias of participants who were offered the intervention, it likely had an impact on estimations of resource use. Thus, without randomization of participants, the differences seen between groups should be interpreted with caution.
Conclusions
The brief Sofia intervention model aimed at emphasizing children's situation in the family, paying attention to their needs and helping families to communicate about issues related to substance use problems. Although the Sofia model enabled communication regarding the SUD during intervention sessions, the intervention failed to enhance communication regarding SUD in the families. There was a lack of focus on the children's needs and the co-parent felt neglected. Children and co-parents in the Sofia model received only a little more individual support than the reference families. Parents voiced a need for more comprehensive support over time for their children and themselves.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Uppsala municipality.