
Abstract
Keywords
Introduction
More personalized approaches are needed to understand how to match children exposed to trauma to the best level of care. Understanding which child psychotherapy treatments work for whom is still limited (Mullarkey & Schleider, 2021). Stepped care interventions provide treatments in phases where interventions and/or dosages are provided in steps to best match client needs (Bower & Gilbody, 2005). Stepped care trauma-focused cognitive behavioral therapy (SC-TF-CBT) includes a parent-led therapist-assisted treatment as the first step (Step One) and standard therapist-led TF-CBT as the second step (Step Two) for children needing more intensive treatment (Salloum et al., 2014). Approximately 47% to 70% of children respond to Step One, and SC-TF-CBT is less costly than standard TF-CBT (Salloum et al., 2022a). Identifying potential pre-treatment characteristics that may be used to match children to the best level of care within SC-TF-CBT (i.e., Step One or Step Two) may increase treatment response to Step One, prevent delays for children needing more intensive treatment, and provide a more personalized approach. TF-CBT is an effective treatment for childhood trauma (de Arellano et al., 2014; Mavranezouli et al., 2020). Characteristics that have been associated with poorer outcomes for TF-CBT and other trauma-focused treatments for children may inform predictors of non-response to Step One. Thus, this study explored potential predictors of non-response to Step One such as critical life events, demographics, trauma-related factors, and child and parent symptomatology.
Critical Life Events
Critical life events, including financial stressors during treatment (e.g., caregiver's loss of job, not having insurance to cover costs, and moving), may present challenges to parents for staying engaged in treatment. Cost is a barrier to parents accessing mental health treatment for their children, especially in the United States, and includes other financial barriers such as transportation or loss of wages (Reardon et al., 2017). Bornheimer et al. (2018) found that among poverty-affected families, critical life events during treatment such as moving further from the clinic, change of job, and having children move out of the home significantly decreased the likelihood of attending eight or more sessions.
Critical life events during treatment may also decrease completion of treatment homework tasks. For example, in a study exploring barriers contributing to homework non-completion in TF-CBT, one trainer stated
Demographics
The use of TF-CBT has been effective in improving outcomes for children from various racial and ethnic backgrounds (e.g., Diehle et al., 2015; Dorsey et al., 2020; Lang et al., 2010; Lenz & Hollenbaugh, 2015; Webb et al., 2014). However, studies examining data from the National Center for Traumatic Stress Network in the United States from sites delivering a range of trauma-focused interventions suggests that African-American families are more likely to drop out of child trauma treatment (Sprang et al., 2013) and Hispanic families are less likely to utilize such services (Choi et al., 2018). TF-CBT has developed applications for Hispanic/Latino families (de Arellano et al., 2012) and more recently for African-American youth (Metzger et al., 2021), although these approaches have not been incorporated into Step One of SC-TF-CBT.
There have been mixed findings associated with the relationship between age and treatment outcomes for children. Meta-analyses of CBT for youth with post-traumatic stress disorder (PTSD) have found larger treatment effects for older children compared to younger children (Gutermann et al., 2016; Lenz & Hollenbaugh, 2015). However, in a TF-CBT randomized controlled trial for children and adolescents ages 7 to 17, younger participants benefited more from treatment (Goldbeck et al., 2016). In terms of gender, some trauma treatment studies have found that girls have poorer treatment response than boys (Craig & Sprang, 2014; Knutsen et al., 2020), while other studies have not found gender differences (Cohen et al., 2011; Kane et al., 2016). Children from lower socioeconomic backgrounds may be at risk for attenuated treatment effects (Rudd et al., 2019) and their families may need more resources (Lowe et al., 2014; Panisch et al., 2020). Thus it is possible that income may be a predictor of treatment response to Step One. Taken together, treatment outcomes may vary based on demographics warranting the exploration of treatment response to Step One by race, ethnicity, age, gender, and family income.
Trauma-Related Factors
Children who experience interpersonal trauma versus non-interpersonal trauma may have different psychiatric outcomes. Interpersonal traumas include traumas related to child maltreatment, sexual abuse, and domestic violence whereas non-interpersonal traumas include accidents, illness, natural disasters, and traumatic loss or bereavement (Hughesdon et al., 2021). Interpersonal trauma among youth has been associated with higher externalizing symptoms and impairment (Price et al., 2013); whereas non-interpersonal trauma has been associated with internalizing symptoms (Ford et al., 2011). Cumulative interpersonal trauma among youth has been associated with more severe PTSD symptoms, social problem behaviors, and aggressive behaviors compared to youth exposed to non-interpersonal trauma, although youth with non-interpersonal trauma may also be at risk for social problems (Hughesdon et al., 2021). It is not known if Step One is effective for children who have experienced interpersonal versus non-interpersonal trauma.
In addition to trauma type, it is important to explore if treatment outcome differs between children with single incident trauma and children with more than one type of trauma (e.g., polytrauma). Each additional form of traumatic experience places youth at greater odds of presenting with high-risk behaviors and functional impairment (Greeson et al., 2014). In a sample of 5,058 clinic-referred youth in the United States, youth with co-occurring physical abuse and psychological abuse experienced the highest severity of PTSD and other types of trauma (e.g., domestic abuse, neglect, impaired caregiving) suggesting that cumulative trauma is often in the context of co-occurring risk factors (Hodgdon et al., 2018). TF-CBT has been found to be effective with children presenting with complex PTSD and chronic exposure to multiple traumas (Ross et al., 2021). However, given the complexities related to cumulative trauma in terms of severity of child outcomes and associated environmental challenges, Step One treatment response may differ by single trauma versus polytrauma.
Child Behavioral Health Outcomes
SC-TF-CBT, which includes Step One and Two has been found to be non-inferior to TF-CBT in changes in number of post-traumatic stress symptoms (PTSS), severity and impairment (Salloum et al., 2022a). However, child trauma treatment outcome may vary based on pre-treatment PTSS severity. In a meta-analysis evaluating treatment for children exposed to violence, Miller-Graff and Campion (2016) found that higher PTSD severity was associated with smaller treatment effect sizes. Thus, child PTSS, including severity, and impairment was examined as a potential predictor of Step One non-response.
When comparing SC-TF-CBT (including Step One and Step Two participants) to standard TF-CBT, comparable decreases over time in internalizing symptoms, sleep disturbances, externalizing symptoms, and anger outbursts were observed. However, when conducting the non-inferiority test for completers and intent-to-treat samples, non-inferiority for the completers sample was not supported for internalizing problems at post-treatment and externalizing problems at all time points (Salloum et al., 2022b). A post hoc analysis indicated that Step One responders had lower internalizing and externalizing problem scores at post-treatment than non-responders (Salloum et al., 2022a). Based on pilot work (Salloum et al., 2016, 2017) and prior research (Mannarino et al., 2012), we predicted that high internalizing problems would predict greater non-response to Step One. Internalizing behaviors are highly prevalent among trauma-exposed children (Farley et al., 2021; Fowler et al., 2009; Hébert et al., 2018; Moussavi et al., 2021), and children with internalizing symptoms may need a tailored treatment approach (Carpenter et al., 2014; Herres et al., 2016). In a meta-analysis of nine TF-CBT studies including child depression as an outcome, de Arellano et al. (2014) found that while treatment effects were strong for PTSS, effects were not as robust for depressive symptoms. While research on sleep as an outcome for child PTSD treatments is limited, a study with youth receiving prolonged exposure therapy found evidence that insomnia and nightmares were predictors of poorer treatment response (Brownlow et al., 2016). In line with these findings, youth receiving treatment for depression who have sleep disturbances may have poorer treatment response outcomes (Manglick et al., 2013; McGlinchey et al., 2017). Thus, it is likely that children with high internalizing scores at baseline are not likely to respond to Step One treatment, and exploring sleep disturbances as a potential predictor of Step One treatment response is warranted.
Externalizing problems and, more specifically, anger outbursts may be predictors of non-response to Step One. In a meta-analysis of TF-CBT studies, five of seven studies found significant pre-post decreases in general behavioral problems (de Arellano et al., 2014). TF-CBT includes behavioral interventions to help children with externalizing problems (Cohen et al., 2010). Step One includes many of these strategies and offers two additional sessions that may be used to address problematic behaviors (Salloum et al., 2014). Some evidence suggests that youth with high levels of anger show less decrease in PTSS post-treatment, which may be due to poor emotion regulation skills (Kaczkurkin et al., 2016). Thus, in the current study, both externalizing problems and anger outbursts were explored as predictors of Step One treatment response.
Parent Distress
Caregivers play an important role in TF-CBT, although research examining caregiver characteristics as moderators and predictors of treatment is limited (Brown et al., 2020; Danzi & La Greca, 2021). Parental PTSS has been associated with child PTSS (Alisic et al., 2011; Scheeringa et al., 2015). However, parental depression may have more of an influence on child treatment outcomes for PTSD than parental PTSD or stress (Martin et al., 2019). In Step One, parents take a more active role than in TF-CBT as they lead the meetings with children at home without the therapist. Thus, while parental depression has been shown to moderate treatment outcomes in trauma-focused treatment (Danzi & La Greca, 2021; Martin et al., 2019), parents’ PTSD, including avoidance behaviors, may inhibit parents from helping children directly process their traumas. Parenting stress may also contribute to difficulties meeting with and directing children to complete activities. Thus, parental PTSS, depression, and parenting stress were explored as potential predictors of non-response to Step One.
Aims
The purpose of this study was to examine potential predictors of Step One outcome. The specific aims were two-fold:
to examine the association of internalizing problems and anticipated critical life events and Step One treatment response. Specifically, the following two hypothesis were tested:
Hypothesis 1. Children with high internalizing symptoms would be less likely to respond to Step One than those children with fewer internalizing symptoms. Hypothesis 2 to explore potential predictors of Step One including demographic variables (e.g., race, ethnicity, age, gender, income), trauma-related variables (interpersonal trauma vs. non-interpersonal trauma, and polytrauma vs. non-polytrauma), and child outcomes (child PTSS, impairment, internalizing, externalizing, severity, sleep disturbances, anger outbursts) and parent outcomes (PTSS, depression, parenting stress).
For the second exploratory aim, we explored associations between demographic variables, trauma-related variables, child outcomes, and parent outcomes and tested significant associations as potential predictor variables of Step One.
Method
Study Design
Data from the current study are from a community-based randomized clinical trial where children ages 4 to 12 and their caregivers were randomly assigned to SC-TF-CBT or standard TF-CBT (1:1 ratio). Assessments occurred at baseline, during treatment (including mid-treatment), post-treatment and 6- and 12-month follow-up assessments. A block randomization, generated by R (Uschner et al., 2018) was used to balance treatments for high/low internalizing symptoms (T-scores > or ≤ 71) and high/low anticipated critical life events (score > or ≤ 16). The high and low scores were based on pilot data from SC-TF-CBT (Salloum et al., 2016, 2017) that suggested participants with high scores were not as likely to respond to Step One than those with low scores. The study was approved by the University of South Florida Institutional Review Board (clinical trial registration: NCT02537678).
Participants
Given that the current study aims were to examine predictors of Step One, only participants who participated in Step One and were classified as responders and non-responders were included. Thus, the sample consisted of 63 parent–child dyads with 43 responders of Step One and 20 non-responders. Details of inclusions and exclusions for the clinical trial as well as patient flow and retentions can be found elsewhere (see Salloum et al., 2022a).
Children were ages 4 to 12, had experienced at least one traumatic event after 36 months of age, and had at least four (for children ages 4–6) or at least five (for children ages 7–12) symptoms of PTSD with at least one re-experiencing or avoidance symptom. Exclusion criteria included any condition that would impair the caregiver's or child's abilities to cognitively participate, suicidality, parental substance abuse disorder (past 3 months), and non-fluency in English. If children were on medications, doses had to be stable for 4 or more weeks or for 2 weeks for benzodiazepines or stimulants. Other exclusions included concurrent trauma-focused psychotherapy, if caregivers were the perpetrators, the perpetrator was living in the home, or if children were having unsupervised face-to-face contact with perpetrators. Siblings were not included.
In terms of patient flow, 43 responders of Step One moved to the maintenance phase and completed the post-treatment assessment. Of the 20 non-responders, 14 stepped up due to non-adherence to Step One (two dropped out of Step Two after 1 and 3 sessions), three stepped up due to a new trauma occurring during Step One, and three were non-responders of Step One although two of these families decided not to step up.
Procedures
Pre-screening (e.g., age, trauma reported, medication, current trauma-focused therapy) for participation occurred via phone by the intake workers at five community-based behavioral health non-profits and at one university community clinic. If caregivers were interested in participating in the trial, a screening/baseline assessment was scheduled at the agency. Prior to the baseline assessment, caregivers provided written informed consent and children (ages 7–12) provided assent to participate. The study was explained to young children (4–6) by the therapist and parents at the first therapy session since they did not attend the baseline assessment. Compensation totaling $225 was provided for assessments: baseline ($25), mid-treatment ($30), during treatment ($20), and post-treatment and 6- and 12-month follow-up assessments ($50). Clinician-administered assessments were completed by independent evaluators (IE) who were located at the university via a secure HIPAA-compliant web platform. Self-report measures were completed via Qualtrics (Qualtrics, Provo, UT).
Measures
Demographics
During the baseline assessment, caregivers provided the caregiver and child demographic information including race, ethnicity, age, gender, and household income ranges. Race and ethnicity of the parent/caregiver and child were both reported as these data slightly differed (see Table 1). These demographics were used in the current study to explore race, ethnicity, age, gender, and income as potential predictors of Step One.
Comparison of Step One Responders vs. Non-Responders for Anticipated Life Events, Demographics, Trauma-Related Variables, and Child and Parent/Caregiver Outcomes.
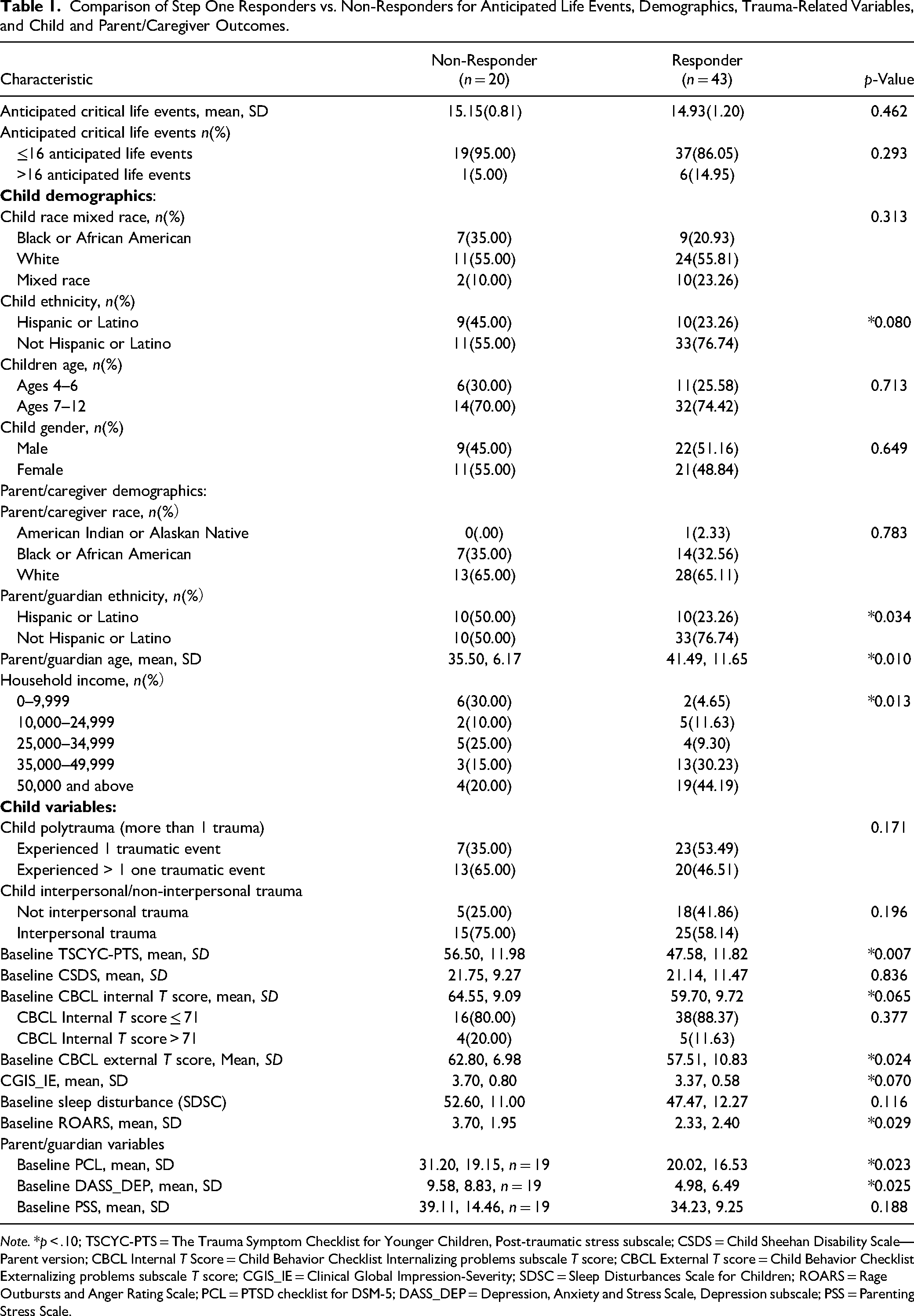
Note. *p < .10; TSCYC-PTS = The Trauma Symptom Checklist for Younger Children, Post-traumatic stress subscale; CSDS = Child Sheehan Disability Scale—Parent version; CBCL Internal T Score = Child Behavior Checklist Internalizing problems subscale T score; CBCL External T score = Child Behavior Checklist Externalizing problems subscale T score; CGIS_IE = Clinical Global Impression-Severity; SDSC = Sleep Disturbances Scale for Children; ROARS = Rage Outbursts and Anger Rating Scale; PCL = PTSD checklist for DSM-5; DASS_DEP = Depression, Anxiety and Stress Scale, Depression subscale; PSS = Parenting Stress Scale.
Barriers to Treatment
The Barriers to Treatment Participation Scale Critical Life Events (Kazdin et al., 1997) is a parent self-report 14-item list of events that may result in attrition (e.g., medical insurance will not cover treatment costs, moving, illness, loss/change of job and/or income, separation/divorce, legal problems, child school change) with a response format of yes = 1 or no = 2 (range 14–28). The measure was adapted such that parents were asked at the baseline assessment to indicate if they thought that any of the events would occur during the next 3 months (the estimated time of treatment). Anticipating two or more critical life events (a score of 16 or above) was considered high. This measure was administered during the clinical trial to use in the current study to test anticipated barriers as a predictor of non-response to Step One.
Trauma-Related Variables
The following two semi-structured interviews of childhood PTSD were used in the current study to measure and test trauma-related variables (e.g., interpersonal trauma vs. non-interpersonal trauma, and polytrauma vs. non-polytrauma) as predictors of Step One response.
The diagnostic infant and preschool assessment (DIPA; Scheeringa, 2014) for DSM-5 is a semi-structured interview administered with caregivers regarding mental health disorders specific to young children. Caregivers of children ages 4 to 6 were administered the PTSD module for total number of symptoms for responder status in Step One, type and total number of traumatic events, index trauma, PTSD diagnosis, and suicidality for screening. The interviews were recorded and a second rater who was also blinded to treatment reviewed a random sample of 22.4% of all PTSD interviews at baseline, mid, and post-assessment. Interrater agreement was .852, .894, and .745 (p < .001 for all time points).
The Kiddie schedule for affective disorders and schizophrenia (K-SADS; Kaufman et al., 1997; 2016) for DSM-5 is a structured diagnostic interview for children ages 7+. The child/parent versions were administered independently by the IE to assess presence of PTSD and type, index trauma, and total number of PTSD symptoms. The interviews were recorded and a second blinded rater reviewed a random sample of 13.4% of all PTSD interviews at baseline, mid and post-assessment. Interrater agreement was .896, .828, and .902 (p < .001 at all assessments). K-SADS was used to screen for child psychosis, mental retardation, autism spectrum disorder, and child suicidality.
Interpersonal and non-interpersonal and polytrauma variables were developed based on the responses from the DIPA and K-SADS. Children's index traumas were coded as either interpersonal trauma (e.g., sexual abuse, physical abuse, domestic violence; coded as 1) or non-interpersonal trauma (e.g., accidents, illness, death; coded as 0). More than one traumatic event indicated on the DIPA or K-SADS was recorded as polytrauma (coded as 1) and only one traumatic event was recorded as not polytrauma (coded as 0).
Child Outcome Measures
The following child outcome measures were used to measure the primary (Salloum et al., 2022a) and secondary outcomes (Salloum, et al., 2022b) in the clinical trial. In the current study, the child outcome measures are used to test child PTSS, severity, internalizing problems, externalizing problems, sleep disturbances, and anger outbursts as potential predictors of Step One.
The trauma symptom checklist for younger children (TSCYC; Briere, 2005) is a 90-item caretaker-report of trauma symptomology in children ages 3 to 12. The total score of the 27-item post-traumatic stress subscale (TSCYC-PTS) was utilized in the current study to measure the child's PTSS (range = 27–108, ≥40 in the clinical range; current study α = .90).
The Child Sheehan Disability Scale—Parent version (Sheehan & Sheehan, 2008; Whiteside, 2009) is an adapted, 5-item, 11-point Likert scale caregiver report assessing the interference of the child's PTSS on daily functioning (current study α = .84). This measure was used in the current study as a measure of impairment. Clinical global impression-severity (CGI-S; National Institute of Health, 1985) is a one-item, 7-point Likert scale to measure severity. The CGI-S scale was completed by the IE after the baseline assessment, and the rating was discussed with the last author for consensus. This measure was used in the current study as a measure of severity.
The child behavior checklist (CBCL) is a caregiver report that assesses the internalizing and externalizing behavior for children ages 1½ to 5 years (Achenbach & Rescorla, 2000) or ages 6 to 18 (Achenbach & Rescorla, 2001). In the current study, T-scores for internalizing and externalizing behaviors were used. The Cronbach's alpha for internalizing (α = .92, α = .88) and externalizing problem behaviors (α = .94, α = .89) were both high for children ages 4 to 5 and ages 6 to 12, respectively. T-scores were used for the hypothesis test as a continuous measure as well as for comparing children with extremely high internalizing T-scores greater than 71 versus those less than 71. T-scores ≥ 64 indicate children within the clinical range and our unpublished pilot data suggest that children with a score > 71 were less likely to respond to Step One.
The Sleep Disturbances Scale for Children (SDSC; Bruni et al., 1996) is a 26-item caregiver report of children's sleep behaviors and disturbances and was used in the current study to measure child sleep disturbances. Each item includes a 5-point Likert scale with increased severity of sleep disturbances indicated by higher values (total score ranges from 26 to 130, with a score of 39 indicating disturbed sleep; Bruni et al., 1996). The SDSC has demonstrated acceptable reliability and validity (Bruni et al., 1996) (current study α = .85).
The Rage Outbursts and Anger Rating Scale (ROARS; Budman et al., 2008) includes three items rated on 4-point Likert scales to assess the frequency, intensity, and duration of explosive outbursts in the past week and was used in the current study to measure child anger outbursts. Frequency in the past week ranges from no rage episodes, 1–2 rages, 3–7 rages but not every day, or at least one every day. Intensity ranges from absent = 0, mild = 1 (e.g., brief tantrums, not destruction), moderate = 2 (e.g., threating, hurtful verbalization, destruction of property but not credible threats of physical harm to the child or others), and severe = 3 (e.g., danger to self and others, highly destructive behaviors, threatening with weapons, requires hospitalization). Duration ranges from none = 0, mild = 1 (e.g., 5 minutes or less), moderate = 2 (e.g., 6–15 minutes), and severe = 3 (more than 16 minutes). The IE completed the measure with the caregiver. For the total score scale, 0 to 3 corresponds with mild outbursts, 4 to 6 indicates moderate outbursts and 7 to 9 indicates severe outbursts, with total scores ranging from 0 to 9. This measure has demonstrated acceptable psychometric properties (Storch et al., 2012) (current study α = .87).
Parent Outcome Measures
The following parent outcome measures were used to measure secondary outcomes in the clinical trial (Salloum et al., 2022b). In the current study, the parent outcome measures are used to test parent PTSS, depression and parenting stress as predictors of Step One.
The PTSD checklist for DSM-5 (PCL-5; Weathers et al., 1994) is a 20-item, 5-point Likert scale self-report of DSM-5 PTSD symptoms that was completed by caregivers about themselves. The range is 0 to 80 with a cut off score of ≥ 31 indicating possible PTSD. The PCL-5 has demonstrated strong psychometric properties (Blevins et al., 2015) (current study α = .95).
The Depression, Anxiety and Stress Scale (DASS-21; Lovibond & Lovibond, 1995) is a 21-item, 4-point Likert scale self-report measuring depression, anxiety and stress in caregivers. For the current study, the depression subscale was utilized. The total score on the depression subscale (range = 0–21) was multiplied by 2 for a total range of 0 to 42 and the sum of 7 items was taken and multiplied by 2 (current study α = .89). Higher distress is indicated by higher scores with categorical ranges indicating normal (0–9), mild (10–13), moderate (14–20), severe (21–27), and extremely severe (+28; Lovibond & Lovibond, 1995).
The Parenting Stress Scale (PSS; Berry & Jones, 1995) is an 18-item, 5-point Likert scale self-report measure of parenting stress inclusive of both positive (pleasure) and negative themes of parenting. Parents indicated the degree to which they agreed or disagreed with each item. The total score ranges from 18 to 90 with higher stress indicated by higher scores (current study α = .86).
Responder Status Criteria and Additional Measures
Treatment response to Step One was defined by (1) the child having 3 or fewer symptoms of PTSD for children ages 4 to 6 based on the DIPA PTSD module (Scheeringa, 2014), and 4 or fewer PTSD symptoms for children ages 7 to 12 based on the K-SADS PTSD Module (Kaufman et al., 2016); (2) below the clinical cutoff score on the TSCYC-PTS (Briere, 2005) or on the UCLA-PTSD Reaction Index revised (Pynoos & Steinberg, 2015). The TSCYC-PTS (Briere, 2005) was used for ages 4 to 6, and the UCLA-PTSD Reaction Index revised (Pynoos & Steinberg, 2015) was used for children ages 7 to 12; and (3) an IE rating of improved (a rating score of 3) or higher on the Clinical Global Impression-Improvement (Guy, 1976).
Treatment non-response was determined if treatment response criteria was not met or if there was non-adherence to Step One or a new trauma. If the parent had not completed at least three of the four at-home meetings prior to attending therapist session two, they were considered a non-responder and the parent and child were asked to step up. If a new trauma occurred during Step One, they were considered a non-responder and the parent and child were asked to step up. For this study, treatment response was coded as 0 = non-responder to Step One, and 1 = responder to Step One.
Step One Treatment
Step One is a parent-led therapist-assisted treatment based on the knowledge base of TF-CBT (Cohen et al., 2017) and CBT for PTSD for preschoolers (Scheeringa et al., 2011). Similar to TF-CBT (Cohen et al., 2017), if abuse has occurred by a parent, the treatment involved the non-offending parent or caregiver. In vivo and imaginal exposure are utilized as a main component of Step One and psychoeducation, parenting strategies, relaxation, affect modulation, trauma narrative, conjoint sessions, and safety are included. There are three planned therapist sessions and two additional as-needed sessions led by therapists with caregivers and children, and 11 parent–child meetings led by caregivers at home with children. During the 11 parent–child meetings, caregivers work with children in an empirically supported activity book called Stepping Together (Salloum et al., 2009, 2010) that is based on the Preschool PTSD Treatment manual (Scheeringa et al., 2011). Psychoeducation information is provided via the internet from information posted on the National Center for Childhood Traumatic Stress website. Also, video demonstrations for caregivers on relaxation and imaginal and in vivo exposures are posted on the Stepping Together website. Therapists provide weekly phone support (∼10–15 minutes) to check-in with caregivers about the progress of the meetings. Details about Step One may be found elsewhere (see Salloum et al., 2014). Step One responders ended trauma-focused treatment and proceeded to the maintenance phase for 6 weeks to practice skills learned, and non-responders stepped up to Step Two, therapist-led TF-CBT. In the current study, there were nine therapists who provided Step One treatment (three licensed clinical social workers, one registered intern clinical social worker, two licensed mental health counselors, two registered intern mental health counselors, and one licensed marriage and family therapist).
Data Analysis
Descriptive statistics for anticipated life events, demographics, trauma-related variables, and child and parent/caregiver outcomes are presented in Table 1. To initially evaluate the factors associated with responder status to Step One, t-tests and chi-square tests were used to compare continuous and categorical factors between responders and non-responders, respectively (Table 1). An unadjusted model was built with results from backward stepwise logistics regression of predictors with p < .10. Besides predictors in the unadjusted model, demographics including child gender, age and race were included in the partially adjusted model. In addition, three child primary outcomes were added for full adjusted model. The area under the receiver operator characteristic curve (AUC) was reported for the three models. Generally, discrimination of a logistic model can be assessed as follows: AUC = 0.5 = no discrimination; 0.5 < AUC < 0.7 = poor; 0.7 ≤ AUC < 0.8 = acceptable; 0.8 ≤ AUC < 0.9 excellent; and AUC ≥ 0.9 = outstanding (Hosmer & Lemeshow, 2000). Site was not included in the model, as it was not associated with responding status (p = .120). Results were presented as adjusted odds ratios (AOR) and 95% confidence intervals (95% CI). Statistical significance was defined as a p-value of <.05. All analyses were conducted using the SAS System (Version 9.4, SAS Institute Inc., Cary, NC).
Results
The parents/caregivers leading the treatment were mostly mothers (n = 50, 79.37%). Grandmothers (n = 7, 11.11%), fathers (n = 3, 4.76%), aunts (n = 2, 3.7%), and one uncle (1.59%) also led the child's treatment in Step One.
Hypothesis 1
Children with high internalizing symptoms would be less likely to respond to Step One than those children with fewer internalizing symptoms. For the first hypothesis, children with high internalizing scores (T-score > 71) were as likely to respond to Step One as children with low internalizing scores, p = .377, OR = 1.90, 95% CI = [0.45, 8.01]. There was no statistical difference in the mean T-scores of child internalizing symptoms at baseline between responders (M = 59.70, SD = 9.72) and non-responders (M = 64.55, SD = 9.09, p = .065, Cohen's d = .50, CI = [0.24, 0.76]). Thus, Hypothesis 1 was not supported.
Hypothesis 2
Parents/caregivers with high anticipated critical life events would be less likely to respond to Step One than parents/caregivers with fewer anticipated critical life events. Children of parents/caregivers with high anticipated critical life events were as likely to respond to Step One as children with low anticipated critical life events, p = .293, OR = 0.33, 95% CI = [0.04, 2.89]. There was no statistical difference in the mean scores of anticipated critical life events at baseline between responders (M = 14.93, SD = 1.20) and non-responders (M = 15.15, SD = .81, p = .462, Cohen's d = .20, 95% CI = [-0.05, 0.45]). Thus, Hypothesis 2 was not supported.
For the second exploratory aim, child age, child race, child gender, interpersonal/non-interpersonal trauma, polytrauma or not, child impairment, child sleep disturbances, and parenting stress were not associated with response to Step One. Thus, these variables were not included in the full model. Potential predictor variables with a p value of less than .10 that were included in the full model included child ethnicity (p = .080), parent age (p = .010), parent ethnicity (p = .034), parent income (p = .013), TSCYC-PTS total (p = .007), CBCL internalizing scores (p = .065), CBCL externalizing scores (p = .024), angry outbursts (p = .007), parent PTSS (p = .023), and parent depression symptoms (p = .025). See Table 1.
After utilizing the backward selection method with the 10 variables with a p value < .10 entered into the full model, the results of the unadjusted model indicated that parent depression, child anger outbursts and parent ethnicity were the strongest predictors of Step One response (see Table 2). Each additional point on the DASS-depression subscale was associated with 18% decreased odds of responding to Step One (AOR = .82, p = .023). Each additional point on the ROARS was associated with 27% decreased odds of responding to Step One (AOR = .73, p = .025). Lastly, parents/guardians who were Hispanic or Latino were less likely to respond to Step One with a decreased odds of responding to Step One of 78% (AOR = .22, p = .026).
Unadjusted Model with Parent Depression, Child Anger Outbursts, and Parent Ethnicity.
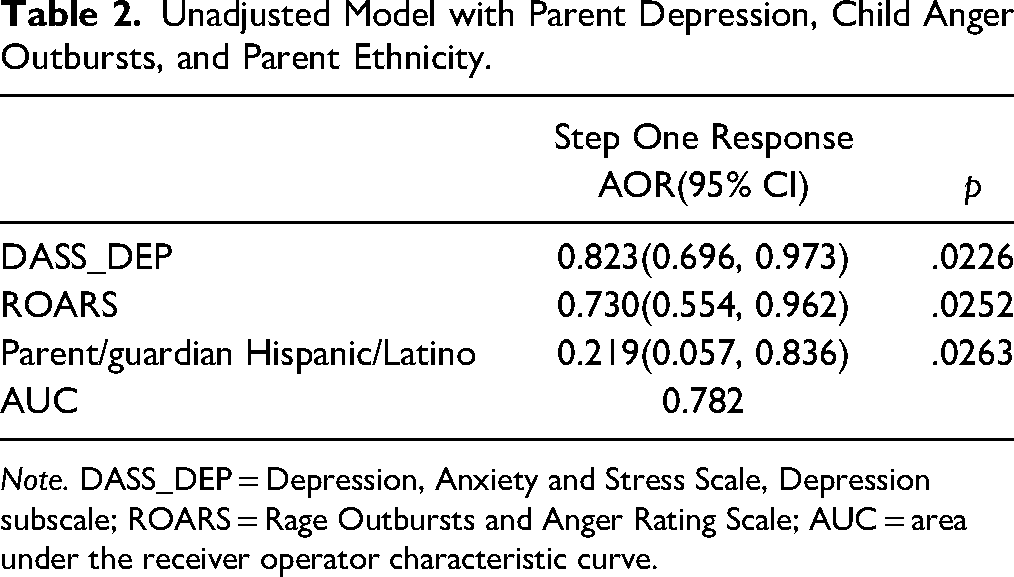
Note. DASS_DEP = Depression, Anxiety and Stress Scale, Depression subscale; ROARS = Rage Outbursts and Anger Rating Scale; AUC = area under the receiver operator characteristic curve.
We further examined if the association of these three predictors would remain statistically significant after controlling for child demographics (e.g., child gender, child race, and child age). Parent depression, child anger outbursts, and parent ethnicity remained statistically significant predictors of Step One after controlling for demographics (see Table 3).
Partially Adjustment Model with Demographics.
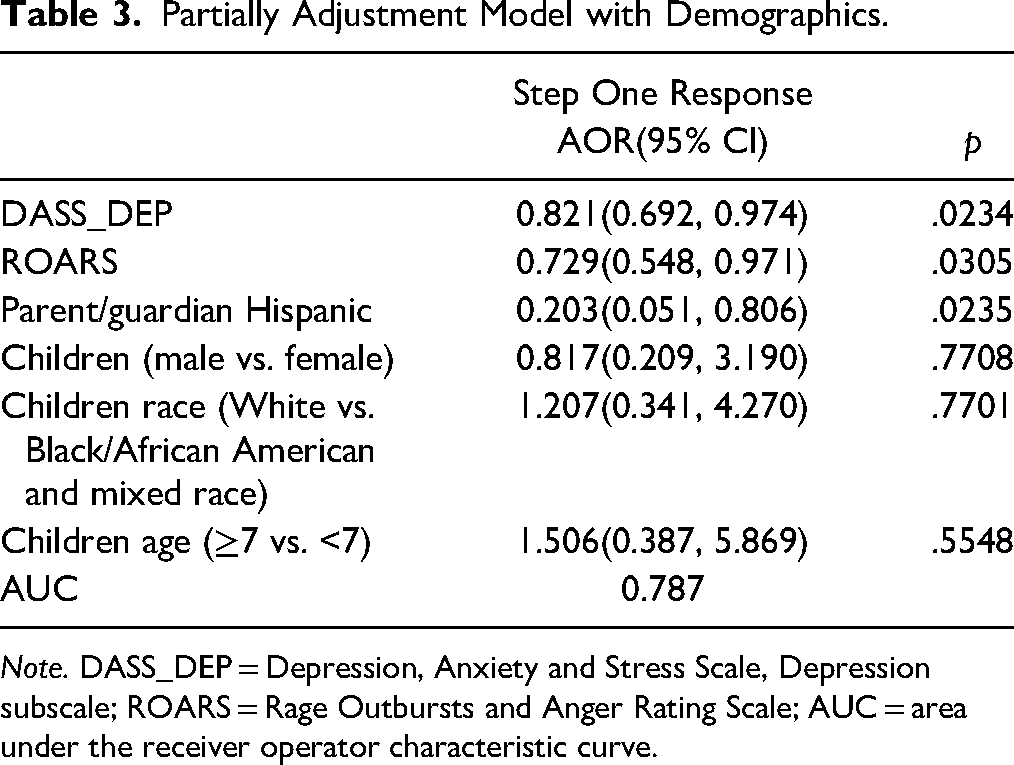
Note. DASS_DEP = Depression, Anxiety and Stress Scale, Depression subscale; ROARS = Rage Outbursts and Anger Rating Scale; AUC = area under the receiver operator characteristic curve.
To further examine the stability of the association of parent depression, child anger outbursts and parent ethnicity, we added the child primary outcomes to the model which included child PTSS, impairment and global severity to the fully adjusted model. The results were essentially unchanged with parent/guardian depression, child anger outbursts and parent ethnicity as significant predictors for Step One (see Table 4).
Results of the Logistic Regression Analysis Examining the Association Between Parent Depression, Child Anger Outbursts and Parent Ethnicity, Demographics, and Child Treatment Outcomes: Full Adjusted Model.
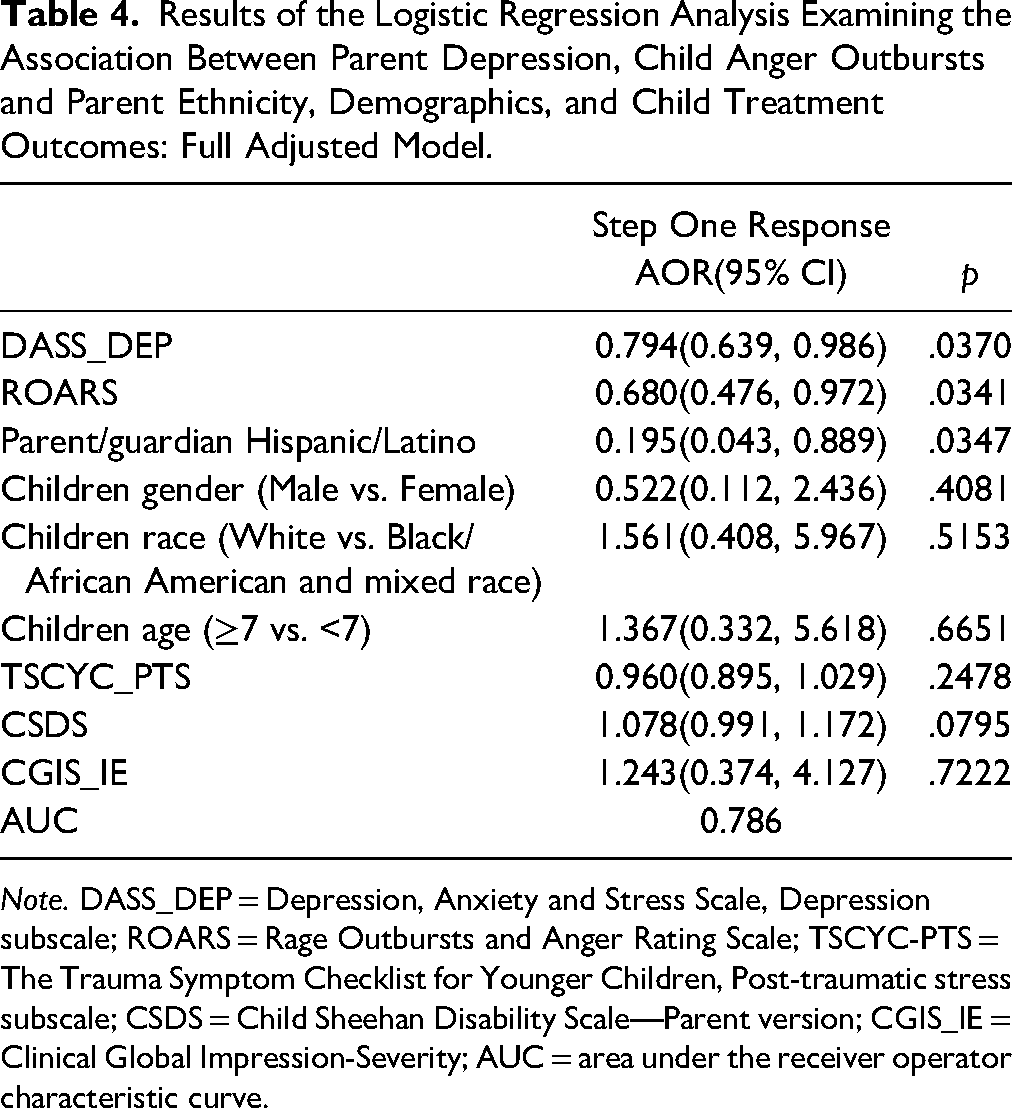
Note. DASS_DEP = Depression, Anxiety and Stress Scale, Depression subscale; ROARS = Rage Outbursts and Anger Rating Scale; TSCYC-PTS = The Trauma Symptom Checklist for Younger Children, Post-traumatic stress subscale; CSDS = Child Sheehan Disability Scale—Parent version; CGIS_IE = Clinical Global Impression-Severity; AUC = area under the receiver operator characteristic curve.
Because Hispanic/Latino families were less likely to respond to Step One we conducted a post hoc analysis to examine responder status after Step One, and after Step Two. There were 20 Hispanic/Latino parents/caregivers that completed the assessment after Step One and 50% responded to Step One compared to 76.74% non-Hispanic or Latino responders (n = 33 responded and 10 did not respond) indicating a significant association between parent ethnicity and response to Step One (p = .034). At the post-treatment assessment, 90% of the Hispanic or Latino children responded (n = 18 responders, and n = 2 non-responders) compared to 100% of the non-Hispanic or Latino children (n = 37), and there were no significant differences between parent ethnicity and treatment response status (p = .104).
Discussion and Applications to Practice
SC-TF-CBT provides an alternative treatment approach to therapist-led TF-CBT such that care is stepped with a parent-led therapist-assisted treatment as Step One and therapist-led standard TF-CBT as Step Two. Not all children will respond to Step One, thus it is important to learn what characteristics suggest the likelihood of a child needing standard TF-CBT so that these children might proceed directly to Step Two. Child internalizing symptoms and anticipated critical life events did not predict Step One treatment response. However, exploratory analyses suggested that the best predictors of Step One non-response were parental depression, child anger outbursts, and Hispanic/Latino parents even after controlling for child demographics (gender, race, and age), child PTS scores and severity and impairment.
We expected that baseline internalizing symptoms would predict Step One treatment response given that we found previously that child responders of Step One had lower internalizing scores post-treatment than non-responders (Salloum et al., 2022b). One possible explanation is that the interpersonal time that children received during their parent–child meetings helped the children feel less withdrawn. The in vivo activities often included going to places children had previously avoided which may have helped children's depression if children were not engaging in activities due to avoidance. Parents spending additional structured time with children and helping children with processing trauma may be a way to tailor trauma-focused treatment for children with depression.
Anticipated critical life events did not predict Step One response. However, this finding should be interpreted with caution as there were only 7 of 63 (11.11%) caregivers that anticipated having two or more critical life events occur during treatment. Critical life events (Reardon et al., 2017) and barriers that are related to finances (Bornheimer et al., 2018) have been associated with decreased participation in treatment. A number of factors may have contributed to critical life events not being a predictor of Step One treatment response. Parents may not have been able to accurately anticipate these events, or perhaps the type of event rather than the number impairs parents’ completion of Step One. Also, if parents were able to anticipate a critical life event such as loss of income or other event, they may have been able to plan for the event and the burden was minimized. Further, we do not know if therapists were aware when a critical life event occurred during Step One and if one did occur, what efforts were taken to support the family and keep them engaged in treatment. More research about the role of critical life events on Step One completion and response are needed.
In terms of child and parent outcome variables, one parent measure and one child measure emerged as predictors of Step One non-response. Consistent with studies finding that parent depression is associated with poorer child outcomes in therapist-led trauma-focused treatment (Danzi & La Greca, 2021; Martin et al., 2019), parent depression was associated with 18% decreased odds of responding to Step One for each additional point on the depression subscale. While parental depression was a significant predictor of Step One response, the mean score of non-responders was only 9.58 (compared to 4.98 for responders), which is in the normal (0–9) to mild (10–13) range for the DASS-21. This suggests that even mild parental depression may be a concern.
While externalizing behaviors broadly defined did not predict response status, one specific externalizing behavior, anger outbursts, predicted 27% decreased odds of responding to Step One for each point increase. The ROARS assesses the frequency, intensity, and duration of explosive outbursts in the past week. A child's anger outbursts may make it difficult for parents to lead the parent–child meetings. The mean ROARS score of non-responders was 3.70, which is in the moderate range (4–6). The mean score of responders was 2.33, which is in the mild range (0–3). This suggests that angry outbursts do not need to be severe to potentially interfere with therapy.
The one demographic variable found to be a predictor of Step One was caregiver ethnicity as Hispanic or Latino. Of the 20 Hispanic/Latino families in SC-TF-CBT, 50% responded to Step One. Nevertheless, the post hoc analysis indicated that treatment was effective for the majority of the Hispanic/Latino families that stepped up. Of importance to note, the parent–child activity book was provided in English which may have contributed to Hispanic/Latino parents stepping up if English was not their primary language. Learning about what might have been different for these families that did engage with the treatment might help inform future implementation of Step One with Hispanic/Latino families.
The current study findings have direct implications for practice. Children with problematic anger outbursts and caregivers with even mild depression might benefit from starting with therapist-led treatment. Both the DASS depression subscale and the ROARs are brief measures with simple scoring instructions, which community clinicians could easily administer at baseline to determine the suitability of starting with Step One. Hispanic/Latino families might also consider starting with therapist-led treatment until further modifications of Step One demonstrate success with Hispanic/Latino families. If caregivers or children with one of these three characteristics (i.e., child problematic anger outburst, caregiver depression, and caregiver being Hispanic/Latino) want to start with Step One due to factors such as preference, time, and cost, it is important to monitor treatment closely and allow for an open option to step up at any time.
Step One materials including the therapist manual as well as the parent–child Stepping Together activity should be translated into Spanish. Cultural adaptations that have been incorporated in standard TF-CBT (see de Arellano et al., 2012) also should be integrated into Step One. For example, Step One should incorporate familismo (a family focus) rather than just one parent leading the child's treatment. In addition, parenting strategies that are congruent with parents’ beliefs should be incorporated or explained in a way that is congruent with the family's beliefs such as framing behavioral interventions as a way to increase respeto (respect) from the child.
Limitations
Study limitations should be noted. First, we did not monitor for critical life events during treatment. The occurrence of a new trauma was assessed during Step One but critical life events that could not be anticipated may have occurred during treatment. Future studies should assess for critical life events during Step One and at outcome assessment. Second, the sample size was limited. Notably, there were only nine children with extremely high internalizing scores (e.g., >71) which may have limited the ability to detect an effect. Future studies with larger samples are needed. Finally, all of the child measures on symptoms and behavioral problems were via parent report as were the parent distress measures.
Conclusion
SC-TF-CBT is designed to be an alternative delivery system to address some treatment barriers. While research indicates that approximately 70% respond to Step One (Salloum et al., 2022a), learning who is most likely to respond to Step One and who would be better served by more intensive therapist-led trauma-focused treatment is critical. Understanding the characteristics of children and parents most suited for Step One treatment might also minimize drop out. The current study explored demographic variables (e.g., race, ethnicity, age, gender, and income), trauma-related variables (interpersonal trauma vs. non-interpersonal trauma, and polytrauma vs. non-polytrauma), child outcomes (child PTSS, impairment, internalizing, externalizing, severity, sleep disturbances, and anger outbursts), and parent outcomes (PTSS, depression, and parenting stress) as possible predictors of Step One non-response. Parent depression, child angry outbursts, and Hispanic/Latino caregiver were the best predictors of Step One non-response. Future research and development of Step One might consider how to tailor Step One to address these three characteristics.
Footnotes
Acknowledgements
The Crisis Center of Tampa Bay and all of the community-based agencies are gratefully acknowledged for their partnership on this study. The authors thank the caregivers/parents and children for their participation. They also thank Tanya K. Murphy, MD, Wei Wang, PhD, Stephanie Evans, LCSW, Jessica Turpin, MPH, Zoe Blair-Andrews, BA, and Yuan Xu, MPH for their assistance with this project.
Clinical Trial Registration Information
Stepped Care for Children after Trauma: Optimizing Treatment: https://clinicaltrials.gov: NCT02537678.
Data Statement
Some data used in preparation of this article reside in the National Institute of Mental Health (NIMH) Data Archive (NDA). NDA is a collaborative informatics system created by the National Institutes of Health to provide a national resource to support and accelerate research in mental health. For demographics and the primary outcomes see Dataset identifier(s): NIMH Data Archive Digital Object Identifier (DOI: 10.15154/1520865). This manuscript reflects the views of the authors and may not reflect the opinions or views of the NIH. Given that the ethical committees agree, additional data used in the current study are available on reasonable request from the principal investigator of the study.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Alison Salloum receives grant support from The Norwegian Centre for Violence and Traumatic Stress Studies, Department of Education, Office of Special Education and Rehabilitative Services and royalties from Taylor and Francis. Further, Dr. Salloum is a co-author of Stepping Together a treatment manual used in stepped care TF-CBT and holds a licensing agreement with Guilford Press for adaptation of some of the handouts and worksheets in the manual. Dr. Salloum is also a national trainer for TF-CBT. Yuanyuan Lu receives grant support from National Cancer Institute. Omar Ali has no conflicts to disclose. Dr. Henian Chen receives grant support from NIH (NCI, NIMH, and NICHD), and Florida Department of Health. Dr. Kristen Salomon receives grant support from NIH and NSF. Dr. Judith A. Cohen receives grant support from NIMH, the Substance Abuse and Mental Health Services Administration and the National Institute of Child Health and Human Development, and royalties from Guilford Press, Up To Date and the Medical University of South Carolina related to TF-CBT books and training materials. Dr. Michael S. Scheeringa receives royalties from Guilford Press, Central Recovery Press, and Psychology Today. Dr. Quast has no conflicts to disclose. Dr. Eric Storch receives grant support from NIH, the Ream Foundation, Greater Houston Community Foundation, International OCD Foundation, and Texas Higher Education Coordinating Board. He receives book royalties from Elsevier, Springer, American Psychological Association, Jessica Kingsley, Oxford, and Lawrence Erlbaum. He was a consultant for Levo Therapeutics; he currently consults for Biohaven and Brainsway. He owns stock in NView. He co-founded/owns Rethinking Behavioral Health, which is a behavioral health consulting group.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health and the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health for use of the Clinical and Translational and Preclinical-Clinical Core facilities (grant number R01MH107522, P50HD103555). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NMH or National Institutes of Health.