
Abstract
Introduction
Ageing is a universal and natural process of life that is usually accompanied by a higher possibility of suffering from multiple health disorders (Akosile et al., 2018). In most countries, old age begins when the active contribution is no more possible, and this corresponds to ages of 60 to 65 (McGuire et al., 2006). Due to economic progress, technological advances, and improved healthcare, the human lifespan is increasing across the world (Tabah et al., 2010). This has led to a profound and irreversible demographic shift, as older people are living longer and healthier than ever before (United Nations, 2013; World Health Organisation et al., 2011). The proportion of people aged 60 and over worldwide is thus growing faster than any other age group (González-Celis & Gómez-Benito, 2013). Between 1970 and 2025, there is an expected 223% increase in the global number of older adults; and this figure is expected to double by the year 2050, with 80% of these older adults living in developing countries (González-Celis & Gómez-Benito, 2013). This demographic shift has been described as both a major societal achievement and a challenge (Chachamovich et al., 2008), with the associated shift ensuring a profound impact on a broad range of economical, political, and social conditions (Figueira et al., 2008). Increased longevity has brought with it a longer period of morbidity that can adversely impact the quality of life (QoL) of older adults. Consequently, great attention is being paid to age-related morbidities and the needs of older adults, and one important area usually assessed is QoL (Chachamovich et al., 2008).
QoL, defined as the perception of the individual's position in life, expectations, standards, and concerns (Liu et al., 2013; Pernambuco et al., 2012), can be adversely impacted by ageing processes (Chou et al., 2012; Gureje et al., 2008). It is a very broad and dynamic construct that takes cultural, social, physical, economic, psychological, and environmental individuality into consideration (Figueira et al., 2010). QoL of older adults has been reported to be associated with several factors including age, financial status, health, functional disability, and social support and networks (Akosile et al., 2014, 2018; Jakobsson et al., 2007). According to Gerritsen et al. (2010), clinical indicators only are not sufficient to describe health status; consequently, it is increasingly recognized that the impact on QoL of disease and treatment of disease and its consequences should be taken into account when assessing health status and evaluating treatment outcomes. In order to ensure an adequate and reliable assessment of QoL, standardized valid, and reliable QoL scales need to be made available.
Many standardized QoL scales are available in the literature. Some are generic, while others are disease- or population-specific scales. The commonest generic ones are the World Health Organization QoL Questionnaire-BREF (WHOQOL-BREF) and the Short Form 36-Item Health Status Questionnaire (Liu et al., 2013). There seem to be only three older-adults-specific QoL scales: the Older People's QoL Questionnaire, the World Health Organization Quality of Life Questionnaire-version for older adults (WHOQOL-OLD), and the Control, Autonomy, Satisfaction, Pleasure-19 items (Bowling & Stenner, 2011). Generic scales offer opportunities for comparison of data across populations and disease conditions; but, unlike population-specific scales, may not capture the in-depth peculiarities of different populations and disease conditions (Chachamovich et al., 2008; González-Celis & Gómez-Benito, 2013; Pernambuco et al., 2012). Hence, for in-depth and more accurate measurement of QoL among older adults, QoL scales primarily developed for older adults will logically be preferred to generic scales.
The WHOQOL-OLD is a 24-item, 6-facet module, self-report instrument specifically developed to assess the QoL of older adults, thus ensuring that important areas concerning old age are covered by the instrument (Chachamovich et al., 2008; González-Celis & Gómez-Benito, 2013; Pernambuco et al., 2012). Unlike other older adults-specific QoL scales, the WHOQOL-OLD was designed to be suitable for cross-cultural comparisons, and it exists in over 20 languages (Bowling & Stenner, 2011). It has acceptable psychometric properties (Conrad et al., 2014; Peel et al., 2007). In as much as cross-cultural variations were taken into consideration during the development of the WHOQOL-OLD, just like many other scales, the original WHOQOL-OLD was written in the major international languages (English Language inclusive). This makes it difficult to administer the WHOQOL-OLD among older adults that are not literate in these languages. This has necessitated the cross-cultural adaptation (which usually includes initial translation, synthesis, back translation, expert committee review, pilot testing, and psychometric evaluation) of the scale in different languages and cultures (Arafat et al., 2016; Beaton et al., 2000).
With the Nigerian adult illiteracy level in English language standing at 42.1% (National Bureau of Statistics, 2018), many Nigerian older adults will not be able to complete the English version of the WHOQOL-OLD, thus necessitating the availability of QoL measures specific to Nigerian culture and languages. A previously validated instrument also does not necessarily mean it is valid in another time, culture, or context (Beaton et al., 2000). Despite this, no available QoL scale is primarily developed for use in a Nigerian environment. Hence, stakeholders in Nigerian older adults’ well-being are left with either of two choices: developing new instruments or cross-culturally adapting the existing ones. The latter choice is usually better as it is more economical and also allows for cross-cultural comparisons across populations and studies both nationally and internationally (Beaton et al., 2000). Consequently, attempts had been made previously to cross-culturally adapt and validate some generic QoL measures (the WHOQOL-BREF and the SF-36) in Nigerian languages (Akinpelu et al., 2006). No older adult-specific QOL scale has been adapted and validated in Nigerian culture. The present study was therefore designed to cross-culturally adapt and validate the English version of WHOQOL-OLD among Igbo older adults in Anambra State. Igbo is one of the three major native languages in Nigeria, the most populous black nation (Odinye & Odinye, 2010). It was hypothesized that the Igbo version of the WHOQOL-OLD would display acceptable psychometric properties.
Methods
This study involved cross-cultural adaptation and validation of the WHOQOL-OLD among consecutively recruited Igbo community-dwelling older adults in a conveniently selected community, Nnewi in Anambra State, Southeast Nigeria. Nnewi is a semi-urban commercial and agricultural community with a population of about 1,050,860 in 2020 (World Population Review, 2020). The study was approved by the Ethics Committee of Nnamdi Azikiwe University Teaching Hospital, Nnewi. Participants of this study were male and female healthy older adults (65 years and above) who were residents of the Nnewi community. They were well-oriented in time, place, and position, and had no communication impairment. The participants varied considerably in their marital, educational, and employment statuses. Those that were involved in the pretesting and cognitive debriefing interview could understand both Igbo and English languages. Informed consent was obtained from each participant after the objectives and the procedures of the study had been thoroughly explained to them. Participants gave their consent by either signing or thumb-printing the consent form. The socio-demographic variables (age, gender, level of formal education, marital status, employment status, and period of living in the community) were then recorded. Data collection was done at participants’ homes or churches and was done from February to July 2018. A sample size of 109 has a 90% power to detect a moderate change of 0.3 at an alpha level of significance of 0.05. The sample size was calculated using G* Power 3.0.10 (Faul et al., 2007).
Research Instrument
The World Health Organization Quality of Life Questionnaire-version for older adults (WHOQOL-OLD), a 24-item QoL measure, was developed by the WHOQOL Group as an add-on module to their QoL measures (WHOQOL-100 and WHOQOL-BREF), specifically for use with older adults. The WHOQOL-OLD 24 items are assigned to six facets: “Sensory Abilities” (SAB), “Autonomy” (AUT), “Past, Present and Future Activities” (PPF), “Social Participation” (SOP), “Death and Dying” (DAD) and “Intimacy” (INT) (Conrad et al., 2014). Response scales are all 5-point (1–5) but vary in their wording (“Not at all” to “An extreme amount”/“Completely”/“Extremely”; “Very poor” to “Very good”; “Very dissatisfied” to “Very satisfied”; “Very unhappy to Very happy”) (Bowling, 2009). Each of the facets has 4 items, thus for all facets the score of possible values can range from 4 to 20, provided all items of a facet have been completed. The scores of these six facets or the values of the 24 single items of the WHOQOL-OLD module can be combined to produce a general (“overall”) score for QoL in older adults, denoted as the WHOQOL-OLD module “total score” (28). The total score ranges from 24 to 120 with a higher score denoting better QoL. The WHOQOL-OLD has acceptable psychometric properties with evidence of acceptable internal consistency (Cronbach's alpha = .61–.93) and constructs validity (Conrad et al., 2014; Peel et al., 2007).
Procedure for Data Collection
The procedure for this study followed the guidelines for cross-cultural adaptation by the American Academy of Orthopedic Surgeons as developed by Beaton et al. (2000). The procedure for the study was in three phases. Phase one involved forward translations of the English version of WHOQOL-OLD to the Igbo language; synthesis of the translations; and backward translations of the synthesized Igbo version to the English language. Phase two involved adaptation of the WHOQOL-OLD to the Igbo culture and environment. Phase three involved validation of the adapted version of the WHOQOL-OLD.
Phase One: Translation Stage
This phase involved two forward translations of the WHOQOL-OLD from English to the Igbo language by a physiotherapist and a graduate of Igbo language who were bilingual and have the Igbo language as their mother tongue. Translator 1 (physiotherapist) was aware of the concept (QoL among older adults) being examined in the English version of the WHOQOL-OLD, while translator 2 (linguist) was not aware of the concepts being quantified, and had no medical or clinical background. The second translator offered a translation that reflected the language used by the population. The two translators and a recording observer synthesized the two translations to produce a common translation (T-12) with a written report on each of the issues that were addressed and how they were resolved. The T-12 version was translated back into the English language by two translators (physiotherapy lecturers) who did not know about the original version. This process was to make sure that the translated version reflected the same item content as the original version. Ideally, the two backward translators were supposed to be native speakers of the English language. However, no such translators were available, thus necessitating the use of experienced physiotherapy lecturers. This kind of improvisation is common in literature.
Phase Two: Adaptation Stage
The WHOQOL-OLD was adapted to Igbo culture and environment by a panel of experts at a meeting. The experts comprised the forward and back translators, four physiotherapy lecturers experienced in the process of cross-cultural adaptation, and a lay person. The lead author acted as the moderator while the third author acted as the secretary. All the experts were familiar with the Igbo culture and environment and had lived and worked in Igbo land for at least eight years. The semantic, experiential, idiomatic, and conceptual equivalences of the items on the WHOQOL-OLD in Igbo culture were provided by the experts where necessary. The pre-final Igbo culture-adapted version of the WHOQOL-OLD was administered through interviews to 30 Igbo individuals recruited from the conveniently selected Okofia communities in Nnewi. The 30 participants also participated in a cognitive debriefing interview. The participants were queried on comprehensiveness, comprehensibility, and clarity of the items and response options on the WHOQOL-OLD. They were also queried on whether each item tapped into relevant areas in Igbo culture and environment. Each participant was expected to answer a "YES" or a "NO" to each query. Any query with a percentage "YES" of less than 80% would warrant modification of the corresponding item or response option. Findings from the pre-test and cognitive debriefing interview were reviewed by the expert panel at a second meeting to produce the final Igbo culture adapted WHOQOL-OLD.
Phase Three: Validation Phase
This was the final phase of the process. It involved the testing of the final Igbo version of the PASE (I-WHOQOL-OLD). The research instruments (the I-WHOQOL-OLD and the E-WHOQOL-OLD) were administered to apparently healthy older adults residing in Nnewi North LGA who understood both English and Igbo Languages. According to Consensus-based Standards for the selection of health Measurement Instruments (COSMIN) a sample size of ≥100 is very good for ascertaining structural validity, internal consistency, and construct validity of a scale (Consensus-based Standards for the Selection of Health Measurement Instruments, 2020). A sample size of 109 was therefore used in the present study. Using G* Power 3.0.10. A software, with a sample size of 109 has a 90% power at a 0.05 alpha level of significance (Faul et al., 2007). The sequence of administration of the instruments was done by simple randomization. Participants who picked “I” responded to the Igbo language version of the WHOQOL-OLD while those who picked “E” responded to the English version of the WHOQOL-OLD first and vice-versa.
Analysis of Data
The obtained data were analyzed using Statistical Package for Social Sciences (version 21). The demographic and clinical variables as well as the scores from the questionnaires were summarized using frequency counts, percentages, range, mean, and standard deviation. The questionnaire scores were tested for normality using the Kolmogorov–Smirnov test. Mann–Whitney U was used to compare the participants’ scores on both the I-WHOQOL-OLD and the E-WHOQOL-OLD. The Spearman rank order correlation test was used to estimate the level of correlation between participants’ scores on the two versions of the WHOQOL-OLD (in order to provide evidence of known-group validity of the I-WHOQOL-OLD). Bland and Altman plotting was used to assess the heteroscedasticity of scores on the I-WHOQOL-OLD and the E-WHOQOL-OLD. The convergent and divergent validities of the I-WHOQOL-OLD were also calculated using the Spearman rank order correlation test. For convergent validity, it was expected that item scores would correlate better with their domains. For divergent validity, items were expected to correlate less with other domains.
The questionnaire was tested for ceiling and floor effects. The questionnaire would be regarded as having a ceiling or floor effect if more than 20% of the participants scored maximum and minimum scores, respectively (Power et al., 2005). Cronbach's alpha was used to determine the internal consistency of the items on the I-WHOQOL-OLD. A Cronbach's alpha of 0.70 or higher was supposed to indicate adequate internal consistency. The standard error of the mean (SEM) of the I-WHOQOL-OLD was also calculated. The SEM was used to calculate the minimal detectable change (MDC) which is a statistical estimate of the smallest change detected by a measure that corresponds to a noticeable change in ability that is not due to measurement error. The MDC was calculated using the formula: MDC = 1.96 x SEM x √2 (De Vet et al., 2006; Okoye et al., 2020a). Factor analysis (principal component analysis) was used to determine the structural validity of the I-WHOQOL-OLD. The suitability of the data for factor analysis was assessed, and the following criteria had to be met before factorial analysis could be performed: the Kaiser–Meyer–Olkin measure of sampling adequacy must exceed the recommended value of 0.6; Bartlett's test of sphericity must reach statistical significance; the coefficients of correlation of each of the items on the scale with one another should exceed the recommended value of 0.3. The alpha level was set at .05.
Results
Translations and Cross-Cultural Adaptation Process of the WHOQOL-OLD
The translation was uncontroversial, with all the items on the E-WHOQOL-OLD being judged by the expert panel as relevant for measuring QoL among Igbo older adults living in South-eastern Nigeria or Igbo land. However, it was difficult translating the word “senses” in item 1 as it has no exact Igbo equivalent. In order to reduce ambiguity, the panel suggested that the word “senses” still be retained in parentheses in the Igbo version. The thirty older adults (43.3% males; mean age = 70.56
Validation of Igbo Culture Adapted WHOQOL-OLD Measure
Socio-Demographic Distributions of the Participants
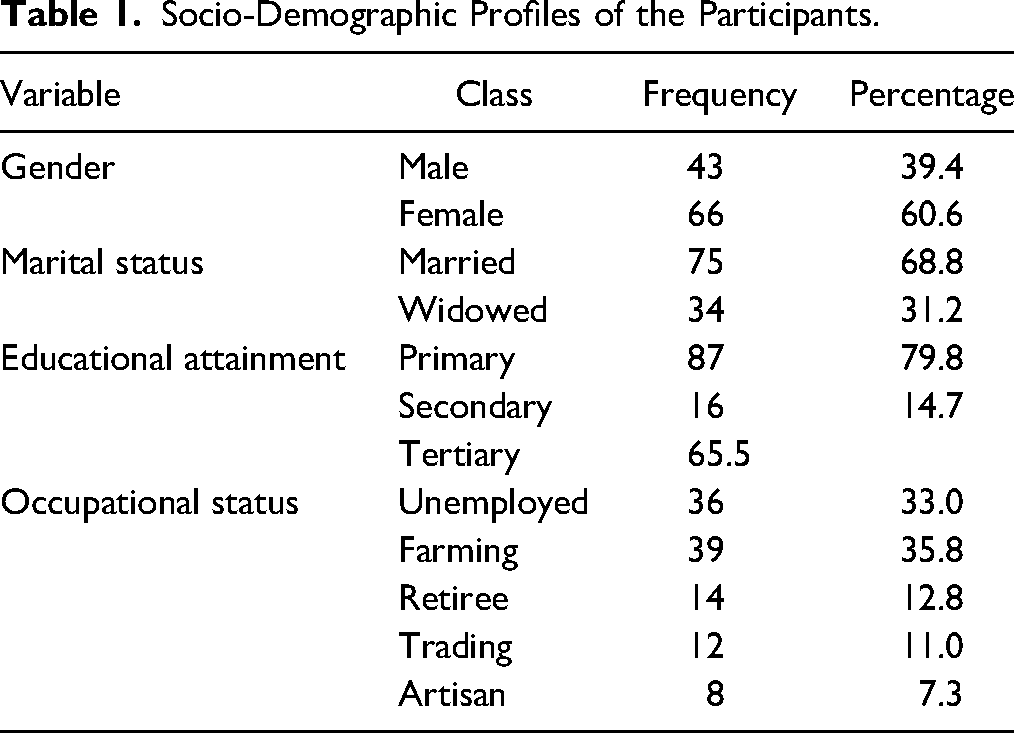
A total of 109 older adults (39.4% males; mean age = 73.04
Socio-Demographic Profiles of the Participants.
Participants’ Scores on E-WHOQOL-OLD and I-WHOQOL-OLD
The mean domain and total scores of the participants on the E-WHOQOL-OLD and I-WHOQOL-OLD are similar and are displayed in Table 2. A comparison between the corresponding total and domain scores on the E-WHOQOL-OLD and the I-WHOQOL-OLD using the Mann–Whitney U test showed no significant difference in any of the scores (p > .05) thus indicating that the two instruments produced equivalent scores.
Comparison of Participants’ Scores on the English and Igbo Versions of the World Health Organization Quality of Life Questionnaire-Version for Older Adults.
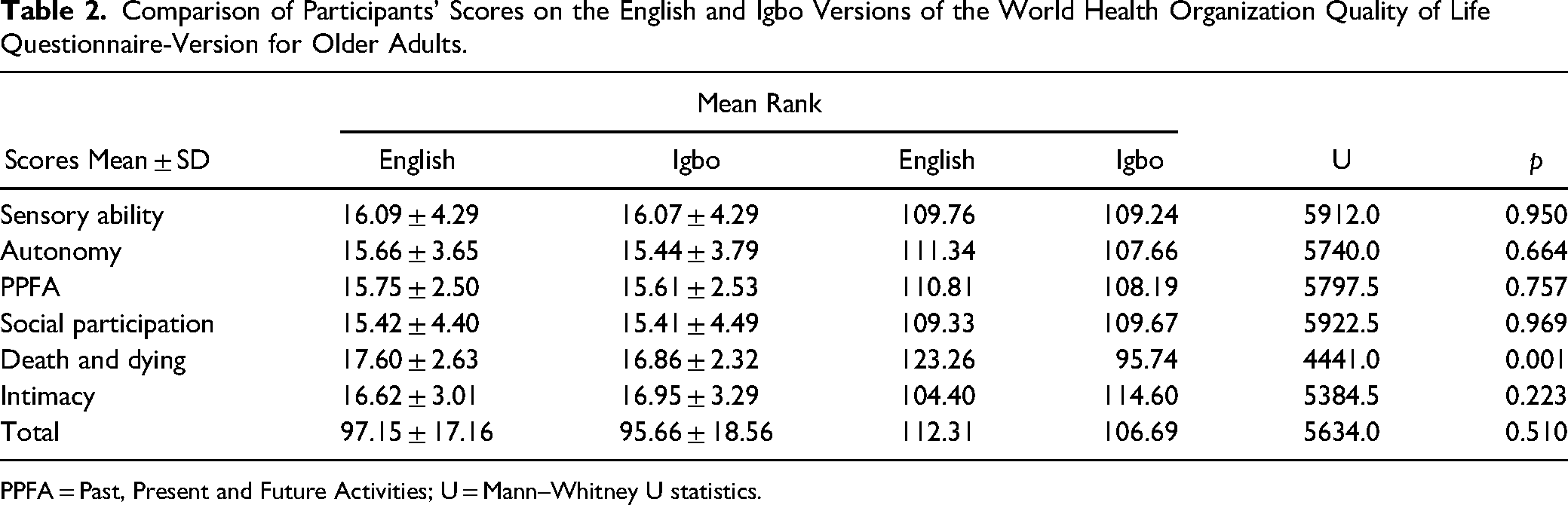
PPFA = Past, Present and Future Activities; U = Mann–Whitney U statistics.
Psychometric Properties of I-WHOQOL-OLD
Known-group Validity
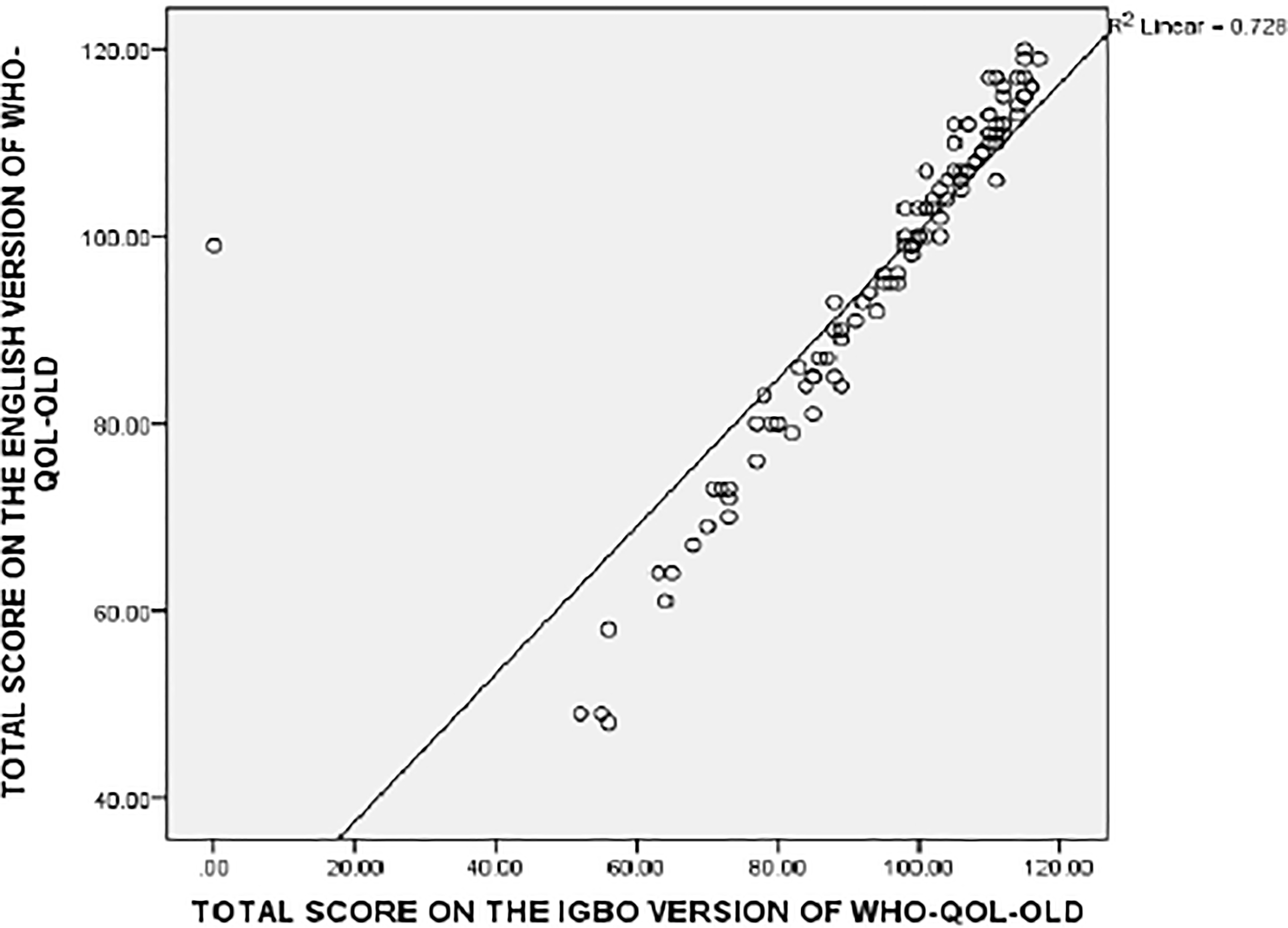
Scatter diagram for the correlation between total scores on the English and the Igbo versions of the world health organization quality of life questionnaire-version for older adults.
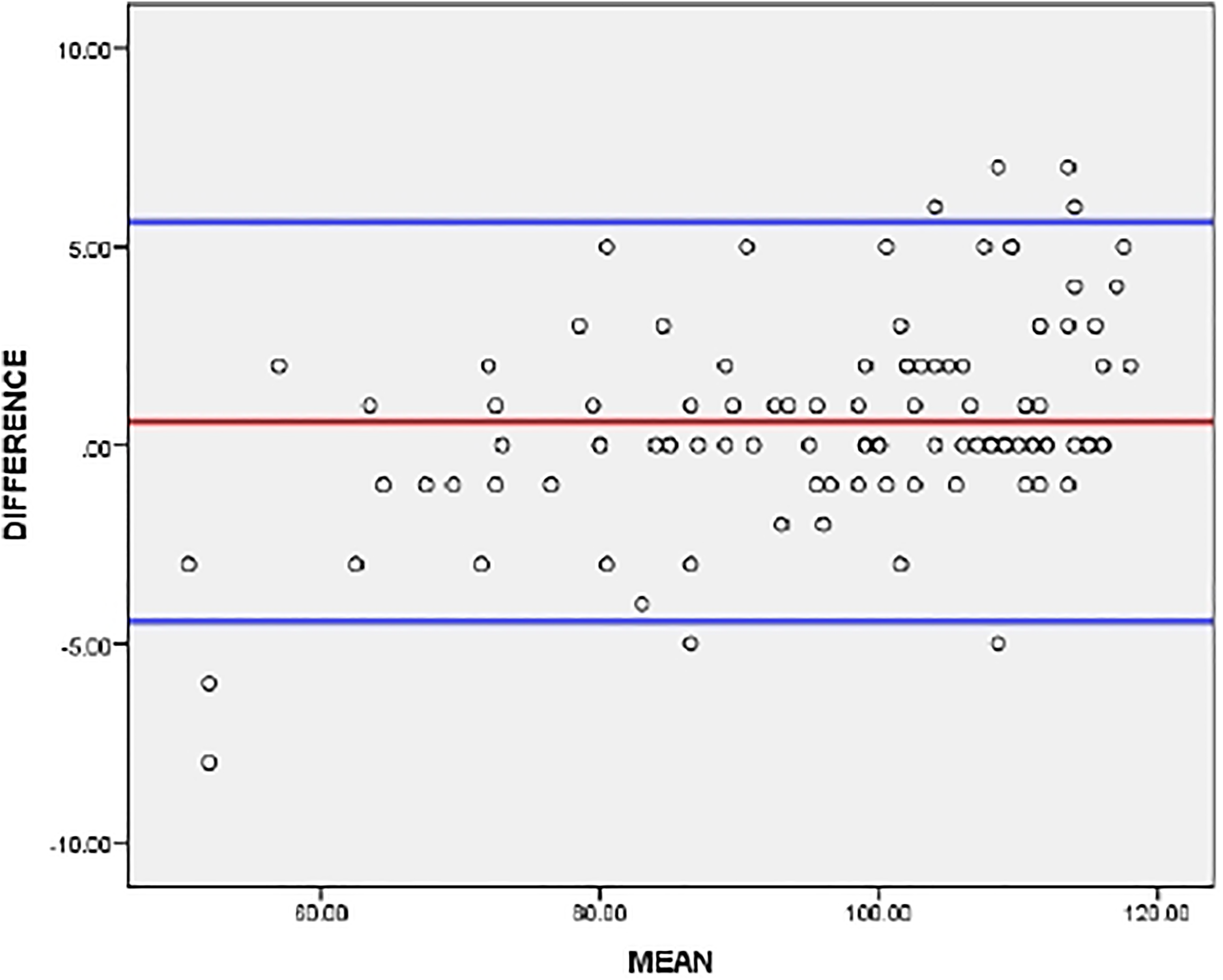
Bland Altman's plot indicating the heteroscedasticity of scores on the English and the Igbo versions of the world health organization quality of life questionnaire-version for older adults.
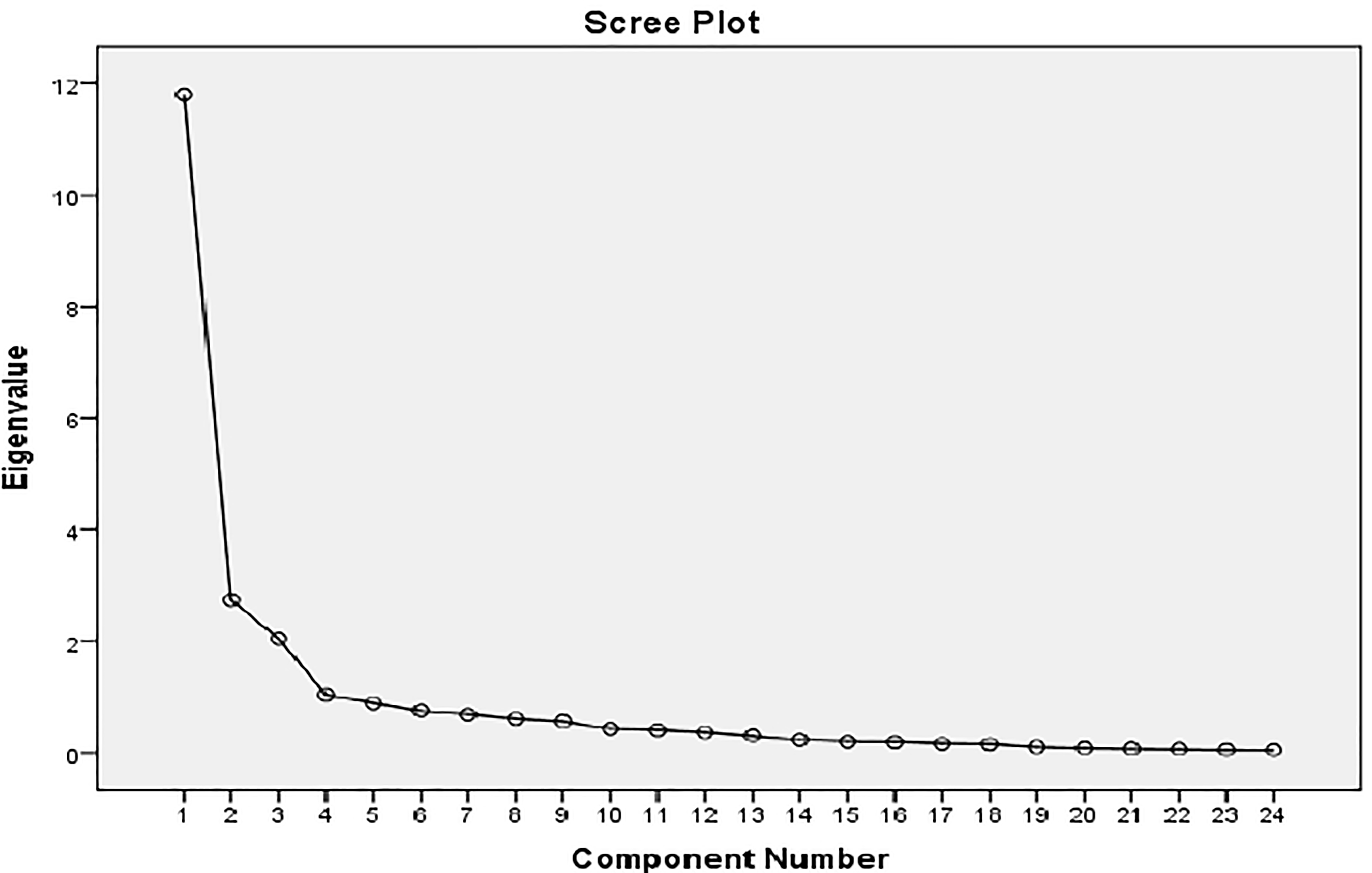
Scree plot indicating the factors present following factorial analysis of the Igbo version of the world health organization quality of life questionnaire-version for older adults.
Domain by Domain Correlation Between the Domains in the Original English and Igbo Version of WHOQOL-OLD Using the Spearman Rank Order of Correlation.
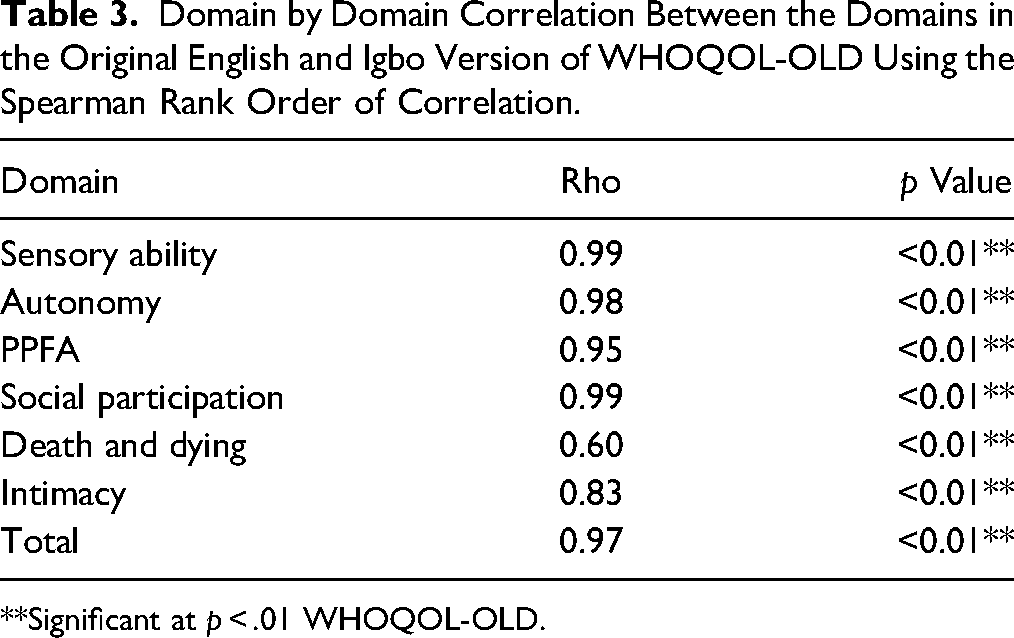
**Significant at p < .01 WHOQOL-OLD.
Ceiling and Floor Effects: No participant had either the highest or lowest total scores on the I-WHOQOL-OLD indicating that the instrument had no ceiling or floor effects. None of the domain scores of the I-WHOQOL-OLD displayed a significant floor effect. However, sensory abilities (33.0%), social participation (22.9%) and intimacy (29.6%) domains exhibited a significant ceiling effect (Table 4).
Internal Consistency, Ceiling and Floor Effects, Standard Error of Mean and Minimal Detectable Changes of Total and Domain Scores on the I-WHOQOL-OLD.
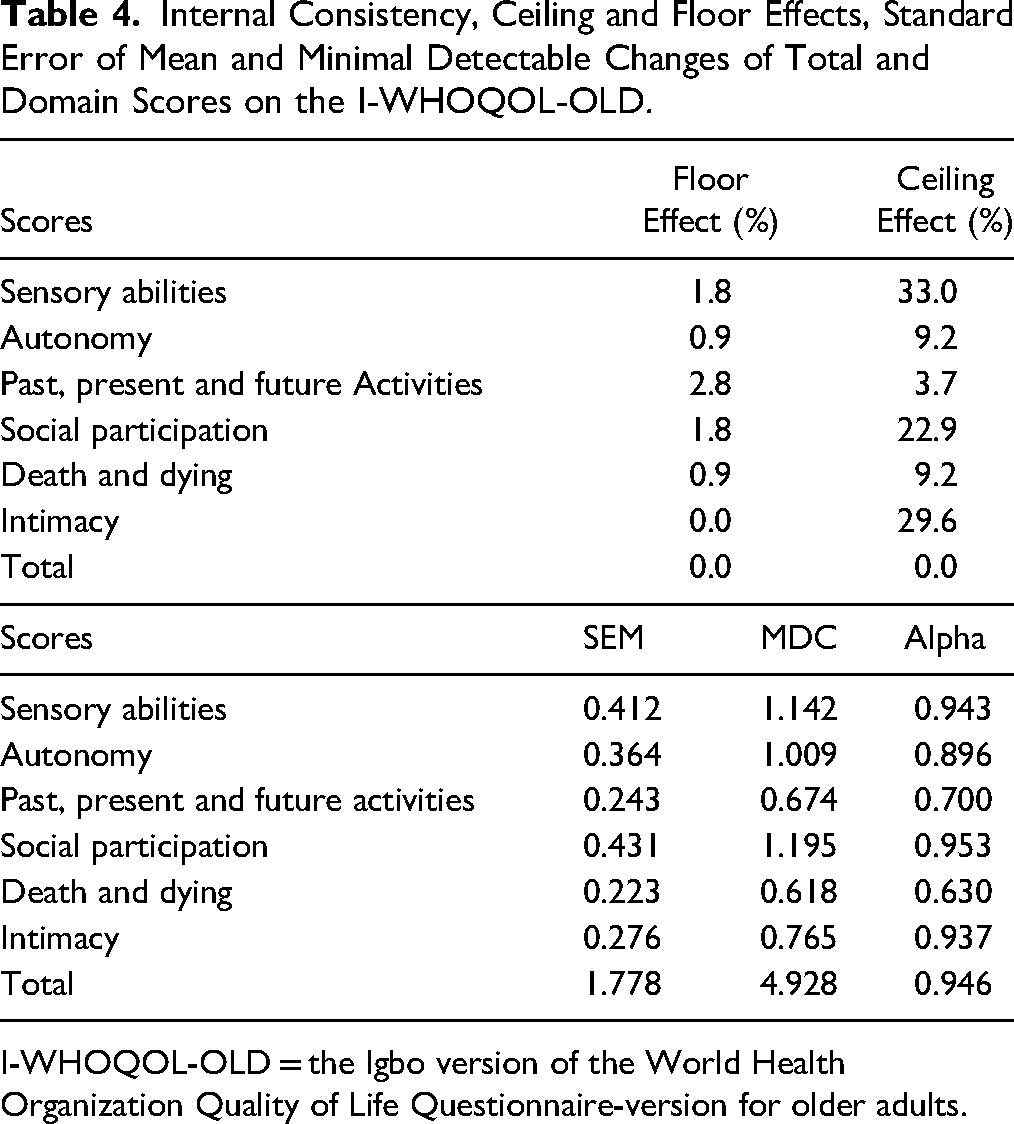
I-WHOQOL-OLD = the Igbo version of the World Health Organization Quality of Life Questionnaire-version for older adults.
SEM and MDC: The MDC of the total score on the I-WHOQOL-OLD was 4.928 which is the smallest change detected by the I-WHOQOL-OLD that corresponds to a noticeable change in QoL which is not due to measurement error. The MDC of the domains of the I-WHOQOL-OLD ranged from 0.618 to 1.195 with the death and dying and the sensory abilities domains having the lowest and the highest scores, respectively (Table 4).
Internal Consistency: The internal consistency coefficient of all the items on the I-WHOQOL-OLD which was estimated by considering the 109 participants in the study by means of Cronbach's alpha was excellent and had a value of 0.946 thus indicating that the items on the I-WHOQOL-OLD measure different aspects of the same construct. The internal consistency of the domains ranged from 0.630 (fair) to 0.953 (excellent) with the death and dying and social participation domains having the least and highest scores respectively (Table 4).
Convergent and Divergent Validities: All the items correlated highest with their domains except item 12 (To what extent are you satisfied with your opportunities to continue achieving in life?) that correlated better with autonomy (rho = 0.865) and social participation (rho = 0.864) domains than its domain (Past, Present and Future Abilities domain; rho = 0.844). Items (6, 7, 8, and 9) within the death and dying domain displayed the best convergent and divergent validities as they only displayed a significant correlation with their domains, thereby making the death and dying domain the most distinct domain. This was followed by the intimacy domain. There were significant overlaps between the remaining four domains (Sensory Abilities; Autonomy; Past, Present, and Future Abilities; and Social Participation) as each domain's constituting items still correlated highly with the other domains.
Structural Validity (Factor Analysis)
Inspection of the correlation matrix reveals the presence of many coefficients above 0.3 except for the four items (items 6, 7, 8, and 9) for the death and dying domain which had coefficients of < 0.3 in their correlations with items on other domains, but had coefficients of 0.3 and above in item to item correlation between themselves (death and dying items). This suggests reasonable factorability. The Kaiser–Meyer–Olkin measure of sampling adequacy was 0.906 exceeding the recommended value of 0.6, and Bartlett's test of sphericity reached statistical significance (x2 (276) = 2566, p = .0001) (Table 5).
Spearman Rank Correlation Test Showing the Relationships Between Item and Facet Scores on the I-WHOQOL-OLD.
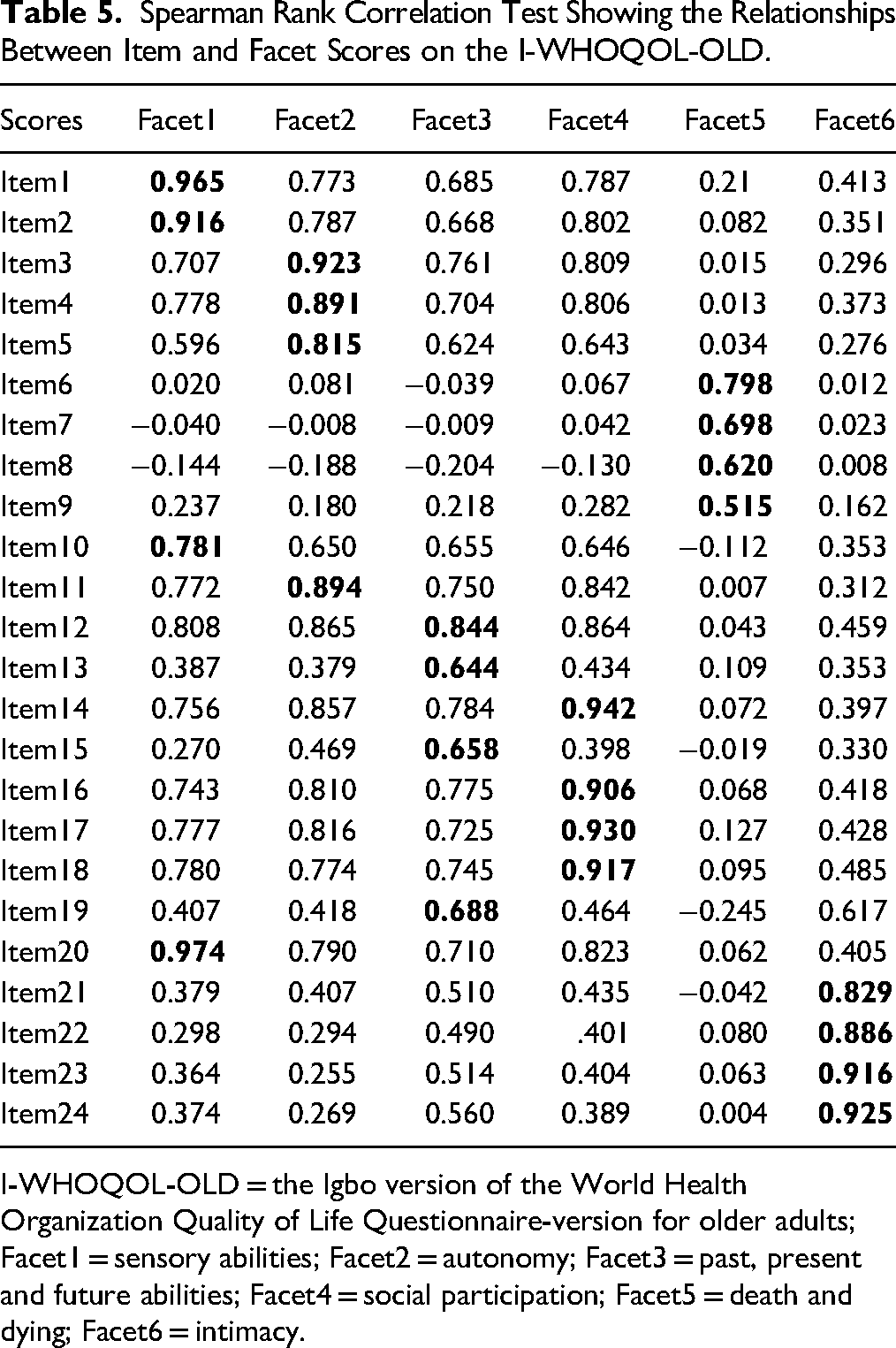
I-WHOQOL-OLD = the Igbo version of the World Health Organization Quality of Life Questionnaire-version for older adults; Facet1 = sensory abilities; Facet2 = autonomy; Facet3 = past, present and future abilities; Facet4 = social participation; Facet5 = death and dying; Facet6 = intimacy.
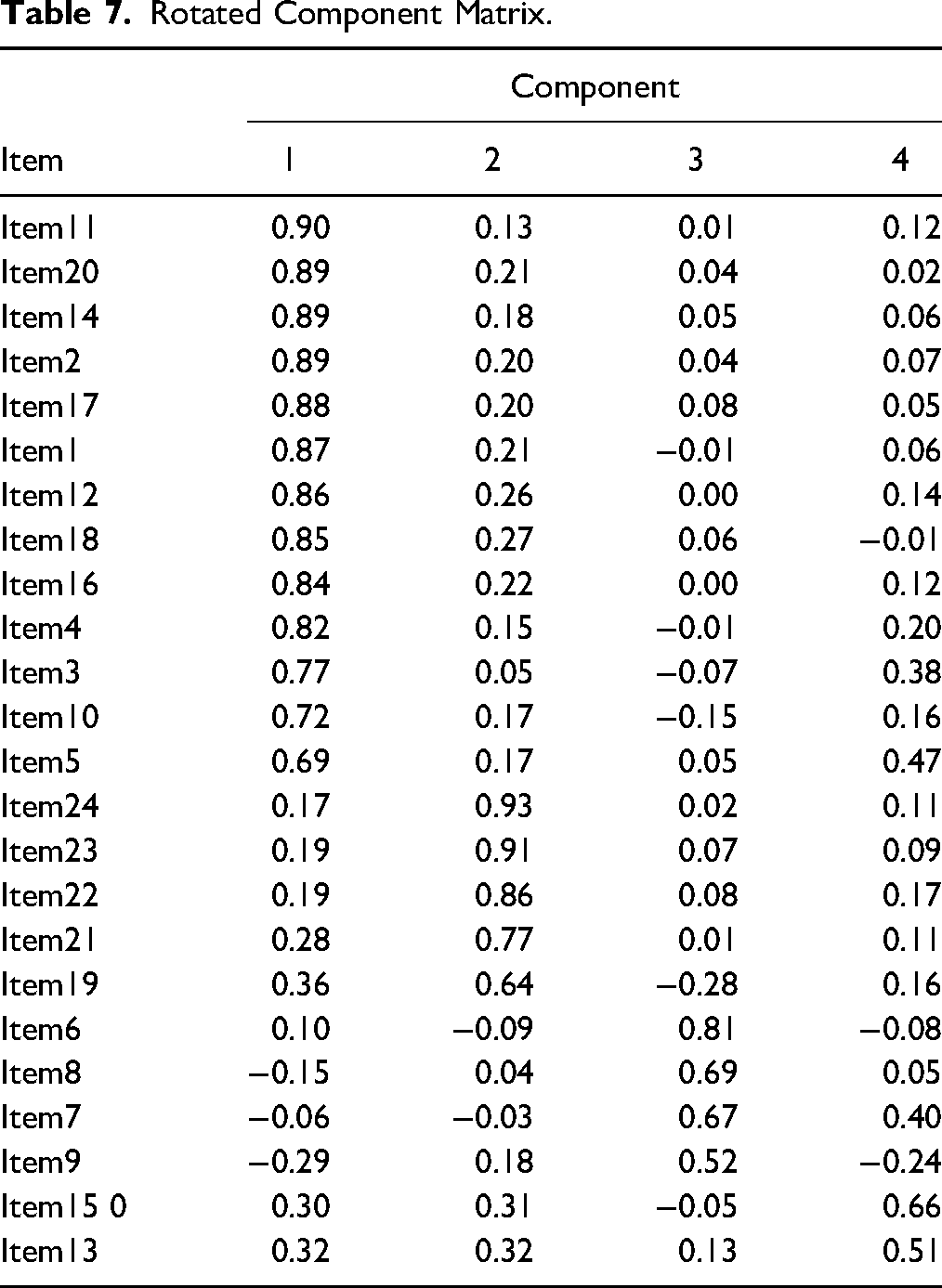
Results revealed that the factor loading of each of the 24 items on the scale after extraction was >0.3 which indicated that all the items are to be retained for use on the scale. Principal component analysis revealed the presence of four factors with eigenvalues exceeding 1, explaining 49.16%, 11.41%, 8.53%, and 4.33% of the variance, respectively. The four-component solution explained a total of 73.41% of the variance. Other factors had eigenvalues less than 1 (Table 6). The extraction is based on the Kaiser criterion, i.e, only factors that had eigenvalues greater than 1 are retained. An inspection of the scree plot revealed a kink after the second component, then a clear break after the fourth component (Figure 3). Using Catell's scree test, it is decided to retain four components for further investigation. This was further supported by the results of the Monte-Carlo parallel analysis, which showed only four components with eigenvalues exceeding the criterion values for a randomly generated data matrix of the same size (24 variables × 109 respondents). Table 4.9 reveals the items that loaded highest in each component. Thirteen, five, four and two items loaded highest in components 1, 2, 3, and 4 respectively (Table 7).
Factor Analysis for Parallel Analysis of Igbo Version of the WHOQOL-OLD.
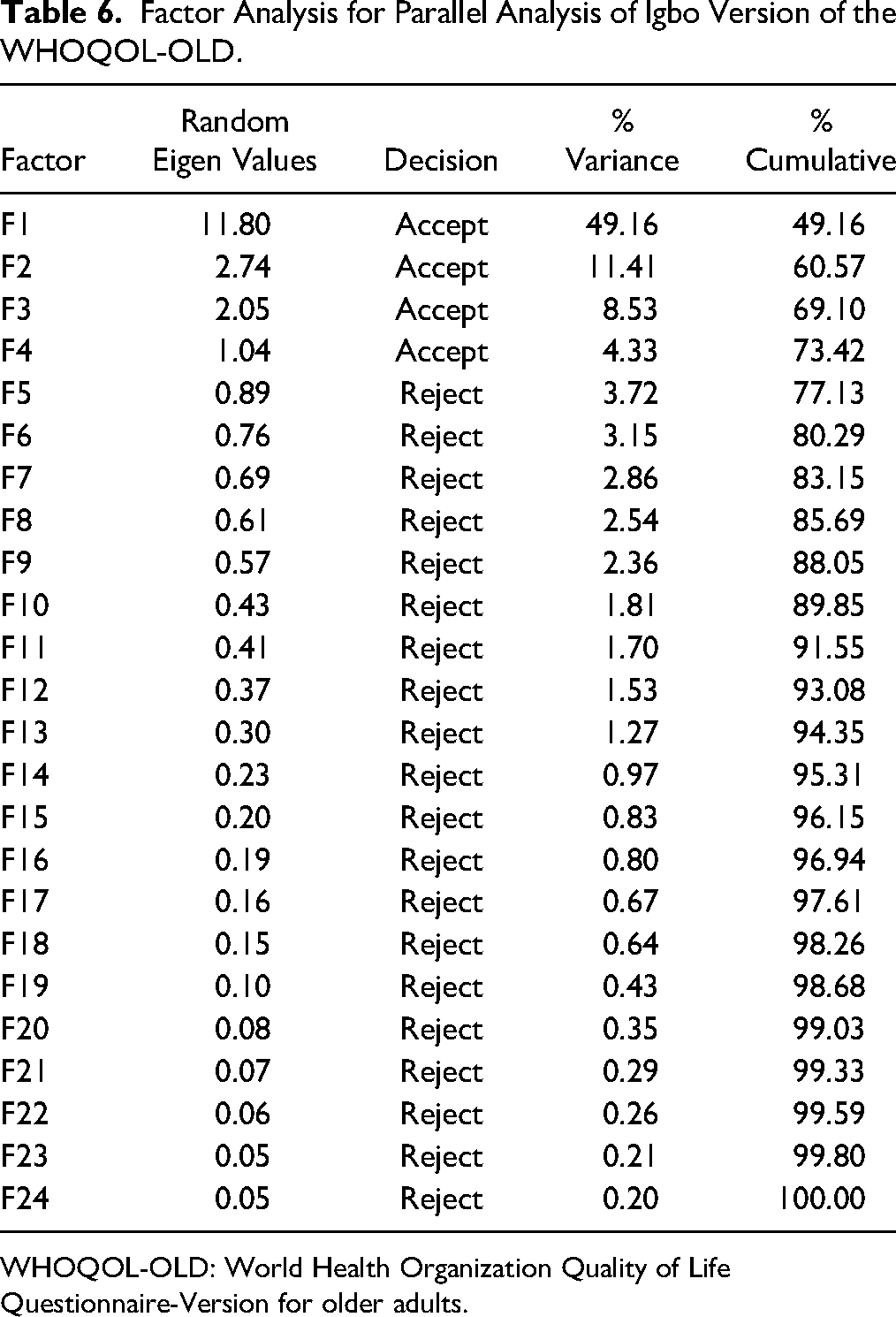
WHOQOL-OLD: World Health Organization Quality of Life Questionnaire-Version for older adults.
Rotated Component Matrix.
Discussion and Applications to Practice
This study was designed to cross-culturally adapt and validate the original English version of the WHOQOL-OLD into the Igbo language, which is one of the three major native languages in Nigeria (Laurie, 2007). An internationally acclaimed guideline (Beaton et al., 2000) was used in this study in order to minimize bias. The process of translating the original English version of WHOQOL-OLD into the Igbo version (I-WHOQOL-OLD) was uncontroversial, as the minimal difficulty was encountered in achieving an acceptable translation. The testament of the older adults that participated in the pretesting to the clarity and ease of understanding of all the items on the scale is a pointer to a decent translation of the original scale into the Igbo language. The word “sense” was retained in the I-WHOQOL-OLD since it is a frequently used word while speaking the Igbo language to the extent that even monolingual Igbo speakers usually understand its contextual meanings. Other words in this category include “busy,” “since,” and so on. In this study, with help of linguists, the central Igbo dialect was utilized. Though the Igbo language has several dialects, the central Igbo dialect is the officially accepted dialect for formal communications by both national and international bodies. This dialect is fairly understood by barely all Igbo language speakers (Nwachukwu, 2021). Hence, the results of the present study can be fairly generalized to all Igbo speakers despite the fact that the data was collected from a restricted group in Igbo land.
There were significant and excellent correlations between the participants’ total and domain scores (except in the death and dying domain which was moderate) on the two versions of the WHOQOL-OLD, suggesting an excellent (and moderate for death and dying domain) known-group validity of the I-WHOQOL-OLD. To our knowledge, the present study is the first to assess the known-group validity of the WHOQOL-OLD. These correlations suggest that the two versions of the instrument are conceptually equivalent and could therefore substitute each other. This was buttressed by the lack of significant difference in the corresponding total and domain scores (except in the death and dying domain) on the I-WHOQOL-OLD and E-WHOQOL-OLD. The lowest observed correlation coefficient in the death and dying domain is similar to previous reports in the literature on the Brazilian (Chachamovich et al., 2008), Portuguese (Fleck et al., 2006), Turkish (Eser et al., 2010), and Taiwanese (Yao & Chien, 2013) versions of the scale. This is however against what was obtained in the original version of the instrument. This usual peculiar performance of the death and dying score especially outside the western world was attributed to cultural differences between western and other populations (Eser et al., 2010). In the same vein, Gibbons & Skevington (2018) reported that previous studies using the WHOQOL instruments have shown that the relationship between individual items and the underlying QoL construct may differ between cultures. As against the western world, Africans view death as a sacred phenomenon that should not be freely discussed. As a result, most Africans are averse to discussing their death or the death of their loved ones; writing their wills; and setting out money for their own burial rites.
The global score on the I-WHOQOL-OLD neither had significant ceiling nor floor effects, indicating that the instrument is capable of differentiating individuals at the same tail end of the scoring chat. This is similar to previous reports on Persian (Rezaeipandari et al., 2020), Portuguese (Fleck et al., 2006), Spanish (Lucas-Carrasco et al., 2011), and Turkish (Eser et al., 2010), and South-African (Van Biljon et al., 2015). In the same vein, none of the domain scores of the I-WHOQOL-OLD displayed a significant floor effect, suggesting that they could still differentiate between individuals with very low QoL. However, sensory abilities (33.0%), social participation (22.9%), and intimacy (29.6%) domains exhibited significant ceiling effects, revealing that these domains might find it difficult to distinguish between participants with high QoL scores. The WHOQOL-OLD has been previously shown to display a ceiling effect (Haywood et al., 2005; Streiner et al., 2015). The I-WHOQOL-OLD showed acceptable internal consistency similar to what was obtained in previous studies (Conrad et al., 2014; Eser et al., 2010; Fleck et al., 2006; Gobbens & van Assen, 2016; González-Celis & Gómez-Benito, 2013; Liu et al., 2013). This result points toward the fact that the items on the I-WHOQOL-OLD are homogeneous, internally consistent, and assess different aspects of the same construct (QoL). Considering the maximal possible total (120) and domain (20) scores on the I-WHOQOL-OLD, the recorded MDCs seem to be small enough to ensure adequate responsiveness of the questionnaire. However, future sensitivity-to-change studies on the scale are required to ascertain its responsiveness.
Factor analysis is intimately involved with the question of validity, and it is the heart of the measurement of psychological constructs (Odole et al., 2016). It evaluates whether the collected data are in line with the theoretically expected pattern, or structure of the target construct and thereby determines if the measures used have indeed measured what they are purported to measure (construct validity). The choice of principal component analysis was informed by the fact that the scale has already been established on an existing theory by the original authors of the English version and there is no need for the exploratory factor analysis (Marsh et al., 2014). The I-WHOQOL-OLD displayed a different structure from that of the original scale. It had four components, as against six in the original instrument. The German (Conrad et al., 2014), Brazilian (Chachamovich et al., 2008), Chinese (Liu et al., 2013), Norwegian (Halvorsrud, 2010), Turkish (Eser et al., 2010) and South-African (Van Biljon et al., 2015) versions had equally revealed structures that were different from that of the original questionnaire. In the present study, the death and dying domain, as well as the intimacy (which only added item 19) domain, retained the same items as in the original domain, suggesting that these domains might have similar distinct values across cultures. This notion was also supported by the fact that convergent and divergent validities of the domains of the I-WHOQOL-OLD confirmed the two domains as most distinct since their constituting items (especially in death and dying domains) displayed good correlations only with their domains. In the new structure, there were significant overlaps in the items of the former sensory abilities, autonomy, past, present, and future abilities, and social participation domains, with all the constituting items (except items 15 and 13 that formed another distinct component) forming a single component that could be designated as the “ability” domain. This may be highlighting the fact that these previous four domains are highly interwoven in Igbo culture and could be pooled into one domain. This view is supported by the poor divergent and good convergent validity coefficients displayed by the items of these domains. Even though all the items (except item 12) correlated highest with their domains, the items on the four aforementioned domains also correlated highly with one another's domain similar to a previous result (Yao & Chien, 2013) indicating that they might actually not be considered distinct entities in the present study. Item 12 even correlated higher with the autonomy and the social participation domains than its domain of past, present, and future abilities, thus highlighting the close nit relationships among these domains in the present study.
The present study did not only make available to social workers and other stakeholders in elderly care a culturally adapted scale for assessing QoL among Igbo older adults, but it also provided a psychometrically sound and widely utilized QoL scale that will enable easy international comparison. Before now, the assessment of QoL of monolingual Igbo older adults posed a challenge to social workers who either avoided QoL assessment of this group or resorted to self-translation of different QoL scales that unavoidably introduced bias in the assessment. This study has potentially solved this problem and could enhance elderly care as social workers and other stakeholders in health may predictably be more favorably disposed to assess the QoL of older adults in the setting of this study.
The present study has some limitations. Data were collected from a single community rather than from diverse Igbo groups with different dialects. However, the use of the central Igbo dialect that is understood by all Igbo speakers could have ensured that the present study is generalizable to all Igbo older adults. Due to a lack of native English speaker who was fluent in the Igbo language, the back translations of the scale were not performed by native English speakers as recommended by Beaton et al. (2000). However, the back translators were performed by academic physiotherapists who were very experienced in the cross-cultural adaptation, and this could have ensured good translation process. This kind of improvisation has been made in previous studies (Al-Hadethe et al., 2016; Okoye et al., 2020a, 2020b, 2019).
The I-WHOQOL-OLD is a reliable and valid tool that has demonstrated good internal consistency, ceiling and floor effects, known-group and convergent validity, and thus can be used as an outcome measure for QoL of Igbo-speaking individuals. The structure of the I-WHOQOL-OLD however differed from that of the original WHOQOL-OLD. It is recommended that future studies should explore other psychometric properties like (test-retest reliability, responsiveness, and discriminant validity) of the I-WHOQOL-OLD. The WHOQOL-OLD should also be translated and validated in other major Nigerian languages, such as Hausa and Yoruba. If made available in these languages, the instrument may enhance clinical assessment and evaluation of QoL among older adults who speak those languages, thereby helping to improve the health outcomes of older adults.
Footnotes
Author Contributions
All the authors made a substantial contribution to this paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.