
Abstract
Social Support
As a theoretical construct, social support represents a configuration of social and relational patterns that stabilize, decrease stress, and promote positive coping (e.g., Herrenkohl et al., 2016; Negash & Maguire-Jack, 2016). Considered an important feature of personal health and well-being through the lifespan (e.g., Cohen & Wills, 1985; Negash & Maguire-Jack, 2016; Nunes, et al., 2020; Thompson, 2015), the resources provided can be independent or collective, and can help the beneficiary in coping and adapting with stressful life events or close relations.
Social support is a multidimensional construct, as there are different types of supportive functions provided by social relations that may be differentially advantageous depending on the types of stressors or situations (Lagdon et al., 2018). Considered as an echo of how well and deeply connected an individual is to their family and friends (e.g., Herrenkohl et al., 2016; Thompson, 2015), a strong perceived availability of social support boosts people’s confidence to cope without actually activating their network resources (Gottlieb & Bergen, 2010). Therefore, it can be defined as a social resource, whether it is perceived as available or actually provided to individuals by nonprofessionals of their surrounding contexts (i.e., members of formal and informal support groups or relationships) (Cohen et al., 2000; Lagdon et al., 2018).
Social support is a different construct from the social network, which is the sum of all the relationships that an individual perceives as being significant or differentiated (Rocha et al., 2019). Actual received support sometimes can fail to mitigate individuals’ distress and may even aggravate it (e.g., Zee & Bolger, 2019). Thus, support visibility has been studied as an important variable to help us understand the different effects of social support, and it can be defined as the degree to which help is perceived or recorded by beneficiaries as support (e.g., Zee & Bolger, 2019).
Social support can be defined according to three different types: emotional (referring to aspects such as intimacy, affection, comfort and care, having close relationships), tangible (referring to the provision of material assistance; help with financial or instrumental needs) and informational or companionship (referring to the advice, guidance or information relevant to a specific situation; the presence of people to “hang out” or engage with in leisure activities) (Barrera, 1986; Lagdon et al., 2018). The form of support that demonstrates the most the availability and concern of family and friends with the situation one is experiencing is emotional support. This kind of support provided by the relationships that offer understanding, empathy, and encouragement (Rocha et al., 2019).
Social support plays an important role children and adults’ development (e.g., Herrenkohl et al., 2016), affecting personal well-being and directly families and relationships well-being (Negash & Maguire-Jack, 2016). It influences the quality of parenting practices and has a direct impact on the relationships between parents and their children (e.g., Ayala-Nunes et al., 2017; 2018; Negash & Maguire-Jack, 2016).
Stronger social relatedness can promote the process of coping with the demands and stresses of daily life as a parent (Negash & Maguire-Jack, 2016), and parents with a strong family and community network are more likely to have children who developed emotional and social optimally (e.g., Hidalgo et al., 2018; Negash & Maguire-Jack, 2016).
Some research on families with history of maltreatment has confirmed that these parents tend to have smaller social networks and with less frequent contact with their network members (Price-Wolf, 2015; Thompson, 2015). Faced with deprivation of social support, people feel more socially isolated, which is related to poorer psychological function, and a serious risk of child maltreatment (e.g. Martin et al., 2012; Thompson, 2015), and this relationship has been found to transcend cultural specificities (e.g. Negash & Maguire-Jack, 2016).
Measuring Social Support
Research on social support measures began in the 1970’s (e.g., Cobb, 1976; Zimet et al., 1988). Cohen et al. (2000) emphasized that one can find measures of perceived support (e.g., Barrera, 1986), measures of received support (e.g., Norris & Kaniasty, 1996), and measures using both (e.g., Dunkel-Schetter & Bennett, 1990). The measures of social support can be clustered as: unidimensional scales (e.g., Seeman & Berkman, 1988); brief compound measures (e.g., LaRocco et al., 1980); broad scales of close and diffuse support (e.g., PSS, Procidano & Heller, 1983; SSQ, Sarason et al., 1983; FRI and WRI, Holahan & Moos, 1983; SESS, Brown et al., 1986); multidimensional inventories (e.g., ISEL, Cohen et al., 1985; SS-B, SS-A, Vaux et al., 1986, 1987); and network-based inventories (e.g., ISSB, Barrera et al., 1981).
Studies on social support have faced several problems with respect to well-validated measurement instruments. Some researchers have ignored the differences between structural, functional, and social determinants of social support, and even omitted its multiple dimensions. Other researchers have shown that qualitative and quantitative factors are indeed weakly correlated and they cannot be combined into a general or brief measure, although some investigators have done it; some tainted their measures because they considered several independent constructs simultaneously (e.g., perceived quality or closeness of interaction, voluntary initiation of social activity, hobbies, marital status; Broadhead et al., 1988).
There are several instruments that measure (or include) social support (Gottlieb & Bergen, 2010), some of which have been translated and adapted to the Portuguese context. However, the few that are adapted to assess the family context are not comprehensive or expensive and time consuming. For instance, Sarason et al. (1983) developed The Social Support Questionnaire (SSQ; Portuguese version Moreira et al., 2002), a 27 items-scale, providing a total score for number of supports and a total score for support satisfaction. Although this questionnaire has a reasonable track record, it does not provide subscores for any particular support function, nor does it distinguish between different sources of support (Wills & Shinar, 2000).
The Interpersonal Support Evaluation List (ISEL; Cohen et al., 1985; a 5-items Portuguese version was available by Batistoni et al., 2009) is a 40-item inventory that measures people’s perception of the availability of four different types of support: appraisal (emotional), belonging (companionship), esteem, and tangible (instrumental) support. It was widely used in several studies in the health field and has proven adaptable to a variety of populations. Wills and Shinar (2000) pointed as a possible constraint the fact that the instrument does not include a separate scale that clearly indexes advice and guidance, and supplementation of content might be desirable for settings where this function is believed to be especially important.
The Multidimensional Scale of Perceived Social Support (MPSS; Zimet et al., 1988, Portuguese version of Carvalho et al., 2011), is a self-explanatory, simple to use and time saving 12-items scale that assesses three components (i.e., family, friends, and significant others). More than evaluating the different types of perceived social support, this survey captures the individuals’ perception regarding the three sources of support. Another instrument was developed by the Medical Outcomes Study and it is the brief, self-administered, multidimensional Social Support Survey (i.e., MOS-SSS; Sherbourne & Stewart, 1991; Portuguese version Fachado et al., 2007), composed by 19 items, in which individuals are asked about the degree to which they can count on people to support them in different situations. The survey assesses four different dimensions, namely, tangible support and affection support, positive social interaction and emotional/information support. A global scale score is also available. Overall, is a good instrument (López & Cooper, 2011). Although some studies have confirmed the four factor-solution (e.g., Priede et al., 2018) and good reliability levels (i.e., Cronbach alpha coefficient higher than .80), others that found a different factorial structure (e.g., three-factor solution; Griep et al., 2005). One limitation is that tangible support items are more health oriented and discriminate fewer types of support (López & Cooper, 2011).
Finally, the Arizona Social Support Interview Schedule (ASSIS; Barrera, 1980) evaluates perceived and accessed social support, network size, satisfaction with the received social support, need for social support, and finally interpersonal conflict. The ASSIS differentiates six categories of social support: (1) Material aid, (2) Physical assistance (sharing of tasks), (3) Close interaction (in terms of verbal communication), (4) Advice, (5) Positive feedback, and (6) Social participation (Barrera, 1980). There is a Portuguese version that has been used with families at psychosocial risk (Ayala-Nunes et al., 2017). Although some considered the time required to respond and to calculate the scores as obstacles, this instrument allows researchers and professionals to capture rich information about indicators of supportive relationships and of conflict, being also an open-ended measure that allows the collection additional information (López & Cooper, 2011).
The present study will use the DUKE-UNC multidimensional, quantitative and functional measurement instrument (Broadhead et al., 1988).
The DUKE-UNC Functional Social Support Questionnaire
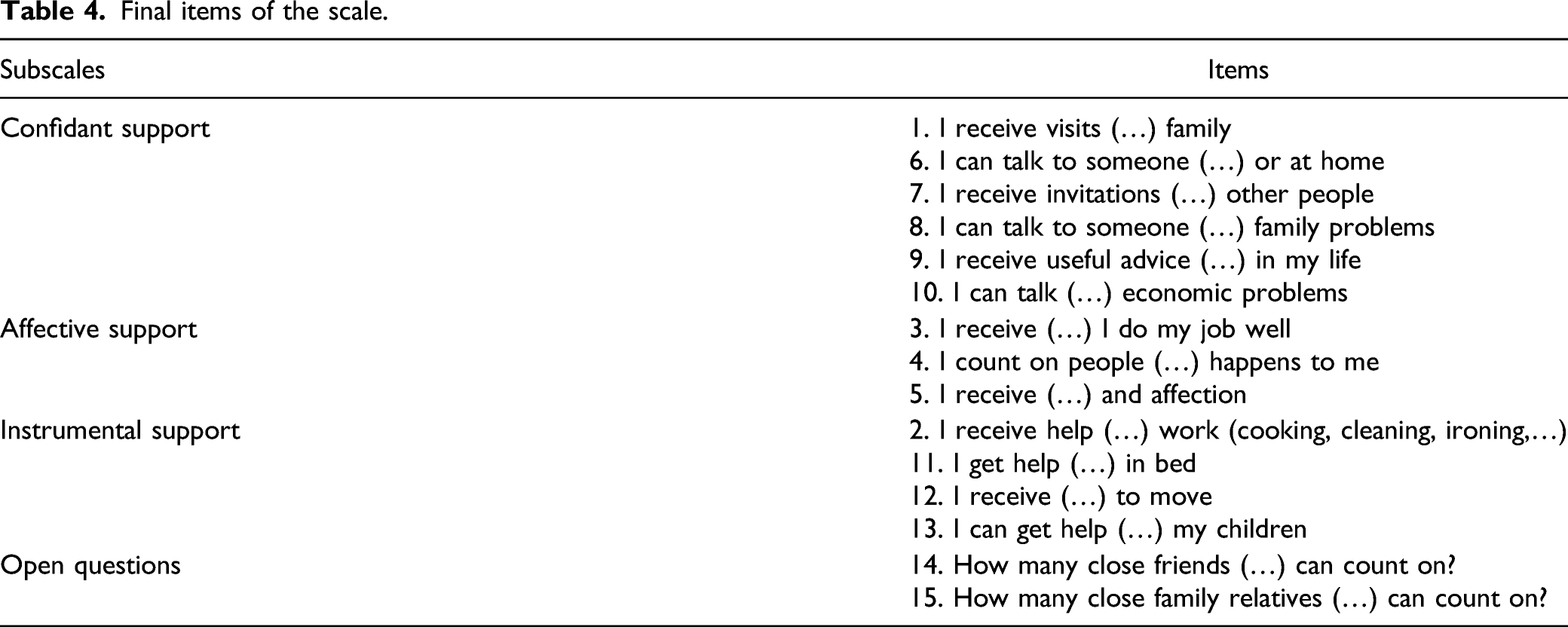
The 14-item multidimensional functional social support questionnaire (Broadhead et al., 1988) assesses four content areas: (1) quantity of support (items 1, 7, 11), (2) confidant support (items 8,9,10), (3) affective support (items 4, 5, 6), and (3) instrumental support items 2,3,13,14). Later, the authors developed a short-form with 8 items evaluating two dimensions (i.e., affective and confidant support) and named it the Duke-UNC Functional Social Support Questionnaire (FSSQ). Although they did not find psychometric support for the instrumental domain, they suggest that, in future studies, items that measure instrumental support and praise should be added.
In their study, although they did not find psychometric support for the instrumental support domain, they propose further study for the single-item measure (Broadhead et al., 1988).
The Consortium for Longitudinal Studies of Child Abuse and Neglect studies (LONGSCAN; Hunter et al., 2003) adapted a 10-item version with 7 items from the original scale (evaluating Bellón Saameño et al., 1996 confidant support and affective support) and 3 more items (i.e., help with transportation, help with cooking or household tasks, and help caring for a child) to contemplate the dimension of instrumental/tangible support.
Several studies have adopted this instrument, using the 14-item version (e.g., Breitbart et al., 2000; Rosenfeld et al., 2006; Saracino et al., 2015), the 8-item version (e.g., Broadhead et al., 1988, 1989), the 10-item version (e.g., LONGSCAN, Hunter et al., 2003), and even an 11-item version (e.g., Bellón Saameño et al., 1996; de la Revilla, et al., 1991).
This instrument has been translated and adapted to several languages and cultures (e.g., Spanish, Bellón Saameño et al., 1996; Caycho Rodríguez et al., 2014; Cuéllar-Flores & Dresch, 2012; De la Revilla et al., 1991; Chinese, Jia & Zhang, 2012) and to a variety of specific populations (e.g., adults, Ayala et al., 2012; caregivers, Artaso et al., 2003; Cuéllar-Flores & Dresch, 2012; chronic patients, Bellón Saameño et al., 1996; schizophrenia, Mas-Expósito et al., 2013; HIV positive, Piña & Rivera, 2007). The studies have shown that the FSSQ is an adequate measure of social support and, although with slight differences in item-distribution, its dimensions are robust.
In the present study we used the LONGSCAN (Hunter et al., 2003) version, composed by 10 items that assess three scales: seven items measuring confidant support and affective support (from the original version; Broadhead et al., 1988, 1989), and three new items assessing instrumental support (an attempt inserted by LONGSCAN study).
The aims of this study were to translate, adapt and validate the Portuguese version of the Duke-Unc Functional Social Support Questionnaire (FSSQ) in a sample of Portuguese parents. We expect that: (1) the three-factor structure of the FSSQ will be confirmed; (2) the FSSQ will show good internal consistency measured by Cronbach’s Alpha; and that (3) the FSSQ will show discriminant validity with the Parenting Styles and Dimensions Questionnaire.
Method
Participants
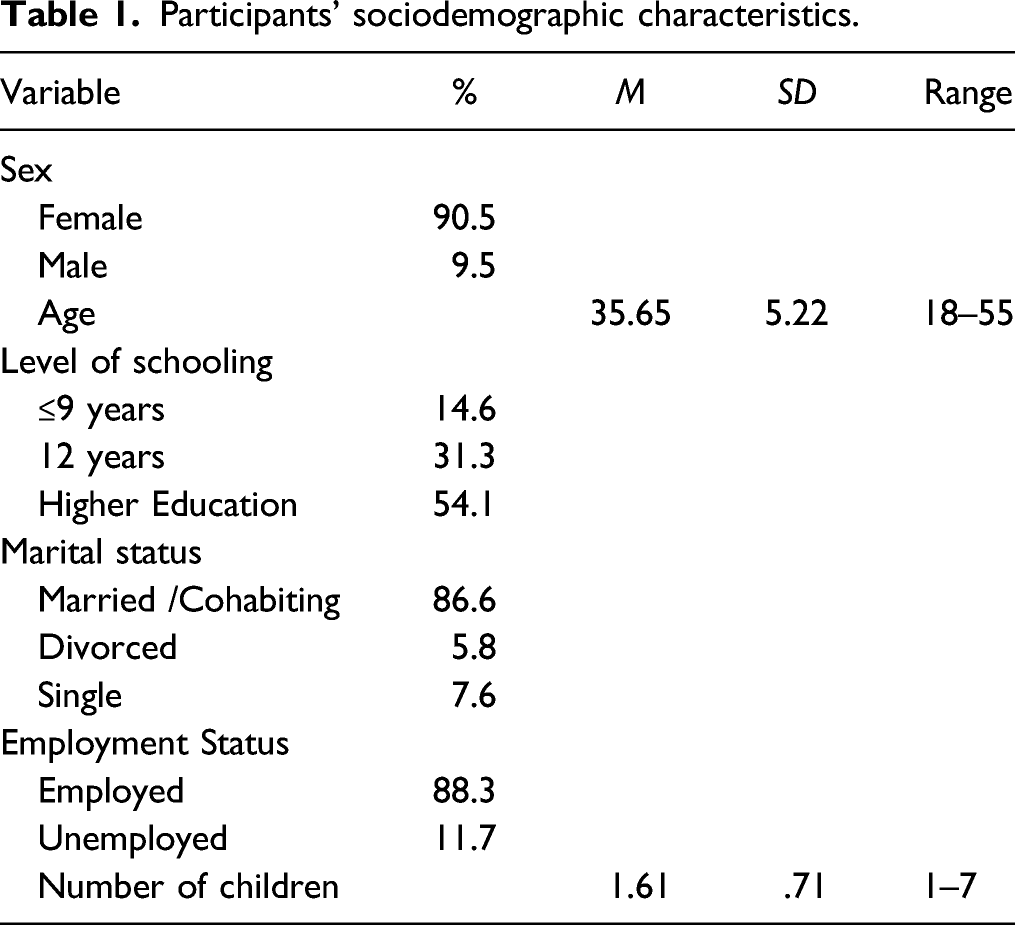
Participants’ sociodemographic characteristics.
Procedures
The present study is part of two ongoing research projects.
The participants could complete the assessment protocol in person (n = 595) or online (n = 470). The assessment protocol included information about the study’s aims, the inclusion criteria, the voluntary nature of participation and compliance with confidentiality and anonymity, and the possibility to leave the study at any time without consequence.
In the first study, the participants who completed the assessment protocols in person were recruited in different regions of the north and south of Portugal, and the data collection was carried out in nurseries, private pre-schools, and informal social network (i.e., snow-ball technique). Regarding the online data collection, the participants were invited by email or via social media. For the second study, half of the 22 pre-school and primary education centers in Albufeira (South of Portugal), in total 11 centers, were randomly selected and questionnaires were given to all the student’s parents.
Both studies were approved by an institutional review board. The first study by Administração Regional de Saúde do Norte (Reference No. 141/2017) and the second was approved by the Scientific Commission of the Psychology and Sciences Education Department, University of Algarve (Reference No. 55/20/12/2017).
Measures
Sociodemographic Questionnaire
Participants completed a sociodemographic questionnaire to obtain data about participants’ age, gender, years of schooling completed, and marital and employment status.
Functional Social Support Questionnaire
The FSSQ is an adaptation of Duke-UNC Functional Social Support Questionnaire that was developed by Broadhead, Gehlbach, DeGruy, and Kaplan (1988) to evaluate the individual´s perception of the amount and type of personal social support. We used the adapted version of the LONGSCAN study (Hunter et al., 2003), as described before. Two additional open questions regarding the number of close friends and family, with whom one can count, were also used.
The Parenting Styles and Dimensions Questionnaire
The PSQD is the Portuguese version (Martins et al., 2018) of the Parental Styles and Dimensions Questionnaire–Reduced Version (Robinson et al., 2001). This questionnaire has 32 items with a 5-point Likert scale (from 1–Never than 5–Always). These items can be grouped into three scales: authoritative parenting style, authoritarian parenting style and permissive parenting style. Each one of these scales has different subscales. The authoritative style includes a Connection dimension (warmth and support), a Regulation dimension (reasoning/induction), and an Autonomy dimension (Democratic participation). The authoritarian style includes a Physical coercion dimension, a Verbal hostility, and a Non-reasoning/Punitive dimension. The last dimension, the permissive style, includes just one subscale, the Indulgent dimension (Martins et al., 2018; Robinson et al., 2001).
Data Analysis
Data analysis was performed using IBM SPSS Statistics software program (v. 25, SPSS Inc., Chicago, IL) and AMOS (v. 25, SPSS Inc., Chicago, IL Initially). Missing data were found across the FSSQ, ranging from 0.1% to 0.3% of the questionnaire items. We used regression substitution to estimate the missing values because the percentage of missing values was lower than 5% in all cases (Kline, 2016).
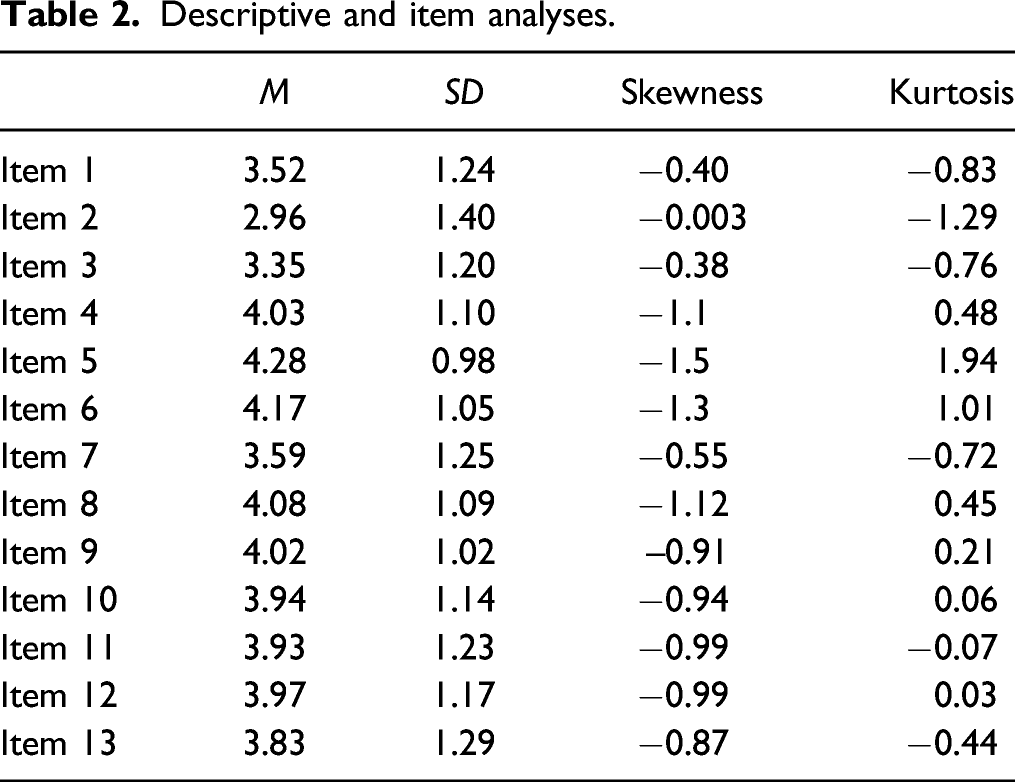
Initially, we studied the psychometric sensitivity of the instrument through measures of central tendency and shape. Items with skewness above 3 and kurtosis above 7, in absolute values, are considered to have sensitivity problems (Kline, 2016).
Three confirmatory factor analysis (CFA) models with different configurations were tested: Model 1 represents a one-factor structure, where all items discriminate in a single component; Model 2 addresses a structure of three-factors without error correlations and Model 3 addresses a structure of three-factors with four correlations between different errors (Figure 1). Several fit indices were used to evaluate the adequacy of the models. The following fit indices were used: chi-square (χ2), chi-square and degree of freedom ratio (χ2/df), comparative fit index (CFI), Tucker-Lewis index (TLI), goodness of fit index (GFI), incremental fit index (IFI), the root mean square error of approximation (RMSEA), Bayesian information criterion (BIC), and Akaike Information Criterion (AIC). The model fit was considered suitable for χ2/df values below 5, CFI, TLI, IFI, and GFI above .90 (Bentler, 1990; Bentler & Dudgeon, 1996), SPMR and RMSEA below .80 (Hu & Bentler, 1999) and have the smallest BIC and AIC (West et al., 2014). Model 3: Factor loadings and covariances for the three first-order latent factors structure.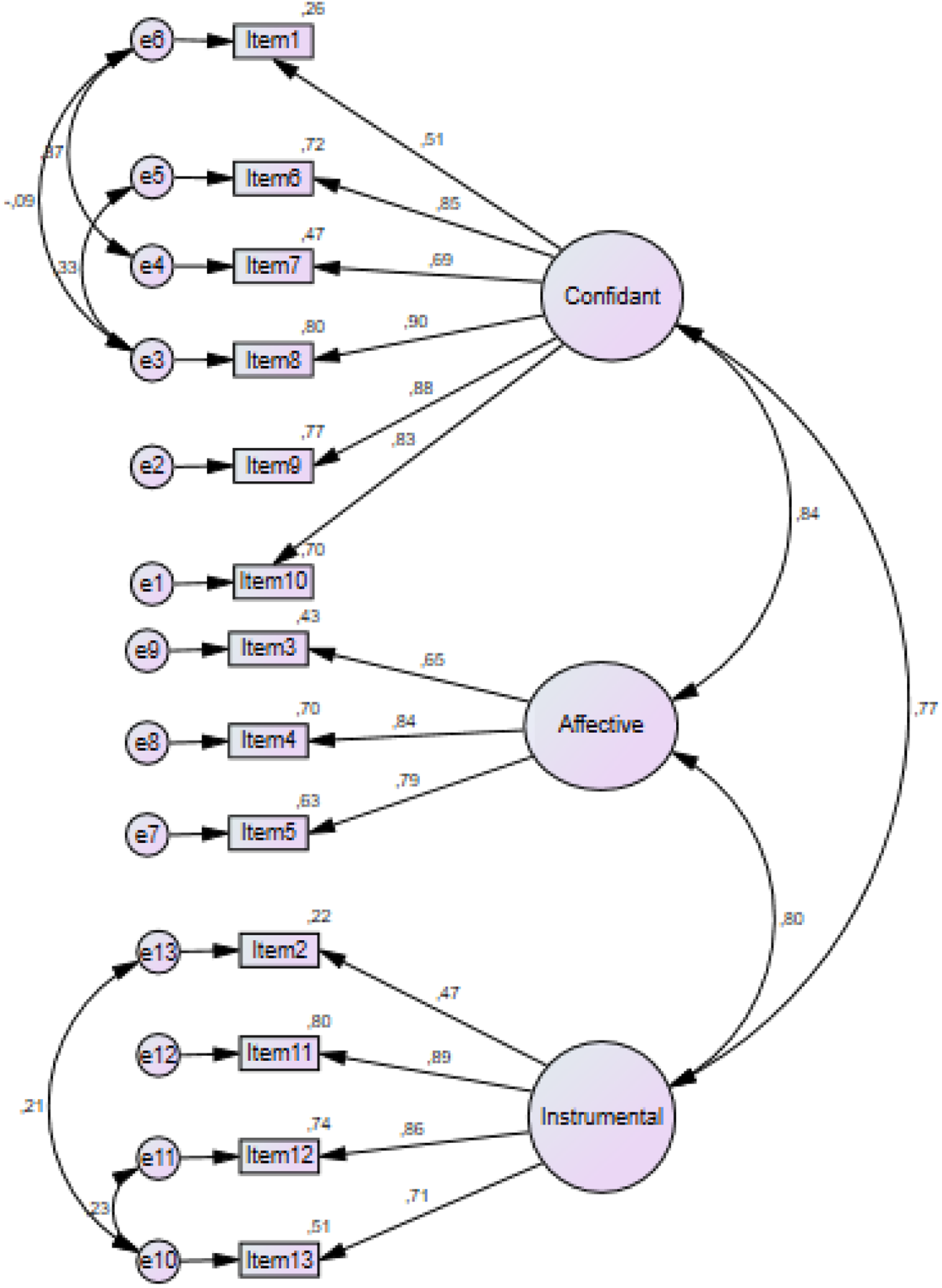
In order to assess internal consistency, Cronbach’s alpha was computed, with values above .70 considered acceptable and illustrating a good level of internal consistency (Tabachnick & Fidell, 2019). Descriptive statistics were conducted to analyze the items 14 and 15 about social support network size. To conclude, discriminant validity was evaluated using Pearson correlations between the mean scores for the FSSQ subscales and the PSDQ subscales, with values above .80 considered very strong, values between .60 and .80 considered strong, values between .40 and .60 considered moderate, values between .20 and .40 considered weak, and values below .20 considered negligible (Benesty et al., 2009).
Results
Psychometric Sensitivity
Descriptive and item analyses.
Confirmatory Factor Analysis
Confirmatory factor analysis models fit indices (n = 1064)

Legend: AIC–Akaike Information Criterion; CFI–Comparative fit index; TLI–Tucker-Lewis index; GFI–Goodness of fit index; IFI–Incremental fit index; RMSEA–Root mean square error of approximation.
The one-factor structure of the FSSQ (Model 1) was examined through CFA. Indicators of acceptable model fit were not provided.
Then we examined the original three first-order structure of the FSSQ (Model 2) through CFA. Indicators of acceptable model fit were provided by chi-square statistic (χ2 (62) = 685.84, p < .001), CFI (CFI= .93), TLI (TLI = .92), IFI (IFI = .935) and GFI (GFI = .90) but not by RMSEA (RMSEA = .10, 90% CI [.05, .10]). Through the inspection of the modification indices (MI), we concluded that improved model fit would result from adding measurement error covariance between the following items: 1 and 7, 1 and 8, 6 and 8, 2 and 13, 12 and 13.
Therefore, the most adequate structure was the one represented by Model 3 (Figure 1) with correlation between errors, addressing three first-order latent factors (χ2 = 3.85.81, p < .000, χ2/df = 6.77, CFI = .97, GFI = .95, TLI= .95, IFI = .975, RMSEA =.07).
Final items of the scale.
Correlations Between the FSSQ Total Score and Subscales
The FSSQ total score and its subscales were positively and significantly (p < .001) correlated with each other, as presented in Table 5. The correlations between total score and all subscale were very strong. The correlations between different subscales were strong.
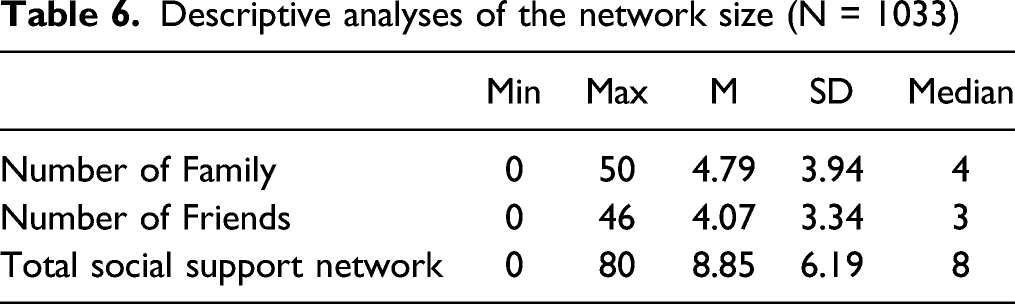
Social Network Size
Correlations between the FSSQ total score and subscales

**p < .01.
Reliability: Internal Consistency
Descriptive analyses of the network size (N = 1033)
Discriminant Validity
Cronbach’s alphas, mean inter-item correlations, and corrected item-total correlation ranges.
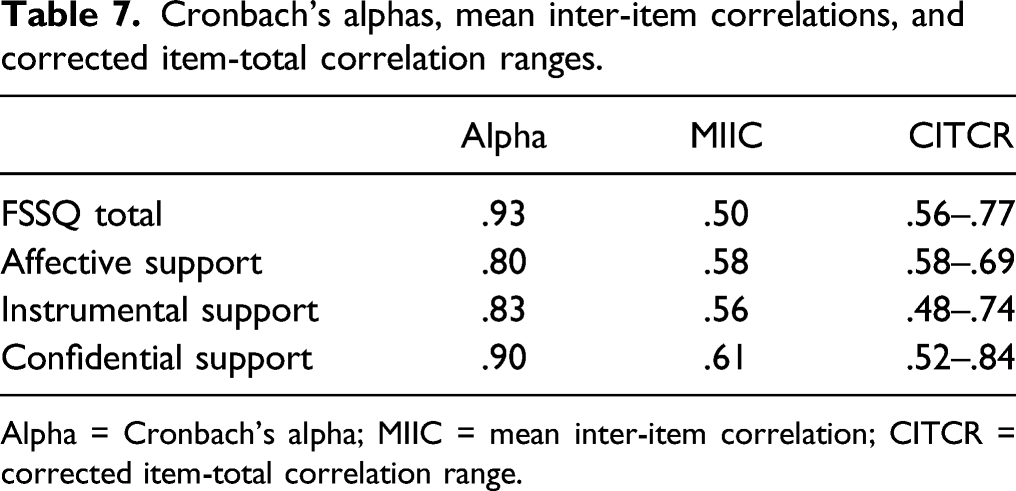
Alpha = Cronbach’s alpha; MIIC = mean inter-item correlation; CITCR = corrected item-total correlation range.
Pearson correlations testing concurrent validity between the FSSQ questionnaire subscales and PSDQ.
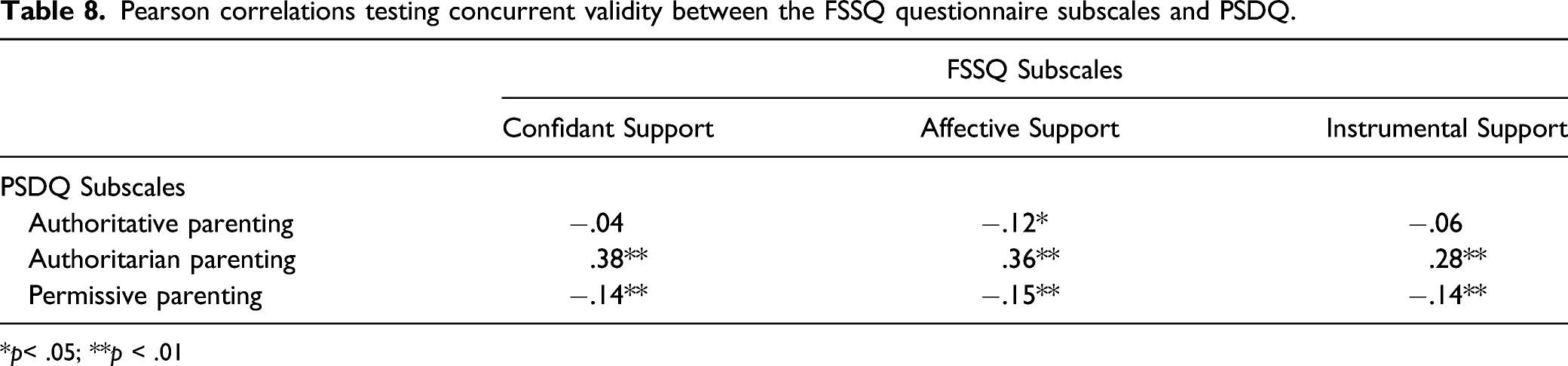
*p< .05; **p < .01
Discussion
The aim of this study was to examine the structure and correlates of the adapted Portuguese version of the Functional Social Support Questionnaire. As mentioned above, the LONGSCAN version used in the current research corresponds to a slightly modified form of the original scale (Broadhead et al., 1988; Hunter et al., 2003). This modified form retains all the seven items from the original one, adding three more items covering aspects of instrumental support deemed as essential for primary caregivers. The additional element was thus supplementary to the previous two designated functional aspects of social support, specifically confidant relationship support and affective support. Besides, the three additional items were added to the core content without altering the featured brief, self-administered measurement instrument of functional social support that showed good psychometric indices and substantial evidence of its utility for research in a wide range of family studies. The original study of the scale was developed with obstetric patients with a mean age of 36.8 years (Broadhead et al., 1988). The Portuguese sample had a similar mean age and were mothers and fathers of young children.
Three confirmatory factorial models were tested: a one-factor structure (Model 1), three first-order factors, representing the theoretical structure (Model 2) and three first-order factors representing the theoretical structure with error items correlated (Model 3). Results showed that Model 3 had fit indices of acceptable values (Bentler, 1990; Bentler & Dudgeon, 1996), confirming the original theoretical structure: Confidant Support (items 1, 6, 7, 8, 9 and 10), Affective Support (items 3, 4 and 5), and Instrumental Support (items 2, 11, 12 and 13).
As for reliability, good indices of internal consistency were obtained for the three subscales. The Confidential Support had the highest value. Similar coefficients were found in other studies with the scale. The study authored by Bellón Saameño et al. (1996) with the Duke-UNC-11 version found similar values for internal consistency in two scales Confident Support (.88) and Affective Support (.79). In the study that was developed by Hunter et al. (2003), the internal consistency values (between .81 and .92) were very similar to those obtained in this study.
When comparing the internal consistency of this scale with other social support scales (e.g., Procidano & Heller’s Perceived Social Support from Family and Friends Scale, Glozah and Pevalin, 2017), we can conclude that the FSSQ presents better values
In the original study, the researchers used a 14-item questionnaire. However, three items were deleted because of lack of test-retest reliability (Broadhead et al., 1988). The authors suggested the 11-item questionnaire for research use. According to our findings, the items deleted in the original study presented good Skewness and Kurtosis values (Kline, 2016) and the Instrumental Support subscale had a good internal consistency value (Tabachnick & Fidell, 2019). Given the factorial and internal consistency results, we recommend the application of the three subscales of the FSSQ. In future studies, it will be important to include testing its temporal stability (test-retest reliability) for comparison with the original study.
Evidence of discriminant validity was also presented in our study. There were weak and non-significant associations, as expected, between Authoritative Parenting and Confidant and Instrumental Support. As for Affective Support, the associations with the PSDQ subscales were all significant and mostly negative. Four more significant correlations were identified, namely the associations between Confident Support and Instrumental Support and Authoritarian and Permissive Parenting. These associations were weak and this type of validity is unlikely to be questioned (Netemeyer et al., 2003). These findings show us that the two questionnaires assess dimensions underpinning different phenomena: one focusing on social support supplied by family and friends in personal social network (FSSQ), and the other related to the fathers and mothers’ parenting styles (PSDQ). Indeed, some of the tenuous correlations may impair to take a more clear-cut vision of the pattern of relations of the distinctive parenting styles and the perceived social support. Nonetheless, these trends support the vast empirical evidence that high levels of social support in the personal social network endorse the parents’ attitudes and skills (e.g., caring and monitoring practices) due to an increased probability of counting with good role models providing them encouragement and confidence boosts toward the parenting tasks (Péres-Padilha et al., 2017; Rhoad-Drogalis et al., 2020). Besides, the availability of early social support is deemed as critical to pave the agency and the self-efficacy of mothers with children under three years-old (Chang, 2017).
About social network size, the results of this study show that the support network made up of family members had a higher average score than the network of friends. General, the participants in this sample considered that the support received comes, on average, from nine people, being them family or friends. A similar size of network and balance between family and friends was found in other Portuguese studies (Ayala-Nunes et al., 2017; Nunes et al., 2020). In future studies, it will be important to better understand the quality of this support. More than the number of people to turn to, whether they are family or friends, it is important to understand if this support is satisfactory for the family’s needs.
The adequate psychometric properties of the Portuguese version of the FSSQ support its use in research contexts. We anticipate that the questionnaire may also be useful when assessing diverse psychosocial family profiles (e.g., a tool in pre- and post-test for evidence-based parenting interventions), as well as for different professionals, like social workers (e.g., a tool to identify vulnerabilities and potentials in family assessments and interventions). Indeed, these additional studies will be important for validating this measure in families at different levels of risk. Notwithstanding having been initially developed having in the health field, namely within family medicine and pediatric consultations (Broadhead et al., 1988), later studies with clinical (Hunter et al., 2003) and community populations (Ayala-Nunes et al., 2017) have proven its empirical validity and utility in social research and social services to measure qualitative and quantitative aspects of social support available for the family.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.