
Abstract
In order to prevent relapse in sexual crimes, measures such as treatment programs for individuals who have committed sexual offenses are important. The matter of the evidence however is highly debated among scholars. Some have suggested there is evidence for sexual offender treatment programs (Kim, Benekos, & Merlo, 2016; Marshall & Marshall, 2007), while others have expressed doubts and argued there is still a of lack of high-quality methodological study designs (Dennis et al., 2012; Grønnerød, Grønnerød, & Grøndahl, 2015; Långström et al., 2013; Seto et al., 2008). A large number of meta-analyses and systematic reviews demonstrate significant decrease in recidivism, especially for treatment programs based on cognitive behavioral therapy (CBT) and adherence to the Risk-Need-Responsivity (RNR) model (Bonta & Andrews, 2017; Gannon et al., 2019; Hanson et al., 2009; Kim et al., 2016; Mpofu et al., 2018; Schmucker & Lösel, 2008, 2015, 2017; Soldino & Carbonell-Vayá, 2017). In short, the RNR model (Bonta & Andrews, 2017) proposes rehabilitation intensity should increase for individuals with higher risk of recidivism (the Risk principle). Moreover, rehabilitation ought to target criminogenic needs, that is, factors related to recidivism risk (the Need principle). Finally, according to the Responsivity principle, rehabilitative measures need to be in line with evidence regarding effective intervention modes for the population (so-called general responsivity), in the case of criminal offenders, CBT-based approaches seems to be most effective. In addition, the responsivity principle asserts interventions need to be adapted to the specific individual’s needs (specific responsivity), which may be influenced by for instance concentration problems or the level of motivation.
One large-scale single study evaluation from England and Wales, however, demonstrated a small but significant increase in recidivism after attending treatment program (Mews, Di Bella, & Purver, 2017), thus yielding further debates (Lösel et al., 2020). The problems regarding evidence are partly due to methodological limitations related to ethical and practical obstacles when conducting randomized controlled trials (RCTs) within the prison and probation setting (Lösel et al., 2020; Marshall & Marshall, 2007) and the generally low base rates of recidivism (Hanson, 2014). A majority of sexual crimes goes undetected (DeLisi et al., 2016; Drury, Elbert, & DeLisi, 2020; Westfelt, 2008); thus, conclusions about recidivism drawing on verdicts may not be valid (Scurich & John, 2019). Accordingly, there is a need to explore different aspects of treatment outcomes for this population. Scholars highlight the need for research using other types of outcome measurements in addition to the traditional crime statistics, such as behavioral change within treatment (Hanson, 2014; Harkins & Beech, 2007; Jung & Gulayets, 2011; Levenson & Prescott, 2014; Marshall, Marshall, & Olver, 2017). One way is to examine outcomes in terms of change in criminogenic needs, or dynamic (changeable) risk factors, using pre- and posttest designs. In this article, I present a study utilizing this design, with the unique combination of therapists’ ratings and participants’ psychometric tests, to examine the feasibility of a sexual offender treatment program within a prison and probation population of individuals convicted of a sexual offense (ISO) in Sweden.
Criminogenic Needs
Criminogenic needs refer to dynamic factors related to the risk of recidivism, that is, factors that are changeable and therefore should be targeted in offender treatment programs (Bonta & Andrews, 2017; Mann et al., 2010). There is substantial empirical evidence for the risk factors (Bonta, Blais, & Wilson, 2014; Eisenberg et al., 2019; Gutierrez, Wilson, Rugge, & Bonta, 2013; Olver, Stockdale, & Wormith, 2014; Wooditch, Tang, & Taxman, 2014), often referred to as the Central Eight (Bonta & Andrews, 2017). The Central Eight include antisocial history, antisocial personality pattern, pro-criminal attitudes, pro-criminal associates, substance abuse, family/marital deficits as well as deficits regarding school/work and leisure/recreation. How are these risk factors addressed in rehabilitation, or treatment programs, for individuals convicted of an offense? A comprehensive antisocial history, including early onset of rule-breaking behaviors, implies higher risk of recidivism, suggesting such individuals are in need of intensive rehabilitative measures (however, it should be noted this specific risk factor is static rather than dynamic, in the sense that a history cannot change.) Antisocial personality traits can be targeted for instance by skills training to enhance impulse control. Pro-criminal attitudes, such as neglecting the consequences of criminal behaviors, should be challenged in treatment and the individual will need help to develop a social network of prosocial peers, instead of associates endorsing and reinforcing criminal behaviors. Furthermore, rehabilitation needs to include support for substance abuse and measures to ensure a stable work situation. Dysfunctional relationships may be the result of communication skill deficits, which can be addressed in treatment as well as helping the individual in taking steps to find or develop meaningful and prosocial leisure activities. The Central Eight risk factors are of relevance in preventing recidivism in general crimes as well as sexual crimes. However, there are additional risk factors, specific for re-offense in sexual crimes. These include, among others, hypersexuality, intimacy deficits (Hanson & Morton-Bourgon, 2005), and locus of control (Fisher, Beech, & Browne, 1998). The Central Eight risk factors were examined in this study by therapist ratings. The participants’ self-reports addressed the three specific risk factors stated before. For compliance reasons, filling out three questionnaires was deemed an appropriate amount for participants; hence, it was not feasible to investigate all Central Eight risk factors from a participant’s perspective. Since treatment components addressing problematic sexual behaviors have been especially developed in the treatment program studied, Sex Offender Program with an Individual Focus (SEIF), and there is a paucity of studies examining treatment change in this regard, one questionnaire targeted hypersexuality. Improving relationship skills and intimacy deficits is a central part of SEIF, whereas relationship styles were selected as the second relevant measure. Furthermore, an increase in internal locus of control is associated with treatment success over a range of dynamic risk measures (Fisher et al., 1998). In addition, research suggests facilitation of internal locus of control enhances responsivity (D’Orazio, 2017) (an important aspect of the RNR-model, implemented in SEIF); hence, the third treatment change measure of choice was locus of control. Although these three change measures each are relevant regarding both risk of sexual re-offense and the relevance in relation to SEIF, their interconnectedness has not been very well examined in the existing literature.
Hypersexuality
For decades, sex offender treatment scholars have engaged in the study of effective interventions to alter problematic sexual behaviors related to crime; however, research have focused primarily on sexual deviance, such as pedophilia (Crolley, Roys, Thyer, & Bordnick, 1998; Marshall et al., 2016). During the last decade, hypersexuality has emerged as an important criminogenic need, yet understudied, in terms of possible treatment impact.
Hypersexual disorder, or sometimes referred to as sexual pre-occupations or sex addiction, is a controversial and complex concept, both regarding definition and appropriate measurements (Grubbs et al., 2020; Kingston, 2016), and an established definition is lacking (Kingston & Firestone, 2008; Walters, Knight, & Långström, 2011). Hypersexual disorder was rejected for the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) classification system of psychiatric diagnoses due to the uncertain scientific evidence (Kafka, 2014). However, the diagnosis compulsive sexual behavior disorder has been accepted in the forthcoming version of the International Classification of Diseases 11th Revision (ICD-11), scheduled for implementation in 2022. Compulsive sexual behavior disorder is defined as: A persistent pattern of failure to control intense, repetitive sexual impulses or urges resulting in repetitive sexual behaviour. Symptoms may include repetitive sexual activities becoming a central focus of the person’s life to the point of neglecting health and personal care or other interests, activities, and responsibilities; numerous unsuccessful efforts to significantly reduce repetitive sexual behaviour; and continued repetitive sexual behaviour despite adverse consequences or deriving little or no satisfaction from it. (World Health Organization, 2021)
According to Kingston (2016), there is agreement on the central features of what I hereinafter will refer to as hypersexuality, which include the occurrence of sexual fantasies, impulses, and behaviors that are repetitive and persistent and result in negative social, emotional, physical, or legal consequences, such as sexual crimes. These fantasies and behaviors can be either normophilic or paraphilic (Kingston, 2016); however, empirical studies have demonstrated hypersexuality is strongly associated with paraphilic interests (Långström & Hanson, 2006). Prevalence in the general population is estimated as being approximately 3–6% (Black, 2000); however, the numbers vary greatly between studies (Grubbs et al., 2020). Among the ISO population, the corresponding numbers range between 12% and 40% (Kingston & Bradford, 2013; Marshall & O’Brien, 2012). Despite the confusion regarding the different concepts, hypersexuality is a significant clinical problem, and one of the strongest predictors of recidivism in sexual crimes among ISOs (Hanson & Morton-Bourgon, 2005; Kingston & Bradford, 2013). Zapf, Greiner, & Carroll (2008) suggest that hypersexuality and the risky sexual behaviors often associated with this may serve as a strategy to regulate attachment needs. Hence, research indicates that the inability to control sexual impulses and using sex as coping may increase the risk of sexually coercive behaviors or non-consensual sexual acts. Therefore, hypersexuality is of relevance in sexual offender treatment. According to a recent systematic review on the last 25 years of research, conducted by Grubbs et al. (2020), there is “a virtual absence of high-quality treatment-related research published within this time frame” (p. 1). There is however some evidence and several studies suggesting that psychosocial as well as medical treatment may be effective (Grubbs et al., 2020; Hallberg et al., 2019; Hook, Reid, Penberthy, Davis, & Jennings, 2014; Kjellgren, 2019; Landgren, Malki, Bottai, Arver, & Rahm, 2020; Lewis, Grubin, Ross, & Das, 2017; Lösel & Schmucker, 2005; Malandain, Blanc, Ferreri, & Thibaut, 2020; Miles, Cooper, Nugent, & Ellis, 2016; Savard et al., 2020; Wilson & Fischer, 2018; Winder et al., 2018). Nonetheless, research regarding psychological treatment specifically for a convicted population is lacking.
Locus of Control
Individuals who place responsibility for their behaviors on external factors generally have an increased risk of relapse in the problematic behaviors targeted in psychosocial interventions (Craig, Franklin, & Andrews, 1984). In sexual offender treatment programs, participants are encouraged to take responsibility for their future by formulating plans and taking actions to ensure a prosocial lifestyle (Marshall & O’Brien, 2013), and locus of control constitutes a criminogenic need (Fisher et al., 1998) commonly addressed in these treatments (McAnena, Craissati, & Southgate, 2016). McAnena et al. (2016) cites Rotter (1966) when describing locus of control as a concept that “represents the extent to which an individual perceives their behavior and/or events in their life as being within their own control or that of some external force, for example, fate, luck, or powerful others” (McAnena et al., 2016, p. 95). Furthermore, they conclude that individuals externalizing “therefore feel themselves to be passive agents in their lives, and that events and consequences are outside their control, while those with an internal locus of control feel empowered to control events and outcomes in their lives.” (p. 95). External locus of control, i.e., the perception of not being the agent in one’s life, is associated with violent and sexual re-offense, and studies have demonstrated treatment can impact ISOs’ locus control (Fisher et al., 1998; Mandeville-Norden, Beech, & Hayes, 2008; Olver, Nicholaichuk, & Wong, 2014), including online offenders (Gillespie et al., 2018). The proposed links to sexual offending include locus of control as a mediating factor between an individual’s own sexual abuse victimization in childhood and later offending as well as its association with impulsivity, thus, that sexual offending may serve as a mean to regain a sense of control (McAnena et al., 2016).
Attachment
Although debated, intimacy deficits and problematic intimate relationships are often proposed to constitute risk factors for relapse in sexual crimes (Hanson & Morton-Bourgon, 2005; Mann et al., 2010; Martin & Tardif, 2014; Wielinga, Margeotes, & Olver, 2021). There is a suggested connection between those risk factors and attachment. The hypothesis proposed for this link is that insecure attachment leads to intimacy deficits, which ISOs try to compensate through sexual coercion and deviant sexual behavior (Bushman, Baumeister, & Phillips, 2001; Marshall, 2010; Marshall & Marshall, 2016; Martin & Tardif, 2014; Ward, Hudson, & Marshall, 1996). Attachment theory, developed by Bowlby (1970, 1973), describes how infants interact with attachment figures, forming so-called internal working models, which impact later relationships. It has been suggested that adult attachment styles are malleable and possibly influenced by relationship-specific experiences (Klohnen, Weller, Luo, & Choe, 2005). Empirical research supports the idea that psychotherapy can influence attachment, thus, contributing to the development of a secure attachment in individuals having insecure attachments (Fonagy et al.,1995 as cited in Broberg, Risholm Mothander, Granquist, & Ivarsson, 2008; Levy et al., 2006). Frequency, duration of therapy, and quality of the therapeutic alliance appear to be important factors (Parish & Eagle, 2003). ISOs, to a higher extent, are insecurely attached compared to the general population and in comparison to other offenders (Lyn & Burton, 2004; Marsa et al., 2004; Marshall & Marshall, 2010; Martin & Tardif, 2015; Ogilvie, Newman, Todd, & Peck, 2014; Smallbone & Dadds, 2000; Smallbone & McCabe, 2003; Ward et al., 1996). However, the literature on whether treatment for ISOs actually alter attachment styles is scarce; only one such study was found in the literature search. Grady, Swett, & Shields (2016) conducted a study with incarcerated, adult males attending the Sex Offender Accountability and Rehabilitation program (SOAR) in North Carolina, USA, using Relationship Scale Questionnaire (RSQ 2-factor) (Griffin & Bartholomew, 1994) and Adult Attachment Scale (AAS) (Collins & Read, 1990). Results showed a significant decrease in scores for the anxiety dimension on attachment style but no change regarding the avoidant dimension, posttreatment. The study did not examine if the change in attachment scores was related to other outcomes, such as subsequent re-offending. Hence, although a lot of research has been conducted on attachment issues within the ISO population, research about treatment impact on attachment styles is still needed.
In summary, criminogenic needs relevant for the ISO population have undergone extensive investigation; however, there are still gaps where examining within-treatment change in such needs can enhance knowledge on treatment impact.
Method
Research Question and Hypotheses
The research question guiding this study was: Is there change in criminogenic needs after participation in the Swedish sexual offender treatment program called Sex Offender Program with an Individual Focus (SEIF)? The following hypotheses were tested.
Participants in SEIF will exhibit a statistically significant reduction in hypersexuality posttreatment compared to pretreatment.
Participants in SEIF will exhibit a statistically significant reduction in external locus of control posttreatment compared to pretreatment.
Participants in SEIF will exhibit a statistically significant reduction in levels of anxiety as well as avoidance in their attachment styles posttreatment compared to pretreatment.
Participants in SEIF will exhibit statistically significant higher levels of function regarding criminogenic needs, according to therapist ratings of treatment progress, posttreatment compared to pretreatment.
Description of the Intervention
The study was conducted during the pilot run of a new national sexual offender treatment program in Sweden: SEIF, which is manualized (but flexible), based on cognitive behavioral therapy, and adherence to the RNR-model (Bonta & Andrews, 2017; Kriminalvården Swedish Prison & Probation Service, 2019). The main objective of the program is to reduce the risk of sexual re-offending. The program is delivered by the Swedish Prison and Probation Service, by approximately 80 therapists nationwide, in group-format or individually, to incarcerated ISOs and those on probation or parole. The decision regarding group or individual format is based on both practical circumstances and participant’s characteristics in relation to group dynamics. Most probation offices deliver SEIF individually due to shorter sentences and lack of appropriate amount of participants, whereas group-format is the most common mode of intervention in the prison setting. Moreover, some personality traits may contribute to the use of individual format. Complementary individual sessions are offered when necessary, for example, when addressing sexual deviation. Furthermore, all participants who enter SEIF in prison attend booster sessions during their parole. Sessions in group-format are 3 hours long and held 2 days a week in prison and once a week at the probation office, respectively. Individual sessions are generally held once a week and are 60–90 minutes long. Recommended treatment intensity is 80–250 hours in group or 25–100 hours individually, depending on the specific client’s risk and need assessment, in accordance with the RNR-model. In general, SEIF is accessible for all convicted ISOs, including those who deny their crime despite convictions and female sex offenders. However, it is noteworthy that there were no female participants among the first 99 SEIF-participants who were asked to join this study.
The first phase of SEIF contains individualized assessment elements such as a forensic case formulation (Sturmey & McMurran, 2011) (see figure 1). In SEIF, the case formulation consists of theoretically derived explanations for the origin and possible discontinuation of the individual criminal behavior, that is, hypotheses regarding why and how the problematic behaviors and circumstances, resulting in a sexual crime, have occurred and evolved over time, as well as hypotheses about which treatment components may facilitate the reduction of such behaviors or high-risk situations. Furthermore, the case formulation contains a detailed treatment plan. The case formulation is co-constructed with each participant individually during the initial phase, aiming for collaboration and transparency regarding assessments, treatment hypotheses and planning of treatment components (Kriminalvården Swedish Prison & Probation Service, 2019). Furthermore, assessments of individual criminogenic needs are conducted using the Therapist Rating Scale-2 (TRS-2) (Marshall & Marshall, 2009), as well as an examination of the participant’s valued direction (Hayes et al., 1999), i.e., the formulation of personal long-term process goals, inspired by Acceptance and Commitment Therapy. Description of sex offender program with an individual focus (SEIF): content of the three treatment phases. Note. Lätth (2019), modified.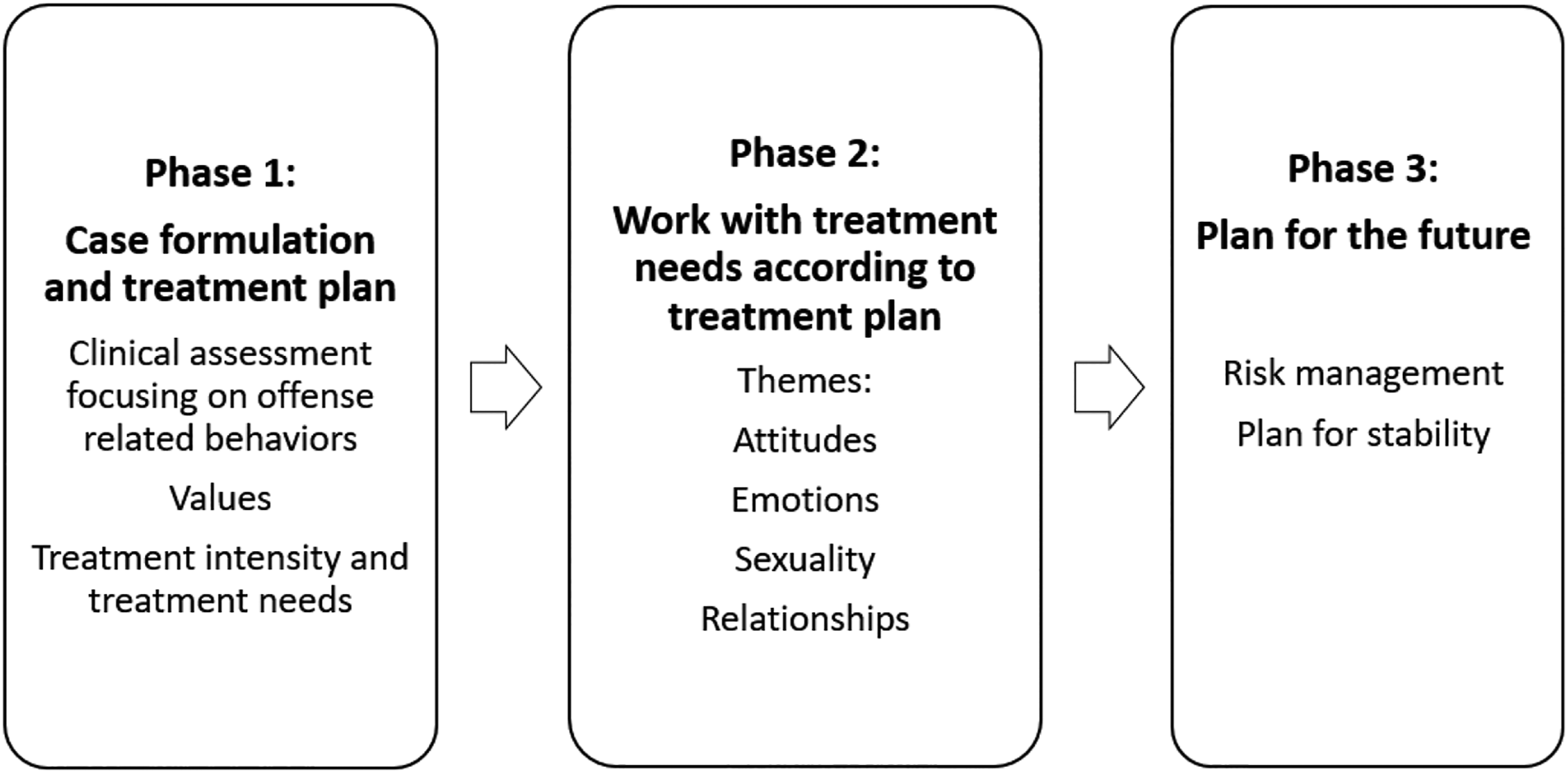
The second phase comprises work directed at individual treatment needs, revolving around themes concerning relationships, sexuality, (pro-criminal) attitudes, and emotions. Treatment components available in the manual are utilized with flexibility and include exercises based on traditional CBT techniques such as functional analysis, cognitive restructuring, self-regulation, role-play, mindfulness, and home assignments, among others. The therapeutic alliance and process is emphasized in SEIF and the therapist style include being non-judgmental, warm, and empathetic, in accordance with existing evidence (Ross et al., 2008; Marshall, 2005). The responsivity principle guides adjustments in the delivery of treatment where for instance sessions with hyperactive participants may include more breaks etcetera. During the last phase of SEIF, the participant establishes a plan for the future, including risk management (Kriminalvården Swedish Prison & Probation Service, 2019). Treatment progress defined as change in criminogenic needs, or reduction of risk factors, is rated midways through treatment and in the final phase using the TRS-2, which assists the therapist in assessing treatment duration.
Study Design and Sample
To test the research question and hypotheses, the study employed a pretest–posttest design to examine within-group change in criminogenic needs within a group of adult male, incarcerated or on probation, ISOs who completed SEIF, using self-report scores from three psychometric tests and therapist ratings. The combination of measurements contributes to answer the research question from different angles, enhancing validity. The study design, however, did not include a control group, which limits validity; these matters are further discussed in the discussion section of this article. Eligibility criteria for inclusion in the study were equivalent to the ones for inclusion in SEIF. The study sample comprised the first cohort of participants in the pilot run of SEIF: 99 male ISOs in five prisons and 14 probation offices all over Sweden were asked to volunteer for the study.
Data Collection
The empirical material comprises two parts: participants’ pre- and posttreatment self-reports and the therapists’ pre- and posttreatment ratings and were collected between August 2017 and February 2019, initiated for an internal pilot evaluation. A SEIF coordinator kept record of the first cohort of participants in SEIF, the 99 individuals comprising the study sample, and instructed therapists regarding data collection. The therapists who delivered SEIF to these participants conducted the therapist ratings, TRS-2, using a pseudonymized electronic document. Moreover, the therapists informed coordinating staff within the Prison and Probation Service, i.e., a probation officer or case manager, which individuals who were included in the study and coordinating staff in turn administrated participants’ pre- and posttests. Tests were filled out individually by pen and paper. The tests included a personal code securing pseudonymity and enabling matching of the pretest with the same participant’s posttest. During the data collection and analysis phase, it became evident that there was quite a large data loss, which I will address in the discussion (see figure 2 for details regarding data collection). Flowchart illustrating the data collection of participants’ self-reports and therapists’ ratings.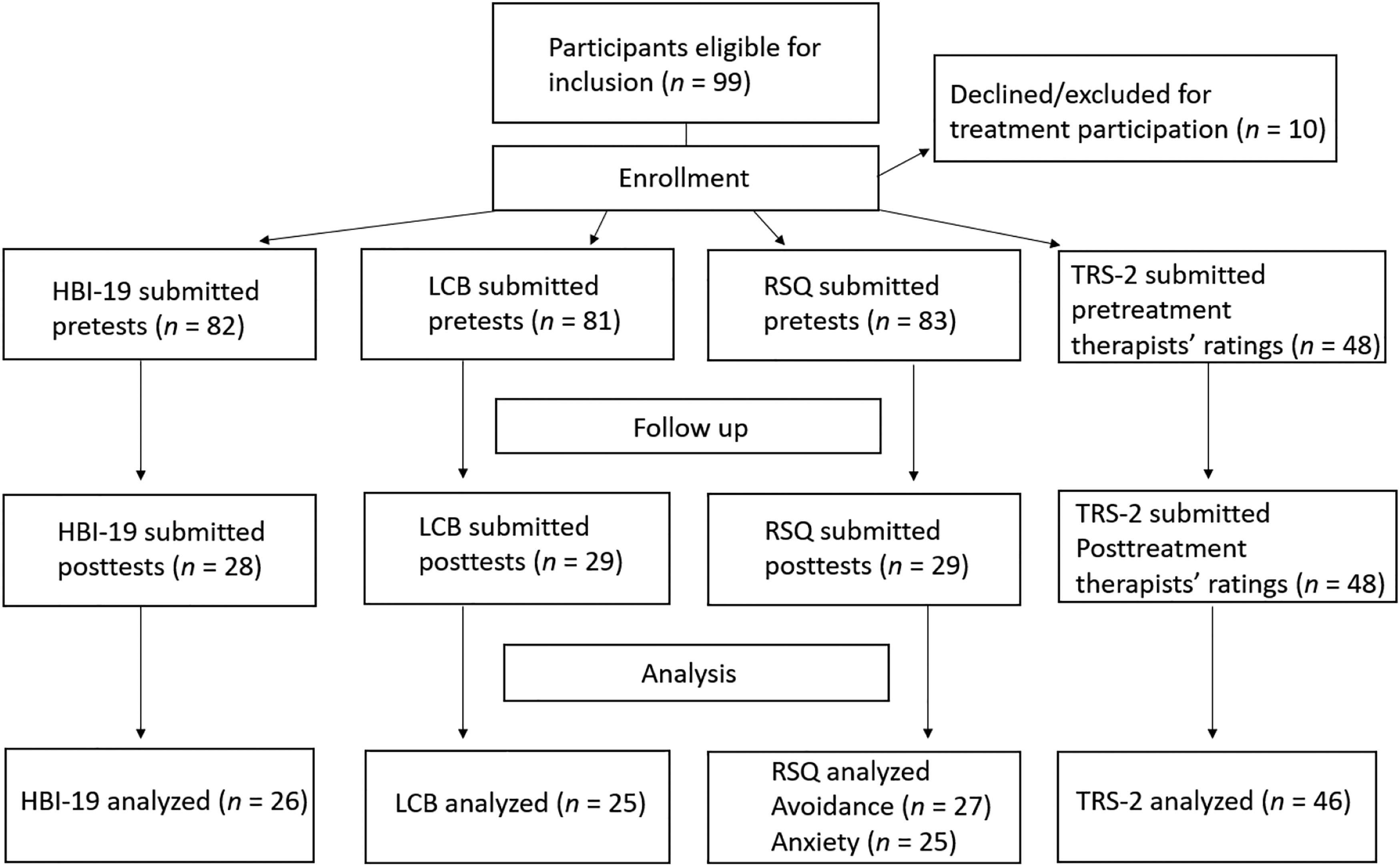
Ethical Approval
The study was initiated during the author’s master studies in social work and is now part of a larger doctoral project at Uppsala University investigating ISOs’ experiences of treatment and support for problems related to sexual offending. Institutional ethics approval was obtained from the Prison and Probation Service as well as from the University responsible for the master’s program (Ersta Sköndal Bräcke University College). The study adhered to the basic ethical guidelines of good research practice, produced by the Swedish Research Council (2017). From the start and throughout the study, all data were pseudonymized; thus, the identity of the participants was unknown. Participation in the study was voluntary and included informed consent, with awareness of the risk of participants feeling pressured to participate, due to the inherent power asymmetry in the Prison and Probation context.
Psychometric Measures and Rating Scale
The Hypersexuality Behavior Inventory-19 (HBI-19) was utilized to measure participants’ perceived problems regarding hypersexuality. It comprises 19 items, total score is 95 points, ranging from 19 to 95, using a five-point Likert scale where there is no reversed coding of items (Reid, Garos, & Carpenter, 2011). The domains include inability to control sexual fantasies or behaviors, using sex as a coping strategy, and inability to stop such behaviors despite negative consequences. The HBI-19 has demonstrated a high convergent validity in relation to other psychometric tests measuring hypersexuality and related concepts. The internal consistency for the scale overall has been shown to be high with a Cronbach’s alpha at .96, replicated in another study (Reid et al., 2012). Several reviews conclude that the HBI-19 is a reliable psychometric test to measure hypersexuality, within both clinical and non-clinical samples (Marshall & Briken, 2010; Montogomery-Graham, 2016; Stewart & Fedoroff, 2014). Suggested cutoff is at 53 points; thus, scores at and above this indicate clinically significant problems (Reid et al., 2011). Nevertheless, others argue cutoff cannot yet be determined (Bőthe et al., 2019).
To measure participants’ locus of control, the Locus of Control of Behavior Scale (LCB) was employed (Craig et al., 1984). The test includes 17 items, total score is 85 points, ranging from 0 to 85, using a six-point Likert scale and reversed coding for item 1, 5, 7, 8, 13, 15, and 16. Reliability measurements have demonstrated acceptable internal consistency with a Cronbach’s alpha of .79 regarding all items. Its construct validity has been examined through correlation measurements with the resembling Rotter’s I-e Scale, where the correlation coefficient was .67 for men and .66 for women (Craig et al., 1984).
Attachment was measured using the Relationship Scale Questionnaire (RSQ), developed by Griffin and Bartholomew (1994), comprising 30 items concerning aspects of relationships, using a five-point Likert-scale. The RSQ can be analyzed in several ways. Analysis using the four attachment categories, secure, fearful, preoccupied, and dismissing (Bartholomew & Horowitz, 1991) have been shown to range between a Cronbach’s alpha of .41–.70 in reliability measures, indicating limited internal consistency. For this reason, and because of the limited sample, it was decided to instead analyze RSQ employing the 2-factor loading of the anxious and avoidant dimensions. The 2-factor loading of RSQ is based on the model presented by Simpson, Rholes, & Nelligan (1992) and includes items 11, 18, 21, 23, and 25 for the anxiety dimension and items 10, 12, 13, 15, 20, 24, 29, and 30 for the avoidant dimension. Kurdek (2002) demonstrated this as being a more reliable approach, with the anxiety scores yielding a Cronbach’s alpha of .83 and the avoidant scores .77. Total score for the anxiety dimension is 25 points, ranging from 5 to 25, no reverse coding. Total score for the avoidant dimension is 40 points, ranging from 8 to 40, reversed coding for items 10, 15, and 30.
The Therapist Rating Scale-2 (TRS-2) (Marshall & Marshall, 2009) is an assessment tool for treatment needs and treatment progress and is based on research on criminogenic needs within the ISO population. Nonetheless, the items are also related to dynamic risk factors for general crimes, the Central Eight (Bonta & Andrews, 2017). Each item, or criminogenic need, yields a score of 1–4 on two categories of functioning: intellectual understanding and acceptance/demonstration, where the first indicates cognitive progress and the second observed behavioral change (Marshall & Marshall, 2009). Total score for the TRS-2 is 80 points, ranging from 20 to 80 where a total score of 50 points indicate attainment of the treatment goals and scores below 45 points indicate further need of treatment. Corresponding numbers for each of the 10 items is a total score of eight points, ranging from 2 to 8 where a total score of three points on each category, that is, in total six points, is indicative of attainment of the treatment goals for that specific criminogenic need. The TRS-2 is a fairly new instrument, and studies suggest that its psychometric properties are promising; moreover, it seems to be a comparatively valid predictor for recidivism in sexual crimes. The TRS-2 has a high inter-rater reliability and high internal consistency, with a Cronbach’s alpha of .97 for the total score, .96 for the intellectual understanding category, and .94 for the acceptance category (for references, see Marshall & Marshall, 2009).
Data Analysis
Data were analyzed using IBM SPSS Statistics 22. To test change in criminogenic needs, comparative analyses were conducted using non-parametric tests for paired groups using the Wilcoxon Signed Rank Test (Pallant, 2016). Mann Whitney-U tests were conducted for comparisons between independent sub-groups (participants on probation or in prison). The choice of non-parametric tests was due to several outliers and the limited sample size. To measure the size of significant changes, effect size was calculated (Cohen, 1988). Mean score was added for four tests on the LCB and three on the HBI-19 where only one value was missing, in order to enlarge the sample of matching pairs of tests. Cases missing one test (pre- or post-) were excluded, as well as cases with two or more missing values in either of the tests. Pseudonymized descriptive statistics of the 99 participant’s characteristics were obtained from the Prison and Probation Service.
Results
Participants
Results: participants. Assessed risk for recidivism in general and sexual crimes (n = 99).

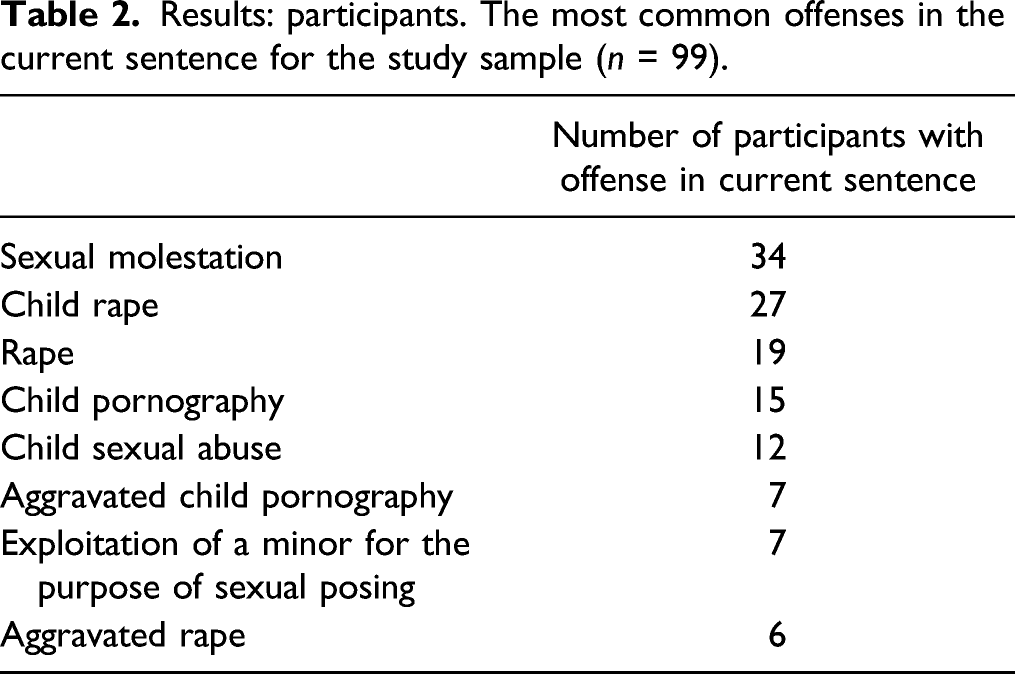
Results: participants. The most common offenses in the current sentence for the study sample (n = 99).
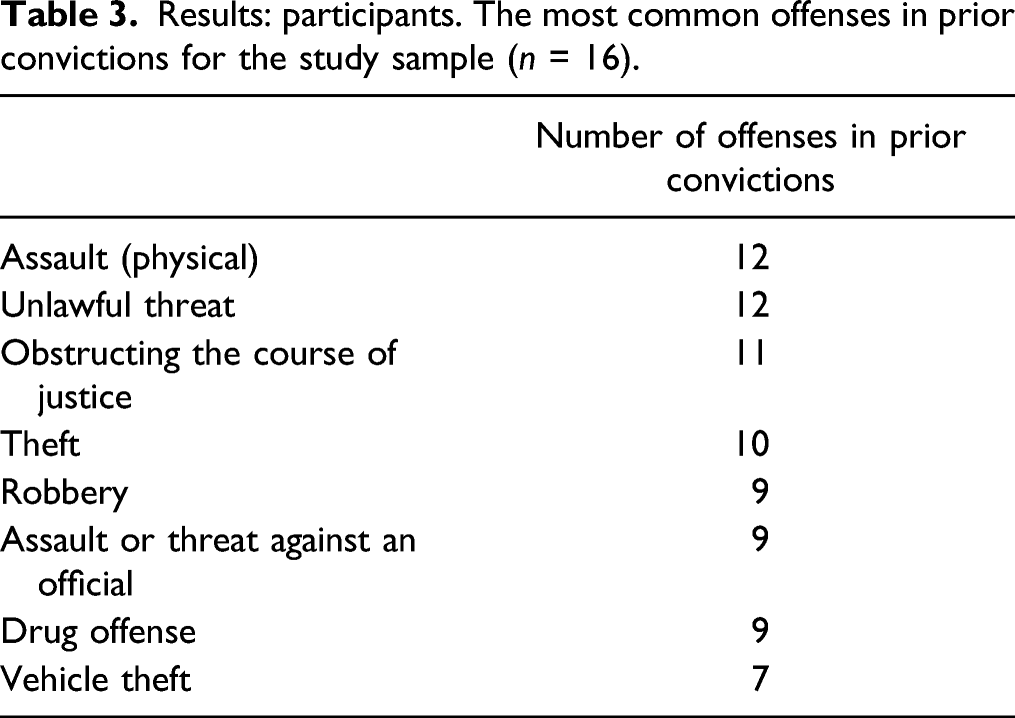
Results: participants. The most common offenses in prior convictions for the study sample (n = 16).
Data describing treatment intensity for all 99 participants were not available; however, data from the first 33 participants who finished SEIF during the study period show that on average, treatment intensity was 53 hours in total for participants on probation (M = 87 hours for group-format and M = 44 hours for individual format). For incarcerated participants, treatment intensity was 142 hours in total on average (M = 152 hours for group-format and M = 58 hours for individual format). The participant, of these 33 individuals, with lowest treatment intensity had 25 hours treatment in total and the one with highest intensity had 205 hours of treatment in total. As previously discussed regarding intervention format, the majority of probationers in the study received individual treatment and the majority of incarcerated participants received group treatment.
The 38 therapists participating in the study were all employed at the Prison and Probation Service. They had different educational backgrounds: 13 were licensed psychologists, nine had a bachelor’s degree in social work (four of them with additional basic psychotherapy education/training), nine had a bachelor’s degree in behavioral science, and the remaining seven had various bachelor’s degrees within the social sciences. Therapists who did not have basic psychotherapy training or a psychologist license received 12 weeks of basic training in cognitive behavioral therapy, before the specific SEIF training, described later. Specific experience of sexual offender treatment ranged between <1 and 9 years, with an average of 3.99 years. The average experience of any criminal offender treatment program was 9.27 years, ranging from <1 to 23 years.
The therapists engaged in 3 weeks of SEIF therapist group training, which included the theoretical foundations for SEIF, manual guidance, and skills training (experienced therapists who had previously worked with sexual offender treatment received 4 days of training). There was also specific training in working with sexual risk factors. In addition, the therapists completed an, on average 2–3 years, individual certification process. During this time, thus, the study period included, all therapists recorded their sessions, by audio or video, and they were under supervision of licensed psychologists, thus controlling for fidelity to the SEIF manual.
Hypersexuality (HBI-19)
The lowest possible score on HBI-19 is 19 points, and the total score is 95 points, where low scores indicate fewer problems related to hypersexuality. When analyzing all complete pretests, 11 participants (15%) scored at proposed cutoff or above (=> 53, Md = 25, M = 31.14, SD = 16.14, n = 72), thus, indicating clinically significant hypersexual problems. According to hypothesis 1, participants in SEIF would exhibit a statistically significant reduction in hypersexuality posttreatment compared to pretreatment. A comparison using the Wilcoxon Signed Rank Test for paired groups, of participants with complete pre- and posttests (n = 26), demonstrated a significant decrease in hypersexual problems posttreatment (p = .034, two-tailed), with a small to medium effect size (r = .29). The median score pretreatment was 30 (M = 31.12, SD = 11.83, n = 26) and posttreatment 24 (M = 27.92, SD = 15.07, n = 26). Thus, hypothesis 1 was supported and the null hypothesis was rejected. As demonstrated in figure 3, participants who experienced most problems regarding hypersexuality were also the ones with a larger decrease in scores. Since it is conceivable that hypersexual behaviors would decrease as a natural consequence while incarcerated, because of limited access to sexual stimuli, a comparison was made using Mann Whitney-U Test for independent groups between the two sub-groups in the study sample, i.e., participants on probation and participants in prison. This test did not demonstrate any significant difference between the probation and prison group, neither between pretreatment scores of each group nor between posttreatment scores. Hence, the reduction of hypersexual problems is not attributable to the sub-group of participants in prison alone, indicating that other factors beyond the restricted prison context, possibly SEIF, contributed to the changes identified. Results: hypersexuality pre- and posttreatment. Note. This figure demonstrates comparison of participants’ total scores on the HBI-19, where the y-axis reads the pretreatment scores and the x-axis posttreatment scores of each participant (n = 26). Participants above the diagonal reference line have lower scores posttreatment, thus indicating change in intended direction. The vertical and horizontal lines mark the proposed cutoff at 53 points.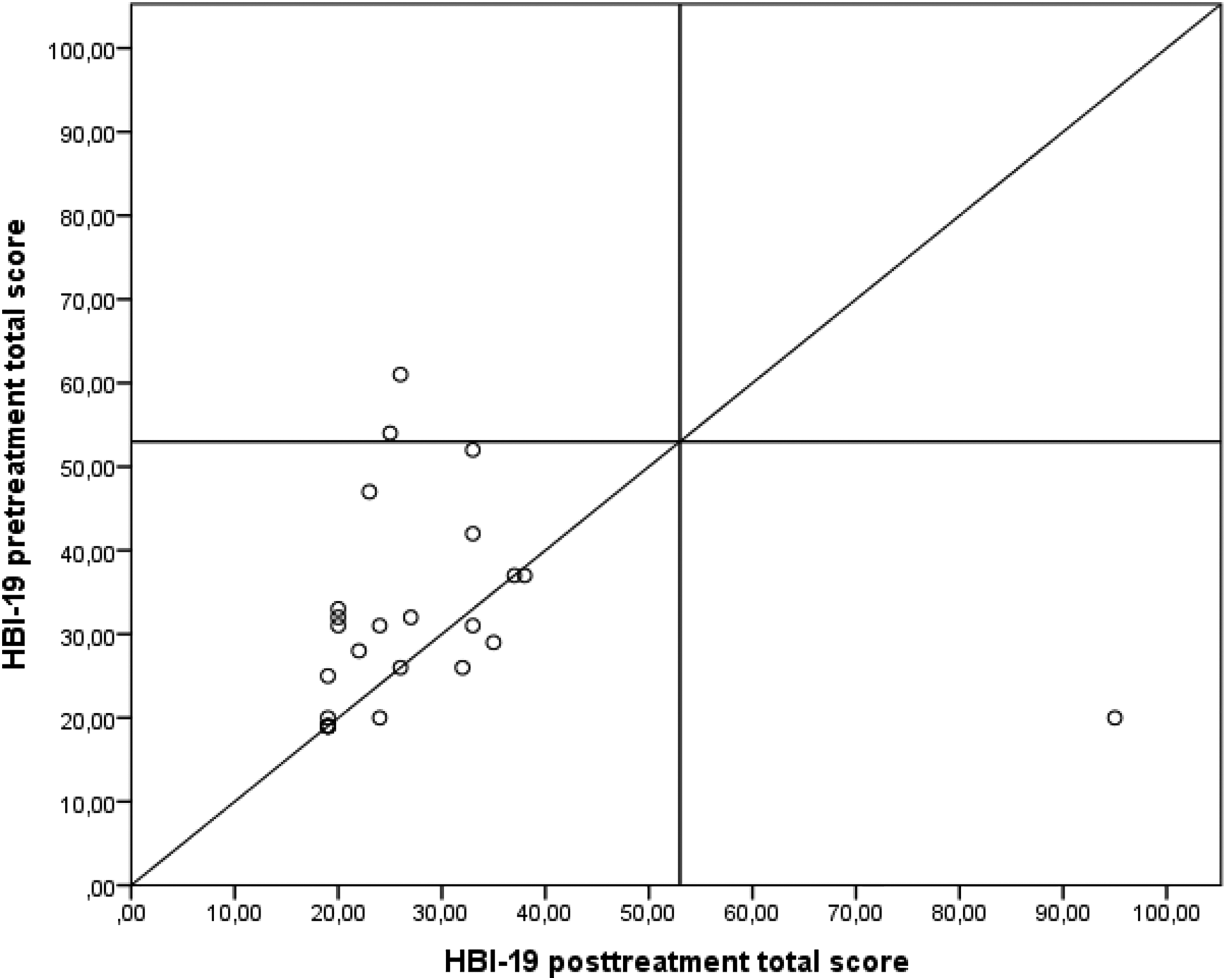
Locus of Control (LCB)
According to hypothesis 2, participants in SEIF would exhibit a statistically significant reduction in external locus of control posttreatment compared to pretreatment. A reduction of scores on LCB represents a decrease in external locus of control, or an increased internal locus of control, thus an indication of change in the intended direction. Mean score at pretreatment was 28.68 (SD = 10.43, n = 25) and at posttreatment 26.12 (SD =14.32, n = 25). A comparison using the Wilcoxon Signed Rank Test for paired groups demonstrated there was no statistically significant difference (p > .05, two-tailed) between the pre- and posttreatment scores, thus, hypothesis 2 was not supported and the null hypothesis could therefore not be rejected. However, there was a tendency for change with a small effect size (r = .19), where the median score at pretreatment was 28 and at posttreatment 22 (n = 25). This equals a 21% reduction of the median score. Seventeen of the participants (68%) lowered their scores posttreatment; thus, they experienced an increase in internal control. For six participants (24%), there was an increase in external locus of control.
Attachment (RSQ)
According to hypothesis 3, participants in SEIF would exhibit a statistically significant reduction in levels of anxiety as well as avoidance in their attachment styles posttreatment compared to pretreatment. Low scores on the RSQ are preferred, thus indicating low levels of anxiety or avoidance in the individual’s attachment style. There was no significant difference (p > .05, two-tailed) on either one of the dimensions between the pre- and posttreatment scores when conducting a Wilcoxon Signed Rank Test for paired groups. The mean score for the anxiety dimension was 10.80 (SD = 3.46, n = 25) and median 10 pretreatment, respectively, 11.28 (SD = 5.23, n = 25) and median 11 posttreatment. For the avoidance dimension, the mean was 20.74 (SD = 5.41, n = 27) and median 20 pretreatment, respectively, 19.78 (SD = 4.93, n = 27) and median 21 posttreatment. Accordingly, hypothesis 3 was not supported and the null hypothesis could not be rejected. Participants’ attachment styles did not change following treatment.
Therapists’ Ratings of Criminogenic Needs (TRS-2)
According to hypothesis 4, participants in SEIF would exhibit statistically significant higher levels of function regarding criminogenic needs, according to therapist ratings of treatment progress, posttreatment compared to pretreatment. The total rating of the TRS-2 ranges between 20 and 80 points, where a total of 50 points indicate attainment of the treatment goals. Thus, the therapist assesses the participant to have a normative function (corresponding to the levels of function expected in the general population) regarding the criminogenic needs assessed in this scale (Marshall & Marshall, 2009). Ratings less than 45 indicate treatment should continue, given the remaining treatment needs. A Wilcoxon Singed Rank Test for paired groups demonstrated a significant change (p < .001, two-tailed), in total scores between pre- and posttreatment ratings with a large effect size (r = .68). The mean pretreatment was 40.20 (Md = 41, SD = 10.29, n = 46) and posttreatment 51.78 (Md = 54, SD = 8.33, n = 46). Sixty percent of the participants were assessed to have reached the normative level of function, whereas 17% were assessed as being in need of further treatment. Pretreatment, the corresponding ratings were 20% for normative function and 63% for insufficient function, respectively.
Results: Therapists’ ratings of change in criminogenic needs pre- and posttreatment.
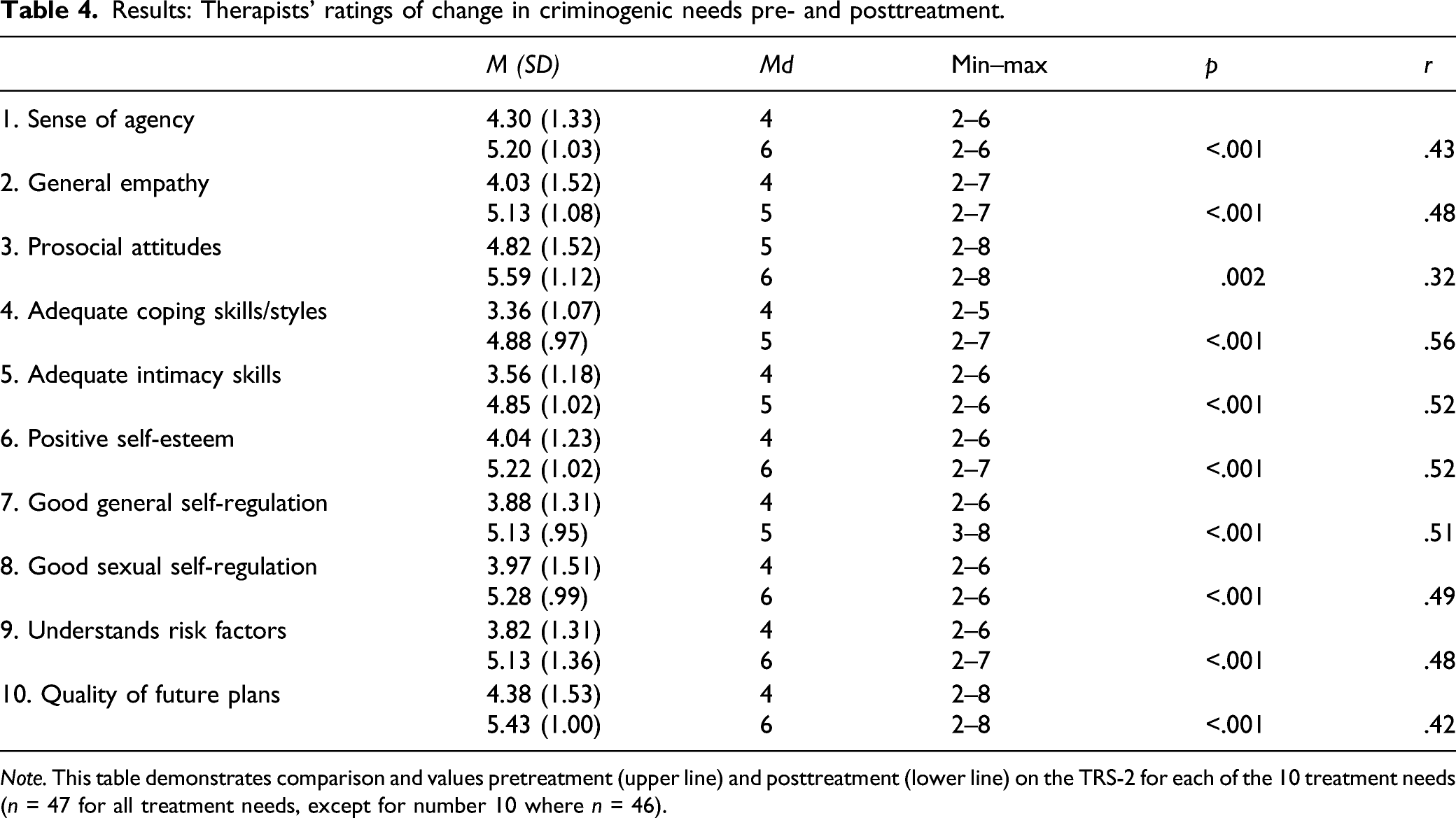
Note. This table demonstrates comparison and values pretreatment (upper line) and posttreatment (lower line) on the TRS-2 for each of the 10 treatment needs (n = 47 for all treatment needs, except for number 10 where n = 46).
Another comparison analysis was conducted between pre- and posttreatment ratings of the two categories of the TRS-2 called intellectual understanding and acceptance/demonstration, where the ratings range between 10 and 40 points. A Wilcoxon Signed Rank Test for paired groups demonstrated there was a significant difference for both categories (p < .001, two-tailed), with a large effect size (r = .56 for intellectual understanding and r = .57 for acceptance/demonstration, respectively). The mean rating for intellectual understanding pretreatment was 21.47 (SD = 5.34, Md = 22, min = 10, max = 31, n = 46) and posttreatment 27.42 (SD = 4.18, Md = 29, min = 13, max = 34, n = 46). For the acceptance category, the mean rating pretreatment was 18.74 (SD = 5.23, Md = 19, min = 10, max = 29, n = 46) and posttreatment 24.36 (SD = 4.35, Md = 25, min = 11, max = 31, n = 46).
To reach the normative (desired) level of function posttreatment, for each of the 10 treatment needs, the participant needs to reach a rating at a minimum of three points on both the intellectual understanding and acceptance category. The proportion of participants reaching this level for each treatment need in the TRS-2 is demonstrated in figure 4. Results: therapists’ ratings of treatment progress. Note. This figure demonstrates comparison between pre- (a) and posttreatment (b) ratings of each treatment needs in the TRS-2. The bars represent the proportion (%) of participants who have been rated to reach the normative level of function, that is, attainment of the treatment goals, on both intellectual understanding and acceptance/demonstration categories (n = 47, except for treatment need 10, where n = 46). 1. Sense of agency, 2. general empathy, 3. prosocial attitudes, 4. adequate coping skills/styles, 5. adequate intimacy skills, 6. positive self-esteem, 7. good general self-regulation, 8. good sexual self-regulation, 9. understands risk factors, and 10. quality of future plans.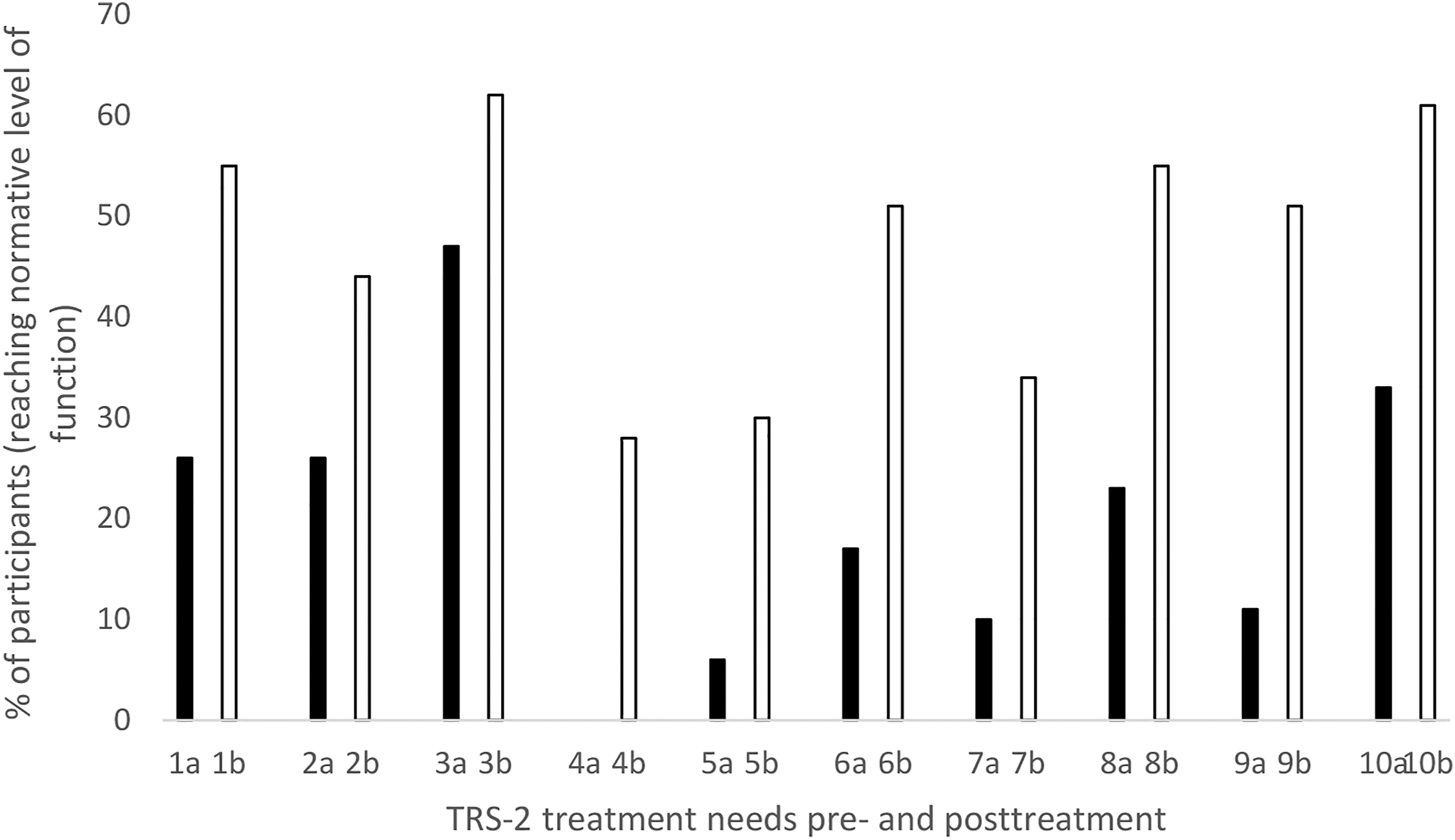
Discussion and Applications to Practice
The results of the participants’ self-reports demonstrate a significant decrease in hypersexuality (small to moderate effect size), a non-significant increase in internal locus of control, but no change regarding attachment styles. In addition, the therapists’ ratings demonstrated a significant decrease in all criminogenic needs (which include the Central Eight risk factors), with medium to large effect size, and 60% of the participants were assessed to have achieved the treatment goals posttreatment, according to the TRS-2. Both the therapist ratings and participants’ self-reports point in the same direction, indicating the positive outcomes are valid. The main difference is that therapist ratings demonstrate change in all studied areas and with larger effects than participants’ self-reports, which can be a result of therapists’ confirmation bias, thus, a non-deliberate exaggeration of treatment progress.
In Sweden, there is lack of research regarding psychosocial interventions in general, although the number of studies is growing. Sundell and Åhsberg (2018) highlight the need for service providers to examine interventions in terms of potential harms and benefits. The results suggest SEIF does not appear to have negative effects (the outlier in figure 3 is most likely a result of inaccurate responses); on the contrary, the study indicates SEIF may reduce problems related to increased risk of recidivism, especially hypersexuality. These findings motivate further implementation of SEIF. However, this study cannot evaluate the effectiveness of the program, due to limitations as discussed later. Hence, further studies are necessary. Nevertheless, the results are in line with previous research indicating that CBT-based sexual offender programs that adhere to the RNR-model are effective (Hanson et al., 2009). The improvements demonstrated in this study can be interpreted using Bandura’s concept of self-efficacy (Bandura, 1997), explaining how the participants’ beliefs in their function and abilities to manage events and obstacles in their lives were strengthened by the engagement in SEIF.
The fact that the specific elements of SEIF, targeting sexual self-regulation, seem to be particularly successful, especially for participants with severe hypersexual problems, is worth noting since it is one of the strongest predictors of recidivism (Hanson & Morton-Bourgon, 2005). This result is in line with previous studies of a non-offending population (Hallberg et al., 2019; Hook et al., 2014; Kjellgren, 2019; Miles et al., 2016; Wilson & Fischer, 2018). Since it has been suggested that hypersexuality is dimensional, reflecting differences in degree rather than kind (Walters et al., 2011), reductions in scores of participants who, pretreatment, scored below the proposed (Reid, Garos, & Carpenter, 2011), as well as the debated (Bőthe et al., 2019) cutoff, might also be of significance. These findings are relevant to practitioners and highlight the need to focus explicitly on sexual problems for ISOs experiencing hypersexuality. Therapists in this study had special training in working with participants’ sexual self-regulation and it is conceivable that such specific training is important due to the sensitive nature of this topic.
Approximately two-thirds of the participants experienced a (non-significant) increase in internal locus of control, which corresponds to the results of other studies, indicating psychological treatment can increase internal locus of control in the ISO population (Fisher et al., 1998; Mandeville-Norden et al., 2008; Olver, Nicholaichuk, & Wong, 2014). This study also supports previous findings (employing other types of psychometric tests) that specifically CBT for ISOs can have a positive impact on internal locus of control (Jung & Gulayets, 2011; McAnena et al., 2016). The fact that the above-mentioned studies demonstrated significant effects on locus of control, in contrast to this study, might be due to a larger sample.
SEIF did not seem to have an impact on the participants’ attachment styles. The only study of change regarding the attachment styles of ISOs posttreatment found in the literature review, also using RSQ 2-factor, demonstrated, in line with this study, that there was no change in avoidant attachment styles. However, the opposite was evident for the anxious dimension (Grady et al., 2016). One possible explanation for the differences may be that the treatment program in the latter study was more intensive, since frequency and duration of therapy have been suggested to be of importance (Parish & Eagle, 2003). Another explanation is that attachment styles are developed throughout the course of life and are fairly stable in their nature and therefore perhaps not as easy to alter, in comparison to other treatment targets. The study of attachment in relation to stability and change, especially in the ISO population, is however very complex. Thus, conclusions should overall be drawn cautiously (see discussions in Martin & Tardif, 2015; Martin & Tardif, 2014).
The results from the TRS-2 show that the levels of the intellectual understanding of criminogenic needs are higher than for the acceptance/demonstration category. Hence, one might speculate whether the behavioral change is preceded by cognitive change or whether the treatment program is more effective in addressing cognitive processes than behavioral processes. Moreover, the therapist ratings (see figure 4) demonstrate that salient criminogenic needs in this study sample appear to be inadequate coping styles and intimacy skills and that it may be possible to achieve improvements in these areas with cognitive-behavioral treatment components. This can be put in relation to the participants’ own perceived decrease in hypersexual behaviors; hence, improved coping and intimacy skills may reduce the need to use sex as emotion regulation, or a substitute for attachment-related needs, as well as facilitate control over excessive sexual behaviors.
It should be noted that this study does not reveal whether participants’ recidivism risk was altered; furthermore, it does not show whether the changes in criminogenic needs persisted, since there was no follow-up. Previous studies have supported the use of psychometric self-reports and ratings of treatment gains as valid predictors of recidivism (Allan, Grace, Rutherford, & Hudsonet, 2007; Beggs & Grace, 2011; Craig, Thornton, Beech, & Browne, 2007; Thornton, 2002), while others have not (Barnett, Wakeling, Mandeville-Norden, & Rakestrow, 2012; 2013; Olver, Kingston, Nicholaichuk, & Wong, 2014; Wielinga et al., 2021). However, some of these varied results may be related to the risk relevance of the construct measured (Wielinga et al., 2021). The use of self-reports in general can be questioned from a methodological standpoint, specifically those regarding attachment (Martin & Tardif, 2014; Stirpe, Abracen, Stermac, & Wilson, 2006). Another caution, previously mentioned, concerns the therapists’ ratings in this study, which highly likely were influenced by confirmation bias and overstatements of client improvement (cf. Walfish, McAlister, OʼDonnell, & Lambert, 2012). Participants’ self-reports could also reflect social desirable responding, even though this may not necessarily be the case (Fisher et al., 1998; Pham, Nunes, Maimone, & Hermann, 2021).
Although the results indicate positive outcomes, there are several methodological limitations to this study. The study comprised a small convenience sample without a control group; hence, it cannot be ruled out that the measured change was due to other factors than the intervention and generalizability is limited. However, the ecological validity of the study is high since it was conducted in the regular setting, studying regular activities, within the Swedish Prison and Probation Service. It was unfortunately not possible to compare therapists’ ratings with participants’ self-reports because the material was pseudonymized and no code key existed. Another significant limitation is the large amount of missing data. Because data were pseudonymized, it was not possible to analyze potential differences between the participants who dropped out and those that completed the treatment program and/or the self-reports. Ten participants, of the initial 99, never started the treatment for different reasons. Statistics for all the SEIF-participants during the study period (not only those included in the study) demonstrate that in general, for one-third of SEIF-participants, treatment was not completed or they were transferred for different reasons. The remaining data loss, regarding the participants’ self-reports, could be accounted for by those who simply did not wish to further participate in the study. In addition, some self-reports did not contain the personal code; thus, pre- and posttests could not be matched. The therapists handed in only 46 completed pre- and postratings from the TRS-2 out of a total of 99. This might partly be due to the participants’ dropout rates but also therapists’ retirement, employment termination, sick and parental leave, or non-compliance because of workload or other reasons.
In future research on sexual offender treatment, it could be of relevance to look into participants’ self-reports of other types of criminogenic needs demonstrated to have a high impact on recidivism, such as antisocial behaviors and general self-regulation (Hanson & Morton-Bourgon, 2005). In addition, the risk of social desirable responding in self-report studies could be managed using, for instance, residual change scores, as demonstrated in the 18-year follow-up study of treated ISOs by Olver, Nicholaichuk, and Wong (2014) or by adding formalized risk assessment tools. In similar pilot or feasibility studies on new treatment programs, additional data could be collected, exploring the implementation process. A randomized, controlled effectiveness study of SEIF, investigating outcomes in terms of re-offense using a larger sample, is necessary. A qualitative study of SEIF on treatment experience from a participant perspective is ongoing at the moment.
Footnotes
Acknowledgments
The author would like to thank the Swedish Prison and Probation Service, especially Cecilia Fielding, Johanna Lätth, Josefine Börjesson, and Martin Lardén, as well as all the participants, therapists and staff involved in the study. Also, thanks to Ann Björkdahl at Ersta Sköndal Bräcke University College, for guidance, especially regarding data analysis and the Emotion-Justice-Interaction research group as well as PhD supervisors Stefan Sjöström, Maritha Jacobsson, and Rafael Lindqvist at Center for Social Work (CESAR), Department of Sociology at Uppsala University, for valuable input.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. However, the author was employed by the Swedish Prison and Probation Service when data for this study was collected.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.