
Abstract
Purpose:
To test an empirical model of the effects of a trauma-informed organizational environment on service user outcomes in the context of concurrent disorder treatment.
Methods:
Service users (n = 172) were surveyed while in treatment to determine the effects of trauma-informed organizational dynamics (i.e., safety, trust, choice, collaboration, and empowerment) on service user intrapersonal development outcomes (i.e., self-awareness, outlook, coping ability, self-worth, and self-determination) and improvements with concurrent disorder behaviors. After testing for validity and reliability of latent factors, data were analyzed using multivariate analysis.
Results:
As a concise analytical model, the trauma-informed organizational environment was found to significantly positively predict all service user intrapersonal outcomes as well as a reduction in concurrent disorder behaviors.
Conclusions:
This study informs developments in the design and implementation of trauma-informed practice frameworks for concurrent disorder treatment and emphasizes the importance of adapting organizational environments to support improved client outcomes.
Keywords
Recent research and practice in human service program delivery has focused on the efficacy of trauma-informed practice in contributing to service user positive outcomes in a variety of contexts such as treatment centers for substance misuse (Hales et al., 2019; Shier & Turpin, 2017), domestic violence shelter services (Kulkarni, 2019; Sullivan et al., 2018), and child welfare services (S. M. Brown & Bellamy, 2017; Tullberg et al., 2017). As knowledge is developed in this field, researchers and practitioners alike can begin to develop frameworks for organizations that apply a trauma-informed lens to the provision of services aimed at supporting groups with histories of trauma. This study aims to provide an empirical model that can be implemented and support organizational development within current disorder treatment programs—that is, services that seek to support the recovery of individuals experiencing adverse symptomology arising from both a substance misuse and mental health concern (Skinner, 2005). A cross-sectional quantitative design is employed to validate a model of trauma-informed organizational experiences before using it to test for service user outcomes in a concurrent disorder treatment program.
Trauma-informed practice is conceptualized as “an approach to organizing treatment that integrates an understanding of the impact and consequences of trauma into all clinical interventions as well as all aspects of organizational function” (American Association of Residential Centers, 2014). Similar definitions (Bailey et al., 2019; Donisch et al., 2016) also make the distinction between implementing trauma-informed practice at both a service and organizational level, while emphasizing the role of structural frameworks which can be used to guide an approach to service provision that is sensitive to previous trauma experienced by service users (Akin et al., 2017; Bailey et al., 2019). Furthermore, trauma-informed practice has been studied to occur in various contexts and at different levels of an organization (Maguire & Taylor, 2019; Record-Lemon & Buchanan, 2017). Largely absent from this body of literature is research evidence of the effects of trauma-informed organizational dynamics on service user outcomes. Furthermore, also absent is the development and application of organizational models of trauma-informed practice that are tested in specific service contexts. By focusing on concurrent disorder treatment, the following research addresses this gap by providing a population-specific account of developing trauma-informed organizational dynamics to suit service user needs. The research highlights the importance of adapting and developing organizations as an important intervention tool to enhance service user outcomes. This research is informed by the following research question: How do trauma-informed organizational dynamics effect service user outcomes in concurrent disorder treatment and recovery?
Literature Review
Identifying trauma-informed organizational experiences was done by assessing seminal research outlining the tenets of trauma-informed practice. This research builds from a highly cited (Hales et al., 2017; Lang et al., 2016; Levenson et al., 2016; Martin et al., 2017; Wolff et al., 2015) model by Harris & Fallot (2001), which is comprised of five core values including safety, trust, empowerment, choice, and collaboration. Fallot and Harris (2009) also indicate that trauma-informed practice can be applied to service users and staff alike and has been confirmed in research such as a study by Izzo et al. (2016), which found that the development of trauma-informed care at the staff and organizational levels led to improved well-being for youth at a residential child care center.
Safety
Safety in trauma-informed practice refers to the physical, psychological, and emotional comfort of service users (Harris & Fallot, 2001). Safety can be developed at the individual, social, and cultural levels of an organization (Shier & Turpin, 2017; Wilson et al., 2015) and often includes both interpersonal and structural dynamics (Kusmaul et al., 2019). Commonly, safety is related to physical security, which has been accomplished through the decreased use of seclusion and restraints for inpatient units (Muskett, 2014; Wilson et al., 2015) and night checks in residential treatment (Kusmaul et al., 2019). However, less tangible (but equally important) aspects of safety include psychological and emotional domains, which have been supported by creating a welcoming physical environment (J. M. Wilson et al., 2015) and setting policies for risk management (Wolf et al., 2014). Other examples of promoting safety include continuity of engagement with the same staff throughout a program (Ashby et al., 2019), development and reviewing of safety plans with service users (Heffernan & Blythe, 2014), clear policies for maintaining service user confidentiality (Shier & Turpin, 2017), and the use of respectful and trauma-sensitive language (Baker et al., 2018; J. M. Wilson et al., 2015). Finally, screening and assessing for trauma has been found to contribute to safety as program staff can use this information to establish parameters for individualized trauma-sensitive care (Drabble et al., 2013).
Trust
Trust is generally conceptualized as the forming of genuine and transparent relationships between service users and staff that set clear expectations about service delivery (Muzik et al., 2013). The cultivation of respectful and nonjudgmental trusting relationships has been cited as a key component of therapeutic relationships (Shier & Turpin, 2017); these aspects are found to lead to more positive program outcomes as they increase service user engagement (J. D. Brown et al., 2017; Muskett, 2014). Building trust is often associated with program models that are flexible and allow for individualized service responses (Heffernan & Blythe, 2014). Common characteristics of highly individualized services include the development of thorough service user profiles (Kusmaul et al., 2019), following through on program agreements (Reeves, 2015) and the development of a shared understanding of a service user’s key goals and outcomes (Shier & Turpin, 2017; A. Wilson et al., 2017; Wolf et al., 2014). Once trust has been established, the open and genuine connection between the service user and the service provider allows the opportunity for the service user to share their experiences in a safe and nonjudgmental space (Kirst et al., 2017; Reeves, 2015). This finding has been validated in studies such as an evaluation of a Colorado maternity program conducted by Ashby et al. (2019), which found that a safe and trustworthy clinic environment led to an increased number of visits by service users.
Choice
Choice is generally defined as providing the service user with control and input over the services they receive (Harris & Fallot, 2001). Choice is found to follow an empowering approach, as service users are better informed and better equipped to make decisions regarding the level and type of service they need (Hunt et al., 2018). Providing choice to service users can include providing a range of available services and/or allowing a service user to decide on their own level of participation (Murshid & Bowen, 2018; Shier & Turpin, 2017). Providing choice has been identified and studied in various service contexts; examples include providing youth their choice of food, clothing, and de-escalation techniques in residential treatment (Latham et al., 2010), offering patients in acute mental health settings a choice of how to regulate their emotions (A. Wilson et al., 2017), and providing an option to share or not share personal traumatic stories at a domestic violence program (J. M. Wilson et al., 2015). Some research has indicated the need for flexible and adaptable service models as programs seek to provide choice for service users (Brunzell et al., 2016).
Collaboration
Collaboration refers to developing meaningful partnerships with service users in the delivery of services and balancing the power differential between staff and service users (Harris & Fallot, 2001). In trauma-informed practice, service users should be actively involved with program planning to ensure that organizations are providing relevant services (Kusmaul et al., 2019; Lang et al., 2016). Collaboration can also occur within service user groups to provide peer-based support services (Ashby et al., 2019). These interactions are often fostered within collaborative treatment “spaces” (Vakharia & Little, 2017) where staff and service users integrate treatment experiences together. Moreover, collaboration is often understood at the programmatic level to include the integration of a broad set of services such as medical support, group therapy, childcare, and different types of personal counseling (Drabble et al., 2013; Kirst et al., 2017). Within these programs, collaborative efforts between service users and staff are often described as following a shared decision-making model (Crandal et al., 2019) where both sides join to mutually develop a program plan (Keesler, 2016).
Empowerment
Lastly, human service organizations often empower service users by recognizing their strengths and providing the tools to address psychosocial challenges (Phifer & Hull, 2016). This can be accomplished by developing trauma education and awareness programs which instill coping strategies that can be used outside of the service context (Kusmaul et al., 2019; J. M. Wilson et al., 2015). Within these programs, service users are often positioned as experts on their own life experiences and trauma and are given the opportunity to make informed decisions about their goals and the services they receive (Ashby et al., 2019; Reeves, 2015; Wolf et al., 2014). Relatedly, Scheer and Poteat (2018) have shown that greater empowerment in trauma-informed practice is associated with greater emotional regulation, lower social withdrawal, and better health outcomes for LGBTQ intimate partner violence survivors. Other research has noted the use of peer-based support in residential programs as a way to foster mutual support and empowerment among service users (Turpin & Shier, 2017a). Similar programs have been shown to empower service users by providing the opportunity to give back meaningfully to the community (Heffernan & Blythe, 2014; Muskett, 2014).
A Model of a Trauma-Informed Organizational Environment
While trauma-informed practice has been applied and studied across multiple fields and implemented in various human service agencies (Reeves, 2015), the implementation of trauma-informed practice is best informed by program models which apply directly to specific service contexts and outcomes, especially if the agency is traditionally a very structured environment (Keesler & Isham, 2017; Unick et al., 2019). While research continues to support the positive effects of trauma-informed practice directly on service user groups, such as children (Bailey et al., 2019; Izzo et al., 2016; Murphy et al., 2017), people living with addictions (Shier & Turpin, 2017), people experiencing housing loss (Hopper et al., 2010), and people with intellectual disabilities (Keesler, 2016), it has neglected the development and testing of factors relating to the organizational environment that support the implementation of trauma-informed practice. Given the research summarized above, the following hypotheses were developed about the relationship between trauma-informed organizational experiences and service-user intrapersonal outcomes:
Finally, because this literature provides a conceptual basis for developing a holistic trauma-informed organizational environment, based on the key characteristics of how safety, trust, empowerment, choice, and collaboration are potentially experienced within human service organizations by service users, the final hypotheses is tested:
Method
Procedure
This study utilized quantitative research methods to survey participants (n = 172) of a multisite (three in total) concurrent disorder program about their experiences while engaged in treatment, including the extent to which they achieved specific intrapersonal development outcomes, their level of engagement in concurrent disorder behaviors, and the effect of trauma-informed organizational experiences on these outcomes. Each of the measurement tools used to assess these variables (presented below) were developed from previous qualitative research (Shier & Turpin, 2017; Turpin & Shier, 2017b) that characterizes how each construct is experienced by service users when engaged in concurrent disorder treatment programs at the partner organization. Data were collected with the aid of the Qualtrics online survey platform and followed a repeated measures research design.
The partner organization utilized a general biopsychosocial model of intervention that consisted of psychoeducational group practice and individual counseling that is common in treatment for substance misuse (Turpin & Shier, 2018). Each of the program sites was long-term residential, with program lengths of 6 months to 1 year. Furthermore, as a spiritually based organization, programming also included onsite religious observation (however, this was not mandatory). Abstinence was required to maintain program involvement, and residents had to be 18 years or older.
Sample
Study respondents (n = 172) included adult participants engaged in a concurrent disorder treatment program at one of the three sites, which were managed by the partner organization. Respondents had experienced current issues associated with substance misuse and adverse mental health symptomology, which were being treated by the partner organization at the time of data collection. Eligibility criteria for the concurrent disorder programs were minimal (i.e., age and gender based on program site), which contributed to a diverse demographic spread within the sample. Inclusion criteria for the study were that respondents met inclusion criteria for the concurrent disorder program and completed the program.
Recruitment
Initially, at time of intake into one of the concurrent disorder treatment programs, service users were asked by the intake coordinator whether they would be willing to participate in a program evaluation being undertaken at the organization. They were provided with an informed consent form with details about the study and contact information for the principal investigator (PI). This study received ethics certification from the Health Sciences Research Ethics Board, University of Toronto. The PI provided training to organizational personnel who were aiding in the recruitment and data collection processes. All respondents were informed of their right to leave the study at any point during their treatment, at no consequence to their receipt of services. At the time of program completion, the program staff working with the client for their discharge planning again inquired with the program participant about their willingness to continue participating in this evaluation. They were once again provided with a copy of the informed consent for the study. Those that completed both time points were provided with a small honorarium (i.e., CAD$10 gift card) to show appreciation for their time.
Data Collection
Respondents in agreement to participate were given a research participant identifying number, which was added to their client file and was accessible on a tablet device supplied by the PI. The device was then passed to the respondent to complete the survey at intake and again when leaving the program. The research identifying number was necessary for the purposes of linking data to assess the improvement of concurrent disorder behaviors (i.e., the intended goal of the programming efforts). All data were held in confidence since the PI was the only one who had access to the Qualtrics account where data were collected and stored during the course of the study.
At the time of intake, respondents were asked to complete the Global Appraisal of Individual Needs Short Screener (GAINs-SS) and several demographic and social situation questions. This was used as a baseline source of data upon entry into the partner organization’s programs. At time of program completion, research participants were asked to complete the full survey with measures (listed below) assessing the (1) characteristics of trauma-informed organizational experiences, (2) levels of key intrapersonal factors that help prevent relapse and improve concurrent disorder behaviors, and (3) GAINs-SS to assess concurrent disorder behavior levels.
Measures
GAINs-SS (Version 2.0.3)
GAINs is a questionnaire designed to assess substance use as well as psychological and physical health. It is utilized to assist clinicians in diagnosis and planning of treatment. A short form of the measure that has been modified is employed by the partner organization. The short form comorbidity scales have moderate to high reliability and are highly correlated with the long form (Coleman-Cowger et al., 2013; Dennis et al., 2003; Titus et al., 2008). Construct validity has been found to not differ between the long and short form. The short scale maintains good sensitivity and specificity for predicting diagnostic impressions (Dennis et al., 2003; McDonell et al., 2009; Titus et al., 2008). Symptomologies related to substance user disorder are measured on a 5-point Likert-type scale where lower scores indicate a higher instance of a disorder. For this study sample, using Cronbach’s α measure of internal consistency, the reliability of the total GAINs-SS at intake was .83 and .87 at program completion.
Intrapersonal development outcomes
Intrapersonal development outcome measures were developed and used to assess the related outcomes of service users after their engagement with the program. The measures reflect dynamic developmental areas that have been associated with better recovery and relapse outcomes for individuals with substance use disorders. These outcomes consisted of self-awareness, outlook, coping ability, self-worth, and self-determination. Scale items as shown in Table 1 were identified in an earlier qualitative study (Turpin & Shier, 2017b) using a different sample from the same partner organization, and each has been identified in previous research documenting intrapersonal development-related outcomes that lead to recovery from substance use. Each was measured on a 6-point Likert-type scale with multiple items, with response categories ranging from strongly disagree to strongly agree. To measure the validity of each intrapersonal development measure, a confirmatory factor analysis (CFA) was conducted, including comparative fit index, Tucker–Lewis index, and root mean square error of approximation. Fit indices as shown in Table 2 support the adoption of all five factors, which are shown to have overall strong construct validity for sample sizes under 500 (Kline, 2011). Cronbach’s α measure of internal consistency for each measure ranged from .91 to .94, indicating strong reliability.
Items on the Interpersonal Development Social Outcomes Scale.
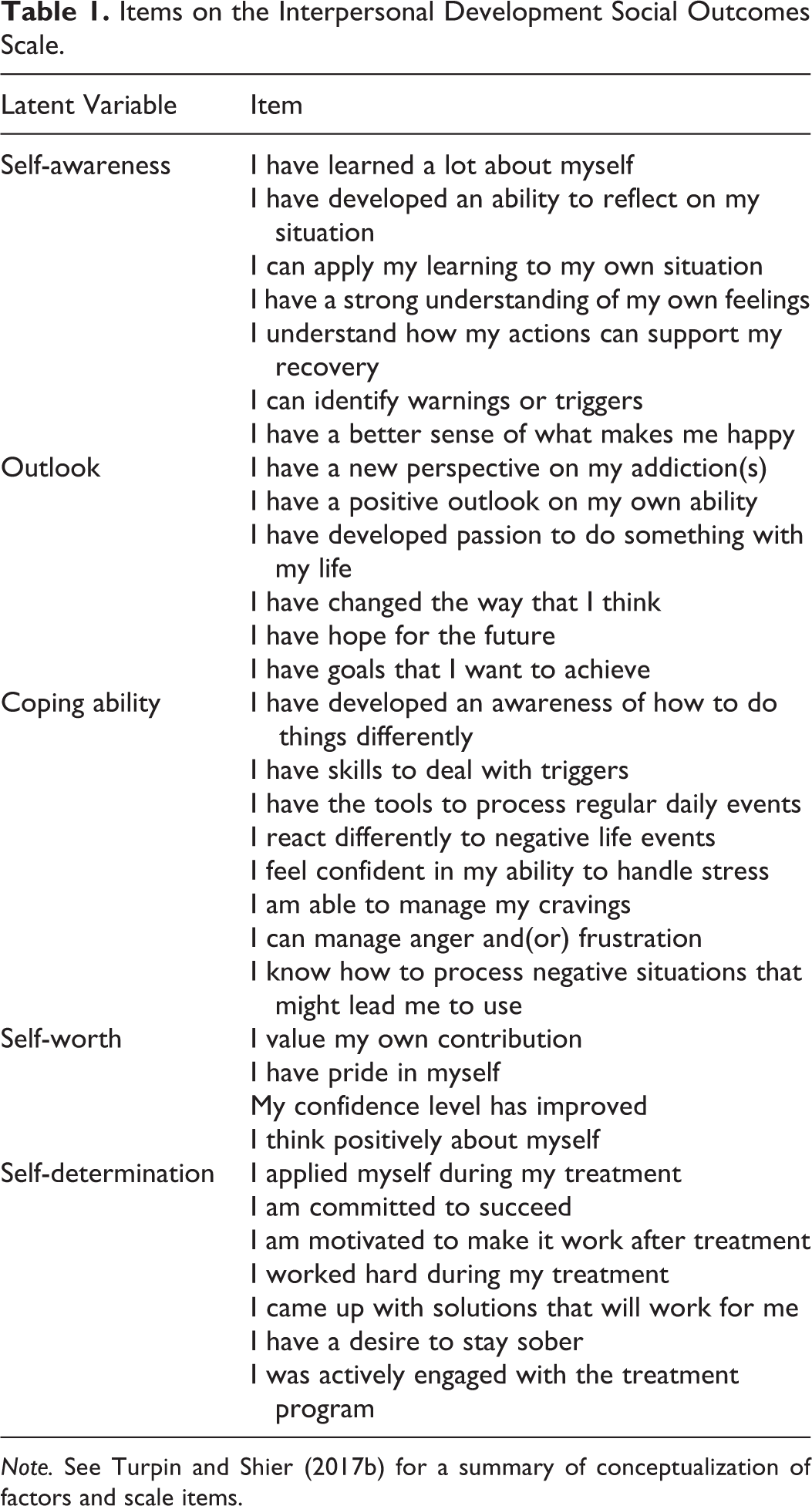
Note. See Turpin and Shier (2017b) for a summary of conceptualization of factors and scale items.
Reliability and Validity of Independent and Dependent Variables.
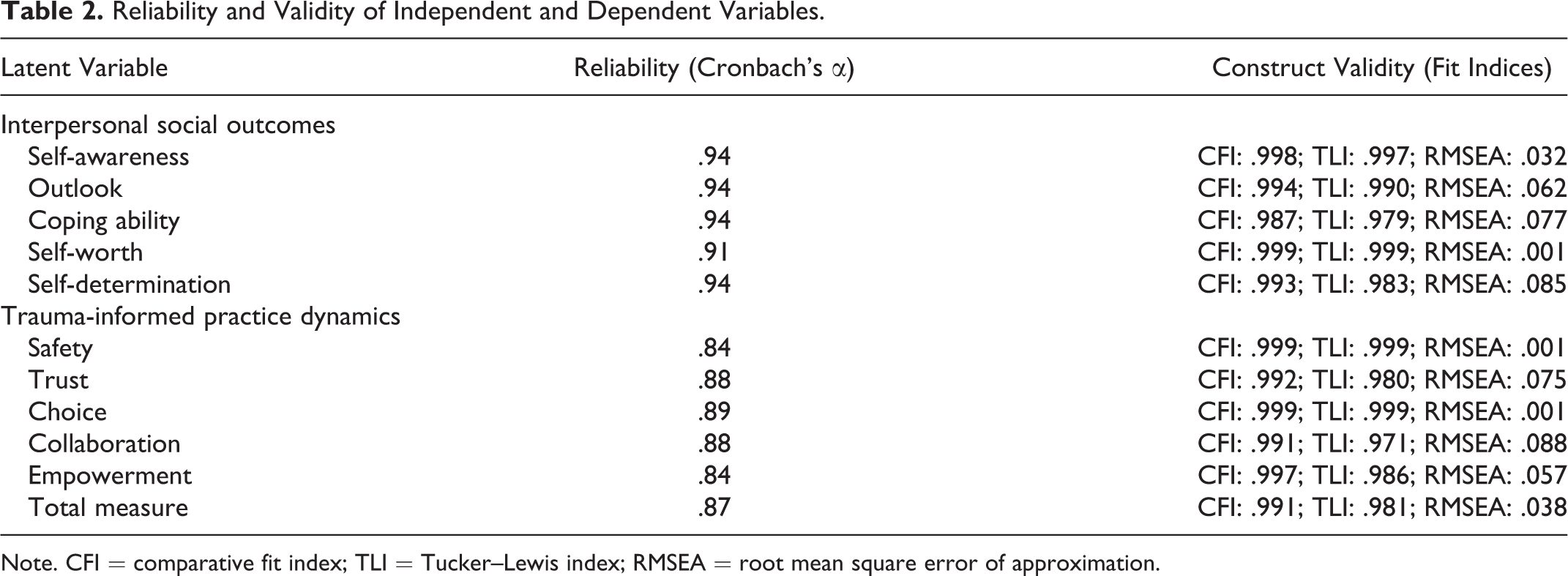
Note. CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation.
Trauma-informed organizational environment
The Trauma-Informed Organizational Environment Scale was developed and used to assess service user experiences with organizational dynamics that define a trauma-informed organizational environment within the human services. These factors included experiences of safety, trust, choice, collaboration, and empowerment. Each was measured on a 6-point Likert-type scale with multiple items as shown in Table 3, with response categories ranging from strongly disagree to strongly agree. This scale was developed from a previous qualitative study (Shier & Turpin, 2017) using a different sample from the partner organization and applies the conceptual work on trauma-informed practice from Harris and Fallot (2001) previously outlined in the literature review section. To assess the construct validity of each of the subfactors as well as the total measure of a trauma-informed organizational environment, a CFA was completed for each latent construct and with each latent construct as a component of a higher order factor. Fit indices from this analysis, as shown in Table 2, indicated strong construct validity for every individual factor, as well as the higher order factor, labeled as a trauma-informed organizational environment. Cronbach’s α measure of internal consistency ranged between .84 and .89 for each of the factors, with the total measure at .87, indicating moderate to strong reliability.
Items on the Trauma-Informed Organizational Environment Scale.
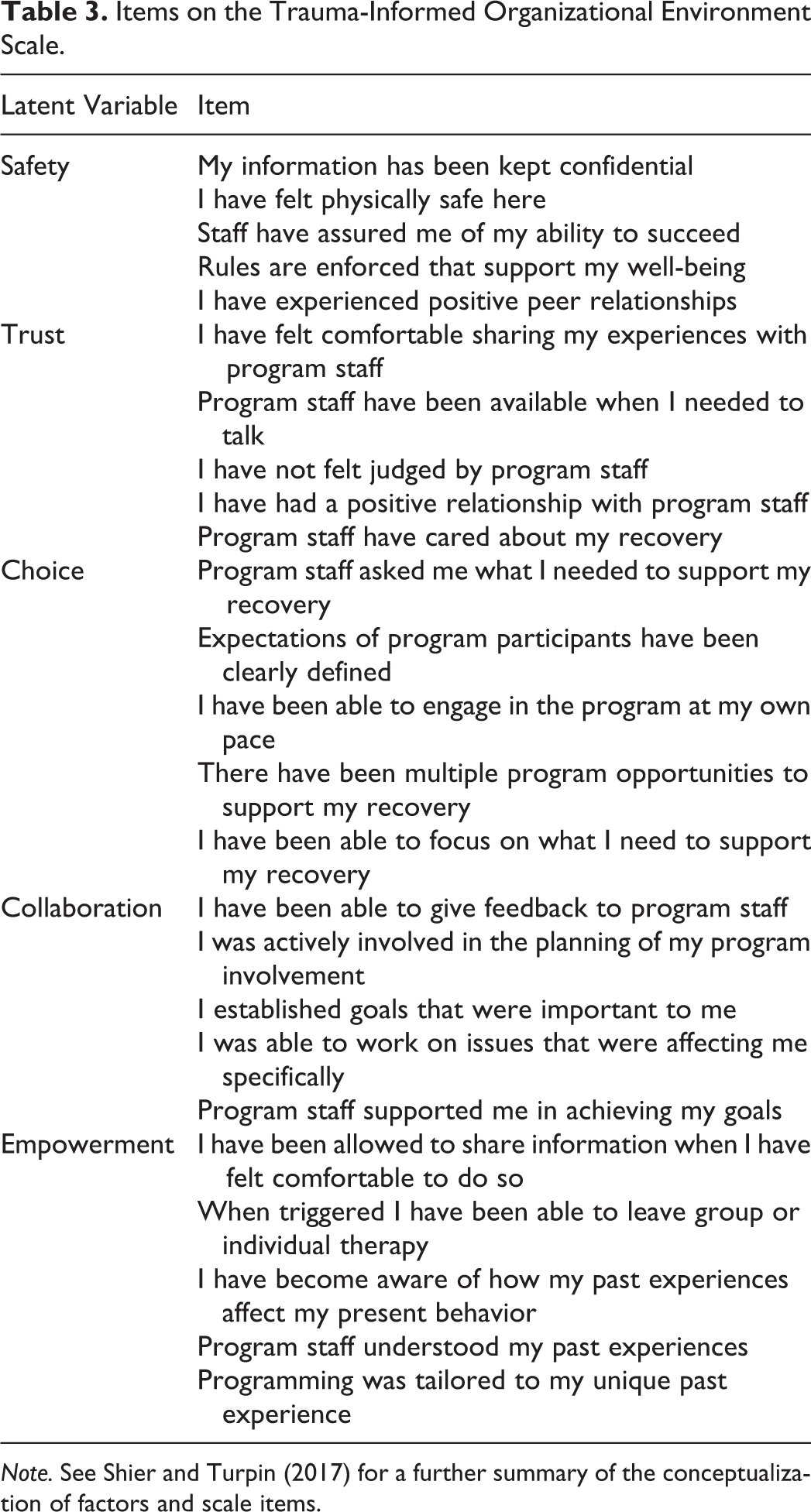
Note. See Shier and Turpin (2017) for a further summary of the conceptualization of factors and scale items.
Analysis
Data were analyzed with the aid of the MPlus statistical software program using maximum likelihood estimation techniques. Initially, each variable reported in the measures section was tested for reliability and construct validity (using CFA techniques with latent constructs). Following this, two multivariate analyses were performed to assess the effect of each independent variable on each of the dependent (i.e., client outcome) variables. This analytical technique was utilized because the unexplained variance among the outcome variables is likely common given their relative interdependence. The models allow for the isolation of the unique direct effect of each independent variable on the multiple dependent variables. A total score difference of the GAINs-SS from Time 1 and 2 is used in the final multivariate analysis to test for significant differences in participant demographic and trauma-informed organizational experiences on this behavioral outcome.
Results
Demographic Statistics
Demographic statistics of the study sample are shown in Table 4. These variables were included in the analysis as potentially confounding variables predicting improvement in outcomes for research participants. Nearly three quarters (n = 121) of the sample identified as male, with the remaining 25.31% (n = 41) female. This is attributable to the gender-specific nature of the programs where the sample was drawn, as two of the three sites were male-only. Further, the vast majority of respondents identified as single (n = 125; 78.62%), did not have a chronic health condition (n = 107; 66.05%), and were unemployed (n = 131; 82.39%). Mean age was 40.42 (ranging from 20 to 65 years) with a standard deviation (SD) of 11.56, showing high variability in this category. For nondichotomous variables, the sample was well distributed throughout. 36.02% (n = 58) of the sample had a high school education, compared to 34.16% (n = 55) with a postsecondary degree and 29.81% (n = 48) with less than a high school degree. Further, 42.77% (n = 68) were living in their own home at the time of completing the questionnaire, while 36.48% (n = 58) were homeless and the remaining 20.75% (n = 33) were living with friends or family. Finally, the majority of respondents (n = 130; 82.74%) had attended at least one treatment program in the past, with 26.09% (n = 42) attending one, 12.42% (n = 20) attending two, 17.39% (n = 28) attending three, and 24.84% (n = 40) attending more than three, compared to 19.25% (n = 31) who were attending a treatment program for the first time.
Demographic Statistics of the Study Sample for Which Data Were Available.
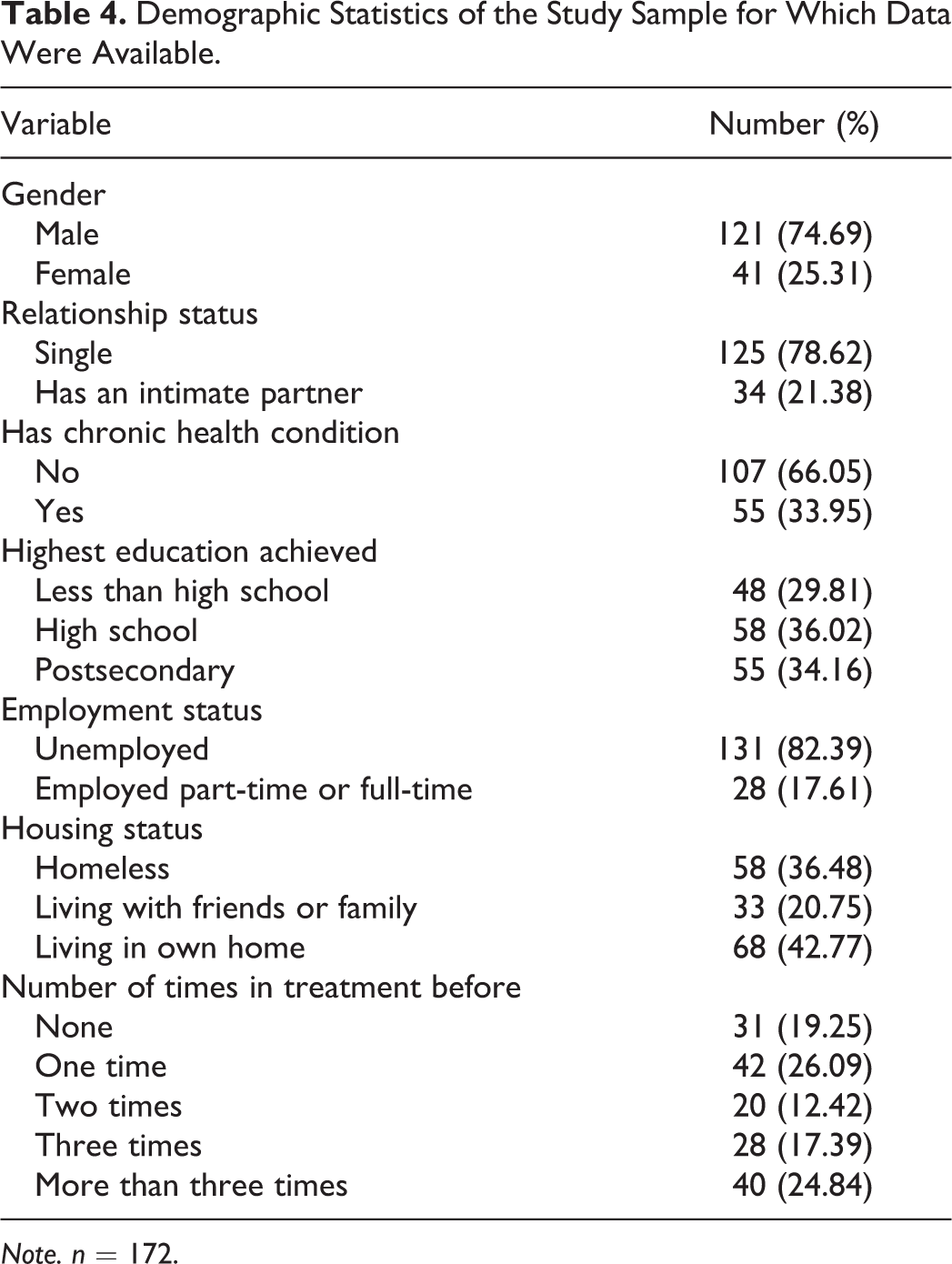
Note. n = 172.
Descriptive Statistics
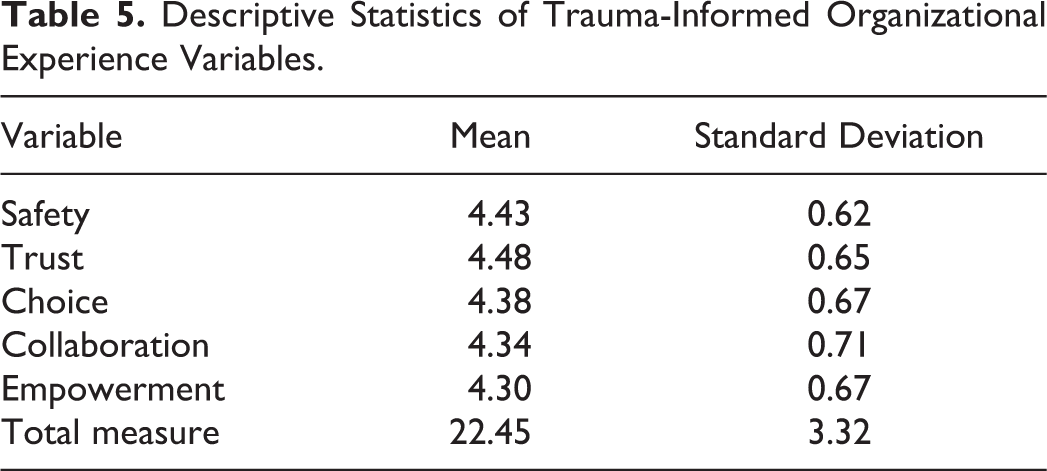
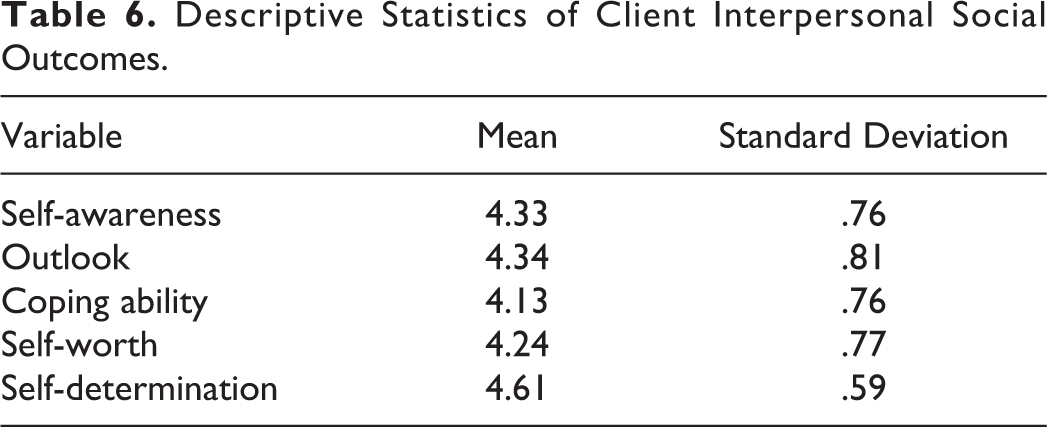
Descriptive statistics for the independent (i.e., trauma-informed organizational experiences) and dependent (i.e., client intrapersonal and behavioral outcomes) variables are shown in Tables 5–7. Mean scores for each factor in the Trauma-Informed Organizational Environment Scale shown in Table 5 were high and ranged from 4.30 to 4.48 (response range = 0–5), with a total scale score mean score of 22.45 (SD = 3.32; response range = 0–25). Similarly, mean scores for the five intrapersonal social outcome latent variables shown in Table 6 ranged from 4.13 to 4.61 (response range = 0–5), while SDs remained low (0.59–0.81). In Table 7, descriptive statistics of factors on the GAIN-SS at Time 1 and Time 2 are presented. At Time 1, respondents scored high on the internalizing disorder (M = 4.01, SD = 1.09) and substance use disorder (M = 4.48, SD = 1.18) screeners, while scoring moderately (M = 3.09, SD = 1.47) on the externalizing disorder screener, and low (M = 1.49, SD = 1.50) on the crime/violence disorder screener (response range = 0–5). The total mean score for Time 1 concurrent disorder screener was 13.16 (SD = 3.77; response range = 0–20). Mean scores at Time 2 for each factor of the GAINs-SS subfactors were lower than Time 1. Internalizing disorder (M = 3.84, SD = 1.15) and substance use disorder (M = 4.12, SD = 1.62) screeners remained highest, followed by the externalizing disorder (M = 2.98, SD = 1.39) and crime/violence disorder (M = 1.36, SD = 1.51) screeners (response range = 0–5). The total mean score for the concurrent disorder screener at Time 2 was 12.38 (SD = 4.30; response range = 0–20). Results from a paired sample t test showed significant improvement from intake to program completion for the total score, t(139) = 1.8967, p < .05; Cohen’s d = −0.171, 95% CI [−0.406, 0.065]. It is important to note the intention of this study is not to assess the extent of improvement from intake to program completion but to assess the effects of a trauma-informed organizational environment on the variability of improvement.
Descriptive Statistics of Trauma-Informed Organizational Experience Variables.
Descriptive Statistics of Client Interpersonal Social Outcomes.
Descriptive Statistics of Factors on the GAIN-SS at Program Start (Time 1) and End (Time 2) for the Past 12 Months.
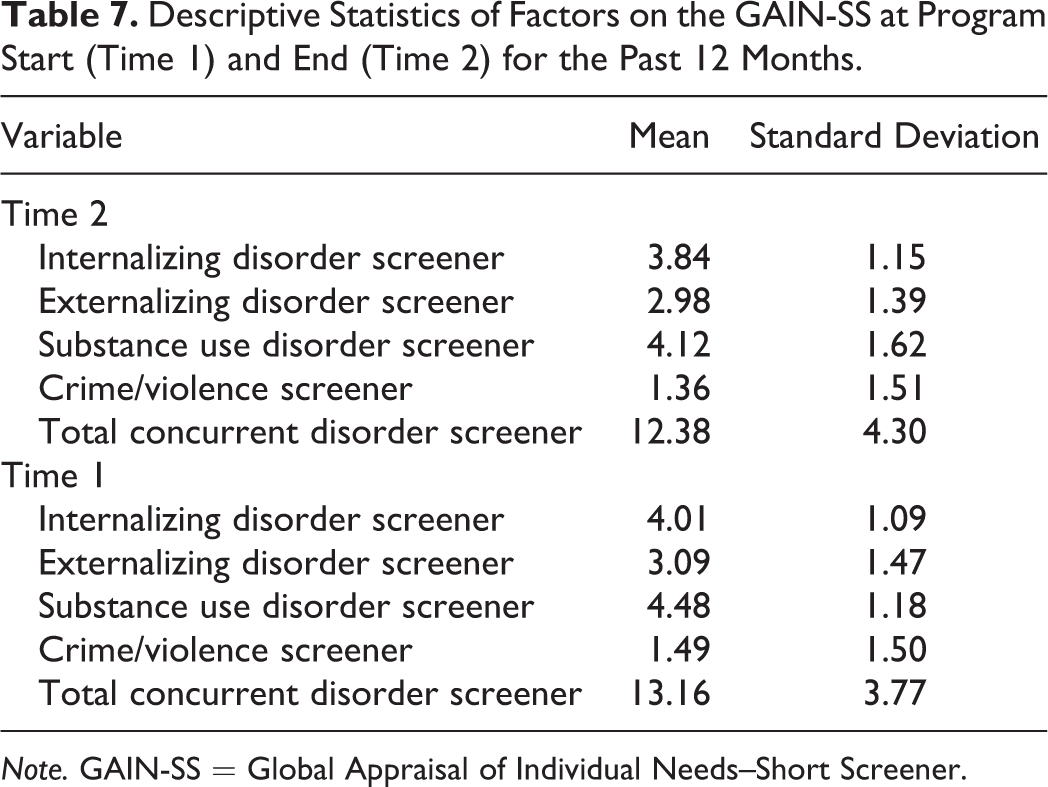
Note. GAIN-SS = Global Appraisal of Individual Needs–Short Screener.
Multivariate Analyses
One multivariate analysis was conducted to test the effect of each trauma-informed organizational environment factor, along with various participant demographic variables (including as potential confounding variables) on each intrapersonal social outcome and improvement on the GAINs-SS. A second multivariate analysis was undertaken to assess the effects of the higher order factor/latent construct (i.e., trauma-informed organizational environment) on each of the intrapersonal social outcomes and the total improvement in concurrent disorder behaviors in treatment. Results are shown in Table 8.
Results From Multivariate Analysis of Trauma-Informed Organizational Experiences on Client Intrapersonal Outcomes and Improvement on the GAINs-SS Total Disorder Screener.
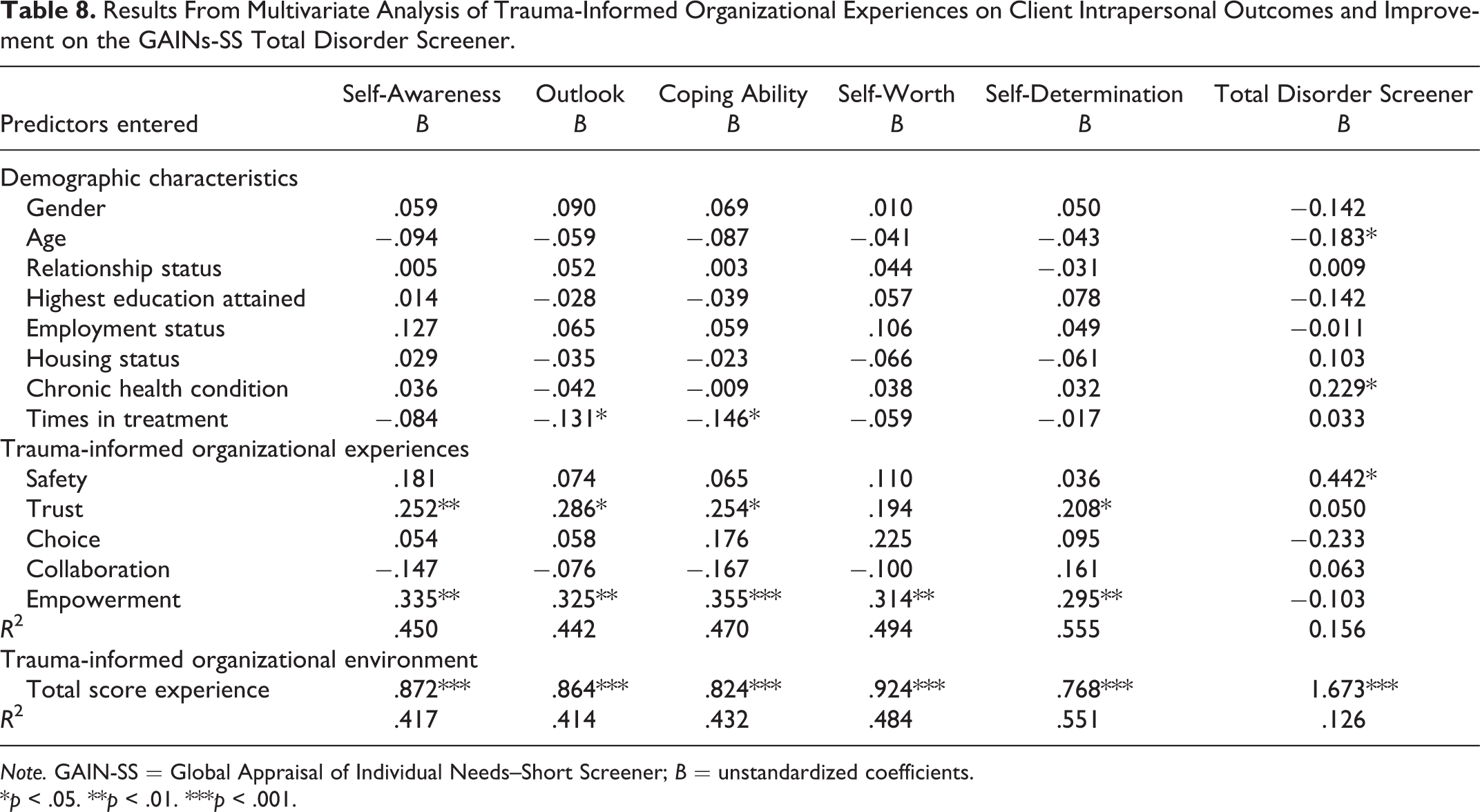
Note. GAIN-SS = Global Appraisal of Individual Needs–Short Screener; B = unstandardized coefficients.
*p < .05. **p < .01. ***p < .001.
The results support Hypothesis 1 (i.e., trauma-informed organizational experiences related to safety will positively predict service user social and behavioral outcomes in treatment), Hypothesis 2 (i.e., trauma-informed organizational experiences related to trust will positively predict service user social and behavioral outcomes in treatment), Hypothesis 5 (i.e., trauma-informed organizational experiences related to empowerment will be positively associated with service user social and behavioral outcomes in treatment), and Hypothesis 6 (i.e., a trauma-informed organizational environment will be positively associated with service user social and behavioral outcomes in treatment).
Empowerment was found to significantly positively predict all intrapersonal social outcome variables at p < .01 level, while trust also significantly positively predicted all intrapersonal outcome variables with the exception of self-worth, and these relationships were slightly weaker at p < .05 level. The latent construct of safety was the only factor to share a significant relationship with improvement on symptomology of concurrent disorder behaviors assessed by the GAINs-SS total score at p < .05 level. Finally, the results show that each of the social and behavioral outcomes is positively predicted by increased overall experiences with a trauma-informed organizational environment in treatment.
Discussion and Applications to Practice
This study utilized a quantitative methodology to explore the effects of trauma-informed organizational experiences on the intrapersonal development social outcomes and concurrent disorder behaviors of service users in treatment for substance use. Five salient aspects of a trauma-informed organizational environment (i.e., safety, trust, choice, collaboration, and empowerment) were measured and tested as predictors of service user self-awareness, outlook, coping ability, self-worth, self-determination, and concurrent disorder behaviors. Various demographic variables were also included in the model as potentially confounding factors supported by previous research.
The study sample included service users participating in a concurrent disorder treatment program across three sites that were overseen by a large human service nonprofit organization. Demographic findings characterize this sample as fairly typical when compared to similar groups. For example, one third of the sample identified as having a chronic health condition, which is common given similar rates of comorbidity found in related studies (Ford & Håkansson, 2020; Hensel et al., 2018). Further, this sample was characterized by high unemployment, moderate-to-high levels of homelessness, and low education. These attributes are also commonly found in samples of service users in concurrent disorder treatment (John et al., 2018; Krausz et al., 2016; Lugoboni et al., 2017). Of note, 82.74% of service users identified multiple experiences with treatment in the past (at least one time previously), supporting the recurring nature of treatment in the lives of individuals with substance use and mental health symptomology (Durazzo & Meyerhoff, 2017; Flanagan et al., 2016).
Some demographic factors were found to predict specific treatment experiences of service users. Interestingly, age shared a significant negative relationship with concurrent disorder behaviors. It could be that older service users have had more time to learn and employ healthy substance use management techniques and therefore are less likely to rate their symptomology as severe. However, recent research (John et al., 2018) has offered conflicting findings, and further scientific examination is required to ascertain any empirical relationship between age and concurrent disorder symptomology. Having a chronic health condition also significantly positively predicted improvements in concurrent disorder behaviors in treatment, which reflects the high instances of chronic health conditions in the sample and supports related research on risk factors associated with this demographic (Han et al., 2018; Walker & Druss, 2017). One final demographic variable—number of times in treatment—shared a significant negative relationship with service user outlook and coping ability. In other words, service users with more previous experiences in treatment were less likely to have a generally positive outlook while lacking effective coping strategies to manage a concurrent disorder, compared to those who had less. Treatment programs should focus on this group as potentially requiring additional support in developing skills that contribute to positive coping mechanisms and an overall positive perception of living with a concurrent disorder.
The primary contribution of this study is the development and testing of the measurement and predictive model of a trauma-informed organizational environment. Organizational development is an important meso-level intervention tool to aid in the improvement of service user outcomes. Mean scores show that service users at this organization had high overall trauma-informed organizational experiences, where staff engaged in behaviors that supported the development of safety, trust, choice, collaboration, and empowerment within concurrent disorder treatment programs. Specific interactions between subscales of a trauma-informed organizational environment and the dependent variables show some evidence of the utility of incorporating trauma-informed organizational dynamics within concurrent disorder treatment settings. For example, the trauma-informed organizational environment subscale Trust was found to significantly positively predict all service user intrapersonal social outcomes, with the exception of self-worth. Forming trusting bonds with program staff is broadly understood as a fundamental aspect of trauma-informed work and a prerequisite for therapeutic interactions in treatment (Stuen et al., 2015; Turpin & Shier, 2018). High trust in organizational staff has been found to lead to conditions that support work on the self through programming that targets intrapersonal development in service users (Treloar et al., 2016; Turpin & Shier, 2018). It may be that self-worth is not a significant part of this process and can be developed by engaging in other activities such as employment and volunteering (Prangley et al., 2018) or physical activity (Muller et al., 2016).
Another subscale, Empowerment, was found to significantly positively predict all client intrapersonal outcomes. This finding underscores the salience of empowerment in the process of developing a strong sense of self for service users in concurrent disorder treatment. The model outlines how the use of empowering techniques, such as strengths-based approaches (Goodhew et al., 2019; Larsen & Sagvaag, 2018) can lead to intrapersonal development in service users. Empowerment has been found to lead to intrapersonal development by contributing to service users’ personal identity and social support (Barringer et al., 2017) while developing a strong belief system (Powell & Peterson, 2014). Some research has suggested that programs can support processes of empowerment by engaging in activities such as providing opportunities for service user feedback (Larsen & Sagvaag, 2018) and incorporating community-based resources and community participation (Barringer et al., 2017; Powell & Peterson, 2014).
Other aspects of trauma-informed organizational and practice experiences, including safety, choice, and collaboration, are important parts of developing service user intrapersonal outcomes but were not found to be as powerful in predicting related outcomes in this study. In this study, choice and collaboration are characterized as comprising external aspects of treatment that may lead to feelings of security and welfare for service users. As such, these aspects of the organizational environment can be understood as prerequisites to service user intrapersonal development, but not an intrinsic part of it. Further quantitative research investigating these factors as possible predictors of interpersonal outcomes would complement this study by providing a more fulsome understanding of the different pathways in which trauma-informed organizational experiences can influence concurrent disorder treatment.
Finally, one subscale of trauma-informed organizational and practice experiences—Safety—was found to positively predict a decrease in concurrent disorder behaviors during treatment. Curiously, safety did not predict any service user’s intrapersonal social outcomes. This finding puts impetus on the treatment environment as having a greater influence on concurrent disorder symptomology, including aspects that ensure service users feel prepared and ready to engage in treatment. When service users feel safe in treatment, they can direct all of their psychological attention to program activities (Kusmaul et al., 2019) and are not preoccupied with factors that may be perceived as dangerous or harmful. While this study did not find that safety contributed to any intrapersonal social outcomes, it does highlight a direct link between a treatment environment that promotes service user safety and a reduction in substance use disorder. This supports the theory that individuals with concurrent disorders misuse substances to better cope with unwanted feelings of insecurity, anxiety, and/or vulnerability (L. Wilson et al., 2018) and that removing environmental threats that lead to these feelings by developing a safe treatment space can help reduce maladaptive behaviors (such as substance use) that are associated with these threats (Flanagan et al., 2016; Norman et al., 2019). Correspondingly, treatment programs should support the long-term well-being of service users by addressing unwanted feelings associated with mental health symptomology and practice coping strategies that support more adaptive behaviors in service users. Related strategies will provide service users with healthier responses to environmental triggers outside of the treatment environment.
Finally, some comments on the implementation of the model proposed in this study as a whole are warranted and in particular the support for Hypothesis six with these study results. Findings from this model provide a more fulsome conceptualization of the effects of trauma-informed organizational environments as a whole on service user intrapersonal social outcomes and substance use disorder symptomology. These findings can be used to inform a framework of trauma-informed organizational development which is also supported on an organizational level, for example, through program development by making decisions that support and enhance levels of safety, trust, choice, collaboration, and empowerment. This model can also be used to assess trauma-informed organizational experiences within concurrent disorder treatment programs by asking service users about specific aspects of programs that may lead to intrapersonal development and reduce concurrent disorder symptomology. This information can then be used to adjust how a concurrent disorder treatment program is provided to ensure that service users’ previous trauma is accounted for and related symptomology is reduced, thereby maximizing treatment effectiveness through organizational development, and in particular those areas that increase experiences related to safety, trust, choice, collaboration, and empowerment that reflected in the Trauma-Informed Organizational Environment Scale.
A few limitations of this study are also worth noting. Regarding the sample, participants in this study were recruited from three sites that were overseen by a single large community-based nonprofit organization. Although the sample was diverse, the context within which services were delivered may be limited. Organizations operating in different contexts (e.g., for-profit treatment centers) should be cautious in applying findings while accounting for unique aspects of organizational structure and programming that may contribute to differences in how service users experience treatment. Another sample-related limitation is the overrepresentation of males, who outnumbered females by a ratio of three-to-one. This gender imbalance was due to the gender-specific nature of programming provided to respondents in this study, as two of the three sites where sampling occurred were male-only. Researchers and practitioners should be aware that findings from this study may be more applicable to male service user populations and may choose to also consult similar research utilizing female and/or nonbinary majority samples to account for missing information as a result of this limitation. A final note about the study sample is the sample size, which may be interpreted as being on the lower end, potentially limiting the analytical and predictive power of the statistical tests performed in this study (i.e., increasing the potential of type two statistical errors). There were no issues in running the models, and the fit indices for assessing construct validity are adequate with smaller sample sizes (Kline, 2011). However, program size and attrition in substance use treatment limited researchers from collecting large amounts of data between Time 1 and Time 2. Future research may seek larger programs and samples to correct this limitation. Finally, though one variable (concurrent disorder behaviors) was measured using pre- and postprogram data points, all other variables were cross-sectional (i.e., collected at program completion). This may affect the generalizability of the study as it fails to provide data on long-term program outcomes using follow-up measures. Future research can build on these findings by implementing longitudinal designs where service users are followed into the community at specified time intervals (e.g., a 3- and 6-month follow-up) to determine whether outcomes are lasting beyond the treatment period. However, based on the intention of this study, which was to develop and assess a measurable model of a trauma-informed organizational environment, this study achieved that end by providing an initial, empirically tested, framework that can assess the organizational context for these trauma-informed elements, as experienced by service users, and support organizational development and innovation in ways that can become more trauma-informed.
A potential further limitation of this study is not controlling for the duration of program involvement among participants as a potential confounding factor. It could be possible that individuals who were involved for more time might have had better outcomes; however, the program itself was very structured—in terms of group practice, individual counseling, and onsite residential support, including assessment (or readiness) for discharge—that it was perceived that respondents would generally demonstrate similar types of outcomes at discharge (no matter what length of time they participated). Furthermore, the study participants completed the program. Further research could investigate the experiences of those individuals that exited their programs prior to completion.
With regard to the holistic nature of this model, we note that the organizational dynamics that were assessed related to trauma-informed organizational environments are relational and programmatic in nature. Within human service organizations, it is generally recognized that organizational dynamics are broad and encompass a number of different dynamic but generally encompass aspects of five key interrelated areas: leadership, organizational culture, management practices, interpersonal dynamics, and programming, each of which encompasses a number of other factors and all together contributing to this idea of a Complex Human Service Organization. While some of these other dynamics (e.g., leadership, organizational culture, or management practices) might also contribute to a trauma-informed organizational environment, service users can only generally comment on interpersonal and programmatic experiences. This might be considered a limitation in the development of a more holistic model based on this study’s focus (i.e., that the focus of this research was exploring these constructs from the perspective of service users), however at the same time, this research provides a step toward understanding that more holistic trauma-informed organizational environment, which could be further supported through research conducted with organization personnel and observational assessment of organizational processes and procedures related to these constructs of safety, trust, choice, collaboration, and empowerment. These are further areas of research to consider in supporting more comprehensive transformation of human service organizations toward being trauma-informed.
The research outlined in this study provides clear evidence of the positive effects of a trauma-informed organizational environment on key service user outcomes in concurrent disorder treatment. While trauma-informed practice and experiences have become widely identified as an important factor leading to improved outcomes, there is limited research that empirically measures such experiences from the perspective of service users, nor tests the effects that these organizational experiences might have on service user outcomes. This study is one of the first to demonstrate this relationship. Furthermore, limited research exists that highlight the intervention role of organizational dynamics on service user outcomes. Most research focuses on the experiences of a specific treatment modality or intervention type. This study provides evidence of the positive effects of service user experiences with broader organizational dynamics (albeit related to trauma-informed organizational dynamics) and treatment-related outcomes, providing evidence that practitioners when assessing treatment-related outcomes should also consider the procedures and interpersonal dynamics of treatment as contributing to service user outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.