
Abstract
Background:
In the context of political demands for social justice, we analyzed determinants of capabilities in community-based clinical social work. Within the scope of an explorative study with two measuring points, people with chronic mental disorders were questioned regarding capabilities as well as psychosocial, sociodemographic, disease-, and care-related aspects in community mental health-care services in Germany.
Results:
Overall, capabilities were rated as medium and did not change significantly over time. A path model showed empowerment and social inclusion to be the strongest determinants on the improvement of capabilities.
Conclusion:
Community-based clinical social work should foster empowerment and social inclusion through socio-therapeutic or, rather, psychosocial interventions in order to alter capabilities among chronically mentally ill people. This could include psycho- or socio-education as well as family interventions that aim to reduce stress in the family or training in life skills such as dealing with money, personal hygiene, or communication competencies.
Keywords
The implementation of freedom of choice demanded by the United Nations Convention on the Rights of Persons with Disabilities (2006) is still “work in progress.” Mentally disabled and chronically mentally ill people benefit from this process because they have been and still remain partially excluded from society and equal treatment (Hofer et al., 2003; Morgan et al., 2007; Richter et al., 2006). A useful and widespread framework to understand the complex interplay of these aspects is the capabilities approach (CA). The CA is especially worked out by Amartya Sen, Nobel laureate in Economics in 1988, and Martha Nussbaum, an American philosopher, to rethink social justice in terms of capabilities. Sen (2009) is concerned about the problems of the dominant contemporary theories about social justice, especially Rawls theory of justice understood as fairness. He argues that an approach to measure injustice in the way that shows how people actually can live a life that they have reasons to value is needed. Nussbaum (2006, 2011) developed an approach that delivers more “practical” hints to increase social justice and support a life that guarantees people’s dignity, especially for state-funded social services. For this purpose, she argues for a definite list of central capabilities that people need for living a good life. Capabilities can be defined as “substantive freedoms” (Sen, 2009) in the sense of subjective choices that allow people to live in the way they wish (Nussbaum, 2011). Capabilities are generally understood to represent the “real opportunity” to achieve those things in life that a person “has reason to value” (Sen, 2009). Nussbaum (2011) argues that these capabilities should be governmentally guaranteed and should include, for example, aspects of bodily health, integrity, and freedom from discrimination as well as the ability to value people and nature and to exercise political influence. Following Nussbaum, capabilities can be divided into internal and combined capabilities. The latter are the product of internal capabilities that could be developed or used in a supportive surrounding with sufficient resources and opportunities. In some aspects, the CA is in line with the International Classification of Functioning, Disability and Health (World Health Organization, 2001) that defines disability as a result of individual and societal factors affecting participation. Saleeby (2007) argues that the CA supports this idea of a bifocal understanding of disability by regarding capabilities as necessary to overcome social problems resulting from individual impairments such as mental illness and the related societal reaction.
Since social work is dedicated to social change (Doostgharin, 2010; Kam, 2014) and human development in terms of equal rights and opportunities (Chu et al., 2009; International Federation of Social Workers, 2014), it is an important and significant starting point to foster people’s capabilities (Anand, 2005; International Social Work, 2014). As an interdisciplinary approach, clinical social work can provide beneficial circumstances for such a process since it addresses psychological as well as social factors that cause or exacerbate mental disorders and helps clients to gain, to stay in, or to return to a suitable societal position (Bebbington, 2010). Through interventions such as social therapy, counseling, group work, crisis intervention, and low-threshold opportunity meeting points for chronically mentally ill people (Perkins & Burns, 2001), clinical social work fosters the enhancement of individual competencies, the extension of social networks, and the development of satisfying relationships. Thereby, it enhances clients’ opportunities to choose what they wish to do or who they wish to be (International Social Work, 2014; Leff, 2010). However, individual support depends on a surrounding that provides social support by nonprofessionals such as neighbors or colleagues. Therefore, a clinical perspective has to be extended by a community-based approach. In Germany, the assistance of people with severe mental disabilities (ambulant integration assistance) has been refined in the last decades. These state-funded care services support mentally as well as physically handicapped people in taking advantage of their resources and in balancing out handicap-related disadvantages in order to allow for a mostly self-determined life (Berlin Senate for Integration, Work, & Social Affairs, 2019). The services follow the needs of the clients and, for example, can cover supporting activities regarding work, housing, daily structure, social relationships, sportive, or cultural events. Social services and the governments seek for the best way to prevent exclusion and help clients to be a recognized part of networks.
So far, there is little empirical data on how capabilities are created (Heckman & Corbin, 2016) and how community-based clinical social work could enhance capabilities (Albers, 2015; Baumgartner, 2016; James, 2016; Muffels & Headey, 2013). Determinants of capabilities theoretically drawn from a general “top-down” perspective in terms of political frameworks to provide social justice for citizens are rarely precisely defined (Nussbaum, 2011; Pockett & Beddoe, 2017; Volkert, 2014). Robeyns (2005), for example, mentions “personal, social, and environmental factors” as determinants of capabilities; a more precise definition of these broad aspects is not given. Volkert (2014) discusses individual potential and well-being as determinants of capabilities, but what lies behind these concepts and how they could be fostered is not further explored. In this broad sense, psychosocial interventions can be considered successful treatment in clinical social work with regard to the enhancement of the individual potential and well-being of people with mental illnesses. This is achieved, for example, by fostering self-efficacy and psychosocial functioning (Heidenreich et al., 2018), reducing severity of symptoms (Linden et al., 2008; Nowack et al., 2011), reducing crisis and hospital admissions (Heidenreich et al., 2018; Linden et al., 2008; Tomasi et al., 2010), or preventing suicide (Petrakis & Joubert, 2013). To our knowledge, a link to the concept or measurement of capabilities, especially regarding effects over time, has not been realized so far. Against this background, we conducted an explorative study among chronically mentally ill people seeking community-based social work regarding status quo, development, and bio-psycho-social determinants of capabilities.
Method
Participants
Within the scope of a multicenter survey with two measuring points, we questioned chronically mentally ill people who seek ambulant integration assistance according to the German Social Code Book XII in community-based social service units. Between t0 and t1, subjects of this study took advantage of the services provided by those units. The survey was conducted in urban and rural areas in northern Germany between June 2015 and January 2017.
In the city of Hamburg, which was used as an example of an urban area, 50 organizations providing ambulant integration assistance existed at the time of recruitment. Due to limited resources, it was not possible for the research team to include all organizations into the survey. Thus, based on an overview of all providing ambulant integration assistance organizations provided by the Hamburg Office for Social Issues, Work, Family, and Integration (2015), 20 of these 50 organizations were randomly chosen. Of these 20 organizations, 17 agreed to participate in the survey. These 17 organizations provided 31 different community mental health-care services located all over the city of Hamburg at the time of recruitment. Taken together, these 31 community mental health-care services had cared for 1,254 clients at that point in time.
In the state of Mecklenburg-Western Pomerania, which was used as an example of a rural area, the overall amount of organizations providing ambulant integration assistance is not officially recorded due to structural differences in the care system. Thus, it was not possible to arrange a random sampling there as well. Therefore, all members of the Social Psychiatry Organization of the State of Mecklenburg-Western Pomerania were written to in order to take part in the survey. We chose this procedure because it was the most reasonable alternative to a random sampling since most of the organizations that provide ambulant integration assistance in Mecklenburg-Western Pomerania are a member in that organization. Twenty-five community mental health-care services providing ambulant integration assistance agreed to participate. Taken together, these services cared for 471 clients at that point in time.
All participating services in Hamburg and Mecklenburg-Western Pomerania were asked to invite every client meeting the following criteria to participate in the survey: (1) sufficient German-language abilities, (2) no cognitive impairments, and (3) written informed consent. Every client participating in the survey was questioned 2 times (t0, t1), with a period of 8 months in between. Study flow, nonresponder, and dropout analysis of both cohorts are displayed in Figure 1. Prior to the beginning of the survey, the study protocol was approved by the ethics committees of the University of Applied Sciences Hamburg and the University of Greifswald.
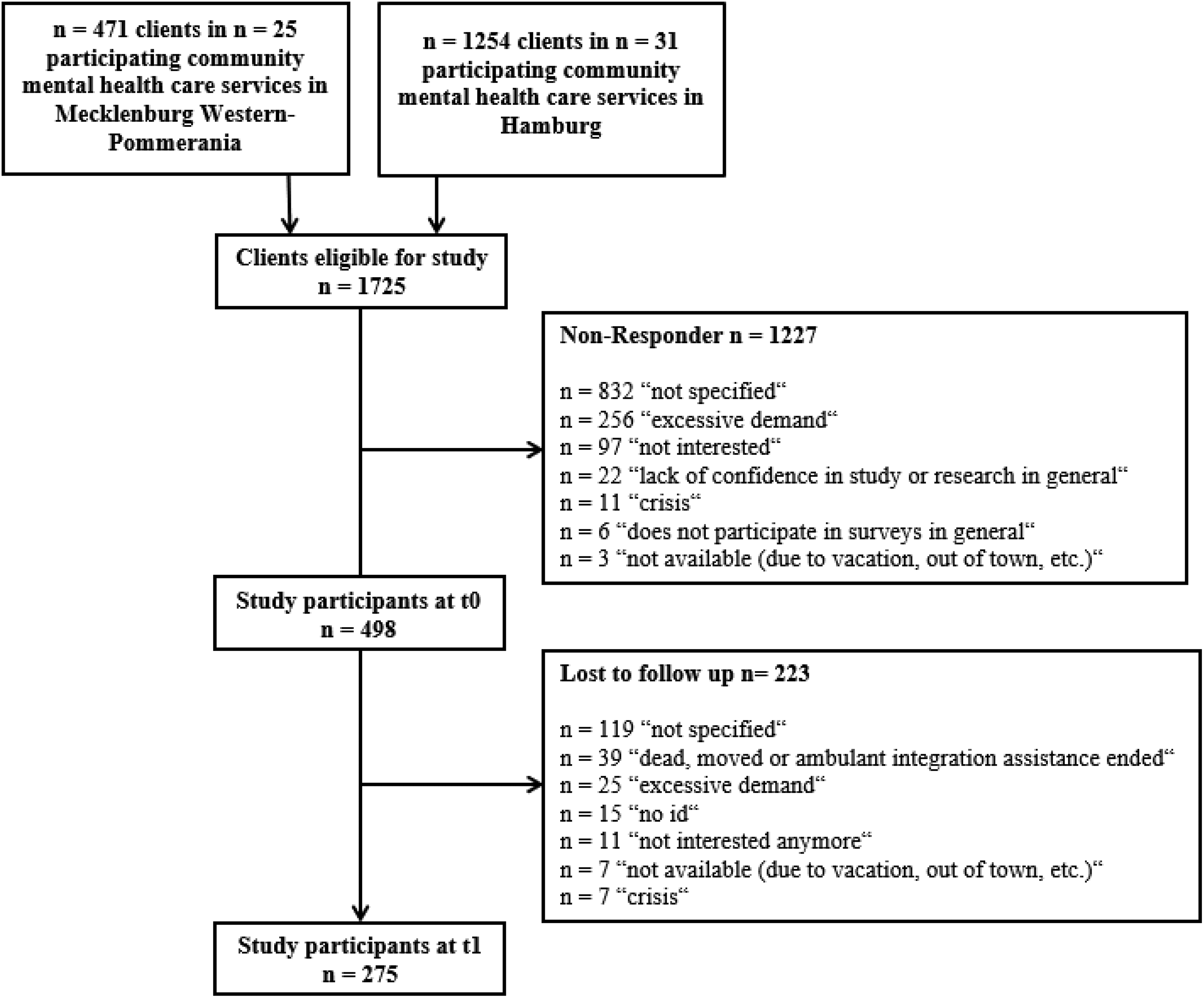
Study flow, nonresponder, and dropout analysis of the overall study cohort.
Assessments and Measures
The study was constructed as a pilot to examine how capabilities and other parameters of severely mentally ill people will develop and how this development could be measured. Because of a lack of objective data about the life situation of these clients and about the effects of clinical social work, we had to rely on self-ratings. Furthermore, in Germany, it is very hard to get access to objective data of severely mentally ill people, for example, from insurances or by federal or regional statistical offices. We found that this study field has been a “black box” in which we were the first ones to set up a study, we hadn’t comparable studies in Germany so far.
Capabilities
We applied the self-reported measure Oxford Capabilities-Mental Health to capture capabilities (Simon et al., 2013) and slightly adapted the German version of this assessment in terms of expression (Baumgardt et al., 2018; Simon et al., 2018). The questionnaire contains 17 items and represents the capability approach as one domain. One item deals with reasons for discrimination, has a multiple-choice format, and is analyzed separately. The unequally directed, five-stage response scale of the other 16 items was adapted into a rectified response format according to the corresponding scoring manual (Simon & Laszewska, 2015). Thus, after data preparation, the answers ranged from 1 (totally disagree or always) to 5 (totally agree or never). High values mark high capabilities such as “Does your health in any way limit your daily activities, compared to most people of your age?” Finally, the data were transferred into the suggested capability index, the CAPINDEX16. At present, no standardized threshold values for this index exist. The internal consistency of the total score was high, with Cronbach’s α = .84.
Empowerment
Since the concept of empowerment implies, inter alia, internal abilities, and a surrounding that doesn’t hinder people to live a self-determined life, it is tightly connected to the CA. Thus, empowerment is theoretically proposed to be a central factor for the enhancement of individual capabilities (Bonvin & Moachon, 2008). We assessed empowerment with the questionnaire Empowerment in the Psychiatric Treatment Process for People with Schizophrenic Disorder (EPAS; Kilian et al., 2014). The EPAS contains 43 items with a five-stage answering format ranging from 1 (totally disagree) to 5 (totally agree). It is divided into seven subscales: coping with everyday life, social relationships, treatment and medication, hope and self-efficacy, self-esteem and acceptance, care for under-aged children, and working life (Kilian et al., 2014). Data were transferred into mean scores of each subscale according to the corresponding scoring manual. High values mark high empowerment, such as “I cope well with new demands.” Internal consistency for the single scales was diverse, ranging from Cronbach’s α = .45 to .87.
Quality of life
Since capabilities are tightly connected with quality of life, a multidimensional concept that includes aspects of physical and psychological as well as social well-being (Eack, 2012), we applied 16 questions from the German version of the Manchester Short Assessment of Quality of Life (Hemmerle et al., 2010; Priebe et al., 1999). These questions cover psychosocial domains of life and the patient’s satisfaction level. Four questions utilize a two-stage response scale from 1 (no) to 2 (yes), and 12 questions are rated on a 7-point scale ranging from 1 (very unsatisfied) to 7 (completely satisfied; Bjorkman & Svensson, 2005; Priebe et al., 1999). The data presented in this article refer to the latter items as recommended by the authors of the questionnaire. High values mark high quality of life such as “How satisfied are you with your health?” The internal consistency was high, with Cronbach’s α = .86.
Social inclusion
Social inclusion was analyzed with one scale of the German measure for participation and social inclusion for use in people with a chronic mental disorder Fragebogens zur Erfassung sozialer Inklusion und Partizipation (F-INK), which is closely connected to the CA as well (Schuetzwohl et al., 2017). This questionnaire contains 13 questions with response values ranging from 1 (not at all) to 4 (very much). High values mark high social inclusion such as “How included into and respected by your neighborhood and your neighbors do you feel?” The internal consistency of the total score is high, with Cronbach’s α = .91.
General self-efficacy
Self-efficacy was assessed with the German version of the General Self-Efficacy Scale (GSE) since the ability to cope with daily hassles as well as to adapt after experiencing all kinds of stressful life events can be considered psychological capital and thus can influence capabilities (Muffels & Headey, 2013; Schwarzer & Jerusalem, 1995). The GSE contains 10 questions to be rated on a four-stage scale ranging from 1 (do not agree) to 4 (totally agree). High values mark high self-efficacy such as “I can always manage to solve difficult problems if I try hard enough.” The internal consistency of the total score was high, with Cronbach’s α = .91.
Global assessment of functioning
We captured psychological, social, and vocational functioning using the third-party-rated Global Assessment of Functioning Scale (GAF) because capabilities are argued to be affected by those aspects over time (Jones et al., 1995; Muffels & Headey, 2013; Piersma & Boes, 1997; Saß et al., 2003). GAF values range from 1 to 100, with a value under 10 referring to “[…] persistent danger of severely hurting self or others (e.g., recurrent violence), persistent inability to maintain minimal personal hygiene, or serious suicidal act with clear expectation of death” and a value of 90 or higher referring to superior functioning in “[…] a wide range of activities, life’s problems never seem to get out of hand, is sought out by others because of his or her many positive qualities or to no symptoms.”
Severity of symptoms
For the same reason, severity of symptoms was assessed with the self-rating measure SCL-K-9, a short version of the Symptom Checklist 90-R for people with mental disorders that assesses a person’s psychological stress during the last 7 days (Klaghofer & Brähler, 2001; Prinz et al., 2013). The questionnaire contains nine questions to be rated on a five-stage scale ranging from 0 (not at all) to 4 (very strong). High values mark strong symptoms within the past week such as “feeling nervous when you are left alone.” The internal consistency was high, with Cronbach’s α = .85.
Sociodemographic, care-, and disease-related characteristics
Sociodemographic characteristics (sex, age, having a child, migration background, living independently, being in a relationship, school-leaving qualification, vocational qualification, currently working) were assessed with a questionnaire adapted from the German Socio-Economic Panel (Wagner et al., 2007). Questions regarding disease-related aspects (severely disabled, kind of psychiatric disorder) were self-developed and adapted to the cohort of interest. Satisfaction of care was assessed with the self-rated measurement of treatment satisfaction Klientenbogen zur Behandlungsbewertung (KLiBB) because satisfaction with care is considered to be crucial in remaining in a certain care setting (Priebe et al., 1995). The questionnaire contains 8 items to be rated on an 11-point scale ranging from 0 (no, not at all) to 10 (yes, totally). High values mark high satisfaction with care such as “In general, do you believe you get the right kind of care?” The internal consistency of the total score was Cronbach’s α = .75. Further care-related characteristics (legal guardian, currently in treatment due to mental difficulties, treatment realized by, treatment within the last 12 months) were self-developed and adapted to the cohort of interest as well.
The overall questionnaire was pretested among the target population (n = 12); results were incorporated into the final version of the overall questionnaire. All assessments were supervised by internal staff of the organizations since studies showed no differences in comparison to external supervision if mental health community service users complete self-reports (Gelkopf et al., 2015). The self-reported questionnaires were available in hardcopy form and online. All internal staff was trained in advance regarding the assessment of the overall questionnaire and the application of the GAF as a third-party-rated instrument in particular. The GAF questionnaire was available in hardcopy form only.
Data analysis
All data analyses were conducted using SPSS Version 22 and SPSS AMOS Version 22. Data of the two study cohorts were pooled. Missing data in one-dimensional scales were imputed with individual means if missing items were ≤20% and excluded case-wise if not (Baltes-Götz, 2013). We used an explorative analysis strategy since no empirical model regarding determinants on capabilities existed at the time of analysis. Continuous variables were excluded from reporting and further analysis if more than 20% of participants did not answer. Dichotomous variables with less than 5% in one group were eliminated as well. All variables were used to obtain a path model. Because of the high number of variables, we applied a stepwise approach to reduce the number of variables in the path model. We evaluated the change to t0 (δ) of capabilities and all constructs that were assessed in both survey waves. In a first step, we calculated correlations between change of capabilities and all sociodemographic as well as care- and disease-related variables, which are displayed in Table 1. In the next step, we conducted a multiple analysis of covariance (ANCOVA) including all significant variables from the first step as independent variables and change of capabilities as the dependent variable. Then, Steps 1 and 2 were repeated with constructs showing a significant correlation with capabilities. With these significant variables, a path model was constructed (original path model). We subsequently excluded nonsignificant paths in a backward selection to obtain our final path model. For descriptive statistics, frequency distribution, mean, and standard deviation were used. For bivariate analysis, paired t tests, analyses of variance, point-biserial correlations, and Pearson product-moment correlations were applied. We used p < .05 (two-sided) as the threshold of statistical significance.
Sociodemographic, Care-, and Disease-Related Characteristics of Overall Study Cohort.
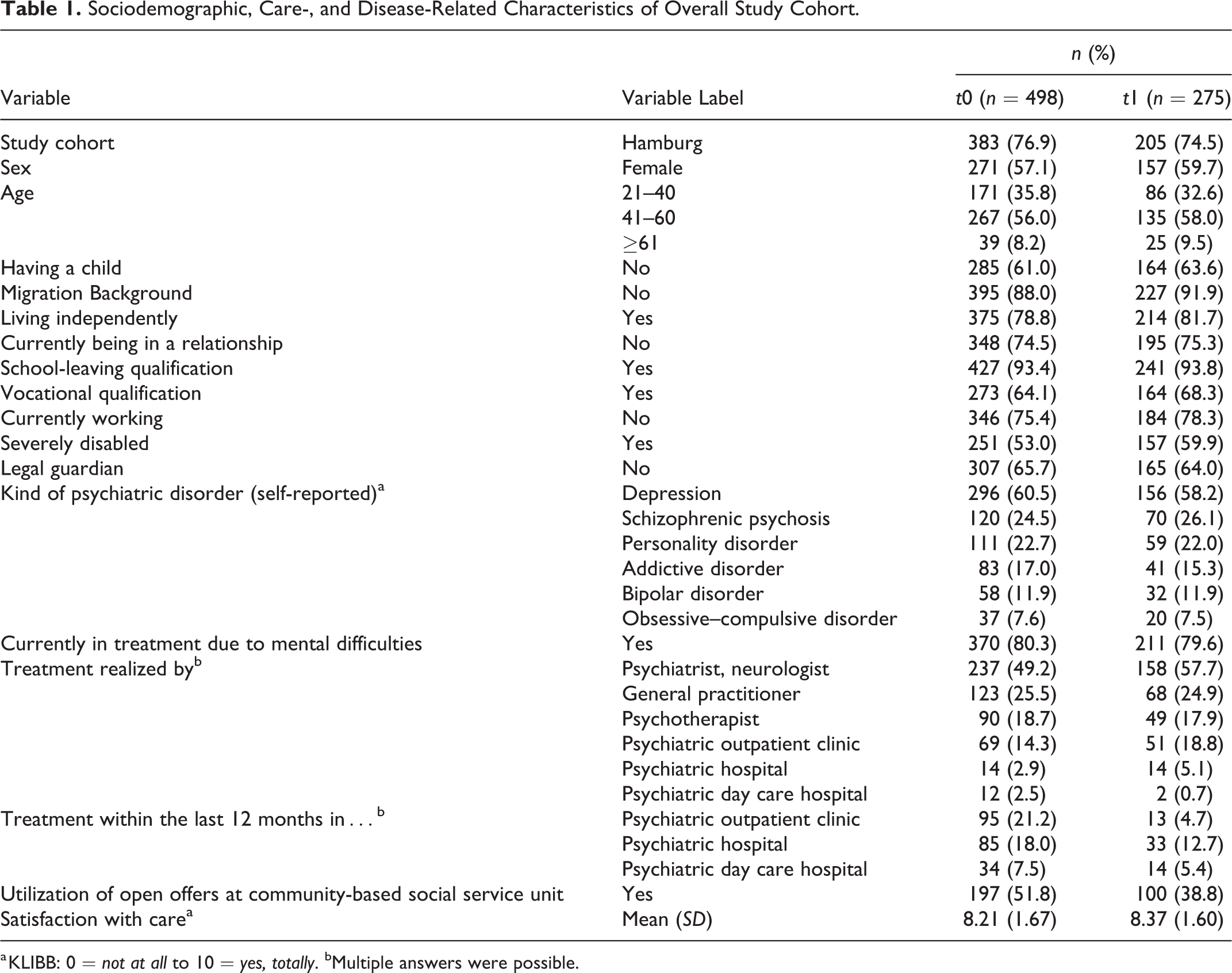
a KLIBB: 0 = not at all to 10 = yes, totally. bMultiple answers were possible.
Results
As displayed in Figure 1, 28.9% (n = 498) of the clients in question responded to our survey at t0; 55.2% (n = 275) of that cohort took part in the second wave as well. The study cohort’s sociodemographic, disease-, and care-related characteristics are shown in Table 1. Dropout analysis showed no differences between t0 and t1 except for three aspects: severely disabled people (χ2 = 5.617, p = .021) and people who had been treated in a psychiatric hospital (χ2 = 3.548, p = .036) tended to remain in the study, whereas people who used open offers at community mental health-care services (χ2 = 10.213, p = .001) tended to drop out of the study.
Mean ratings at t0 and t1, as well as the amount of change of capabilities, social functioning, severity of symptoms, social inclusion, quality of life, self-efficacy, and empowerment, are displayed in Table 2. The outcomes did not change significantly over time except for social inclusion, with only a very small effect size.
Mean Ratings and Change Between Both Points in Time.
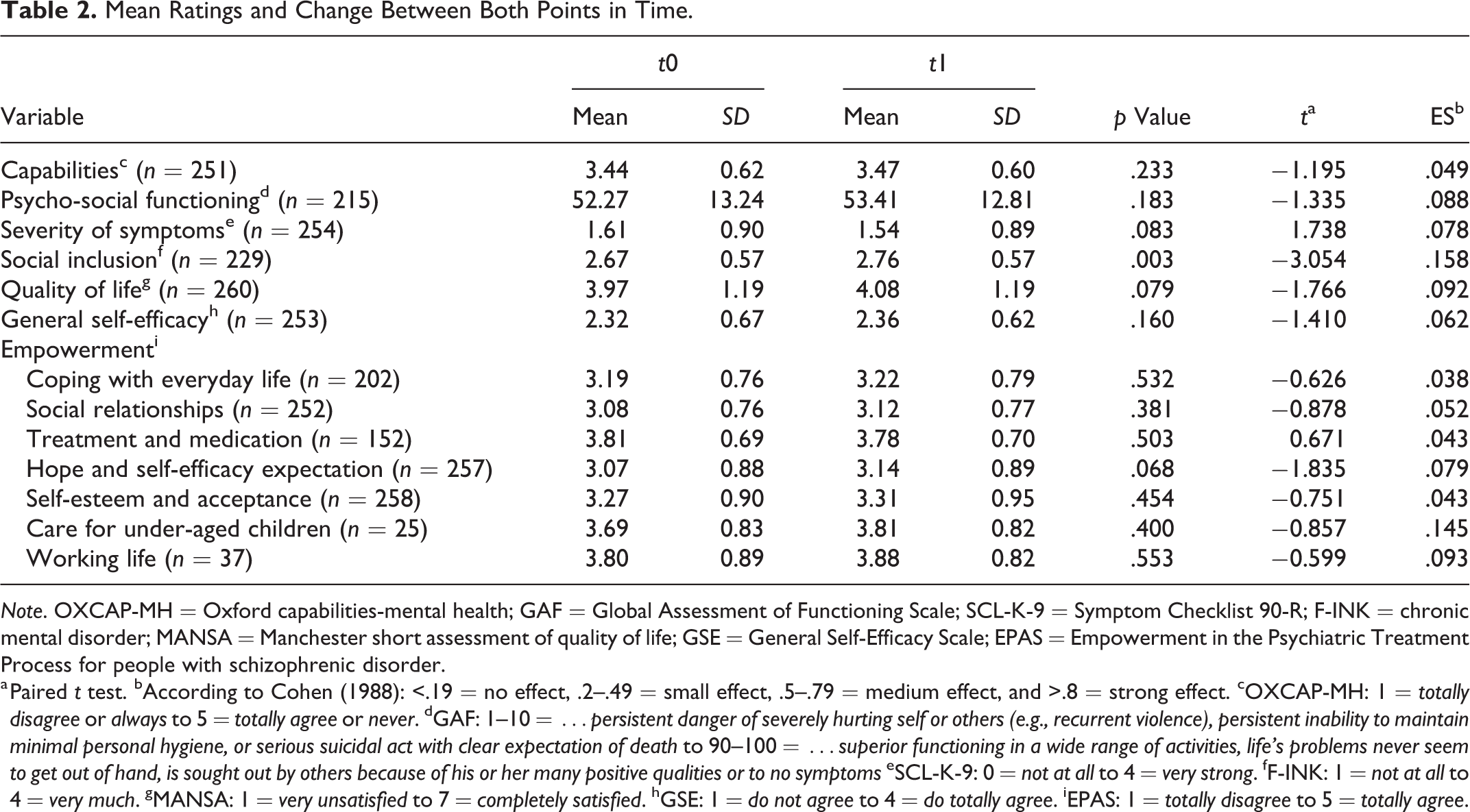
Note. OXCAP-MH = Oxford capabilities-mental health; GAF = Global Assessment of Functioning Scale; SCL-K-9 = Symptom Checklist 90-R; F-INK = chronic mental disorder; MANSA = Manchester short assessment of quality of life; GSE = General Self-Efficacy Scale; EPAS = Empowerment in the Psychiatric Treatment Process for people with schizophrenic disorder.
a Paired t test. bAccording to Cohen (1988): <.19 = no effect, .2–.49 = small effect, .5–.79 = medium effect, and >.8 = strong effect. cOXCAP-MH: 1 = totally disagree or always to 5 = totally agree or never. dGAF: 1–10 = …persistent danger of severely hurting self or others (e.g., recurrent violence), persistent inability to maintain minimal personal hygiene, or serious suicidal act with clear expectation of death to 90–100 = …superior functioning in a wide range of activities, life’s problems never seem to get out of hand, is sought out by others because of his or her many positive qualities or to no symptoms eSCL-K-9: 0 = not at all to 4 = very strong. fF-INK: 1 = not at all to 4 = very much. gMANSA: 1 = very unsatisfied to 7 = completely satisfied. hGSE: 1 = do not agree to 4 = do totally agree. iEPAS: 1 = totally disagree to 5 = totally agree.
An improvement of capabilities was associated with being in a relationship (σ = −2.875, 95% CI [−4.728, −1.021], p = .002), self-reported depression (σ = −2.045, 95% CI [−3.642, −0.447], p = .012), and self-reported bipolar disorder (σ = −3.428, 95% CI [−5.802, −1.055], p = .005) as well as with an improvement of severity of symptoms (r = −.249, p < .001), social inclusion (r = .248, p < .001), quality of life (r = .305, p < .001), self-efficacy (r = .260, p < .001), and empowerment (coping with everyday life: r = .423, p < .001; social relationships: r = .338, p < .001; treatment and medication: r = .281, p < .001; hope and self-efficacy: r = .348, p < .001; self-esteem and acceptance: r = .247, p < .001). The results of the multiple ANCOVA are displayed in Table 3. Improvement of social inclusion, bipolar disorder, and empowerment “coping with everyday life” are determinants of capabilities and are thus explored further in the path model.
Regression Models for Change of Capabilities, Social Inclusion, and Empowerment “Coping With Everyday Life.”
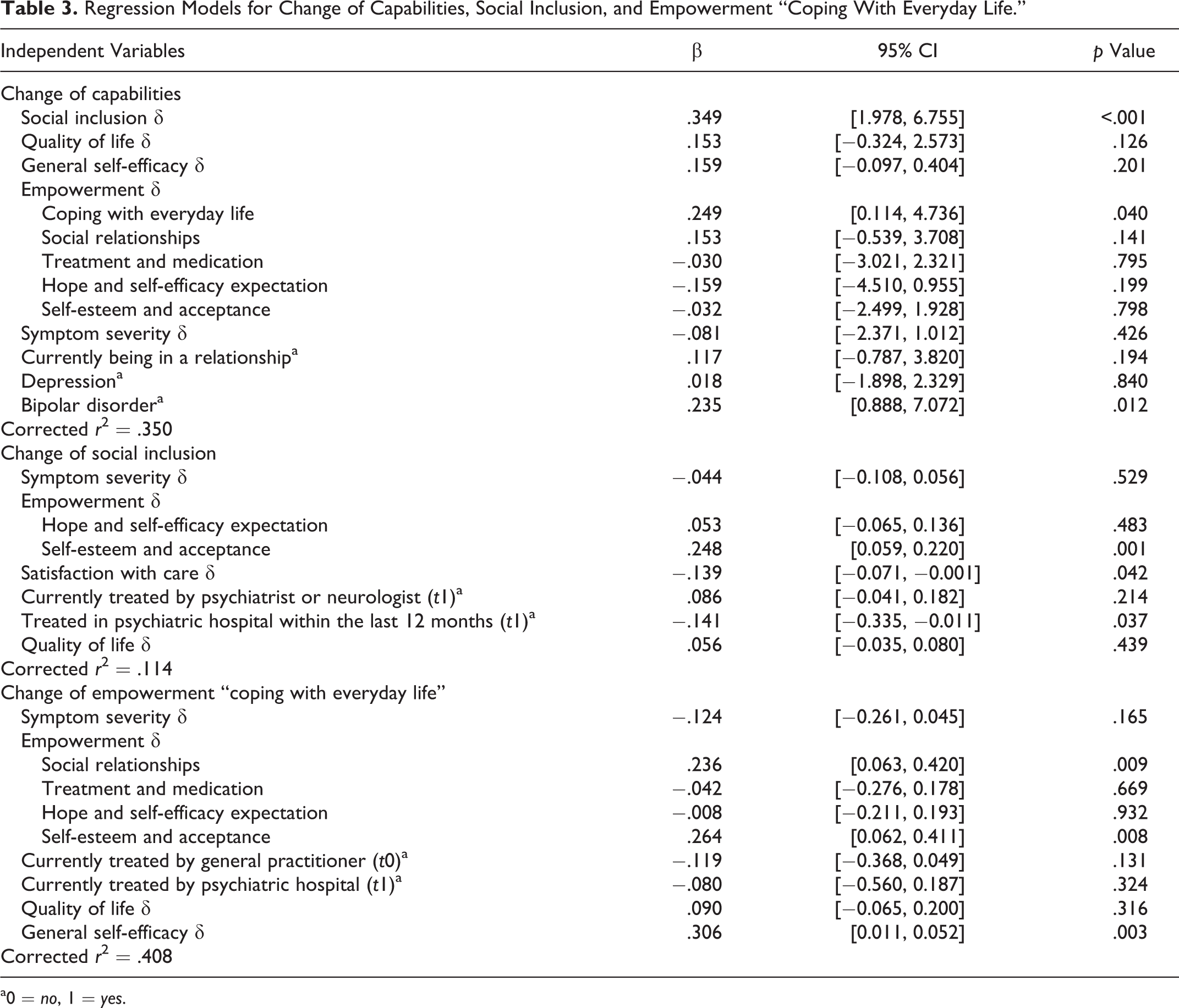
a0 = no, 1 = yes.
Improvement of social inclusion was associated with lower satisfaction with care at t0 (r = −.137, p = .042), being currently treated by a psychiatrist or neurologist at t1 (σ = −0.120, 95% CI [−0.230, −0.010], p = .034), not having been in a psychiatric hospital within the last 12 months at t1 (σ = 0.214, 95% CI [0.045, 0.384], p = .014), and an improvement of severity of symptoms (r = −.152, p = .023), empowerment (hope and self-efficacy: r = .213, p = .001; self-esteem and acceptance: r = .302, p < .001), and quality of life (r = .141, p = .034). Results of the multiple ANCOVA are displayed in Table 3.
Improvement of empowerment “coping with everyday life” was associated with not having been treated by a general practitioner at t0 (σ = 0.191, 95% CI [0.120, 0.370], p = .037), not having been in a psychiatric hospital at t1 (σ = 0.373, 95% CI [0.001, 0.738], p = .045), as well as an improvement of severity of symptoms (r = −.319, p < .001), self-efficacy (r = .510, p < .001), empowerment (social relationships: r = .419, p < .001; treatment and medication: r = .289, p = .002; hope and self-efficacy: r = .421, p < .001; self-esteem and acceptance: r = 4.02, p < .001), and quality of life (r = .240, p = .001). Results of the multiple ANCOVA are displayed in Table 3.
All variables with a significant association in the ANCOVAs with change of capabilities, social inclusion, and empowerment “coping with everyday life” were included in a path model. Global fit indices for estimated models met generally accepted thresholds for good fit (Hair & Anderson, 2010; Kline, 2005) and are displayed in Table 4. The final path model and its statistically significant determinants as standardized estimates are displayed in Figure 2. Statistically significant correlations are omitted for clarity and are displayed in Table 5. The highest standardized total effects on improvement of capabilities originate from an improvement of empowerment (coping with everyday life: βs = .314; social relationships: βs = .142), social inclusion (βs = .182), being in a relationship (βs = .161), and an improvement of quality of life (βs = .148).
Measures of Global Fit for Estimated Models.
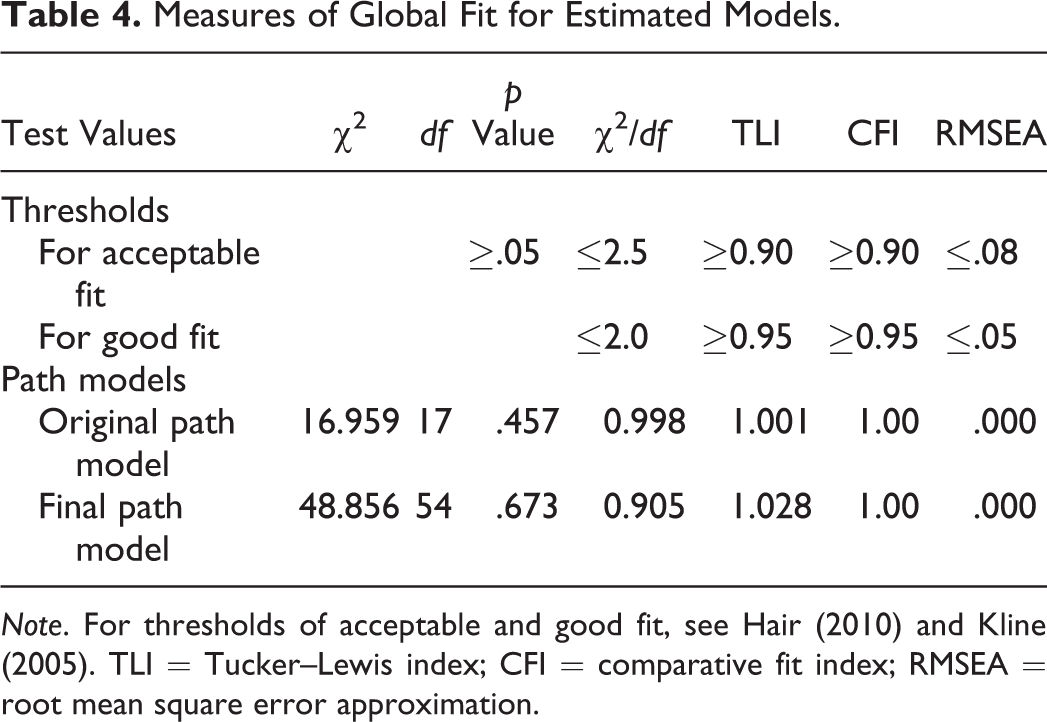
Note. For thresholds of acceptable and good fit, see Hair (2010) and Kline (2005). TLI = Tucker–Lewis index; CFI = comparative fit index; RMSEA = root mean square error approximation.
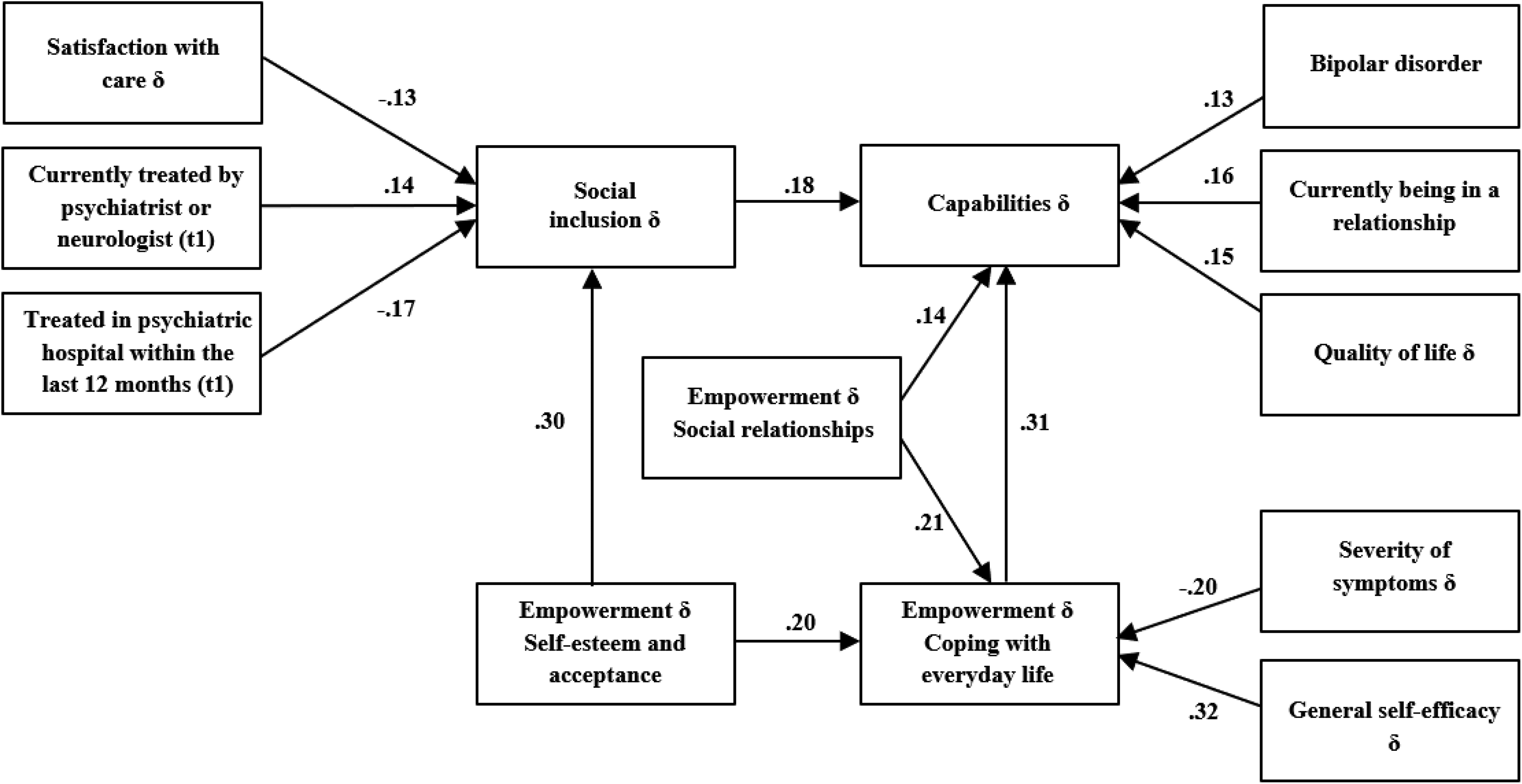
Path model on determinants of change of capabilities (standardized estimators).
Statistically Significant Product-Moment Correlations Between Covariates.
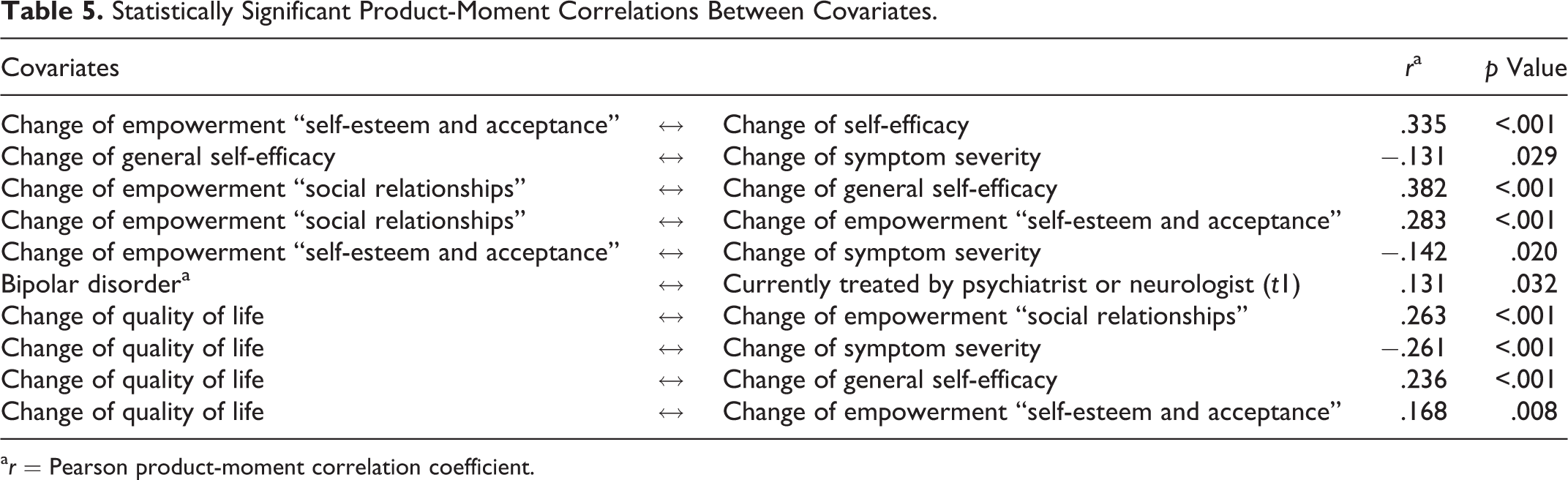
a r = Pearson product-moment correlation coefficient.
Discussion
Sociodemographic characteristics of the Hamburg study cohort are in line with the total population of ambulant integration assistance recipients in that region in terms of gender and migration background (Hamburg Office for Social Issues, Work, Family, and Integration, 2015). For Mecklenburg-Western Pomerania, no such analysis could be conducted since no corresponding statistics are officially available. Compared to the state’s statistics for overall population, study participants are in line regarding migration background and age but differ concerning gender since statistics show a higher proportion of females in Mecklenburg-Western Pomerania (State of Mecklenburg-Western Pomerania, 2016).
Medium ratings of capabilities and no improvement over time indicate a need for action in this field. Our main finding, that improvement of empowerment is the greatest determinant to enhance capabilities, confirms and specifies the according theoretical approaches and empirical findings (Bonvin & Moachon, 2008). Since empowerment in coping with everyday life challenges was found to have the greatest influence, assisting clients in everyday activities, dealing with state authorities, or seeking appropriate medical and psychological treatment might be beneficial forms of intervention. Outreach, person-centered services such as those provided by Case Management, Integrated Care, and Assertive Community Treatment approaches could be a helpful structure for such assistance (Büchtemann et al., 2016; Daßler, 2013; National Association of Social Workers, 2013) if they both empower the beneficiaries and respect their freedom to lead the life of their choice (Bonvin & Moachon, 2008). Core principles of such approaches are strengthening the developmental, problem-solving, and coping capacities of clients, enhancing clients’ ability to interact with and participate in their families and communities and linking them with systems that provide them with resources, services, and opportunities (National Association of Social Workers, 2013).
The finding that social inclusion is the second-largest determinant of the improvement of capabilities is in line with theoretical approaches as well as empirical findings and emphasizes the importance of strengthening this aspect in community-based clinical social work (Riedel-Heller & Richter, 2008; Schuetzwohl et al., 2017). There is no generally accepted definition of what it means to be socially included (Morgan et al., 2007; Schuetzwohl et al., 2017), but it can be assumed that family life, social life, and working life are three key dimensions in this field (Riedel-Heller & Richter, 2008). Community-based social work should foster these areas through socio-therapeutic or, rather, psychosocial interventions such as psychoeducation (Xia et al., 2011), family interventions that aim to reduce stress in the family (Pharoah et al., 2010), or training in life skills such as dealing with money, personal hygiene, or communication competencies (Burkhardt et al., 2007; Stien & Adler, 2007). To foster clients’ social networks, guided peer support (Castelein et al., 2008; Mahlke et al., 2016), a volunteer partner scheme (Sheridan et al., 2015), supported engagement in social activity (Terzian et al., 2013), or psychosocial skills training (Hasson-Ohayon et al., 2014) might be beneficial interventions. To bring more people into the workforce and help them remain there, supported employment has proven to be an effective approach (Burns et al., 2007; Crowther et al., 2001). Social inclusion, in particular, should be enhanced in people who have sought stationary treatment since having been in stationary treatment was found to weaken capabilities. Good communication, cooperation, and networking with stationary stakeholders are key aspects to allow for a smooth transition and integration into outpatient mental health care (Baumgardt et al., 2015).
Our results suggest that stronger empowerment in social relationships and being in a relationship are two further determinants of the improvement of capabilities. Thus, community-based clinical social work should foster stable, reliable, and trustful relationships between caregiver and clients as well as between clients and related persons outside the care system (Chamberlin, 1997). Again, client-centered case management approaches (National Association of Social Workers, 2013; Young et al., 2005) as well as peer support (Corrigan, 2006) might be supportive. Additionally, treatment approaches that focus on social space, social relationships, and social support via community-oriented social work approaches could be beneficial—concepts that have been long called for by researchers as well as by practitioners (Backwith & Mantle, 2009). In Hamburg, the realization of such an approach has led to a compulsory implementation of local open and low-threshold offers for chronically mentally ill people who seek state-funded services and for people in need of such assistance due to psychological difficulties (Hamburg Office for Social Issues, Work, Family, and Integration, 2014). Furthermore, community mental care services have been requested to establish offers and cooperation that reach out to the community to facilitate encounters between people with mental problems and their environment (Hamburg Office for Social Issues, Work, Family, and Integration, 2014). Nowack et al. (2011) reported good results for such open and low-threshold offers that reach out to the community in a pilot project in Germany.
The finding that an improvement of quality of life is connected with an increase of capabilities confirms the overlap between those two concepts (MacLeod, 2014; Nussbaum, 2011; Simon et al., 2013). Thus, aiming to improve quality of life should be another target of clinical social work, for example, through psychosocial day care programs that include social skills training, group therapy, and psychoeducation (Juretić et al., 2016), assertive patient-centered therapeutic engagement, pragmatic crisis intervention and problem-solving techniques, and a focus on community resources (Petrakis & Joubert, 2013). Such interventions should focus on facilitated community linkage to respond to impaired social support (McNiel & Binder, 1997; Rudd & Joiner, 1998) through monitored referral to and engagement with existing community resources.
This study has several limitations. A limitation is the fact that regarding empirical research the field of ambulant integration assistance is a “black box” so far. Therefore, we couldn’t build on previous studies or compare our results with them. Due to study design, results presented are rather “weak,” but since it was practically and ethically not possible to establish a randomized controlled trial, the results presented offer a “first insight” in this “black box.” Since the exact number of benefit recipients in Mecklenburg-Western Pomerania is unknown, we do not know the share of clients in our study cohort compared to the overall study population in that state. Furthermore, the higher number of severely disabled people, as well as the lower number of people who had been in a psychiatric hospital and who had used open offers at community mental health-care services at t1, might have biased the results. Furthermore, no information can be provided on why nearly half of the participants had been subject to experimental mortality between t0 and t1. At least, conclusions drawn from the results must be considered preliminary since this is an explorative study. Despite these shortcomings, we consider the results of this study being important for researchers as well as for practitioners in several ways.
Conclusion
This study offers important insight into the determinants of capabilities in community-based clinical social work. Thus, the results should be considered by social workers and politicians as well as by theoretical and empirical researchers, such as for developing structural frameworks, interventions, and research regarding clinical social work. Community-based clinical social work should foster empowerment and social inclusion through socio-therapeutic or, rather, psychosocial interventions, such as psycho- or socio-education, family interventions that aim to reduce stress in the family, or training in life skills such as dealing with money, personal hygiene, or communication competencies. Nevertheless, the fact that the results of an explorative study like this can only be considered as first hints regarding the questions raised and currently limited evidence in this field, there is a strong need for further research. It has to be identified which components are particularly effective as well as to be determined to what extent community-based clinical social work interventions, in particular, impact patients’ capabilities over time (Anderson et al., 2015).
Footnotes
Authors' Note
Johanna Baumgardt is also affiliated with Department of Psychiatry, Psychotherapy and Psychosomatic Medicine, Vivantes Hospital Am Urban und Vivantes Hospital im Friedrichshain, Charité – Universitätsmedizin Berlin, Germany and Department of Psychiatry and Psychotherapy, Center for Psychosocial Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany.
Acknowledgments
The authors would like to thank their cooperation partner for their vigorous support in the process of data gathering in Mecklenburg-Western Pomerania; the Hamburg Office for Social Issues, Work, Family, and Integration for providing supply information; and all community mental health-care services and the clients who took part in their study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research presented in this article was funded by the public research funding of the city of Hamburg within the research project BAESCAP (Bewertung aktueller Entwicklungen der sozialpsychiatrischen Versorgung auf Basis des Capabilities-Approaches und der Behindertenrechtskonvention der Vereinten Nationen).