
Abstract
Objective:
Foster family care is associated with adverse short- and long-term consequences for the child. A systematic review was conducted on interventions for foster children and foster careers.
Method:
A comprehensive search process was used to find eligible interventions evaluated in randomized controlled trials or quasi-experimental studies. The quality of studies was assessed with GRADE, and effects were synthesized using meta-analytic methods.
Results:
In all, 28 publications of 18 interventions, including 5,357 children, were identified. Only three specific interventions had sufficient confidence of evidence. No study had examined tools for foster parent selection nor had evaluated preservice programs related to outcomes.
Discussion:
These analyses provide new insights and hope into the field of systematic interventions in foster care. The overall results indicate that it is possible to improve eight outcomes but cannot point out which programs are superior. Ethically, social care organizations should systematically collect knowledge about effects and side effects.
Keywords
A sizable proportion (4–6%) of children in Western countries are at sometime placed in foster family or group care during their formative years (Fallesen, Fallesen, Emanuel, & Wildeman, 2014; McGrath-Lone, Dearden, Nasim, Gilbert, & Harron, 2016; Vinnerljung, Hjern, Weitoft, Franzén, & Estrada, 2007). These children are at higher risk than other peers for poor mental/physical/dental health and maladaptive behavior while in care (Vinnerljung & Hjern, 2018). In addition, hardly any study has found better outcomes for young adults grown up in foster care compared to peers raised in adverse birth family environments (Doyle, 2007, 2008; Lindquist & Santavirta, 2014; Olsen, Egelund, & Lausten, 2011; Vinnerljung, 1996; Vinnerljung, Berlin, & Hjern, 2010; Warburton, Warburton, Sweetman, & Hertzman, 2014), regardless of outcome, choice of comparison group, methodological approach, or location of study. Studies attempting to establish causal effects have found that the long-term developmental effects of out-of-home care seem to be at best neutral (Doyle, 2007, 2008; Goemans, van Geel, & Vedder, 2015).
This overall dismal background picture has for several decades led to consistent calls from the scientific community for better knowledge about effective interventions for children in out-of-home care in order to provide meaningful support to policy makers and professionals (Vinnerljung & Hjern, 2018). The aim of this report is to review and synthesize the scientific evidence for supportive interventions, targeting children in foster family care. This project has its origin at the governmental Swedish Agency for Health Technology Assessment and Assessment of Social Services, short SBU (SBU, 2017a).
Previous Reviews of the Efficacy of Foster Care Intervention
Regarding the published research there is a heightened concern that some of the reports are incomplete and untrustworthy (Cumming, 2014; Ioannidis, 2005). Open Science Collaboration (2015) demonstrated that new studies often fail to replicate original results. Converging lines of evidence from systematic reviews and meta-analyses provide far stronger support for findings than single studies. During 1990–2017, at least 80 reviews on foster family care were published, of which 49 were described as systematic. Of these, 11 focused on interventions for children in care. Five of these describe intervention outcomes compared to treatment as usual (Hambrick, Oppenheim-Weller, N’zi, & Taussig, 2016; Kerr & Cossar, 2014; Kinsey & Schlösser, 2012; Leve et al., 2012; Ziviani, Feeney, Cuskelly, Meredith, & Hunt, 2012). Only one (Hambrick et al., 2016) of the five reviews met quality demands, when assessed by Assessment of Multiple Systematic Reviews criteria for systematic reviews (Shea et al., 2007). However, the latter review focused exclusively on child mental health outcome, excluded certain types of interventions (e.g., enhanced foster care and wraparound services), and included trials on other populations as foster children.
Due to this background, we argue that there is a need for a systematic review on intervention effects within foster family care settings.
Purpose of the Study
The purpose of the study was specified in collaboration with four service user organizations, representing individuals who had been in foster care, their birth parents, and foster parents.
This systematic review aims to synthesize the effectiveness of interventions targeting children in foster family care or their foster parents by addressing the following research questions: Are there instruments for foster parent selection that promote the children’s health and adaptive behavior? Are there preservice training programs targeting foster parents that promote children’s health and adaptive behavior? Are there interventions targeting foster children and foster parents that promote children’s health and adaptive behavior? Does foster care interventions in general promote children’s health and adaptive behavior? What ethical challenges arise due to the state of the evidence base with regard to the Questions 1–4?
Method
Inclusion and Exclusion Criteria
Studies were included if they (1) included an experimental and a control group, (2) utilized a pre–post design, (3) provided follow-up data for at least 1 month for children younger than 2 years and at least 3 months for children older than 2 years, (4) included at least 40 foster children, and (5) were published from 1990 to March 2017. Both published and unpublished studies were included.
We specified eligibility (inclusion/exclusion) criteria using the population, intervention, comparison, and outcome approach.
Population
Children up to the age of 17 who are placed in foster family care.
Interventions
Interventions or instruments aiming to select qualified foster parents, preservice training programs targeting foster parents, and interventions targeting children or foster parents during placement in foster family care.
Control groups
Studies that included an active intervention, no treatment, waiting list, or attention control.
Outcome
Interventions that used at least one outcome measure related to child psychological (including internalizing and externalizing symptoms and adaptability), physical and dental health, and social situation (e.g., employment, education, teenage parenthood). Outcomes of a more distal character were also included as placement stability foster carers’ parental skills and foster carers’ internalizing symptoms (e.g., stress).
Studies were excluded if either the experimental or the control group had more than 30% of children placed in kinship foster family care, group care (e.g., residential institutions), or temporary placements (e.g., shelters).
Literature Search and Procedure
Five search methods were used to identify relevant studies. First, 14 databases were searched for articles: Academic Search Elite, Campbell Library, CENTRAL, Cochrane Database of Systematic Reviews, CINAHL, DARE, ERIC, HTA, PsycINFO, PubMed, SocINDEX, Sociological Abstracts, Social Service Abstracts, and Social Care Online. Search terms were modified according to the databases’ thesaurus/subject terms by a specialist librarian and the authors (Online Appendix S1). Second, we searched for relevant articles in local databases in Swedish University libraries and Scandinavian governmental agencies (Online Appendix S1). Third, we searched in the reference lists of all previously published reviews and eligible studies. Fourth, several national scientific journals that only published in their respective languages and without English summary were reviewed: 5 French, 7 Spanish, and 18 German journals. Fifth, known experts from the Scandinavian countries were contacted to identify additional or unpublished data. All principal investigators of the identified studies were also contacted for additional research. Search results (title and abstract) were screened by two authors independently. Discrepancies were resolved by consensus after further detailed analysis and reading. Rayyan, a web and mobile app for systematic reviews, was administered for review screening (Ouzzani, Hammady, Fedorowicz, & Elmagarmid, 2016). The full text assessment was made by two authors independently, and differences were resolved in consensus discussions with the authors of this article.
Risk of Bias Assessment and Data Extraction
Risk of bias was assessed according to the SBU standardized checklists for determining the extent to which studies meet basic quality criteria. The criteria assess risk for selection bias, performance bias, detection bias, attrition bias, reporting bias, and conflict of interest bias. This checklist is similar to the Cochrane checklist (http://www.cochrane.org/) but has additional items (Guyatt et al., 2011; SBU, 2017b). The quality of included studies (i.e., risk of bias) was rated as high, moderate, or low. Only studies with moderate to low risk of bias were considered for grading of scientific evidence and conclusions. Any disagreements on quality rating of individual studies were resolved within the group of reviewers by consensus.
Thereafter, data were extracted from the included publications. All recorded extracted data were checked by the authors in pairs and included first after consensus discussions. All decisions were documented.
Grading of Evidence
The quality of the evidence for outcome measures was assessed according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system (Balshem et al., 2011) with minor modifications done by SBU. The SBU system uses different terminology compared to the GRADE working group using the wordings “strong evidence” (⊕⊕⊕⊕), “moderately strong evidence” (⊕⊕⊕^), “limited evidence” (⊕⊕^^), and “insufficient evidence” (⊕^^^).
The included studies were all first preliminary assumed to have the highest possible quality of evidence (⊕⊕⊕⊕). Thereafter, when assessing the studies according to the criteria (risk of bias, imprecision, inconsistency, indirectness, and publication bias) for rating the quality, one or two points can be deducted for each criterion.
Statistical Procedures
Data related to effect size were entered into Comprehensive Meta-Analysis Version 3.0 (Borenstein, Hedges, Higgins, & Rothstein, 2014). Standardized mean difference (SMD; also known as Cohen’s d) was calculated by taking the difference in pre- to follow-up measure means for each group and dividing these by their pooled standard deviations (McCart, Priester, Davies, & Azen, 2006). When studies did not provide one of these values, Cohen’s d was computed according to Lipsey and Wilson (2000) and the Practical Meta-Analysis Effect Size Calculator (Wilson, 2001). Following the somewhat perfunctory criteria of Cohen (1988), an effect size of d = 0.20 was considered small, an effect size of d = 0.50 was considered medium, and an effect size of d = 0.80 was considered large. In this review, we only considered effects of 0.20 or larger. Outliers were checked based on z values larger than 3.29 or smaller than −3.29 (p < .005; Tabachnick & Fidell, 2013). No outliers were found.
Publication Bias
Studies reporting strong significant associations are more likely to be accepted for publication in a journal (Ioannidis, 2005). Therefore, studies that report nonsignificant results are more difficult to find and may be published only in the so-called “grey literature” (agency reports, working papers, etc.). If this is the case, conclusions may be incomplete. One way to analyze this possibility is by using a funnel plot of the distribution of effect sizes. In this study, it was not deemed relevant to use a funnel plot because of the heterogeneity of the identified studies. However, we searched for “grey literature” without identifying an additional study that met the inclusion criteria.
Ethical Analysis
The ethical analysis was carried out using an existing structured checklist modified for Swedish social services, for inclusion of ethical aspects in health technology (Munthe, Sandman, & Nykänen, 2015) as well as recognized issues in social work (Banks, 2012; Molin & Palmer, 2005). The checklist addresses the aims of foster care, examines possible goal conflicts, and focusses on the responsibility of society for children taken into social care. Further, ethical aspects of research regarding children (Millum & Emanuel, 2007), and uncertainty motivating research (Munthe, 2016), were included. A major premise of the analysis was that when society takes a caring role for children, especially when this is done using legal force, then society also assumes a specific and important moral responsibility to promote the interests of these children (the principle of in loco parentis; Miller, 2003).
Results
The search resulted in 5,298 possibly eligible citations. After excluding nonrelevant articles and those with high risk of bias, our final sample consisted of 18 interventions, comprising 67 effect sizes, based on 5,357 children between the ages 0 and 17 years. The interventions were evaluated in 23 studies and reported in 28 articles (Figure 1).
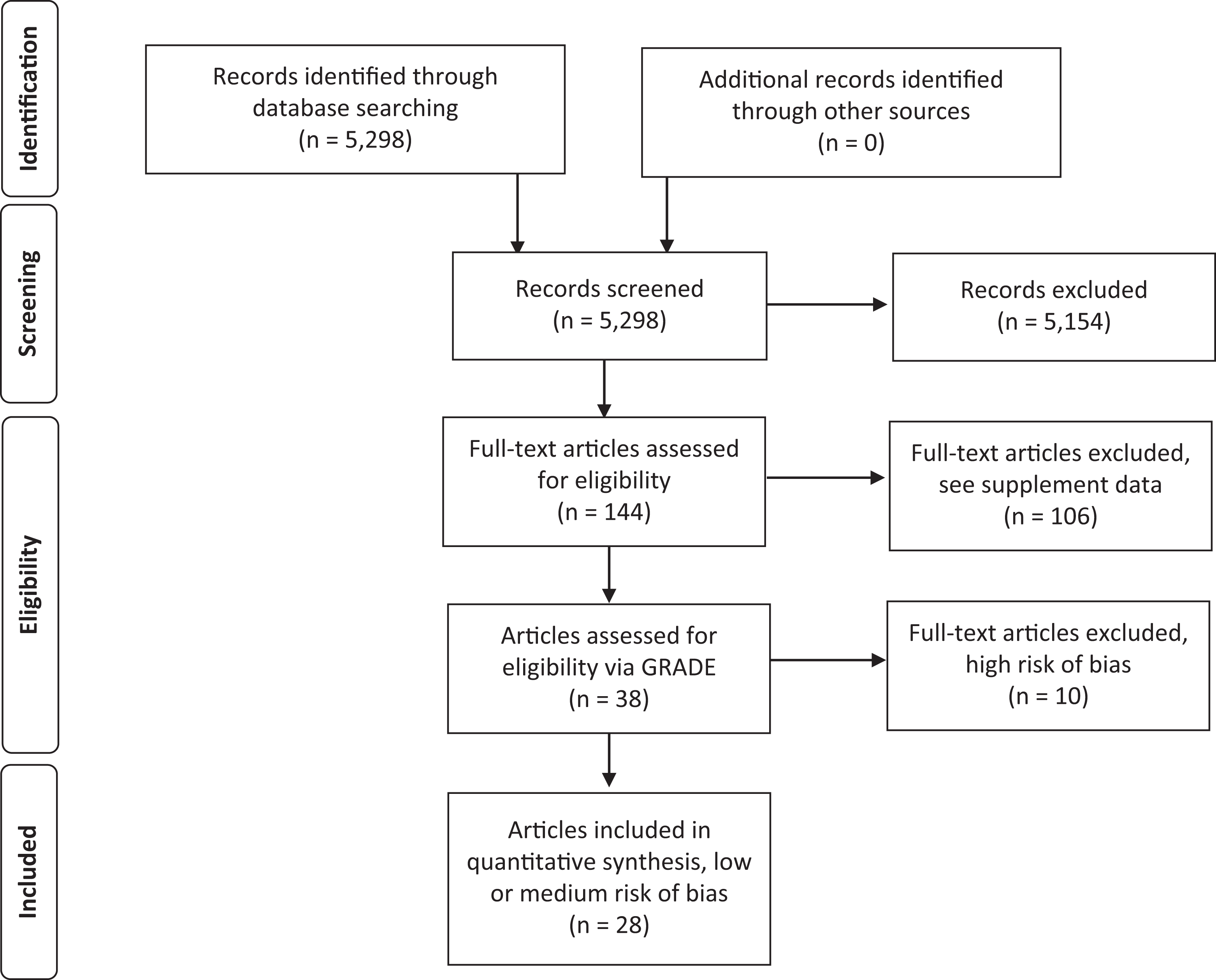
Literature review flowchart (modified Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2009 version; Moher, Liberati, Tetzlaff, & Altman, 2009).
Of the 18 interventions, 5 targeted mainly the child: Better Futures, Fostering Healthy Futures, Incredible Years Dina Program for Young Children, Supporting Sibling in Foster Care, and Take Charge. Eight interventions targeted foster parents: Attachment and Biobehavioral Catch-up (ABC), Foster Family Intervention, Promoting First Relationship, Incredible Years Parenting Program, Keeping Foster and Kinship Parents Supported and Trained, Neighbor To Family, Parent Management Training Oregon, and Promise. The last five interventions targeted both the child and her or his foster parents: Casey Family Programs, Fostering Individualized Assistance Program, Middle School Success, Multidimensional Treatment Foster Care for Preschoolers, and Parent–Child Interaction Therapy.
The articles were published between 1994 and 2017. Most studies were conducted in the United States (n = 20), and only three in Europe (the Netherlands, n = 2, and United Kingdom, n = 1). The majority, 20 of 23, were randomized controlled trials, and the rest, 3, nonrandomized longitudinal trials with a matched comparison group.
All included interventions are characterized by a systematic standardized process of how they are delivered and a well-defined target for what is going to change for whom. Most also specify duration (when the changes should be accomplished) and dose (number of sessions or coordination meetings). The interventions are all manualized. Most include an educational curriculum for staff delivering the intervention, in some cases also a certification process.
The 23 studies are characterized by considerable methodological heterogeneity, including differences in participant characteristics, extent of sessions and outreach in time, lengths of follow-ups, trial design, and a high variety of measured outcomes; more than 50 different outcome measures were used. A further aspect was that many of the studies were undertaken by groups, researchers, or institutions with more or less visible conflicts of interests, usually in the form of financial stakes in the use of trademarked interventions, supply of educational programs for such use, literature to guide this use, and so on. An overview of the studies is presented in Table 1.
Study Characteristics.
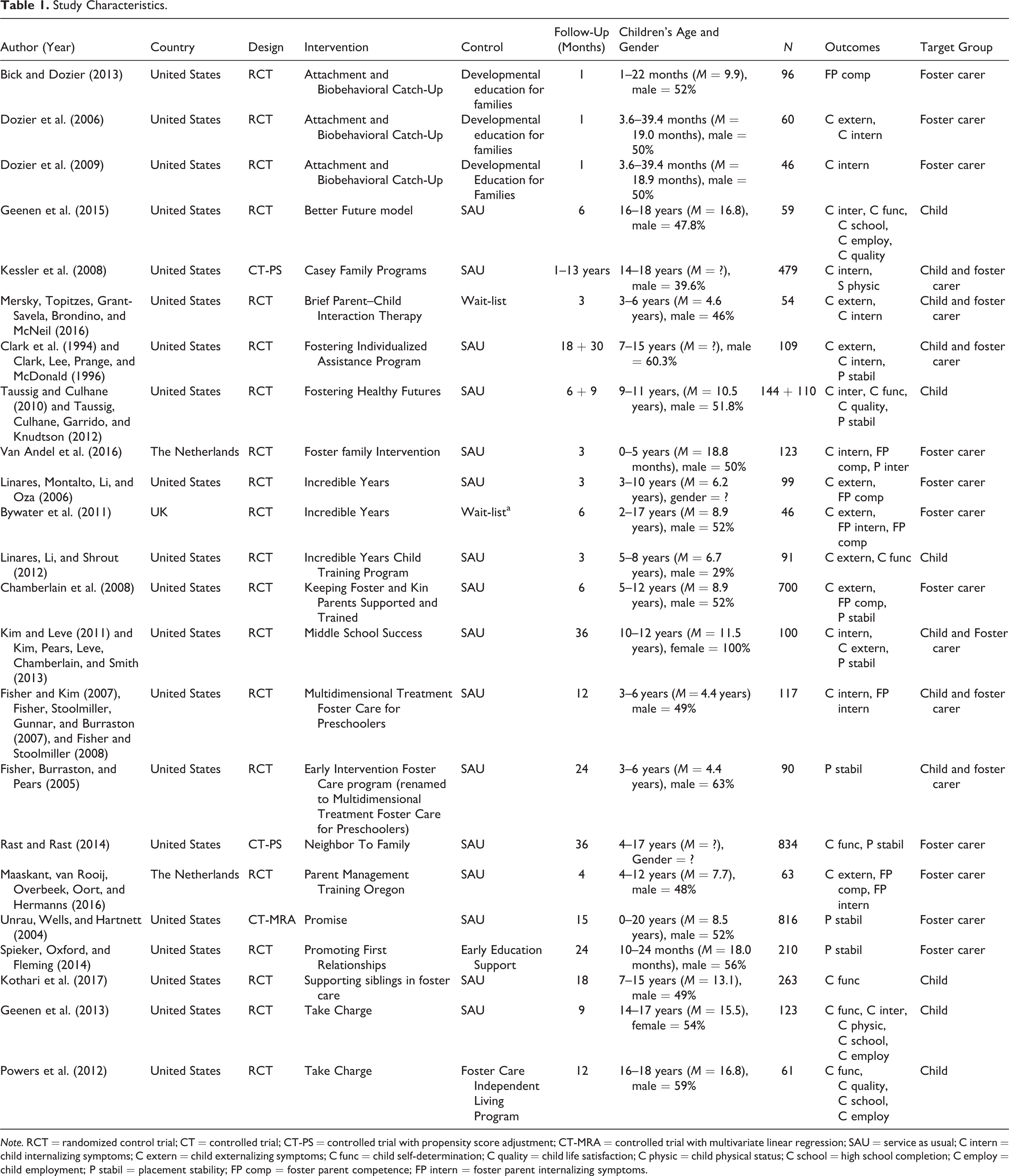
Note. RCT = randomized control trial; CT = controlled trial; CT-PS = controlled trial with propensity score adjustment; CT-MRA = controlled trial with multivariate linear regression; SAU = service as usual; C intern = child internalizing symptoms; C extern = child externalizing symptoms; C func = child self-determination; C quality = child life satisfaction; C physic = child physical status; C school = high school completion; C employ = child employment; P stabil = placement stability; FP comp = foster parent competence; FP intern = foster parent internalizing symptoms.
Instruments for Foster Parent Selection and Preservice Training
None of the studies had assessed instruments/tools for recruiting qualified foster parents or general preservice training of foster parents with outcome measures related to the fostered children.
Interventions Targeting Foster Children and Foster Parents
All included studies dealt with support to foster parents or to children in ongoing care. In most studies, several outcomes were reported (Table 1). The most frequent were the child’s internalizing symptoms as anxiety, depression, and stress (12 studies), externalizing symptoms as aggressiveness and behavioral problems (9 studies), self-determination (7 studies), and placement stability (7 studies). Less frequent outcomes were somatic health (two studies), quality of life (three studies), educational outcomes (three studies), and employment (three studies). Some studies also included measures on foster parents’ abilities (e.g., sensitivity, adaptation to the child’s needs; six studies) and self-reported depressive or stress symptoms (three studies). No study assessed effects on teenage pregnancy or dental health. In addition, no study examined potentially harmful effects of the intervention.
Of the 18 interventions, 15 were evaluated in one single trial, mainly by the program developers. Using GRADE, we conclude that the quality of evidence is insufficient for the effect estimates of outcomes from these 15 studies (⊕^^^).
For three of the interventions, the quality of the evidence is limited (⊕⊕^^) or moderate (⊕⊕⊕^) according to GRADE. ABC may enhance the child’s attachment behavior (Table 2), Incredible Years may increase foster parents’ parenting competencies as well as the child’s externalizing and conduct problems (Table 3), and Take Charge probably improves the youth’s self-determination and employment status in late adolescence and may increase high school completion (Table 4).
The Effect of Attachment and Biobehavioral Catch-Up Compared to Developmental Education for Families for Foster Care Infants.
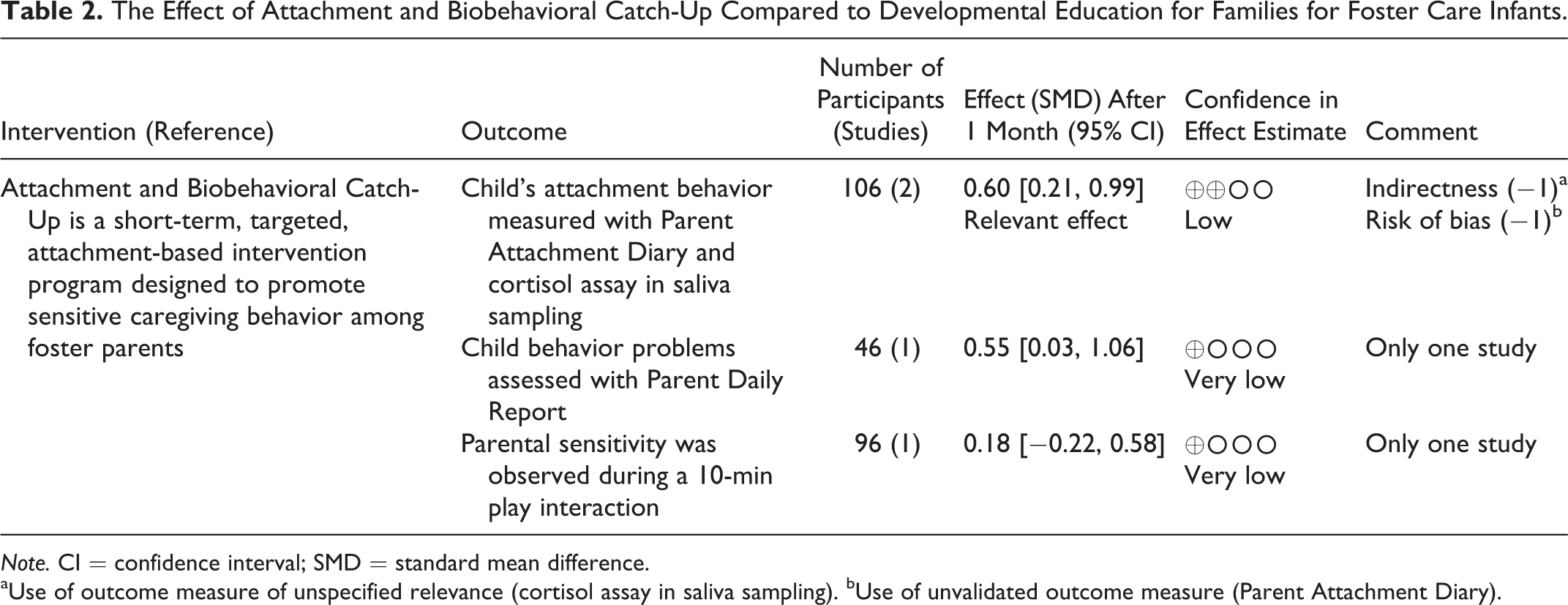
Note. CI = confidence interval; SMD = standard mean difference.
aUse of outcome measure of unspecified relevance (cortisol assay in saliva sampling). bUse of unvalidated outcome measure (Parent Attachment Diary).
The Effect of Incredible Years Compared to Usual Service for Foster Children of Various Ages.
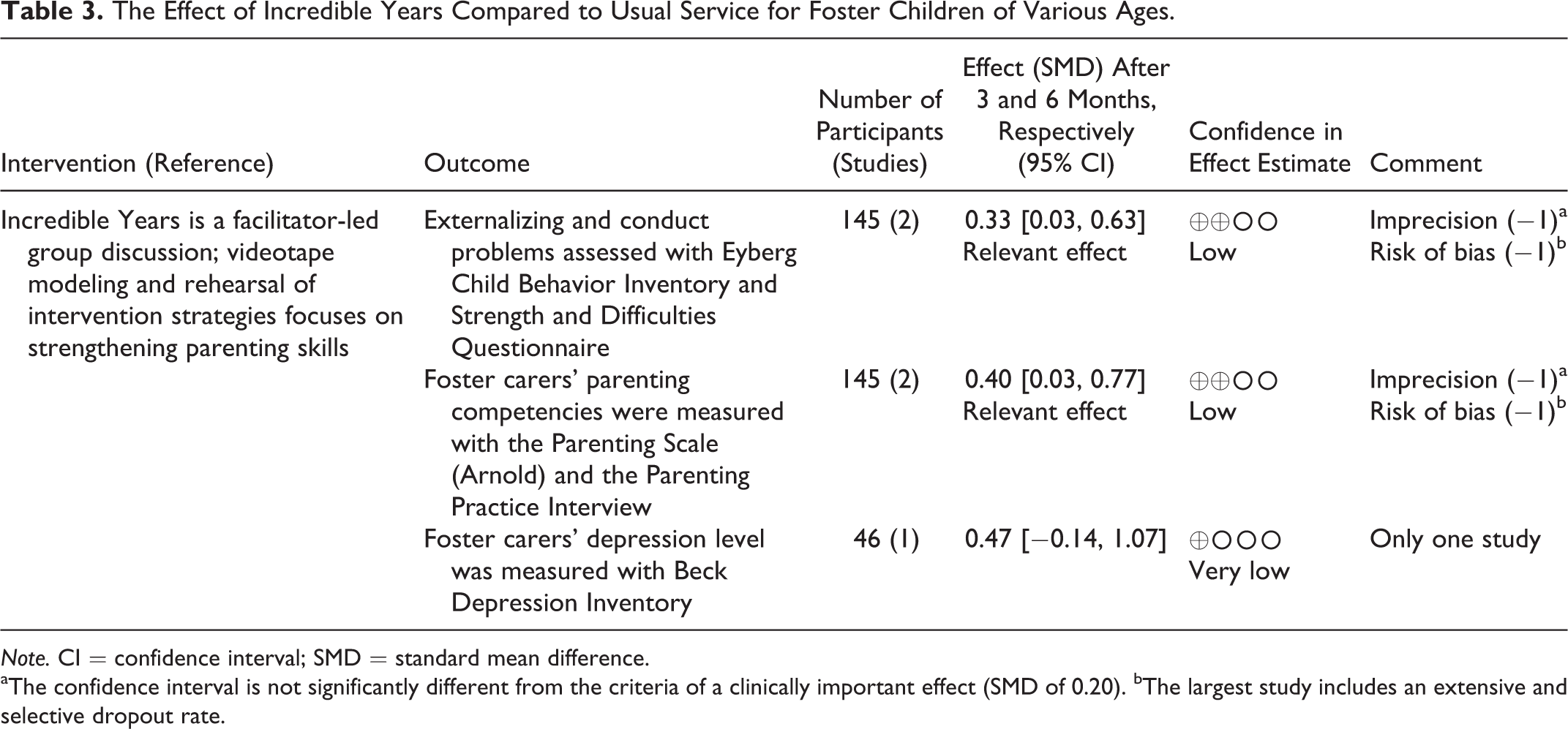
Note. CI = confidence interval; SMD = standard mean difference.
aThe confidence interval is not significantly different from the criteria of a clinically important effect (SMD of 0.20). bThe largest study includes an extensive and selective dropout rate.
The Effect of Take Charge Compared to Service As Usual Respectively Foster Care Independent Program for Foster Care Youth.
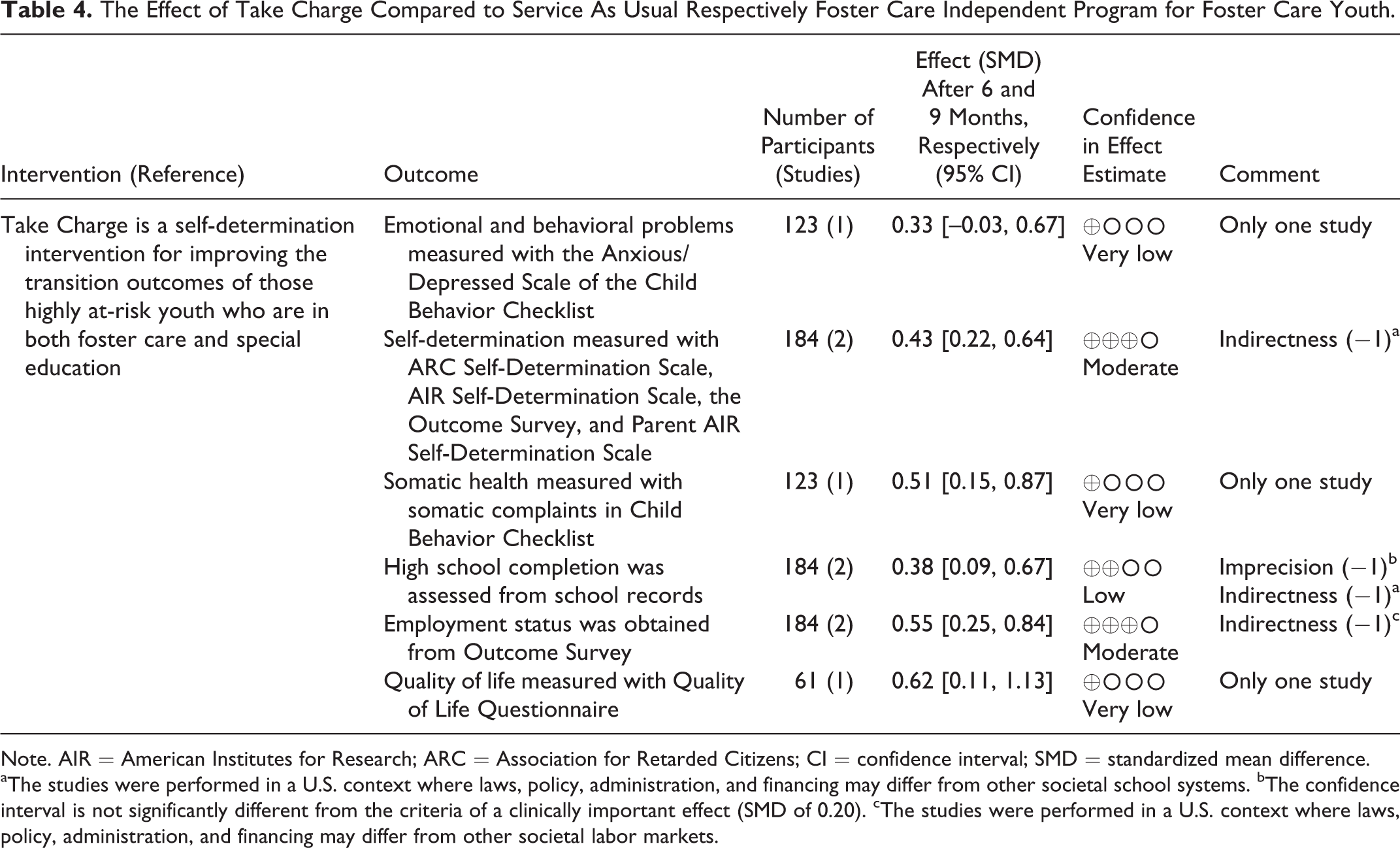
Note. AIR = American Institutes for Research; ARC = Association for Retarded Citizens; CI = confidence interval; SMD = standardized mean difference.
aThe studies were performed in a U.S. context where laws, policy, administration, and financing may differ from other societal school systems. bThe confidence interval is not significantly different from the criteria of a clinically important effect (SMD of 0.20). cThe studies were performed in a U.S. context where laws, policy, administration, and financing may differ from other societal labor markets.
Effects of Foster Care Interventions in General
Although we have low confidence in each of the singular effect estimates for 15 of 18 interventions, their overall results indicate that it is possible to affect 8 of the 10 outcomes. In Figures 2 –11, the effect sizes are presented for each of the outcomes. We did not calculate a weighted mean effect size because of the heterogeneity across the 23 studies.
Effect sizes (Cohen’s d) of studies assessing internalizing symptoms.
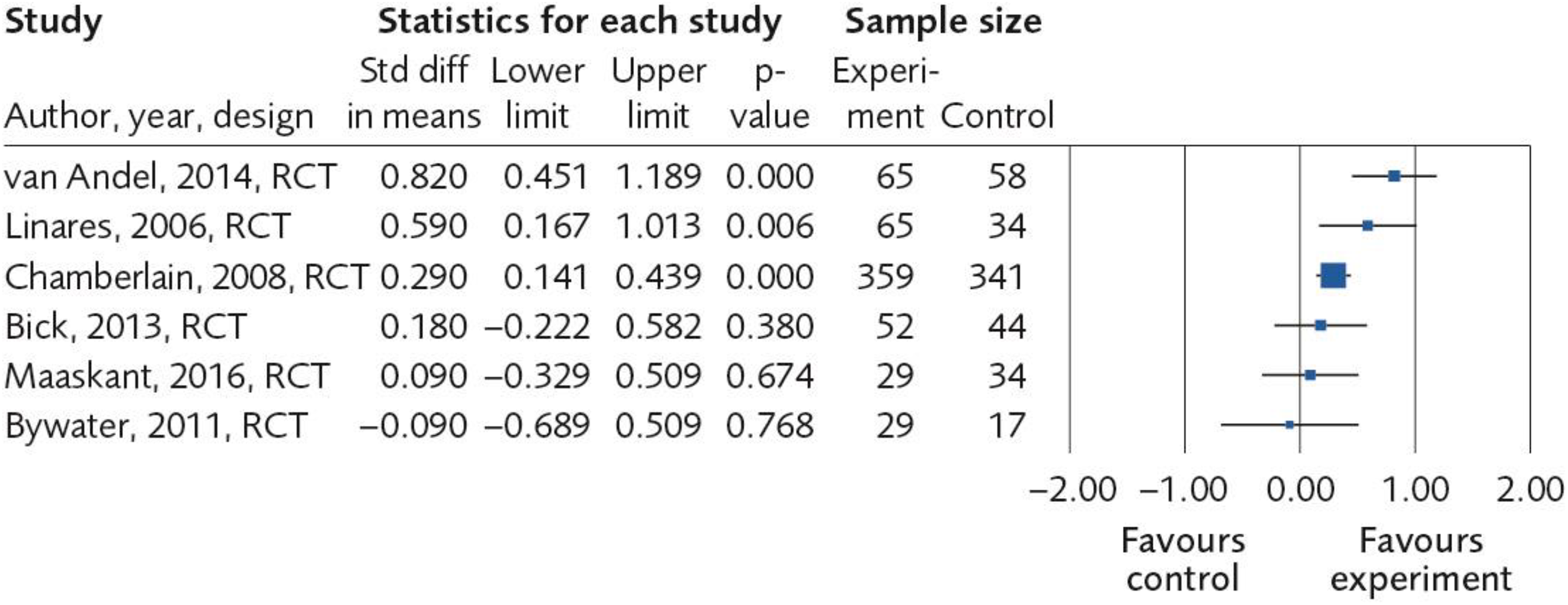
Effect sizes (Cohen’s d) of studies assessing externalizing symptoms.
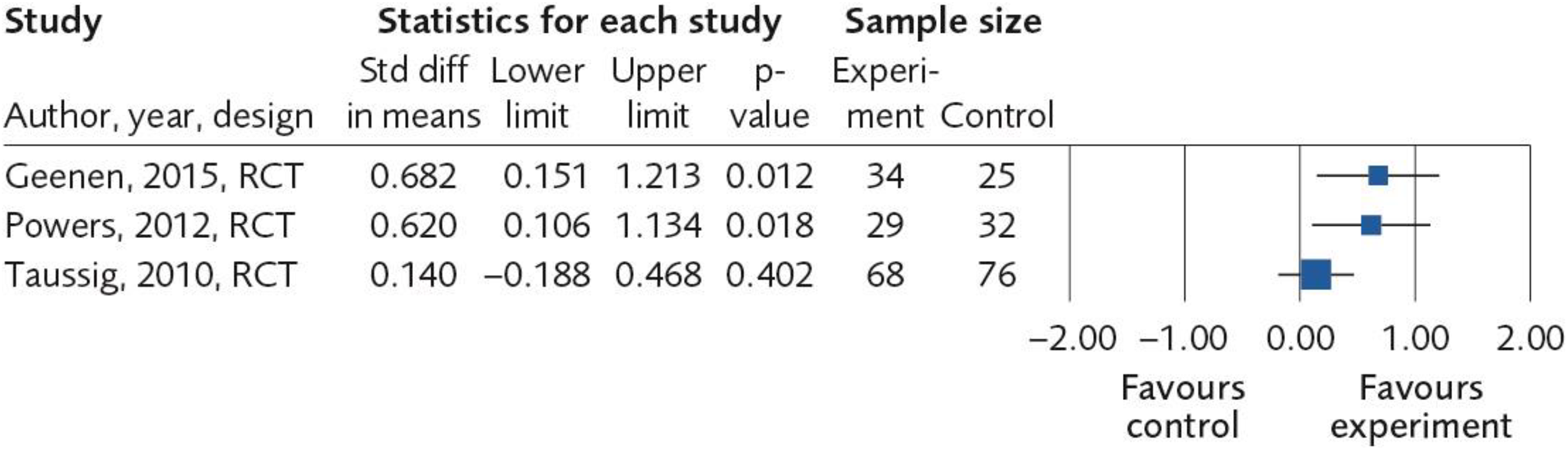
Effect sizes (Cohen’s d) of studies assessing self-determination.
Effect sizes (Cohen’s d) of studies assessing placement stability.
Effect sizes (Cohen’s d) of studies assessing physical health.
Effect sizes (Cohen’s d) of studies assessing education.
Effect sizes (Cohen’s d) of studies assessing employment.
Effect sizes (Cohen’s d) of studies assessing life satisfaction.
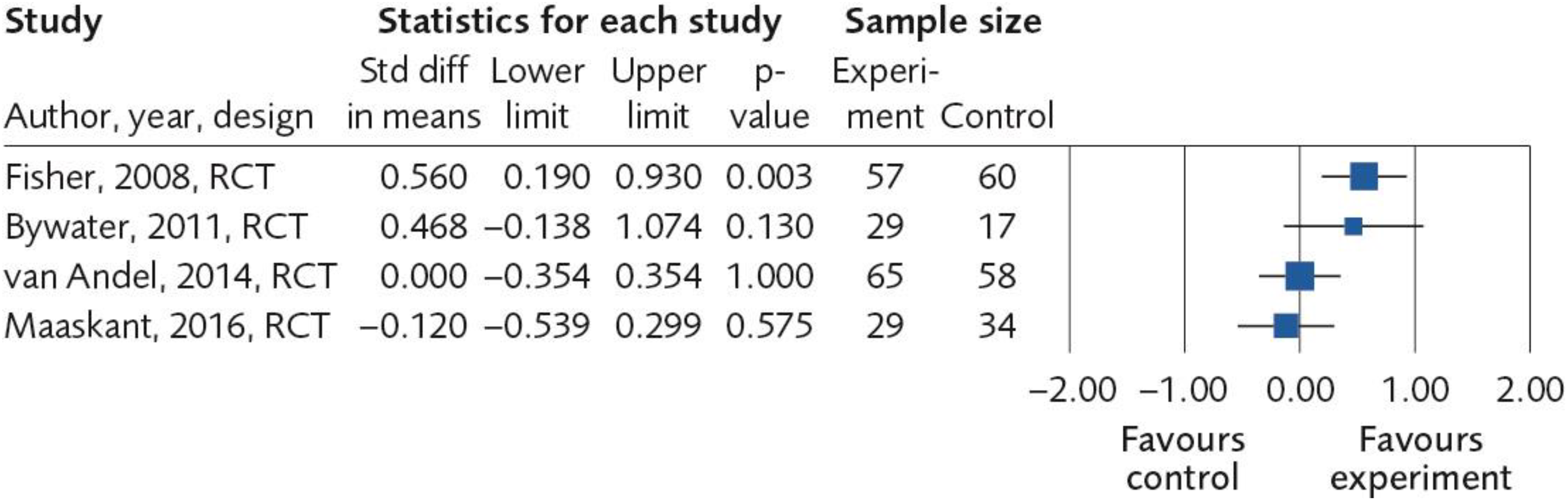
Effect sizes (Cohen’s d) of studies assessing foster parent competence.
Effect sizes (Cohen’s d) of studies assessing foster career internalizing symptoms.
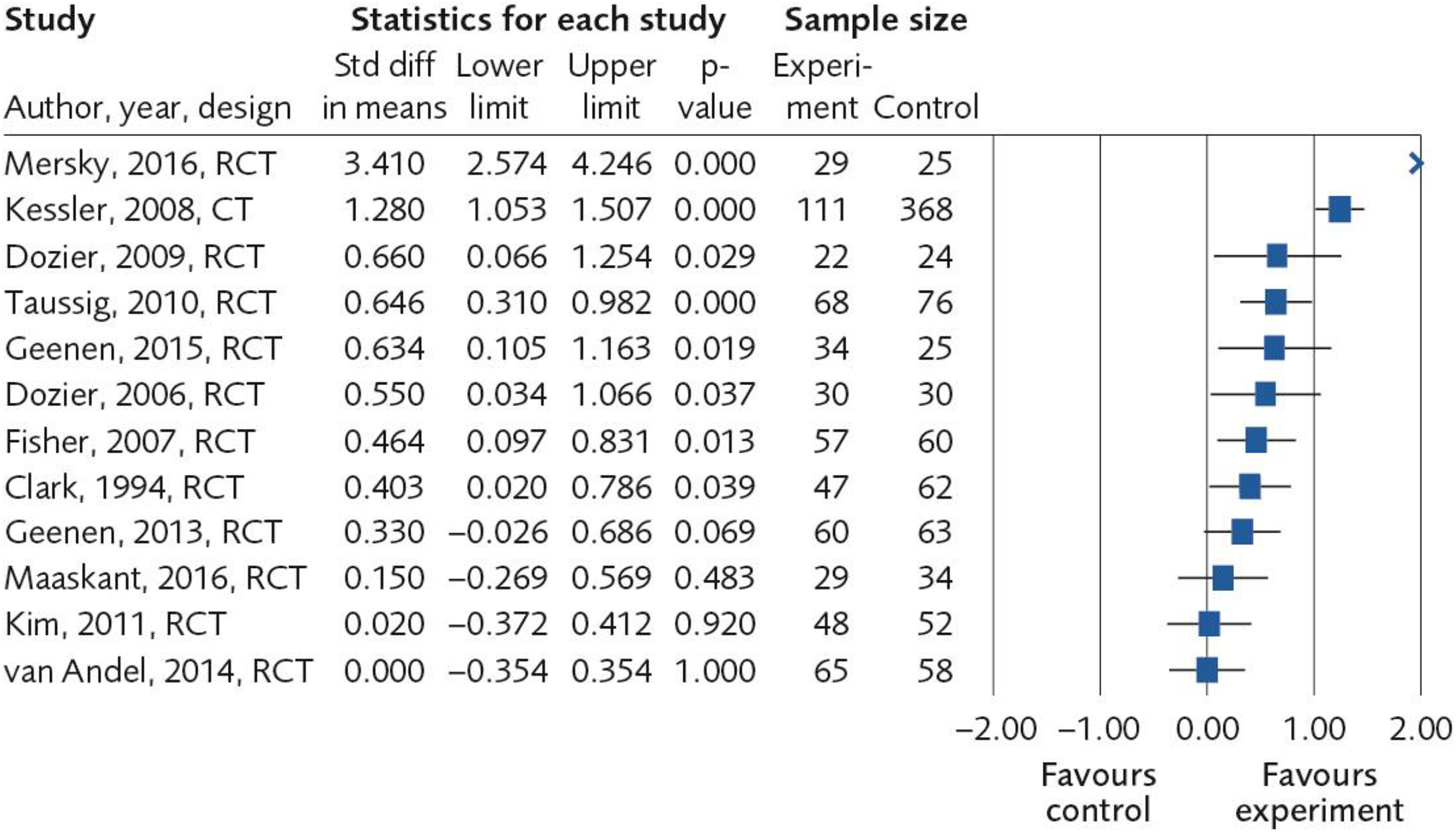
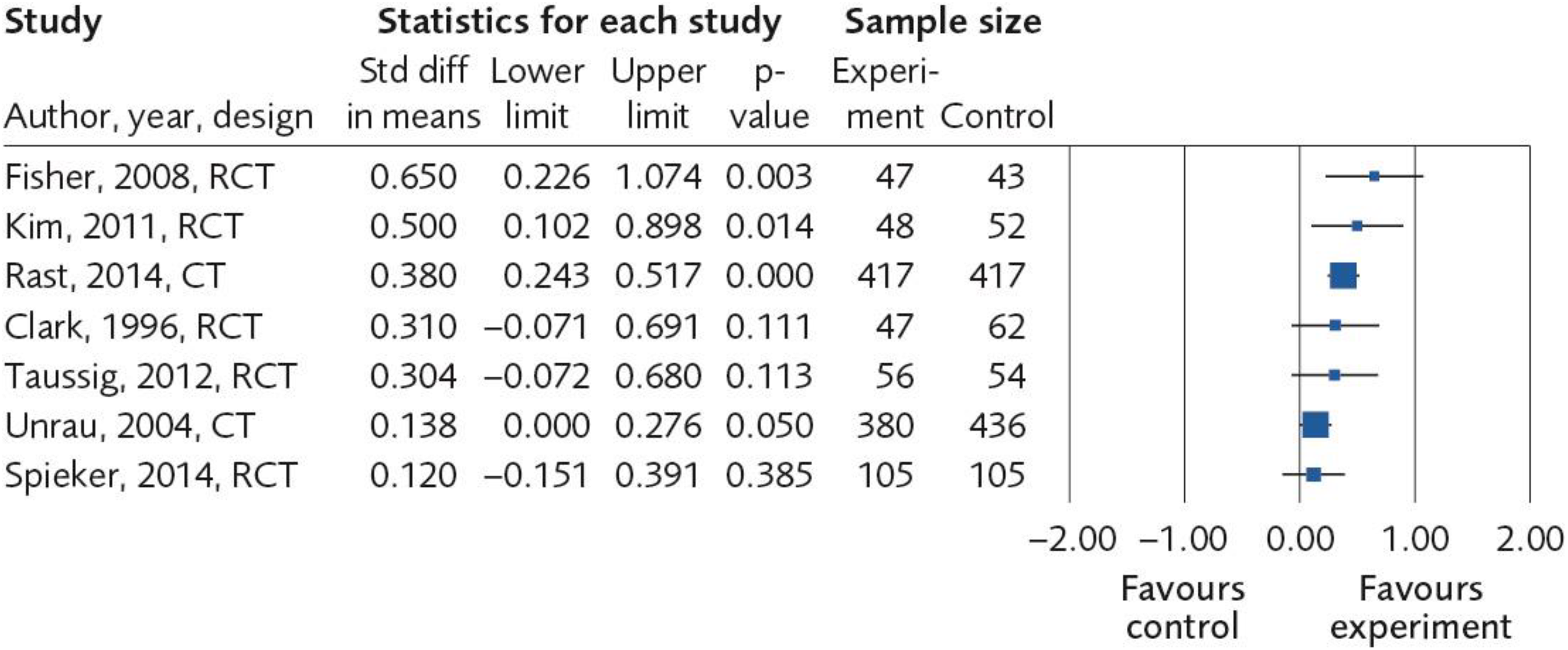
Of the 12 studies that included internalizing symptoms (e.g., anxiety, depression, and stress) as an outcome, 9 reported SMD above 0.20 (Figure 2). In 11 of these 12 studies, the control group received service as usual (SAU), with an average follow-up of 12 months of 1,477 children. According to GRADE, the quality of the evidence is limited (⊕⊕^^) because seven different measures were used to assess internalizing symptoms (risk of bias, −1) and because 3 of 12 studies did not reach SMD 0.20 (imprecision, −1).
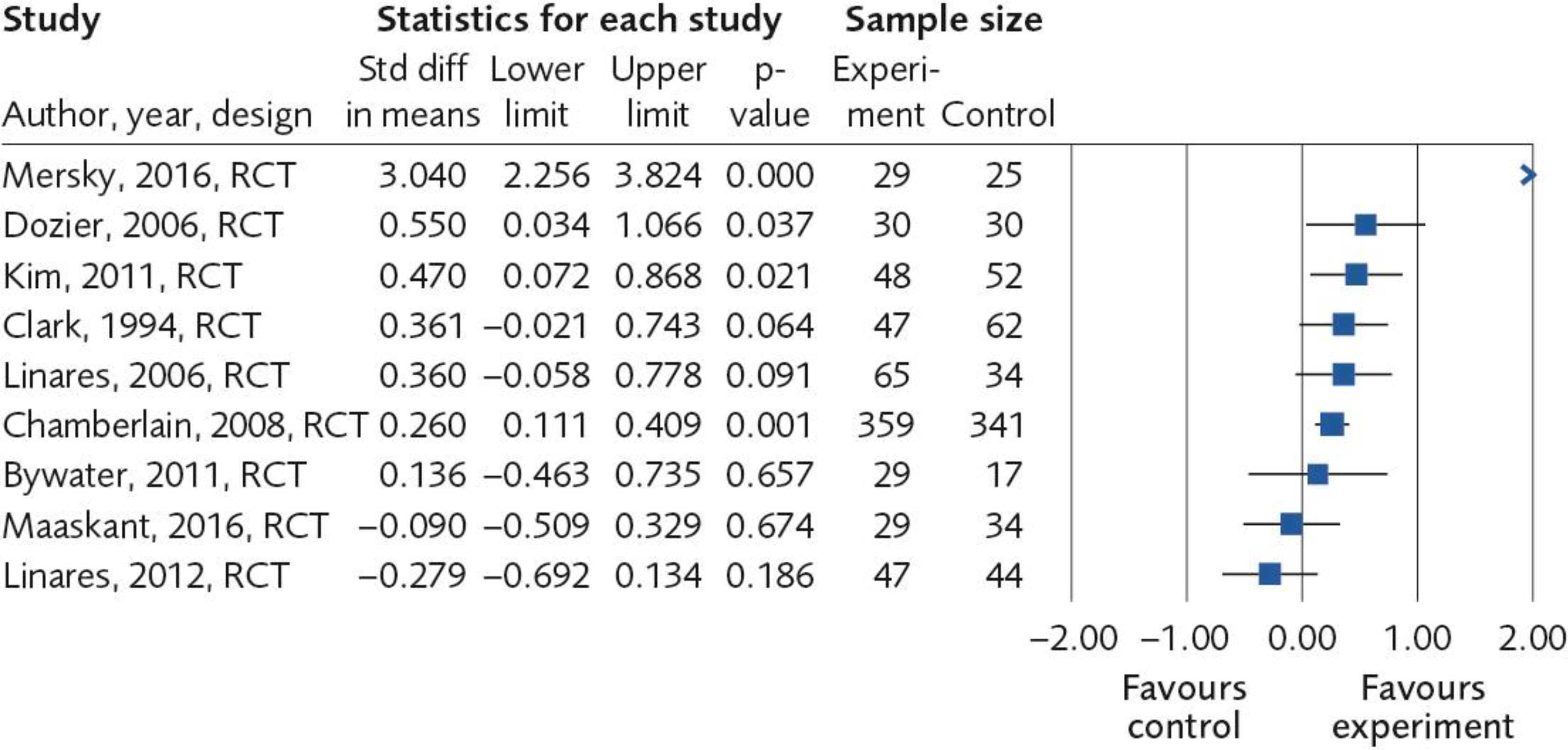
Externalizing symptoms (e.g., criminality) were assessed in nine studies, including 1,322 children and an average follow-up time of 9 months (Figure 3). Of the nine studies, six reported effects exceeding SMD of 0.20. The comparison group was in eight of nine publications SAU. The quality of the evidence is considered limited (⊕⊕^^) because five different measures were used to assess externalizing symptoms (risk of bias, −1) and because three of nine studies did not reach SMD 0.20 (imprecision, −1).
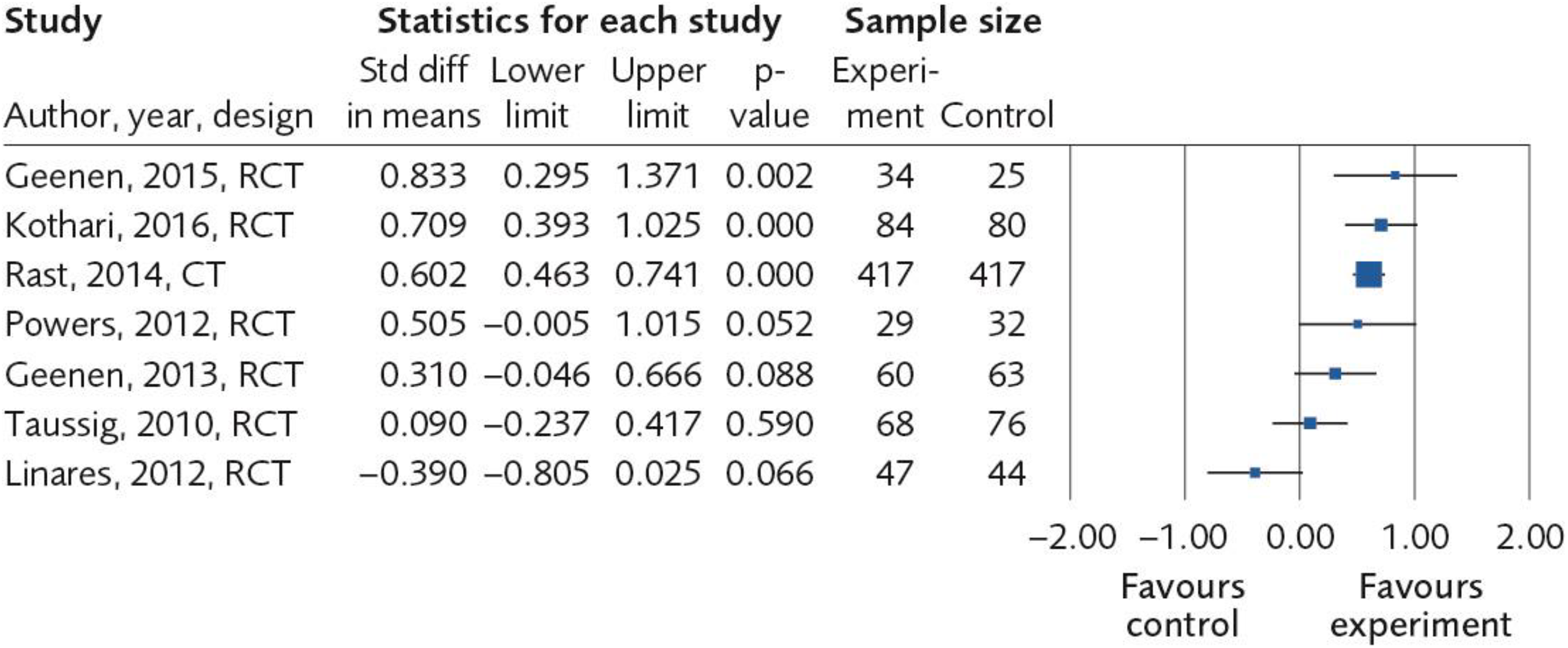
Seven studies included an outcome of the child’s adaptive behavior (e.g., self-determination; Figure 4). These studies included 1,575 children, and the comparison was in six studies SAU. In five of these seven studies, the SMD exceeded 0.20. The average follow-up time was 13 months. The evidence was graded as limited (⊕⊕^^) because seven different measures were used to assess adaptive behavior (risk of bias, −1) and because two of seven studies did not reach SMD 0.20 (imprecision, −1).
Stability in care was measured in seven studies (Figure 5). The comparison was in six publications SAU, and the average follow-up was 18 months. In five of the seven studies, the SMD exceeded 0.20. The evidence was graded as moderate (⊕⊕⊕^) because two of seven studies did not reach SMD 0.20 (imprecision, −1).
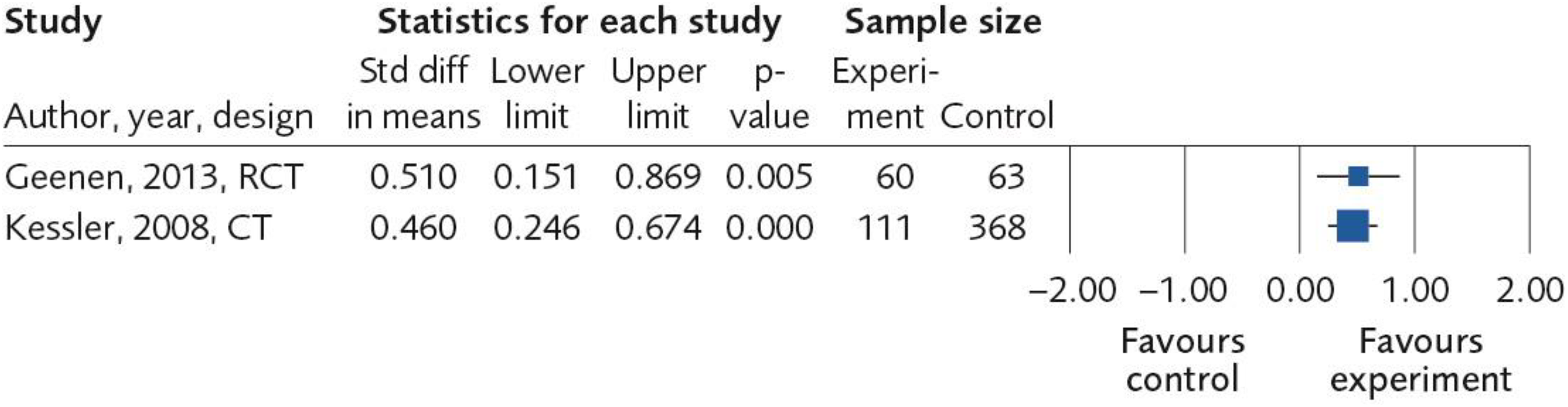
Two studies including 602 children examined somatic health, with follow-up time of 9 and 66 months (Figure 6). Both studies used SAU as comparison, and both studies’ SMD exceeded 0.20. The quality of the evidence is rated as moderate (⊕⊕⊕^) because two different measures were used to assess physical health (risk of bias, −1).
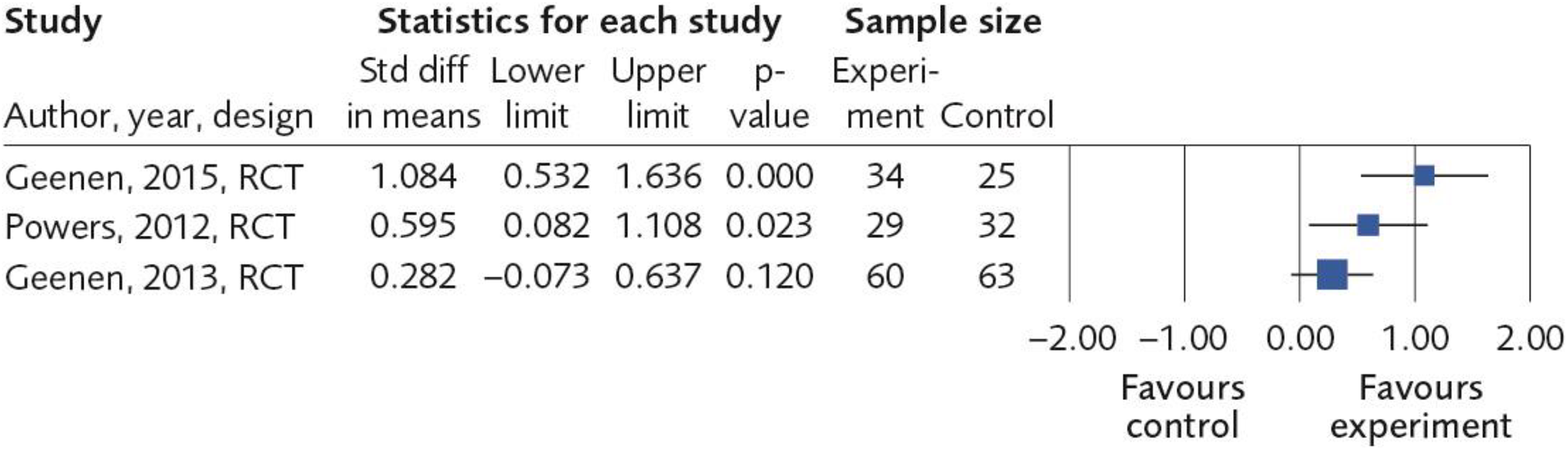
Educational accomplishment was an outcome in three studies including 243 adolescents (Figure 7). The comparison group consisted of SAU in two and all three reported SMD exceeding 0.20. The follow-up time was between 6 and 12 months. The quality of the evidence is rated as moderate (⊕⊕⊕^) because the school system of Sweden and the United States differ (risk of indirectness, −1).
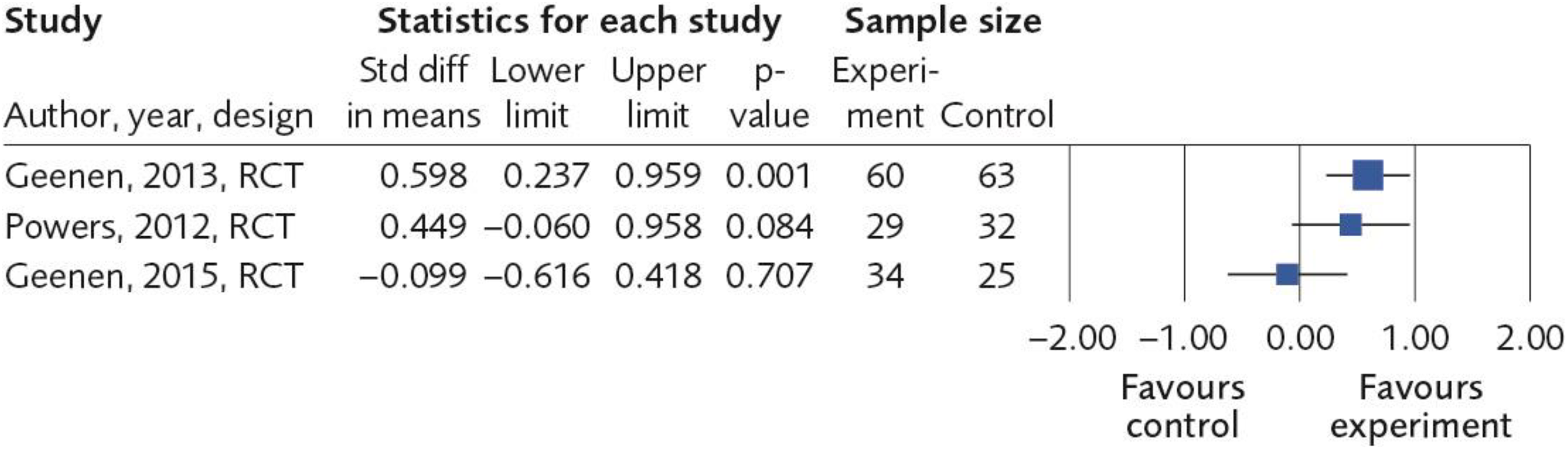
Three studies investigated whether the interventions improved the possibilities of employment after leaving school (Figure 8). The studies included 243 adolescents and 2 of them had SAU as comparison. For two of the studies, SMD exceeded 0.20. The follow-up time was between 6 and 12 months. The evidence was graded as limited (⊕⊕^^) because of differences in the labor market systems that regulate youth employment in the United States versus other national contexts (risk of indirectness, −1) and because one of three studies did not reach SMD 0.20 (imprecision, −1).
Quality of life was assessed in three studies including 264 children (Figure 9). Two of these studies had SAU as comparison, and two studies had SMD exceeding 0.20. Follow-up time was between 6 and 12 months. The evidence was graded as limited (⊕⊕^^). One point was deducted because two measures were employed to assess quality of life (risk of bias, −1) and because one of the three studies did not reach SMD 0.20 (imprecision, −1).
For two outcomes, evidence was considered insufficient (⊕^^^). Foster carer’s parenting skills (e.g., adaptability to child needs) was used as outcome in six studies, including 1,127 foster parents (Figure 10). In three studies, SMD exceeded 0.20. One point was deducted because each study employed different measures to assess parental competence (risk of bias, −1) and because three of six studies did not reach SMD 0.20 (imprecision, −2). The other outcome was foster carer’s internalizing symptoms. It was assessed in four studies and 349 adults (Figure 11). Two of these studies reported SMD exceeding 0.20. One point was deducted because each study employed different measures to assess internalizing symptoms (risk of bias, −1) and because two of four studies did not reach SMD 0.20 (imprecision, −2).
Discussion and Applications to Practice
The purpose of the systematic review was to examine outcomes of instruments for foster parent selection, preservice training programs, and foster care interventions targeting outcomes of health and other aspects of children in foster family care. The systematic review resulted in a total of 23 controlled studies, consisting of more than 5,000 children, and 67 effect sizes were included.
In response to first research question, no study was identified that assessed effects of instruments for foster parent selection related to outcomes for the foster children. This result is in line with a previous review focused on how foster carers are recruited and assessed (Luke & Sebba, 2013).
As for the second research question, no relevant study had assessed the effects of basic preservice foster parent training on children’s mental and physical health. This result is in line with an earlier review (Festinger & Baker, 2013).
The third research question dealt with the effects of interventions targeting foster children or foster parents. Three interventions meet the GRADE criteria of limited or moderate evidence. Meta-analyses indicate that ABC targeting foster parents may improve children’s attachment behaviors (⊕⊕^^), and Incredible Years Parenting Program may improve parenting abilities of foster parents as well as decrease children’s externalizing behaviors (⊕⊕^^). The third intervention, Take Charge for young people, probably improves children’s self-determination skills (⊕⊕⊕^), high school completion (⊕⊕^^), and probably increases their likelihood of employment after high school (⊕⊕⊕^). All effect sizes were small to moderate. Numbers needed to treat (the average number of children that needed to receive the intervention for one to be successful) was five to eight children.
As for the fourth research question, when all 18 interventions were compiled together, the results indicate that intervention programs seem to produce effects. However, due to the differences in interventions and methodological variation of evaluations (including a high variation of outcome measures), it is not possible to determine which interventions or components are more effective than others.
The fifth research question concerns the ethical implications of the answers to Questions 1–4. Weak evidence in different types of decisions regarding foster care is a distinct ethical challenge to the justification of such decisions. At the same time, there are interventions for which differing degrees of evidence exist, and here the ethical challenge may instead be that those interventions are not implemented. This situation implies further ethical problems for social work research. First, there are ethical reasons to examine interventions in areas where studies are lacking. Second, such studies may create new ethical dilemmas for social workers, for example, children might have to be randomly assigned to control and experimental groups, which raises the issue of how informed consent can be obtained from minors as well as the elevated risk of a “therapeutic misconception,” where experimental actions are confused with proven treatment (Appelbaum, Lidz, & Grisso, 2004). Third, researchers need to be more transparent with possible conflicts of interest, for instance, if researchers evaluate interventions that they also are financially involved in.
This systematic review provides good cause for hope. The overall message is that included interventions may improve foster children’s well-being and stability of placement. Three interventions demonstrate that they probably are effective in at least one specific respect, one each targeting toddlers (ABC program), younger children (Incredible Years), and adolescents (Take Charge). For the other 15 interventions, there were not sufficient studies to assess their specific effects, when applying the GRADE model. The absence of robust evidence for these interventions does not imply that they are ineffective, rather that the empirical evidence is not up to GRADE standards. The message to those working with foster family care is to closely monitor and document the progress of individual children when using any kind of systematic intervention program.
The project where this report has its origins conducted a survey on interventions in use in foster family care in Sweden (SBU, 2017a). A questionnaire was sent to a random selection of 106 municipalities as well as all 38 private sector service providers. A total of 30 different interventions were identified. However, none had been evaluated in controlled research. This strongly indicates the need within foster care for enhanced strategies when selecting new interventions to implement. Furthermore, a clear majority claimed to use instruments for foster care selection as well as preservice training of foster parents, but only 34% had access to interventions for supporting foster children of foster parents during ongoing care. This means that in Swedish foster care, focus is on tools for foster parent selection and preservice training that lack empirical support, while evaluated interventions are rare. This state of affairs was strongly questioned by representatives from the four service user organizations that were consulted in preparation of this systematic review (SBU, 2017a). In unison, they called for empirically supported services within foster care.
There are some implications for future research. First, there is a need for replicational studies of interventions. Among the 18 interventions studied here, there exists only one controlled trial for 15 of them, making it hard to assess the quality of the evidence. Are these 15 interventions also effective in other contexts? Or is the fact that they just exist in one context a result of that they are difficult to implement in another context than the original context?
A second implication is the need for less heterogeneity in research methodology. Meaningful comparisons and syntheses of individual trial results depend on a sufficient level of uniformity between trials (Higgins et al., 2011) but also on reasonably comparable constructs of outcome measures. If this is not the case, clinical heterogeneity, including differences in participant characteristics, trial methods, and choice of outcome measures, can moderate the magnitude of the intervention effect, risking the introduction of nonsystematic bias in reviewers’ conclusions and, by extension, threaten the internal validity of those conclusions. Today, initiatives have been done by Consensus-based Standards for the selection of health Measurement Instruments (www.cosmin.nl) and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (www.prisma-statement.org) to enhance homogeneity. We need these initiatives.
A third implication is the need for research on some important outcomes. None of the included studies assessed interventions targeting teenage pregnancy, dental health or examined potentially harmful or undesired effects. Studies that highlight cost-effectiveness are also few. Future controlled trials should include these outcomes.
There are limitations of this study. First, because of the methodological and clinical heterogeneity of studies, and a lack of information on sample characteristics, implementation quality, and program fidelity, we choose not to perform meta- and moderator analyses to compare specific intervention to SAU.
Second, a complication is that research on foster care populations frequently mix target groups. For instance, children in nonrelative foster family care are sometimes mixed with children in kinship care. Including those studies would cause increased heterogeneity in the results since kinship care has been reported as superior when it comes to children’s psychological health (Winokur, Holtan, & Batchelder, 2014). Another example is that comparison groups may include both children in foster care and in residential care, where the latter have elevated risks of externalizing problems compared to peers in foster family care (Strijbosch et al., 2015). To handle the dilemma with heterogenous populations, we decided that studies were only included if the experimental or comparison group contained less than 30% of children in kinship care and/or residential care.
Third, the choice of minimum follow-up time for studies to be included in the review was 1 month posttest for children younger than 2 years and 3 months for children 2 years or older. This may be considered rather short for attempts to estimate effects. However, most studies had a comparably longer follow-up time (Table 1).
In sum, this systematic review provides new insights and hope into the field of systematic interventions for children in foster care. The review found support for the efficacy of three interventions: ABC, Incredible Years Parenting Program, and Take Charge. The results also suggest that most systematic intervention programs included in this review produced positive effects. Due to a high methodological variation, available data do not permit any sound conclusions about what programs are superior to others. Ethically, social care organizations should prioritize implementation of services that have empirical support from research but also strive to initiate and encourage evaluations of new programs to gain knowledge about effects and side effects. Such research should at the same time consider and clarify ethical challenges.
Supplemental Material
Supplemental Material, Supplement_bilaga-4-sokstrategier - Interventions in Foster Family Care: A Systematic Review
Supplemental Material, Supplement_bilaga-4-sokstrategier for Interventions in Foster Family Care: A Systematic Review by Martin Bergström, Marianne Cederblad, Kickan Håkansson, Ann Kristine Jonsson, Christian Munthe, Bo Vinnerljung, Ingegerd Wirtberg, Pernilla Östlund and Knut Sundell in Research on Social Work Practice
Footnotes
Authors’ Note
This systematic review is a part of project by the Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU). Supplemental data for this article can be accessed on SBU’s website: excluded articles (Online Appendix 2) and search terms (Online Appendix 4; https://www.sbu.se/sv/publikationer/SBU-utvarderar/insatser-for-battre-psykisk-och-fysisk-halsa-hos-familjehemsplacerade-barn/).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.