
Abstract
This review examines key factors, both established and lesser known, driving the resurgence of pneumoconiosis in central Appalachia, the region with the highest disease incidence in the United States. It synthesizes findings from peer-reviewed literature and grey sources, including government reports, focusing on underground coal miners in the region. Four key factors are identified: historical economic trends, geologic conditions, technological changes, and health monitoring participation. The shrinking mining workforce has reduced operational size but increased productivity, raising individual exposure to respirable dust. Extensive mining has depleted accessible coal, forcing operators to mine adjacent rock layers, which increases exposure to toxic silica in dust. To maintain production, risky practices such as slope mining, new cleaning techniques, and powerful mining machines are being adopted, generating higher dust concentrations and smaller particulates, further exacerbating exposure. The presence of quartz-bearing formations also contributes to hazardous conditions. Finally, low participation in health screening programs disrupts disease detection and protective efforts.
Chronic occupational exposure to respirable coal mine dust (RCMD) has long been associated with a variety of debilitating diseases. One longstanding, completely preventable disease unique to the mining occupation is Coal Worker's Pneumoconiosis (CWP), commonly known as black lung disease. 1 Additional insight into CWP disease characteristics and historical prevalence can be found in the supplemental information (SI). RCMD consists of small particles that can be deposited into the distal airways and gas-exchange region of a miner's lung.1,2 Both shape and size affect deposition into the respiratory tract. Many constituents of coal mine dust are solid particle aerosols formed by mechanical disintegration of parent material (i.e., coal and surrounding rock), due to such activities as crushing or grinding. 3 These include: coal, mined rock adjacent to the coal seam, rock-dusting products, crystalline silica (quartz), and others. However, not all constituents of RCMD are formed by mechanical disintegration. For example, particulate matter from diesel exhaust is formed by combustion. 2 Some components of RCMD are known to be carcinogenic or otherwise toxic. Their health effects include heart or lung disease. 4
Likely due to the successes of the safety provisions established by the Coal Act of 1969, the several decades following its passage saw a significant decrease in the prevalence of CWP in underground miners with mean tenures over 25 years. Rates fell from over 30% in 1970 to about 5% in 2000. 5 However, around the turn of the twenty-first century, an unexpected rise in CWP cases became apparent among underground U.S. coal miners, with a pronounced increase in illness in the Appalachian Mountains, particularly in central Appalachia. 6 To understand some of the reasons for this increase in disease incidence, the National Academies of Sciences, Engineering, and Medicine (NAS) produced a comprehensive report in 2018. In addition to the explanations it provided, the report recommended further investigation into a variety of problems facing the mining industry. This literature review attempts to fill information gaps identified in the 2018 NAS publication entitled Monitoring and Sampling Approaches to Assess Underground Coal Mine Dust Exposures. 7 Specifically, we examine key areas highlighted in the report, including advancements in mining technologies and practices, the characterization of RCMD, medical surveillance programs, and barriers to the implementation of such programs. The review is framed around the report's recommendations: Recommendation 8, which calls for systematic evaluation of changes in mining technologies and practices to determine their role in increased rock extraction and disease hot spots; Recommendation 9, which emphasizes the need for comprehensive characterization of RCMD, including its chemical composition, particle size, shape, and crystalline silica content; Recommendation 10, which urges the development and validation of improved measurement technologies for more rapid and reliable real-time monitoring of harmful dust constituents; and Recommendation 11, which highlights the importance of strengthening medical surveillance programs by expanding participation, enhancing periodic health examinations, and better linking surveillance data to exposure and monitoring records.
The central Appalachian coal fields are typically associated with portions of eastern Kentucky, western Virginia, southwest West Virginia, and, in older epidemiological studies, northern Tennessee. Antao et al. (2005) were one of the first to describe this region as a “hotspot,” noting a clear trend of rapidly progressive CWP cases at higher rates in eastern Kentucky and western Virginia, compared to other US mining locations. In Central Appalachia, coal miners with ≥ 25 years of tenure show disproportionately high prevalence of CWP, while increases are also observed among miners with shorter careers. The 25-year threshold is widely applied in surveillance studies because it approximates a full mining career, allowing for comparison of disease risk between lifetime-exposed miners and those with fewer years of underground work. 8 Studies have shown central Appalachian miners to be subject to a more rapid onset of CWP,6,9 increased prevalence of primary myelofibrosis (PMF),10,11 years of potential life lost attributed to CWP, 12 and a rise in federal black lung disability compensation claims. 13
From the 1980s through the early 2000s, there was an eightfold increase in the proportion of central Appalachian coal miners with radiographic patterns consistent with silica exposure; during the same period, this measure did not change for the rest of the country.8,14 Silica is considered to be a potential determinant for the recent CWP resurgence. From 2006 to 2015, Central Appalachia accounted for 75% of all reported CWP cases in the United States.15,16 In 2015, PMF among long-tenured miners in central Appalachia was above 5%, the highest rate ever recorded. An epidemiological study found that between 1999 and 2016, the states of Kentucky, West Virginia, Virginia, and Pennsylvania accounted for 78.3% of all CWP deaths among persons aged 25 to 64. 17 In the same states, there was an 8.6-fold increase in the prevalence of PMF when comparing disease prevalence in the two-time intervals, 1994–1998 and 2008–2012, respectively. According to Coal Workers’ Health Surveillance Program (CWHSP) data, 18 as of 2018, the national prevalence of CWP in long-tenured miners exceeded 10%, and 20.6% of long-tenured miners in central Appalachia had been diagnosed with CWP. The national increase in CWP prevalence is largely attributable to the high rates in central Appalachia, where CWP prevalence is four times higher than that of long-tenured underground miners in other regions of the United States. CWHSP collects data continuously and frequently reports trends using five-year summary intervals. The most recent period with publicly available data is 2010 to 2014. For that period, Central Appalachia made up 39.4% of all underground mining in the United States but accounted for 57% of all CWP cases. In the same period, 12.7% of central Appalachian underground miners sampled in the CWHSP had CWP.19,20 Based on NIOSH CWHSP data sorted by Mine Safety and Health Administration (MSHA) regional mining districts, Figure 1 depicts the definitive rise in CWP diagnoses in Central Appalachia (MSHA districts 4, 5, and 12) compared to all other MSHA districts (2, 3, 7, 8, 9, and 10). 15
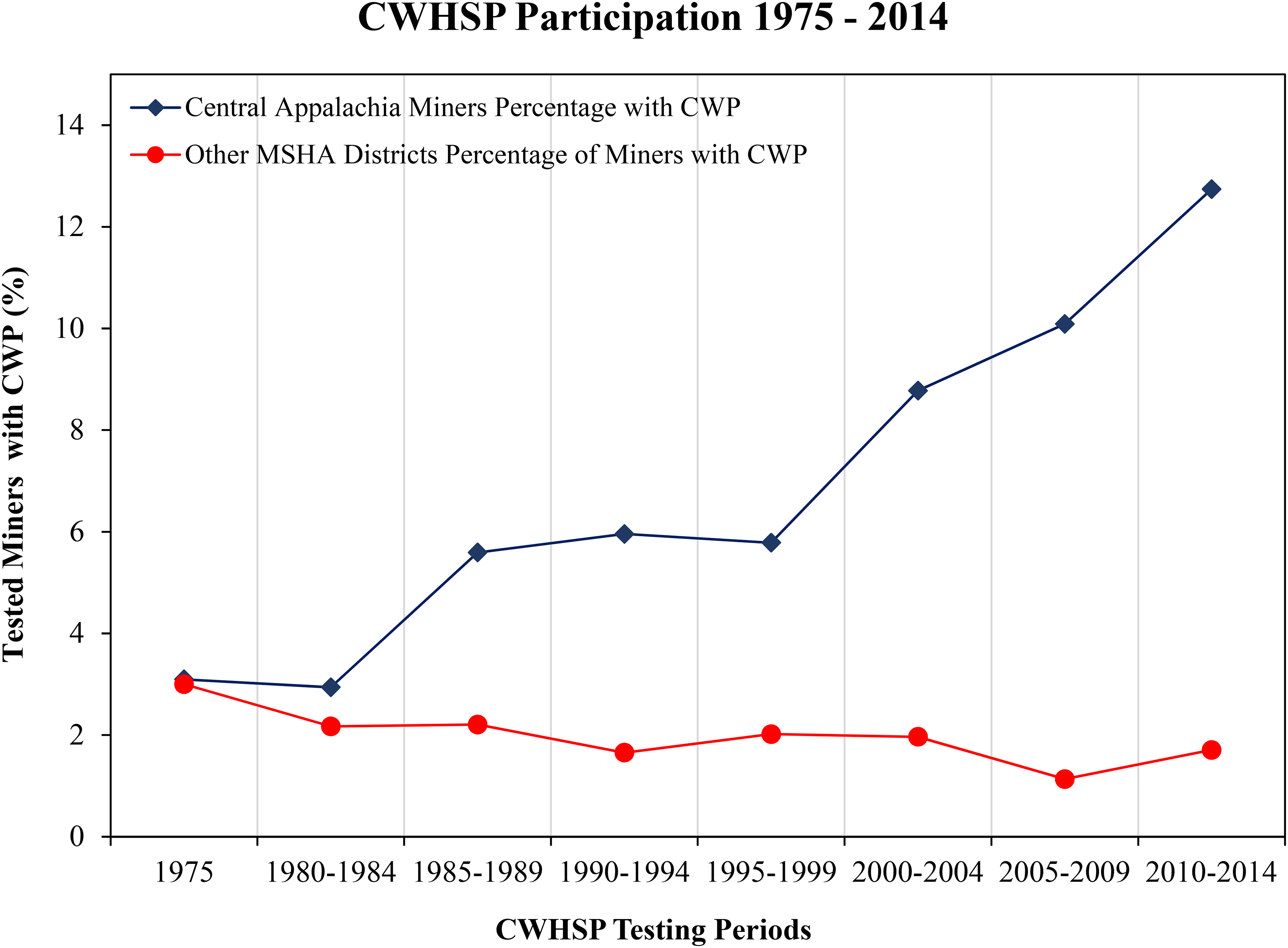
Comparison of CWP incidence in Central Appalachian Districts with other MSHA districts.
This review primarily investigates the potential etiologic factors of CWP in central Appalachian underground coal miners. Compared to surface miners, underground workers tend to have a higher prevalence and severity of CWP 21 due to elevated respirable dust concentrations in the underground environment. 22 Yorio et al. (2018) found that underground coal mines had an approximately 8.00 (IRR, Model 1) to 9.78 (IRR, Model 2) times higher probability of reporting a case of pneumoconiosis during 2006–2015 compared with surface coal mines. 16 Notably, the rise in severe disease in Central Appalachia has occurred alongside a regional shift toward surface mining.10,23 Importantly, more data is becoming available for these types of miners since surface miners were recently (as of 2014) included in federal medical surveillance. 24 For example, a 2020 study found that surface miner CWP prevalence in central Appalachia was 4.2 times higher (CI: 2.9–6.2) compared with the rest of the country. 25 These findings suggest that region-specific factors are contributing to the disproportionate increase in pneumoconiosis incidence in Central Appalachia. In particular, geologic conditions such as thin coal seams with high silica content, dust-intensive mining practices, and operational characteristics like smaller mines with limited dust-control resources have all been implicated as potential contributors.
A synthesis of published research, data, and grey literature (i.e., government documents, reports, or policy literature) is utilized to describe the possible reasons for the observed increases in CWP cases among underground miners in Central Appalachia. This report summarizes both well-documented and lesser-known potential determinants of Central Appalachian CWP, in addition to new information that has arisen since the 2018 NAS report. Since the latency period between initial exposure and diagnosis can take many years, the following was considered in the review: historical shifts in economic factors, unionization trends, mining technology and practices, mine type, geology, worker employment, and CWP prevention methods. To date, this is the first literature review that aims to elucidate potential etiologic factors associated with the recent CWP resurgence in underground miners, specifically in Central Appalachia.
Methods
Literature Search Strategy
This literature review article was guided by the recommendations provided in the 2018 NAS, which provided a framework for examining critical areas in coal mine dust research, including changes in mining technologies and practices, characterization of RCMD, development of improved measurement and monitoring methods, and strengthening medical surveillance programs. A comprehensive search was conducted using academic search engines, including Google Scholar, PubMed, JSTOR, and ScienceDirect, to access peer-reviewed journals and technical documents. The key search terms used in these databases are listed in the Notes. a Additionally, grey literature was sourced through local search engines on government websites, including MSHA, EIA, CDC, and various state web pages. The grey literature collected included federal agency reports, CWHSP data (in Excel format), public requests, legal settlements, and state legislation.
Inclusion and Exclusion Criteria
A total of 204 articles were identified through database searches. After applying the inclusion and exclusion criteria, 111 articles were selected for this review. The methodology for selection is outlined in Figure 2, illustrating the specific inclusion and exclusion criteria. Only documents published in English were included, with no restrictions on the type of study, report, epidemiological design, or country of origin. While there were no restrictions on publication date, the most recent research and data were prioritized when available.
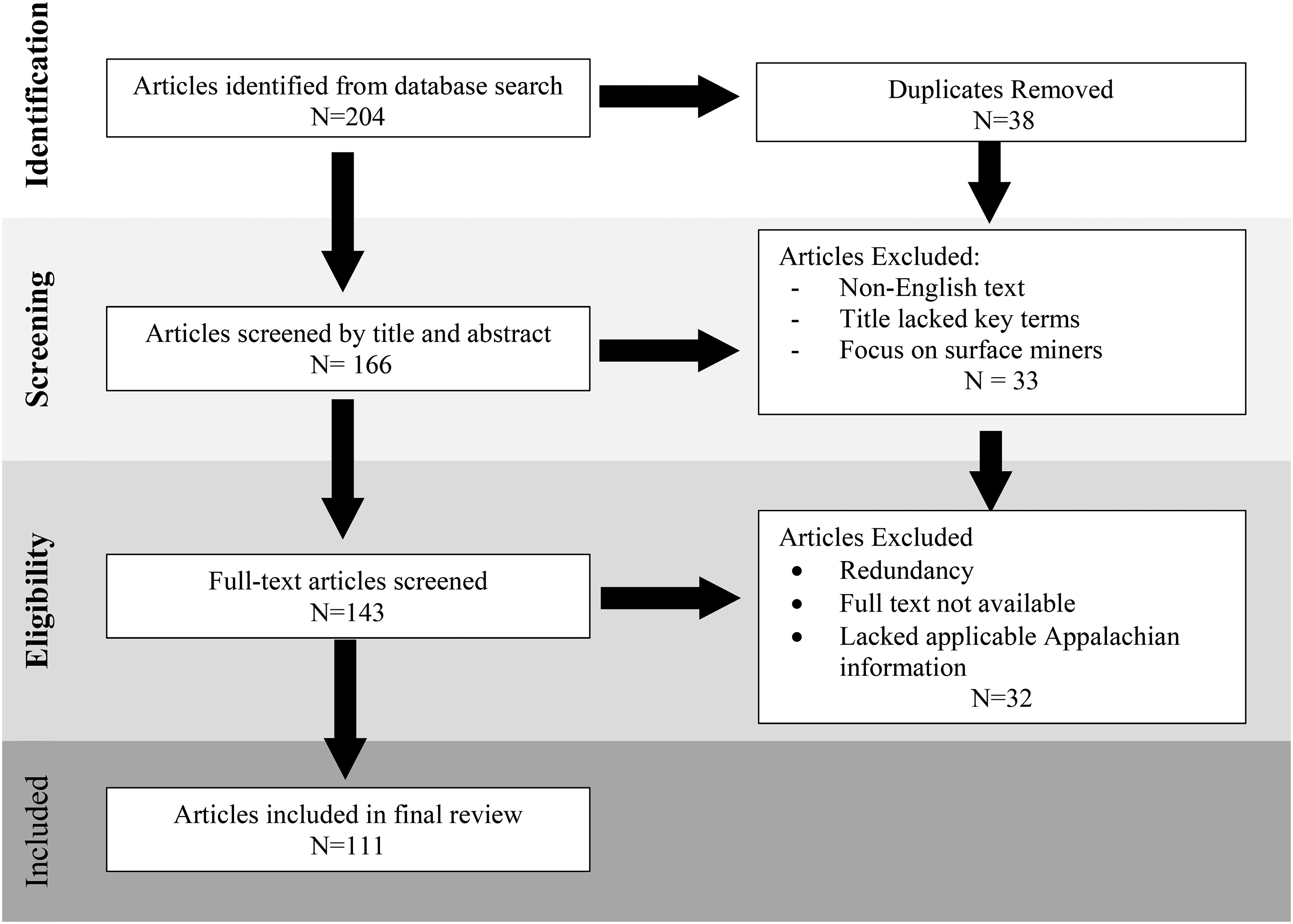
Inclusion and exclusion criteria framework used in the present review methodology.
Data Extraction and Synthesis
Data extraction was performed by two scientists (Yi-Hsuan and John-Paul), focusing on key elements such as study design, sample size, outcomes, and other relevant findings. The extracted data were organized by thematic areas, allowing for the identification of patterns and trends in the literature. The review process was conducted by the whole group, with discrepancies resolved by consensus. Visualizations of key data were created using Microsoft Excel to present relevant figures and results.
Results and Discussion
US Mining Economy and Labor Productivity
Given CWP's long latency period, typically over 10 years, with some studies indicating over 20 years, it is necessary to evaluate historical changes in the mining economy.26,27 The consolidation of mining companies has contributed to a continuous decline in the number of mines, the number of miners employed in those mines, and the size of the operations. Beginning in the second half of the 20th century and continuing until peak production in 2008, American coal mines as a whole witnessed an overall reduction in employment while seeing an increase in overall short tons mined. 28 Compared to 1980, in 2005, coal production was 33% higher (>1,100 million tons), with 70% fewer mines (1,600 mines total, 650 underground mines, and 950 surface mines) and 50% fewer miners (105,000). There were also sharp overall gains in US miner labor productivity (based on short tons/miner day), as much as an estimated 6.6% annual increase from 1980 to 1995. 29 MSHA found that from 1978 to 2007, hours worked (per miner) in underground coal mines increased by 25.6%, approximately 1800 to 2400 h per worker per year. 30 As of May 2021, full-time coal miners worked an average of 49.6 h per week. 31 Hypothetically, working a 10-h shift in the mine leads to 25% more dust entering the lungs compared to a regular 8-h shift (assuming all other factors are equal) and less time for dust to be cleared from the respiratory tract.
Although CWP remains most prevalent in Central Appalachia, broader trends in mining production and workforce dynamics may be contributing to the nationwide increase in CWP incidence. 32 The MSHA permissible exposure limit (PEL) for coal dust, 1.5 mg/m3 (when silica concentrations are less than 5%), is based on an 8-h time-weighted average. 33 For shifts longer than 8 hours, compliance is determined by sampling the worker for the entire shift, with airborne dust concentrations not exceeding 80% of the PEL to account for the extended exposure period. For example, during a 10-h shift, dust levels must remain below 1.2 mg/m³ to be in compliance. As miners are increasingly working longer hours, maintaining exposures below the adjusted PEL may be more challenging, potentially increasing the risk of CWP.
According to information provided by the US Energy Information Administration (EIA), Central Appalachia in 2019 had more active underground mines than any other MSHA region in the country and employed the most underground miners, accounting for over a third of the nation's underground mining force (10,918 out of 31,881). Specifically, Central Appalachia, which includes parts of Kentucky, Tennessee, Virginia, and West Virginia, produced 13,945 thousand short tons of coal in 2019. 34 Due to greater RCMD exposure in underground mining, the greater share of underground miners in Appalachia compared to the rest of the country may be contributing to the higher incidence of CWP. Additionally, an increase in miner productivity and hours worked is thought to be associated with greater RCMD exposure and an increased likelihood of developing CWP. 35
Mine Size and Union Status
Due to a history of aggressive mining in central Appalachia, coal production and employment in the region have generally declined since the 1980s, resulting in smaller mining operations, even as national production increased during parts of this period. 36 The central Appalachian states of Kentucky, West Virginia, Virginia, and the greater Appalachian state of Pennsylvania account for most of the nation's small underground mines (defined as ≤50 active employees). 7 In 2008, 262 out of 373 (70%) active underground mines in the Appalachia region had fewer than 50 workers. In 2010, the median number of employees per mine was 73 in central Appalachia compared to 273 workers per mine in the other regions. 37 Compared to larger mines, small mines have been shown to be a more hazardous workplace with a greater number of injuries 38 and exhibit a wider variety of dust conditions with a tendency to exceed applicable dust standards. 39
A 1990s sampling exercise conducted by MSHA showed an increasing trend in dust levels with decreasing mine size. 35 More recently, it has been shown that miners working in smaller operations were more likely to be affected by CWP than those in larger workplaces.40,41 Compared to large mines, small mines were found to have a five times higher likelihood of PMF prevalence 13 and a two times higher likelihood of having CWP. 41 Indeed, it appears the abundance of small mines in Appalachia is associated with coal mine lung diseases (CMLDs), CWP, and impairment of lung function in Appalachian miners. 41 Several reasons have been proposed to explain why small mines in Appalachia are more dangerous: lack of safety resources, fewer dedicated environmental health staff, older equipment, generally younger (less experienced) employees, and excessive exposure to silica and mixed RCMD due to increased likelihood of thin seam mining. 13
Additionally, in 2019, central Appalachia accounted for 10,278 out of the total 24,820 (41%) non-unionized underground miners. The entire Appalachia area accounted for 64% of all non-unionized underground miners. 34 Anecdotal evidence and interviews suggest that unionized mines placed a stronger emphasis on safety and adherence to exposure limits. Empirical studies support this, showing that union presence is associated with significant reductions in workplace fatalities and injuries. 42 Evidence also indicates that union certification strengthens enforcement of workplace-safety regulations, promoting compliance and safer working conditions. 43 International research reinforces these findings, demonstrating that unionized workers tend to experience better occupational safety and health outcomes. 44 Personal accounts indicate that from the 1980s onward, a weakening of coal miners’ unions undermined protections established by the Coal Act, leaving workers more vulnerable. 45
Central Appalachia Mine Geology: Seam Size, Silica, and Coal Rank
Appalachia has been a major source of coal production in the United States for over a century, leading to the depletion of large, easily accessible coal seams. Consequently, the remaining coal deposits are typically found deeper underground and within thinner seams.46,47 Thin seam mining increases the chance for rocks and minerals other than coal to be mined, including quartz-bearing rock.48,49 Central Appalachia has smaller average coal seam heights than all other MSHA districts. 31 For example, the Powder River basin in Wyoming has coal seams more than 100 feet in certain areas and located near the surface, which is well-suited for large-scale strip mining. 50 Such large coal seams allow mine operators to use large, highly efficient mining machines. Notably, 96% of US mines with thin seam mines are located in the Appalachian states of Kentucky, Virginia, and West Virginia. 51 Therefore, the prevalence of thin seam mining in Appalachia provides a plausible explanation for higher exposure to silica, a human carcinogen, in regional RCMD.
Although the dust produced by mining large amounts of rock strata potentially exposes miners to a wider range of harmful constituents, the average RCMD concentrations between 1989 and 2018 across all mining regions (including Appalachia) have declined according to regulatory compliance measures. 52 These data suggest that RCMD composition and the characteristics of mine geology may be more important etiologic factors with regard to the increase in disease than RCMD concentrations as a whole. In contrast, respirable crystalline silica concentrations in Central Appalachia have consistently exceeded the PEL over the past 30 years, and silicosis can occur even at exposures below the regulatory limit.52,53 Compliance samples, while useful for regulatory monitoring, may underestimate actual occupational exposures, as sampling often occurs under average conditions, may not capture peak dust events and do not reflect variations across different work tasks or shifts. Therefore, readers should interpret compliance data with caution: although overall RCMD concentrations appear to have declined, silica exposures may have remained elevated or even increased in thin-seam mining, highlighting a persistent risk for pneumoconiosis and silicosis despite regulatory compliance.
The location of a mine determines its mineralization or ore quality. Different mining regions have been shown to vary significantly regarding mine dust components. 54 In the case of central Appalachia, the underlying sandstone formation in eastern Kentucky is composed of more than 90% quartz. 55 The region has had the highest number of PEL violations for silica, and from 2006 to 2015, nearly half (49%) of all US coal mines in violation of the silica PEL and on “reduced standard” were found in central Appalachia.15,49 Between 1982 and 2017, the geometric mean concentration and mean percentage for respirable quartz were significantly higher in central Appalachia compared to the rest of the United States. 15 There appears to be an inordinate amount of dust generated from cutting rock strata, which are the layers of rock above, below, or interspersed with coal seams. 56 The most recent studies show that central Appalachian mines have the highest percentages of silica and aluminosilicates from rock strata. 54 One 2020 study found a significantly higher percentage of silica particles in the lungs of modern deceased miners (born after 1940) with PMF compared to historical samples (born before 1940). 57 This is an important finding: although silica has always proved to be an occupational mining hazard, modern CWP and PMF in the Appalachian region are thought to be more closely tied to silicosis lung pathology. 12 With confidence, silica-laden dust is thought to be a main driver in the resurgence of CMLDs, CWP, and PMF in the Appalachian mountains.14,15,18,58,59
Another potentially important geologic feature regarding Appalachian CWP is coal rank. Coal rank indicates the progressive geological alteration and thermal maturation from the lowest rank, lignite, to sub-bituminous to bituminous, followed by the highest rank, anthracite, reflecting both the energy content and carbon concentration of the coal. 2 As of 2023, the Appalachian region remains a major source of U.S. coal, contributing a substantial share of the nation's bituminous coal production.60,61 High coal rank has been shown to potentially be a risk factor in the development of CWP disease because bituminous and anthracite coals are harder and more brittle, producing finer, more respirable dust with higher crystalline silica content than lower-rank coals.6,62–66 A mine's geology ultimately determines the components found in its dust. As discussed, the natural geology of the central Appalachian region, coupled with very thin coal seams that require surrounding rock strata to be mined, creates a situation in which miners are exposed to disease-causing constituents, particularly silica, that are unique to central Appalachian mines. While the geology of central Appalachia likely contributes to the resurgence of CWP, the technologies and practices used in coal mining (and the production of RCMD) remain less researched but may be equally important in influencing dust generation and worker exposure.
Mine Technology and Practices
Modern mine technology is highly productive. Advances in mining equipment have yielded more powerful cutting machines for coal production activities, which are likely to generate greater amounts of dust and smaller (i.e., sub-micron) particles that can penetrate deeper into the lungs than larger-sized RCMD.67,68 Recent changes in mining technology are of particular importance since most of the recent (1999–2016) CWP deaths (68%) came from mining machine operators. 17 Also, miners with rapidly progressive CWP were significantly younger than other miners with CWP, 33 suggesting that more recent changes in mining technology and work practices may be contributing to accelerated disease progression. The use of more powerful cutting machines, increased production demands, and higher exposure to fine respirable coal mine dust and sub-micron silica particles may be creating conditions in which younger miners are developing severe disease in a shorter timeframe. This pattern contrasts with older cohorts, who typically experienced slower disease progression, and underscores the potential impact of modern mechanized mining operations on respiratory health.
In addition to advances in mining technology, changes in mining practices and techniques have further increased exposure risk. Coal separation and washing techniques that were developed in the 1990s are one of the examples. These techniques made it increasingly profitable to mine thin seams of coal and cut large amounts of rock. 14 In the 1970s, it would not have been feasible to cut a 6-foot-high section if 3 feet of that were rock. Modern separation techniques enable operators to cut rock and remove it from the coal after it leaves the mines. The new technology enables mining of thinner seams in the central and southern Appalachian coal fields. Nevertheless, mining greater volumes of rock exposes miners to higher concentrations of respirable crystalline silica and other mineral dust, which remain in the air during cutting and handling. Even though improved coal cleaning technologies reduce non-combustible content post-extraction, miners are still exposed to the dust generated during extraction. This increase in dust exposure directly contributes to higher risks of CWP and rapidly progressive forms of the disease among workers in these regions. 14
In 2018, researchers interviewed a group of Appalachian miners with large opacities exhibiting PMF (defined as opacities >1 cm). Most interviewees reported cutting substantial amounts of rock and sandstone with continuous mining machines. 69 This study highlighted the dangers of a recently adopted practice, known as “slope mining,” that may contribute to lung disease in central Appalachian miners. In slope mining, mechanized mining units (MMUs) operate continuous miner machines, designed to cut coal and other soft rock. They cut shafts through hundreds of feet of sandstone to reach underground coal seams. Slope mining greatly increases the chance for miners to be exposed to higher concentrations of respirable silica and other dust components besides coal. 70 Additionally, the miners in the study reported a failure to control RCMD concentrations due to inadequate ventilation and deliberately manipulated sampling strategies, indicating dust concentrations lower than reality (e.g., placing dust samplers in clean air intakes).
Two dominant types of modern mining machines, longwall and continuous miners, are not originally designed for rock cutting, though retrofits have enabled this capability. However, the increase in mining equipment horsepower has yielded machines that can easily cut rock to access remaining coal beds, which have become increasingly thin, potentially exposing workers to smaller, more harmful dust particles. 68 This type of rock cutting results in greater wear and tear on the machines and cutting heads, which can lead to greater dust generation. 71
CWHSP Participation and Secondary Prevention Measures
Powerful machines, along with the current dominant hazardous mining practices, have changed the way coal is extracted in the Appalachian region, which may be leading to deleterious working conditions that were not of concern a few decades ago. The CWHSP has made it possible to correlate temporal changes in mining practices with localized CWP incidence. Therefore, participation in the CWHSP is an essential tool in the timely detection of pneumoconiosis and the implementation of necessary mitigation strategies.
Secondary prevention measures consist of conducting medical screenings that attempt to detect disease at an early stage to establish eligibility for a job transfer program designed to reduce worker exposure to respirable dust and reduce respiratory disease progression. The NIOSH-operated CWHSP approves medical facilities to perform lung function tests, chest radiographs, and respiratory assessment questionnaires according to national and international standards. 72 If a miner is found to have evidence of CWP, they are legally able to transfer to a less dusty part of the mine and still retain the same benefits of the previous position. This transfer program, operated by MSHA, is known as the Part-90 option. 73 CWHSP and Part-90 are separate programs operated by different organizations, yet they work closely together to ensure the protection of coal miners’ health. The CWHSP participation is generally mandatory upon entry into the mining industry and voluntary every four or five years thereafter, whereas the Part-90 program is completely voluntary. Both programs have had historically low participation.7,24,74
Based on the number of radiographs, central Appalachian miners consistently have the lowest participation rates in the CWHSP compared to other MSHA districts. 19 According to the most recent CWHSP data, from 2010 to 2014, out of the 18,906 estimated miners in central Appalachia, only 1,821 participated in CWHSP chest radiograph surveillance, a 9.6% participation rate. During the same period, the remaining MSHA districts had about a 45% participation rate, 12,954 out of 29,102. Looking at the periods between 1975 to 1979 and 2010 to 2014 (see Figure 3), the overall CWHSP participation in all MSHA districts decreased from 66% to 30%, respectively. Looking at central Appalachia specifically, the CWHSP participation rate decreased from 68% to less than 10%. Since screening for CWP in underground miners is so low in central Appalachia, it is thought that the true prevalence of the disease is understated.70,75
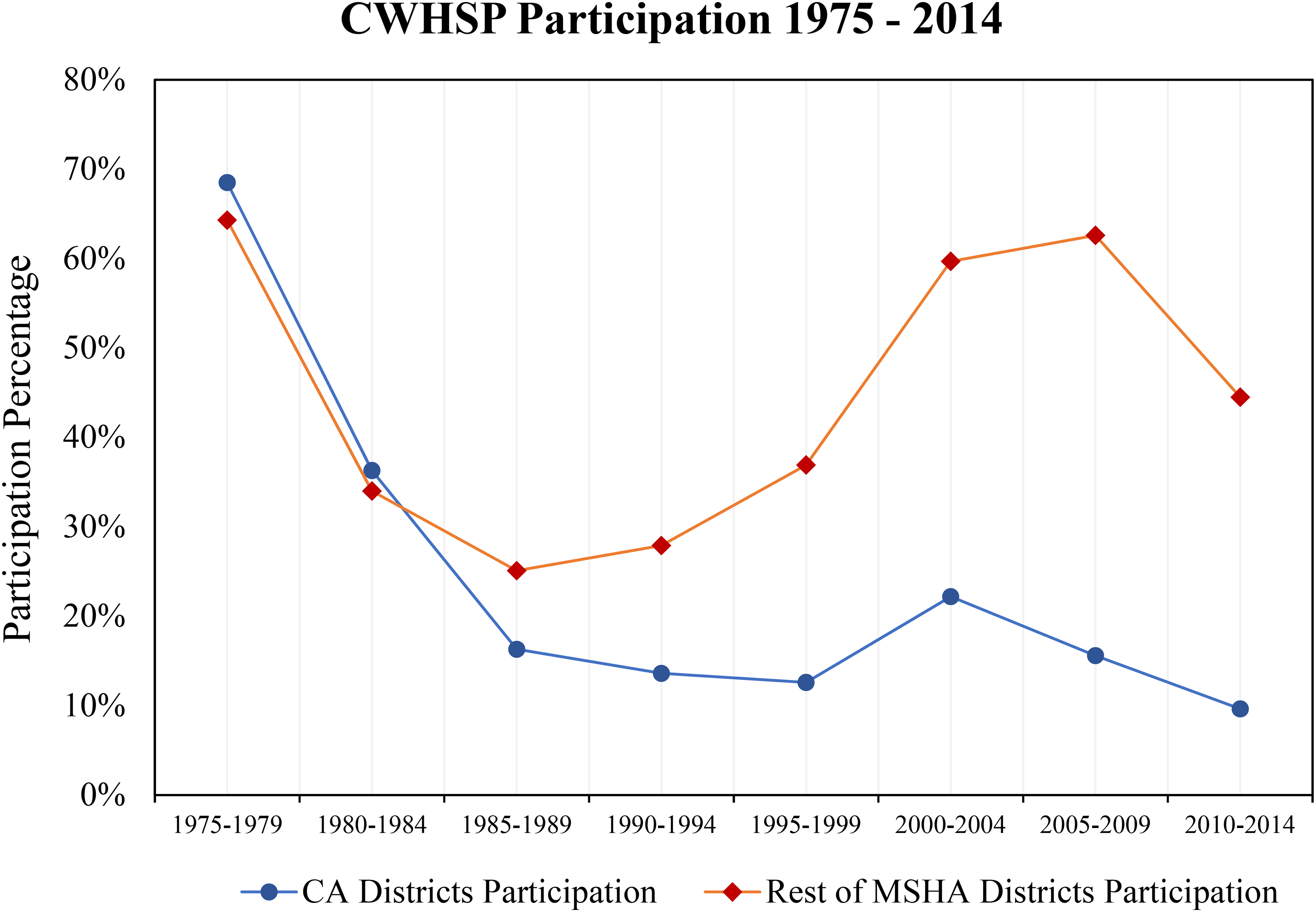
Participation in CWHSP: Central Appalachia (CA) compared with other MSHA districts.
Utilization of the Part-90 option is also not a common practice. Only 12.6% (513 out of 4077) eligible miners participated in the Part-90 job transfer option between January 1981 and November 2016. 76 Miners from central Appalachia were the least likely to utilize the Part 90 option, despite this area having the highest disease prevalence. 77 Miners exercising the Part-90 option in central Appalachia had longer mean tenures than those working outside this region (25.8 years vs. 20.0 years), suggesting that miners in Appalachia tend to wait until later in life to utilize the Part-90 option. 69 Central Appalachian miners, compared to miners working in other states, were statistically less likely to exercise their Part-90 option (13.1% vs. 17.4%). 78 Such findings suggest that region-specific disincentives and barriers may exist that reduce participation and the effectiveness of secondary prevention strategies.
Barriers to CWHSP and Part-90 Participation
In 2018, through a public request for information (RFI) posted to the Federal Register (Docket CDC-2018-0110), NIOSH solicited feedback regarding barriers to participation in the CWHSP. Responses from a diverse range of stakeholders, including representatives from industry, medical organizations, and labor groups, were collected and posted to the CDC's online docket. Key concerns identified from these submissions, along with other publications, include privacy issues, fears of job loss or reprisal, limited access to testing facilities, a shortage of approved testers, inefficiencies in state and federal workers’ compensation systems, concerns about inaccurate diagnoses, and potential damage to personal and professional reputations.79–81
Fear of job reprisal, economic loss, and a lack of privacy are consistently cited, both in scientific and grey literature. Linking compensation and health surveillance data of US miners, one study surprisingly found that a large portion of miners (39%) did not apply to the CWHSP and thereby missed opportunities for secondary prevention. 82 State legislation can disincentivize early detection through laws that provide a narrow window of time for miners to file workers’ compensation claims in the case of diagnosis. For example, in Kentucky and Virginia, certain codes dictate that a miner with CWP must notify their employer within a short period (i.e., < 60 days for Virginia) of their diagnosis. 81 The notification and filing requirements in Kentucky and Virginia originated from historical efforts to balance workers’ compensation coverage with employer protections. In Kentucky, the Workers’ Compensation Act of 1972 required miners to notify their employers within a short period after an occupational disease diagnosis, including CWP. Similarly, Virginia's workers’ compensation laws established a 60-day notification period to provide employers with prompt notice of potential claims. These laws have created barriers for miners seeking early diagnosis and participation in surveillance programs, as workers may fear job loss, reduced income, or career disruption if they report disease too early.
Additionally, in the case of central Appalachia, there is a dearth of approved radiograph screening testers. Under current law, only physicians who obtain certification as a “B Reader” are capable of classifying chest radiographs for the CWHSP. This limitation becomes even more significant in light of the 2018 Kentucky workers’ compensation law (House Bill 2), which prohibits miners from using chest radiograph evidence of CWP if the interpretation is done by a radiologist.83,84 Instead, this law requires that such evidence be provided by a pulmonologist. House Bill 2 was enacted amid rising rates of black lung disease in central Appalachia. It standardizes diagnoses by relying on physicians with specialized training in lung disease. In doing so, it has restricted access to qualified testers, as radiologists who are equally trained in interpreting chest radiographs are excluded. As of 2019, there were only approximately 10 NIOSH-certified B Readers, comprising six radiologists and four pulmonologists in the entire state of Kentucky. 85 In the case of Kentucky, the lack of B Readers creates a challenging situation in which it is difficult for miners to be diagnosed with occupational lung disease, successfully file workers’ compensation claims, and secure benefits. Moreover, in central Appalachia, the lack of B Readers is compounded by limited access to testing facilities, which directly hinders both disease surveillance and data collection. Given the region's largely rural and isolated nature, miners are often required to travel long distances to reach testing sites. To make matters worse, miners typically are not compensated for these trips and may need to take time off work to access testing, further creating barriers to timely diagnosis and claims filing. 81 Fortunately, recent developments by the U.S. Department of Labor's Office of Workers’ Compensation Programs (OWCP) may help address some of these challenges. In 2014, the OWCP announced a final rule allowing both film and digital chest X-rays to be recognized equally in claims adjudication under the Federal Black Lung Program. In December 2024, OWCP implemented additional measures requiring self-insured coal operators to post full security for their black lung benefit liabilities, ensuring that miners’ benefits are fully funded. These updates also streamline the appeals process, setting clear timelines for documentation and decision-making. Although this change helps streamline the process and reduces the burden on miners to find facilities with outdated equipment, access to trained professionals, and affordability issues remain critical concerns.
Job reprisal in the mining workplace is a real threat that creates additional barriers to the utilization of secondary prevention programs. Unlike the compulsory program applied in other countries (e.g., Australia), the voluntary nature of participation in the CWHSP causes a significant challenge in identifying cases in the US. The Appalachian Citizens’ Law Center, which often represents miners, suggested that a history of discrimination against Part-90 participants leads current miners to forego using surveillance programs to avoid even receiving a Part-90 election letter from NIOSH. 86 Miners with CWP, considering the Part-90 option, may be forced to choose between a lucrative job with potential salary advancement and their health. 87 Privacy concerns driven by fear of employer retaliation lead miners to elect Part-90 status only near the end of their career.24,86,88 Until recently, protections for miners’ personal and medical information were limited primarily to confidentiality policies under the CWHSP and federal workers’ compensation regulations. While these policies restricted employer access to health data, miners often remained concerned that participation could negatively affect their employment or career advancement. In December 2024, updates by the OWCP and broader federal and state privacy regulations have nominally strengthened protections for miners’ health and personal data. However, enforcement gaps, inconsistent compliance, and documented violations of existing privacy laws by the Department of Government Efficiency (DOGE) 29 mean that these protections remain uneven in practice, and miners may still face risks of employer reprisal or loss of confidentiality.
Despite these potential barriers being more likely to result in underestimation of disease prevalence in the population, other authors and the responses collected by the NIOSH CDC's public RFI provide some solutions to increasing participation in secondary prevention programs, as highlighted in the recommendations below. Additionally, NIOSH recently executed several mine projects to address the underestimation and avoid a higher silica exposure level.
Recommendations
Mandatory engagement in secondary prevention programs has been proposed by MSHA as a potential solution to address low participation rates. 76 Changing participation in the CWHSP and Part-90 programs from voluntary to mandatory would increase earlier detection of respiratory diseases in the occupational population and eliminate many of the stigmas felt by proactive miners. 89 However, logistical concerns, economic constraints, regulatory challenges, and ideas of personal liberty oppose a legal mandate for participation.
The federal 1980 Part-90 update notes that if Part-90 participation does not increase soon, MSHA will reconsider the appropriateness of a mandatory transfer program. 89 Such action was never followed through, and participation rates continue to remain poor. In the case of Part-90 miners, the workers are legally entitled to the same wage rates they were offered in their prior position. Many miners often work overtime hours, which provides considerable wage bonuses. However, working in another part of the mine may not provide similar overtime and/or production bonus opportunities, creating a loophole situation that may safeguard worker health but decrease net pay for the Part-90 miner and stunt career progression.
On December 12, 2024, the Department of Labor promulgated reforms requiring coal companies to secure their Black Lung Disability Trust Fund liabilities and implemented procedural updates within the OWCP to streamline the self-insurance process, aiming to improve the feasibility of adopting these. 90 However, the implementation of these reforms was significantly disrupted by large-scale layoffs at NIOSH, which occurred without Congressional authorization. On April 1, 2025, the new administration dismissed the entire CWHSP staff 91 and temporarily stopped accepting requests for miner lung disease screenings. 92 Although many NIOSH staff members were reinstated within a month under political pressure, 93 fewer than 350 NIOSH employees were reinstated out of the approximately 900 who had been let go. This significantly reduced NIOSH's capacity for surveillance, data processing, and mobile testing, constraining the implementation of the new Black Lung reforms despite the partial restoration of CWHSP operations. 94
The reduction in staff and the resulting constraints on NIOSH operations have had lasting effects on program delivery. Consequently, while mobile CWHSP testing services continue to be available in some locations, coverage remains sparse, particularly in rural areas, and after-hours access is minimal. Participation in Part-90 has not meaningfully increased, as miners continue to face concerns about employer reprisal, confidentiality, and potential loss of income or career advancement. On the regulatory side, reforms requiring coal companies to better secure their Black Lung Disability Trust Fund liabilities have been implemented, ensuring long-term funding for miners’ benefits, but logistical and systemic barriers to surveillance and timely diagnosis persist.
If mandatory participation remains unfeasible, further investment in worker training programs must emphasize the purpose of CWHSP, the Part-90 option, and the associated health benefits of reduced exposure to respirable coal mine dust. 24 Additionally, the augmentation of NIOSH's mobile surveillance, which travels to different mine locations, can improve miner access to convenient CWP testing, reduce travel time away from work, and provide a screening service that is considered to be less intimidating than a doctor's office. 95 However, even maintaining mobile surveillance at its 2024 level will be a challenge, given the cuts to NIOSH. To address the shortage of NIOSH-certified B Readers, several steps can be taken to expand radiographic testing capacity. This includes reversing hostile laws such as those in Kentucky and allowing nurse practitioners and physician assistants to order, perform, and interpret diagnostic tests in daily practice.
Other suggestions to improve testing site access, documented in the various responses to the 2018 NIOSH RFI, include providing access to after-hour facilities, developing or certifying facilities in rural areas, and incentivizing CWHSP participation. Some ideas proposed for policy and practice improvements include reformation of the adversarial nature of black lung compensation claims (i.e., a sliding scale of benefits for miners with CWP diagnosis or changing the three-year filing window), and an increase in the coal excise tax to eliminate the Black Lung Benefits Trust Fund debt to secure funding for future claimants. 89
Conclusions
This review highlights four key factors that are likely contributing to the resurgence of CWP: historical economic shifts; mining conditions and geology; changes in technology and practices; and the insufficient participation and effectiveness of secondary prevention programs. Together, these factors and the specific subfactors outlined in the review are likely driving the concerning increase in pneumoconiosis cases among underground coal miners in central Appalachia. A deeper understanding of these etiologic determinants can provide insight to industry professionals, occupational health specialists, and policymakers to identify ways to improve current conditions and ultimately reduce the prevalence of the disease.
To improve working conditions for miners in Appalachia and the nation as a whole, investment in primary and secondary prevention measures is required. Primary prevention utilizes engineering, administrative, and personal protective equipment controls to reduce overall dust exposure. This also includes the development of real-time RCMD monitors that can distinguish between dust components, namely silica, which can help miners quickly detect dangerous levels of air contaminants and allow them to change operations accordingly to reduce worker exposure. Equally important is the uptake of suggested interventions made by industry experts to mitigate the barriers to participation in the CWHSP and Part-90 option. Focusing on private and government agencies to enhance the effectiveness of these secondary prevention strategies may result in timely improvement for Appalachian miners, as such actions will improve the accuracy of known disease prevalence and prevent further damage to miners with existing health conditions.
Overall, this systematic review is beneficial in investigating the primary root causes of the increase in CWP rate. The cause-and-effect relationship of CWP is a challenge to establish. Additionally, the prevention-control system is complex and dynamic in the US. Nevertheless, our cross-scope findings can provide a comprehensive understanding of potential etiologic factors of CWP in central Appalachian underground coal miners. Future studies are still needed to address this problematic, international, and high-priority occupational health issue.
Supplemental Material
sj-docx-1-new-10.1177_10482911251400417 - Supplemental material for Uncovering the Factors Behind Rising Pneumoconiosis Rates: Central Appalachian Underground Coal Miners as a Case Study
Supplemental material, sj-docx-1-new-10.1177_10482911251400417 for Uncovering the Factors Behind Rising Pneumoconiosis Rates: Central Appalachian Underground Coal Miners as a Case Study by Yi-Hsuan Chen, John-Paul Angulo, Jürgen F. Brune and Candace Su-Jung Tsai in NEW SOLUTIONS: A Journal of Environmental and Occupational Health Policy
Footnotes
Author Contributions
The manuscript was written through the contributions of all authors. All authors have approved the final version of the manuscript. Conceptualization and methodology: Y.H.C. and J.P.A. Investigation and formal analysis: Y.H.C. and J.P.A. Writing—original draft preparation: J.P.A. Writing—review and editing: Y.H.C. and C.S.J.T. Supervision: C.S.J.T. and J.F.B. Project administration: C.S.J.T. All authors have read and agreed to the published version of the manuscript. The contents are solely the responsibility of the authors and do not necessarily represent the official views of UCLA or the Colorado School of Mines. The authors thank Dr. Cara Halldin at NIOSH for technical advice, comments, and help with reference selection and data analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the financial support to Yi-Hsuan Chen by the Alpha Foundation for the Improvement of Mine Safety and Health, Inc. [grant number AFC820-43; Project title: The effect of coal and mine respirable dust size on lung cells and exposure assessment] and also acknowledge support to the trainee, John-Paul Angulo, provided by the Centers for Disease Control and Prevention [grant number 5T42OH008412-16] to Southern California Education Research Center.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.