
Abstract
We explored how Canadian academics manage their mental ill-health while at work and whether they do so informally, seek formal help or workplace accommodations, or take leaves of absences. Results from a survey of 342 academics (71% women) indicated that mental ill-health was common. A higher percentage of women reported having experienced mental health issues over their careers. Less than a quarter of those who experienced mental health issues took formal leaves of absence because they felt their issues were not severe enough to warrant leave. They were concerned about stigma and the impact that taking a leave would have on their colleagues’ workload. More often, respondents manage the occupational stressors themselves by using sick days and vacations to retreat from work, reduce their workload, and seek help from health professionals. Using this information, the authors recommend specific interventions for academics experiencing mental ill-health.
Introduction
Mental ill-health, particularly anxiety, depression, and burnout, is estimated to affect 17 percent to 20 percent of people in the workforce in any 12-month period and is a leading cause of absenteeism and sickness leave.1–6 Levels of stress, anxiety, and depression have been reported to be at least as common in academia as in the general workforce.6–8 Although the work-related factors that give rise to mental-ill health in academia have been examined,9,10 less is known about how academics manage the mental health issues that affect their ability to work. 11 Given that poor mental health for academics can have detrimental effects for research productivity, for students who may receive a lower quality educational experience, and for universities if faculty members are absent, 12 a better understanding of the strategies academics use when experiencing work-related mental ill-health is essential.
Managing Mental Ill-Health at Work
Taking steps to manage mental ill-health in an academic context is likely to be challenging for many. Just like many occupations, academics face high workload pressure, which contributes to a tendency to work when they are sick, 13 often with the belief that this is indicative of their dedication and commitment. 14 Academics tend to have a great deal of autonomy and flexibility to work when and how much they choose. For many, this blurs the boundary between work and personal time, eliciting guilt when resting or taking time away from work. 15 Rather than buffering the effects of stress, the autonomy and flexibility inherent to academia can make it more difficult for academics to prioritize improving their mental health in the context of heavy workloads and rising performance expectations. Individuals struggling with their mental health may not even recognize that they need to seek help or support because they may lack awareness of their limitations and their reduced capacity to focus on their work. 16
When academics acknowledge that their mental ill-health is negatively affecting their work, what can they do? Urbina-Garcia, 11 in a systematic review of research on academics’ mental health, found only three studies addressing strategies that faculty members use to face academic demands, all of which focused on individual coping behaviors. Based on findings of research on other professions, we believe that academics could have several informal and formal options to address their mental ill-health issues while working. The first option may be self-accommodation, that is, informally making changes to their work or approaching sources of support and assistance that they believe would be most effective for them 17 without involving the employer (i.e., the university). Potential changes might include, for example, reducing research output in favor of meeting teaching obligations or using sabbatical time to rest. Much academic work can be undertaken from locations other than the workplace. For some, working from home may allow them to hide their mental health issues and related reduced productivity from others in the university.
A second option that academics could use to manage their mental ill-health is to ask formally for accommodations from their employers. Accommodations are modifications to a job or a workplace intended to help overcome work performance limitations so individuals can perform the required tasks. 18 Reasonable accommodations for individuals with mental health disabilities are legally required in Canada and the United States.19,20 However, formal accommodations require a degree of medical intervention and disclosure to the employer that many workers believe is risky for career progress. 21 Further, accommodations often involve a graded-activity approach, 22 such as reducing work tasks or hours, but such an approach may not be appropriate for academics. Academics must balance research, teaching, and service work, making it difficult to determine which barriers can be addressed using a graded approach so that academics with mental ill-health remain on equal footing with other academics. 23
A third option is a leave of absence for mental health reasons, which is a form of workplace accommodation to which many employees are entitled if there is reason to believe that the leave of absence will be effective, lead to recovery, and enable the employee to return to work within a specified period. 24 Mental health leaves of absence are typically lengthy, averaging almost 100 workdays. 25 Leaves of absence may be easier to obtain in unionized environments or in organizations with strong employee wellness plans because there are established procedures for access. However, taking a leave of absence in academia can be challenging because of perceived stigma.26,27 Academics must consider how much they are willing to disclose to department heads and colleagues, 28 as disclosure could have a lasting impact on their career progress and professional status. Obtaining a leave of absence requires documentation, usually from physicians rather than mental health professionals, 24 even if the physicians are unfamiliar with the mental health of the individuals and their working conditions. Further, even when a temporary replacement for teaching or student supervision is found, there is often an expectation that teaching time will be made up in the future, adding to the burden of taking a leave. 29
The Roles of Gender and Academic Position
Given that occupational stressors in academia are often gendered,6,30 gender may affect how academics manage their mental ill-health at work. Academic women continue to face systemic sexism,31,32 which can exacerbate work-related stress. They tend to spend less time on research and spend more time on teaching and service compared to academic men. 33 This expectation to focus more on teaching and service can negatively impact career advancement and contribute to stress. In addition, academic women often experience career disruptions and reduced productivity due to pregnancy, child care, and elder care responsibilities. 34 Although these stressors increase their risk of mental ill-health, women are also more likely than men to seek social supports, 35 which can buffer against occupational stress. Transgender academics experience an added layer of microaggressions in addition to the other stressors, 36 further shaping their approach to managing their mental ill-health. These gendered differences in exposure to stressors and access to coping resources suggest that academic men and women are likely to navigate their mental ill-health in distinct ways.
Academic position, whether a person is tenured, tenure track, or employed on contract, is likely to influence how academics manage their mental ill-health at work. Even though much of the research on the mental health of academics has focused on tenured faculty or has not differentiated between those with and without tenure, 37 there are clear differences in the type and impact of work stressors experienced by academics in different career positions. Pre-tenure faculty are expected to produce an increasing number of highly cited scientific publications on a relatively tight timeline. 38 The workload and uncertainty around tenure expectations set these early-career academics up for a high risk of anxiety and burnout. 39 Contract academics often experience uncertainty about contract renewal, which often happens at the last minute, and ambiguity about longer-term career possibilities in academia.40–44 This is particularly concerning because of the high association of uncertainty with mental ill-health and because tenure-track positions are being reduced in favor of hiring contingent academics who teach or conduct research on short or mid-range contracts.43,45,46 In contrast, tenured faculty have job security, which is a considerable stress-buffering resource 47 ; however, they are expected to take on additional administrative, supervisory, and mentorship roles, adding to their role overload.
Research Purpose
The purpose of this research was to explore how Canadian academics manage their mental ill-health while at work and whether they do so informally, seek formal help or workplace accommodations, or take leaves of absence. We explored mental health issues along the lines of gender and academic position. Although the research was conducted during the COVID-19 pandemic when mental health significantly declined in academics, 48 our research considered mental health over the course of the academic's career and thus was not limited to the pandemic.
Methods
Respondents and Procedure
Our respondents were drawn from universities across Canada that included research-intensive, comprehensive, and undergraduate-only institutions. All were universities with unionized faculty members whose collective agreements typically include some mental health care benefits. As part of a larger study of seven Canadian health and professional occupations, 342 academics responded to a bilingual (French and English) online survey about their mental health and leave of absence experiences. Between November 2020 and May 2021, recruitment was undertaken using a range of crowdsourcing methods including direct social media posts on Twitter (now X), Facebook, and LinkedIn, newsletters, and, in some cases, direct email from of our research team, our partner organizations (e.g., faculty unions), and a Canadian market research company. Recruitment materials contained a link to an online questionnaire hosted on the Qualtrics web-based survey platform. Ethics approval was secured initially from the University of Ottawa (S-05-19-2508), with secondary approval secured from 16 other universities of the broader team members.
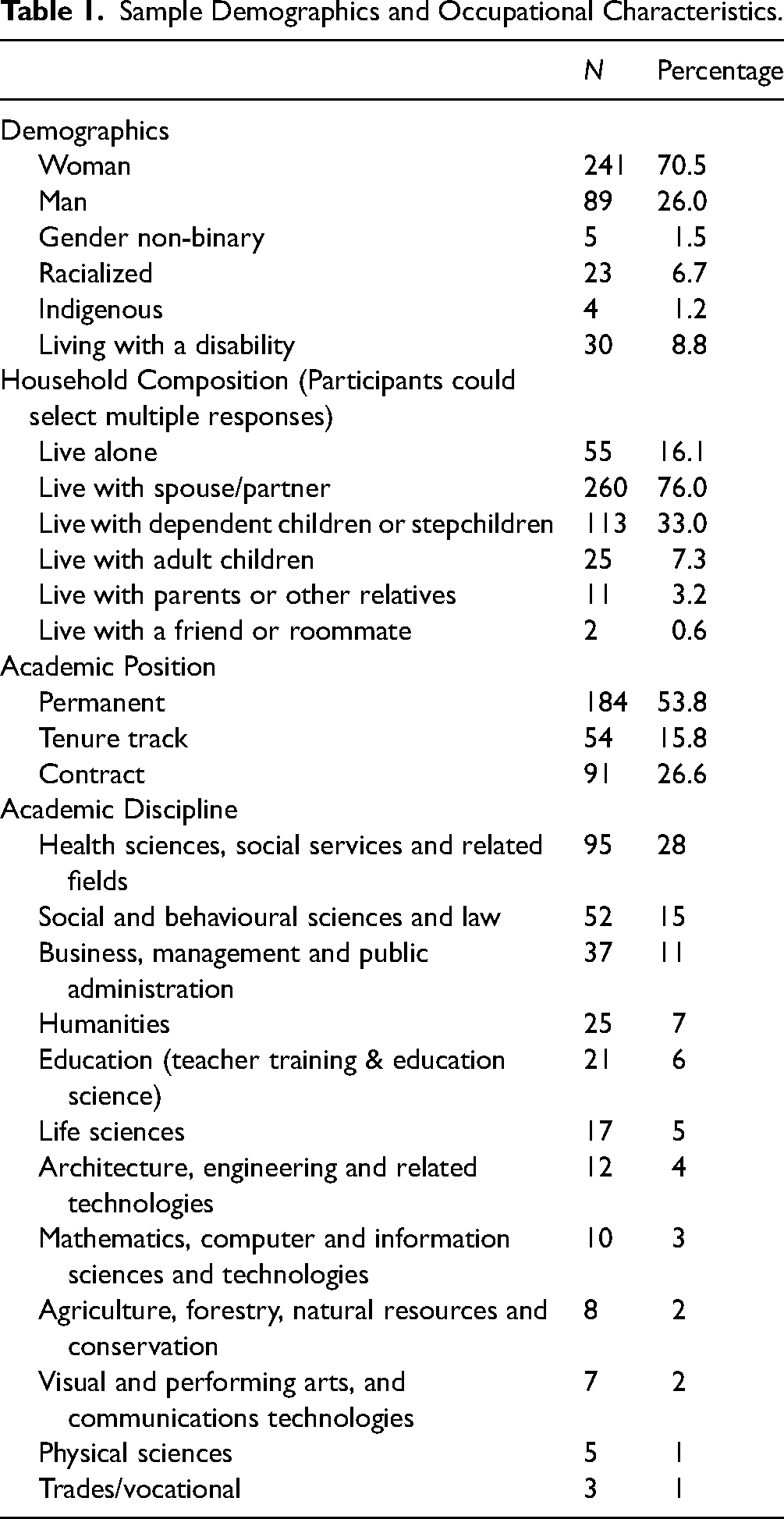
The sample had an average age of 49.4 years (SD = 11.7) and was predominantly tenured with a mean of 17.9 years (SD = 11.8) of experience in their field. Most participants identified as women (70.5 percent), and most lived with a spouse/partner (76.0 percent). For those who indicated living with dependent children or stepchildren (33.0 percent), the average number of children requiring homeschooling or care was 1.64 (SD = 0.76). Further details on sample demographics and occupational characteristics are in Table 1.
Sample Demographics and Occupational Characteristics.
Measures
Respondents were asked demographic information, including gender, age, and household composition. They were also asked for their academic position, that is, whether they were permanent, tenure-track, or in a contract position (term, sessional, or postdoctoral position), their primary academic discipline, and how many years they had been working in their profession. Respondents responded either yes or no to whether they had ever had a mental health issue over the course of their careers or training, defined as mental or psychological stress or distress, burnout, anxiety, depression, other mood disorders, substance use or dependence, post-traumatic stress disorder, or serious thoughts of suicide.
Respondents who indicated that they had experienced mental health issues over the course of their careers were asked whether or not they had ever made changes to their work in response to mental health issues (yes/no). Those who responded yes were asked to choose one or more potential changes (retreated/took sick days/vacations, reduced workload/amount of work, changed type of work tasks, self-medicated, sought social support at work, sought support from union, other: please specify) from the list of response options developed for this study.
Respondents who indicated that they had experienced mental health issues over the course of their careers were asked to indicate whether they had ever used one or more formal mental health supports from a list of options developed for this study (family physician, workplace mental health initiative, Employee and Family Assistance Program, formal peer support program, confidential helpline, therapist/counselor, other: please specify). In addition, they were asked whether or not they had ever formally requested workplace accommodations related to mental health (yes/no). Those who responded yes were asked whether or not they had obtained the workplace accommodations they had requested (yes/no) and to choose one or more potential accommodations from a list of response options developed for this study (change hours, reduce workload, job share, change position/employer, change in employment status, change in setting, change speciality, other: please specify).
Respondents were asked whether they had ever considered taking formal leaves of absence from their work due to mental health issues (yes/no), whether they would be able to take leaves of absence due to mental health issues if needed (yes/no/I don’t know), and whether they had ever taken formal leaves of absence from their work due to mental health issues (yes/no). Those who had not taken formal leaves of absence were asked to select one or more potential reasons for not doing so (mental health issue was not severe enough, professional impact, impact on students, lack of replacement instructor, impact on colleagues, finances, had professional supports in place, other: please specify).
Data Analysis
All statistical analyses were conducted using Stata version 17. Descriptive statistics were conducted on variables representing demographic and occupational characteristics, including means, standard deviations, and ranges for continuous variables (e.g., age, years in profession) and frequencies and percentages for categorical variables (e.g., gender, educational sector). For the main questions exploring mental health and leaves of absence, we computed frequencies and percentages for all academics, by gender (man, woman), and by academic positions (permanent, tenure track, contract). Note that only five respondents indicated they were gender non-binary, and five others gave responses that did not fit our classification, resulting in a category that had insufficient power to be included in quantitative analyses.
Results
Prevalence of Mental Health Issues and Informal Work Changes
Of the 342 academics in our sample, 218 (64 percent) reported having experienced mental health issues in the course of their career or training. More women (66 percent) reported mental health issues than did men (54 percent). Over half (n = 119, 55 percent) of the academics who reported having had mental health issues responded by making changes on their own. However, 99 (45 percent) indicated they did not make changes. The most common changes (see Table 2) were to reduce workload, to use sick or vacation days, and to seek social support. It is notable that seeking support from one's union or changing types of work tasks were the least selected changes.
Changes Made by Academics in Response to Mental Health Issues.
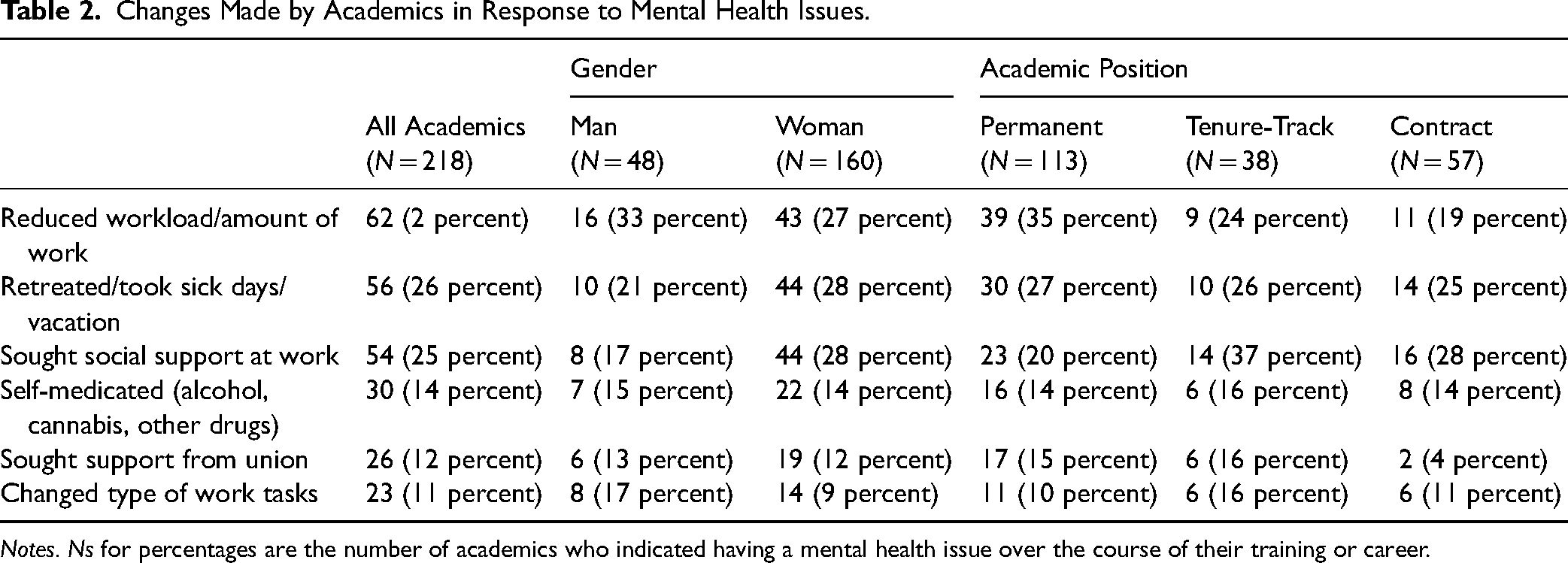
Notes. Ns for percentages are the number of academics who indicated having a mental health issue over the course of their training or career.
Formal Help-Seeking and Workplace Accommodations for Mental Health Issues
Of the 218 respondents who reported having experienced mental health issues in the course of their careers, just over three-quarters (n = 171; 78 percent) sought help from one or more of the sources of formal mental health supports shown in Table 3. Most respondents said they sought help from therapists, followed by family physicians and Employee and Family Assistance Programs. Four participants indicated they sought help from other sources (community health programs, culturally-specific spiritual support). The percentage of women (82 percent) who sought formal supports was higher than that of men (71 percent). The percentage of tenured academics (n = 93, 82 percent) who sought formal supports was also slightly higher as compared to tenure track (n = 29, 76 percent) and contract academics (n = 42, 74 percent).
Formal Supports Accessed by Academics with Mental Health Issues.
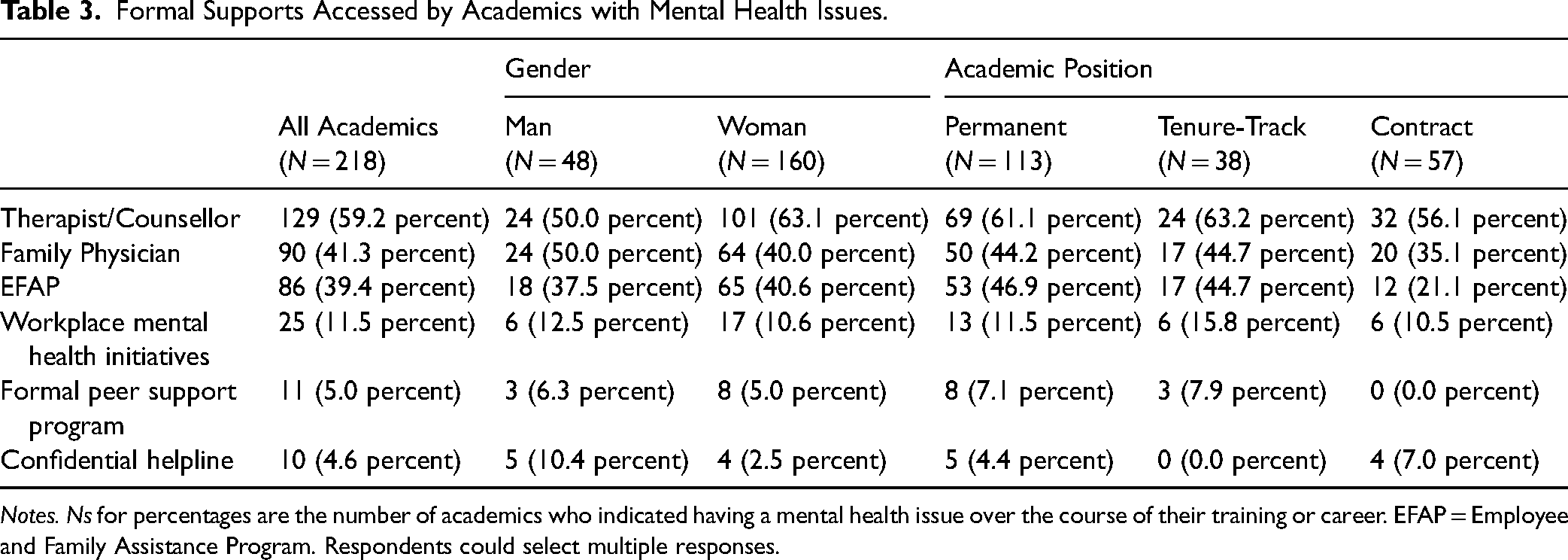
Notes. Ns for percentages are the number of academics who indicated having a mental health issue over the course of their training or career. EFAP = Employee and Family Assistance Program. Respondents could select multiple responses.
Only 41 (19 percent) of the 218 academics who indicated having had mental health issues at some point in their careers formally requested workplace accommodations for mental health. The most frequently requested accommodation was a reduced workload (n = 21, 10 percent) followed by changes in work hours (n = 8, 4 percent), work setting (n = 6, 3 percent), position/employer (n = 5, 2 percent), shift (n = 3, 1 percent), or specialty/area of focus/type of task (n = 3, 1 percent). Job sharing was requested by 1 (0.5 percent) participant. One participant wrote they had requested accommodations for mobility concerns. Of the 41 people who requested accommodations, only 25 received the accommodations they requested.
Formal Leaves of Absences in Response to a Mental Health Issue
Over half of the academics who reported having had mental health issues at some point during their careers indicated that they would have been able to take leaves of absence (n = 118, 54 percent) and almost as many considered taking leaves (n = 104, 48 percent). However, just under one-quarter (n = 50, 23 percent) took formal leaves of absence due to mental health issues (see Table 4). Of the 50 academics who took leaves, 39 had each taken a single leave. For a small number, there were multiple leaves of absence – 5 took 2 leaves, 2 took 3 leaves, 1 took 5 leaves, and 3 took 10 or more leaves. The rates of men and women who considered taking a leave and who took a leave were similar. More tenured faculty than tenure track or contract faculty knew they could take leaves of absence for mental health.
Being Able to Take a Leave of Absence, Having Ever Considered Taking a Leave of Absence, and Having Taken a Leave of Absence by Gender and Academic Position.
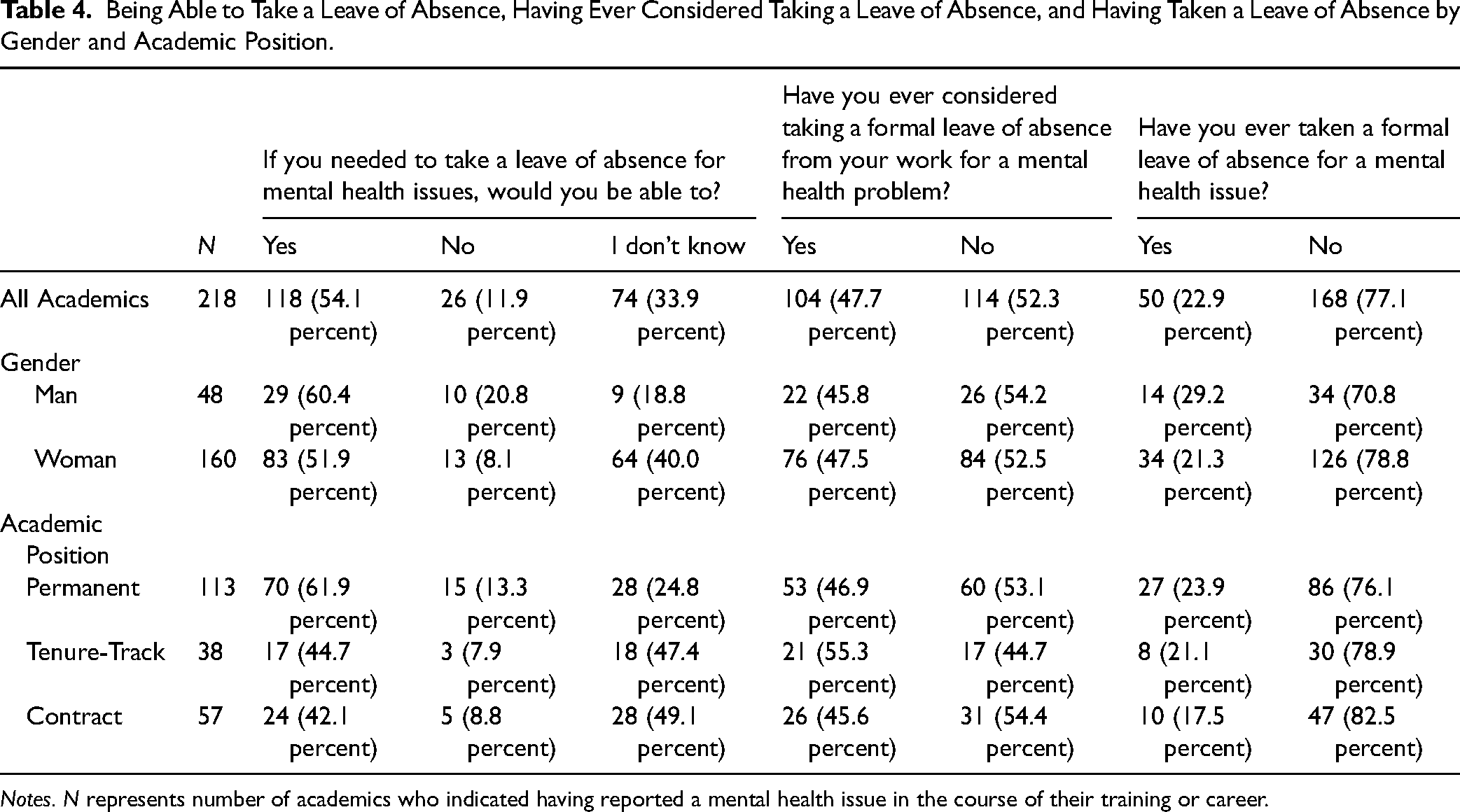
Notes. N represents number of academics who indicated having reported a mental health issue in the course of their training or career.
The most frequent reasons respondents gave for not taking a leave (n = 168; 77 percent) were believing the mental health issues was not severe enough to warrant it, stigma and the negative impact on their careers, and concern for the impact that taking a leave would have on their colleagues’ workload and on their students (see Table 5). It is noteworthy that having supports in place to help remain at work was indicated by very few academics (n = 19, 11 percent). Two participants wrote open-ended responses that working was helping with their mental health. One participant indicated that they were told they did not qualify for a leave of absence. More women than men reported concern about the impact of a leave of absence on their finances.
Reasons for Not Taking a Leave of Absence by Gender and Academic Position.
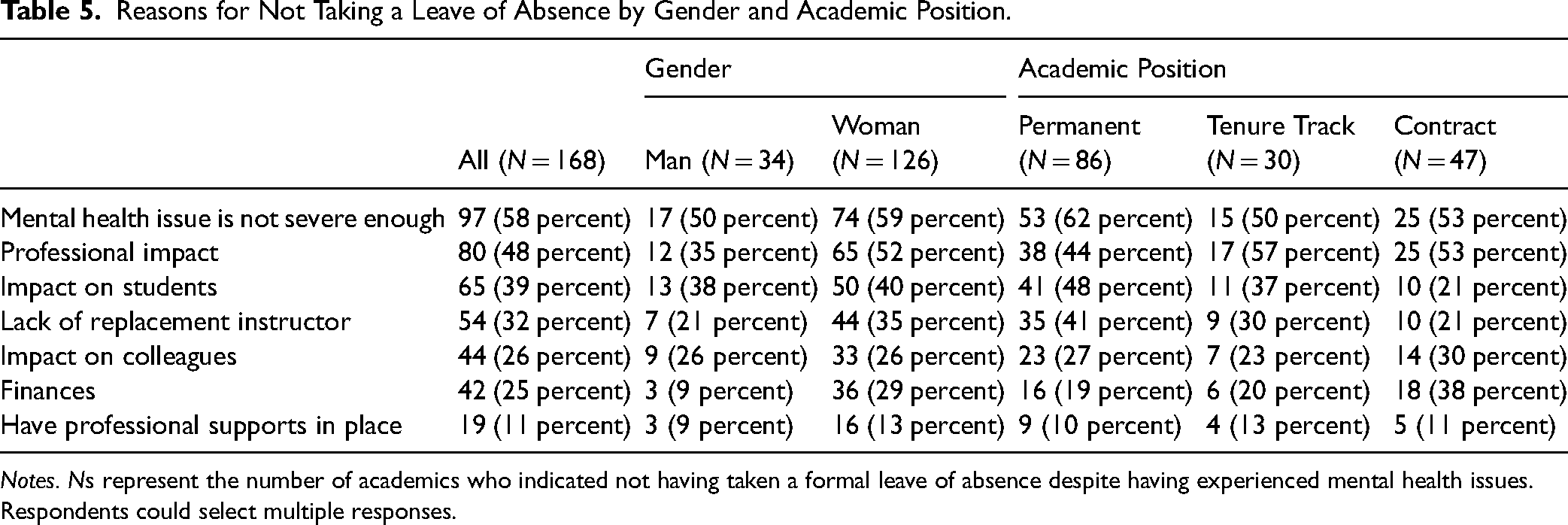
Notes. Ns represent the number of academics who indicated not having taken a formal leave of absence despite having experienced mental health issues. Respondents could select multiple responses.
Discussion
Our work aims to widen the discussion about academics’ mental health beyond contributing factors by focusing on how academics actively manage mental ill-health while working. 10 Because occupational stressors are gendered,6,30 for example, women faculty members do more of the work to support students with mental health issues, 49 and because these stressors vary by career stage, we presented the breakdown by gender and academic position. 50 We took a retrospective approach, asking about any instance of mental ill-health over one's career, knowing that mental health can wax and wane over the years depending on one's circumstances. 51
Almost two-thirds of our sample indicated that they had mental health issues at some point in their careers. This prevalence is slightly higher than in the recent American Healthy Minds Survey 50 which reported 43 percent of faculty and staff in their sample had been diagnosed with mental disorders at some point during their lifetimes. In our study, we asked faculty to report their own mental health conditions. These self-reports may include struggling with a particular issue in a way that may or may not have required diagnosis and treatment. We believe inclusion of these subclinical issues is more in keeping with the mental health continuum than limiting our research to diagnosed mental disorders. 25 Reports of having had mental health issues during one's career were similar across participants in permanent, tenure-track, and contract academic positions. Factors that negatively impact mental health may vary by career stage, but we did not ask our participants at what career stage their mental health issues occurred. The finding that fewer men reported having had mental health issues relative to women, particularly in academia, is consistent with the broader literature. 9 Historically, men and boys have been socialized to be self-reliant and emotionally stoic. Admitting to having mental health issues and asking for help violates such social norms of masculinity. 52 As such, some men avoid telling others, not because they are not dealing with mental health issues, but because they feel pressure to appear unaffected. Such an effect may be amplified in academia, which tends to prize intellectual competence over emotional well-being. 53
In the present study, only about one-half of academics with a mental health issue made any changes to their work. The most common responses were reducing workload, using sick days or days off to manage their symptoms, and seeking social support. It is likely that the autonomy academics experience enables such self-accommodation, allowing them to hide mental health concerns from colleagues, department heads, or Deans, possibly to avoid appearing unable to do their jobs and risking long-term career consequences. The pressure to publish, which is particularly associated with high anxiety and increased likelihood of burnout, 54 may lead faculty with mental ill-health to focus their available energy on the tasks that are most visible and most likely to be counted. 55
Our results suggest that academics, regardless of gender or position, may prefer to go to external supports rather than to formal supports provided by their employers. Whereas more than half of the academics who reported having had mental health issues at some point during their careers sought assistance from therapists or family physicians, very few used workplace mental health resources, peer support programs, or confidential helplines. The number of academics who used their Employee and Family Assistance Programs was comparable to those who went to their family physicians. However, this is likely because such assistance programs are viewed as external to the university. It is possible that academics prefer to go to external supports because they do not trust the confidentiality of employer-sanctioned mental health programs due to stigma and the potential for negative effects on one's career. 21 However, we did not specifically query this.
Wang and colleagues 56 reported that only one-third of people in the workforce with diagnosed anxiety or depression receive workplace accommodations, even though the purpose of accommodations is to help people maintain work performance. Similarly, few of our respondents sought workplace mental health accommodations, despite being entitled by law. 20 Even fewer received accommodations. Indeed, we found that 48 percent of our sample did not take a leave because of concern about professional impact. It is likely that academics are reluctant to disclose their mental health issues, which is required for accessing accommodations, due to the stigma that remains about mental health and the potential for harm to their career trajectories. 57 In addition, many academics might believe accommodations would be performative rather than useful, in the same way that faculty perceive universities are far more invested in student mental health than in faculty mental health. 50
Another key barrier to requesting accommodations could be that academics and those arranging for accommodations have difficulty determining appropriate formal accommodations. 57 One of the more common types of accommodation involves changing job tasks or work requirements. 58 However, academic roles include responsibilities for teaching, research, and service, each involving a wide range of activities, which makes this strategy difficult to apply. It is not always obvious what “doing less” entails: Should an academic teach fewer courses, take on fewer students, publish less, or reduce service commitments? How would reductions in any of these categories affect their career? Without clear or flexible models for adjusting these interdependent responsibilities, faculty members may find the process of seeking accommodations confusing or discouraging. When available accommodation strategies are limited or not well adapted to the realities of academic work, it is understandable that some faculty members may hesitate to disclose mental health concerns or pursue formal supports that may not meet their needs.
Even though half of our respondents with mental ill-health knew that mental health leaves of absence were available to them, only about one-quarter took a leave. Similar rates were reported by gender and by academic position. Respondents indicated three key reasons for not taking leave: 1) they believed their mental health issues were not so severe as to require a leave; 2) they were concerned about the negative impact that mental health stigma would have on their careers; and 3) they were concerned about the negative impact their absence might have on their colleagues or students. These findings suggest that formal availability of leaves is not sufficient on its own. Cultural and relational barriers play a critical role in shaping whether academics feel able to make use of mental health accommodations.
The low number of those who took mental health leaves of absence and accommodations, despite the large number of academics who reported mental ill-health at some point in their careers, indicates there is likely a high level of presenteeism. It is common for people struggling with their mental health to be unaware of how poorly they are doing and how little quality work they are producing. 16 It is often only in hindsight that people recognize that they should have taken leave. There remains considerable concern amongst academics about keeping work in the pipeline because ‘temporary invisibility’ can result in serious career consequences in terms of being granted tenure or promotion or receiving grant funds.59,60 Pressure to keep research in the pipeline may result in working while unwell. 59
In a system in which academics are working to capacity and beyond, academics with mental ill-health are concerned about the impact their absence would have on students and colleagues. They do not want to ask already overburdened colleagues to take on courses, particularly those in progress, or the supervision of students, out of concern for their well-being. Too often, there are no colleagues with both the qualifications and the time to take on ongoing grant-funded research. As a result, taking mental health leaves of absence does not feel realistic until a breaking point is reached.
Only 12 percent of our sample sought assistance from their unions despite the fact that almost all universities in Canada have faculty unions or professional associations. 61 It is not that Canadian faculty members do not trust their unions or faculty associations, but rather, they consider the context in which they wish to consult with these representing groups. Most human rights legislation states that employers have the obligation to accommodate mental health, up to the point of undue hardship,19,20 therefore, employees are more likely to begin their quest with their manager or with Human Resources. Often, academics turn to their unions only to seek formal action after requests for accommodations or leaves of absence have been denied or employers have provided inadequate accommodations or leaves.
Limitations
Because the research was retrospective, respondents may not have remembered their experience exactly and under- or over-reported the actions they took to manage their mental health. Further, respondents self-selected for this research and are likely those academics who are interested in issues of mental health. As such, it was likely not a representative sample. Future research would do well to randomly sample academics from all disciplines in multiple universities. However, based on past research,6,7 we would expect the rates of mental health issues in a representative sample to be similar to those reported here.
Although we gathered data on household composition, we did not include these variables in our analyses due to our focus on gender and academic position. The gender imbalance in the sample (71 percent women) limited our ability to conduct parallel subgroup analyses across men and women. Future studies with more balanced samples could explore how living arrangements and caregiving responsibilities intersect with gender to shape mental health experiences and help-seeking among academics.
Policy Implications
Our research underscores the need for greater awareness and conversations about the mental ill-health of academics by highlighting the reluctance of academics to disclose or to seek workplace supports. In addition to concern about stigma, academics may perceive accommodations as infeasible because of the complex mix of teaching, research, and service that defines their roles. Such complexity is a core problem for accommodations and leaves of absence in academia because of the question of what level of productivity in each capacity is sufficient without harming the academic's career.
Mental ill-health in academia is not simply an individual issue but reflects the structural conditions of academic work. Institutions have a responsibility to create environments that protect and promote the mental health of their faculty members. Without action, universities risk long-term academic staff consequences such as burnout, decreased productivity, and the untimely departure of talented scholars from academic careers. Institutional policies, workplace norms, and leadership practices all play key roles in determining whether mental health challenges are recognized early and whether effective support is accessible.
Universities should offer accommodations before an academic's mental health deteriorates to the point of needing to take a leave of absence. However, formal accommodations are often coordinated through university Human Resources offices and require documentation provided by a physician. 24 Neither physicians nor university human resources offices tend to be intimately familiar with academic roles. Human resources staff are professionals educated and trained in general HR practices, such as recruitment, payroll, benefits, labor relations, and compliance. They understand the process of accommodations and leaves of absence, but are not trained to understand the multiple complex roles that academics have. As a result, proposed accommodations often address the underlying problems poorly. It takes creativity to determine the best accommodations for each individual, which requires collaboration among the individuals needing accommodations, their departments, and university leadership, with support from their unions or faculty associations and Human Resources. An equity-based approach would tailor teaching, research, and service loads to individual needs and abilities. To manage this, each university should fund a position or office dedicated to coordinating accommodations and leaves of absence and to helping faculty members navigate the leave process, design phased returns, and determine appropriate accommodations. This would ensure that accommodations are the best possible fit for each individual. Additional research is required to determine the extent to which such an office would be effective.
Universities should modernize existing policies for leaves of absence. Some current policies rigidly require academics on leave to discontinue all work-related tasks, including communication with students and trainees, who rely on them for supervision. Because research and teaching are often central to the identities of academics, not being permitted to do any work at all can be more harmful than helpful once an individual recovers from acute symptoms of mental ill-health. Being able to work at their own graduated pace while on leave and when returning to work can help with recovery and alleviate concerns regarding lost productivity. Even if work overload is at the root of the mental health issue, working can contribute to psychological well-being by acting as a source of structure and meaning. 25
Systemic change across academia is necessary to address the widespread mental health challenges that stem from structural pressures rather than individual shortcomings. Interventions that target the individual academic (e.g., therapy, mindfulness) imply that the issue is with the person rather than the larger social system. Even when it is acknowledged that mental health issues in academia are systemic, most solutions are “hacks” that target actions at the individual level. 60 Such interventions are bandaid solutions, helping academics cope just enough to stay on the ever-accelerating treadmill.
Implementing interventions at the local level to address workload expectations is challenging when the broader academic culture perpetuates productivity pressures not specific to a department, university, or country that are linked to anxiety, depression, burnout, and substance misuse. 6 Despite having autonomy in research and work schedules, academics face relentless pressure to produce. They know that their productivity is constantly being evaluated and that they are expected to meet publication and funding benchmarks. Universities have been described as greedy institutions, 62 continually raising the bar for acceptable levels of productivity.
Academics have to produce more research of greater complexity to remain competitive for grants that are becoming scarcer and for a changing journal landscape. Although many universities have explicit criteria for tenure and promotion, there is a sense that these standards have been escalating over time, requiring larger data sets, more complex analyses, or multi-disciplinary research teams. At the same time, university budgets in many countries are declining. Universities are reducing their reliance on tenure-track instructors, 63 but many also are required to limit their reliance on contract instructors as a means to cut immediate costs. 64 Even with such cost-cutting measures, universities require more students to keep them afloat, and so class sizes get larger, requiring teaching faculty to reorient their pedagogy and classroom management 65
If the issue originates at the level of the academic system, interventions must operate at the same level. 9 Although it may be the start of a Herculean task, academic associations at the country level or discipline level must point out the increasing expectations for research output, accompanied by increasing time demands. They should develop guidelines defining a reasonable workload and highlighting the mental health benefits of rest. Grant eligibility should require fewer publications. The academic culture that prioritizes quantity over quality publications has led to pressure to engage in dubious research practices. 66 Allen 67 recently suggested the development of a G + index to acknowledge positive academic behaviors, including good science practices, generosity, mentorship, and investment in the careers of others. The G + Index would give recognition to the often invisible “academic housework” that is disproportionately done by women. 68 Such measures could help shift norms around productivity and reduce the structural factors that contribute to mental health crises among academics. We certainly want all academics to live up to their full potential. At the same time, we want to avoid the likelihood that “tall poppies” 69 will benefit at the expense of others or at the risk of harming themselves with lack of attention to their own mental or physical health needs. As an academic culture, we need to pay attention to the rewards given for unhealthy behavior. 70
Ultimately, universities and academic associations must recognize that protecting mental health is essential to sustaining a vibrant and innovative academic workforce. Institutions should treat mental health not as an individual vulnerability to be managed quietly, but as a systemic concern requiring proactive, structural, and well-resourced solutions.
Conclusion
Mental ill-health is an issue that many academics will face at some point in their careers. There remains a reluctance for academics to tell others in the university about their mental health struggles. This is not surprising given systemic issues with overwork and the competitive nature of academia. 10 Rather than risking negative effects that disclosing mental ill-health could have on their careers, it is likely that academics use their work autonomy and flexibility to manage on their own, or “self-accommodate”, rather than take a leave of absence or request formal accommodations. As mental health literacy increases in workplaces, including academia, and young workers are less willing to sacrifice their mental health for work, we are likely to see an increase in seeking accommodations and leaves of absence. With the reduction in mental health stigma, we expect to see improvements in university support of faculty mental health. It is an issue that should be taken on at the highest possible level.
Footnotes
Acknowledgements
The authors would like to acknowledge the assistance of Natasha Ball, Sam Morton, Christina Young, and Henrietta Boateng for their assistance with data collection and data preparation and Audrey Kruisselbrink who coordinated the review of ethics.
Author Contributions
JM (conceptualization; methodology; writing - original draft; writing-review & editing), CT (formal analysis, methodology, writing - original draft, writing - review & editing), NP (conceptualization, writing - review & editing), IB (conceptualization; funding acquisition, project administration, writing - review & editing)
Consent for Publication
Not applicable
Data Availability
The datasets used during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethics approval was obtained first from the University of Ottawa (S-05-19-2508) and subsequently from 15 Canadian universities with participating researchers in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research and Social Sciences and Humanities Research Council of Canada Partnership Grant for Healthy and Productive Work, (grant number 895-2018-4014).