
Abstract
Keywords
Introduction
In the United States (U.S.) the opioid epidemic has resulted in over a million deaths between 1999 and 2020. In 2021, the number of overdose deaths involving opioids (prescription, illicit, and synthetic) was 10 times greater than in 1999. 1 A number of factors have contributed to the opioid epidemic, including but not limited to: the excessive prescription of opioids for acute injuries and chronic pain syndromes which have created opportunities for diversion of legitimate prescriptions in the 1990s and 2000s; elevated heroin use in the 2010s; and the continuing rising availability and access to illicit synthetic opioids (e.g., fentanyl).2–4 Physiologic dependence on these aforementioned substances have led to increasing opioid use/misuse—using illicit opioids and/or misusing prescription opioids—and substance use disorders (SUDs). 5 Unfortunately, the opioid epidemic was exacerbated by the COVID-19 pandemic resulting in a syndemic or “twindemic”. 6 In the early COVID-19 pandemic, job loss, financial strain, altered living arrangements, increased isolation, decreased access to social support services, decreased access to medical services, and exacerbated health disparities contributed to elevated rates of nonfatal and fatal opioid overdose—resulting in the most recent wave of the ongoing opioid epidemic.6–9
One of the ways in which communities have sought to address the opioid epidemic is through policies aimed at substance use deterrence in a variety of spheres of life, including the workplace.10–13 Workplace drug policies aim to discourage and have historically disciplined those who use substances, in and outside the workplace, since itcan affect their workplace performance. While workplace drug policies are not new, they should be reexamined as to whether they are truly beneficial to the workplace and the workers—especially in light of the ongoing opioid epidemic and the number of workers in recovery.14,15 Punitive workplace drug policies became commonplace after the passage of the Drug-Free Workplace Act of 1988, which applied to some federal contractors and all federal grantees. This act was prompted by President Reagan's concern about illicit drug use and prescription medication use/misuse among military and enlisted personnel.16,17 These laws explicitly targeted workplace substance use/misuse and gave employers the legal power to take action against substance use and impairment in the workplace by implementing varying degrees of punitive policies (e.g., immediate termination, revocation of payment for services, denial of future work).11,17 By the early 1990s, the establishment of workplace drug policies in the private sector became commonplace with 50% to 75% of workplaces conducting drug testing.11,18 Despite their widespread adoption, there is little empirical evidence that punitive workplace drug policies decrease substance use/misuse among workers or support those with SUDs.10,19
Workplace drug policies are an important intersection between the opioid epidemic and workplace mental well-being initiatives. A 2019 survey from the National Safety Council found that 75% of employers reported that opioid use has impacted their workplace but only 17% reported being extremely well-prepared to address the issue.
20
In 2022, the U.S. Surgeon General published a report on “Workplace Mental Health & Well-Being” which states that, “Work affects both our physical and mental well-being—in good ways and bad.”
21
While the report discusses an inclusive framework to support worker well-being centered around worker voice and equity, it does not directly address the opioid epidemic—a prominent public health crisis—except for a link to “Drug-Free Workplace Resources” from the Substance Abuse and Mental Health Services Administration. This is a concerning omission, given the large body of research establishing that psychological distress is linked to opioid use/misuse.22–24 Furthermore, this policy document lacks meaningful discussion of the relationship between mental well-being, workplace drug policies, and opioid use/misuse. This study sought to address this gap by using data from the 2020 National Survey on Drug Use and Health (NSDUH), the most comprehensive surveillance system of substance use in the U.S. population. For this study, we had three research questions and hypotheses:
RQ1: Are employed individuals with past year psychological distress more likely to also have misused opioids in the past year compared to those without psychological distress? H1: Those with past year psychological distress will have a greater likelihood of also having misused opioids in the past year. RQ2: Is there a difference in the proportion of individuals employed at workplaces with versus without punitive drug policies who report past year opioid misuse? H2: There will be a higher prevalence of opioid misuse in workplaces with punitive drug policies compared to those without. RQ3: Do individuals with more past year psychological distress, in combination with punitive workplace drug policies (compared to those with less distress and/or nonpunitive policies) have a higher prevalence of past year opioid misuse? H3: People who have psychological distress in the past year and punitive workplace drug policies will have the highest prevalence of past yearopioid misuse compared to those with less psychological distress and/or nonpunitive workplace drug policies.
To the best of our knowledge, this is the first study to examine how punitive workplace drug policies relate to opioid use/misuse and psychological distress among the U.S. workforce. Empirical research that addresses the ways that psychological distress and opioid use/misuse relate within the context of the workplace is needed to inform more comprehensive policy guidance, as well as to identify opportunities for stakeholders to collaborate on efficacious and long-lasting approaches to address the opioid epidemic.
Methods
Data Source and Analytic Sample
We analyzed data from the NSDUH, a cross-sectional, nationally representative survey of approximately 40 000 individuals aged 12 and older. It assesses use of alcohol, tobacco, illicit and prescription drugs, SUD, and mental health conditions, among other topics. 25 Data are collected annually and are publicly available. We examined data collected in 2020 as it was the most recent data available at the time of analysis. Data from the first quarter of 2020 were conducted in-person, as in previous years. Data collection was paused due to the COVID-19 pandemic, and resumed in the final quarter of 2020, using web-based interviewing. The NSDUH advises against comparing 2020 data to prior years, due to differences in data collection procedures. 26
This analysis was limited to respondents 18 years and older who stated that they are employed (full- or part-time). Those who were unemployed or did not work due to disability, being in school/training, being retired, or other reasons were excluded from primary analyses. This subpopulation of the NSDUH resulted in a sample size of 18 038, all of whom also had data on opioid use/misuse and psychological distress. For analyses involving workplace drug/alcohol testing policies, only those respondents who are employed and stated that they knew their workplace's policy for testing positive on substance use test at work were included, resulting in a subpopulation of 6687. Those who did not know their workplace's drug policy (n = 744) were excluded from those analyses.
Measures
Opioid Use/Misuse
Our primary outcome of interest was opioid use/misuse (including illicit opioids and prescription pain medication not used as directed a ), which was measured by misuse over the past year (dichotomous, yes/no). We also examined type of opioid used (illicit opioids, prescription medication, or both); however, the vast majority of those who misused opioids reported using pain relievers only (94.1), 2% used heroin only, and the remainder reported both pain relievers and heroin (3.9%). We also explored the Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV and V criteria for opioid use disorder in the past year. However due to limited sample sizes for these variables, they were only used to characterize the severity of opioid use/misuse among those who reported misuse in the past year.
Psychological Distress
The Kessler-6 (K6) psychological distress scale27,28 (6 items each ranked on a 5-point Likert-scale, total score ranges from 0 to 24) was used to index nonspecific symptoms that are associated with depression and anxiety. To assess the relationship between past year serious psychological distress and past year opioid use/misuse, we operationalized psychological distress as meeting criteria for a “serious” score (i.e., warranting clinical intervention) using the established threshold of scores ≥ 13. In supplemental analyses we also indexed psychological distress using the K6 as a continuous score and past year major depressive episode (MDE) as defined by the DSM-V. 29 Results using these two variables were consistent with the main analysis using the dichotomous K6 score.
Punitive Workplace Drug Policies
Workplace drug policies were measured by respondent self-report , that is, the employee, conditional on being aware of their employers’ policies on these matters (described above). We defined a punitive workplace testing policy as immediate termination versus no termination (e.g., warning, referral) in response to an employee's first positive drug test. To give context into other workplace drug policies, we also descriptively examined whether the respondents’ workplace has a written policy on employee substance use, whether the workplace tests employees for drug use, tests for drug use as part of hiring, tests for drug use on a random basis, provides education on substance use, and offers an assistance program for substance use.
Demographic Covariates
We included a range of demographic covariates to understand differences within groups and to identify vulnerable sub-populations. These include age (18-25, 26-34, 35-49, 50-64, and 65+), sex (Male, Female), race/ethnicity (Non-Hispanic White, Non-Hispanic Black/African American, Non-Hispanic Native American/Alaska Native, Non-Hispanic Native Hawaiian/Other Pacific Islander, Non-Hispanic Asian/Asian American, Non-Hispanic Bi-/Multi-racial, and Hispanic), respondent's total income (less than $10k, $10k-$19.9k, $20k-$29.9k, $30k-$39.9k, $40k-49.9k, $50k-$74.9k, and $75k+), and educational attainment (less than high school, high school graduate, some college/associates degrees, college graduate).
Cell sizes for interactions were examined ahead of running multivariate logistic regression models. We opted to dichotomize demographic covariates when cell sizes of subcategories were not large enough to power three-way interactions being investigated (i.e., smaller than four observations). We dichotomized age at the median value (<35 and 35+), race/ethnicity into Non-Hispanic White (NHW) and remaining categories (Black, Indigenous and People of Color; BIPOC), income at the median value for those who were employed (<$40k vs $40k+), and educational attainment at the high school degree level (HS graduate or less vs some college and beyond).
Statistical Analysis
The complex design of the NSDUH and sampling weights were accounted for in the analysis using a combination of the svy package in Stata version 14.2 and the survey package 30 in R version 4.2.1. Hypotheses were preregistered through Open Science Framework (OSF) at https://osf.io/5w4jx. Research questions have been slightly re-worded for clarity since preregistration; scripts used for analysis are available on OSF. 31
Three sets of models were constructed to address our primary research questions. First, we fit models examining the relationship between psychological distress and opioid use/misuse (RQ1). Second, we fit models testing whether an employee's workplace having a punitive drug policy was related to opioid use/misuse (RQ2). Finally, we fit models testing whether there was an interaction between having a punitive workplace drug policy and psychological distress (RQ3) on opioid use/misuse. We used a multistage analytical approach described by Heeringa et al.32,33 In the first stage for each model, we initially specified the complex design features of the NSDUH and then examined bivariate associations between opioid use/misuse with independent variables and covariates; the significance of these associations were assessed using Rao–Scott Chi-squared tests. In the second stage, we fit multivariable logistic regression models to examine the relationship between workplace drug policies, opioid use/misuse, and psychological distress together; these models included covariates and interactions between variables. In this stage we used a hierarchical approach, where the primary independent variables were entered first, followed by covariates, followed by interactions between variables. When models included significant interactions, a further model was run removing nonsignificant interactions. In the third stage, which in practice coincided with the second stage, we evaluated the significance of individual predictors using design-adjusted Wald Chi-squared tests and the overall models for fit using design-adjusted Akaike information criterion (AIC) and design-adjusted likelihood ratio tests (LRT). Final models were selected based on overall model fit. The fourth stage involved interpretation of the final models.
Results
From the NSDUH, weighted, design-based estimates indicate that of the 147 831 081 workers aged 18 and above who were employed full- or part-time in 2020, 3.38% (5 003 425) reported misusing opioids in the previous 12 months. Of those who reported opioid misuse, 15.36% met DSM-IV criteria for opioid use disorder and 24.60% met DSM-V criteria for a SUD. Table 1 displays the bivariate weighted psychological, demographic, and workplace characteristics of employees aged 18+ stratified by past year opioid misuse. Opioid misuse was more common among women relative to men and most common among Non-Hispanic Native Americans/Alaska Native workers (9% with past year misuse) followed by NHW workers (4% with past year misuse). Lower-income workers (incomes between $10 and $30 000) had higher rates of opioid misuse than other income groups. People who reported opioid misuse had significantly more sick days (1.75 vs 0.83 days).
Bivariate Design-Based Tests of Association Between Past Year Opioid Misuse and Independent Variables.
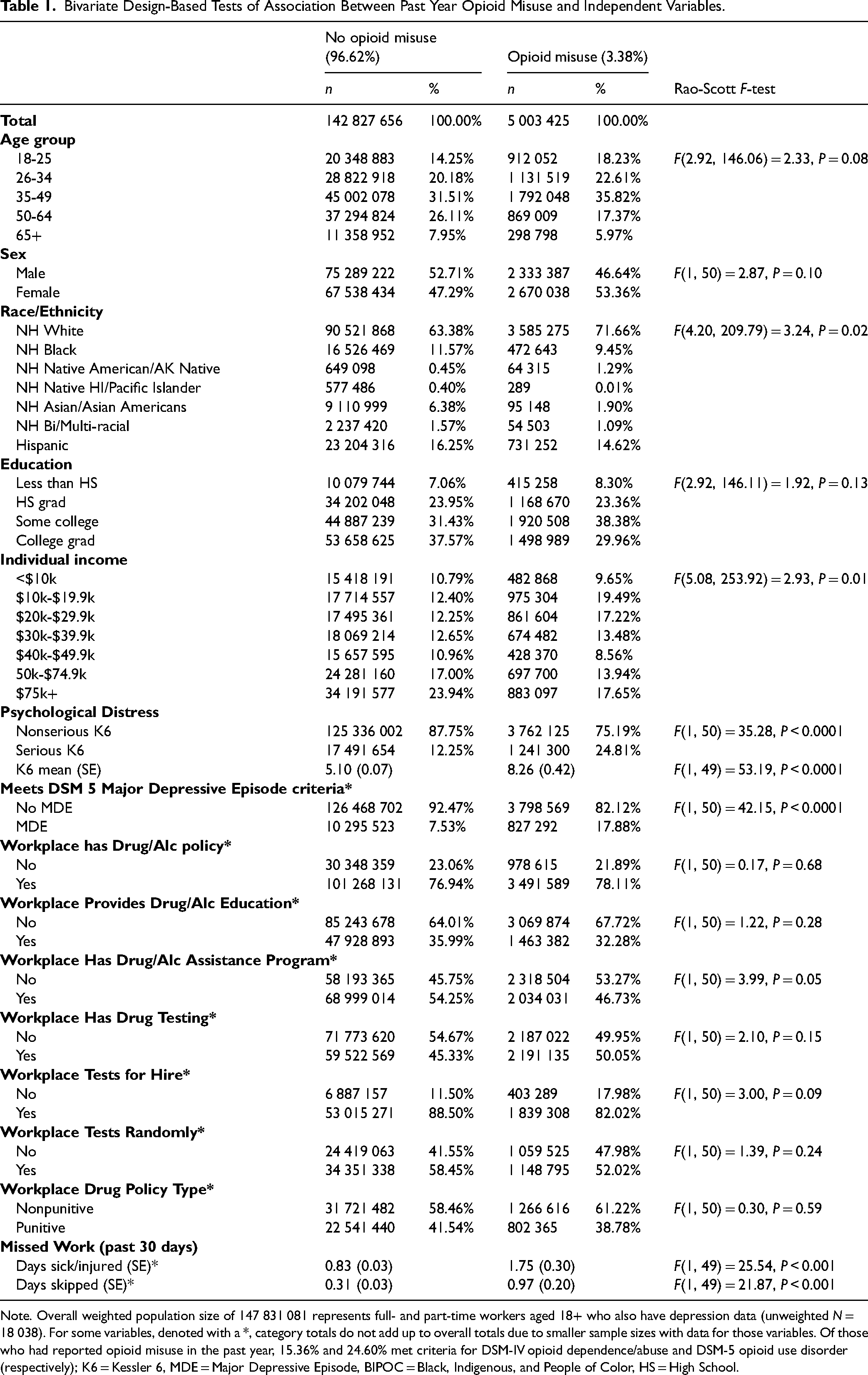
Note. Overall weighted population size of 147 831 081 represents full- and part-time workers aged 18+ who also have depression data (unweighted N = 18 038). For some variables, denoted with a *, category totals do not add up to overall totals due to smaller sample sizes with data for those variables. Of those who had reported opioid misuse in the past year, 15.36% and 24.60% met criteria for DSM-IV opioid dependence/abuse and DSM-5 opioid use disorder (respectively); K6 = Kessler 6, MDE = Major Depressive Episode, BIPOC = Black, Indigenous, and People of Color, HS = High School.
Of those who reported opioid misuse, there were no significant differences in any demographic variables in likelihood of using illicit opioids, Fs < 2.73, ps > 0.10. Similarly, misuse of prescription pain relievers did not vary by age or sex, Fs < 0.41, ps > 0.53. NHW employees, employees with higher education, and higher income employees were more likely to misuse prescription pain relievers than their respective BIPOC, lower education, and lower income counterparts, Fs > 5.83, ps < 0.03.
Opioid Misuse and Psychological Distress
Workers who reported past year opioid misuse were significantly more likely to have a K6 score > 13, indicating serious psychological distress, and were also more likely to have had a MDE in the past year. In our multivariate models (Table 2), the best-fitting model included main effects but no interactions. We found that, after adjusting for covariates, those with an elevated K6 score were 2.10 times more likely to also report opioid misuse. Furthermore, BIPOC were only 63% as likely as NHW workers to report opioid misuse. Finally, workers with a college degree were least likely to report opioid misuse, although categorical differences were only statistically significant between those with a college degree and those with some college education.
Estimates of Adjusted Odds Ratios for Past Year Opioid Misuse by Past Year Serious K6 Score and Demographics (Model 1).
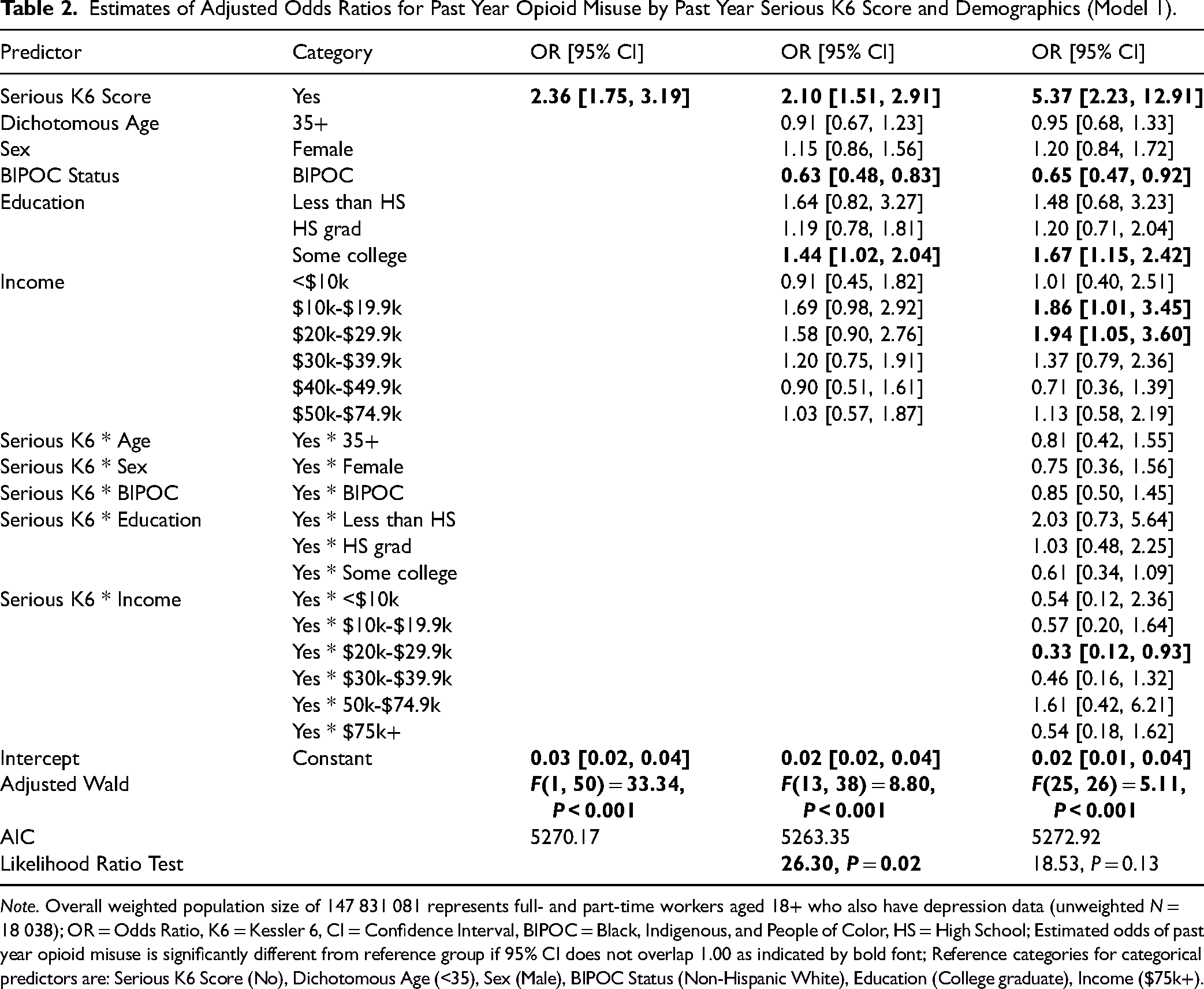
Note. Overall weighted population size of 147 831 081 represents full- and part-time workers aged 18+ who also have depression data (unweighted N = 18 038); OR = Odds Ratio, K6 = Kessler 6, CI = Confidence Interval, BIPOC = Black, Indigenous, and People of Color, HS = High School; Estimated odds of past year opioid misuse is significantly different from reference group if 95% CI does not overlap 1.00 as indicated by bold font; Reference categories for categorical predictors are: Serious K6 Score (No), Dichotomous Age (<35), Sex (Male), BIPOC Status (Non-Hispanic White), Education (College graduate), Income ($75k+).
Opioid Misuse and Workplace Drug Policy
Overall, there were no significant differences in past year opioid misuse as a function of having, compared to not having, a workplace drug policy (Table 1) or having a punitive, compared to nonpunitive, workplace drug policy (Table 3). Models that included covariates as well as interactions were significant, Fs > 2.31, ps < 0.03, but did not improve model fit from the bivariate model of punitive policy and reported opioid misuse. The best fitting model, with a LRT = 29.47, P = 0.03 relative to the baseline mode, pruned nonsignificant interactions F(15, 36) = 2.58, P = 0.01 and showed two significant interactions with a punitive policy including dichotomized age (18-34 vs 35+) and dichotomized race/ethnicity (NHW vs BIPOC). Specifically, prevalence of opioid misuse was significantly higher for workers 34 and under who had punitive workplace drug policies compared to those of the same age with nonpunitive workplace drug policies (Figure 1); however, this relationship was reversed for workers 35 and over. In terms of race/ethnicity, there was no relationship between punitive workplace drug policies and opioid misuse among NHW workers, however BIPOC workers with a nonpunitive policy had higher rates of reported misuse than BIPOC workers with a punitive policy. Furthermore, BIPOC workers with a punitive workplace drug policy had significantly lower rates of misuse than all other groups.
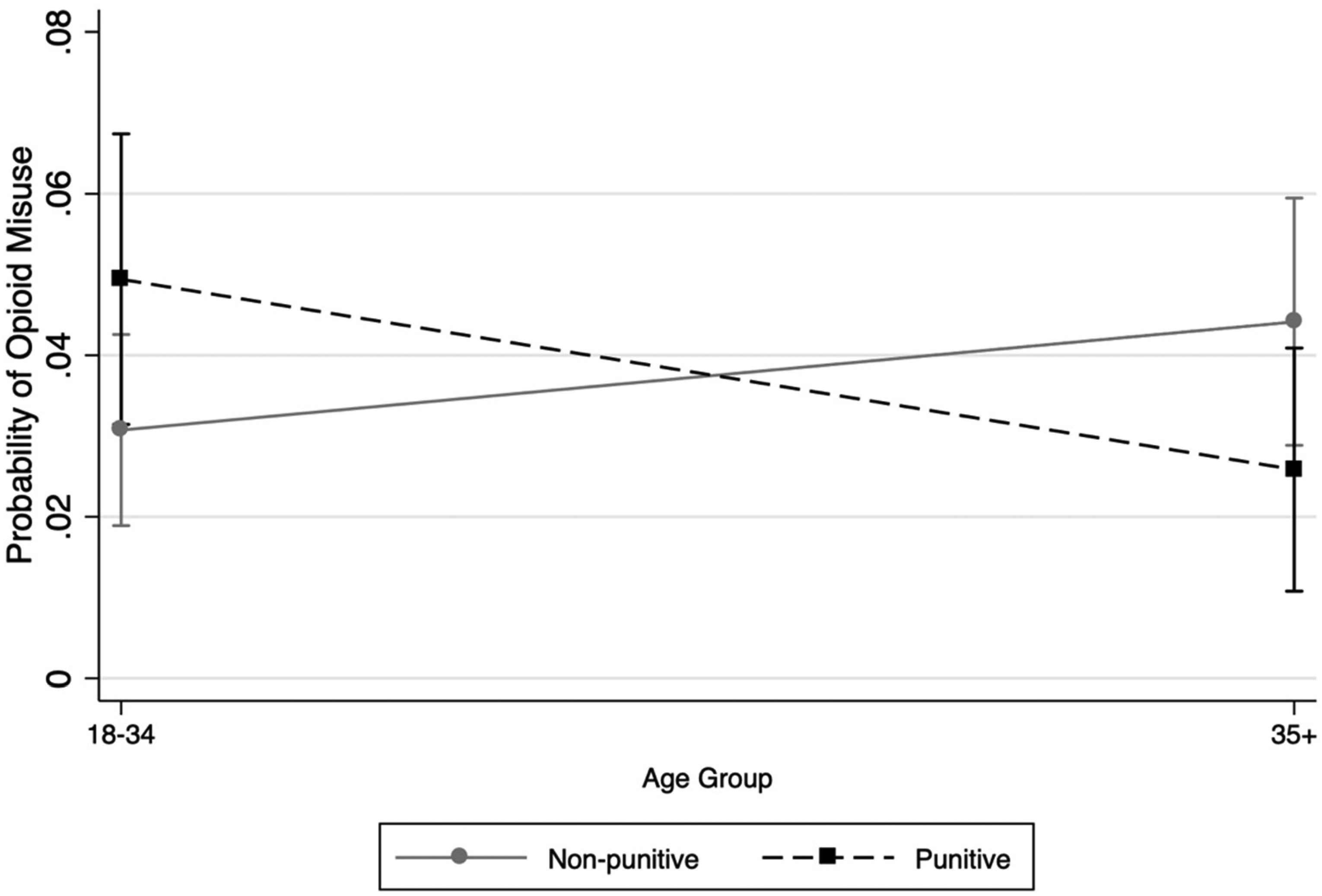
Predictive margins of opioid misuse by workplace drug policy.
Estimates of Adjusted Odds Ratios for Past Year Opioid Misuse by Last Workplace Punitive Policy and Demographics (Model 2).
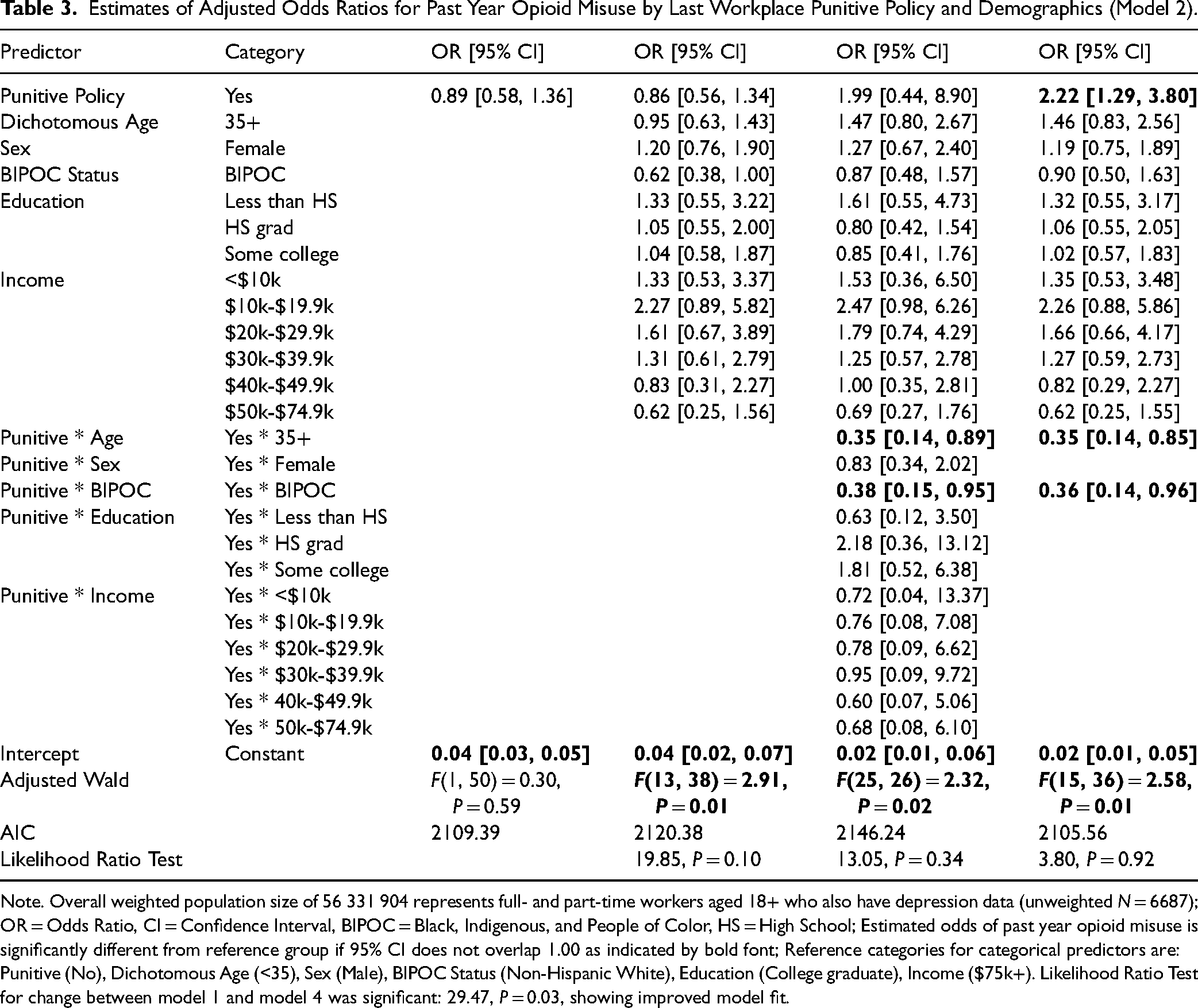
Note. Overall weighted population size of 56 331 904 represents full- and part-time workers aged 18+ who also have depression data (unweighted N = 6687); OR = Odds Ratio, CI = Confidence Interval, BIPOC = Black, Indigenous, and People of Color, HS = High School; Estimated odds of past year opioid misuse is significantly different from reference group if 95% CI does not overlap 1.00 as indicated by bold font; Reference categories for categorical predictors are: Punitive (No), Dichotomous Age (<35), Sex (Male), BIPOC Status (Non-Hispanic White), Education (College graduate), Income ($75k+). Likelihood Ratio Test for change between model 1 and model 4 was significant: 29.47, P = 0.03, showing improved model fit.
Opioid Misuse, Psychological Distress, and Workplace Drug Policy
Although having a punitive workplace drug policy was not associated with probability of misusing opioids in the bivariate analysis (Table 1), multivariate logistic regression analyses indicated a more complex relationship. Table 4 shows the best fitting model which includes psychological distress, workplace drug policy, main effects of demographics, and significant interactions. This model identified two notable interactions. First, as with models addressing RQ2, punitive workplace drug policy interacted with dichotomized age in the same direction. Next, the significant two-way interaction between BIPOC status with workplace drug policy, and a two-way interaction between BIPOC and psychological distress, was further illuminated by a three-way interaction. The nature of this interaction is illustrated in Figure 2. Consistent with models addressing RQ2, for NHW employees, there was no difference in reported opioid misuse by workplace drug policy, and furthermore, having a serious level of psychological distress was associated with a greater probability of opioid misuse regardless of their workplace's drug policy (although this was only marginal for comparing psychological distress among workplaces with nonpunitive policies). For BIPOC employees, however, having a serious level of psychological distress was associated with a greater probability of reported opioid misuse for those with punitive workplace drug policies compared to those in serious distress with nonpunitive workplace drug policies; but for BIPOC employees without serious psychological distress, those with a nonpunitive workplace policy had greater rates of misuse than those with a punitive policy.
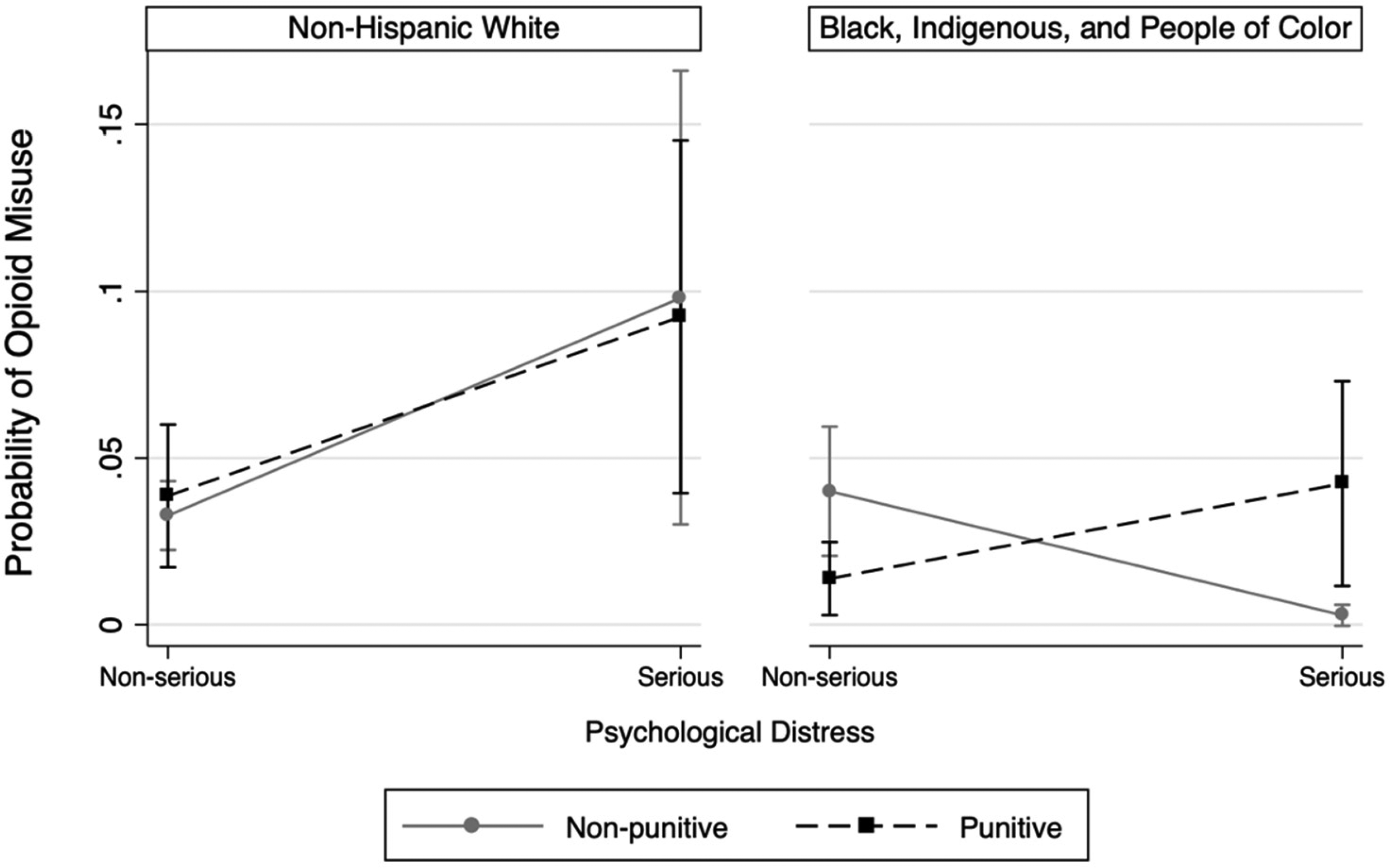
Predictive margins of opioid misuse by psychological distress and BIPOC identification.
Estimated Logistic Regression Models for Past Year Opioid Misuse by Past Year Serious K6 Score, Workplace Drug Policy, and Demographics (Model 3).
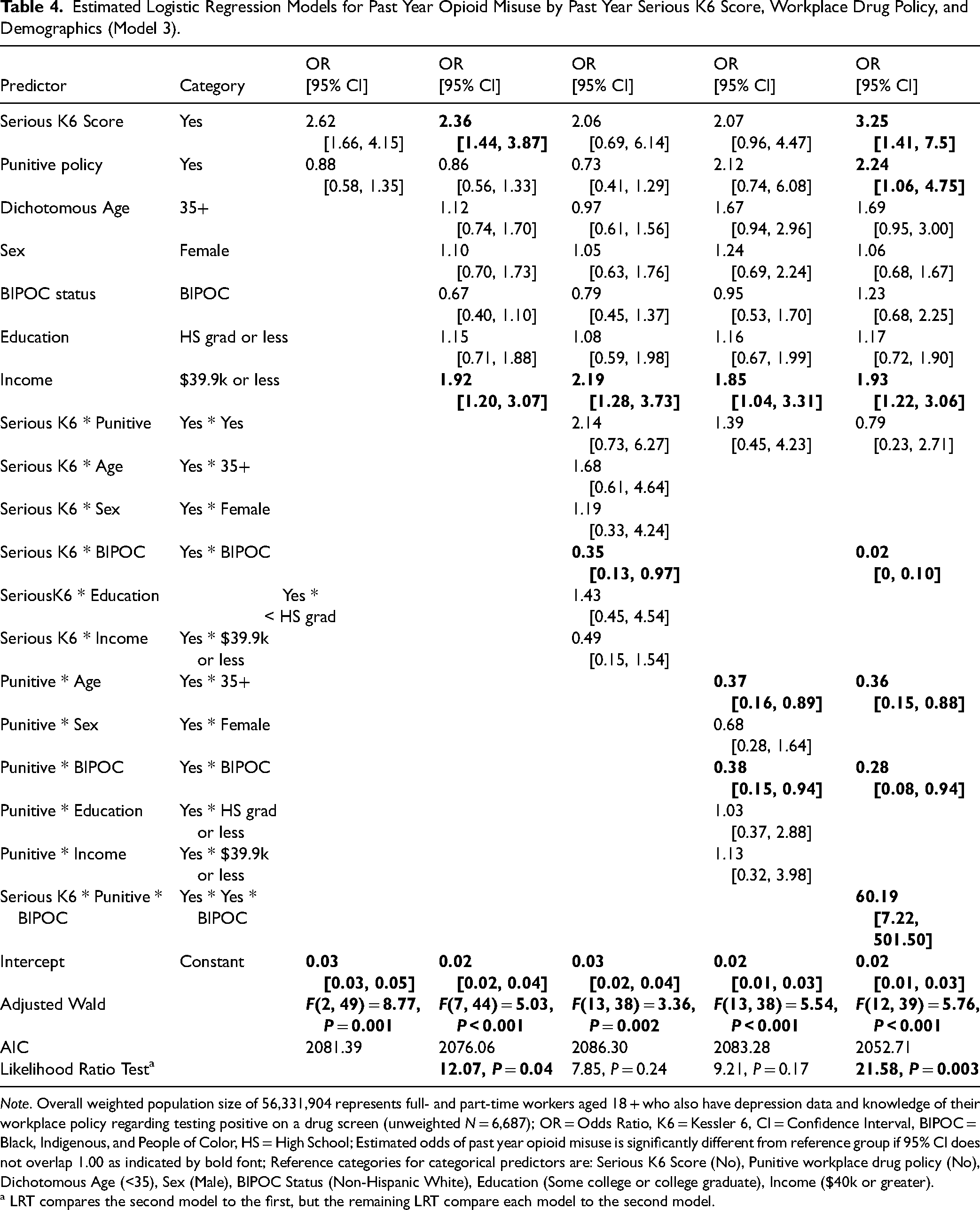
Note. Overall weighted population size of 56,331,904 represents full- and part-time workers aged 18 + who also have depression data and knowledge of their workplace policy regarding testing positive on a drug screen (unweighted N = 6,687); OR = Odds Ratio, K6 = Kessler 6, CI = Confidence Interval, BIPOC = Black, Indigenous, and People of Color, HS = High School; Estimated odds of past year opioid misuse is significantly different from reference group if 95% CI does not overlap 1.00 as indicated by bold font; Reference categories for categorical predictors are: Serious K6 Score (No), Punitive workplace drug policy (No), Dichotomous Age (<35), Sex (Male), BIPOC Status (Non-Hispanic White), Education (Some college or college graduate), Income ($40k or greater).
a LRT compares the second model to the first, but the remaining LRT compare each model to the second model.
Variation in Psychological Distress, Socioeconomic Status, and Workplace Characteristics by Race/Ethnicity
Table 5 shows the results of a post hoc exploratory analysis of the three-way interaction between BIPOC status, psychological distress, and workplace drug policies. Compared to NHW workers, BIPOC workers were significantly less likely to have serious psychological distress or meeting criteria for MDE; BIPOC workers had lower educational attainment and lower income relative to NHW workers. In terms of workplace characteristics, BIPOC individuals were more likely to work in places with substance use education, but less likely to work in places with substance use assistance programs, compared to their NHW counterparts. Although there were no differences in whether workplaces tested for drug use randomly, BIPOC workers were marginally more likely to report that their employer used drug testing for hiring purposes relative to NHW workers. Consistent with the main analyses, BIPOC workers were more likely to be employed in a workplace that had a punitive drug policy that is termination after a first offense of testing positive on a drug screen.
Weighted Characteristics of Non-Hispanic White and BIPOC Employees 18+.
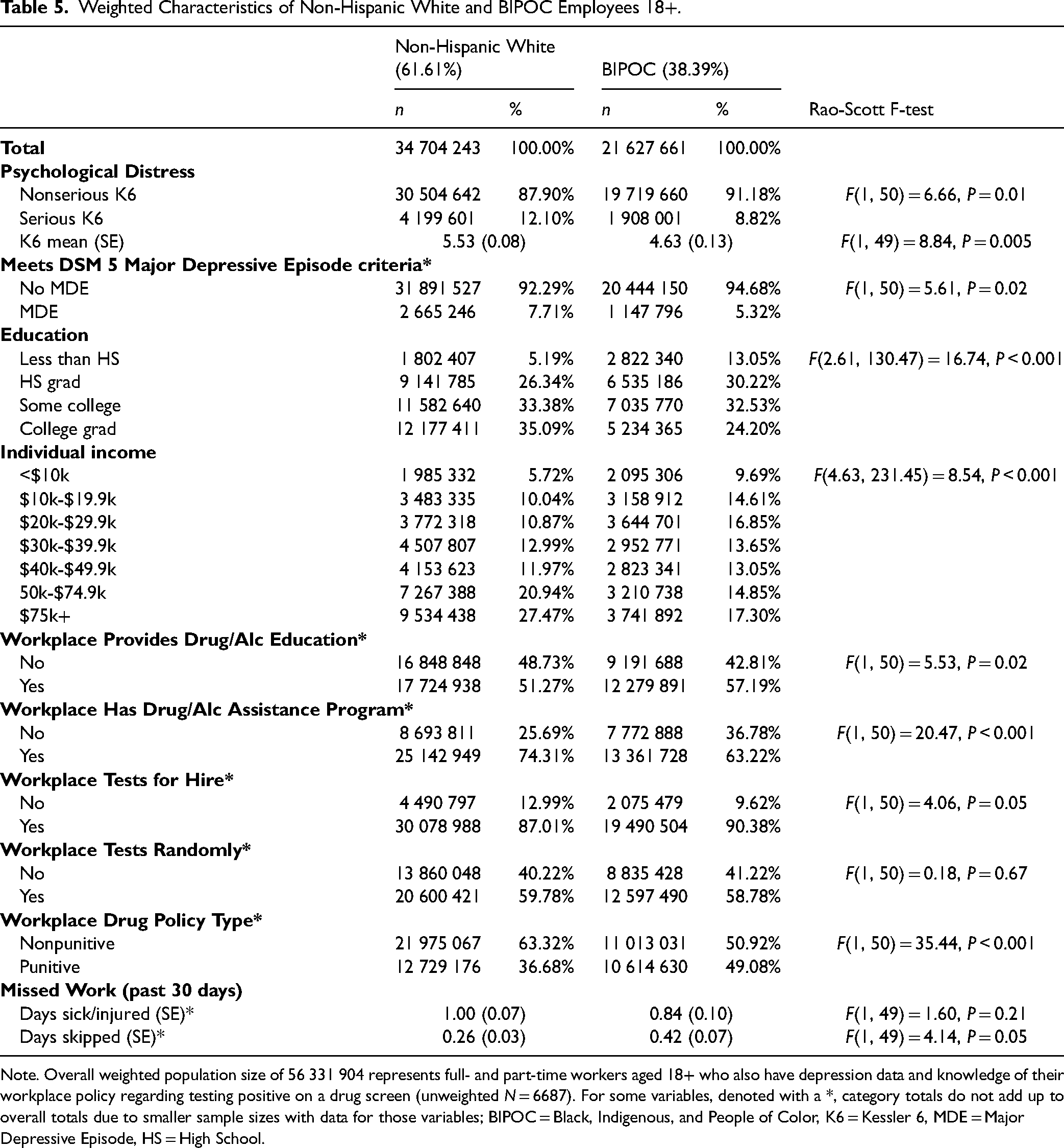
Note. Overall weighted population size of 56 331 904 represents full- and part-time workers aged 18+ who also have depression data and knowledge of their workplace policy regarding testing positive on a drug screen (unweighted N = 6687). For some variables, denoted with a *, category totals do not add up to overall totals due to smaller sample sizes with data for those variables; BIPOC = Black, Indigenous, and People of Color, K6 = Kessler 6, MDE = Major Depressive Episode, HS = High School.
Discussion
This study explored the intersections between punitive workplace drug policies, opioid misuse, and psychological distress utilizing the largest U.S. survey of drug use. We found that individuals with past year serious psychological distress were more likely to misuse opioids in the past year. Secondly, contrary to our hypothesis, we found that punitive workplace drug policies were not associated with opioid misuse overall; however there were important interactions with race/ethnicity and age that suggest more complex relationships Finally, the relationship between psychological distress and opioid misuse varied as a function of punitive workplace drug policies and race/ethnicity. Two of our three hypotheses were supported. In addition, stress—including work-related stressors—is a well-established risk factor in the development of addiction and vulnerability to relapse.34–38 The COVID-19 pandemic exacerbated the ongoing opioid epidemic and its interrelationship with psychological distress in the workplace, prompting calls for action from policy makers, business leaders, employers, and workers to take stock of how mental well-being is addressed in the workplace.39–41 Though some employers may believe that workplace drug testing policies are net-beneficial to workplace well-being because they reduce physical hazards, such as drug-related workplace accidents and illnesses, 17 this study's findings indicate that such policies may simultaneously interact in harmful ways with psychological distress and are not universally associated with lower opioid misuse among workers. The net result of workplace drug policies may harm worker well-being more than they help. Employers may conduct post-incident drug testing if there is a reasonable possibility that employee drug use could have contributed to the reported injury or illness. However, if employee drug use could not have contributed to the injury or illness, post-incident drug testing would likely only discourage reporting without contributing to the employer's understanding of why the injury occurred. Drug testing under these conditions could constitute prohibited retaliation. 42 This calls for contextualizing punitive workplace drug testing policies within a broader conversation about mental well-being. 42
Consistent with prior studies, we found that the prevalence of reported opioid misuse varied by race/ethnicity among this sample of currently employed U.S. adults. There are several reasons for this variation. The high rate of reported opioid misuse among NHW is thought to reflect, in part, greater access to prescription pain relief; many studies have shown that NHW are more likely to be prescribed opioids by physicians than their BIPOC counterparts in nonemergency and emergency situations.43–46 Additionally, workers with higher education and higher income employees were more likely to misuse prescription pain relievers than their respective BIPOC, lower education, and lower income counterparts, which may be indicative of differences in access to healthcare services. However, this may also reflect documented health care provider/prescriber biases and the false beliefs that BIPOC have higher thresholds of pain and therefore do not need prescription opioids, and/or perceptions that BIPOC are more likely to misuse the opioids and therefore are prescribed these medications at a lower frequency than NHW.43–46 Evidence that these racial/ethnic differences in opioid misuse persist within this sample of employed adults suggests that multiple mechanisms are likely relevant.
Workplace Drug Policies, Race/Ethnicity, and Psychological Distress
These findings show that the relationship between workplace drug policies, psychological distress, and opioid misuse differed by race/ethnicity. NHW workers with serious psychological distress, regardless of their employer's drug testing policy, were more likely to misuse opioids. In contrast, for BIPOC workers, psychological distress was associated with greater reported opioid misuse if their employer had a punitive drug testing policy. These findings align with the notion that punitive workplace drug policies can exacerbate existing disparities in the social determinants of health that are more prevalent among BIPOC individuals such as lack of health care access, loss of social support networks, and greater instability due to precarious financial situations compounded by the negative health effects of racism.47–50 Thus punitive workplace drug policies may worsen existing chronic stress giving rise to poorer health outcomes and increased psychological distress for BIPOC workers.
Practical Applications
The fact that the Surgeon General's report on workplace wellbeing was largely silent on opioid use/misuse itself is indicative that, while SUDs commonly co-occur with depression, burnout, anxiety, and otherconditions, they are often carved out from conversations about population mental well-being. 47 Below we offer recommendations at multiple levels to address the relationships among opioid use/misuse, psychological distress, and punitive workplace drug policies and their impact on workers.
Workplace/employer level
Apositive effect of the COVID-19 pandemic is greater acknowledgement that work is a determinant of health, and that the workplace can influence individual mental well-being for better or worse.51–53 While many workplaces are providing some mental health services to their employees (e.g., employee assistance programs) or supporting recovery friendly workplaces14,15,47 there is still much work to do to normalize providing and seeking mental well-being resources (e.g., SUD treatment, support, therapy). Each employer should develop and implement a protocol to address mental health crises in the workplace. This should include partnerships with community mental health centers, university practitioners and researchers, and other community-based organizations to get mental health experts to provide education and resources specific to each employer's workplace. Employers should provide routine confidential screening for depression and anxiety. This can be normalized by participating in national mental health screening days. In addition, each employer should develop and implement a plan to train employees in mental health first aid. Employers should display and provide information about mental health resources and community crisis services to their employees. 54 More workplaces should also adopt a recovery-friendly model. With current shortages in labor across all U.S. industries , more individuals with opioid use/misuse disorder or in recovery need to be recognized as an existing part of the workforce. A new analysis by the National Safety Council and NORC at the University of Chicago revealed that employers spend an average of $8817 annually on a worker with an untreated SUD—due to absenteeism, loss in productivity, and replacement—but those in recovery from a SUD can save up to $8500; moreover, employer-initiated treatment was more successful than treatment initiated by the workers’ families or friends. 55 The study also found workers in recovery missed 13.7 fewer work days than those with an untreated SUD and when actively in recovery, helped employers save $8175 in turnover, replacement, and healthcare costs. 55
It is important to recognize that the workplace itself plays a critical role in the opioid epidemic: it is a source forinjuries that are commonly treated with these medications.56,57 From a primary prevention perspective, employers and professionals who oversee workplace health (e.g., industrial hygiene [IH] or occupational and environmental health and safety [OEHS] professionals) should conduct worksite ergonomics assessments to reduce the musculoskeletal disorders (MSDs) which may lead to chronic pain, opioid prescription, and potential opioid use/misuse disorders.39,58,59 Robust primary prevention may include:
establishing formal ergonomics programs to prevent musculoskeletal disorders; using administrative controls, such as scheduling, to limit workload so as to not overburden workers; and addressing negative psychosocial factors (e.g., low supervisor support, high job demands, low job autonomy) that research has demonstrated does indeed affect workers’ mental and physical health outcomes, especially in relation to musculoskeletal disorders incidence.39,59–62
Workers’ compensation programs can make important contributions to secondary prevention by continuing to place limits on the quantity and circumstances under which providers can prescribe opioids and can require employers to shoulder the costs of nonpharmacological pain management approaches (e.g., physical therapy, acupuncture, massage therapy, etc.) to address acute and chronic pain caused by work-related injuries.63–65
It is important for organizations and employers to reassess their workplace drug policies to determine if they are net beneficial or not. Obviously, for the safety, productivity, and environment of the workplace, no one wants workers to perform their duties while physically and/or cognitively impaired. However, with an estimated 9% of the workforce (13.6 million workers) and nearly 9% (13.3 million) reported to be in recovery, 56 it is impractical to exclude these individuals from the workforce or jeopardize their livelihood with punitive workplace drug policies. Additionally, aforementioned, punitive drug policies may suppress injury and hazard reporting, in turn making it more challenging to identify and address hazards that may lead to injuries, opioid prescriptions, etc. 42 Moreover, turnover is extremely costly. The U.S. Department of Labor estimates that recruiting and training a replacement worker costs about 20% of the employee's annual salary and benefits. 66 Thus, it may behoove organizations and workers to critically analyze and revise their workplace drug policies.
State and federal government level
State governments and the federal governments are also working towards normalizing seeking mental well-being resources, as it relates to the workplace and opioid use/misuse. In November 2023, the Biden Administration released the Recovery-Ready Workplace Toolkit: Guidance for Private and Public Sector Employers in an effort to assist business and employers to respond more effectively to substance use/misuse, build their work force by hiring those in recovery, and develop a supportive work environment for recovery. 66 The toolkit also can be adapted to state and local governments, labor organizations, and nonprofits. This resource is one example of furthering the Nation's Drug Control Strategy to de-stigmatize SUDs by expanding employment opportunities for people in recovery and openly prioritizing it inthe nation's agenda. 66
From a federal policy level, it is necessary that the Occupational Safety and Health Administration (OSHA) draft a new ergonomics standard that reflects current day society, evidence-based research on MSDs, and the changing workforce. Without an OSHA standard to hold organizations and employers to, there will never be an impetus for workplaces to take it upon themselves unless they recognize the return-on-investment (ROI) ergonomic programs can bring, including decreasing the need for prescription opioids. Currently, ergonomics falls under the OSHA General Duty Clause but does not offer workers the number of protections needed for as costly as MSDs and other ergonomic issues are. 67 The last attempt at an ergonomics standard was over two decades ago but Senate Joint Resolution 6 rescinded that standard. The Congressional Review Act, “prohibits the agency from issuing a rule that is substantially the same as the former one.” 68 Thus, it is strongly recommended that OSHA lobbyists convey the need and potential benefit of an ergonomics standard for both workplaces and the economy so that Congress will repeal Senate Joint Resolution 6, making it possible for OSHA to re-issue the ergonomics standard.
Strengths and Limitations
There are several key limitations that should be considered when interpreting the findings of the results of this study. First, the NSDUH does not collect data from persons who are experiencing homelessness or housing instability, active-duty military personnel, or persons who are hospitalized or incarcerated; as a result, the prevalence of opioid use/misuse may be underreported, and our estimates cannot be generalized to these subpopulations. Second, the data collected are self-reported and therefore may be subject to recall bias and social desirability bias, although the audio-computer assisted self-interview (ACASI) data collection procedures used in this survey are considered the most reliable manner of collecting data on sensitive topics at scale. Third, some respondents did not know whether their workplace drug policies were punitive or not; those who did know their workplace drug policy was punitive may have been already directly impacted by such a policy and were more likely to be aware of it. Fourth, the NSDUH is cross-sectional, but this design is intentional, in part, to protect participant confidentiality and encourage truthful reporting. However, this means that causation cannot be inferred; we recognize there may be a bidirectional relationship between opioid use/misuse and psychological distress. Lastly, this study solely focused on opioids; looking at additional substances would have added more variables to the statistical models, making them unstable. While opioids are driving many nonfatal and fatal overdose rates in the U.S., it should be acknowledged there are other substances of concern for employers. This study also has several strengths: research questions and hypotheses were preregistered before analysis began and the data and scripts used for the analysis are publicly available, which increases the rigor and reproducibility of these findings. Additionally, the NSDUH is the most comprehensive survey of drug use in the U.S., and its findings are regularly used to inform policies around drug use and mental well-being.
Conclusion
Punitive workplace drug policies need to be re-assessed to reflect a comprehensive approach to promoting worker well-being while decreasing psychological distress. While a workplace policy is meant to apply to the entire employee workforce, it does not capture the impact and nuance of such policies on the intersectionality of individual identity (e.g., Black, low-income) and the social determinants of health. Punitive workplace drug policies (i.e., immediate termination upon first offense) may not be net-beneficial for the workplace well-being nor the psychological state of workers at scale, particularly for BIPOC individuals. Future research, ideally primary data collection conducted on a nationally representative sample, is needed to determine what impact (positive or negative) punitive workplace drug policies are having on the workplace (e.g., productivity, safety, turnover rates, etc.). The days of zero tolerance drug policies in the workplace must end in the face of the realities of today's workforce. We must continue to advocate for worker well-being, de-stigmatization of substance use disorders, and recognition of the workplace as a setting for interventions to improve health outcomes in and outside of work.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Eisenberg Family Depression Center at the University of Michigan.