
Abstract
There is an urgent need for stronger protection from aerosol-transmissible diseases in healthcare settings—for workers, patients, volunteers, and visitors. Concerned that the Centers for Disease Control and Prevention (CDC) Healthcare Infection Control Practices Advisory Committee (HICPAC) lacks diversity in expertise and experience and has not consulted widely with all concerned parties regarding a planned update to the 2007 Guideline for Isolation Precautions, a workshop was developed to consider the science and lessons learned before and during the COVID-19 pandemic. Sponsored by the New York/New Jersey Occupational Safety and Health Center, Preventing Aerosol-Transmissible Diseases in Healthcare Settings: The Need for Protective Guidelines and Standards was held on October 13, 2023, with these goals: describe current CDC/HICPAC infection prevention guidelines, review current scientific understanding of aerosol-transmissible pathogens, and consider perspectives from a wide range of groups currently excluded from the CDC HICPAC process.
Keywords
Introduction to the Document
There is an urgent need for stronger protection from aerosol-transmissible diseases in healthcare settings—for workers, patients, volunteers, and visitors. Concerned that the Centers for Disease Control and Prevention (CDC) Healthcare Infection Control Practices Advisory Committee (HICPAC) lacks diversity in expertise and experience and has not consulted widely with all concerned parties regarding a planned update to the 2007 Guideline for Isolation Precautions, a workshop was developed to consider the science and lessons learned before and during the COVID-19 pandemic. Sponsored by the New York/New Jersey Occupational Safety and Health Center, Preventing Aerosol-Transmissible Diseases in Healthcare Settings: The Need for Protective Guidelines and Standards was held on October 13, 2023, with these goals: describe current CDC/HICPAC infection prevention guidelines, review current scientific understanding of aerosol-transmissible pathogens, and consider perspectives from a wide range of groups currently excluded from the CDC/HICPAC process. The workshop report reviews the agenda, summarizes speaker presentations and stakeholder statements, and based on participant input, sets forth recommendations for updating the CDC infection control guidelines.
Executive Summary
There is an urgent need for stronger protection from aerosol-transmissible diseases in healthcare settings—for workers, patients, volunteers, and visitors. Concerned that the Centers for Disease Control and Prevention (CDC) Healthcare Infection Control Practices Advisory Committee (HICPAC) lacks diversity in expertise and experience and has not consulted widely with all concerned parties regarding a planned update to the 2007 Guideline for Isolation Precautions, a workshop was developed to consider the science and lessons learned before and during the COVID-19 pandemic. Sponsored by the New York/New Jersey Occupational Safety and Health Center, Preventing Aerosol-Transmissible Diseases in Healthcare Settings: The Need for Protective Guidelines and Standards was held on October 13, 2023, with these goals: describe current CDC/HICPAC infection prevention guidelines, review current scientific understanding of aerosol-transmissible pathogens, and consider perspectives from a wide range of groups currently excluded from the CDC HICPAC process. Scientific presentations, stakeholder statements, and participant input resulted in the following recommendations:
Ensure guidance is based on science by conducting a thorough review of the peer-reviewed literature from all relevant disciplines. Gather wider input from all groups who will be impacted by the updated guidance. Ensure guidance includes strong, clear, science-based requirements for infection prevention that do not allow flexibility for healthcare employers to prioritize costs over protecting patients and healthcare personnel. Fully recognize the role of aerosol transmission for many infectious pathogens. Recognize that numerous pathogens are transmissible via inhalation. Adopt the precautionary principle that novel pathogens are aerosol transmissible until demonstrated otherwise. Recognize and account for the role of asymptomatic/presymptomatic cases in aerosol transmission of diseases (e.g., influenza and SARS-CoV-2). Collaborate with the Occupational Safety and Health Administration (OSHA) and National Institute for Occupational Safety and Health (NIOSH) for essential expertise on occupational protections for healthcare personnel. Incorporate a multi-modal infection control strategy that relies on the hierarchy of controls. Establish prevention measures for the full range of healthcare settings. Establish clear, explicit, and robust standards for all healthcare facilities to improve indoor air quality through ventilation, filtration, and other measures. Recognize that NIOSH-approved respirators must be used to prevent healthcare personnel exposure to aerosol-transmissible diseases. Consider universal masking for source control for all healthcare personnel, patients, and visitors and broader use of respirators for healthcare worker, patient, and visitor personal protection. Address preparedness for outbreaks and pandemics of novel pathogens.
More details including recordings, presentation materials, and additional resources may be obtained on the workshop website.
1
The next HICPAC meeting is scheduled for November 2 and 3, 2023. Registration for oral comments has closed. Written comments may be submitted between November 1 and 6 to hicpac@cdc.gov.
Introduction
The massive toll of disease and death during the COVID-19 pandemic underscored the urgent need for stronger protections for aerosol-transmissible diseases. The Centers for Disease Control and Prevention (CDC) is currently updating the 2007 Guideline for Isolation Precautions through the Healthcare Infection Control Practices Advisory Committee (HICPAC).
Concerned about the lack of transparency in HICPAC's process for updating the 2007 guidelines and lack of input from a wide range of scientists and key stakeholders, including workers, patients, and their advocates, a letter was sent to the CDC Director requesting a more open, inclusive, and transparent decision-making process. The CDC responded that stakeholders must wait for the proposed revisions to be posted to the Federal Register for public comment.
This is too late to provide any meaningful input to the updated guidelines. There is still time for CDC to create a more inclusive process that considers the full range of science and lessons learned before and during the COVID-19 pandemic. With this in mind, a workshop Preventing Aerosol-Transmissible Diseases in Healthcare Settings: The Need for Protective Guidelines and Standards was arranged with the following goals:
Describe the purpose, content, audience, and application of the current (2007) CDC Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings and the 2022 Core Practices. Describe the current scientific understanding of:
Modes of pathogen transmission (e.g., inhalation of infectious aerosols vs droplet/airborne paradigm) Specific organisms that transmit person-to-person infection by aerosol inhalation, including influenza, SARS, SARS-CoV-2, RSV, noroviruses, etc. Risk factors for aerosol transmission (e.g., role of distance, duration of exposure, ventilation, and aerosol concentration) Controls for aerosol transmission (e.g., risk and exposure assessment, hierarchy of controls, effective controls) Reflect upon and consider the perspectives of stakeholders currently excluded from the CDC/HICPAC process. Recommend updates to the current guidelines:
Ensure updated guidance is consistent with and does not undermine federal and state Occupational Safety and Health Administration (OSHA) infectious disease and related standards. Consider other healthcare settings in addition to acute care hospitals, such as home health, corrections, and skilled nursing facilities.
The workshop, sponsored by the New York/New Jersey Occupational Safety and Health Center, was held online from 12-3 PM ET on October 13, 2022. More than 900 people from a wide range of backgrounds registered for the workshop and 490 attended the online session.
Recommendations
During registration individuals were asked to make recommendations for revisions and updates to the 2007 Guideline for Isolation Precautions. Throughout the workshop, participants were asked to respond as often as they wanted to the following question: Based on today's presentations and your experience, what should CDC include in its revision of the healthcare infection control guidance?
The Planning Committee reviewed these responses in addition to input from workshop speakers to arrive at the following set of recommendations for CDC and HICPAC's update to the 2007 Guideline for Isolation Precautions:
Include patient advocates and healthcare personnel from a wide range of healthcare settings in the development and review of the guidelines.
Correct the false dichotomy of near/droplet versus far/airborne transmission. Recognize that respiratory aerosols are emitted in a wide range of sizes, can travel long distances, may stay suspended in the air for long periods of time, and can be inhaled near and far from a source. Incorporate expertise from industrial hygienists and aerosol scientists.
Update the guidelines to include influenza, RSV, adenovirus, MERS, SARS-CoV-2, norovirus, and pertussis, among others, as aerosol-transmissible diseases. Recognize that endemicity and seasonality do not determine protective measures for aerosol-transmissible pathogens.
Consider pre-procedure/pre-admission testing of patients for such pathogens.
Require compliance with the OSHA Respiratory Protection and other applicable standards.
Establish appropriate measures across hospitals, long-term care/nursing facilities, home health, outpatient clinics, physician offices, prisons and jails, dental care settings, etc.
Review relevant existing recommendations and standards and incorporate expertise from ventilation engineers and experts. Require updates to ventilation, filtration, and similar measures in all healthcare settings. Increase capacity for isolation of patients with aerosol-transmissible diseases. Require reporting of air quality measures to patients and healthcare personnel. Acknowledge that surgical/medical masks cannot be used as respiratory protection against hazardous aerosols. Require employers to conduct a risk assessment and prepare an exposure control plan, including identifying higher-risk situations where higher levels of respiratory protection are warranted. Emphasize that respirators must be worn within the context of an OSHA-compliant respiratory protection program.
Require personal protective equipment (PPE) stockpiles, emergency staffing plans, and plans for expanding or modifying ventilation and isolation practices. Require stockpiling of NIOSH-certified N95 filtering facepiece, elastomeric, and powered air-purifying respirators.
Program
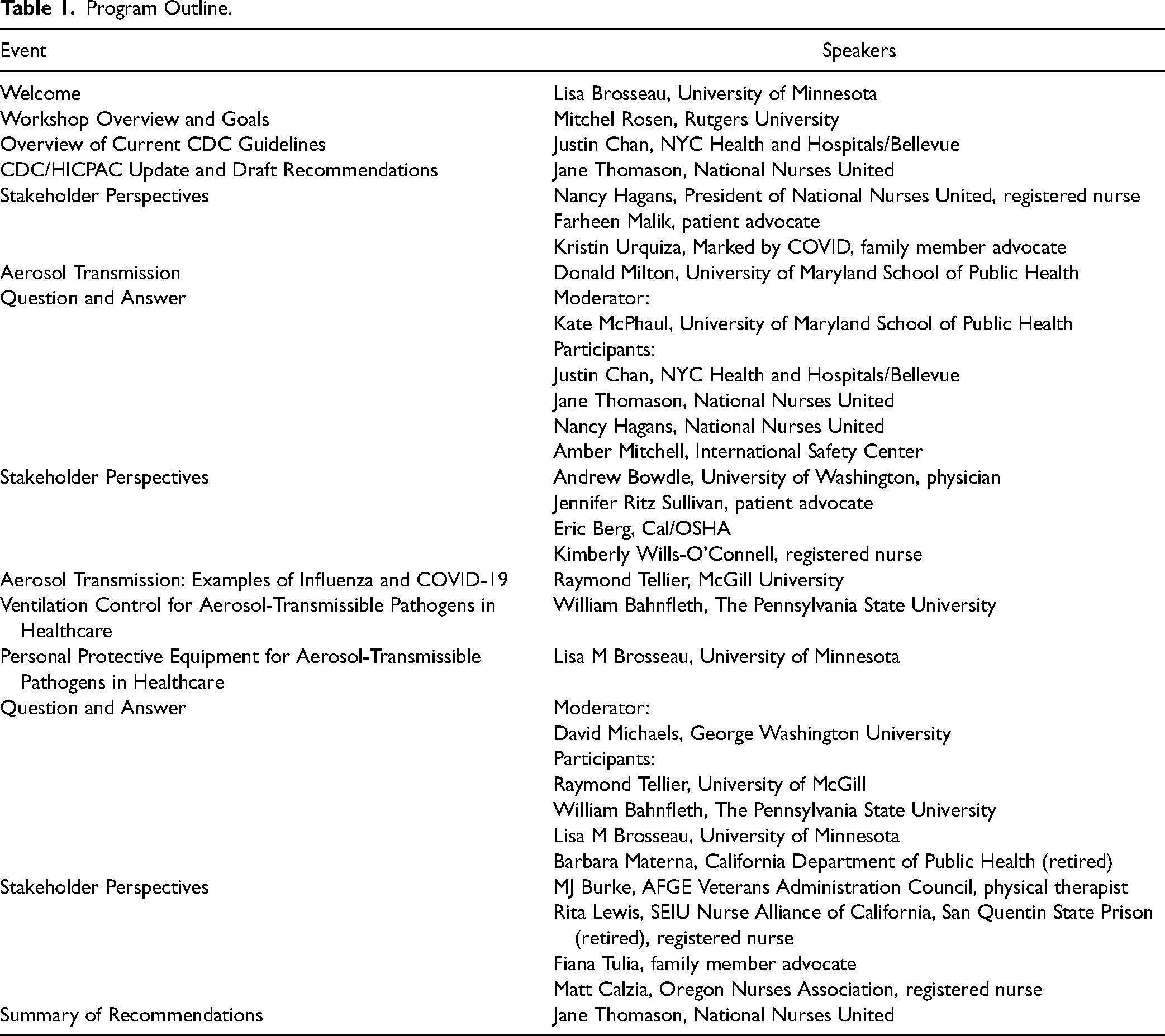
The program consisted of 3 sets of presentations, 3 sessions of stakeholder statements, and 2 question and answer sessions (Table 1). Speaker recordings and presentations can be accessed on the workshop website. Speaker biographies can be found at the end of this report.
Program Outline.
Presentations
Overview of Current CDC Guidelines for Isolation Precautions
Dr. Justin Chan from NYC Health + Hospitals/Bellevue addressed the 2022 Core Infection Prevention and Control Practices for Safe Healthcare Delivery in All Settings. These practices are considered fundamental standards of care for infection prevention and control for all settings where healthcare is delivered, including inpatient, outpatient, homes, pharmacies, etc., and all healthcare personnel with potential exposure to infectious patients or materials. The Core Practices address leadership support and accountability, assurance of sufficient resources, education and training of healthcare personnel, education of patients, families and caregivers, and performance monitoring and feedback.
Dr. Chan then described CDC's Standard and Transmission-Based Precautions. The former apply to all patient care in all settings, irrespective of a patient's infectious status, and include hand hygiene, environmental cleaning and disinfection, injection and medication safety, use of appropriate PPE commensurate with activities, methods for minimizing potential exposures such as point of entry screening, and reprocessing of reusable medical equipment. Transmission-Based Precautions include additional measures for patients with suspected or confirmed diagnoses where exposure poses a significant risk of transmission beyond the use of standard precautions. These must be implemented as soon as there is a suspected diagnosis and communicated to all care providers.
Dr. Chan noted that the current CDC guidelines discuss 3 modes of transmission: direct or indirect contact, droplet, and airborne. Precautions for contact transmission include a single room (preferred) or at least 3 ft. of separation between beds in multi-patient rooms and the use of gowns and gloves by healthcare personnel. Droplet precautions also call for a single room, if possible, or beds separated by 3 ft. and a curtain in multi-bedrooms and a medical mask. Airborne precautions require an airborne infection isolation room (AIIR) and N95 filtering facepiece or higher-level respirators. He noted, however, that transmission of respiratory diseases is not dichotomous, and the droplet versus airborne paradigm may not accurately represent exposure to infectious aerosols.
Dr. Chan noted that worker health and safety is very important to infection control and prevention. He mentioned the importance of immunization, sick leave policies that avoid presenteeism, and policies that implement OSHA standards for bloodborne pathogens, personal protective equipment, respirators, and the OSHA tuberculosis compliance directive.
HICPAC's Process and Proposals to Update the 2007 Isolation Precautions Guidance
Jane Thomason from National Nurses United (NNU) explained that HICPAC, governed by the Federal Advisory Committee Act (FACA), consists of 8 members with expertise in infection control and prevention who are affiliated with large healthcare corporations and universities. There are also 5 ex-officio members from other Health and Human Services agencies and 23 liaisons. None of the latter represents front-line healthcare workers or their representatives.
HICPAC convened an Isolation Precautions Work Group to propose updates to the 2007 Guidance on Isolation Precautions. The Work Group began closed meetings in February 2022 in meetings and presented updates and summaries of some proposals to HICPAC at quarterly public meetings.
NNU submitted Federal Advisory Committee Act (FACA) and Freedom of Information Act (FOIA) requests for Work Group minutes, drafts, and other documents to CDC, which were initially rejected. Recently, Work Group meeting summaries from February 2022 through May 2023 were shared with NNU, which made them publicly available: https://www.nationalnursesunited.org/cdc-hicpac-work-group.
NNU's review of these materials concluded that:
The HICPAC Work Group prioritized feasibility and flexibility over robust protections. The Work Group has been focused on recommending fewer precautions than in the current guideline for ventilation, respirators, gowns, and gloves. The Work Group states that they rely on their own “expert opinion” where scientific evidence is lacking.
In June 2023 the Work Group proposed 2 new transmission pathways of “air” and “touch” to replace “droplet” and “airborne.” Pathogens would be identified as spreading through a major pathway, although minor pathways might contribute to spread. Pathogen transmission epidemiology would be informed by observing patterns of infection spread.
Jane Thomason discussed the Work Group's Evidence Review for surgical masks versus respirators, presented at the June 2023 HICPAC meeting and concluded that it was biased. The Work Group cherry-picked data excluded an essential randomized controlled trial by MacIntyre et al. 2 that evaluated continuous use of N95 respirators, excluded the extensive body of laboratory and workplace research on the effectiveness of respirators against hazardous aerosols, included flawed studies, and failed to evaluate whether respirators were used in the context of an OSHA-compliant respirator program.
The Work Group's proposals for precautions to prevent transmission by air are two-fold. Routine Air Precautions would require medical or surgical facemasks and no AIIR for pathogens like seasonal influenza and seasonal coronaviruses, which does not recognize their well-established potential for aerosol inhalation. Novel Air Precautions would require an N95 respirator and eye protection but no AIIR for diseases like MERS, SARS-CoV-1, and “pandemic-phase” SARS-CoV-2. This is a downgrade from the 2007 guideline for “airborne” diseases and current practices for these pathogens. Extended Air Precautions would be reserved only for diseases like tuberculosis, measles, and varicella, which are currently classified as “airborne” and require respirators and AIIR.
Important shortcomings of the HICPAC process were then discussed. The Work Group does not seek any input from the public and has been unwilling to engage with additional experts. When the Work Group presents its updates and expert opinions to HICPAC for review and discussion, there is limited opportunity for public input. The Work Group's written documents are not shared with the public prior to the HICPAC vote, and historically HICPAC has voted prior to hearing public comments. By the time the proposed changes are approved and sent to CDC for posting to the Federal Register, it will be difficult for the public to have any impact on the revisions. Participants were encouraged to register and comment at the November 2 and 3, 2023, HICPAC meeting.
Protecting the Workforce From Aerosol Transmission of Communicable Respiratory Pathogens
Dr. Donald Milton, University of Maryland School of Public Health, described the current understanding of respiratory pathogen transmission, which he places in 3 categories: inhalation, spray, and touch. He emphasized that inhalation could occur both near and far from an infected source, while spray is only likely when very near a source. He pointed out the significant proportion of respiratory disease transmission that occurs via asymptomatic infections. For influenza, 70% of those are infected each year and develop a new immune response but do not experience any symptoms. This “iceberg” of infections means that it should be assumed that everyone—patients and staff—could be infected and contagious, which means that local exhaust ventilation and masks or respirators used only for known or suspected cases will not be effective at limiting transmission. Rather, source control must be used for everyone in the facility.
Dr. Milton noted that respirators are significantly superior to face masks as source control, as demonstrated by his and others’ research. In research being prepared for publication, Dr. Milton found that N95 respirators had only 2% outward leakage of infectious aerosols from human subjects, while KN95 respirators and surgical masks had outward leakage of 30%, and cloth masks were generally ineffective with 87% outward leakage. Finally, Dr. Milton discussed the importance of pathway or engineering controls, including ventilation, filtration, and air disinfection.
Aerosol Transmission: The Examples of Influenza and COVID-19
Dr. Raymond Tellier from McGill University discussed the scientific data that support aerosol inhalation as an important mode of transmission, using influenza and COVID-19 as examples. He noted that there are several decades of evidence for aerosol transmission. Influenza A is seasonal but can become pandemic. In laboratory experiments, influenza A is capable of remaining viable for many hours at low relative humidity. It is possible to recover viable aerosols from the exhaled breath of influenza-infected individuals, although culturing viruses is difficult because the methods are not very sensitive. Several studies have also demonstrated there is influenza A present in air samples from hospital settings as well as at least 1 study that has shown viable virus.
A study in the 1960s with human subjects demonstrated that it was possible to cause infection by aerosol exposure. The infectious dose by aerosol was 100 times less than by intranasal exposure (droplets). The aerosol route replicated all of the symptoms of influenza, while intranasal instillation produced a much milder disease. This is an example of anisotropic infection, where different routes of transmission have different infectious doses.
Dr. Tellier described several studies of influenza outbreaks demonstrating aerosol transmission. He also noted that there are several animal models that have demonstrated aerosol transmission and described a study showing that novel H1N1 influenza is much more capable of transmitting by aerosols than the usual influenza A strains.
Dr. Tellier then described the same types of data for COVID-19 that support aerosol transmission. He also noted that other viruses, such as adenovirus, are likely to be aerosol transmissible.
Ventilation Control for Aerosol-Transmissible Pathogens in Healthcare
Dr. William Bahnfleth from the Pennsylvania State University described the role of ventilation for controlling aerosol transmission in healthcare settings. In April 2020 the American Society of Heating, Refrigerating, and Air-Conditioning Engineers (ASHRAE) stated that transmission of SARS-CoV-2 through the air was sufficiently likely that aerosol exposure to the virus should be controlled. The next year was spent arguing with public health officials about the truth of that statement. He noted that there is evidence that environmental controls can make a difference in preventing or amplifying transmission.
Dr. Bahnfleth noted that indoor ventilation is more than bringing in outdoor air. It is defined by ASHRAE as outdoor air plus recirculated air that has been treated by filtration to remove particles. He then discussed a new ASHRAE standard, 241-2023, Control of Infectious Aerosols, and the use of “equivalent air flow” as a unifying concept. Methods for treating recirculated or room air can be accomplished with dilution, filtration, or disinfection. Local exhaust can also be used near the source, such as on a patient bed. Pressurization can also be used to manage the direction of airflow. Germicidal ultraviolet irradiation has also been used for many years in certain settings.
Dr. Bahnfleth then discussed the importance of ensuring that clean air is delivered where it is needed. Thus, airflow direction matters as much as the quantity of air. There is still much more to learn about managing airflow direction.
He described current standards relevant to healthcare settings, including the recent ASHRAE 241 which includes several healthcare spaces with relatively high required airflow rates (e.g., surgical suites, AIIR). ASHRAE/ASHE 170 indicates a wide range in outdoor air, supply air, and types of filters for recirculating air requirements for different healthcare spaces. He noted, however, that many spaces where COVID-19 infections occurred, such as staff breakrooms, are not covered by ASHRAE standards or guidelines: “We can’t just focus on these special environments.”
Areas of concern that warrant improvements to standards include response to surge capacity in hospitals, protection in non-critical spaces, and ventilation in outpatient and residential care facilities. Dr. Bahnfleth concluded that there are strong reasons to make healthcare standards more stringent.
Personal Protective Equipment for Aerosol-Transmissible Diseases in Healthcare
Dr. Lisa Brosseau from the University of Minnesota discussed the importance of the hierarchy of controls in selecting interventions for worker and patient safety, with a focus on source and pathway controls. She noted that workplace studies have demonstrated that respirators are effective when used properly, and there is no reason to conduct a clinical study of respirator performance in healthcare settings. She described the features of surgical masks that make them inappropriate for preventing aerosol inhalation or as source control for human-generated aerosols.
Dr. Brosseau then discussed the importance of fit testing and why it is required for workers to wear respirators in all workplace settings. She noted that elastomeric respirators could have prevented the supply chain issues experienced during the pandemic and freed up filtering facepiece respirators for other workers. Wearing filtering facepiece respirators for many hours can lead to skin damage and other stresses, which can be prevented by taking breaks and possible use of skin protectants or barrier creams.
Dr. Brosseau then reviewed a few studies demonstrating positive impacts of universal surgical mask or respirator use during the pandemic, which indicates that the HICPAC Work Group should be conducting a more thorough review of the scientific literature for this intervention.
She noted a Cochrane study of infection control guidelines that found that patients and workers were infected in healthcare settings when guidelines were not adequate, implemented, or followed. The review recommended that workers should be included in policymaking and implementation and workers need better communication, management support, training, and access to PPE.
Dr. Brosseau recommended that the HICPAC guidelines need to be based on science and lessons learned from SARS, n-H1N1, and COVID-19. As well, they must be aligned with OSHA PPE standards. She noted that there were numerous peer-reviewed scientific articles addressing necessary improvements based on experiences from the COVID-19 pandemic.
(Citations to studies mentioned here can be found in Dr. Brosseau's presentation, which is posted on the workshop website.)
Stakeholder Statements
Patients, patient advocates, family members, healthcare workers, healthcare worker advocates, and a state OSHA official joined the workshop to present their first-hand experiences on the need for strong infection control guidelines and practices in healthcare settings.
Farheen Malik: Patient and Patient Advocate, People's CDC
Farheen Malik lives with multiple chronic illnesses that put her at high risk for severe outcomes from COVID-19 or other infections. Despite her self-advocacy and need for regular support, access to safe healthcare has been difficult since masks became optional for her providers, and this has exacerbated her health challenges, including delaying needed diagnoses, treatment, and surgery. CDC's updated guidelines need to recognize aerosol transmission of diseases and should include provision and utilization of N95 respirators, ventilation, and universal masking to protect high-risk individuals, all patients, and healthcare workers.
Jennifer Ritz Sullivan: Disabled Patient
Jennifer Ritz Sullivan is disabled and suffers from chronic illnesses that put her at high risk if she contracts COVID-19 or other infections. She lost her mother from COVID-19 in 2020, and early this year she contracted COVID-19 despite being up to date on COVID vaccinations. She was very ill and now is further disabled by long COVID. Her healthcare center has dropped requirements for masking, and each visit requires multiple requests asking healthcare providers to mask, with some providers becoming hostile and uncooperative. No one should be forced to subject themselves to disability or death to receive medical care. [Jennifer Ritz Sullivan, Disabled individual and long COVID sufferer]
Fiana Tulip: Family Member Advocate
Fiana Tulip's mother, Isabelle Papadimitriou, was a Hispanic respiratory therapist in Dallas who spent her life helping others breathe. She was infected by COVID at the hospital where she worked and died a week later in July 2020. Isabelle was not informed if her patients were COVID positive and received no training or respiratory protection, only expired surgical masks, and no COVID tests. We need a change now in healthcare facilities—better infection control, respirators, education, and training to protect healthcare workers who are the backbone of our healthcare system. I implore the CDC and HICPAC to heed our experiences, respect the science, and truly recognize the lasting toll of these diseases. We must reinstate our healthcare institutions as safe havens, ensuring not a single additional life is needlessly lost. [Kristen Urquiza, Patient advocate]
Kristin Urquiza: Patient Advocate, Marked by COVID
Kristin Urquiza lost her father, Mark, to COVID in 2020. Her mother was also infected and survived, but was not unscathed and has been battling long COVID for more than 3 years. Her mother's health is in continued decline, and she faces surgery and a potential cancer diagnosis. Kristin's predominant fear is not the procedure nor cancer but her mother's potential exposure to COVID while in a hospital setting. The anguish of potentially losing her only other parent is overwhelming.
Andrew Bowdle, MD: Healthcare Provider
Andrew Bowdle is a cardiac anesthesiologist, who along with his colleagues has taken steps throughout the COVID pandemic to protect themselves and patients by wearing N95 respirators throughout the hospital and using HEPA-rated air purifiers in their offices, practices that were much more protective than their hospital's policies.
The lack of these stronger measures led hospitalized patients to become infected with COVID-19, some of whom died. He advocates the use of universal masking with N95 respirators whenever possible during substantial prevalence of aerosol-transmissible diseases and urges CDC to include these measures in the new infection control guidelines. In addition to protecting ourselves, we are very concerned about protecting our patients, many being elderly, immunosuppressed and with other risk factors. We have seen patients become infected with COVID-19 while hospitalized and some of those patients have died of COVID-19. We believe that in many instances these patients were not protected as well as they could have been. [Andrew Bowdle, MD, Healthcare Provider]
MJ Burke: Physical Therapist, Veterans Administration Council, American Federation of Government Employees
MJ Burke is a physical therapist and represents healthcare workers at Veteran's Administration (VA) facilities. The VA used to have a robust safety and respiratory protection program including the use of elastomeric respirators, but resources were cut, and the program deteriorated. Many of the healthcare workers at the VA, including physical therapists, work in very close physical contact with patients, often face to face. These workers were provided only surgical masks during the early stages of COVID-19 and couldn’t get respirators; many were infected. The CDC guidelines need to require stockpiling of respirators, including elastomerics, regular fit testing, and regular and frequent training on infection control including donning and doffing of respirators and PPE.
Matt Calzia: Registered Nurse, Oregon Nurses Association
Matt Calzia has been heavily involved in efforts to protect nurses from COVID-19 and other infectious diseases and served on Oregon OSHA's advisory committee for an emergency standard on COVID-19. Healthcare employers opposed proposals for a strong COVID-19 standard, including respiratory protection, claiming that there was no aerosol transmission of COVID-19. When workers bought their own more protective respirators, including elastomerics, they were faced with discipline if they used them at work. The Oregon OSHA COVID-19 standard is no longer in effect, but healthcare workers continue to be infected causing outbreaks, widespread staff absences, and severe disruption to the provision of needed medical care.
Nancy Hagans: Registered Nurse, President, National Nurses United and New York Nurses Association
Nancy Hagans has been a nurse for 37 years and works at a hospital in Brooklyn, NY, that was at the epicenter of the COVID-19 pandemic. The hospital was unprepared, and the nurses had to fight to get PPE. Many employers had N95 respirators in storage but locked them up and wouldn’t provide them to staff; nurses were forced to use surgical masks or reuse respirators for many shifts. Employers maintained that they were following CDC guidelines, which had been weakened to give employers greater flexibility to prioritize profits. Many patients, healthcare workers, and their family members were infected. Many nurses have quit and left the profession due to the lack of safety and health protections. A rollback in CDC infection control guidelines will worsen conditions and undermine patient care.
Rita Lewis: Registered Nurse, SEIU Nurse Alliance of California
Rita Lewis worked for 15 years as an RN in California's state corrections facilities, most recently at the San Quentin State Prison. While there are a lot of written procedures for protecting patients and inmates, they are not and were not followed during COVID-19. There was no attempt to limit the movement of or contact with people. There was no screening when inmates were transferred and a lack of testing and infection control, leading to tens of thousands of infections and hundreds of deaths. Many correction facilities received fines—over $400,000 for San Quentin—for their failure to protect workers, but these were paid out of taxpayer dollars, and no one in the management was held responsible for these failures. Today, workers and inmates face RSV, influenza, and COVID-19, but nothing has changed—there's no PPE, no training, no improved ventilation, or no additional infection control measures. Healthcare workers and inmates remain at risk.
Kimberly Wills-O’Connell: Registered Nurse, Pennsylvania Association of Staff Nurses and Allied Professionals
Kimberley Wills-O’Connell has been a critical care nurse for more than 30 years and works in the Philadelphia area. She along with other healthcare workers was on the frontline of the COVID-19 pandemic with little support and inadequate protection. The mixed messages from CDC about how the virus was transmitted and appropriate mitigation measures created chaos and mistrust and caused unnecessary infections and deaths. The inability of healthcare workers to provide proper care for patients, holding their hands while they suffered and died, left deep emotional scars. Healthcare workers want CDC and HICPAC to rectify the damage and the mistrust that has been caused as the agency updates the infection prevention guidelines, by being transparent, disclosing the science being considered, opening up the process, inviting the participation of others, and issuing guidelines that protect public health and safety in the future. We were unarmed warriors sent to fight a hopeless battle with no leadership. [Kimberly Wills-O’Connell, critical care nurse]
Eric Berg: Deputy Chief of Health, California Division of Occupational Safety and Health (Cal/OSHA)
Early in the pandemic in February 2020, California's state OSHA plan issued written guidance that COVID-19 should be treated as an airborne infectious disease requiring NIOSH-approved respirators, specific training, source controls, ventilation, and other controls to protect healthcare, corrections, and other workers exposed on the job. These measures were and continue to be required for COVID-19 and other infectious diseases by law under California's Aerosol Transmissible Disease standard. CDC's failure to recognize COVID-19 as airborne and its much weaker infection control recommendations than California requirements created much confusion, with many employers not complying with the ATD standard, which led to deadly outbreaks. NIOSH-approved respirators, not surgical masks, are necessary to protect workers from airborne particles, including the SARS-CoV-2 virus. Weak, less effective HICPAC/CDC infection control guidelines will continue to create confusion and undermine California's strong protections for healthcare workers. To state there is no difference in the effectiveness of a surgical/medical mask and a NIOSH-approved respirator to prevent transmission of airborne diseases is false, is unacceptable, puts workers in danger and is not supported by science.[Eric Berg, Cal/OSHA]
Workshop Attendees
A total of 937 people registered for the workshop, and 490 were in attendance. Employment was fairly evenly distributed across academia, government, non-profit, and private industry (Table 2). The majority of registrants were from the United States (87%) and Canada (5%); the remainder were from 34 other countries or territories.
Registrant Demographics (Total = 937).
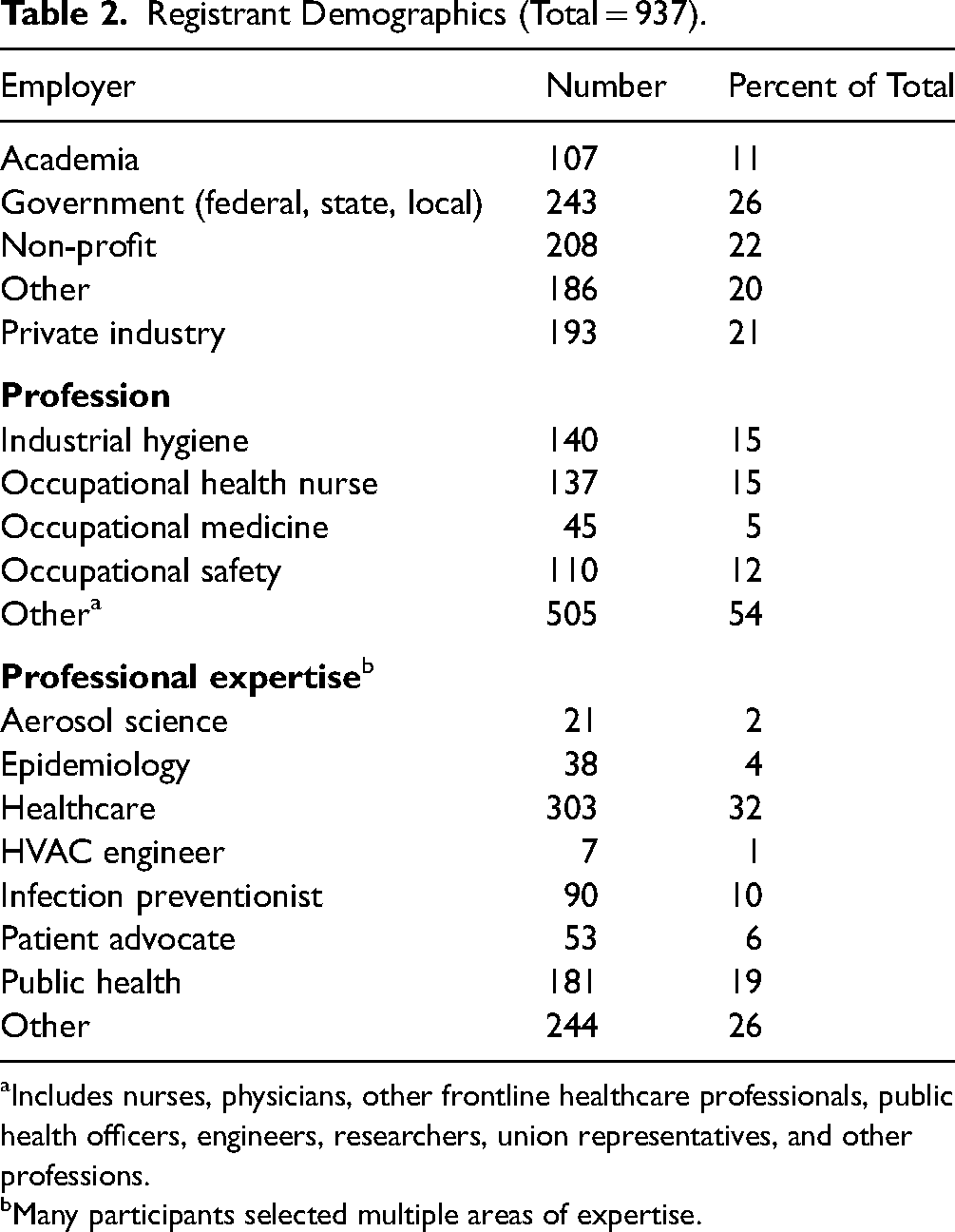
Includes nurses, physicians, other frontline healthcare professionals, public health officers, engineers, researchers, union representatives, and other professions.
Many participants selected multiple areas of expertise.
Planning Committee
Lisa M. Brosseau, University of Minnesota, Center for Infectious Disease Research and Policy
Deborah (Deeg) Gold, California Division of Occupational Safety and Health (Cal/OSHA) (retired)*
Kathleen Harriman, California Department of Public Health*
Barbara Materna, California Department of Public Health (retired)*
Kate McPhaul, University of Maryland School of Public Health
Jonathan Rosen, AJ Rosen and Associates, LLC
Mitchel Rosen, Rutgers School of Public Health
Peg Seminario, AFL-CIO (retired)
Jane Thomason, National Nurses United
*Organization listed for identification purposes only. The Workshop Speaker Biographies are added as an Appendix in the article.
Workshop Co-Sponsors
American Federal of Labor and Congress of Industrial Organizations (AFL/CIO)
American Industrial Hygiene Association (AIHA)
Occupational Health Section of the American Public Health Association (APHA)
Association of Occupational Health Professionals (AOHP)
Association of Occupational and Environmental Clinics (AOEC)
Canadian Aerosol Transmission Coalition
Health Watch USA
National Emerging Special Pathogens Training and Education Center (NETEC)
People's CDC
University of Maryland School of Public Health
University of Minnesota Center for Infectious Disease Research and Policy (CIDRAP)
Footnotes
Acknowledgments
We thank our co-sponsors and the many individuals and organizations that helped us advertise the workshop. We thank all the presenters and speakers who shared their expertise, views, and experiences and all the attendees for their active participation. We thank, in particular, Dr. Mitchel Rosen and the team at the Center for Public Health Workforce Development at the Rutgers School of Public Health for their timely and skillful assistance and willingness to host this workshop with very limited lead time.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.