
Abstract
An exploratory qualitative case study investigated how different sectors of a highly industrialized community mobilized in the 1990s to help workers exposed to asbestos. For this study, thirty key informants including representatives from industry, workers, the community, and local politicians participated in semi-structured interviews and focus groups. The analysis was framed by a “Dimensions of Community Change” model. The informants highlighted the importance of raising awareness, and the need for leadership, social and organizational networks, acquiring skills and resources, individual and community power, holding shared values and beliefs, and perseverance. We found that improvements in occupational health and safety came from persistently communicating a clearly defined issue (“asbestos exposure causes cancer”) and having an engaged community that collaborated with union leadership. Notable successes included stronger occupational health services, a support group for workers and widows, the fast-tracking of compensation for workers exposed to asbestos, and a reduction in hazardous emissions.
Introduction
More than 30% of cancer deaths, according to the World Health Organization, 1 could be prevented by modifying or avoiding key personal risk factors. A report from the Canadian Cancer Society and Cancer Care Ontario states that over 50% of cancers that will be diagnosed over the next twenty years, caused by individual lifestyle factors and occupational and environmental exposures, could be either prevented or detected early before they become a serious health problem. 2 This study focuses on the occupational exposures that are preventable. Since it is estimated that 8.0% to 19.2% of just lung cancer in American men can be directly attributed to workers being exposed to occupational hazards, 3 it is important to reduce the exposure of vulnerable workers to workplace carcinogens such as asbestos, nickel, silica, diesel, benzene, and many other substances.4–6 However, raising public awareness of the carcinogenicity of occupational hazards is not easy, and more importantly, even when there is awareness of exposures, there is still the question of how to raise awareness of the impact on worker health and encourage the prevention or reduction of exposures to workplace hazards.
This gap between awareness and taking action has been investigated by numerous fields of inquiry, including public health, psychology, sociology, and in particular, the field of knowledge transfer (KT). Awareness seems to be necessary for change, but it is not always sufficient to lead to action. For example, society has known with reasonable certainty for many decades, maybe for more than a century, that asbestos can cause cancer, 7 and asbestos exposure is the single largest on-the-job killer in Canada, accounting for more than a third of total workplace death claims approved last year and nearly a third since 1996. 8 Despite this awareness, change has been very slow, socially, economically, and legally. The last asbestos mine in Canada closed as recently as 2011, and shockingly, according to Statistics Canada figures, imports of asbestos-related items rose to C$6-million last year from C$4.9-million in 2013 and exports continue. 9
The objective of this exploratory study was to try to understand what helps to bridge the gap between awareness of occupational exposures and taking action to reduce exposure and protecting workers who have been exposed. This question is fundamental to the field of KT. The study of KT (commonly known in the United States as dissemination and implementation science) focuses on the transfer and adoption of evidence-based knowledge and the subsequent behavioral change (usually at a community, organizational, or social level).
In this study, we asked how a community progressed from the awareness of the health impact of asbestos to taking action to achieve support and compensation for workers who had become ill from workplace exposures. We explored the fulcrums-of-change that helped to bridge this gap from multiple perspectives: workers, industry, community, and local politicians. We attempted to identify the pivotal facilitators and barriers that the community encountered. We also explored whether this awareness about asbestos has continued or transferred to other chemical industry-related hazards in the workplaces and the community.
The City of Sarnia was chosen for this study. It is a small (population 72,000), relatively isolated, racially homogeneous city in Ontario, Canada, that is dominated by the petrochemical industry. It is located where Lake Huron flows into the St Clair River at the Canada–United States border, directly across from Port Huron, MI. It is a predominantly white community (where people speak either English or French as their first language). 10 In 2011, only 3.6% of its population identified themselves as a visible minority 11 as compared to 25.9% of Ontarians in general. 12 The city is bordered by the Aamjiwnaang First Nations Reserve to the south. 13
The city hosts nearly 40% of Canada’s chemical industry with sixty-two industrial facilities along its border region. 14 These refinery and chemical plants are found in a 25 km radius of the city in what is known as Chemical Valley. At its peak in the 1970s, Sarnia had the highest standard of living in the country, with a per capita disposable income 35% greater than the national average. 15 For several years, an iconic image of the city’s petrochemical industry graced the back of the Canadian ten-dollar bill.
Sarnia has high rates of particulate air pollution and higher rates of cancers when compared to other cities. 16 For example, a report using 2005 data, noted that 5.7 million kg 16 of air pollutants were emitted from the region resulting in several Ministry of Environment Orders. 17 Using 2011 data, the community ranked first, fourth, and eighth in emissions of tetrachloroethylene, chloroform, and nickel, respectively, of 159 Canadian cities.13,14,15 According to a 2011 report by the World Health Organization, Sarnia was rated as having the worst air quality in Canada.14,18 Recently supplied 2008–2010 data from Cancer Care Ontario says cancer in Sarnia-Lambton (a merged municipality) is more prevalent than elsewhere in the province, with a local cancer rate of about 433 cases per 100,000 people. This being noted, recent regional advances in air quality have been observed.19,20 Over the last ten years, nitrogen dioxide and sulfur dioxide emissions have dropped 50% largely due to community concerns and efforts in conjunction with local industry. 19
A timeline of community awareness and action: the history of Sarnia’s demand for recognition of the impact on workers’ health from exposure to asbestos.

Note. OHCOW = Occupational Health Clinic for Ontario Workers; WSIB = Workers’ Compensation Board; CEP = Communications, Energy and Paperworkers Union of Canada; CAW = Canadian Auto Workers; OFL = The Ontario Federation of Labour; VOVC = victims organization; MOL = Ministry of Labour.
Conceptual Framework
This case study is a historical account, as remembered by key informants, of how the increasing community and worker awareness of the health effects of occupational exposures, especially the growing knowledge of how asbestos caused mesothelioma and lung cancer, led to community and union action. It examined the roles and interactions of the different players in these efforts to prevent this hazardous exposure and the actions that led to support for sick workers and their families and explored whether and how companies changed their processes to reduce workers’ exposure to asbestos.
The study was informed by an adapted version (with permission from Minkler et al.) of a conceptual model that comes from the field of community development24–26 and the “Dynamic Model of the Dimensions of Community/Partnership Capacity, their Contextual Factors, and Potential Outcomes (See Figure 1).”
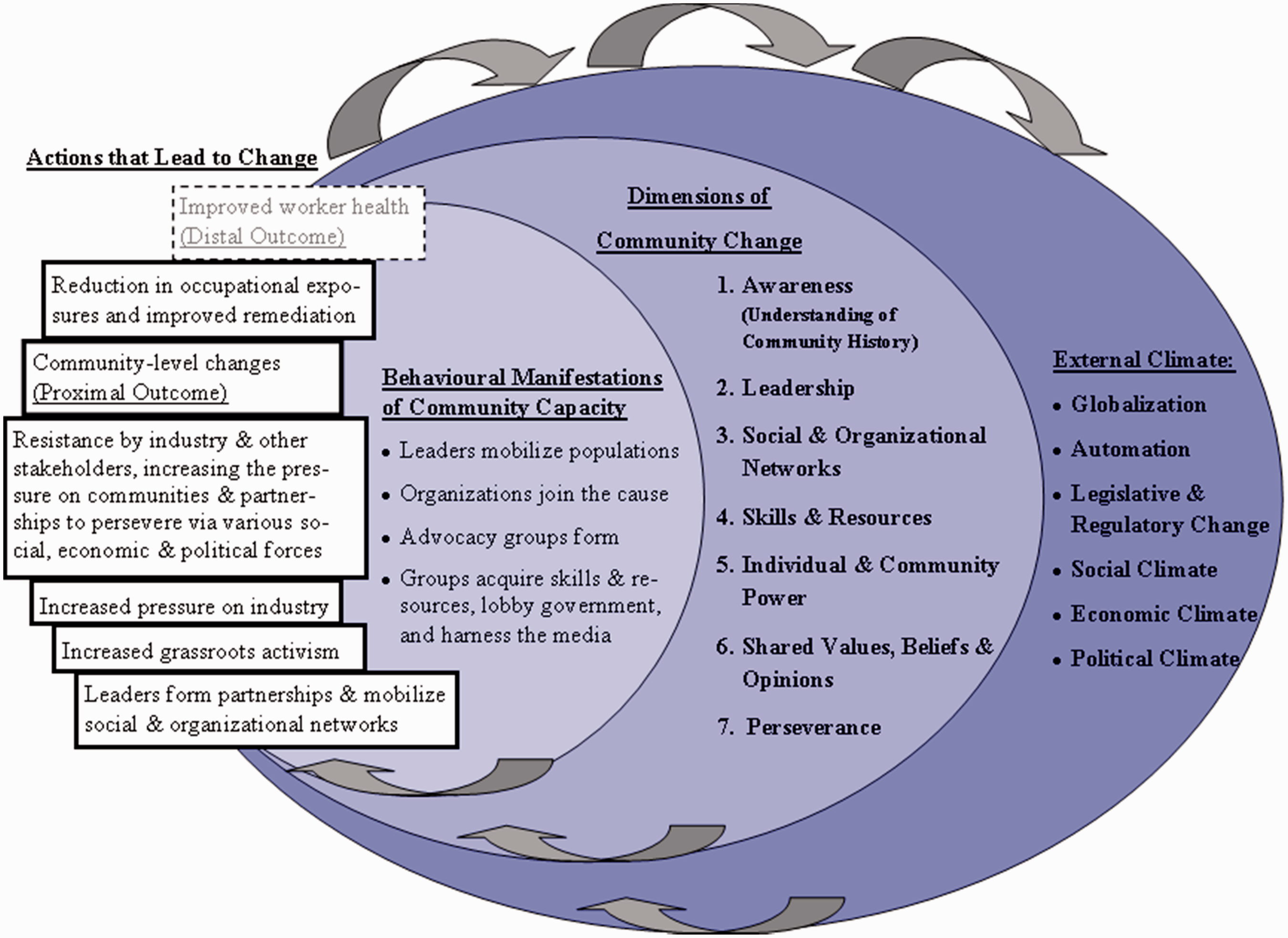
The conceptual model was selected for this study because it includes a number of dimensions of community change and also takes into account the external climate. 24 It has been used to identify the pivotal variables for racial and ethnic communities taking on community initiatives such as reducing diesel emissions from idling buses in Harlem, stopping the use of mine tailings in construction unless contained, getting routine lead testing for at-risk children in Ottawa, and getting a moratorium on industrial hog operations in Halifax.25,27
The “Dimensions of Community Change” model helped frame the questions that the researchers asked of the thirty participants, their team discussions, and their analysis of the interviews. The model evolved as a result of emerging knowledge gained during this study. The community change level of the model originally had ten dimensions; they were condensed to seven. They were rearranged in order of importance, and some were altered to a similar, but more applicable concept. The seven are Awareness; Leadership; Social and organizational networks; Skills and resources; Individual and community power; Shared values, beliefs, and opinions; and Perseverance. Although the model includes the external climate as an essential part of the change process, so few respondents responded to questions on social, economic, political, and global pressures, that these have been excluded from the following analysis.
Research Methodology and Procedures
The study received ethical approval from the Community Research Ethics Office, based in Kitchener, Ontario. Seven site visits were made to the city over a period of two months to conduct interviews and focus groups. The research team recruited a convenience sample of participants based upon their existing network. Since many of the interventions that can reduce workers’ exposure are dependent on workplace parties, the recruitment process emphasized industry management and union representation. Interviews were conducted with labor, 7 community members, 9 local politicians, 6 and industry representatives 8 to capture various perspectives. The seven interviewees in the labor category included mostly people who had been at the time of interest (early 1990s) union representatives or were members of organizations sponsored by the unions. Half of this group had worked in the petrochemical industry, including a member of the Aamjiwnaang First Nations Reserve.
The six local politicians were local municipal representatives, leaders from the local community college, and members of the Better Business Bureau. The eight industry interviewees were members of the Sarnia-Lambton Environmental Association (SLEA). SLEA is made up of representatives from twenty of the sixty-two petrochemical companies in Chemical Valley, some of the largest in the area. The organization is nearly fifty years old, and its objective is to monitor and report industrial emissions. The members are plant managers, senior production managers, and health and safety directors. In the past, they have had a difficult relationship with the community and with the Aamjiwnaang First Nations Reserve due to the perception of underreporting.
The nine community members included a mixed group of activists who were associated with the VOCV, the Sarnia-Lambton Community Health Study, and three representatives from the First Nation community. The VOCV was one of the first initiatives of the unions and is made up primarily of widows. This group of mainly women ended up carrying the moral authority of the action, although most of the key actors were male workers, union representatives, and management. The Sarnia-Lambton Health Study was initially formed in 2008. It has representatives from municipalities, First Nations, business, labor, industry, occupational health, victims of occupational illness, and public health. It recently received a commitment from SLEA that the companies will fund 30% of an environmental health impact study (a percentage that was negotiated to ensure the impartiality of the study and its results). The remaining money to cover the cost of the study is still to be obtained.
In total, four First Nation community members were interviewed. As mentioned, one was included in the labor group since he had worked in the petrochemical industry for decades, and the other three were included within the community group to protect their anonymity. There would have been many advantages to having the voices of more members of the Aamjiwnaang First Nations Reserve represented. The research group is under discussions to make that a focus of future research noting the research protocol guidelines as outlined by Canada’s Assembly of First Nations. 28
Since Sarnia is such a tight-knit community where individuals often span multiple categories, some participants spoke from multiple perspectives. The researchers emphasized to the interviewees that all data would be aggregated, and no identifying information would be used to ensure their anonymity and confidentiality and that of their companies.
Semi-focused interview schedules were created based upon the conceptual framework. Four slightly different schedules were created depending upon which group the interviewee fit. They were modified during the study reflecting evolving knowledge. With the exception of two people (one industry and one politician), all requests for interviews were accepted. Four of the participants were interviewed more than once. Each semi-structured interview lasted about an hour; to achieve consistency, all the interviews were conducted by the lead researcher.
Special attention was paid to the person’s awareness of occupational exposures and whether that individual thought such exposures were an issue in the community; what changes the interviewee had seen over the last ten to fifteen years, and what role he or she had played in that change; what actions they thought the community or unions had taken to support the reduction in occupational exposures; what changes the companies had made; whether industry management treated critical safety issues differently from workplace exposures with long latencies; what resources were needed to make change at the community level (leadership, skills, expertise, time, perseverance); and what, if any, external environmental factors impacted their stories.
Two focus groups were also facilitated. One with community activists and another with a group made up of management representatives from different petrochemical companies. Other supportive data were collected such as information on websites, annual reports, emission reports, and historical reviews that were available at the time. The data helped inform or contextualize the findings. The researchers also asked the companies for access to any exposure data they were comfortable sharing that demonstrated improvement over time. Although one data set was offered, permission to use it in the study was not granted for reasons of company confidentiality. Newspaper headlines about important historical events in the city were turned into posters and used in the focus groups to encourage memory and reduce recall bias.
The interviews and focus groups were digitally recorded and transcribed by a research-team member. The team met often to discuss the findings relative to the conceptual framework. Discussions focused on where the findings converged and diverged from the framework and on emerging themes.
Data Analysis
Interviews were conducted until saturation of themes was reached, and the research team achieved an in-depth knowledge of the community and multiple perceptions on what influenced the awareness-to-action process. The qualitative analysis was guided by the conceptual framework. However, as mentioned, the interviews only had rich data on the inner circle of the framework, the Dimensions of Community Change, and hence this is where the analysis has focused.
Matrices were developed; one axis had the seven key components of community change and the other axis divided the interview data into the four informant groups. The matrices helped to organize, summarize, and code the text in a continuous iterative process, which facilitated a comparison between the four groups, allowed for dominant themes to emerge, and helped the research team draw conclusions from the data.
Coding for the interviews was done by one member of the research team and then discussed with two other members to ensure agreement on categories and themes. All data were aggregated and anonymized to protect the privacy of individuals and companies.
This study reports on its results in two ways in order to gain as much understanding as possible of the research question: How did this community go from awareness to taking action on occupational exposures?
Matrix of illustrative quotes from the four community groups.

The second part of the analysis focuses on the four groups—industry, workers, community, and local politicians—and their perspectives on whether awareness had been necessary to reduce workers’ exposures to hazards in the workplace, what changes had taken place to reduce these exposures, whether the workplace was a better place now in comparison to the past, and if there was an improvement, what did the interviewees see as the fulcrums of change that had achieved this change. This section has been called the Fulcrums of Change.
Dimensions of Community Change
Awareness
This study was predicated on the assumption that there has existed a high level of awareness of the negative health effects of occupational exposures in Sarnia since the late 1990s. Even before there was public awareness, workers said that they were always aware they were working in an environment that could damage their health.
In the late 1990s, the media, including the Globe and Mail, Canada’s national newspaper, began reporting on the illnesses and tragic deaths of workers, and public awareness of occupational exposures came into focus. The media coverage was facilitated by the analysis of the problem by an academic occupational health leader. A number of respondents noted that he reviewed Sarnia’s elevated levels of mesothelioma, and by virtue of his research, his personality, and the support he had from the unions and community activists, he raised the city’s awareness to the dangers. The concept of the “credibility of the messenger” is a very important one in the field of KT. 29
As other union and community advocates joined the effort, the unions (the Communications, Energy and Paperworkers Union of Canada, the Ontario Federation of Labour, and the Canadian Autoworkers) held multiple intake clinics for exposed workers at two plants: the Holmes Foundry and Fiberglas Canada (and later, others). These clinics helped workers organize the necessary paperwork to submit compensation claims. At this point, public awareness increased through discussions and shared stories. One worker who became a union representative noted this incremental growth in awareness: As the years went by, and you start to see people getting ill, then of course the awareness of the hazards became embedded pretty solidly in people who work in the industry. When you start to see people who you were on the same shift with, developing disease, exposure-related disease, then yeah. Then you get it.
Other ways that people became aware included the sickness or death of a loved one, involvement with unions, legislation, labeling on hazardous materials, learning from family members in industry, exposure to the health care sector, and industry outreach.
However, the level of awareness and hence potential demand for improvements in the work environment was also suppressed due to the inherent conflict between the benefit of having a well-paying job and the risk of becoming ill after a long latency period. A dirty and dangerous environment was considered inherent by many workers to their work, and there has always been a culture of gratitude toward the companies that have provided well-paying jobs and an acceptance that risk to one’s health is part of the job. Advocates recalled how difficult it was to raise awareness because criticizing the companies was not acceptable: “This was never discussed. It was not public knowledge”, said one worker. This emerged as a dominant theme.
Another identified issue, which was validated by almost every respondent, was that the publicity focused in on the health impact of only asbestos, and not necessarily on occupational carcinogens in general.
A unionist said: Asbestos is bad for you, we know that. People in this community, most of us, we know that. Whether you’re a white collar worker or a blue collar worker, a member of a family of somebody who works in the trades or in the Chemical Valley, you know that asbestos is bad for you
The level of awareness and activism has declined since the 1990s, and the reason given is that the environment and workplaces in Sarnia have improved significantly in the last couple of decades. Many of the interviewees from each of the groups stated that occupational exposures (mostly referring to asbestos) were no longer an issue today. They considered such exposures to be a “legacy issue” and not a current problem. They talked with emphasis about how things have improved since “the bad old days.” This view was not universal. An opposing voice came from the widows of the VOCV who continue to try to maintain the community’s awareness of the health impacts of asbestos and to advocate for a ban on asbestos, and some industry workers who acknowledged that although there have been substantial improvements, they are aware of carcinogens and potential exposures that still exist in the plants.
Despite occupational exposures losing their spotlight, there is currently much public interest in an emerging community health study. It is predicted that the study will take three to four years and cost $4.8 million, and it will attempt to assess the community’s health in response to concerns regarding environmental emissions. The study is receiving a third of its funding from the SLEA, 30 contingent upon the study also receiving government financial support.
Leadership
Depending on their perspective, all four groups considered the role of leadership as essential, although they identified leadership differently. Advocacy efforts were multipronged and required different people with different expertise, skills, and networks. Labor and community members spoke about the importance of leadership as a resource when trying to raise awareness about occupational exposures. They identified union activists as leaders who organized the intake clinics, supported the occupational clinic, formed the victims’ advocacy group—the VOCV, took the widows to Toronto to lobby the provincial government, and helped sick workers and widows file for compensation.
The community said their leadership came from a diverse group of individuals, which included the occupational health clinic leader, union leaders, the VOCV, health-care workers, and certain senior local politicians. Many identified the occupational health clinic leader as “the key glue, the key player” in their attempt to raise awareness of occupational exposures.
As mentioned, the industry members were mostly plant managers and senior production engineers who spoke from the perspective of their companies. They spoke about the improvements they had made since the 1990s. They focused on the ways in which their companies were leaders compared to other chemical companies. They were proud of their low injury rates, their improving connections with the neighboring Aamjiwnaang First Nations Reserve and the Sarnia community, and their environmental performance. They noted that recent changes were a significant improvement from what had existed previously, and that these workplace and community initiatives were important to them. Their activities were supported by their head offices, but they took personal credit for the changes since they had led the initiatives. (It is worth noting that it was not possible to validate the stated positive relationship between industry and the local First Nations since the number of First Nation interviews was too small.)
A number of the chemical companies have taken leadership as a group by forming the Sarnia Lambton Environmental Association (as mentioned, SLEA mostly monitors and reports on ambient air quality), the Industrial Education Cooperative (which works with the construction companies and unions to standardize occupational health and safety training for construction workers in the Chemical Valley), the Community Awareness and Emergency Response Board (which notifies the community, including the Aamjiwnaang First Nations Reserve, about emergency spills or emissions), and the Chamber of Commerce (which represents about one-third of the businesses in Sarnia).
The politicians take a leadership role in many causes that affect their communities including protesting against land being set aside for windmills, advocating for developmentally delayed and disabled persons, lobbying for rail transportation at the federal level, ensuring high standards for landfill sites, raising money for the local college’s expansion and renovation, and passing smoking by-laws. But in this context, the major leadership role of the politicians was to act as the broker between the needs of the community and industry, and the community felt that few of the politicians took on this difficult role. It has been seen as politically dangerous to stand up to the petrochemical companies who are so important to the community, although none of the interviewees expanded upon what consequences they might face if they did take on an advocacy role.
Social and Organizational Networks
Social and organizational networks are regarded as essential for community change. They act as resources, spread awareness, create a critical mass of protest, and demonstrate power. When networks are active, they improve literacy in dealings with industry, government, and occupational and environmental exposure science; provide social support and increase members’ sense of power (self-efficacy); 31 provide financial support; increase access to peripheral networks; and share technology, training materials, and professional expertise. They are also essential when it comes to effective advocacy for occupational health and safety.
Most participants, when speaking of the past, remembered becoming aware of occupational exposures as a result of interpersonal interactions across groups. The “social construction of knowledge” is a key concept in KT. The participants spoke about the exchange of knowledge that occurred between groups, and strong bonds that were created between the union activists and the community, which led to the creation of the VOCV and in turn led to the media becoming aware, the industry getting involved, and hence even further heightened community awareness.
However, when participants spoke about connections in the present, they said that the link between the unions, the VOCV, and the occupational health clinic is no longer strong. The unions created the VOCV, but community knowledge of that seems to have been lost over time. The annual walk for victims, organized by the VOCV is no longer well attended by union representatives or local politicians. The occupational health clinic is no longer a hub of community activity.
Skills and Resources
Having access to skills and financial resources are related needs for communities attempting to engender change. Respondents said that money was necessary to fund advocacy efforts; for example, money was needed for the occupational health clinics, union activities, access to the legal system, and to conduct independent environmental monitoring. A community activist credits her daughter’s skills with computers as being essential in getting out the message to other community members.
Worker advocates also cited skills as necessary tools for change. Training and literacy in dealings with government and industry and knowledge of occupational and environmental exposure science were important. Some advocates felt ill-equipped to navigate these systems and wished that the public school system had “taught this stuff.” One labor representative mentioned that the courses he had taken through the Workers’ Health and Safety Centre (a Ministry of Labour-funded, but union-run, teaching center for unionized and non-unionized workers) were important because the information gave him a knowledge base to inform his advocacy efforts. Industry members cited their occupational health and safety programs, policies and procedures, and metrics and personnel as vital for ongoing delivery, monitoring, and improvement.
Scientific information was an important resource. The availability of data on mesothelioma rates, lung cancer rates, and mortality in Sarnia were cited as essential in leveraging the unions and the community to advocate for protection in the workplace. These data were used at the government level to initiate environmental regulations such as lowering occupational exposure limits (OELs). Industry used government guidelines along with internal data to ensure they were compliant. Advocates and union representatives acknowledged that regulations and legislation are important, but said that enforcement is usually lacking. The politicians were the most supportive of legislation as a resource, since it “gives advocacy efforts teeth”.
Interestingly, in this context, the large room at the occupational clinic was considered a valuable resource for the different community groups to meet, network, and strategize. The large room with big windows that could comfortably seat about hundred people eventually was removed. Its loss was a very tangible indication that the advocacy role of the occupational clinic had been discontinued.
Individual and Community Power
The representatives of the different groups had different perceptions of their individual sense of efficacy, their group’s power, and the power of other groups. Not surprisingly, the dominant theme that emerged was the perception that industry is the dominant power in the community. Support for this idea came from industry’s role as the source of high-paying jobs, having many resources at its disposal including money, professional networks, legal resources, public relations departments, and so forth. In turn, the representatives from industry stated that they have attempted to balance this perception by engaging in multiple activities to improve their reputation in the community. The industry representatives said that they would like to be perceived as good corporate citizens and are also motivated by personal moral reasons. In recent years, they have demonstrated transparency by publishing ambient air quality data in newsletters, investing in emergency response systems, sponsoring community events, opening their doors during “Family Days,” and creating community advisory panels. Their agents spoke about the respect they showed to the neighboring First Nation community, such as moving noisy activities away from the cemetery, keeping the community informed about leaks and explosions, and having regular communication. They acknowledge that more communication is always needed.
However, many labor respondents talked about job insecurity. Workers and retirees expressed concern that if they demanded improved health and safety, there would be retribution, such as getting fired, losing contracts, losing pensions, or even plant closures. Of note, trade workers felt particularly vulnerable to these power structures since they were not unionized, and a number said that if they advocated for improved working conditions, their contract renewal would be threatened. Finally, a few community activists stated their concern about speaking out against the companies due to a potential backlash on their personal or professional lives.
Interestingly, although politicians are expected to have power, and although Sarnia’s local politicians were involved in multiple matters that affected their community, most did not feel they had the power to affect change on a provincial or national scale. They felt “disconnected from Queen’s Park” (the site of Ontario’s provincial legislative building) and felt that their community’s advocacy and initiatives were irrelevant to higher levels of government.
Shared Values, Beliefs, and Opinions
Sharing values, beliefs, and opinions is considered essential if different groups are coming together to advocate for change. There needs to be a fundamental agreement on what change is necessary, and why. The overarching values expressed by participants were split between social justice and business values; occupational and environmental justice was included in social justice. While some groups identified predominantly with one value-set, many spanned both. The clearest and most commonly expressed value of worker’s rights came from labor activists or from community members who had a family member afflicted with an occupational disease. They felt that industry had an obligation to ensure a safe and healthy working environment: “There’s something wrong when a person commits their life to an employer and their reward for it is to lose the last part of their life,” said a unionist. While all industry members acknowledged this responsibility, some argued that it was a two-way street; workers should also take responsibility to protect themselves by using supplied personal protective equipment and following the occupational health and safety (OHS) regulations set out by their workplaces.
An idea, mostly mentioned by the labor group, was the concern that the values that are foundational to OHS and the need to be profitable are often in opposition, and that the companies were resistant to investing in OHS, as it would have a negative effect on profitability. Although more commonly expressed by labor and community representatives, some industry representatives also mentioned that industry cared only about “the bottom line” or profits to the exclusion of consideration for OHS.
A different perspective on values was expressed by industry members who commonly talked about business ethics, accountability, transparency, and responsibility in relation to OHS and the environment. They understood that protecting workers and the environment was a necessary part of running an ethical business, and examples of these values were given by all industry members. The other three groups echoed these values when they supported worker and environmental justice, objective monitoring of industry to ensure accountability, increasing transparency on the inner workings of industry, earlier and more transparent notification of spills and emissions, and taking responsibility for past actions that have led to poor health and negative environmental outcomes.
Perseverance
Individuals spoke about their personal and group perseverance in terms of grassroots advocacy efforts and the need to continue to protect workers’ health and safety. Community members and the workers spoke about their ongoing struggle to increase awareness and change community norms around occupational illness. “I think you need to constantly be bringing it up to the public and having a lot of public input and just keeping it out there because I think people get complacent,” said a community member. Although the ability to persevere in any change initiative over many years and against multiple obstacles was cited as an important tool for change, many advocates admitted that it has been tough to maintain. A worker advocate who was very active in the early 2000s has slowed down and reluctantly admitted that, “to re-engage, to truly re-engage … is a big effort.” In contrast, advocates and industry members alike expressed that a big event such as a death, tragedy, or industry spill can renew one’s vigilance. Some of the community members said that the companies expected (and depended upon) community advocacy efforts “petering out” over time due to emotional burn-out, career responsibilities, personal health problems, family demands, and leisure activities. Despite how difficult it was for advocates to persevere, things like social support and professional leadership were cited as resources that made it easier to continue.
Others who are still working in or tied to industry spoke about the need to keep focusing on this issue. “Sometimes complacency sets in after long periods of time when nothing’s happened,” said an industry member. When industry representatives spoke about the need to maintain vigilance in OHS, they included the need for continuous improvement and monitoring of workers using their personal protective equipment. The reasons for this approach included protecting workers, improving their reputation in the community, disseminating safety culture, and avoiding the horror of relaying the news of a husband or father’s death to the family.
Fulcrums of Change
This study inquired how a community progressed from the awareness of the health impact of asbestos to taking action to achieve support and compensation for workers who had become ill from workplace exposures. We attempted to identify the pivotal facilitators and barriers that the community encountered. We also explored whether this awareness about asbestos continued or transferred to other chemical industry-related hazards in the workplaces and the community. Unfortunately, the answers did not emerge with clarity. Alternatively, a case study emerged about how a community, at a certain point in time, with the help of the unions, attempted to raise the awareness of occupational exposures (asbestos in particular) and achieve community-level action. The four groups—labor, community, local politicians, and industry—had different perspectives on whether change was needed, and if so, what change, and what they saw as the essential tools, or necessary resources to help achieve change, or as we have called them, the “fulcrums” of change.
Labor
In the labor group, there was a strong division between those who were grateful to the companies and others who resented having been exposed to life-threatening occupational hazards. Most interviewees were happy with their good jobs, wages, and work environment. For the most part, they have enjoyed their work and have had successful and fulfilling careers, and hence they have an overall satisfaction with the status quo.
Most of the workers acknowledged that there has been a significant and notable decrease in occupational and environmental exposures over the last two decades. Many workers stated that workplaces are now much better places to work than they were in the past. However, it needs to be noted that many of the interviewees, but especially those in the labor group, indicated that they believe that profits and productivity fuel the decision-making in industry, and that any improvements that have been made to reduce occupational and environmental exposures, and hence occupational illness, have often been unintentional (although advantageous) outcomes of the profit motive. As one worker said, Industry’s going to make more product, so they’re going to upgrade their plants because they can sell more. Oh, while they’re doing the upgrades they’re going to buy new seals and new pumps and they’re all state-of-the-art and they don’t leak like they used to, etc. So those health risk changes come about incidentally.
The labor interviewees also spoke about the fact that even though exposure to asbestos is no longer the huge issue that it once was, workers are still exposed to a cocktail of chemicals, including benzene, that are potentially even more toxic to their health than asbestos (although the latency period between exposure and developing cancer hampers scientific investigation). However, this awareness does not act as a barrier to doing work from which they get enormous satisfaction. One worker described his work with great glee: Pretty much if it’s nasty and can kill you, I’m the person who’s going to be working with it …. Every year we [deal with] more interesting chemicals. I recently did my first nitrogen transfer with hexane, two weeks ago, and that’s extreme! It’s like 10 times more flammable than gasoline. So that was a fun one!
Most thought it was reasonable that the cost of a good job for more than thirty years might be illness and death: “We live ourselves to death. I hope that’s the way I go”, as one worker said representing the views of many of his colleagues. These workers were not angry with their companies—an attitude that is consistent with decades of OHS research and activism that shows that workers accept dangerous work as just “part of the job” rather than as something that can and ought to be prevented. They also emphasized how much worse occupational exposures had been in the past, and many considered occupational hazards, and exposure in particular, as a “legacy issue” that had now been solved. “Yeah, to me it’s 100% better than it was in the ’50 s and ’60 s”, said an older worker. Interestingly, many of these workers did not acknowledge the role that the unions, or OHS activists have had in achieving these gains.
But a sense of gratitude to industry for their well-paying jobs, sometimes an expression of satisfaction at having exciting work which was often dangerous work, and focusing on the improvements that have occurred over the decades, was not expressed by all. Another voice from the workers expressed anger toward the companies and blamed them for not doing enough “when they could have and should have” prevented a human health disaster.
The activists from labor expressed pride in their achievements from the late 1990s. They gained significant media exposure on the devastating effect of asbestos on the health of the workers, they held intake clinics for workers, and through the occupational clinic, obtained compensation for more than 700 workers. Those who were involved reflected on that time with a sense of awe and wonder at what they had achieved. Notable was getting the funding to establish a permanent occupational clinic in Sarnia. “There was a resolution to have the [occupational] clinic funded fully. We were surprised when they actually did fund it fully.”
However, when these changes were taking place there was a strong and large union membership in Sarnia and the leadership of multiple unions came together to help Sarnia and its sick and dying workers. The unions were well connected to the community and shared their values. They became well informed and were resourced by their national membership. This base of power has since been eroded by the precipitous decrease in unionized membership and the threat of plant closures and layoffs. Consequently, in the decades since the unions rallied to help the community, the union leadership has been diverted to more urgent survival issues; examining exposures that might have a latency period of thirty years or more has dropped in their priorities.
Community
The participants who fell into the “community” group were the most diverse. Nevertheless, themes did emerge. The community members saw the major fulcrums of change as leadership, credible research, a sense of their own power, and the endurance and perseverance to keep focused over many years. But they did not necessarily share values, opinions, and beliefs. Those who had been directly affected, including falling ill themselves or losing a loved one, were the clearest in their ideation that the companies had failed in their responsibility to care for their workers. However, a conflicting theme that emerged even from the widows in this group was that their late husband had had a good job, had given their family a good life, and now that compensation was available, he was still looking after them.
The VOCV have made occupational illness their own personal battle and continue to be angry with the companies, with their community which they perceive as turning complacent, and the lack of leadership from the unions to help continue the crusade. As one said: “I just want it all fixed. I know that we can’t change the legacy of the past. I know that we can’t do that. But my goodness … it’s not ok anymore. I’m not disposable, you know.” The VOCV continue to lobby for awareness and action on the dangers of exposure to asbestos. Recently they changed their name to the Victims of Asbestos and Occupational Exposures, acknowledging that there are other dangerous chemicals in the petrochemical industry to which workers continue to be exposed, and potentially expanding their advocacy beyond Chemical Valley.
The other community groups have other issues on their mind (health, education, employment) and thus occupational exposure, regardless of its high profile in the city, is no longer their priority. Having workers die early has become part of the accepted background of living in the city. A member tried to explain, “This is our normal. This is what we live every day, and, oh well, some day it’s going to kill me!”
The community activists are proud of what they have achieved, but the change process has been long, and many of the community members are now tired and discouraged and weighed down with other responsibilities. As another stated in despair, “You know, by the time all of [the political lobbying] unfolded, I was ill. Like really sick. To the point that for weeks and months I could hardly stand. I stopped my [advocacy] work.”
Local Politicians
The politicians who contributed to the study were representatives at the city level. In regard to “the asbestos problem,” the Mayor of Sarnia, Mike Bradley, took the lead within this group in raising awareness and supporting the victims. As early as 2001, he led an initiative for Sarnia City Council to endorse a resolution requesting the Federal and Quebec Governments to ban the exports of asbestos outside of Canada. Sarnia was the first city to officially make this plea to the Canadian federal government. In 2008, the Council reaffirming their position to once again call upon the Federal Government and the Government of Quebec to stop the export of asbestos out of Canada. In September 2011, on the tenth anniversary of the first resolution, the Mayor again led the Members of Council to reaffirm their resolution and support a Candlelight Vigil and a Walk “to bring the community together to demand the Federal and Quebec Governments stop the export of asbestos”. 32 By 2013, Canada had stopped exporting asbestos.
The local politicians were very self-conscious of the limitations of their power to make major change at the municipal level since decisions about occupational or environmental legislation, transportation, or location of major industries are made at the provincial level. A representative quote was: “As far as taking a leadership role and going out and beating a drum and trying to make something specific happen, only in my own municipality for my own people is the limit of what I do.”
The local politicians said that they were obliged to consider the multiple voices in their city. There were many other issues that took priority over occupational exposures and illnesses, such as the need to get the college funded; the need for a railway link between Sarnia and London; the need to reopen the jail; the need for a top quality hazard landfill site.
There were mixed results depending upon whether the community was talking about the local politicians, or whether the politicians were reporting on their own actions. Key activities in support of awareness of the occupational and environmental impact of industrial emissions included: participating in the annual community Walk to Remember Victims of Asbestos, and supporting the pending Community Health Study to examine the impact of environmental emissions. The Council has recently supported the remediation of a park that is heavily laced with asbestos, lead, carcinogenic hydrocarbons, and metals; the remediation plan and execution has been done with relative speed because of the high awareness that the community has of asbestos. However, even these issues are not supported by all councillors. One of them admitted in amazement that he had heard this comment from a peer in regard to the park: “Just take the fences down and let people take their chances.”
What is considered most important by most of the local politicians is a thriving petrochemical industry. Industry supports the city in tangible ways by offering employment but also by contributing to the college, the hospital, and ceremonies to celebrate the city’s 100th birthday. The reputation of the city is also important. The politicians are working on rebranding the community so that it is no longer synonymous with “Chemical Valley.” They are considering ways to diversify the economy including attracting the alternative energy sector, expanding applied health-care training in the local college by extending nursing training to four years, and attracting a retirement population. They are upset that the media will not report on the “good news” stories of how the community has improved. To bring occupational exposure back onto the radar for this group, the community would have to yet again build this issue as a major focus. It would have to be a bottom-up movement.
Industry
The industry representatives all mentioned that acute injuries were a strong priority for them, and they have policies, procedures, and programs in place to prevent these. However, they all commented that initiating policies, procedures, and practices to reduce occupational exposures (which are from chronic exposure) is not equally straightforward. Decisions on occupational exposures need to compete with multiple competing priorities: Immediate safety issues take priority over long-term exposures; research evidence on the health effects of chemicals and processes can be confusing; risks versus hazards need to be balanced; how to best handle existing asbestos remains an unresolved issue; the substitution of chemicals and processes can be very expensive and not necessarily less toxic to workers; keeping up with the regulatory environment in Canada, which is more stringent than that of other countries is already a competitive issue; the shareholders need to be pleased, and hence, the highest priority remains productivity. As one of the managers said: At the end of the day, you’re faced with a whole myriad of pressures and things to consider before making a decision. And it’s difficult …. Small stuff we can do, and we continue to do. And even some of the big stuff we do, which is part of [our company’s] commitment. But it comes down to [making decisions based on a] matrix of frequency and severity.
Since many of the companies in Sarnia are branch-plants of multinationals, the companies’ safety standards are usually set by head offices that are not in Canada. Health and safety programs are evaluated by metrics such as lost-time injuries. However, that does not preclude the role and the power of the individuals themselves and the actions they take to make change at the local level. As mentioned, as a group, the eight industry participants who are plant managers, engineers, production managers, and health and safety specialists, see themselves as leaders in the community in monitoring and reducing short- and long-term occupational exposures and environmental emissions and are making some significant changes to improve their standing in the community and on safety in their plants.
Some mentioned how a critical incident in their past had led them to focus on safety, I’ve been involved with fatalities and having to go and talk to families. The most recent one was after a mother was killed at work. Not her fault, but an accident at work. Talking to [children] about their mother passing away, and speaking at her funeral was tough. Don’t want to ever do that again.
Others mentioned their love for their work. I like to make plants run really well from all aspects: safety, environmental performance, reliability, profitability. I like being part of keeping manufacturing alive in Ontario and keeping valuable jobs in Ontario and value added, like the contribution we make to the economy.
Summary
The “story of Sarnia” which emerged from the interviews and focus groups is that, beginning in 1996, there was community- and union-led organization to recognize the health effects of exposure to asbestos in the workplace. Emerging from this concerted effort were a number of benchmark changes that have made a significant improvement in the lives of the sick workers, the widows, the surviving children, and the community in general. Compensation is now awarded relatively easily to workers from Sarnia with cancer or their survivors. A hospice was built for sick and dying workers. An occupational clinic achieved permanent status in the community. Environmental monitoring is now conducted regularly. There is a more collaborative relationship between industry and the neighboring First Nations community. The economy is beginning to diversify. At a smaller level, local funding has been secured for the Centennial Park remediation, and a third of the needed funding has been secured from the petrochemical companies for the Community Health Study. According to the conceptual framework (See Figure 1), these changes will hopefully lead to an overall reduction in occupational exposures, improved remediation, and ultimately, improved worker health.
To achieve these community-level changes, union and community leaders formed partnerships and mobilized their social and organizational networks. Then, grassroots activism emerged that engaged the media which increased the pressure on industry. Finally, the resolution to fund and make permanent the occupational clinic sparked the beginning of the community-level changes.
The successful campaign to raise awareness about the carcinogenicity of asbestos was dependent upon a number of factors. First was the clear, concrete definition of the issue and its easy communication throughout the community. Irrefutable evidence shows that asbestos causes asbestosis, mesothelioma, and lung cancer. Asbestos was widely used throughout the sector, with workers at the Holmes Foundry and Fiberglas Canada being particularly vulnerable.
Second, a confluence of events helped raise awareness of this problem and supported the action. The city had credible leadership, an educated workforce, social and organizational networks, skills and resources, individual and community power, shared values, beliefs and opinions, and perseverance. At the time, there was a large population of unionized workers. This circumstance gave the Communications, Energy and Paperworkers Union of Canada (CEP), and the Canadian Auto Workers (CAW) (who have now merged into a new union called Unifor) the power to initiate change. A union representative, with the support of the CEP leadership and the larger provincial labor federation (the Ontario Federation of Labour), took on the project of supporting sick workers and bringing them together to map their exposures. A leader with knowledge of the health effects of asbestos and external credibility was introduced into the community and took over management of the occupational clinic. A union leader helped create a widows’ support group, the VOCV, which had the moral and emotional authority to challenge the status quo and could enroll the local media. The unions and the Clinic helped hundreds of workers and widows file for compensation.
Sarnia is a small, relatively isolated, homogeneous city heavily dominated by the petrochemical industry. It was small enough to be well-connected, and it was rare for someone not to know of or be directly affected by the illness of a worker, and hence it was feasible for the whole community to feel involved in the issue. The community- and union-supported occupational clinic became a hub for community meetings and action. There was political support especially from local senior politicians, and this helped increase media awareness. When the campaigning started, the companies were operating in a successful economic climate and hence possibly were more able to change practices and processes. Not mentioned by any of the interviewees, but relevant nonetheless, is the number of environmental regulations that were introduced at this time.
However, the concerted community and union effort to reduce workers’ exposure to hazardous chemicals is now all but over. Although asbestos remains on the radar in the community and continues to be influential, as demonstrated by the speed with which the remediation of Centennial Park has been undertaken, the advocacy effort and the strong collaboration on the issue of occupational health and safety between the unions and the community has all but ceased. Asbestos has now been relegated to be a legacy issue. This may be a reasonable conclusion as demonstrated recently when this group of researchers engaged eight union locals in Sarnia to “find” sick and ill workers over a three-month period, who thought they may have been exposed to asbestos but had not yet filed for compensation, and none were identified (publication in process).
What is less clear is why the awareness of the carcinogenicity of asbestos has not generalized to other occupational health and safety issues. Workers in the petrochemical sector are still exposed to a variety of dangerous chemicals that are potentially carcinogenic. However, the research to determine the causal link between those exposures, and cancer is at present not as strong as the body of research on asbestos and cancer. The causal link between these other exposures and cancer is probably more nuanced and potentially multifactoral and hence the awareness of potential harm is not as high, as it was of asbestos.
Another reason why the action on asbestos has not generalized to other workplace exposures could be because of wider external climate factors that were not mentioned by the interviewees. Globalization, automation, and even free trade have led to companies closing down in Sarnia and a severe reduction in the unionized work force. There has been a concurrent erosion of union power. Unemployment and job and food insecurity has also become an issue in this previously wealthy city. The social, political, and economic climate in Sarnia is no longer as supportive of worker rights as it was fifteen years ago, nor is there the same level of community support. The leadership that was active then has been diminished; there is only so much perseverance an individual can maintain, and interviewees told us that a younger generation of leaders has not yet emerged.
Lessons Learned
This exploratory study has limitations. It is a unique case study of a small city with one major industry which was afflicted with an intense exposure to one lethal occupational carcinogen, asbestos. Since many of the interventions that can reduce workers’ exposure are dependent on workplace parties, the recruitment process emphasized industry management, and union representation. The thirty interviewees and participants in the focus groups were a convenience sample recruited with the help of the research team’s existing network. The Aamjiwnaang First Nations Reserve who live within the boundaries of the city and have been very affected by the industrial environmental emissions were under-represented in this study. Only four First Nations were interviewed. Future research may potentially remediate this lack.
Despite its limitations and its potential lack of transferability, this study may offer advocates of change and the field of KT some useful ideas. The study points to the importance of empowering people or the community, the role of strong stakeholders, and the use of clear and strong messages, backed by credible research, directed to the outcomes/impacts on workers’ health, in order to be successful in advancing social justice.
Another is that it is important to have champions and leaders who have supportive organizations or unions. They will provide the power and perseverance needed, even if the demand for change takes years and individuals falter. The other relevant points are linked: ensure that the person/workplace/community has the skills and resources to advocate for and make the change; ensure that all the relevant stakeholders are networked, linked, and engaged; and build a body of shared values, beliefs, and opinions and a sense of community by building alliances and working in solidarity on a focused mission. This will, in turn, create the groundswell of support and the critical mass for change that is needed to bridge the gap between awareness and action.
The third lesson of this study is that the timing is everything. Good advocates know that they must be ready to identify a rising trend and be ready to catch the wave of change. It is not all about the strength, power, or leadership skills; sometimes the times are not right. Even the most charismatic leaders will not be able to make change if they are not supported by a strong organization, whether community, union, political body, or company. The late 1990s were a good time for occupational health and safety in Ontario, with improvements occurring at multiple levels including new legislation. This provided a good backdrop for the activism in Sarnia. The remaining activists in Sarnia are hoping that equally auspicious times will return.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for the study was received from the Community Research Ethics Office in Waterloo, Ontario.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project received funding from the Canadian Cancer Society Research Institute (CCSRI) through its Innovative Grant competition (awarded March 2014).
Acknowledgments
Sincere thanks are extended to the thirty participants from industry, the unions, the community, and local politics, who volunteered their time and knowledge to this study.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.