
Abstract
Background. In early 2020, the novel
Innovation. We developed a two-part hybrid
Conclusion. We believe that the combination of a video tutorial followed by an interactive
Keywords
Background
In early 2020, the novel coronavirus pandemic forced communities around the globe to shut down and isolate (Khanna et al., 2020; Nicola et al., 2020; Park, 2020). In the medical education community, social distancing has transformed classroom and laboratory education into online remote learning while also restricting medical students from participating in direct patient contact activities (Association of American Medical Colleges, 2020; Rose, 2020). Routine graduate medical education activities have also been suspended as resident and fellow physicians-in-training have been re-deployed to support critical patient care services (Accreditation Council for Graduate Medical Education, 2020). Educators have turned to distance education, including asynchronous self-directed learning and online video conferencing technologies to continue meeting the educational needs of learners (Chipps et al., 2012; Haile-Mariam, Koffenberger, Connell, & Widamayer, 2005; Masic, 2008). This is more difficult when it comes to simulation-based educational activities that require group interactions, and thus have largely been cancelled because of social distancing restrictions.
Telesimulation leverages video conferencing technologies to augment remote learning experiences. As defined by McCoy et al. (2017), telesimulation is a “process by which telecommunication and simulation resources are utilized to provide education, training, and/or assessment to learners at an off-site location.” (p 133). These encounters often involve a group of learners, an instructor, and simulation resources situated in different locations linked together by video conferencing technology. When the learners are physically engaged in the same location as the simulation resources, a remote instructor may observe the simulation and provide debriefing expertise from a separate location (Hayden et al., 2018). An alternate configuration of telesimulation reverses this paradigm. Resource-limited learners can participate together in a remote simulation conducted by an instructor via video conferencing technologies at a distant site. In this model, a simulation center leverages its resources and expertise to provide distance education for remote learners who are often gathered in a classroom setting (McCoy et al., 2019; Okrainec et al., 2010). Neither of these methodologies, however, successfully distances all parties involved according to social distancing guidelines during the coronavirus pandemic.
We developed a two-part hybrid model of telesimulation to teach COVID-19 ventilator management strategies while physically separating a group of learners and an instructor from one another. Learners consisted of non-ICU health care providers from multiple specialties with limited experience in ventilator management who were being redeployed to manage ICU level COVID-19 infected patients.
Methods
Our innovative education design was developed by simulation educators in the Departments of Emergency Medicine, Medicine, and Pediatrics at Weill Cornell Medical College/NewYork Presbyterian Hospital, and followed best practices in instructional design (Clapper, 2014) separated into two parts. As shown in Figure 1, all learners were required to view a high-yield, 30-minute video tutorial designed to review the fundamentals of ventilator management in COVID-19 patients with acute respiratory failure. Learners then registered to participate in a five-participant post-tutorial remote telesimulation. This allowed participants to practice, process, and apply (Clapper, 2014) what they learned from the video.
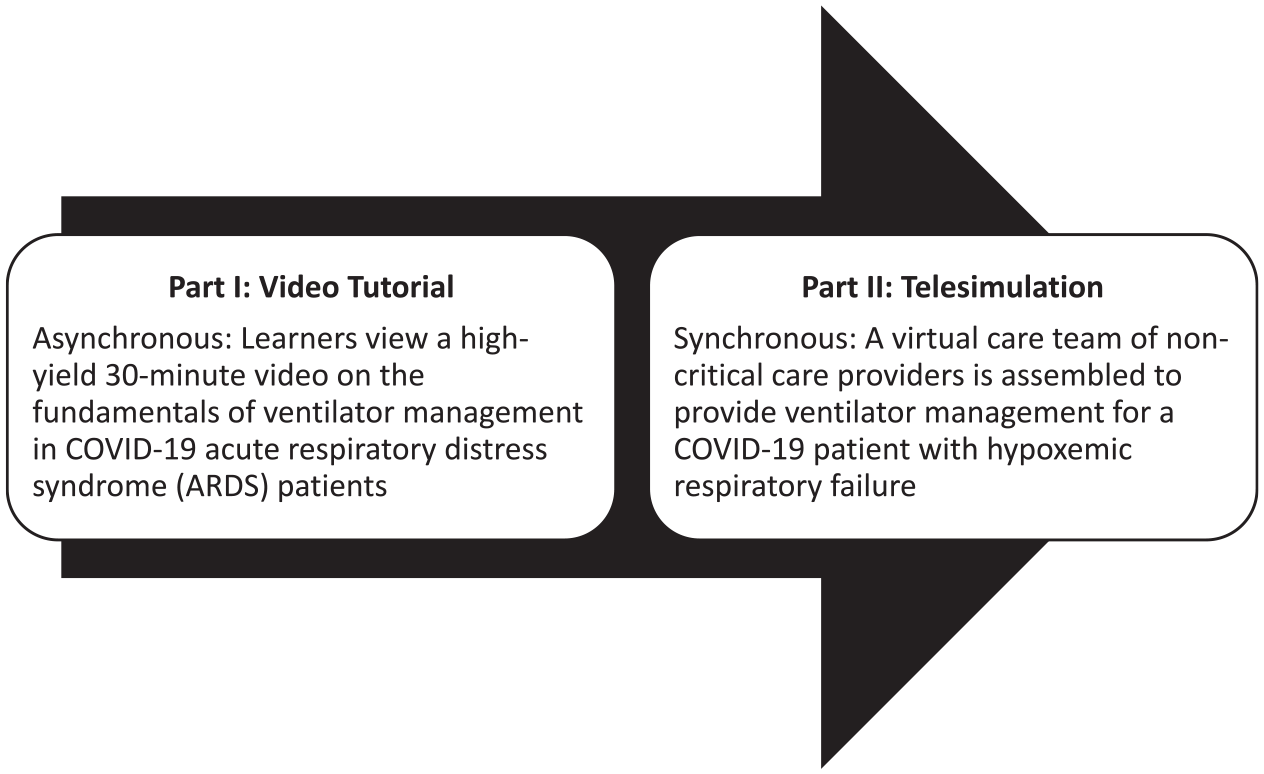
Hybrid design of telesimulation innovation.
In the second part of the training, a high-fidelity adult manikin simulator (HAL S-3201, Gaumard, Florida) was set up inside our simulation center and operated locally by a wireless tablet computer. The manikin’s vital signs were displayed on a monitor that was also wirelessly operated by the same computer. A set of test lungs (TL2 PRO Test Lung System; South Pacific Biomedical, California) was positioned over the manikin’s chest (underneath a gown) and connected to a mechanical ventilator (LTV 1200; Vyaire Medical). A circumferential band was wrapped around the test lungs to mimic the reduced lung compliance of a patient with acute respiratory distress syndrome (ARDS). A portable camera system (Live Capture; B-Line Medical, Washington, DC) was used to provide real-time images of the ventilator and vital sign monitor. This camera system was connected to a laptop with an integrated webcam that provided real-time images of the simulation faculty and manikin’s head and torso. Web video conferencing software (Zoom Video Communications, Inc. San Jose, CA) installed on the laptop was used to create a virtual meeting room for remote participants to join via invitation. The laptop screen was shared with all the participants in the virtual meeting room so that cycling through all three cameras provided views of the manikin (with faculty), vital sign monitor, and ventilator throughout the simulation. Each group of five participants formed a virtual care team assigned to care for a newly intubated adult COVID-19 patient with hypoxemic respiratory failure. The virtual care team was tasked with managing the ventilator in response to the patient’s vital signs, measured ventilator pressures, and arterial blood gas values. A faculty member operated the ventilator locally on camera according to the team’s instructions via the video conference. Directed feedback was used to optimize the achievement of learning objectives in this short session. A 20-minute post-simulation debrief led by the simulation faculty member focused on the team’s clinical decisions in ventilator management and reviewed key concepts, such as low tidal volume ventilation, plateau pressures, and breath-stacking/auto-PEEP (positive end-expiratory pressure). The latter part of the debriefing allowed us to generate feedback about the value of the experience as well.
Discussion
The Center for Disease Control (CDC), local government, and hospital models predicted that the number of critically ill COVID-19 patients requiring mechanical ventilation would overwhelm our available critical care and anesthesiology teams (Ajao et al., 2015; CDC, 2020). For New York City, the epicenter of the virus in the United States, this intense and unprecedented demand required (and continues to require) urgent, effective training to educate non-critical care providers assigned to assist in the care of critically ill and mechanically ventilated COVID-19 patients with ARDS. Consequently, we operationalized our training immediately, but also knew it was necessary to assess how our hybrid, two-part model of telesimulation would be received so we could make iterative changes as needed.
End-of-course feedback suggests that learners found this two-part model of telesimulation innovation very useful. The combination of a video tutorial followed by an interactive telesimulation allowed healthcare providers to participate remotely from their home environment while also scheduling their limited availability during the coronavirus pandemic. In just the first week, the video tutorial has been viewed over 500 times and we have facilitated 15 telesimulation sessions, including 51 participants comprised of hospitalists, emergency medicine physicians and physician assistants, pediatric residents, nurses, and a nurse educator. All participants shared with us that this hybrid model of telesimulation improved their knowledge of ventilator management for COVID-19 ARDS patients. Although these sessions were facilitated through video conferencing, many participants shared with us that the telesimulation felt similar to a typical in-person simulation because they were able to remotely manipulate the ventilator settings through the faculty at the simulated patient’s bedside. Interestingly, while most participants stated that the education experience was extremely beneficial, some of the comments from the more experienced physicians suggested that they desired the ability to move beyond initiation and adjustment of ventilator settings to troubleshooting acute problems that may arise during a course of mechanical ventilation. These comments may reflect advanced learners (i.e. competent or advanced beginners) or individuals apprehensive about their ability to respond to problematic situations. Typically, telesimulation features a simulation like that in Part II of our experience, where the learner decisions are executed by a person at the bedside of the patient simulator (McCoy et al., 2017). Since operating a ventilator can be a complicated skill to learn, we felt that the requirement for learners to gather knowledge through the Part I video tutorial prior to practicing was especially important. The learners could stop, replay, and view the content at their leisure as many times as they needed to prepare for the telesimulation practice. In fact, many of the learners referenced the video tutorial while making decisions during the simulation.
While telesimulation has been described in the literature previously, there is still minimal research published demonstrating its breadth of utility (McCoy et al., 2017, 2019). Given the overall positive feedback, we believe that this learning session was successful in providing timely education during a coronavirus pandemic. Furthermore, it reinforced the value and flexibility in which simulation education could continue conveniently for learners despite significant restrictions in place during the coronavirus pandemic. As the driver for development of this module was to provide urgent education in the midst of a clinical crisis, we did not formally assess the impact on learning and performance. Explicit research is needed to assess the efficacy of this hybrid intervention in preparing healthcare workers and to determine if the knowledge is successfully transferred to the clinical setting.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Contact:
Contact:
Contact:
Contact:
Contact: