
Abstract
Challenging behaviors (CBs) are frequently observed in children with autism spectrum disorder (ASD) and are known to have negative effects on parents’ stress and well-being, as well as on overall family quality of life. Research has shown that professional support such as the Prevent-Teach-Reinforce (PTR) program has the potential to alleviate those effects. Although several studies have empirically demonstrated this positive behavior support program in managing children’s CB, its implementation by community-based educators among parents of children with ASD has yet to be examined. This study assessed the facilitators and obstacles to this program’s implementation as perceived by 19 parents using interviews and questionnaires. Participants emphasized the significance of setting clear expectations, defining roles, and providing continuous feedback during the implementation process to promote their initiative and enhance their active participation. They recognized the difficulties of implementing the program within a family setting but emphasized the valuable presence of educators in the home, which improved their understanding of family dynamics. Parents valued effective and respectful support from educators, although some encountered disagreements during coaching sessions, highlighting the need for improved educator training with practical coaching and a greater recognition of the family’s perspective.
Autism spectrum disorder (ASD) is a neurodevelopmental disorder that can include impairments in communication, social interactions, and restricted or repetitive behaviors, interests, or activities (American Psychiatric Association, 2013). In Canada, where this study took place, the prevalence is approximatively 1 in 50 in children with 54% being diagnosed before the age of 5 (Public Health Agency of Canada, 2022). In addition to the symptoms associated with this diagnosis, young children with ASD often display comorbidities such as challenging behaviors (CBs; Maskey et al., 2013; Nicholls et al., 2020; Ooi et al., 2011). These behaviors can take many forms, including aggression (e.g., kicking, hitting, biting), self-injury, or tantrums (Peña-Salazar et al., 2022), and they have damaging repercussions on children’s well-being and integration (Baker-Ericzén et al., 2005; Blacher et al., 2005; Fitzpatrick et al., 2016; McGill et al., 2018). Moreover, CB may also impact family functioning and parental well-being (Corcoran et al., 2015; Hastings & Johnson, 2001; Mackintosh et al., 2012). Indeed, the presence of CB in children is correlated with higher levels of parenting stress (Estes et al., 2013; Lecavalier et al., 2006; Mello et al., 2022; Rivard et al., 2021; Shawler & Sullivan, 2017) and of depressive symptoms (Kim et al., 2016) in parents. Furthermore, CB are often associated with social stigma that may further exacerbate parenting stress and mental health issues (Smart et al., 2023). This can further contribute to isolate parents from informal social support and their child from rich learning environments (Zaidman-Zait et al., 2014). A recent survey showed that more than half of parents of children with special needs reported feeling inadequate in addressing their children CB because they lack support (Grenier-Martin & Rivard, 2022). Indeed, social and professional support are linked to better family quality of life, child development, and parental well-being (Vasilopoulou & Nisbet, 2016).
Educators working in a community-based setting are mandated to provide free services to children with ASD under age 7 (Ministère de la Santé et des Services sociaux, 2003) and dispense early intensive behavioral intervention (EIBI) in the child’s daycare or at home. While the exact level of intensity (i.e., hours per week) may fluctuate based on the individual child’s requirements, EIBI educators are frequently expected to assist and support the child’s family. A needs assessment study was conducted among community-based EIBI educators across the province concluded that they needed training and supervision to implement a CB management program that would involve parents (Rivard, Morin, et al., 2015). Following these findings, a team consisting of researchers, managers, educators, and parents followed a community-based participatory process (Collins et al., 2018) to collaboratively select a CB management program to be implemented by parents in their homes, assisted by their children’s EIBI educators.
Prevent-Teach-Reinforce: A Positive Behavior Support Program
The Positive Behavior Support (PBS) approach is currently considered a best practice in interventions for individuals with CB (Gore et al., 2013; Hieneman, 2015; National Institute for Health and Care Excellence, 2018). Its positive effects on children, parents, families, and staff have been extensively documented in a wide range of context such as homes, schools, specialized services, and in residential settings (e.g., Carr et al., 2002; McGill et al., 2018). PBS is an individualized approach that utilizes a comprehensive format to gain a deeper understanding of and subsequently decrease CB. This approach encompasses various elements such as modifying the person’s surroundings, enhancing their skills, offering targeted support, and creating reactive strategies (National Institute for Health and Care Excellence, 2018). It is found in many models and programs that can be adapted to different settings and age groups (Carr et al., 2002). Common features across all PBS models are data collection, functional behavior assessment, and the implementation of a behavior support plan (Carr et al., 2002; Gore et al., 2013).
One specific PBS program that have been shown to be effective in children with CB is the Prevent-Teach-Reinforce (PTR; Dunlap et al., 2010). Initially developed to help primary school teachers or other school personnel address CB in classrooms (Dunlap et al., 2010, 2018a), this program was later adapted for preschool children in PTR for Young Children (PTR-YC; Dunlap et al., 2013). The PTR-YC program also encourages family involvement and participation in every step of the process. It may be especially suited to meet the needs of families of children with ASD along with EIBI educators’ desire to collaborate with, and directly support, parents in managing CB. PTR-YC is tailored to young children’s developmental characteristics and to early educational childhood settings. It aims the promotion of functional behaviors in children and reduction of CB by implementing prevention strategies, teaching appropriate alternative behaviors, and emphasizing positive reinforcement and quality of life (Dunlap et al., 2013, 2022).
The structure of PTR remains the same across versions and models. The person in charge of implementation guides a team comprised of significant individuals in the child’s life (e.g., parents, siblings, school or daycare staff, other professionals, etc.) through the program’s steps: (a) identification of the target behavior, (b) data collection, (c) functional behavior assessment, (d) implementation of a behavior support plan, and (e) support and coaching for the family (Barnes et al., 2020; Dunlap et al., 2018b). The behavioral support plan should incorporate strategies from all three categories: prevent, teach, and reinforce. Preventive strategies involve proactively modifying the child’s environment, routines, and interactions to reduce known antecedents for CB (e.g., creating a more supportive and structured environment, reducing triggers, etc.). Teaching strategies focus on equipping the child with appropriate behaviors that serve the same function as the CB (e.g., communication skills, social skills, or alternative means of expressing needs). Reinforcement strategies aim to encourage appropriate behaviors while minimizing CB (e.g., positive reinforcement, intentional ignoring, etc.). For a detailed overview of all available strategies, please refer to the PTR-YC manual (Dunlap et al., 2022).
Involving and collaborating with the family is at the heart of this program and promoted in every step of implementation. Additional positive features of PTR-YC are its user-friendly materials (e.g., implementation manual, data collection grid, functional behavior assessment questionnaire) and the fact that it does not require costly, official certification. Owing to these characteristics, the PTR-YC program was selected for implementation in community-based services for ASD because it could meet parents’ need for support and structure in managing their child’s CB with the guidance of their EIBI educator.
Two studies provide empirical data supporting the effectiveness of PTR-YC (Dunlap et al., 2018b; Harvey et al., 2021). In their randomized controlled trial involving 169 children, Dunlap and colleagues (2018b) reported a significant reduction in CB and an increase in social skills for the experimental group, although the effect size was small for both variables (η²p = .062). In a recent case study with three children, Harvey et al. (2021) examined the effectiveness of PTR-YC and reported a decrease in CB and an increase in prosocial interactions. In both of these studies, the facilitator (the person in charge of guiding the PTR team) was a member of the research team with extensive experience in the PTR model and PBS, and the individuals responsible for implementing the program were teachers.
This article is part of a broader investigation, which is the first to evaluate the implementation and efficacy of PTR-YC when facilitated by EIBI educators, rather than a PTR specialist or members of a research team, with parents carrying out the implementation. To date, two papers stemming from this broader investigation have concluded that PTR-YC, when implemented in such a context, reduced CB in children and reduced stress in parents (Rivard et al., 2021), and resulted in positive changes in EIBI educators’ emotional responses to CB (Mestari et al., 2023). This study aims to identify the factors that may hinder or facilitate the implementation of PTR-YC, according to parents’ points of view. In doing so, it seeks to understand their experiences and perspectives in addressing their children’s CB while being supported by EIBI educators.
Conceptual Framework
Research continues to underscore the importance of program evaluation in the field of behavioral intervention (Long, 2023; Parrott & Carman, 2019). Although it is essential for every stakeholder to be heard, the voices of parents are often overlooked. Yet, they play a central role in providing information about their child and family and are critical partners in implementing strategies into their daily routine. This study adopted Chen’s (2015) logical model for program evaluation to help categorizing obstacles and facilitators to implementation into six main components: (a) implementing organization (i.e., a public ASD service provider), (b) intervention (i.e., PTR-YC), (c) specific ecological context (i.e., home-based intervention), (d) implementers (i.e., parents), (e) targeted population (i.e., their children with CB), and (f) partners (i.e., EIBI educators). The six components specific to the PTR-YC program are presented in Figure 1.
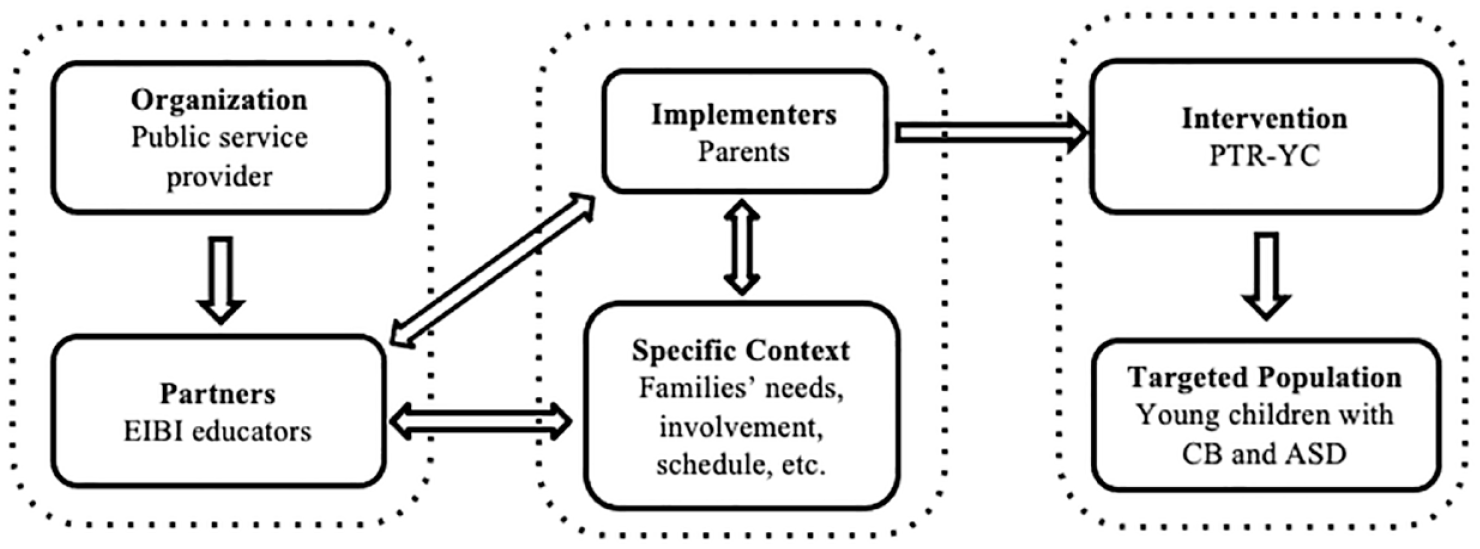
Logical Model of the six Components for the PTR-YC Program Implementation
Even though PTR-YC has been evaluated in term of efficacy, no study to our knowledge document its implementation in a program evaluation perspective. As such, this article is part of an effort to bridge the research-to-practice gap (Romano & Schnurr, 2022) by assessing parents’ perception and experience of the PTR-YC program’s implementation.
Objectives
This article was part of a larger study that aimed to assess the implementation of PTR-YC within public ASD services in the province of Québec (Canada), which was approved by the Université du Québec à Montréal and the public service provider ethics committees. The effects of this intervention on children’s CB and appropriate behavior and on parents and educators’ well-being have been reported in previous papers (Mestari et al., 2023; Rivard et al., 2021). The focus of this article was on parents’ perception of the quality of implementation and their general satisfaction with the program. Specifically, it sought to document the obstacles and facilitators to implementation as experienced by parents using Chen’s (2015) six components logical model for program evaluation.
Method
Design
This study adopted a cross-sectional mixed-methods design (Gaudet & Robert, 2018). More specifically, a concurrent triangulation design was employed in which qualitative and quantitative data were collected simultaneously and analyzed separately before being compared (Creswell & Creswell, 2018). Qualitative data were collected through semistructured interviews and open-ended questionnaire items (Braun & Clarke, 2006), and quantitative data were collected through questionnaires.
Participants
Recruitment was conducted in partnership with the participating public ASD service provider. Of the 30 parents who took part in the larger PTR-YC validation study, 19 (63%) agreed to participate to the interview and complete the questionnaires on implementation. The social and demographic characteristics of participating families are detailed in Table 1. The median age for children was 4 years (range: 4–5); children were mostly boys (72%). Median family income was approximately $60,000. Most families (67%) were nuclear in composition and had both parents born in Canada (78%). For additional socio-demographic data about the children, please refer to Rivard et al. (2021), and for information about educators, consult Mestari et al. (2023).
Social and Demographic Characteristics of Participating Families.
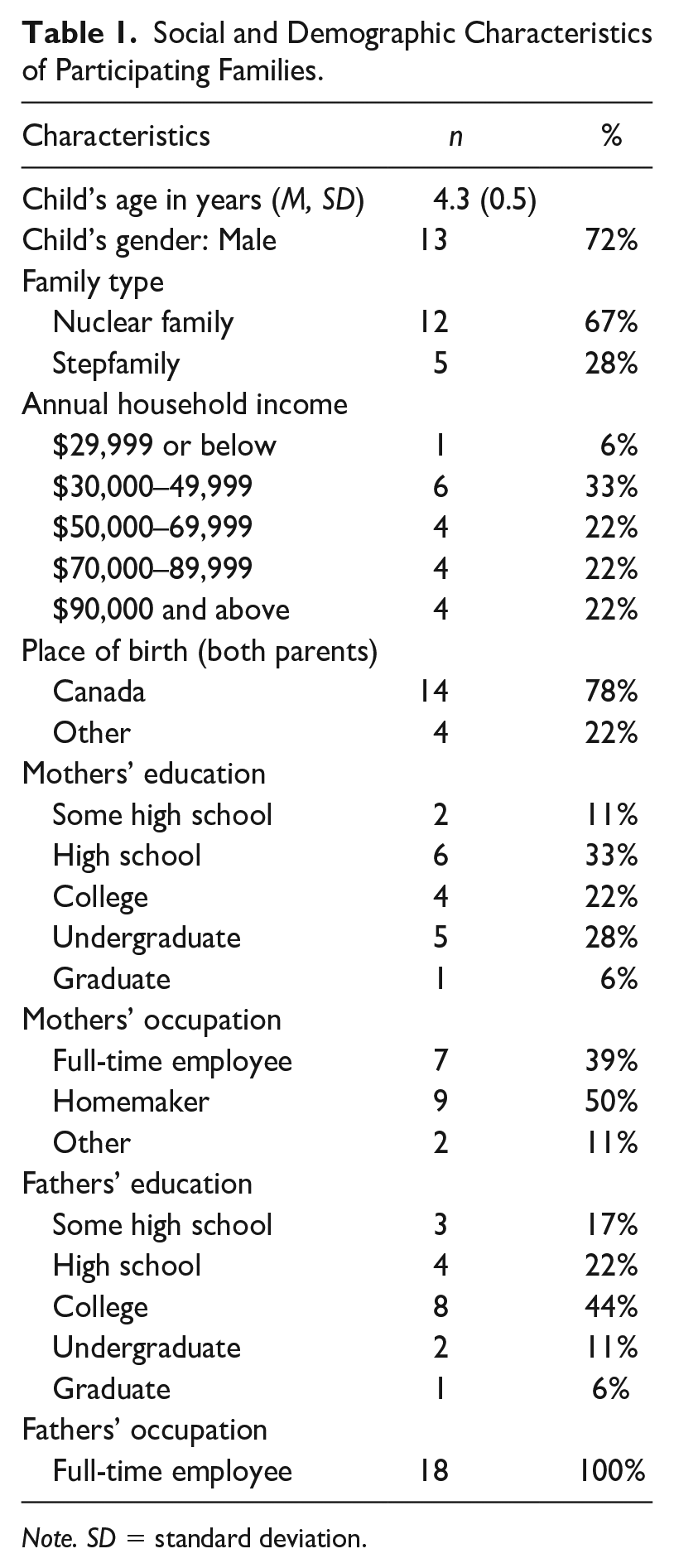
Note. SD = standard deviation.
Intervention
Four members of the research team (one psychologist, two psychology doctoral students, and one board-certified behavior analyst) were responsible for training and supervising the participating EIBI educators. All four researchers received in-person training from one of the primary authors of PTR-YC before implementing the program themselves. Prior to implementation, educators received 12 hours of in-person group training over the course of 2 days. Following this training, each educator implemented PTR-YC with a family. Over the course of 12 weeks, they guided and coached parents through each step of the program in weekly home meetings that lasted approximately 1 hour. Throughout program implementation, educators received weekly supervision by one of the four members of the research team.
Measures
Structured Interview
The first author developed an interview schedule for this study, which was subsequently reviewed independently by four experts, including three qualitative researchers and one clinical psychologist specializing in ASD and CB. The final interview schedule included two sections: (a) general questions about the program (e.g., global appraisal, comments) and (b) experience with the implementation of the program (e.g., its specific steps, meeting with educators, using the materials, etc.).
Satisfaction Questionnaire
This questionnaire was adapted from an instrument used by Rivard, Mercier, et al. (2015) to measure parental satisfaction with an EIBI program. The questionnaire was adapted and revised with the help of two of the authors of the original instrument to fit the context of this study and to incorporate components that were specific to the PTR-YC program. This yielded a table containing 17 general statements on the implementation of the program such as “How satisfied are you with the content of the meetings?” or “How satisfied are you with coaching sessions?” Respondents rated each statement on a 4-point Likert-type scale (from 1 = not satisfied to 4 = very satisfied).
Customer Satisfaction Questionnaire Scale
The Customer Satisfaction Questionnaire Scale (CSQ-8; Larsen et al., 1979) is the product of 12 studies involving nearly 8000 participants. It was reported to have excellent psychometric properties (Attkisson & Greenfield, 1996). The CSQ-8 has been used in a context similar to this study (Rivard, Mercier, et al., 2015) to assess parents’ satisfaction with a community-based EIBI program.
Open-Ended Questions
Participants were asked four open-ended questions at the end of the previously mentioned questionnaires: (a) “Have you noticed changes in your child?,” (b) “What were the effects of the program on your family?,” (c) “What did you like the most about the program?,” and (d) “What changes should be made to the program?” Participants were prompted to answer each question in brief sentences.
Procedure
Data collection took place immediately at the end of the implementation period for PTR-YC. Parents completed the interview and the questionnaires in a single postintervention assessment session. To ensure the neutrality of both the participant and the interviewer, interviews were conducted by a trained research assistant with no prior involvement in the study. Interviews lasted on average 60 minutes and were recorded for subsequent transcription by another research assistant.
Analysis
The qualitative analysis of interview transcripts was conducted in two steps. First, the transcripts were coded by two graduate students. They conducted content analysis (L’écuyer, 2011; Patton, 2014) for each of the six components of the logical model (Chen, 2015). Relevant units of meaning (UoMs) were extracted and compiled into 12 categories (i.e., facilitators and obstacles, respectively, for each of the six components). Both students coded 30% of transcripts to obtain interrater agreement ratio, which was good to excellent (M = 95%; range: 81%–100%).
Second, the two original coders and the first author carried out a thematic analysis (Braun & Clarke, 2006; Creswell & Creswell, 2018; Merriam & Tisdell, 2015). They each independently extracted the themes raised by participants for each component through an inductive open-coding approach. The UoM for each of the 12 categories were coded by two individuals who separately constructed a grid that contained the themes that emerged in the interview. They then compared their results to build a final, consensual coding grid specific to each category. This consensual grid contained all the themes and sub-themes present across interviews. Then, the third person, who had not participated in developing the grid, used it to categorize all UoM into appropriate themes and subthemes. This step yielded the results presented in this article. Written responses to the open-ended questions were analyzed using the same process as the interview transcripts.
Responses to the two satisfaction questionnaires were analyzed quantitatively. Descriptive statistics were computed on dichotomous variables (i.e., frequency and percentage) and Likert-type scales (i.e., mean and standard deviation).
Results
Structured Interview
Overall, 1136 UoM were extracted across all interviews and included in thematic analysis. Facilitators included 727 UoM distributed across the six components as follows: “Organization” 14 UoM (2%), “Intervention” 278 UoM (38%), “Context” 74 UoM (10%), “Educators” 217 UoM (30%), “Children” 23 UoM (3%), and “Parents” 121 UoM (17%). Obstacles included 409 UoM distributed as follows: “Organization” 26 UoM (6%), “Intervention” 97 UoM (24%), “Context” 111 UoM (27%), “Educators” 23 UoM (6%), “Children” 97 UoM (24%), and “Parents” 55 UoM (13%). Tables 2 and 3 summarize themes and subthemes for facilitators and obstacles. These are described in greater detail for each component in the following sections and supported with representative excerpts from transcripts (translated from French).
Classification of 727 Units of Meaning Representing Facilitators by Component.
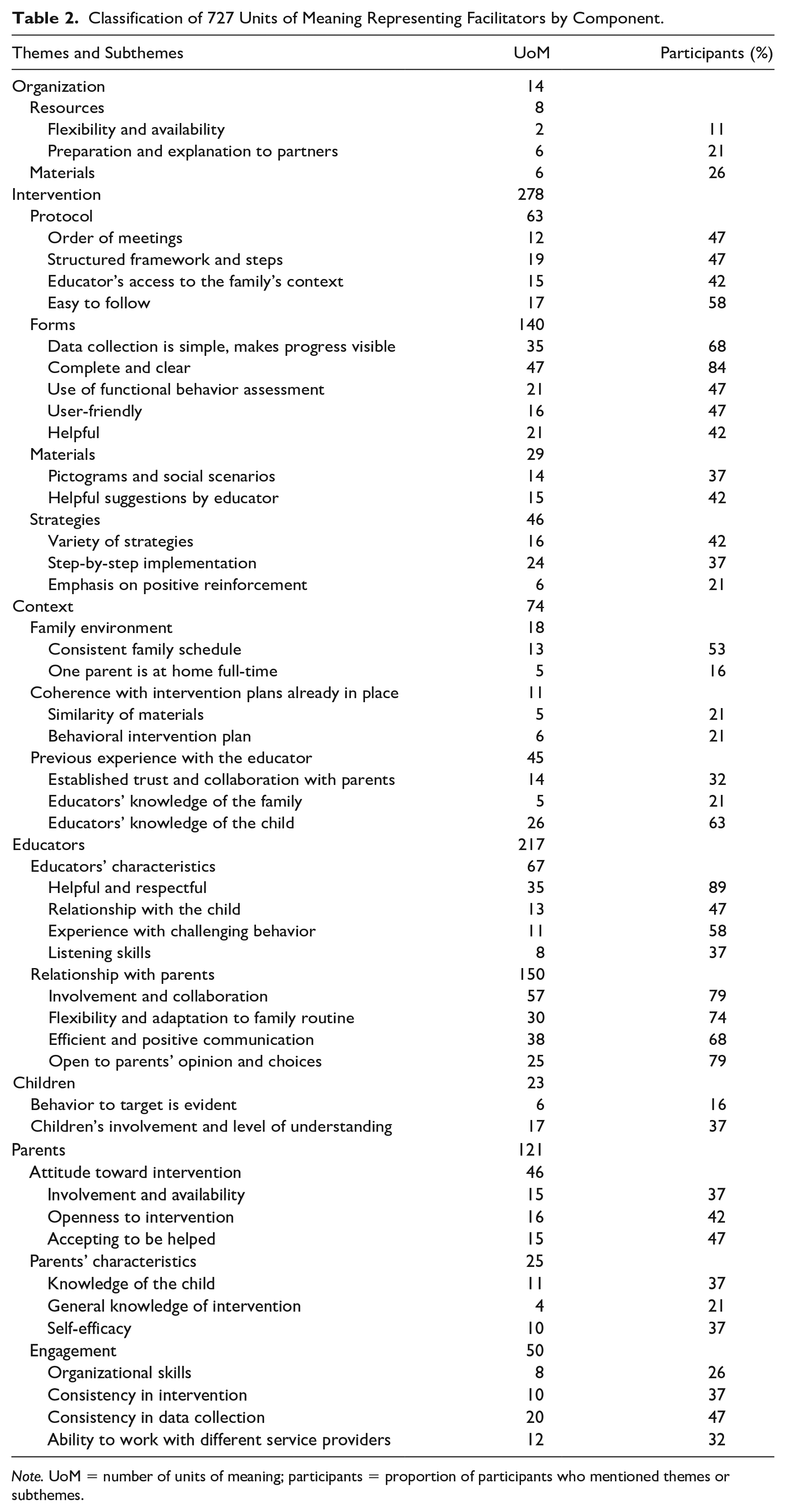
Note. UoM = number of units of meaning; participants = proportion of participants who mentioned themes or subthemes.
Classification of 409 Units of Meaning Representing Obstacles by Component.
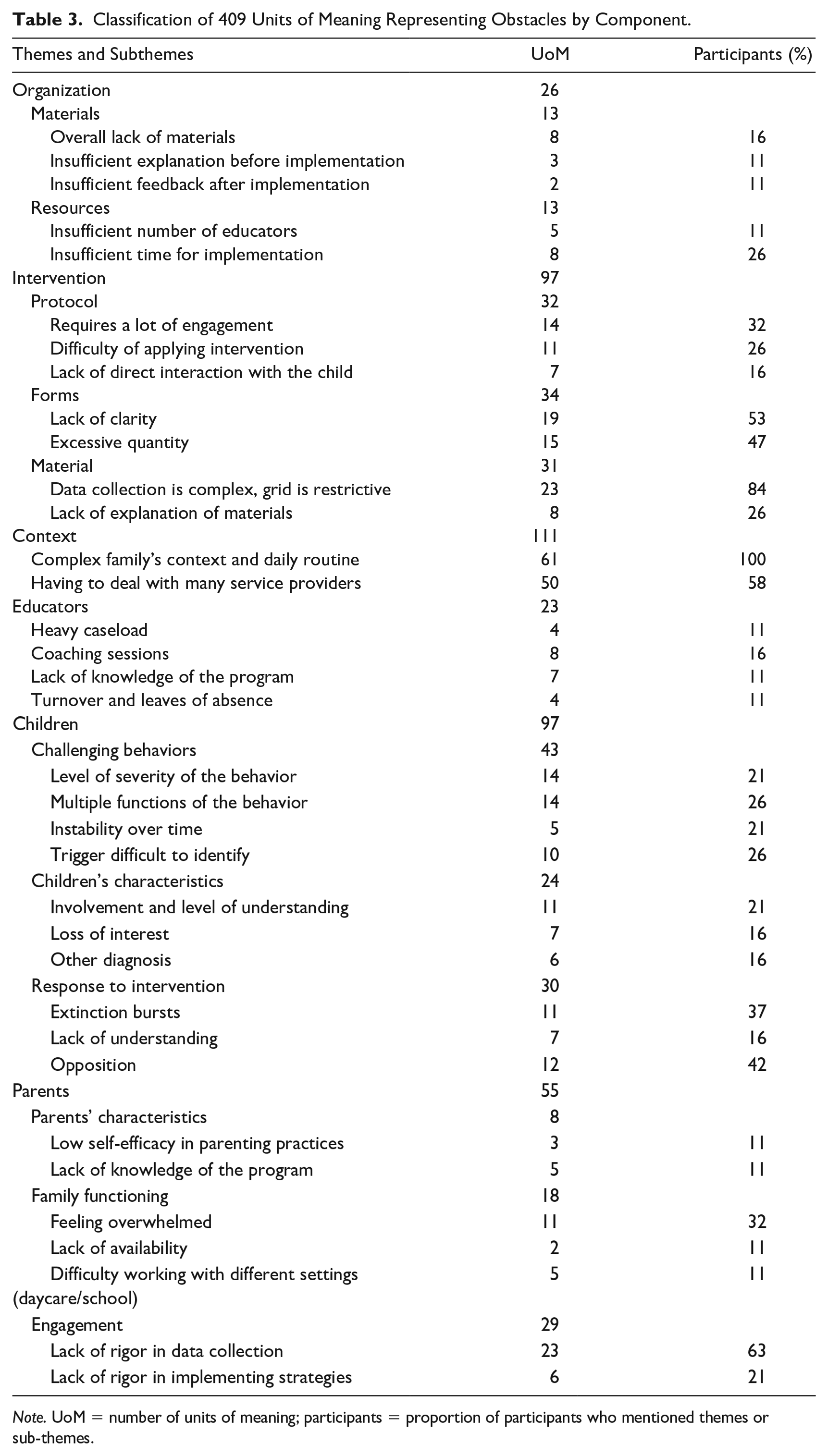
Note. UoM = number of units of meaning; participants = proportion of participants who mentioned themes or sub-themes.
Organization
Two themes were raised in relation to this component: (a) resources and (b) materials. Resources mainly concerned the time and personnel provided by the organization, whereas materials encompassed all the information and documentation provided by the organization.
Regarding resources, some participants mentioned staff availability and flexibility for team meetings (11%) and effective documentation of the main steps of the program (21%) as facilitating factors (“The program is flexible [. . .] I can’t tell you all that we switched, changed and adjusted, but it provided a lot of freedom.”) Conversely, they mentioned a lack of educators in community services (11%), and therefore, educators’ less time to allocate to each family and, by extension, for meetings (26%), as obstacles to implementation (“I would have taken more time with the educator, but I know she had other families to attend to.”)
Participants found the supplied informational materials helpful (26%; “I felt well prepared because, from the start, we had a lot of information about the program, both from the research project and from the educator.”) However, some reported that the insufficiency of materials provided (16%), as well as a lack of information prior to implementation and of feedback after implementation were unsatisfying (11%).
Intervention
Four themes arise regarding the intervention itself: (a) the protocol (i.e., the steps), (b) forms (part of the intervention by design), (c) materials used for implementing intervention strategies, and (d) the strategies themselves were mentioned in relation to the Intervention component. The fourth theme was only mentioned as a facilitator.
Participants found the intervention protocol easy to follow (58%), liked the order of meetings (47%), and enjoyed the structured and step-by-step approach (47%; “So we always started each meeting with a questionnaire or a grid [. . .] and then we ended with new topics or interventions. Honestly, it went so well that it became part of a routine.”). They also mentioned the home visits by the educator for meetings as facilitating direct access to their family’s context (42%). However, some participants criticized the lack of interaction between the educator and the child (16%). They also expressed that the program required more involvement than they had expected (32%) and that they had difficulty applying intervention strategies (26%; “It had positive effects, but it was still a big investment of our time and our life. It takes time to improve [. . .] you have to invest yourself a lot.”)
Regarding the intervention forms, most participants reported they were clear and easy to understand (84%). They also said the forms were user-friendly (47%) and had helped to guide them through the program (42%; “It’s the way things are arranged, the program’s steps, it’s very functional [. . .] there are no secret tricks, it’s clear and it’s concrete and it’s precise and it works!”). They reportedly appreciated the fact that functional behavior assessment was conducted with a questionnaire (47%). However, some participants found that there were too many forms (47%) and that some of these could have been made clearer (53%). While most appreciated the program’s data collection method (68%), many found it complex and sometimes restrictive (84%; “You have to remember to do it, and sometimes [the data collection system] is not adapted to the behavior or the time of day.”).
The materials provided by educators for the intervention, such as pictograms, social scenarios, timers, and clickers (37%), along with suggestions on how and when to use these (42%), were mentioned as facilitators to implementation. In contrast, some parents reported that the lack of program-specific explanations and their uncertainty toward the use of these materials (26%) hindered their implementation of the intervention.
Participants appreciated the variety of strategies included in the program (42%). The step-by-step description of each selected strategy (37%) and the fact that positive reinforcement was strongly promoted (21%) were also valued by parents (“It’s really easy to choose among all the strategies and to use reinforcements in different contexts. It’s really well-made and gives a clear procedure.”)
Context
Three themes were mentioned in relation to this component: (a) families’ context, (b) their experience and collaboration with educator, and (c) the program’s consistency with their child’s ongoing behavioral intervention (i.e., EIBI). There were no subthemes for obstacles associated with this component.
Having a steady routine and a clear family schedule (53%) and, in some cases, a stay-at-home parent (16%) were seen as facilitating factors to implementation. However, parents unanimously reported that the fact that implementation took place in their home (100%) made it inherently more difficult.
Having previously collaborated with the child’s educator was seen as a facilitator because this gave the educator insight about the family’s (21%) and the child’s (63%) characteristics (“She already knew [the child]’s history, so that made it a lot easier. You know, we’re not starting from scratch with someone who doesn’t know our girl, [. . .] she can guide us much more.”). This prior relationship also enabled parents and educators to build trust (32%). However, collaborating with multiple partners (e.g., more than one educator, school, daycare, etc.) proved to be complex and demanding (58%; “We had a lot of meetings outside the program [. . .] for all his other needs. We had a busy schedule. It became a bit of a mountain.”)
The program was seen as consistent with the behavioral intervention (21%) already in place. Indeed, the similarity with materials that parents were already using (21%) facilitated their understanding of PTR-YC intervention strategies.
Educators
This component included three themes related to educators’ (a) characteristics, (b) relationship with parents, and (c) employment and personnel issues. The last theme was not included under the Context component because it related specifically to educators.
Educators’ helpfulness and respectfulness (89%) and their experience working with children who display CB (58%) were the characteristics most often mentioned as facilitators. Participants also mentioned that educators’ positive relationship with the child (47%) and good listening skills (37%) were helpful (“She was so kind! She loved him a lot, my little guy, it showed in the way she interacted with him [. . .] it made him approach her easily because he felt comfortable, accepted.”). However, some parents found that educators’ lack of mastery and knowledge of the program was problematic (11%).
Regarding educators’ relationship with parents, many participants reported that educators’ ability to promote parents’ involvement and collaboration (79%) while leaving room for them to make choices (79%) were major facilitators. Moreover, educators who showed flexibility and adapted to the family’s routine (74%) or used positive vocabulary and communicated efficiently (68%) were appreciated by participants (“The first two or three weeks, she had to come to our home often and at moments where we and [the child] were available.”). Some participants found coaching sessions relationally challenging and a source of disagreements with educators (16%).
Participants only mentioned educators’ working context as an obstacle. Indeed, a heavy caseload (11%) and frequent leaves or educator turnover (11%) were sometimes said to interfere with implementation (“I would have preferred it to be the same educator all year, but after two or three months, we had to change. [The child] knew her, she trusted her, so changing from one day to the next was difficult.”)
Children
This component included three themes in relation to children’s (a) CBs, (b) personal characteristics, and (c) response to intervention. These themes were largely discussed as obstacles by participants.
Although having a straightforward target for intervention (e.g., if the CB was the child’s only CB or the most salient or urgent one) was a facilitator according to some participants (16%), many aspects of CBs were seen as obstacles, such as their high severity level (21%), unidentified triggers or antecedents (26%), multiple functions (26%), or instability over short periods of time (21%; “We went through a lot of trial-and-error because the behavior was so complex. Finding what triggered it and the function it served took us a lot of time and effort, but it paid out.”)
Children’s level of understanding and ability to participate in the PTR-YC process (37%) was the only child characteristic raised as a facilitator (“With some [children] it goes faster, others slower, so everything will depend on the child. The best strategy we had was to go gradually and accept to put some things aside for a time.”) Conversely, children’s low level of understanding of (21%), or rapid loss of interest in (16%), the intervention were seen as obstacles. The child’s other diagnoses (e.g., intellectual disability or learning disability) were sometimes mentioned as hindering implementation (16%).
Children’s response to the intervention, such as their opposition to it (42%) or lack of change (16%) following the introduction of new strategies, was only mentioned as an obstacle. Participants also mentioned extinction bursts (i.e., a sudden and temporary increase in CB following the beginning of intervention strategies) as problematic in some cases (37%; “We started the intervention [. . .] and we just lost her. She goes into a crisis. She’s on the floor, shaking, she wants nothing, she doesn’t want to cooperate anymore.”)
Parents
This component includes the following themes: parents’ (a) characteristics, (b) engagement, and (c) attitudes toward intervention.
Parents’ knowledge of their child (37%), their knowledge and understanding of the program (21%), as well their high level of self-efficacy (37%), were three characteristics perceived as facilitating implementation (“We were quick [. . .] to find ways to reinforce him. Because [the educator] explained the program well and because we know our child, we were confident about what would work easily.”) Conversely, parents’ low self-efficacy (11%) and poor understanding of the program (11%) were reported as obstacles.
Parents’ consistent participation in data collection (47%) and in the intervention (37%), along with their self-organization skills (26%) and ability to deal with many service providers (32%) were facilitators related to parental engagement facilitators. In contrast, parents’ lack of rigor in data collection (63%) and implementing the intervention (21%) were obstacles to the optimal implementation of the program (“It was so hard to always pay attention at the right time, when we had to do something like react a certain way or count the number of behaviors.”)
Participants’ attitudes toward the program could have facilitating effects when this included openness (42%), willingness to accept help (47%), desire to become actively invested in the process (37%). However, according to parents, being unavailable (11%) and overwhelmed (32%) hindered implementation (“It helped me, but there were times where you forgot to write it [the behavior] down. You have other things to do, it’s complicated. There were times that I completely forgot because, you know, dinner, the evening routine, all that.”)
Satisfaction Questionnaire
Table 3 presents the results for the 17 statements regarding parents’ satisfaction with the implementation of the program. Overall, parents reported being satisfied (i.e., >3, Somewhat satisfied) with respect to all but one statement, and their mean satisfaction level was high (M = 3.5, range = 1–4). Participants were most satisfied with the location of meetings (M = 3.9), the educator in charge (M = 3.9), the duration of meetings (M = 3.7), the information provided during implementation (M = 3.6), and the content of meetings (M = 3.6). Participants were least satisfied with data collection (M = 3.0), which was the only item rated below the Somewhat satisfied threshold. Other items with lower satisfaction ratings included the program’s impact on family functioning (M = 3.1) and observed changes in child’s behavior (M = 3.1).
Customer Satisfaction Questionnaire Scale
Table 4 presents results on the CSQ-8. Mean satisfaction across all eight items was high (M = 3.3, range = 1–4). Namely, participants said they “would recommend the program to a friend” (M = 3.7), and that it “improved their quality of life” (M = 3.4).
Quantitative Results Obtained on Two Satisfaction Questionnaires.
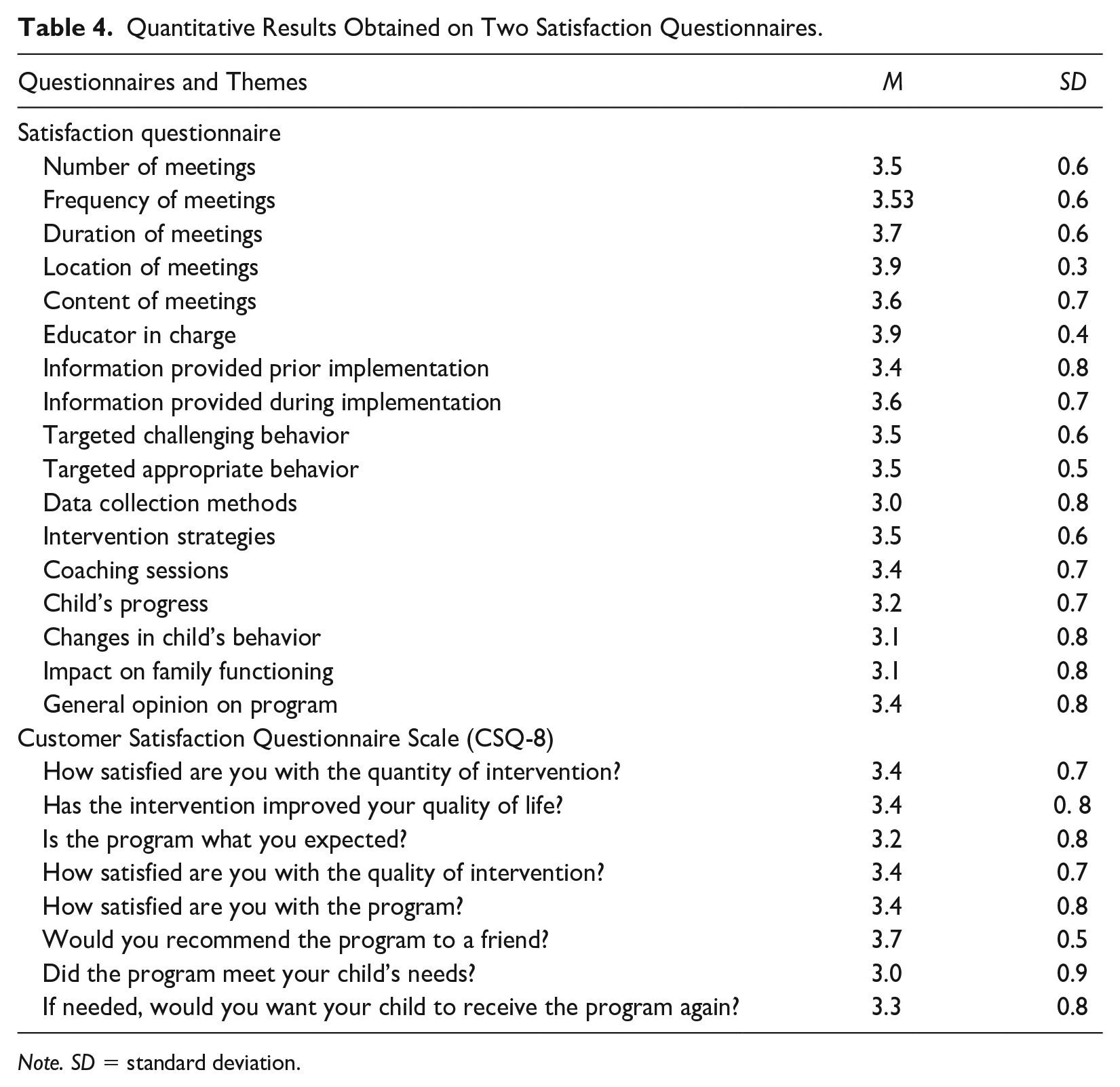
Note. SD = standard deviation.
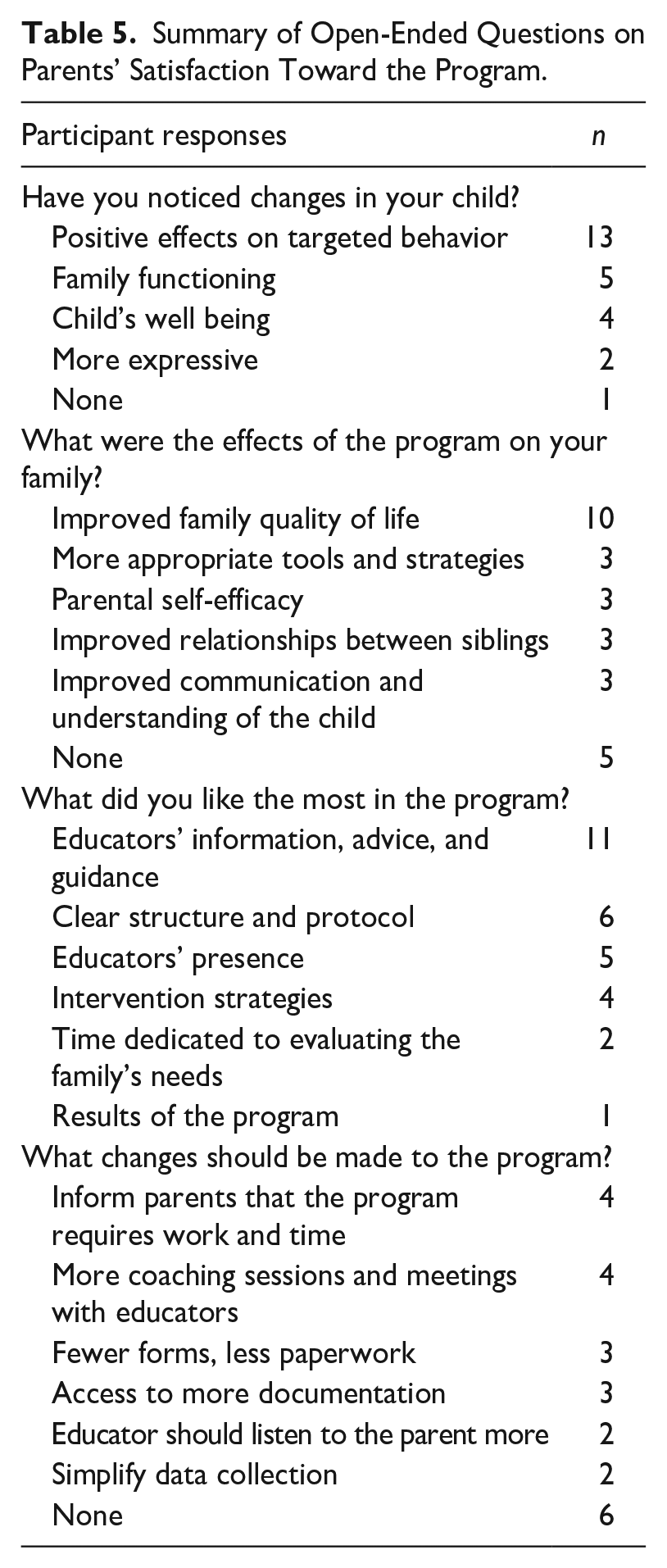
Open-Ended Questions on Perceived Effects of the program
Table 5 presents a summary of parents’ responses to the four open-ended questions about the program and its effect on their child. Many participants reported that they saw positive effects of the program on the target behavior (72%), while some noted changes in family functioning (28%) and well-being (22%). Participants reported that the program overall had a positive impact on family quality of life (56%), but some said it had no effects whatsoever (28%). Participants appreciated educators’ advice and guidance (61%) and their presence in the family home (28%). Participants also mentioned liking the clarity and structure of the protocol (33%) and its intervention strategies (22%). Participants reported that more efforts should be made to inform parents of the time and effort the program requires before beginning implementation (22%). They also mentioned that the program should include more meetings and coaching sessions with educators (22%). It is noteworthy that a third of participants (33%) reported they would not change anything about the program.
Summary of Open-Ended Questions on Parents’ Satisfaction Toward the Program.
Discussion and Implications for Practice
Families of children with ASD can experienced challenges related to the consequences of CB at home and need support in addressing these behaviors (Corcoran et al., 2015; Kim et al., 2016; Shawler & Sullivan, 2017). Community-based EIBI educators have expressed a need for better training in interventions specifically tailored to their young clientele and to support families regarding CB (Rivard, Morin, et al., 2015). The PTR-YC program (Dunlap et al., 2013) was retained for implementation within community-based EIBI services in Québec to support both educators and parents. This study aimed to better understand the perspective of 19 parents who played a leading role in this implementation of the PTR-YC program alongside their child EIBI educators, to provide insights into their point of view.
Overall, parents were satisfied with the program, including how team meetings were conducted and the user-friendly step-by-step protocol, and said they “would recommend the program to a friend.” These findings are in line with previous research on PTR when implemented with families in their homes by a member of the research team rather than an EIBI educator (Argumedes et al., 2021; Bailey & Blair, 2015). They also appreciated the program’s promotion of positive reinforcement and the variety of strategies it offered. Parents valued the supplemental materials provided by educator and participating in the selection of their contents or format (e.g., pictograms and social scenarios). Positive parental attitudes were seen by participants as facilitating the implementation of the program, further highlighting the potential benefits of the program, and providing a clear description of its steps (including the demands these may place on them) could help foster and maintain a positive attitude toward their role. Most parents reported positive effects of the program on their family and their own well-being. These results are encouraging as they suggest that a behavioral intervention on CB can help address issues of parental stress and well-being, despite these not being the focus of the program (Estes et al., 2013; Kim et al., 2016). Similarly, most parents reported a positive impact of the program on family quality of life. However, about a third of parents reported no effects, and it could be hypothesized that these families might have had children who displayed more CB and experienced higher levels of parental stress (Zaidman-Zait et al., 2014). They could also have been vulnerable families in need of additional psycho-social support (Rivard et al., 2021).
When tasked with the implementation of a parent-mediated intervention, community-based centers should ensure that all actors involved (i.e., parents, educators, supervisors, school or daycare partners) know their role and what will be expected of them (i.e., time, effort, and energy required). This could be achieved by providing adequate information prior to the intervention and, subsequently, providing feedback on a regular basis throughout the implementation phase. The amount and quality of information provided is key and a can be achieved via a comprehensive, step-by-step guide and practical tools. Parents reported that their knowledge of their child, their understanding of the program, and their self-efficacy were necessary to a good implementation. It is noteworthy to underline the fact that previous research has shown these families demonstrate a high level of commitment to their children and a remarkable ability to adapt (Chatenoud et al., 2014). This suggests that educators should include parents in the team and recognize the expertise they possess about their own child, while also providing sufficient guidance in the program to foster a sense of competence. While parents recognized that the use of forms are necessary to a good implementation, some found them burdensome and sometimes unclear (i.e., data collection grid, intervention plan). This underscores the importance of providing parents with more support and guidance for data collection and intervention strategy implementation, and suggests that simplifying certain forms could be beneficial. Consequently, a phone or tablet app could facilitate their use and completion. Such resources could empower parents to take initiative, foster a sense of ownership, and discourage excessive reliance on educators (Park et al., 2011). Considering that many parents faced challenges in maintaining consistency with data collection and implementing strategies, educators should be understanding of parents’ circumstances and make necessary adaptations to the program. This may involve shortening data collection intervals, utilizing a reduced number of intervention strategies, or dividing intervention responsibilities between both parents, all while ensuring the program’s integrity is maintained. While parents of children with special needs often reported feeling inadequate in addressing their children CB (Grenier-Martin & Rivard, 2022), educators should be sensitive to parents’ disposition and adapt the program accordingly.
Educators’ presence in the family home was paramount to a good implementation because it allowed them to observe the child and their parents in their environment. It helped them understand the family’s situation, which had a positive impact both on the assessment phase (i.e., selecting the CB to target, data collection, and functional behavior assessment) and the intervention phase (i.e., selecting strategies, implementing strategies, and coaching). Indeed, professional support is known to positively affect family quality of life, children development, and parents’ well-being (Vasilopoulou & Nisbet, 2016). Moreover, it provided educators with better knowledge of the family’s functioning, an understanding of the child, and offered opportunities to build a relationship of trust with parents. These findings strongly support the benefits of educators working at home, and this positive aspect of the program should be maximized, despite the inherent difficulties in coordinating educators’ and families’ schedules. Parents expressed their appreciation for respectful and supportive educators who communicated effectively with them. This is in line with previous research in which parents said the relationship with the educator is an essential source of support and plays a determining role in the quality of their experience of services for their children (Rivard et al., 2016). This indicates the need for educators’ training to include more practical activities for the coaching component of the program and place greater emphasis on the importance of involving families and acknowledging their perspective. They also regarded educators’ experience in managing CB as essential to the implementation of the program, suggesting that it would be pertinent to assign more experienced educators to families with children who exhibit more frequent or complex CB. However, this is often unfeasible due to high staff turnover and labor shortages. Potential solutions include increasing the frequency of parent-educator meetings, establishing closer educator-supervisor meetings, and possibly pairing educators together. Because some parents remarked that coaching sessions were a source of disagreement with educators, educator’s training should include more hands-on activities for this portion of the program. It should also underscore the importance of a parent-educator relationship based on trust, since professional support is linked to better family quality of life, child development, and parental well-being (Vasilopoulou & Nisbet, 2016). In addition, it should emphasize the importance of actively involving parents and recognizing their perspective. Aside from the difficulties they noted, parents enjoyed having their child’s educator act as guide throughout PTR-YC implementation and expressed appreciation for their advice and guidance. Indeed, it was shown that parents find a sense of recognition and awareness of accomplishments, with each milestone of their child’s development offering new learning opportunities (Myers et al., 2009).
Parents had the most difficulty working with CB that were severe (in terms of frequency, intensity, or duration), had unclear antecedents (i.e., the CB’s triggers were difficult to ascertain), or had multiple functions (i.e., obtaining something they want, avoidance, attention-seeking, self-stimulation). In such cases, a more experienced educator could be assigned to the child. It may also be helpful for the educator to meet with parents more frequently (e.g., meeting twice a week) and to receive closer supervision. Because parents found it beneficial to involve the child in the process, (e.g., in selecting reinforcers or building their own social scenarios), the training provided to educators prior to implementation could be enriched with tips to promote the child’s participation. Parents reported that extinction bursts, although temporary, were unsettling. It may therefore be useful to explicitly incorporate an explanation of this common phenomenon in planned meetings with educators and prepare parents for this possibility prior to implementing intervention strategies.
Limitations and Future Research
The setting in which this study took place came with many limitations. Caution should be exercised when generalizing the findings to other contexts, since external validity of the results is potentially compromised due to the highly specific context in which this study took place. As another limitation, children were determined to present CB as reported by the parent and confirmed by educators without the use of a standardized assessment. Since this aticle specifically aims to report parents’ perceptions, the reliance solely on parents’ self-reporting should not be considered a limitation. However, only two-thirds of the parents were interviewed after their participation, which is one limitation of these results.
While most parents shared positive outcomes of the program on their family and personal well-being, there were some who reported no noticeable effects. It is crucial for future research to investigate these findings further, aiming to identify potential adjustments in program implementation and explore possibilities of integrating additional psycho-social support alongside such program. While further research is required to identify the factors and variables contributing to families’ success in managing CB, future implementations of similar programs involving parents should consider the perspectives of these parents. In addition, extending the perspective beyond a 12-week timeframe would allow for the observation of how the perceived effects evolve over time. To provide a more comprehensive perspective, future studies should incorporate input other stakeholders (e.g., educators, managers, partners) to gather their views and expectations on the parents’ role in implementation.
Footnotes
Disposition editor: Cristina Mogro-Wilson
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by an Insight Development Grant, emerging scholar from the Social Sciences and Humanities Research Council (SSHRC) of Canada. Z. Mestari is supported by a bourse de recherche doctorale grant from Fonds pour le recherche du Québec Société et Culture (FRQSC), and M. Rivard is supported by a chercheur-boursier junior 2 grant from the Fonds pour le recherche du Québec en santé (FRQS).