
Abstract
Albeit the height of COVID-19 has ended, clinicians have continued to regularly provide online therapy services. In the spring of 2021 during the third wave of COVID-19, we conducted an online survey study to examine psychosocial experiences among mental health clinicians (N = 196). The survey included two open-ended questions about the use of online therapy as a mode of service delivery. Using a qualitative content analysis of those responses, this article reports the findings on clinicians’ perceptions of online therapy. The following themes identified are: (a) greater access to specialized mental health services, (b) contested notion of therapy as a “safe space,” (c) less immersive clinical interventions, and (d) enhanced opportunity for professional growth. Implications for online-based social work practice are discussed.
Virtual mental health care is neither new nor uncommon. Clinicians have increasingly provided online therapy services over the last few decades (Kanani & Regehr, 2003; Mishna et al., 2014). There are several forms of online therapy, including videoconferences and instant messages, that rely on electronic or internet-based forms of communication to deliver mental health care synchronously (i.e., real-time) or asynchronously (i.e., not real-time) (McGrath et al., 2018; Stoll et al., 2019). The global outbreak of the COVID-19 pandemic prompted significant challenges for social workers and mental health clinicians—particularly with regards to mental health service delivery. At the same time, the risk of contagion rendered it difficult and oftentimes unsafe for clinicians to continue to provide in-person interventions. During the pandemic, many regions and countries required the rapid adoption of social distancing and quarantine protocols which provoked an abrupt transition from in-person formats to online modalities, including online videoconference platforms to deliver mental health care (Mishna et al., 2021; Olwill et al., 2020; Walter-McCabe, 2020). Although only a small portion of mental health practitioners in North America, including psychotherapists and social workers, conducted their clinical work through online modalities prior to COVID-19 (range: 13–29%; Ashcroft et al., 2022; Disney et al., 2021; Pierce et al., 2020), more recent studies have shown that a vast majority of clinicians (range: 74–86%) provided online mental health services during the pandemic (Ashcroft et al., 2022; Lin et al., 2021; Pierce et al., 2020). Once considered an optional or complimentary format, online therapy quickly became central to the delivery of accessible and safe mental health care services (Mishna et al., 2020; Rosen et al., 2020).
Online therapy has proven to be a valuable and effective modality. Online therapy has consistently demonstrated good user satisfaction (Lewis et al., 2019), as well as clinical effectiveness and outcomes comparable to in-person services (Hilty et al., 2013; Hubley et al., 2016). In addition, online therapy is known to be more accessible and can provide greater flexibility for some users (Connolly et al., 2020; Markowitz et al., 2021). Studies have also shown that clinicians are able to effectively develop a strong therapeutic alliance online with clients to the same degree as they would in-person (Pugh et al., 2021; Simpson et al., 2021). Results from a qualitative study of social workers in Canada (n = 11) suggested that mental health clinicians developed creative strategies during COVID-19 to maintain their therapeutic relationships with clients, such as by incorporating art and music during a videoconference session (Mishna et al., 2021). Studies prior to the pandemic have identified various advantages of online therapy for both clients (n = 33) and clinicians (n = 22), including increased accessibility, flexibility and immediacy, and the ability to create more space for reflective processes (Fang et al., 2018). A number of studies (e.g., Békés & Aafjes-van Doorn, 2020; Khatib et al., 2022) identified a positive correlation between clinicians’ prior experience with online therapy and their positive attitudes toward this mode of practice. In other words, clinicians who had previous experiences with online therapy were more likely to hold positive attitudes regarding virtual services and to be more confident in online therapy effectiveness. This suggests that online therapy can be a valuable mode of practice for clinicians who normally provide in-person therapy as long as they get a chance to use it as a mode of practice.
Conversely, literature has also highlighted several challenges to online therapy, including clinicians feeling tired, distracted, less competent or authentic (Békés & Aafjes-van Doorn, 2020; Békés et al., 2021; Weinberg, 2020). During the pandemic, scholars have suggested that clinicians may experience a sense of detachment or impersonality with clients (Connolly et al., 2020; Pascoe, 2021) and may feel unprepared or that they lack adequate training for online therapy (Khatib et al., 2022; Kotera et al., 2021). Compared with traditional in-person therapy, clinicians perceived more difficulty in implementing common therapeutic skills (e.g., empathy, warmth, reflection, active listening) in online modalities (Lin et al., 2021; Messina & Loffler-Staska, 2021). Clinicians also expressed more concerns with professional boundaries, confidentiality, and their ability to genuinely connect with clients over virtual modalities (Békés et al., 2021; Chiauzzi et al., 2020; Disney et al., 2021; Kotera et al., 2021; Mishna et al., 2021; Pascoe, 2021). In addition, several studies have documented various drawbacks to online therapy including technological challenges, barriers to assessing body language and nonverbal cues, and legal concerns related to safety, confidentiality, risk, and liability (Baird & Tarshis, 2022; Connolly et al., 2020; Disney et al., 2021; Fang et al., 2018; Kotera et al., 2021).
Method
The Current Study
The current study draws from one part of a larger online survey study on mental health clinicians’ experience during the COVID-19 pandemic. We report participants’ qualitative responses to two open-ended questions that asked about their experiences with online therapy. To put clinicians’ context-specific knowledge of and experience with online therapy at the forefront of this research, pragmatism was the epistemological paradigm that guided our study. By appraising knowledge based on principles of utility and practical application, including what is helpful and for whom in specific contexts (Borden, 2013; Kaushik & Walsh, 2019; Morgan, 2014), pragmatism is a well-suited approach for research on social work practice because it highlights clinicians’ experiences to strengthen virtual service provision and better supports clinicians who work in such realms. Informed by this pragmatic approach, we asked the following research question for this study: What are clinicians’ perceived benefits and limitations of online therapy?
Participants
Participant eligibility included licensed or registered mental health professionals located in Canada or the United States with a minimum of a Master’s degree in social work, counseling, psychology, or related fields. In total, 196 mental health clinicians completed the survey in whole. Participant characteristics can be seen in Table 1. Participants were distributed between Canada and the United States, with most participants residing in Canada (80.1%) followed by the United States (19.9%) respectively. The majority of participants were cisgender women (84.2%) and identified as white (72.5%). Participant’s age ranged from 24 to 71 years old, with a mean age of 39. Most participants held a Master of Social Work degree (70.4%) at the time of survey completion, while others held another type of Master’s degree (e.g., counseling degree, 15.3%), a doctorate degree (9.7%), or a Doctor of Medicine degree (MD, 4.6%). When asked about their scope of practice, most participants identified working in counseling (43.9%) or health care (29.1%), with remaining participants working in higher education (5.6%), schools (5.1%), children’s mental health (3.1%), or other (13.2%). Prior to the COVID-19 pandemic, participants primarily provided in-person services (94.4%), whereas only 19.4% of participants provided services in-person at the time of survey completion during the third wave of COVID-19. Participants who completed the survey were compensated with US$27.00 for their time in the form of an electronic gift card.
Sample Demographics (N = 196).
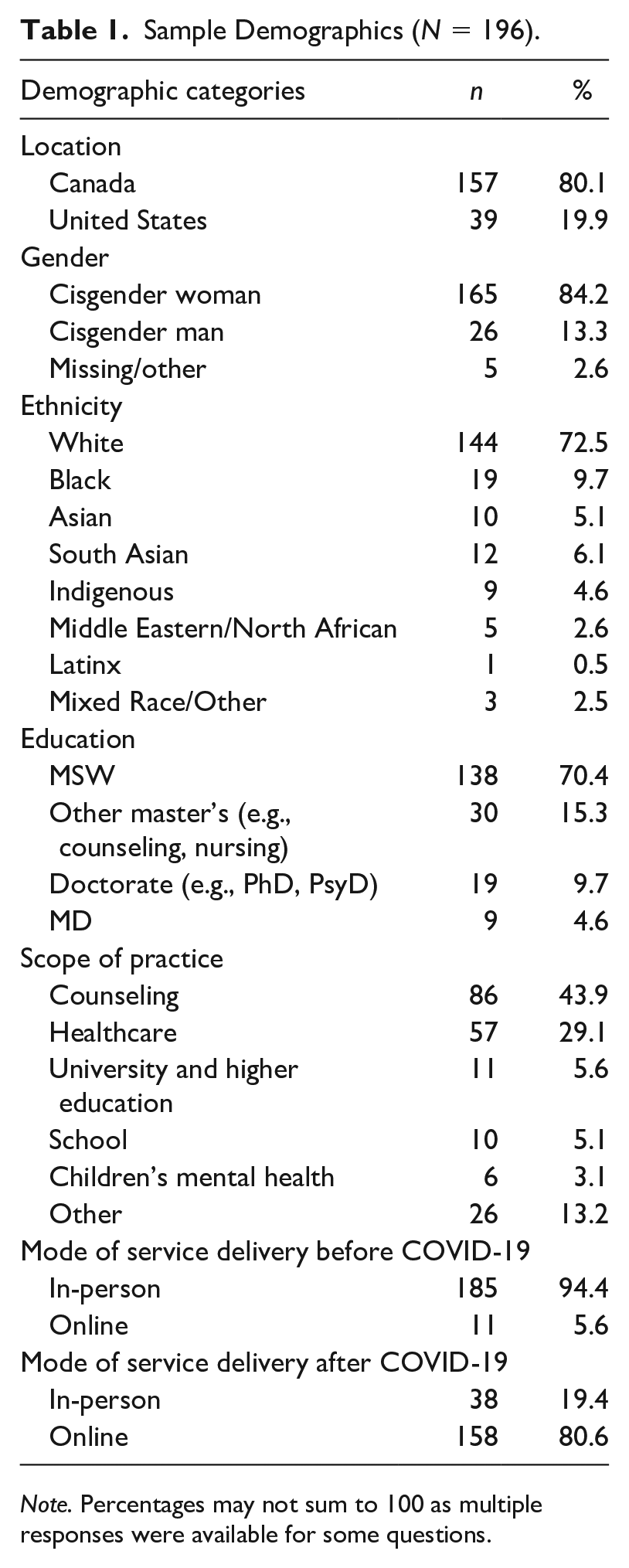
Note. Percentages may not sum to 100 as multiple responses were available for some questions.
Data Collection
From March to April 2021, we conducted an online survey study during the third wave of the COVID-19 pandemic. The survey was distributed to social workers and other mental health practitioners in Canada and the United States using Qualtrics. Professional listservs and social media groups were used to recruit social workers and other mental health practitioners. The purpose of this larger study was to explore mental hea-lth clinicians’ experiences assessing client stress online as well as to explore the psychosocial impacts of the pandemic on the clinicians’ own well-being. Derived from this larger study, this article reports the results from the following two open-ended questions about the participants’ perceptions of online therapy: “Please briefly describe your previous experience of assessing or working with clients through online therapy platforms (e.g., Zoom)” and “What limitations and/or benefits have you experienced in using an online platform in your own practice?” The first question invited participants to describe their experiences in providing online therapy, whereas the second specifically asked participants to reflect on the benefits and limitations of online service provision. Participants were invited to respond to these questions by inputting their response into a text-entry box directly in the Qualtrics survey. More detailed descriptions of the larger study can be found elsewhere (Asakura et al., 2023). Response data from the open-ended questions were exported from Qualtrics onto Excel for data downloading. The first author cleaned the data by removing all other non-relevant data (i.e., responses from the other questions in the survey) and by formatting the responses from the above open-ended questions into a readable table format. All research materials were reviewed and approved by the university’s Research Ethics Board.
Data Analysis
Qualitative content analysis was used as a systematic, flexible, and pragmatic approach to generate meaning and elucidate a particular phenomenon from existing qualitative data (Bengtsson, 2016; Elo & Kyngas, 2008). It also permits for inductive and deductive analyses individually and as a collaborative team (Cho & Lee, 2014). Both approaches were employed repeatedly and reciprocally to analyze, explore, refine, and test emergent themes. The first and second authors, who were social work research assistants for this study, collaboratively coded the responses from the open-ended questions using MS Word. Following initial coding, both researchers then met regularly to review preliminary codes. Any disagreements were collectively discussed and reconciled at team meetings. We used consensus to determine the initial codes and grouped them into themes. Through our team meetings, participant responses from the open-ended questions were compared to identify patterns and differences, refined, and merged into categories that served the basis for our themes. For instance, preliminary codes referring to therapeutic modalities that were more difficult to engage online (e.g., “containment,” “trauma work,” “crisis interventions,” “grounding”) were collated into what became one of our core themes: that clinicians found some clinical interventions as less immersive. Using consensus, all initial codes were re-examined, re-organized, and re-defined in our team meetings to create our final set of themes that reflect clinician perceptions of online therapy.
All authors embodied different racial, gender, and other social identities and professional experiences. Some of us were practicing clinicians and had experienced this shift from in-person to online therapy during the COVID-19 outbreak, whereas others were full-time rese-archers committed to the advancement of clinical practice. What brought us together was our shared concern about the impact of the COVID-19 pandemic on professional practice and our desire to highlight the voices of clinicians providing online therapy. To ensure trustworthiness of the study, we engaged a consensus-based and reflexive team approach to analysis. We maintained individual memos throughout the analysis process. We consulted with each other and shared our respective observations, reflections, and preliminary codes. We maintained a team consensus on results and collected exemplary quotes from participants to illustrate each theme when writing the results. Not only did these collaborative discussions allow us to harness our multiple perspectives and positionalities to form a shared understanding of the core themes, but they also served as a tool for reflexive practice in data analysis (Deggs & Hernandez, 2018). Finally, we maintained a detailed audit trail of research activities, including the consultation meeting minutes on our decision-making on the coding and analytic processes.
Findings
The following themes were identified about the use of online therapy: (a) greater access to specialized mental health services; (b) contested notion of therapy as a “safe space”; (c) less immersive clinical interventions; and (d) enhanced opportunity for professional growth.
Greater Access to Specialized Services
Participants shared that online therapy allowed for the provision of more flexible services—not just for the clinicians themselves who found remote working more accessible but also for client communities that may have been otherwise harder to reach (particularly for clients with long commutes, caregiving responsibilities, social anxiety, compromised immune systems and fears of contagion). Here, participants described their own experiences with more accessible provision of specialized services as well as their perceptions of client access. For instance, participants described online therapy providing “accessibility and flexibility, for both me and my clients” (Participant 27). Participants reflected on their own increased accessibility of this mode of virtual service delivery, including “not having to commute” (Participant 20), “working from home . . . which is much easier than trying to get to an office” (Participant 27), and not having to “pay office rent or parking fees” (Participant 135). Participants also described how online therapy afforded them a greater capacity to “reach people I may not be able to see otherwise” (Participant 15), including client populations “without transportation or a flexible work schedule” (Participant 22) and client populations with “school/work barriers” (Participant 43) who may have otherwise been unable to access in-person therapy.
Participants reported that online therapy not only increased general convenience and flexibility of therapy but it also enhanced access to more specialized, identity-specific mental health services among clients of color and other minoritized clients. As one participant shared, “clients [are] being able to have more accessibility in accessing sessions, particularly for marginalized clients who may be living in an area where there is a lack of therapists who would be able to meet their needs” (Participant 3). In discussing the accessibility of online therapy, one participant described that “clients have increased access to psychotherapists because they are not bound by location; this has been especially beneficial in working with clients in remote areas and those seeking psychotherapy in languages other than English” (Participant 76). These participants highlighted how the shift to online therapy allowed them to access a harder-to-reach and oftentimes disenfranchised clients: “I’m now able to see clients anywhere in the state, which gives me a broader client pool to draw from and improves access to treatment for clients who live in more rural areas” (Participant 27). Some suggested that online therapy provided clients with enhanced access to services from clinicians across geographic regions who specialized in working with marginalized communities, such as queer and trans communities and Black, Indigenous, and people of color (BIPOC) communities. For example, one participant noted that “clients who are geographically isolated have been able to access therapy that is trans-affirming, BIPOC-affirming and this was harder to do before with the options near them” (Participant 7). Participants reported that this specialized access was not as readily accessible prior to the COVID-19 pandemic. Notably, this study was conducted during a rapidly growing public awareness of social and racial unrest across North America, including the Black Lives Matter movement, anti-Asian racism, and other racial disparities during the pandemic. As seen in this participant’s reflection, racist police violence encountered by members of the Black community has a dramatic negative impact on mental and physical health. That stress takes a toll . . . The availability of Black psychotherapists in even a major North American city like Toronto is so limited. As a white clinician, I see it as a priority to find Black therapists for Black clients. (Participant 4)
It is plausible that a need for specialized services brought by these sociopolitical climates was, at least partially, met because of the availability of online therapy and clinicians’ abilities to either offer these specialized services or to leverage their online networks and refer clients to specialized services.
Contested Notion of Therapy as a “Safe Space”
In our study, the notion of physical and emotional safety was challenged in several ways. Primarily, participants suggested that the idea of therapy as a “safe space” is contested when services are provided online. In working with some clients, the shift from in-person to online negated the traditional understanding of therapy as a safe space—particularly when the client’s home environment was deemed to be unsafe. Several participants echoed this sentiment and many identified the loss of safety in online therapy: “video therapy has removed the ‘safe space’ aspect of counseling for a lot of people” (Participant 104) and “not knowing who is around makes me question if the client is safe and can freely disclose” (Participant 113). This was particularly the case for participants working with clients who might face family violence or intimate partner violence (IPV): Some clients are more comfortable in their home setting, so they are more likely to engage in vulnerable conversations. However, this can also be a barrier depending on the client’s home situation. I deal with many women escaping violence so if they can have one less stressor coming to the appointment, then that is a great thing. It gets complicated if someone is unstable in a session or if it comes to my attention that they are unsafe. (Participant 79)
In contrast, online therapy allowed other clients to feel safer and more comfortable in their home environments. Here, participants reflected that the transition to online modalities alters the notion of “safe space” in therapy and is contextually defined by the participants’ respective situations and environments. For instance, one participant noted that “this format was helpful in that it allows clients to be comfortable in their own home while speaking with me” (Participant 35). Another participant described the role of personal items and pets within clients’ living space in encouraging feelings of comfort within the session: “one benefit [of online therapy] is that some clients have expressed feeling more comfortable due to being surrounded by their pet or having other personal items around them that brings them comfort” (Participant 106). Interestingly, participants also noticed that this sense of safety within their home surroundings encouraged clients to be more forthcoming, which was evidenced by a quicker pace of disclosing personal information or delving into vulnerable topics: “Clients are sometimes more comfortable in their home environment and therefore more forthcoming [because] clients have access to other tools for self-soothing in their home” (Participant 136). Notably, some participants suggested a potential link between clients’ sense of physical safety (e.g., of being in their own home) and clients’ sense of psychological safety in the virtual therapeutic space: “clients are more comfortable in their home setting, so they are more likely to engage in vulnerable conversations” (Participant 37).
Finally, participants also suggested that online therapy provided a heightened sense of physical protection or safety during the pandemic because it abided by social distancing, quarantining, and isolating protocols. Whereas the above participants described a dynamic notion of physical and psychological safety in online therapy that is contextually defined, other participants reflected on a pandemic-specific sense of safety that was free from COVID-19 contagion. Here, participants described that they can provide online therapy services “without the fear of contracting COVID-19” (Participant 39). Participants felt more comfortable “knowing [they were] protecting [themselves] from COVID-19” (Participant 80) by ensuring that there were “no chances of contacting or spreading COVID-19” (Participant 130). For these participants, safety meant that online therapy lessened their risk of direct exposure to the virus.
Less Immersive Clinical Interventions
Participants shared difficulties employing certain interventions and therapeutic exercises online. These participants found online therapy as “less immersive than in-person work” (Participant 5). Examples shared by participants included using grounding and co-regulation exercises, facilitating containment work, conducting accurate client assessments, and engaging in trauma processing. Participants described “the difficulties with creating a sense of containment . . . when we are communicating [with clients] through a screen” (Participant 27) or that online therapy “does not give [clients] the same ‘container’ for experiencing emotions safely” (Participant 26). One participant shared: A limitation is not being able to assess the energy in the room. It has been difficult to do trauma assessments and grounding virtually. There is a disconnection over virtual therapy. Internet connection can distort the information flow and the nuances of tempo and cadence are often lost. In particular with trauma work, eye to eye connection is so important to ground the client, and with the camera to screen disconnection that grounding technique is lost. (Participant 37)
Other participants agreed with these sentiments. Participants noted that the screen between themselves and clients “makes the call feel ‘less personal’” (Participant 112), “feels disconnected” (Participant 1), and “has more limited ability to focus on a person’s story or their experience because there is a screen between us” (Participant 2). Another participant explained how being unable to fully see and feel the relational and embodied component prompted a sense of depthlessness in the online space: There are certain three-dimensional things that are missing when we do things by Zoom and that becomes problematic because there’s something about negotiating space in the counseling room and looking at body movements that are not constrained by a screen that are important. (Participant 116)
For this participant, the lack of in-person presence with clients rendered clinical interventions as less immersive as a result.
Conducting suicide risk assessments and suicidal ideation interventions with clients in crisis was particularly difficult for clinicians in an online context. As some participants explained, it is “difficult to conduct suicidal risk assessments online” (Participant 98) and “assessing risk and ensuring safety are harder when clients are remote” (Participant 125). In a similar vein, “working with people in [imminent crisis] via video may not be the most effective/safe tool for assessment of high-risk populations (i.e., suicide risk)” (Participant 149). These participants identified that supporting clients in crisis was more challenging due to the less immersive nature of online therapy.
Furthermore, technological limitations, in-cluding internet interruptions (e.g., dropped calls, delays between audio and image, pixelation of screen) and not being able to fully see the client’s entire body, seem to further contribute to this sense of depthlessness. As some participants explained, “technical glitches are frustrating and make it harder to build a therapeutic rapport” (Participant 148) and “it is increasingly difficult to read non-verbal cues that I would typically consider in assessment (i.e., body movements when we can only see their face and shoulders), or can’t see them at all as they’ve turned their camera off” (Participant 139). One participant noted that “without body language and other signals, it can be hard to pick up on important subtleties” (Participant 27) that may be required for crisis assessment and intervention. Other participants agreed: You don’t see the whole person, just from mid-chest or neck up. You don’t have the ability to observe “body language” in its entirety or see the “body speak,” which can signal emotional or psychological activation or triggering, or emotionally charged material. This may cause some mis-attunement with one’s client. (Participant 111)
Technological barriers, in combination with a lessened ability to see the client’s full body, appeared to disrupt the participants’ ability to connect with clients at the affective and somatic level that is typically required for the above interventions.
Enhanced Opportunity for Professional Growth
Finally, participants reported that the use of online therapy provided them with an essential opportunity for professional learning and growth. Many clinicians were new to online therapy with little prior experience with the modality. Although only 5.6% of participants had provided online therapy services prior to the COVID-19 pandemic, the majority of participants in this survey (80.6%) had experienced a shift in their mode of service delivery from in-person to online modalities after the COVID-19 pandemic. The shift to online therapy urged participants to pursue additional professional development opportunities to deepen and refine their online therapy expertise and to sharpen their clinical skills to compensate for the distance and challenges associated with virtual practice. Participants reflected on their “own learning curve in this [online] modality” (Participant 11) and saw the need to pursue additional trainings. As such, participants described having to
work a little bit harder at pulling out some of the themes from what the client is saying. I think that during Zoom assessments, I would be asking more direct questions to better diagnose or assess the symptoms of the realms of trauma. (Participant 116)
Another participant stated, There are limitations with reading body language or detecting micro-facial expressions, such as whether someone is starting to tear up very subtly. It’s easier to miss this on Zoom, especially if the connection isn’t good and the screen is blurry. It’s easier for clients to breeze past sadness and keep talking (avoidance), partly because it’s harder for me to pick up on those opportunities to deepen emotions, invite vulnerability, or facilitate emotional expression. I think of it more like a learning curve for me in adapting to telehealth. I’ve learned to slow clients down, actively check in on emotions and body sensations, name that it seems like there are tears coming—whereas in person it’s just “felt” in the room. (Participant 88)
Participants noted that online therapy signaled a need for additional trainings and further professional education on online service provision. Some participants reported taking additional trainings “to improve my skills with how to access the somatic symptoms and connections on a virtual format” (Participant 13) or “make online sessions more fun and enjoyable for clients” (Participant 98). As a result, many participants reported that they needed to improve their active listening skills, learn to be more attentive and attuned to clients’ micro-facial expressions and behaviors, cultivate more empathy and perspective-taking for clients, and carry out more creative therapeutic approaches when working online.
Discussion
In this qualitative study, we explored clinicians’ experiences with providing online therapy during the COVID-19 pandemic. Consistent with other studies (e.g., Markowitz et al., 2021; Mishna et al., 2021; Pierce et al., 2020), most clinicians in this research were new to virtual modalities and had little or no experience with online therapy prior to the COVID-19 pandemic. As seen in previous research (e.g., Fang et al., 2018; Rosen et al., 2020; Simpson et al., 2021), clinicians in our study also found that online therapy facilitated easier access to clients who may be harder to reach due to the pandemic or other factors. Our study highlights the significance of increased client access to clinicians with shared identities as them. Expanding cross-cultural networks and service access outside of geographic regions is imperative for vulnerable, marginalized, and hard-to-reach groups (Disney et al., 2021). Clinicians emphasized the need to leverage online networks to better meet client needs and prioritize cross-cultural work. This finding corroborates the body of literature that advocates for client choice in locating clinicians outside of organizations they typically frequent to access culturally- and racially-sensitive services (Connolly et al., 2020; Disney et al., 2021; McGrath et al., 2018).
Although there were many noted benefits of online therapy in our findings, clinicians also raised several concerns on the use of online therapy. As found in previous literature (Békés et al., 2021; Kotera et al., 2021; Markowitz et al., 2021), there are significant issues related to the safety, confidentiality, and privacy of clients when utilizing virtual modalities. Clinicians noted the risks of online therapy with clients in crisis, especially when assessing suicidal thoughts or ideation. Similar findings have been reported in other studies (e.g., Downing et al., 2021; Markowitz et al., 2021; Pugh et al., 2021), including that body language and other important non-verbal cues may be hidden on camera and crucial signs of distress might be missed by clinicians. Technological interruptions such as dropped calls or delays between audio and image may also affect crisis assessment, which can render clinicians unable to respond to risk in a timely or accurate manner. However, clinicians noted that it may be easier for some clients to discuss difficult content such as trauma or suicidality online and in the comfort of their home rather than in an in-person office setting. When understood together, these results suggest that there are possibilities for crisis and trauma work online, but that client safety and privacy must be prioritized (Baird & Tarshis, 2022). It is important to note that online therapy may not be a good fit for all individuals or groups, diagnoses, and cultures (Disney et al., 2021). A trauma-informed approach that takes into consideration the experiences of trauma and distress is one way for clinicians to approach online therapy and warrants further exploration to better understand the needs of certain populations and marginalized groups (Rosen et al., 2020).
To add, some clinical interventions may be harder to conduct virtually. According to our results, interventions such as grounding exercises and mindfulness activities are less immersive and harder to administer through online therapy. This suggests that clinicians may need more adjustments to their practice and specialized training in online modalities to gain the necessary skills to engage these clinical interventions. Our findings suggest that it is imperative for clinicians to undergo additional training to strengthen their existing clinical skills and develop additional skills for an online therapeutic context. As other scholars have emphasized, clinicians must continue developing their verbal and non-verbal skills and adjust their approaches to effectively conduct more immersive and engaged online interventions (Békés et al., 2021; Lin et al., 2021; Markowitz et al., 2021; Pugh et al., 2021).
Limitations
A limitation of this study is the possible sampling bias of the study and that participants were predominantly comprised of white clinicians. Seeing as these results cannot be generalized and the data are limited to the participant sample (i.e., with most study participants being situated in Canada), readers should be cautious regarding to what extent results can be transferred to their respective contexts and countries of practice. In addition, participants in this study reported both their own experiences with online therapy as well as their impressions of client experiences (i.e., how they thought clients experienced online therapy). Readers should be cognizant of this reporting style as there was no way for the authors to confirm or validate the experiences of clients in this study. Finally, while our study focused on experiences of online therapy exclusively, more recent research shows that clinicians now prefer hybrid modalities (Pink et al., 2022). This highlights the changing nature of the pandemic and the temporal context of our study which must be taken into consideration. Had we conducted this study at a different point in the COVID-19 pandemic, we hypothesize that the data may have likely been affected and different preferences may have been captured.
Implications for Practice
This study provides practice implications and research directions to further explore online therapy and its utility. Although the benefits of online therapy appear to outweigh the risks, additional research is needed to explore online therapy practices for different populations and needs. Given some of the limitations of online therapy such as privacy and safety issues, technological disruptions, and difficulties in showing non-verbal cues, there are several practice recommendations to consider. In terms of safety, clinicians should have an upfront discussion with clients about privacy. For instance, clinicians may consider asking clients if it is safe to engage in therapy at home or whether there is an alternate setting that is more private (e.g., car, library, or vacant park; Kotera et al., 2021; Weinberg, 2020). Considerations of safety and using a trauma-informed approach is essential, especially if there are risks of violence or abuse at home that may require further safety assessment (Baird & Tarshis, 2022).
Scholars have also suggested having both a preliminary and ongoing conversation with clients to ensure that any potential technical issues, such as faulty internet connectivity and dropped calls, are addressed (Pugh et al., 2021; Weinberg, 2020). Clinicians may wish to implement a checklist with clients to ensure that online technology is understood, inquire whether their internet connection is stable, suggest the use of headphones, select a room that is private and well-lit, and troubleshoot what to do if the internet connection drops (see Connolly et al., 2020; Downing et al., 2021; Pugh et al., 2021; Weinberg, 2020).
Clinicians can also work to establish an effective therapeutic or holding environment online (Békés et al., 2021; Lin et al., 2021; Pugh et al., 2021). For example, in-person therapy offices are often staged in such a way that is both comfortable for the client and conducive for therapy. A tissue box is generally placed within reach, seating arrangements are inviting, and the room is favorable for vulnerable conversations. In an online context, clinicians can instruct clients to prepare their environment accordingly (e.g., go to a quiet and private room, select a comfortable chair) to minimize interruptions and create an environment that might feel similar to an in-person therapy office (Weinberg, 2020). Clinicians can also ask clients to move back or adjust their cameras to see them in full view (Weinberg, 2020). In addition, clinicians can refine and build on their existing clinical skills. To show more depth, for instance, clinicians can show exaggerated body language such as hand gestures or move closer to the computer screen to show more physical and emotional intimacy (Pugh et al., 2021). The use of more verbal prompts, such as summarizing, reflecting, and rephrasing, can also help orient the client to the session. Finally, since subtle cues can get lost online, clinicians may want to ask more clarifying questions to make certain that the content was understood (Pugh et al., 2021).
Clients should also be able to easily access clinicians with shared identities and expertise. As we saw in our study, clinicians harnessed their professional networks to connect clients with identity-specific (e.g., queer, trans, BIPOC) resources during the pandemic. As demand increases for culturally- and racially-specific services, especially in regions with scarcer resources, clients are opting to engage with clinicians in other states and provinces. This suggests an important policy implication as some registered clinicians can apply to practice in new jurisdictions by way of endorsement or reciprocity in a new state or province to meet this demand (National Association of Social Workers [NASW], n.d.). This requires a current knowledge of policy stakeholders and regulatory or legal issues to further expand jurisdictions of practice (Markowitz et al., 2021; Rosen et al., 2020).
Finally, our findings prompt the consideration of several ethical implications for online therapy. First and foremost, “practitioners must assess their own competence in the use of technology to deliver social work services” (Reamer, 2022, p. 153). As our findings highlight that clinicians may not feel adequately prepared to use virtual modalities, organizations should integrate available skills training and information on technology-related ethical standards to ensure that clinicians have access to continuous learning opportunities. More integration of technological skills training for online therapy within social work education is paramount in preparing future clinicians for this evolving work mode (Hames et al., 2020; MacMullin et al., 2020). In a similar vein, clinicians should take reasonable steps to ensure that they have access to protocols to adequately assess client safety and privacy concerns in online therapy, particularly for clients facing crisis or emergency situations such as IPV or suicide risk (Reamer, 2018). Finally, clinicians who offer online therapy need to mobilize their resources and networks to bolster increased access to services that better meet the needs of clients and their unique identities and experiences.
Conclusion
This research draws on an online survey with social workers and other mental health clinicians (N = 196) on their experiences with online therapy. Although online therapy can provide wider access to specialized mental health services and create opportunities for clinicians to expand their practice, results suggest that certain therapeutic interventions may be less immersive and difficult to implement online with safety risks to consider. Clinicians will likely continue using a hybrid model of in-person and online care well beyond the COVID-19 pandemic. As clinicians continue to provide online therapy, these findings can be used as an opportunity to strengthen virtual service provision and navigate professional realms and realities of such practice. Continued research and training are required to address these challenges and better support the needs of individuals and communities, and especially populations at risk.
Footnotes
Disposition editor: Cristina Mogro-Wilson
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded to Drs. Kenta Asakura and Amedeo D’Angiulli by the Carleton University COVID-19 Rapid Response Research Grant, the School of Social Work Evelyn Maud McCorkle Research Fund, and the Faculty of Public Affairs Research Productivity Bursary.