
Abstract
The purpose of the study is to compare self-reported health and access to health care among people with early- and late-onset disability. Adults with disabilities 18 to 62 years of age participated in the 2018 U.S. National Survey on Health and Disability (NSHD), which is a nationally representative, internet-based survey that provides data related to health insurance and access to health care. A subsample of participants who reported age at disability onset (n = 1,188) completed measures related to demographics, health status, health insurance, and access to health care services. Results show that people with early-onset disability were significantly more likely to receive Supplemental Security Income (SSI; p < .001), less likely to receive Social Security Disability Insurance (SSDI; p < .001), more likely to have Medicaid (p < .001), and less likely to have Medicare (p < .01). People with late-onset disability were more likely to report service limitations and were more likely to report fair/poor health (p < .001). Overall, study findings suggest that people with late-onset disability report higher out-of-pocket health care expenditures, greater access limitations, and poorer health. Medical professionals and disability service providers should be mindful about assisting this population in locating appropriate health insurance coverage, health services, and financial assistance.
Many differences may exist between people who acquire a disability early in their lifetime (i.e., prior to age 22) and people who acquire a disability later in their lifetime. Although people with early-onset disability must learn to adjust to adulthood as a person with a disability, people with late-onset disability must adjust to life as a person with a disability as an adult. Some previous research suggests differences in self-reported health across people with various ages of disability onset. Results from these studies show that people with early-onset disability consistently report better health status than people with late-onset disability (Coyle & Putnam, 2017; Jamoom et al., 2008; Verbrugge & Yang, 2002). These authors describe several hypotheses for these health disparities including adaptation to disability (Jamoom et al., 2008; Verbrugge & Yang, 2002), disability identity (Jamoom et al., 2008; Verbrugge & Yang, 2002), onset-specific diagnoses (Coyle & Putnam, 2017; Verbrugge & Yang, 2002), and social support (Jamoom et al., 2008). Although these represent sound hypotheses, no known study has examined differences in health insurance and access to health care services among people with early- and late-onset disability. Thus, examining differences in these variables may help to further explain observed differences in self-reported health.
Eligibility for employer-sponsored health insurance may be influenced by differences in employment rates between early- and late-onset groups. For example, some research suggests that people with early-onset disability are more likely to be employed than people with late-onset disability (Loprest & Maag, 2003). These authors suggest that employment rates may be higher among people with early-onset disability because these individuals are more likely to have chosen career paths that closely align with their accommodation needs, whereas people with late-onset disability may be less likely to know what accommodations are available to them, to receive accommodations upon returning to work, or to transition to an alternate career path (Loprest & Maag, 2003). Differences in marriage rates also have the potential to impact receipt of employer-sponsored insurance. For example, some research indicates that people with early-onset disability are significantly less likely to have been married at any point in their lifetimes (Jamoom et al., 2008). Thus, people with early-onset disability may be less likely to qualify for insurance under a spouse’s health insurance plan.
Differences in income between people with early- and late-onset disability may also significantly impact access to health care. Some research suggests that people with early-onset disability are more likely to earn lower wages than people with late-onset disability (Hollenbeck & Kimmel, 2008; Loprest & Maag, 2003). Authors of these studies suggest that people with late-onset disability are more likely to have higher earnings and access to alternative sources of income such as retirement savings, private disability insurance, or work-based disability compensation (Loprest & Maag, 2003). Differences may also exist between people with early- and late-onset disability with respect to eligibility for Supplemental Security Income (SSI) or Social Security Disability Insurance (SSDI). Other researchers postulated that people with early-onset disability are more likely to receive SSI benefits (Loprest & Maag, 2003), whereas people with late-onset disability are more likely to receive SSDI benefits due to a longer duration of employment and higher earnings (Favreault & Schwabish, 2016). However, a person who acquired a disability before the age of 22 may be eligible for benefits paid from a parent’s Social Security earnings record if the parent is retired, disabled, or deceased (U.S. Social Security Administration, 2019).
Eligibility for SSI and SSDI is associated with eligibility for Medicaid and Medicare (U.S. Department of Health and Human Services, 2019a, 2019b). Thus, people with early-onset disability may be more likely to receive Medicaid, whereas people with late-onset disability may be more likely to receive Medicare. Differences in health care services covered by Medicare and Medicaid may help to further explain differences in self-reported health between people with early- and late-onset disability. For example, although coverage varies by state, Medicaid enrollees are more likely to receive additional health benefits (e.g., dental, vision, and personal assistance services) that Medicare recipients do not typically receive (U.S. Department of Health and Human Services, 2020).
Given these reported differences in employment, income, public assistance, and public insurance supports, the purpose of this study is to compare self-reported health and access to health care among people with early- and late-onset disability. Early-onset disability was defined as occurring prior to age 22, and late-onset disability was defined as occurring at age 22 or after, which represents a cut-point based on federal laws designating eligibility for certain benefits as disability beginning before age 22 (U.S. Social Security Administration, 2021). Specific research questions were formulated to examine differences between people with early- and late-onset disability, utilizing a two-tailed t-test to assess differences in reported (a) health status, (b) education, (c) employment, (d) income level, (e) received benefits, (f) type of health insurance coverage, (g) out-of-pocket expenditures, and (h) receipt of needed health care services. Assumptions for normality and homogeneity of variances were met. This study represents the first known effort to assess differences in health insurance coverage and access to health care services among people with early- and late-onset disability. Thus, study results may help to further understanding of differences in self-reported health among these two groups as described by previous researchers (Coyle & Putnam, 2017; Jamoom et al., 2008; Verbrugge & Yang, 2002).
Method
The National Survey on Health and Disability (NSHD) is a nationally representative, internet-based survey of adults with disabilities 18 to 62 years of age that provides data related to health insurance and access to health care (Hall & Kurth, 2019). The 2018 NSHD used a purposive convenience sampling approach and was fielded from February to June of 2018. Recruitment was conducted in cooperation with more than 60 national disability organizations who distributed the survey information and link via their networks, social media, and newsletters. This recruitment method yielded complete responses from 1,246 adults with disabilities. The NSHD classifies a disability broadly and includes a screening question that asks respondents if they have “any physical or mental condition, impairment, or disability that affects daily activities or requires the use of special equipment/devices, such as a wheelchair, walker, TDD, or communication device.” The recruitment method and convenience sampling utilized did not provide a representative national sample of adults with disabilities; therefore, data were subsequently weighted to be representative of adults ages 18 to 62 with one or more disabilities using the 2016 American Community Survey (ACS). We compared unweighted tabulations of sociodemographic characteristics from the sample of 1,246 respondents in the NSHD to weighted estimates from the 138,227 adults ages 18 to 62 with at least one disability and internet access at home in the 2016 ACS. We then used the ipfweight program in STATA (v14) to perform iterative proportional fitting, creating survey weights based on estimated population margins for gender, race/ethnicity, region, and educational attainment from the 2016 ACS.
Information related to self-reported health status was gathered using a 5-point scale (1 = poor to 5 = excellent), and a continuous response measure for the number of days (0–30 days) that the participant reported poor physical health, poor mental health, or that poor physical or mental health prevented usual activities. Information related to access to health care services was gathered using a dichotomous (y/n) response measure to the questions
(1) “Thinking about all of your health care experiences over the past 12 months, was there any time when you needed any of the following [individual response for each of the following service types: prescription medications, general doctor visits, specialist visits, medical tests, dental care, mental health care, durable medical equipment], but didn’t get it because you couldn’t afford it?”; (2) “During a typical week do you get all the help you need in your home with personal care/daily activities?; and (3) “In the past 12 months, has the provider network for your health insurance plans(s) been adequate enough to meet all your health care needs?”
Data were analyzed using IBM SPSS Statistics 25. Mean demographic and health status variables were calculated using descriptive statistics. Frequency variables were calculated as dichotomous variables (e.g., health status was separated into ratings of “fair/poor” and “excellent/very good/good”) by determining the frequency of selection by early- or late-onset respondents and dividing by the total number of responses. Finally, comparisons between people with early- and late-onset disability were made using independent samples t-tests. Informed consent was obtained from all survey respondents with documents and procedures approved by the University of Kansas Institutional Review Board (IRB, Study#00004253).
Results
A total of 1,188 respondents answered the question, “What age were you when your main disability or health condition began for you?” Thus, comparative analyses of early- versus late-onset included responses from participants who reported disability onset as occurring prior to age 22 (n = 732) and participants who reported disability onset as occurring at age 22 or after (n = 456). Table 1 provides results of a comparative analysis of demographic variables, health status, health insurance, and access to health care services among people with early- and late-onset disability.
Comparative Analysis of the Demographics of Respondents With Early- and Late-Onset Disability.
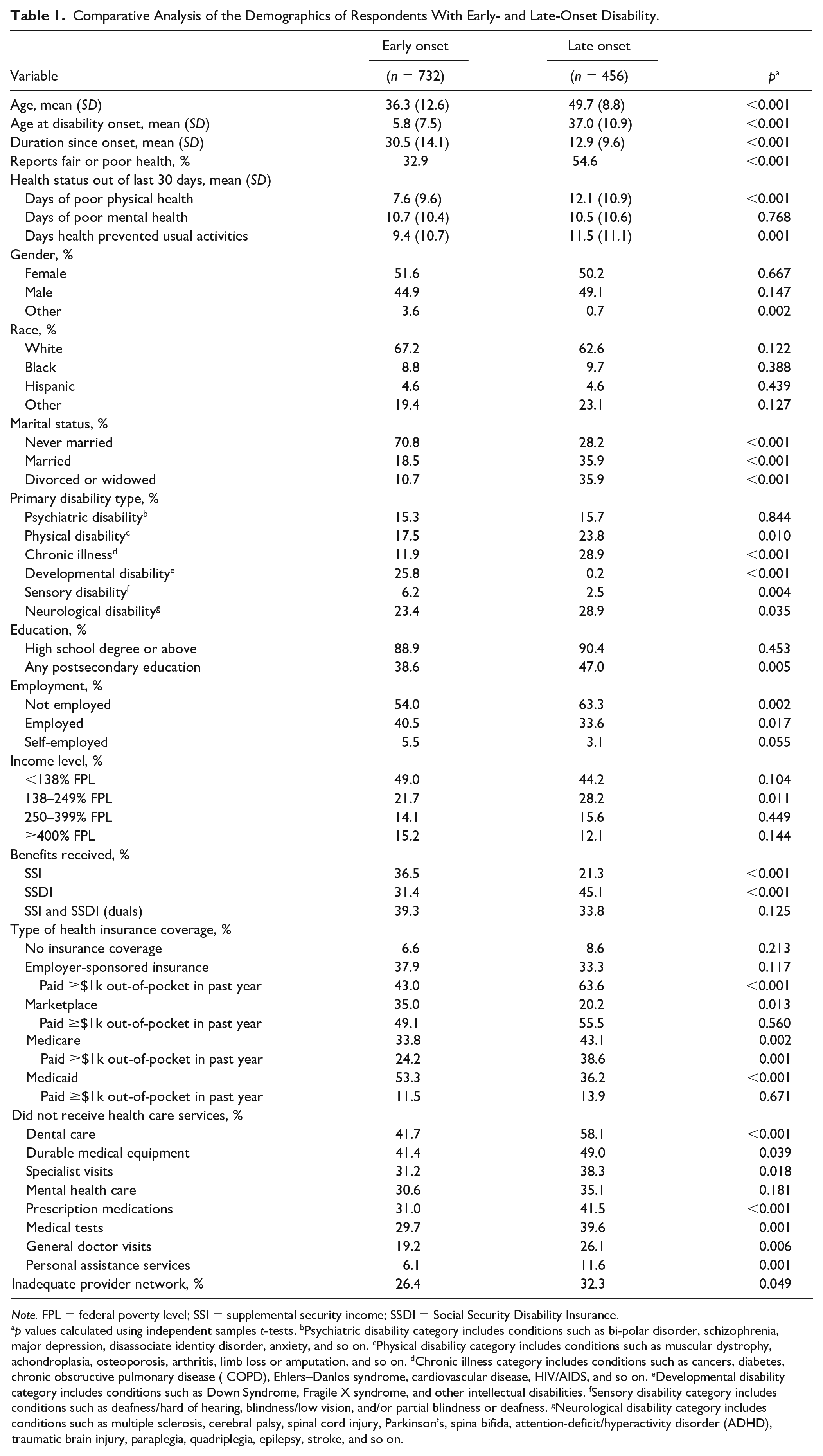
Note. FPL = federal poverty level; SSI = Supplemental Security Income; SSDI = Social Security Disability Insurance.
p values calculated using independent samples t tests. bPsychiatric disability category includes conditions such as bi-polar disorder, schizophrenia, major depression, disassociate identity disorder, anxiety, and so on. cPhysical disability category includes conditions such as muscular dystrophy, achondroplasia, osteoporosis, arthritis, limb loss or amputation, and so on. dChronic illness category includes conditions such as cancers, diabetes, chronic obstructive pulmonary disease ( COPD), Ehlers–Danlos syndrome, cardiovascular disease, HIV/AIDS, and so on. eDevelopmental disability category includes conditions such as Down Syndrome, Fragile X syndrome, and other intellectual disabilities. fSensory disability category includes conditions such as deafness/hard of hearing, blindness/low vision, and/or partial blindness or deafness. gNeurological disability category includes conditions such as multiple sclerosis, cerebral palsy, spinal cord injury, Parkinson’s, spina bifida, attention-deficit/hyperactivity disorder (ADHD), traumatic brain injury, paraplegia, quadriplegia, epilepsy, stroke, and so on.
The two groups did not vary significantly with respect to gender, race, or ethnicity.
However, results show that people with early-onset disability were significantly less likely to have completed any type of postsecondary education (p < .01) than people with late-onset disability, although they were more likely to be employed (p < .05). People with early-onset disability were also significantly more likely to have never been married. In addition, people with early-onset disability were more likely to receive SSI (p < .001), while people with late-onset disability were more likely to receive SSDI (p < .001). People with early-onset disability were also significantly more likely to have Marketplace (p < .05), and Medicaid (p < .001) insurance types, whereas people with late-onset disability were significantly more likely to have Medicare coverage (p < .01). With respect to coverage, results show that people with late-onset disability were significantly more likely to report service limitations related to prescription medications (p < .001), general doctor visits (p < .01), specialist visits (p < .05), medical tests (p < .01), dental care (p < .001), durable medical equipment (p < .05), and personal assistance services (p < .01). In addition, people with late-onset disability were significantly more likely to report provider network limitations (p < .05) and, for those with employer-sponsored coverage or Medicare, to report out-of-pocket medical costs exceeding $1000 in the past year. Results related to self-reported health status show that people with late-onset disability were more likely to report fair/poor health (p < .001), a higher number of days in poor physical health (p < .001), and a higher number of days that their health prevented activities (p < .01) but did not vary significantly on self-reported mental health status.
Discussion
Overall, results show that people with late-onset disability face greater disparities with respect to self-reported health, out-of-pocket expenditures, and access to health care compared to people with early-onset disability. Previous authors (Jamoom et al., 2008) have suggested that differences in self-reported health between early- and late-onset disability groups may be due to differences in adaptation to disability, disability identity, onset-specific diagnoses, or social support. People with early-onset disability are more likely to have a strong sense of disability identity, adapt their life to fit the needs of their disability, and to identify as part of the disability community (Hahn & Belt, 2004). At the same time, people with late-onset disability are more likely to compare their health to the time before they acquired their disability and may be more resistant to lifestyle changes (Finch & Robinson, 2003).
Results from this study, however, suggest that a further reason for health disparities may be differential access to health care. Indeed, people in the late-onset disability group were more likely to have higher out-of-pocket expenditures across all types of insurance coverage and had significantly poorer access to all types of health care services except mental health care. This combination of high costs and poor access to health care is known to result in poorer health outcomes (Sommers et al., 2017).
Although the late-onset group was significantly more likely to be married, members of that group had slightly lower rates of employer-sponsored health insurance coverage and slightly higher rates of uninsurance. Thus, while marriage can be a protective factor in overall health (Wood et al., 2009), it does not seem to have improved health or access to health insurance for this group. Similarly, the late-onset group was significantly more likely to have Medicare coverage than the early-onset group. As noted, Medicare does not typically cover some services, such as dental and vision care and personal assistance services, which may have resulted in access barriers for the late-onset group.
As summarized above, people with late-onset disability reported significantly greater unmet need for dental care, prescription medications, and personal assistance services compared to people with early-onset disability. In addition, results show that certain types of disabilities are significantly more likely to occur as late onset, including chronic illness, and physical and neurological disabilities. Some research suggests that people who develop these types of late-onset disabilities are likely to have high expenditures associated with health care and that people with late-onset disability report higher levels of financial worries compared to people with early-onset disability (Choi, 2018).
Several potential policy actions for Medicare are suggested by these findings. Currently, people with disabilities who experience high medical expenditures may be forced to pay significant amounts because Medicare does not include a cap on cost sharing. Out-of-pocket caps, potentially based on recipient income levels, could be established to support people with late-onset disability who experience health events resulting in oppressive costs. Such caps are needed for Medicare hospital, outpatient, and prescription drug coverage (Parts A, B, and D). Similarly, Medicare could support states in expanding eligibility for Medicare premium and cost-sharing assistance programs for enrollees with lower incomes. Finally, Medicare does not currently cover many common and costly health care needs, such as dental services, vision services, and long-term services and supports (LTSS). Coverage of these health care services is recommended to prevent catastrophic out-of-pocket health expenditures, promote equitable access to needed care, and to potentially prevent higher future Medicare costs and worse outcomes due to delayed or forgone care.
Limitations
These study results combine data from people with a variety of disability types, which may have confounded results given that certain types of disabilities are more prevalent during early or late onset. For example, the most common disability type for the early-onset group was developmental disabilities (25.8%), whereas the most common disability types for the late-onset group were chronic illness (28.9%) and neurological disabilities (28.9%). Moreover, the early-onset group was, on average, 13 years younger than the late-onset group. It is possible that certain types of disabilities may be associated with greater health care needs and costs and that costs increase with age. In addition, people with specific types of disabilities may qualify for disability-specific waivers, which may further enhance their access to health care and needed supports.
This study uses point-in-time data. Future research is needed to examine differences in health among people with early- and late-onset disability across the lifespan or across people who have experienced disability for a long or short duration. Future research is also needed to compare health care access among people with early- and late-disability onset while controlling for disability type. In addition, other information, such as ratings on ability to manage one’s own health, awareness of disability-related supports and services, and current levels of social support could be collected to examine additional variables that may affect self-reported health among people with early- and late-onset disability.
Conclusions
This study is the first known research to compare differences in health insurance and access to health care among people with early- and late-onset disability. Given that people with late-onset disability report higher out-of-pocket health care expenditures and significantly greater access limitations, medical professionals, and disability service providers should be mindful about assisting this population in locating appropriate health insurance coverage, health care services, and financial assistance. With the current political debate opening the possibility of extending Medicare coverage to all Americans, it will be important to assess if the coverage for individuals with late-onset disabilities is sufficient to meet their needs and is affordable. Conversely, efforts to limit protections and coverage for people with pre-existing conditions must also be monitored closely to assure that coverage for this group is not reduced or lost.
Footnotes
Acknowledgements
The authors would like to thank Dr. Adele Shartzer from The Urban Institute for development of the survey weighting methodology.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work and the National Survey on Health and Disability (NSHD, formerly the National Survey on Health Reform and Disability) is part of The Collaborative on Health Reform and Independent Living (CHRIL) funded by the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR, grant number 90DP0075-01-00).