
Abstract
Academic and government policy evidence that quantifies the disadvantage experienced by people with disabilities in the United Kingdom relies on “global” self-reported measures of disability available in large-scale national surveys. Understanding who is captured by such measures and the “process of disablement” is therefore vital. This article applies multivariate regression analysis to nationally representative and uniquely rich data for Great Britain from the Life Opportunities Survey (2009–2011) to investigate the relationship between a well-established measure of activity-limiting disability and the type and severity of impairment. Conditional on personal characteristics, the risk of disability is found to increase with the presence and severity of impairment. It also varies dramatically by impairment type, being highest for those with impairments relating to mobility and mental ill-health, and lowest for impairments relating to vision and hearing.
In line with increasing recognition of disability in government policy and equality legislation, there has been a growth in international evidence within social science that explores the disadvantage experienced by people with disabilities (see, e.g., Baumberg et al., 2015; Berthoud, 2008; DeLeire, 2001; Jones et al., 2006; Jones & Wass, 2013) and evaluates the impact of key policy changes (Acemoglu & Angrist, 2001; Bell & Heitmueller, 2009). Although not without limitations (see, e.g., Bound, 1991), disability is typically measured in these empirical studies by means of a “global” binary self-reported measure that identifies people with disabilities as those who face participation restrictions in life situations, such as in work or daily activity. While the underlying concept of disability itself has been debated (McDermott & Turk, 2011) and its measurement has been recognized as complex (Altman & Gulley, 2009; Berthoud, 2008; White, 2009), understanding such measures is vital, not least because evidence that quantifies and monitors the social and economic impact of disability forms the basis for government policy (e.g., U.K. government commitments on disability and employment (see Powell, 2019)).
While the International Classification of Functioning, Disability and Health (ICF; World Health Organization, 2001) defines disability broadly, collectively referring to impairments, activity limitations, and participation restrictions in the context of social and economic analysis, disability is more usually defined as the threshold for participation restrictions. Although there is no universal characterization, in the framework by Altman (2014), impairments give rise to functional limitations and put an individual at risk of activity limitations and participation restrictions. Therefore, while impairment, defined as a loss in bodily function resulting from a health condition, is typically a prerequisite for disability, impairments do not automatically impose a restriction usually required to define disability, including in U.K. equality legislation. Nevertheless, in line with the ICF, which is based on the biopsychosocial model, participation restrictions are widely understood, including in the United Kingdom, as the outcome of the interaction among the impairment, the person, and their physical, social, and attitudinal environments.
The importance of understanding the concept of disability has been recognized in empirical analysis, which demonstrates the implications of the measurement of disability, particularly the differences between broad and narrow measures, on estimates of prevalence (Altman & Gulley, 2009) and the extent of disadvantage (Burkhauser et al., 2014). While still concerned with the measurement of disability, we ask a simpler and perhaps more fundamental research question, namely, who is most at risk of reporting disability in survey data? We do this by examining the empirical relationship between the presence and type of impairment, its severity, and an extensively used “global” activity-limiting measure of disability similar to that applied in equality legislation. This is made possible by exploiting uniquely rich information on the presence and extent of impairment that is available in a novel and nationally representative survey focused on disability in Britain, the Life Opportunities Survey (LOS). In doing so, we provide new evidence on a key issue in empirical research, that is, who is captured by measures of disability in national surveys.
This emphasis is consistent with growing recognition in the literature that any dichotomous measure of disability is restrictive, neglects substantial heterogeneity within the disabled population, and ignores individuals with functional limitations that are not currently, but could subsequently become, participation restricting (Altman, 2014). Existing studies have already highlighted the value of considering diversity among people with disabilities, including in terms of the nature of impairment, severity, and duration, to understanding the implications of disability (Jones, 2011; Meyer & Mok, 2019) and designing more tailored policy support (White, 2009). Nevertheless, we know relatively little about the preceding step, that is, at what point impairments are disabling, which is the focus of this analysis.
Background
Defining disability is a fundamental challenge in social science research. The theoretical debate in the United Kingdom is captured, at the extremes, by the social and medical models of disability (see Berthoud, 2008, for a discussion). The medical model views disability as a consequence of a physical or mental restriction with the responsibility inherently individual and with emphasis largely on clinical intervention and rehabilitation. In contrast, the social model views barriers to participation as being socially constructed arising through, for example, the physical environment, social attitudes, or institutional practices (Oliver, 1990). In the latter, the emphasis is therefore on promoting social change, such as via improvements in physical accessibility or attitudes toward inclusion. In the United Kingdom, it is the social model that is currently the dominant approach in the field of disability studies (Jones & Wass, 2013), forms the basis of equality legislation (Berthoud, 2014), and informs government policymaking (Office for Disability Issues [ODI], 2011).
Each model of disability has been criticized: the medical model for ignoring the influence of society and the social model for ignoring the impact of impairment (Shakespeare & Watson, 2001). As Imrie (2004) concisely puts it, the distinction is artificial when “biology and society are entwined” (pp. 287–288) and, as such, disability cannot be fully understood using either model in isolation. It is not surprising then that a vast range of views lie between these two extremes (Palmer & Harley, 2012), and models that attempt to integrate these theories have been developed (see, e.g., Nagi, 1991). A comprehensive review of these debates was provided by Berghs et al. (2016), who highlighted alternative theoretical models, including those that stem from the Convention on the Rights of Persons with Disabilities, where disability is related to the ICF but recognized as an “evolving concept.” Nevertheless, in the context of ongoing and changing conceptual debates, an appreciation of the theoretical extremes, albeit necessarily neglecting complexity, provides a useful background from which to explore disability as operationalized in empirical work.
The conceptual debate is often side-stepped in empirical studies that, by necessity, measure disability using existing and predetermined questions available in national surveys. These measures are, at best, likely to partially capture the population defined by the broader disability concept (Altman & Gulley, 2009; Burkhauser et al., 2014) and may be more or less appropriate depending on the conceptual framework and specific research question. Nevertheless, it is important that disability prevalence is measured and monitored, with existing “global” metrics being important in the United Kingdom to identify who is covered by equality legislation (White, 2009), establish the scale and nature of disadvantage associated with disability (Berthoud, 2008), and influence government policy (White, 2009). It is, however, also vital that we understand who is captured by these measures and the implications of this for measuring disability-related disadvantage. The ICF prompted the integration of conceptual and measurement debates (Palmer & Harley, 2012). Although not without limitations (Imrie, 2004; McDermott & Turk, 2011), the ICF framework, which is based on the biopsychosocial approach, seeks to synthesize medical and social models to form a measure of disability reflecting biological, individual, and social perspectives. It has been referred to as “a systemic and comprehensive way of conceptualizing the population with disabilities” (Burkhauser et al., 2014, p. 2) and has informed the design of the measures in the LOS analyzed in this article.
Empirical studies have acknowledged the importance of measurement and the insights provided by recognizing the complexity of disability, including that a binary divide is unnecessarily simplistic and restrictive (Jones & Wass, 2013) and that capturing heterogeneity among people with disabilities advances understanding of its social and economic consequences (Jones, 2011; Meyer & Mok, 2019). In Britain, for example, Berthoud (2014) documented how employment disadvantage varies among people with disabilities on the basis of the severity of impairment, and Jones and Wass (2013) provided a comparison between disadvantage associated with impairment and disability. However, Berthoud (2008) argued that it “has to be questioned whether valid conclusions can be drawn about the impact of disability, when disability itself is not one of the variables under study” (p. 130), and it is understanding the relationship between impairment and disability that forms the contribution of this analysis.
By exploring the empirical relationship between impairment and associated functional limitations, which are inherently more medical, and a “global” measure of disability in the United Kingdom, which reflects the threshold at which such limitations are restricting, this article provides insights into the “process of disablement” (Altman, 2014; Verbrugge & Jette, 1994). In this way, we start to explore the complex relationship between impairment and disability described by Shakespeare and Watson (2001) as “different places on a continuum” (p. 22), making the boundary difficult to distinguish and, recently by Grue (2016), as insufficiently understood in the context of the social model.
In line with the discussion in Berthoud (2008), some might criticize the emphasis on impairment as too aligned to the medical model. However, our analysis does not assume a one-to-one relationship between impairment and disability. Instead, it aims to quantify this relationship, recognizing that the same impairment is not necessarily equally disabling to all individuals, consistent with the social determinants of disability. Furthermore, in controlling for individual characteristics, we are also able to explore the extent to which these broader factors affect the risk of disability. The analysis is made possible by the introduction of the LOS (2009–2014), a specialized survey on disability administered to a nationally representative sample, that provides a unique opportunity to explore these complex questions and further our comprehension of existing measures of disability that underpin a body of statistical evidence on disability-related disadvantage in the United Kingdom.
Method
Data and Measures
The LOS was undertaken in Great Britain between 2009 and 2014 and was collected by the Office for National Statistics (ONS) on behalf of the U.K. government Office for Disability Issues (ODI). It is made available to researchers by the U.K. Data Archive (see Office for National Statistics, Social Survey Division, 2014) and has been used by permission. None of these organizations bear any responsibility for the analysis or interpretation of the data undertaken here. The LOS is a nationally representative survey designed specifically to collect information on the participation of people with disabilities across a range of activities, including work, education, and social participation. It updated previous specialized data collection often based on relatively ad hoc additions of samples of people with disabilities within existing surveys, such as the health and disability follow-up to the 1996/97 Family Resources Survey (see Berthoud, 2008), and provides the most recent comprehensive and specialized information on disability in Britain. Importantly, it addressed a weakness of previous U.K. disability surveys by collecting separate information on impairment and disability.
This analysis focuses on information obtained in Wave 1, collected from a random sample of private households between June 2009 and March 2011. This avoids the complexity introduced by the non-representative data collection at two subsequent waves (after which the survey was discontinued), in which only a subsample of individuals without impairments was re-interviewed. Attention was restricted to the 26,002 individuals of working-age (men ages 16–64 years and women ages 16–59 years) because (a) these individuals are typically the focus of social and economic analysis of disability and (b) several of the control variables of interest were not collected outside this age range. All the results are presented unweighted but do not differ when weighted by the selection weights provided by the LOS (available on request).
Disability
Although not without criticism in relation to both concept and measurement, quantitative evidence in the United Kingdom, as well as internationally, has relied on “global” binary disability indicators regarding activity or participation restrictions collected in survey data. Consistent with this, our disability measure was derived from responses to the following two questions. Initially, individuals are asked “Do you have any long-standing illness, disability or infirmity—by long-standing I mean anything that has troubled you over a period of time or that is likely to affect you over a period of time?” Those who respond positively are subsequently asked “Does this illness or disability (Do any of these illnesses or disabilities) limit your activities in any way?” As is typical in the literature, those who responded positively to both questions are defined as (activity-limited) disabled (15.4% of the sample) and all other individuals were classed as non-disabled. This measure, often referred to as “limiting long-standing illness or disability,” is a harmonized measure, available across other large-scale U.K. surveys administered at that time, including the Health Survey for England and General Household Survey, where the prevalence in 2009 was comparable at 18% and 15%, respectively (see Baumberg et al., 2015). Moreover, activity-limiting disability, albeit measured using a variety of question wordings in alternative surveys, is one of the three established disability definitions in the United Kingdom (see Bajekal et al., 2004), the others being defined by work-limitations and equality legislation (such as the Disability Discrimination Act of 1995 [DDA]). While activity-limiting disability aligns with the definition applied by equality legislation and has been previously shown to produce comparable prevalence rates to the DDA definition (Bajekal et al., 2004), the absence of explicit reference to “day-to-day” activities means that conceptually it fails to clearly distinguish between activity and participation restrictions. The LOS also collects information on disability according to the DDA definition, but its measurement is not consistent with those of other national surveys; we therefore focused on the harmonized activity-limiting disability measure. According to the activity-limiting definition, over 80% of people with disabilities are also considered to have a disability according to the DDA measure, and our findings (not reported in full but available on request) are qualitatively similar, albeit larger in magnitude, when using the DDA definition. We also noted that similar measures are used across countries, for example, in European surveys, but these are neither standardized nor universal. Despite the move to collect internationally comparable information on functional limitations, such as via the Washington Group, to indicate risk of disability, this has not been widely used in the United Kingdom.
Impairment
One of the aims of the LOS is to collect information on the prevalence of a range of impairments and hence address concerns relating to the lack of evidence on how these interact with environmental barriers to create disability (White, 2009). Unlike other surveys in which information on the nature of impairment is often only asked of those persons who report a long-term health problem, the LOS collects information in relation to a range of dimensions of physiological and psychological function among all individuals, facilitating analysis of those “at risk” of disability. The information captures difficulties with vision, hearing, speaking, mobility, dexterity, long-term pain, breathing, learning, intellect, behavior, memory, mental, and an Other category (see online supplemental material Table S1 for definitions). While designed on the basis of international standards, in terms of the framework of Altman (2014), this information relates both to impairment (e.g., mental impairment) and functional limitations arising from impairment (e.g., mobility impairment). Therefore, we cannot clearly distinguish between these concepts that, consistent with the LOS, we refer to as impairment throughout. Before considering each type of impairment, we generated an aggregate measure (“any impairment”), constructed from a positive response to one or more of the above impairment types, and further distinguished individuals with single or multiple impairments.
For those who reported impairment, further information was collected on what we referred to as severity, that is, the intensity of difficulty and frequency of limitation. This information is specific to the particular impairment, for instance, “difficulty communicating with others” (speaking) or “difficulty lifting, grasping, or holding objects” (dexterity). Unlike for the other measures, for physical impairments it is made explicit that the difficulty is assessed after accounting for equipment/aids/medication. For hearing, for example, individuals are asked “(With your hearing aid) how would you describe your difficulty hearing?” where the responses are increasing in intensity: no difficulty (1), mild difficulty (2), moderate difficulty (3), severe difficulty (4), cannot do (5). These questions and responses also differ across impairment types. For long-term pain, learning, intellect, behavior, memory, mental, and Other, the responses were “mild,” “moderate,” and “severe.” The response “cannot do” was possible for some impairment types (e.g., vision, hearing, speaking, mobility, dexterity) and was merged with “severe” in this analysis. The response “no difficulty” was also only possible for some impairment types (e.g., vision, hearing, speaking, mobility, dexterity, and breathing) but was retained as a distinct category in the analysis. For long-term pain, intensity was only asked of individuals in pain so, for consistency, those respondents with impairments who were not asked this were defined as “no difficulty” (less than 1.5% of responses). Unlike some analyses that impose an intensity threshold to define impairment (e.g., ODI, 2011), we used the range of responses to explore the relationship between the intensity of impairment and disability.
For each type of impairment, persons who responded that the intensity of difficulty was at least “mild” are then asked, “How often does this limit the amount or kind of activities that you can do?” Responses were coded as always (1), often (2), sometimes (3), rarely (4), never (5) and were the same across impairment types, facilitating comparability between impairments. Due to small sample sizes, we merged always and often into one category and rarely and never into another category in the analysis of impairment types. This information captured frequency of the limitation as a dimension of severity and was particularly relevant for intermittent impairments. However, as a consequence of focusing on activity rather than functional limitations associated with a specific impairment, it is more directly related to the concept and measurement of disability, and it perhaps illustrates the difficulty in operationalizing such complex and debated concepts. Consistent with this, the information has been used to define impairment (ODI, 2011) and disability (Emerson & Roulstone, 2014) in different contexts. Therefore, while it provides additional and more specific information relative to the “global” disability measure, recognizing the conceptual limitation, we used each dimension of severity separately and estimated the models sequentially, gradually adding this information. In a similar manner, we used both intensity and frequency severity measures on each impairment type and also aggregated to form proxies across impairment types, by taking the maximum intensity and frequency across impairments reported as per the ODI (2011). Finally, similar to the ODI (2011) and Berthoud (2014), we constructed a combined measure set out in Table 1, which interacted both dimensions of severity (intensity and frequency, respectively) without imposing any assumptions about which, if either, is more important.
Descriptive Statistics: Disability and Impairment in the United Kingdom as Reported in Wave 1 of the Life Opportunities Survey.
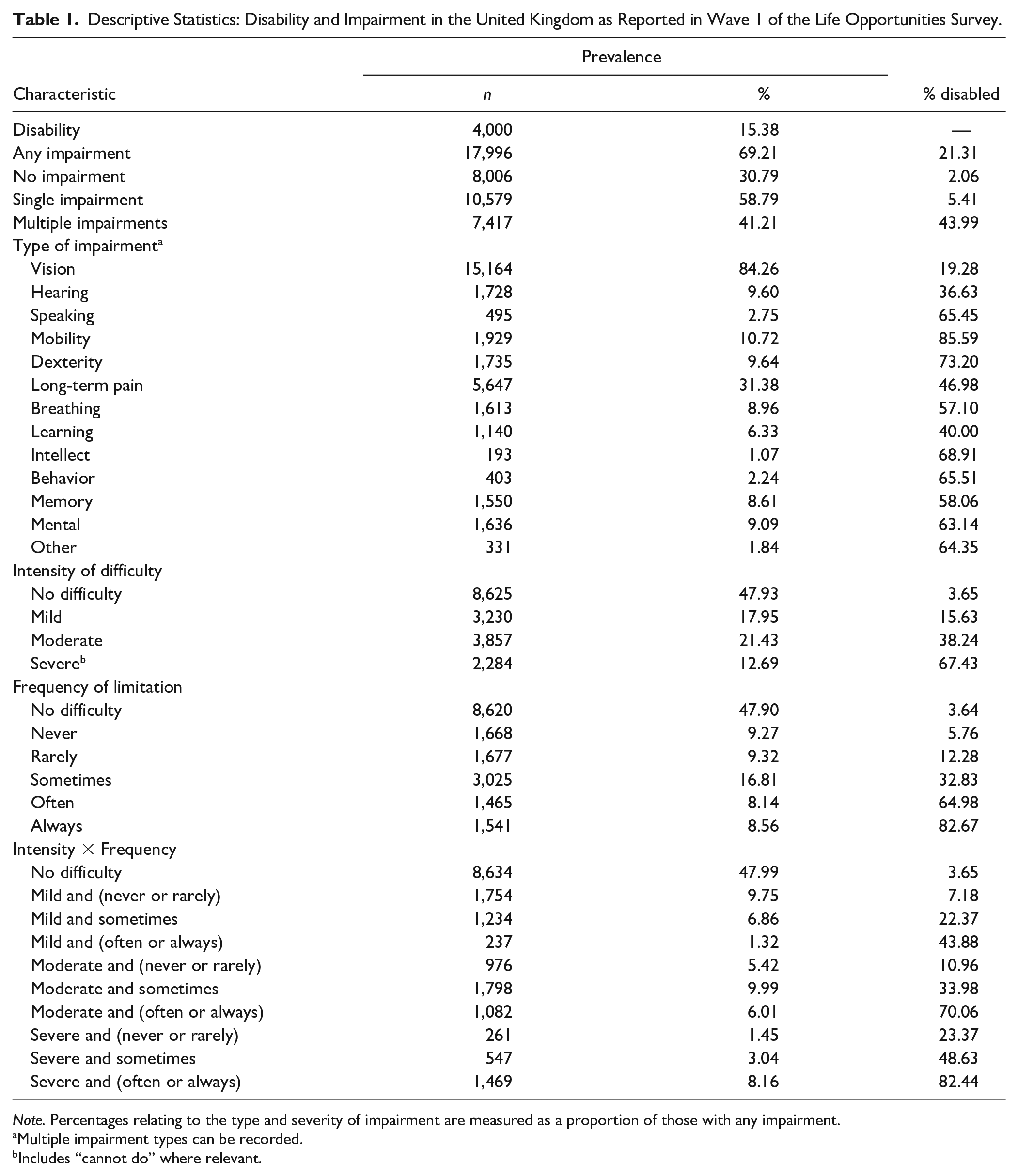
Note. Percentages relating to the type and severity of impairment are measured as a proportion of those with any impairment.
Multiple impairment types can be recorded.
Includes “cannot do” where relevant.
The LOS also contains corresponding information on diagnosed chronic health conditions. Given their distinct nature but potential correlation with impairment, we excluded chronic conditions from our main specifications but subsequently included them in the sensitivity analysis. These results are presented in the online supplemental material (see Figures S1 to S3 and Table S4). The qualitative pattern of results remains unchanged.
Descriptive statistics
Table 1 presents summary statistics for the measures of disability and impairment introduced above. More than two thirds of respondents (69%) reported any impairment, with the most common types being vision (84%) and long-term pain (31%). Consistent with the framework of Altman (2014), we did not find a one-to-one relationship between our measures of impairment and disability. In line with both the social and medical models, disability was largely confined to individuals with impairment (where the prevalence was 21%), with only 2% of individuals without impairment reporting disability (and itself perhaps reflecting an incomplete coverage of impairment in the LOS). However, impairment certainly does not imply disability, and 79% of persons with impairment did not report disability, consistent with the importance of an individual’s environment. Disability is more prevalent among people with multiple impairments (44%) and people with impairments relating to mobility and dexterity relative to impairments relating to vision and hearing. Unsurprisingly, disability was increasing in both the intensity and frequency measures of severity. For example, among respondents who reported frequency of the limitation as always, 83% reported disability. This suggests there is greater overlap between the “global” measure of disability and other, more severe measures of limitation, or what Altman and Gulley (2009) referred to as more conservative measures of the disability process.
Statistical Methodology
Differences in the risk of disability may arise, even conditional on impairment, as a consequence of other personal characteristics being correlated with an individual’s environmental barriers. As such, in addition to information on impairment, we controlled for a range of personal characteristics in the multivariate analysis that follows. This has two advantages: (1) we could estimate the relationship between impairment and disability conditional on a set of personal characteristics, which themselves might be correlated with impairment, and (2) we could explore whether there was a relationship between personal characteristics and disability, conditional on impairment. Given the binary nature of the dependent variable (disability), we estimated a probit model in which the propensity of individual

However, only the binary indicator was observed:
In a similar manner to Jones (2011), personal characteristics in
Our focus, however, is on the relationship between impairment,
We acknowledge that these coefficients reflect associations and cannot be interpreted as causal relationships, particularly given that disability and impairment are reported by the same individual at the same point in time. Although information on disability and impairment is collected in distinct sections of the survey, a common element to individual reporting thresholds would result in the relationship, particularly in relation to severity, being overestimated. Moreover, while we believe the effects to be small, it is also not possible to rule out reverse causality via secondary conditions in the disablement process (Verbrugge & Jette, 1994).
Information is also available in the LOS on whether individuals claimed sickness and/or disability benefits, which are subject to an independent and more objective medical assessment. Studies such as that conducted by Burkhauser et al. (2014) have used this type of information to explore the validity of self-reported disability. While criticized by Altman (2014), not least because eligibility requirements are context specific and application is in part determined by individual preferences, we nevertheless explored the robustness of our key findings to using a broad measure of current receipt of any sickness or disability benefit. This included in-work and out-of-work disability benefits, such as Employment and Support Allowance and Disability Living Allowance, claimed by about 6% of the sample. These results are presented in the online supplemental material (see Figure S4 and Table S5). Although smaller in magnitude, they exhibit the same qualitative patterns—albeit a relatively strong relationship with impairments relating to intellect and behavior—consistent with previous evidence of the prevalence of mental health conditions among benefit recipients.
Results and Discussion
Marginal effects from the disability probit model, evaluated at the mean of the explanatory variables, are presented in Table 2. The measures reflect an aggregation across different impairment types. Personal characteristics are included in all specifications (but are not reported) and even after accounting for the detailed impairment information, disability is negatively correlated with educational attainment. While we cannot rule out that education influences the reporting of disability, the relationship is consistent with education being an environmental factor that reduces the risk of a participation restriction regardless of impairment. As such, the well-established negative correlation between education and disability is not simply a consequence of education being a socioeconomic determinant of underlying health/impairment (Berthoud, 2008).
The Relationship Between Impairment and Disability in the United Kingdom: Intensity and Frequency.
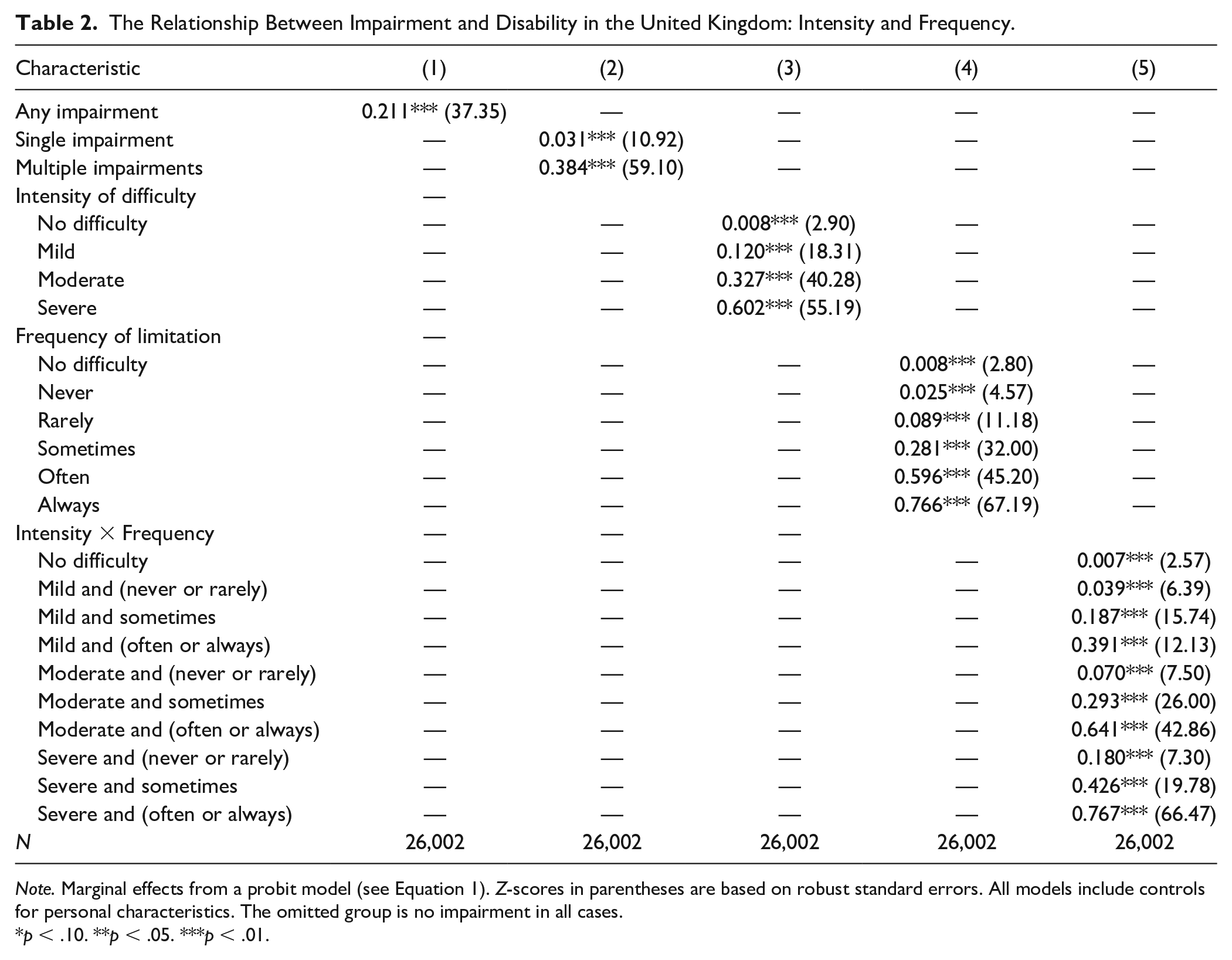
Note. Marginal effects from a probit model (see Equation 1). Z-scores in parentheses are based on robust standard errors. All models include controls for personal characteristics. The omitted group is no impairment in all cases.
p < .10. **p < .05. ***p < .01.
Consistent with impairment and disability being distinct but related concepts, Column 1 indicates that, after accounting for personal characteristics, individuals reporting impairment were 21 percentage points more likely to report disability. Column 2 highlights the importance of the influence of multiple (38 percentage points) relative to single (3 percentage points) impairments. Disability also increases monotonically with the reported intensity of difficulty (Column 3) and frequency of the associated limitation (Column 4). Perhaps unsurprisingly given the nature of the measures, frequency was more strongly related to disability; respondents who reported always being limited were 77 percentage points more likely to report disability than respondents with no impairment.
The two dimensions of severity are combined in Column 5 where, as expected, respondents who reported more intense and frequent limitations were most likely to report disability. However, at a given level of intensity, frequency matters (and vice versa) suggesting each captures a separate element of the relationship between impairment and disability. For example, relative to individuals without impairments, severe impairments that are never or rarely limiting increased the probability of reporting disability by 18 percentage points, but severe impairments that are often or always limiting increased the probability by 77 percentage points. The latter compares to 39 and 64 points for respondents who were often or always limited but who described their impairment as mild and moderate, respectively.
A full set of estimates for the analysis of impairment type are provided in the online supplemental material (see Table S3) but these are presented in Figures 1 through 3 to facilitate comparisons. Figure 1 presents the marginal effects relating to the presence of each type of impairment. After controlling for personal characteristics, impairments associated with mobility (23 percentage points), mental ill-health (17 percentage points), long-term pain (14 percentage points), and breathing (11 percentage points) were most strongly related to disability. All impairment types were positively associated with disability, but the marginal effects relating to vision and hearing impairments were small in magnitude at 1 and 3 percentage points, respectively, highlighting the important distinction between the concepts of impairment and disability as operationalized in the LOS. While it is not possible to identify the precise reasons for the differences between impairment types, which could arise due to differences in medical and/or social drivers, the stark variation confirms the importance of impairment type in understanding the risk of disability.
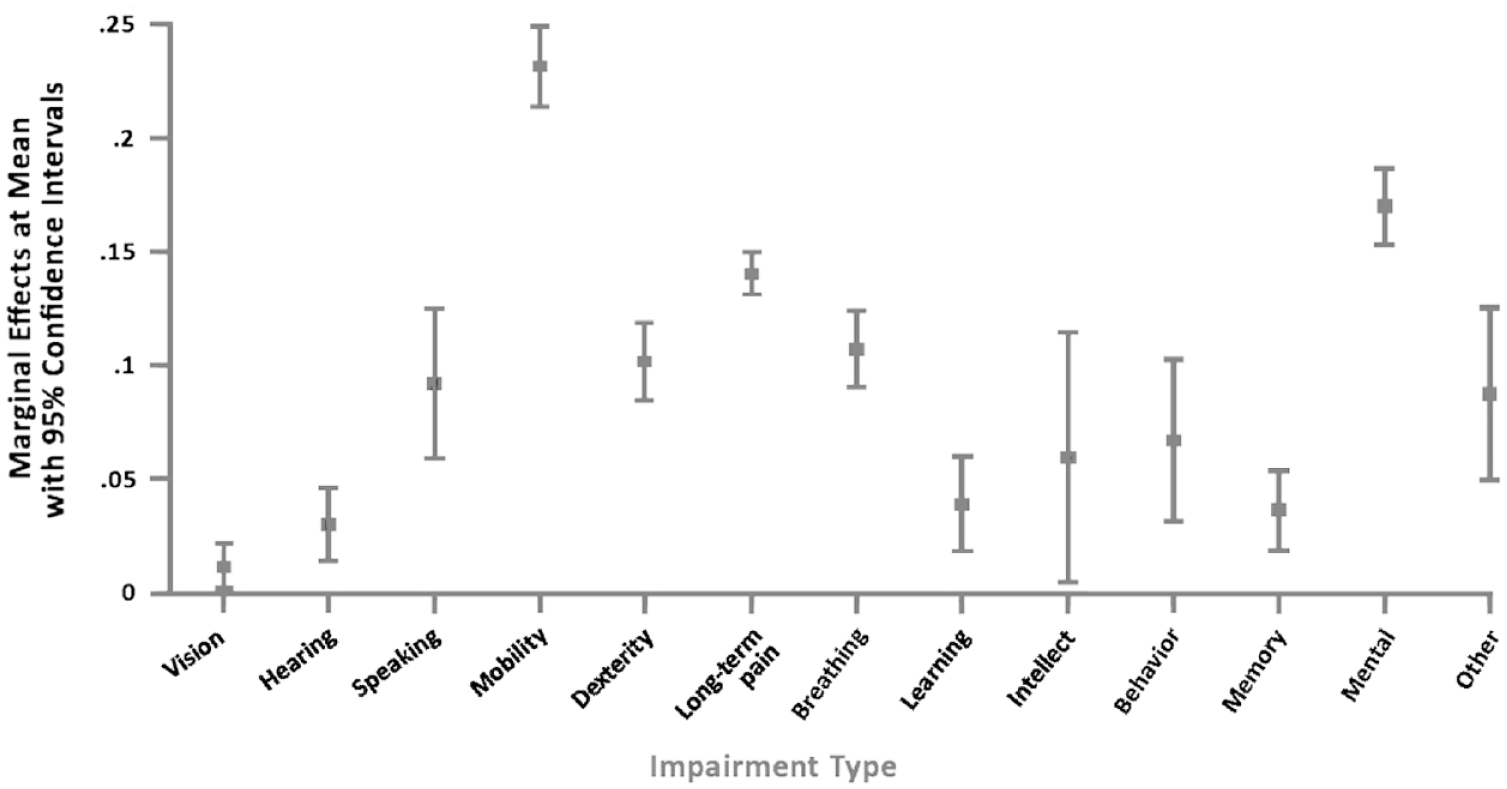
Relationship between the type of impairment and disability.
In Figure 2 the influence of each impairment type was allowed to vary by intensity of difficulty. In general, the probability of reporting disability increased with intensity, although the standard errors, particularly for severe difficulty, were sometimes large. The relationship between intensity and disability was more pronounced among impairments relating to mobility, mental ill-health, and long-term pain and was largely absent among impairments relating to speaking, learning, intellect, behavior, and memory.
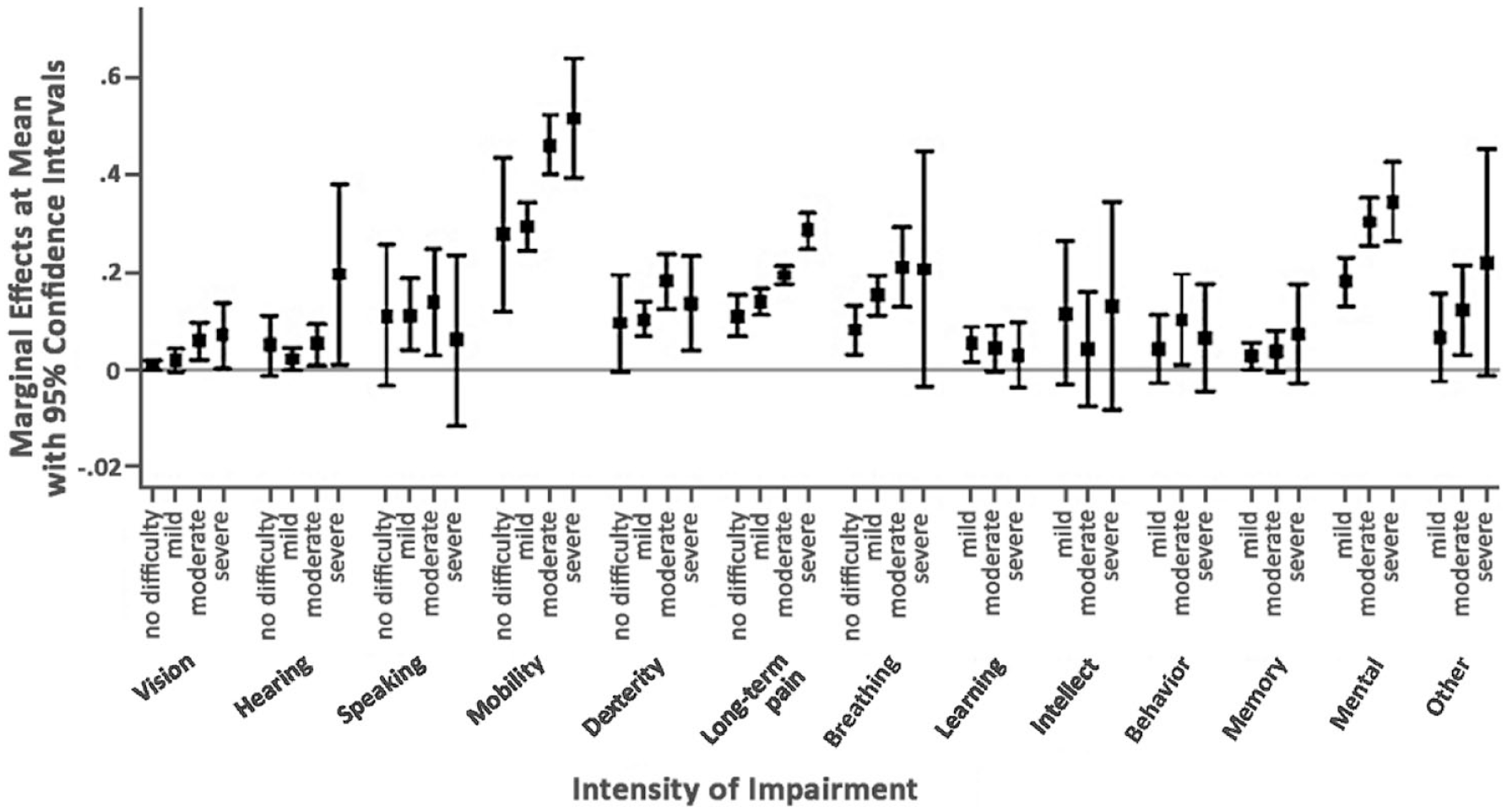
Relationship between the type and intensity of impairment and disability.
Within impairment types, there was typically a clearer relationship between disability and frequency of limitation (see Figure 3). This was particularly pronounced for mental ill-health and long-term pain but was also evident for vision, hearing, and breathing. Impairments relating to vision and hearing needed to be limiting at least sometimes to increase the probability of reporting disability. Indeed, the influence of hearing limitations reported as often/always limiting was of comparable magnitude to mobility impairments that were never/rarely limiting.
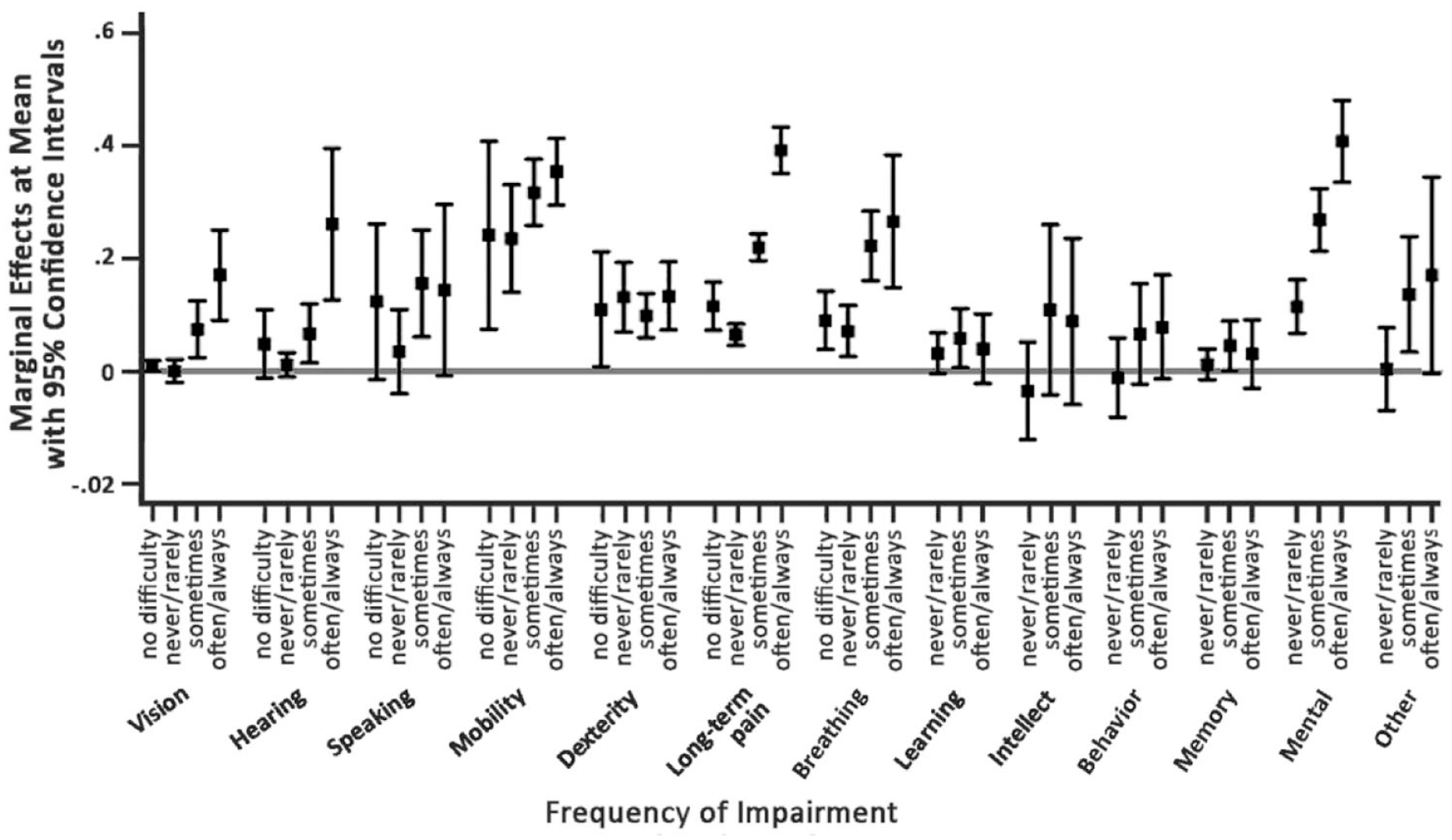
Relationship between the type and frequency of impairment and disability.
Conclusion
One of the reasons the LOS, a large and nationally representative survey focused specifically on disability, was commissioned in Britain was to collect detailed information on the nature of impairments and extent of associated functional limitations among the population. We used this information to explore the disablement process, particularly the relationship between impairment and disability. We did this by examining how the reporting of a widely applied “global” activity-limiting measure of disability varied with the type and severity of impairment, where the latter was measured by both the intensity of difficulty and frequency of limitation. Rather than contributing to the debate on optimal measures of disability, our aim was somewhat simpler: to better understand the relationship between the more objective and medical measures of impairment and the broader social measure of disability. In doing so, we contributed to the empirical literature by enhancing understanding of the composition of people with disabilities captured in U.K. surveys and national statistics, which underpin (national) estimates of the prevalence of disability and a body of evidence on the extent of disability-related social and economic disadvantage, including that used for policy development and evaluation.
Our evidence confirms the important distinction between impairment and disability, with about one in five working-age individuals with impairment reporting activity-limiting disability. Furthermore, we showed that after accounting for personal characteristics, the probability of reporting disability is positively associated with the presence of impairment and, reflecting increasing severity, with the intensity of difficulty and frequency of limitation. Individuals with mobility and mental health impairments have the highest probability of reporting disability, consistent with there being more pronounced restrictions relating to these impairment types. Among both these impairments there was also a clear gradient, with the risk of disability increasing with the intensity of difficulty. Although severity is not directly comparable across impairment types, it is worth noting the scale of some of the differences. For example, severe vision difficulty increased the risk of disability by 7 percentage points compared with 52 percentage points for severe difficulty in mobility, which was potentially a result of differences in the extent to which an individual’s environment limits the restrictions associated with different impairments. Indeed, even after accounting for a comprehensive set of measures of impairment, personal characteristics remained important, with education reducing the risk of reporting disability consistent with its broader social determinants.
This type of information is clearly important in understanding the relationship between impairment and disability, and in identifying those most at risk of disability, which is particularly critical to organizations that seek to support individuals with specific impairment types. Moreover, it is important in enhancing our understanding of the composition of people with disabilities in the United Kingdom that, in turn, is essential to designing effective policy to reduce disability-related social and economic disadvantages. In this respect, current national data collection needs to extend the established collection on “global” measures of disability in non-specialist surveys to regular collection of complementary information on impairment and functional limitations through more specialized surveys. This will enable exploration of how the risk of disability associated with a more objective and medical concept changes over time and, in doing so, will provide an indication of changes in the environmental barriers that limit participation. Such information would also provide an important benchmark from which to enhance our understanding of trends in disability prevalence. While the analysis demonstrates the importance of integration between the concept and measurement of disability, and the significance of precisely designed data collection that carefully considers distinct elements of the disablement process, it also highlights the complexity of this task, especially in the context of ongoing conceptual development and the lack of consistency in measurement. It perhaps also renews questions as to whether disability is best measured as a binary outcome.
Despite using data from a specialized national survey, our analysis was inevitably restricted to the specific measures collected, which we recognize as imperfect conceptually, and in the absence of standardized measures, is necessarily illustrative. Indeed, we acknowledge that there is considerable international variation in the definition and measurement of disability, which limits the generalizability of the findings. We also acknowledge that even within Britain, there are differences in the definition and measurement of disability across surveys and over time. However, by illustrating the complexity underpinning a seemingly simple “global” measure of disability widely used in the United Kingdom, we seek to enhance awareness and encourage further empirical scrutiny of the definition and measurement of disability. There is a clear advantage of future longitudinal data collection on both impairment and disability to facilitate exploration of the dynamic process of disablement, including over the life-course, which would appear complementary to growing evidence on the disadvantage associated with disability onset (Meyer & Mok, 2019). Indeed, in providing evidence closer to identifying a causal relationship between impairment and disability, this type of analysis is key to developing proactive policy to reduce participation restrictions. The latter would also be supported by further investigation into the nature of participation restrictions arising from different impairment types.
Supplemental Material
sj-pdf-1-dps-10.1177_10442073211021532 – Supplemental material for Exploring the Relationship Between Impairment and Disability in Great Britain: Evidence From the Life Opportunities Survey
Supplemental material, sj-pdf-1-dps-10.1177_10442073211021532 for Exploring the Relationship Between Impairment and Disability in Great Britain: Evidence From the Life Opportunities Survey by Melanie Jones and Eirini-Christina Saloniki in Journal of Disability Policy Studies
Footnotes
Acknowledgements
The authors are grateful for comments on an earlier version of this article from two anonymous reviewers, Vicki Wass, Ben Baumberg Geiger, and participants at a seminar at the K. Lisa Yang and Hock E. Tan Institute on Employment and Disability, Cornell University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available on the Journal of Disability Studies website with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.