
Abstract
Introduction:
Nigeria has one of the highest rates of stillbirth in the world. Existing research about the state of bereavement care continues to paint a bleak picture. This study explores the stillbirth bereavement care practices of Nigerian midwives.
Method:
Purposive sampling was employed to recruit a sufficient sample of 11 Nigerian midwives, who were subsequently interviewed using a semi-structured interview guide. Data were analyzed using the template analysis technique, which involved the use of a coding template to organize themes.
Results:
Two main themes were identified: “Family-first, woman later” describes the practice of communicating stillbirth diagnoses to families before informing the woman; “Beliefs-driven care” describes the role of cultural values in facilitating some aspects of care, such as holistic care, while hindering other aspects such as memory-making.
Discussion:
Cultural beliefs influence stillbirth bereavement care practices. Clear clinical guidelines are needed to support midwives in managing cultural issues associated with stillbirth bereavement.
Introduction
In 2019, an estimated 171,428 babies were born in Nigeria with no sign of life at or after 28 weeks of pregnancy (UNICEF, 2020). Given these statistics, Nigeria has the highest rate of stillbirths in Africa and the second highest in the world (UNICEF, 2020). As in any other country, stillbirths in Nigeria occur unexpectedly. But what makes the devastating tragedy of stillbirth more profound in Nigeria is that 50% of stillbirths occur during labor and childbirth (UNICEF, 2020). While poor quality care has been identified as a key cause of stillbirths in Nigeria (Okunowo & Smith-Okonu, 2020), autopsies are rarely carried out after stillbirths (Ezugwu et al., 2022). Consequently, a clear cause is never identified. The absence of an explanation for causation and the fact that half of stillbirths occur at the time of birth indicates that in Nigeria, both stillbirth prevention efforts and quality bereavement care deserve equal attention.
Most research concerning the issue of stillbirth in Nigeria has focused on the causes, characteristics, trends and prevalence of stillbirths (Ezugwu et al., 2022; Okonofua et al., 2019; Okunowo & Smith-Okonu, 2020). This research has consistently revealed that women who did not register for antenatal care, those with a history of stillbirth or hypertensive disorders in pregnancy and those who experience a delay between the rupture of membranes and their childbirth experience higher rates of stillbirth (Milton et al., 2022). A limited number of studies have explored the perspectives of parents who have experienced stillbirth with the findings painting a bleak picture of the reality of parental grief in Nigeria. For example, qualitative studies in Nigeria have revealed that it is common practice for mothers to be quickly separated from their stillborn babies, while also constantly being urged not to linger in their grief (Adebayo et al., 2019; Popoola et al., 2024).
Given these prevailing practices and beliefs surrounding stillbirth in Nigeria, recent research revealing that health care providers may not have the knowledge required to meet the bereavement needs of parents comes as no surprise. For example, research by Kuforiji et al. (2024) and Popoola et al. (2021) identified frequent communication delays between the time of diagnosis of stillbirth and passing on this information to mothers. These communication lapses, as well as insensitive care, and limited emotional counseling (Kuforiji et al., 2024; Popoola et al., 2024) suggest that quality bereavement care remains elusive for Nigerian parents. Midwives’ ability to meet parents’ need for respectful care is important, not only because it has a long-lasting impact on the parental grief journey (Ellis et al., 2016), but also because it provides a means of identifying gaps in bereavement care. In much previous research however, the quality of care received after stillbirth has been mostly captured from the perspectives of parents in Nigeria. As a result, understanding of stillbirth bereavement care in Nigeria is one-sided, with available evidence failing to reveal a comprehensive account of issues associated with stillbirth bereavement care practices in Nigeria.
This article is drawn from a larger qualitative study that aimed to explore the experiences of Nigerian midwives who have experienced a stillbirth in their midwifery practice. The article seeks to describe and understand the stillbirth bereavement care practices of Nigerian midwives.
Method
Research Design
A qualitative descriptive design was used in this study to explore midwives’ bereavement practices. Qualitative description concerns itself with understanding the subjective individual human experience and is an appropriate methodologic approach when little is known about a topic (Doyle et al., 2020). In the context of this study, uncovering the “who” (midwives), “what” (stillbirth bereavement practices), and “where” (Nigeria) components of the research problem are important elements in understanding the findings. Consequently, qualitative description was considered an appropriate research design.
Ethical Considerations
The study was approved by the Human Ethics Committee of Victoria University of Wellington (30705) after a full ethics review. Written informed consent was obtained from all participants before interviews were conducted. The names used to present the findings are pseudonyms.
Participant Selection
Midwives who had experienced a stillbirth during their midwifery practice were purposively recruited from multiple settings of regulated midwifery practice in Nigeria, such as tertiary-, secondary-, and primary-level care, as well as private practice. Recruitment was achieved by emailing the study flyer to midwives in Nigeria for dissemination to their wider networks. Midwives who showed an interest in the study contacted the author and the author subsequently conducted eligibility checks to determine potential participants’ suitability. The eligibility criteria determined that participants should be currently engaged in midwifery practice in Nigeria, aged over 18 years and should have previously encountered stillbirth in their professional practice. Participants who met these criteria were sent the participant information sheet and informed consent was obtained before the phone interviews were conducted. Data saturation was reached with 11 participants when no new information was identified (Doyle et al., 2020).
Data Collection
Data was collected with the use of open-ended, semi-structured questions during telephone interviews that lasted between 22 to 43 minutes. In recognition of the barriers to participating due to shift work and family life, a sample interview guide was sent to each participant in advance of the telephone interviews. Sharing the interview guide in advance facilitated reflexive dialogue and reduced participants’ anxiety about what to expect during the interview. The interview questions were structured around two key areas, describing: (a) a birth that ended in stillbirth and (b) stillbirth management practices. The semi-structured interview questions were developed based on earlier studies of midwives’ experiences with stillbirth and the impact of stillbirth on midwives in other settings (Jones & Smythe, 2015; McDaniel & Morris, 2020). All the interviews were audio-recorded with the approval of the participants. The study was conducted over 4 weeks from December 2022 to January 2023 by the first author, a Nigerian native and PhD-prepared nurse-midwife.
Data Analysis
Recorded interviews were transcribed verbatim and were analyzed using the systematic method of Template Analysis. Template Analysis (TA) is a form of analysis where a coding structure (template) is developed and applied to the data in the analysis process (Tabari et al., 2020). In TA, the analysis starts with the identification of a priori codes, which are codes identified in advance of the main analysis due to their relevance to the issue being studied. The procedure for using TA for qualitative analysis is flexible, but generally follows a seven-step process (Tabari et al., 2020), which are (1) data familiarization, (2) preliminary coding, (3) organization of themes, (4) defining the template, (5) application of the final template to the full dataset, (6) finalization of the template definitions, and (7) writing up. In this study, 50 a priori codes that were highly relevant to the research question were first identified from the summary notes that were written at the end of each interview. These a priori codes and the transcripts were then imported into NVivo software where data familiarization, coding, and the development of the final template were completed. During the reading of each transcript, the a priori codes (template) were modified through the identification of new codes, refining of existing codes or the elimination of irrelevant codes and applied to the whole dataset. The final template comprised the study findings consisting of the themes representing the bereavement practices of Nigerian midwives. The Consolidated Criteria for Reporting Qualitative Research (COREQ) were followed (Tong et al., 2007).
Rigor
Rigor was achieved in this study in the following ways. All interviews were conducted by the same researcher with the same interview guide (dependability). The researcher was aware of the social desirability bias that can present itself, especially since the interview guide was sent ahead of time. As such, a nonjudgmental stance, openness and reflexivity were maintained during and after interviews (credibility). In addition, effective probing questions were used to explore the participants’ initial responses. The findings were also supported with exemplar quotes (confirmability). A schematic representation of the themes was shared with all participants for their comments, and those (six) who responded agreed with the findings, thereby enhancing the credibility of the results. All interviews were conducted by a native Nigerian PhD-prepared nurse-midwife with experience in researching reproductive losses in low- and high-income contexts, ensuring credibility. This positionality strengthened credibility in two ways. On one hand, the researcher’s insider knowledge of the research context helped with understanding the meanings that the participants ascribed to their stillbirth bereavement practices. On the other hand, the researcher’s knowledge of bereavement practices outside Nigeria also helped in recognizing similarities and differences between stillbirth bereavement care practices in Nigeria and elsewhere.
Results
Participants Characteristics
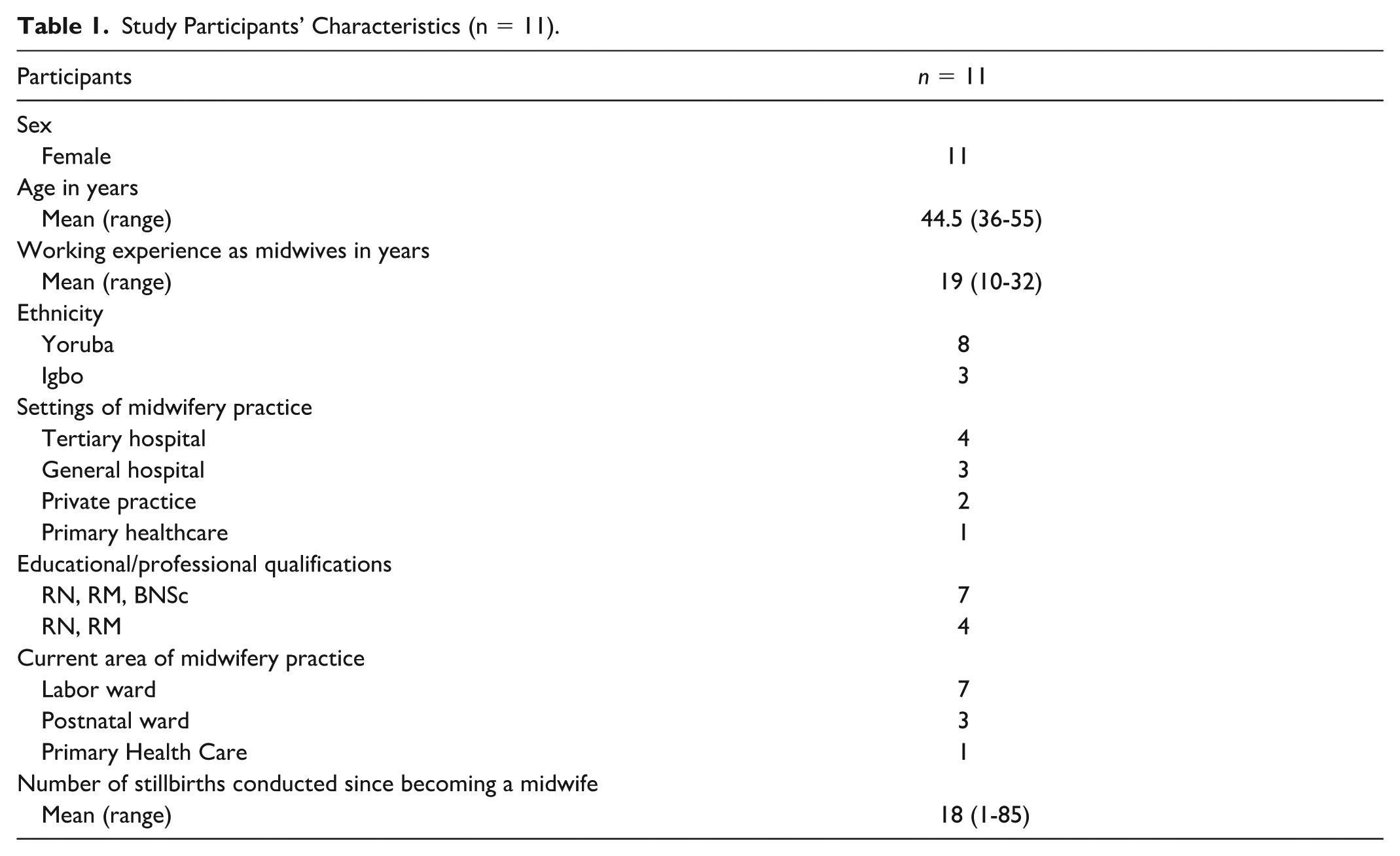
A total of 11 participants, all of whom were female, participated in the study. Their ages ranged from 36 to 55 years, with the average age being 44.5 years. The participants’ years of midwifery experience ranged from 10 to 32 years, with the average being 19 years. All the participants had the basic qualifications required to practice midwifery in Nigeria. These qualifications were registered nurse (RN) and registered midwife (RM) certifications. Participant characteristics are provided in Table 1.
Study Participants’ Characteristics (n = 11).
Findings
Two main themes were constructed from the data to describe the stillbirth bereavement care practices of Nigerian midwives. The first theme, “Family-first, woman later” describes a paternalistic approach to communicating the bad news of a stillbirth. The second theme, “Beliefs-driven care” details the influence of personal, cultural and institutional values in stillbirth bereavement practices.
Family First, Woman Later
The first theme identified in the data highlights the fact that the family was treated with greater consideration than the bereaved mother before, during and after disclosing the stillbirth. Regardless of work settings, all the participants played significant roles in breaking the news of stillbirth to parents, but there were variations in the roles played. In private practice, as well as primary and secondary health care settings, participants were responsible for delivering the diagnosis directly to parents. This is partly due to the shortage of medical doctors in these settings. However, in tertiary hospitals, physicians were more likely to deliver the diagnosis to parents. Despite doctors leading the diagnosis roles in tertiary settings, the interview data indicated that midwives still played a critical role. For example, midwives facilitated the diagnosis event by preparing a private space for the disclosure to take place, and they resumed care of the parents after the doctor delivered the diagnosis. However, regardless of whether a doctor or a midwife delivered the diagnosis, some striking characteristics and similarities were found to exist. First, the diagnosis routinely took place in the form of a family meeting, with midwives being the primary facilitators of the meeting. Involving the family in the process reflected an awareness of the seriousness of the moment of diagnosis. However, breaking the news in the presence of the family was considered also to have other purposes. Participants reported that midwives are often unsure how the mother of the stillborn baby will react to the diagnosis and as such, they often relied on the family to ensure that the mother’s reaction did not lead to self-harm for the woman.
The second characteristic relating to diagnosis of the stillbirth observed in the data was the order in which the diagnosis was delivered. Most of the participants reported that the diagnosis was first delivered to the husband or the family, and only then to the mother. For example, Grace said, “you first break the news to the relative and ask them not to inform the mother immediately.” Seun commented, “. . . we call the father in and break the news to him. Some would tell us not to tell the wife immediately.” This approach was influenced by two main factors. First, the participants reported that there was a practical reason for adopting this approach. In some Nigerian cultures, there are taboos around what the mother of the stillborn baby is allowed to do with the baby’s body. For example, in the Yoruba culture, it is taboo for a mother to bury her own child (Popoola et al., 2022). These taboos often do not apply to the baby’s father or other members of the family. As a result, the midwives interviewed reported choosing to discuss the next steps for dealing with the baby’s body with the family. This is highly significant in terms of the diagnosis process because at this stage many women lost the opportunity to ever see their babies. The second reason for the midwives’ practice in communicating with the family first was the need to deliver the diagnosis at the right moment. Midwives often expressed sympathy for the mother and worried about her emotional readiness to receive such devastating news. Therefore, they first informed the family as a way of gauging how the mother was to react. As an illustration, Kiki said,
. . . most times, we call the fathers in. They are the ones who know the psychological level of their wives. If the husband thinks his wife might not take it well, they sometimes tell us that we should not tell her that the baby had died.
While the participants believed that it was important to find the right time to disclose the stillbirth to the mother, some midwives explained that in some cases, the right time was not achieved until 3 days after the baby had died. In some instances, the family even advised midwives not to break the news to the mother at all, leaving it to the family to break the news at home. Participants reported that, not surprisingly, many women were already worried about their baby’s well-being due to the absence of baby cries and the frantic resuscitation efforts that started soon after birth. So even when the diagnosis had not been communicated to the mother, most women already suspected something was wrong with their baby, which intensified their inquiries about the baby. Participants reported that in situations where mothers inquired insistently about their babies, this eventually obliged the midwives to disclose the news, often in a hurried and unprepared way.
Beliefs-Driven Care
The second theme identified in the interview data highlights the fact that midwives’ bereavement care practices were driven in part by their own beliefs, as well as the beliefs prevailing in their practice environment. These beliefs influenced care in the following areas of bereavement care: memory-making, immediate care and the way forward.
Beliefs About Memory-Making
There were wide variations in memory-making practices among midwives. Some participants believed that women did not want to see their stillborn baby. Jumoke expressed this sentiment, by saying, “no, we don’t show them [mothers of stillborn babies] the baby, except on request. Most of them don’t want to see it.” Such statements echo the religious and cultural beliefs about stillbirth in Nigeria and as such, many of the participants did not readily provide mothers with the option of seeing the baby, except when mothers asked. The data indicated that these beliefs were held not only at the level of the individual midwife, but also at the institutional level. For example, some participants, such as Seun and Kiki, said, “opportunities for seeing the stillborn baby or taking photographs are not allowed in [their] facilities,” leaving memory-making to the discretion of the midwives. However, most of the participants reported that they honored the wishes of women who wanted to make memories with their baby.
On the contrary, two midwives working in teaching hospitals reported that their facilities expressly supported dressing the baby before showing it to the parents, and that memory-making in the form of photographs was actively encouraged. These midwives believed that such memory-making opportunities could bring relief to parents. For example, Adeola said,
we even dress the baby and show them to the parents. That’s what we do most times. Some people will request to take the picture of the baby . . . seeing the baby serves as a type of relief for them too.
The beliefs of midwives regarding the practice of memory-making are significant because those who do not believe in the value of memory-making are more likely to separate women from their stillborn babies and not offer them the opportunity to see their baby unless the woman asks explicitly.
Beliefs About Immediate Care
The interviews revealed that the midwives’ perceptions about what they believed to be the best care for mothers were driven not only by a biopsychosocial model of health, but also by religious and cultural beliefs prevalent in their practice settings. For example, when asked how they supported women after stillbirth, nearly all the participants invoked common religious statements such as telling mothers that “it is a test of faith.” Some also consoled mothers by invoking some popular cultural metaphors such as omi lo danu agbe o fo, which means “it is the water that spilled, the pot is not broken” implying that the mother still has her life to be grateful for. This suggested that despite being socialized into the Western model of health in their midwifery training, the participants still relied on the African concept of diseases and health, which views spiritual powers as important.
Because of the interconnection between the beliefs held by midwives—African beliefs about health and the Western medical model—the participants were able to offer more holistic care catering to women’s need for physical, mental, social and spiritual well-being. For example, many midwives recognized that stillbirth disclosure could trigger physical deterioration and as such, there was a concerted effort to regularly monitor women’s hemodynamic status to prevent and detect conditions such as postpartum eclampsia. This approach was captured by Jumoke, who said, “we make sure we are beside them to give moral support and ensure their blood pressure is not high, so we don’t have postpartum eclampsia.” The participants also recognized that stillbirth affects the whole family, prompting midwives to adopt a family-centered approach. This involved negotiating access for the family to participate in the mourning process, and ensuring that every woman had access to their support network. For example, Adeola said, “we encourage the patient’s husband to come in to give the patient emotional support. They need each other during that time.” Midwives also reported using a combination of strategies to facilitate women’s psychological well-being. For instance, mothers of stillborn babies were discharged to the gynecology ward as opposed to the labor ward, to prevent them from hearing the cries of newborn babies. For instance, Seun said, “we don’t take mothers to lying-in wards where there are babies. We take patients to the gynecology ward to prevent them from falling into depression.”
Beliefs About the Way Forward
The interview data revealed that there was a strong perception among all the participants that a rapid subsequent successful pregnancy was an antidote to the trauma of stillbirth. This perception was reinforced by the mothers’ own desire to understand what they could do to avert stillbirth in future pregnancies. As a result, midwives reported adopting “advice mode” and feeling eager to provide some form of hope or assurance to women. For example, Grace said, “You tell them it will not happen again.” Most of the advice given to women immediately after the disclosure was about preventing stillbirth in subsequent pregnancies. The issue with this approach is that it requires identifying a cause which means responsibility for the stillbirth is routinely attributed to mothers. For example, failing to take medication, missing antenatal classes and delaying presentation for childbirth were some of the pitfalls that mothers were told to avoid in subsequent pregnancies. The participants also believed that the sooner a woman can conceive after stillbirth, the better for her well-being. As such, participants focused on the need for mothers to be mentally, physically and emotionally ready. For example, Bolu said, “we advised her to take it [the stillborn baby] off her mind,” while Neye said mothers were told to “relax your mind, take your drugs, eat very well so that in another 6 months, another baby will come in and you will have your baby.” While it is unclear how often these predictions come to fruition, telling women to suppress their grief so that they can achieve a quicker conception is based on a common cultural belief in Nigeria that links memory-making in stillbirth with prolonged grief and delayed conception (Popoola et al., 2022).
Discussion
This study aimed to describe the stillbirth bereavement care practices of Nigerian midwives. Two key themes emerged from the data: “family first, woman later” and “beliefs-driven care.” The first theme highlights how the timing and manner in which midwives communicate stillbirth diagnoses are influenced by cultural expectations that prioritize the family of the mother of the stillborn baby. In the context of this study, midwives often reported delivering the diagnosis of stillbirth first to the husband or other family members rather than directly to the mother. Similar patterns have been observed in other studies in Nigeria (Kuforiji et al., 2024; Popoola et al., 2024), Kenya, and Uganda (Ayebare et al., 2021; Mills et al., 2021). The preference for a family-first communication approach to delivering bad news in African health care settings extends beyond stillbirth. For example, Schmauch et al. (2023) found that 37.2% of physicians in Mozambique initially shared patients’ transition to palliative care with the family before informing the patient. This suggests that in cultural contexts where a communal mindset is common, such as Sub-Saharan Africa, the family’s role in health care may go beyond supporting the patient to include decision-making.
The findings of this study confirm earlier research (Ayebare et al., 2021; Popoola et al., 2021) that indicates that cultural taboos prohibiting maternal involvement in burial rites influence the family-first communication approach adopted by health care providers in stillbirth care. The midwives in this study demonstrated strong alignment with the cultural realities of their practice settings, often deferring to family members to gauge the mother’s emotional readiness and to negotiate culturally appropriate responses to stillbirth bereavement. While this family-centered approach aligns with the cultural context in Nigeria (Popoola et al., 2022, 2024), relying on family members to assess the mother’s grief response may also indicate midwives’ lack of confidence in managing patient emotions when communicating a stillbirth diagnosis, as other studies have reported (Kuforiji et al., 2024; Popoola et al., 2024).
The second theme reveals how deeply rooted cultural beliefs, reinforced by institutional norms, influence midwives’ care practices related to memory-making, immediate support, and post-loss care. Some participants believed that mothers might not want to see their stillborn babies, leading to the withholding of this option unless explicitly requested, which aligns with findings from other studies (Kuforiji et al., 2024; Popoola et al., 2024). Conversely, some midwives working in tertiary hospitals experienced institutional support for memory-making and engaged in practices such as dressing the baby and taking photographs. These contrasting practices reflect the influence of individual belief systems and workplace norms, which either constrained or enabled parents’ engagement in memory-making.
Immediate care practices were also shaped by cultural beliefs. Many participants offered culturally resonant comforting language, such as religious affirmations or metaphors rooted in local traditions, to help grieving mothers make sense of their loss. For example, expressions such as “it is a test of faith” or “the water spilled, but the pot is unbroken” were used to comfort mothers and facilitate coping. These expressions reflect a worldview in which health and illness are intertwined with cultural and spiritual meanings. Despite receiving training in Western biomedical models to obtain their midwifery qualifications, the participants still drew on their African understandings of health and illness. This blending of belief systems allowed participants to provide holistic bereavement care that addressed mothers’ physical, emotional, social, and spiritual needs. Strategies such as transferring mothers to gynecology wards to avoid the cries of newborns and involving families in mourning rituals align with those reported in other research (Mills et al., 2023), illustrating how midwives adapt practices to protect mothers’ psychological well-being. However, personal beliefs and weak institutional guidelines around stillbirth bereavement care contribute to inconsistent support (Mills et al., 2023), with some mothers receiving more comprehensive care than others. These findings suggest a need for stronger and clearer institutional guidelines that respect cultural diversity while ensuring equitable access to memory-making and emotional support for all bereaved mothers.
Some limitations should be considered when interpreting these results. Although the sample size was adequate for a descriptive qualitative study (Doyle et al., 2020) and participants were recruited from various regulated midwifery practice settings, the stillbirth bereavement practices identified may not represent the full range of practices carried out by all midwives in Nigeria. A larger population of midwives would be needed to validate these findings.
Conclusion
The findings of this study underscore the importance of culturally sensitive and family-centered approaches in transcultural nursing, particularly in the context of stillbirth bereavement care. In many health care settings, midwives play a pivotal role in delivering the diagnosis of stillbirth, often in the absence of physicians. The approach used by midwives in this study when caring for women impacted by stillbirth demonstrates their understanding of cultural taboos and shows their respect for cultural norms. This implies that midwives practicing in transcultural settings need to be aware of cultural practices in their practice settings and be prepared to adjust their communication and care strategies accordingly. Incorporating Western medical models with African spiritual beliefs in the delivery of holistic care reflects a culturally embedded understanding of loss and recovery. Midwifery training programs need to prioritize culturally-grounded communication skills that balance family involvement with addressing the mother’s individual needs, along with cultural humility and flexibility when working across cultures.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.