
Abstract
Introduction:
The continued enforcement of traditional gender roles continues to oppress Arab women. This coupled with the taboo nature of discussing sexual health may contribute to unmet sexual health needs for Arabic women who have had a mastectomy. The aim of this article is to present qualitative findings of Arab women’s sexual health experiences following mastectomy.
Method:
This study was underpinned by social constructivism, feminist perspectives, and storytelling. A sample of 22 Arabic women, 28 to 60 years of age, who had a mastectomy were interviewed with data analyzed thematically.
Results:
Arabic women’s self-worth is inextricably linked with being a wife and mother. Participants experienced low self-esteem and feelings of inadequacy after the loss of their breast, which negatively affected their sexual health.
Discussion:
A woman’s journey navigating breast cancer and mastectomy within a patriarchal culture can be detrimental to not only their sexual health but also overall well-being.
Introduction
Breast cancer (BC) is the most common cancer among women globally and the leading cause of cancer-related mortality (Saadeh & Abdel-Razeq, 2022). While rates are rising worldwide, the Middle East and North Africa report particularly high rates and poorer outcomes (Mahdi et al., 2022). In Arabic women, the incidence of female cancers is higher than the global average, at 53% compared with 48% (Ferlay et al., 2021), though precise data is limited due to underdeveloped cancer registry infrastructure.
Arab women tend to be diagnosed with BC about a decade earlier than women in the United States and Europe, with a median age of 48 to 52 years, compared with just 23% of U.S. cases under 50 (Al-Shamsi et al., 2022). This may reflect both the region’s younger population and the underrepresentation of older women, who are less likely to undergo mammograms or seek care for breast symptoms. In addition, diagnoses often occur at later stages (Abu Awwad et al., 2020), increasing the likelihood of surgical treatment, including mastectomy.
The impact of breast cancer (BC) on women varies significantly, with both diagnosis and treatment affecting well-being, commonly resulting in altered sexual function, poor body image, loss of libido, and relationship difficulties (Arikan et al., 2020). Women who strongly associate body image with self-worth and femininity are at greater risk of poor psychosocial adjustment post-treatment (Oers & Schlebusch, 2020).
In the Arab world, while some women are working to reclaim their sexual identity (Tabahi, 2020), traditional gender roles and taboos surrounding sexual health continue to restrict open discussion and access to support (Liloia, 2022; Zahlan et al., 2020). As a result, many sexual health needs remain unmet. Despite this, there is limited research exploring the sexual health of Arab women after mastectomy. This study addresses that gap and aims to inform culturally appropriate interventions.
The study follows COREQ guidelines for qualitative research reporting.
Aim of the Study
The aim of this article is to present qualitative findings of the sexual health experiences of Arabic women after having a mastectomy due to breast cancer.
Method
This qualitative study was underpinned by social constructivism, feminist perspectives, and storytelling. Social constructivism provided a key lens to explore the sexual health experiences of Arabic women, as it effectively addresses cultural issues (Hazel, 2023). Feminist perspectives were essential in shaping data interpretation and guiding the study’s design, aiming to reduce power imbalances in a patriarchal context. Storytelling played a critical role, allowing women to first share their cancer diagnosis and treatment experiences before transitioning to discussions about sexual health, a topic that is often uncomfortable and taboo in Arabic cultures. Storytelling offers a distinctive way to order experiences and construct meaning, serving as a nuanced form of communication (Zarei et al., 2021) and is recognized as a valuable tool in cancer care (Hamilton, 2021).
Sampling and Recruitment
Sampling and recruitment involved a purposive sample of Arabic women over 18 years old who had survived at least 1-year post-mastectomy. This timeframe was chosen to ensure sufficient recovery from surgery and cancer treatments, including chemotherapy and radiotherapy. Participants were recruited through posts shared on social media platforms (Facebook, WhatsApp, and Twitter), BC support groups, and Arabic community groups.
Data Collection
Data collection involved semi-structured interviews with 22 Arabic women, conducted in English or Arabic. Interviews took place face-to-face, via phone, or through online video calls, using an interview guide that focused on their breast cancer journey and sexual health post-mastectomy. Interviews in Arabic were translated into English by a professional translator. Once transcribed verbatim, the transcriptions were cross-checked by the lead Arabic-speaking researcher, who listened to the audio recordings to ensure translation accuracy and made amendments as necessary.
Data sufficiency was determined when enough information was obtained to address the research aim, with recurring themes indicating saturation.
Data Analysis
Thematic analysis was guided by Braun and Clarke’s (2006, 2021) six-phase framework: (1) familiarization with the data, (2) generating initial codes, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) producing the report. The researchers immersed themselves in the data by repeatedly reading transcripts and listening to audio recordings. Initial codes were developed to capture meaningful features of the data and were then grouped into broader categories. These clusters were analyzed to identify and refine the overarching themes that shaped the findings.
Rigor
Trustworthiness was ensured by employing strategies to enhance credibility, transferability, dependability, and confirmability. Credibility was reinforced through prolonged participant engagement, a professional translator, and the lead researcher’s Arabic fluency. Detailed descriptions of the research context and participant characteristics supported transferability and confirmability. An audit trail was maintained, documenting data, decisions, and analysis (Johnson et al., 2020). Confirmability was achieved by documenting the process and using participant quotes to illustrate analysis.
Ethical Considerations
This study received full ethics approval from the Human Ethics Research Committee at Western Sydney University (HREC approval number H12998) and adhered to the National Health and Medical Research Council (NHMRC, 2007) guidelines throughout. To ensure participants’ autonomy and informed consent, the Participant Information Sheet and Consent Form were provided in both Arabic and English. Written consent was obtained prior to the interviews. Anonymity and confidentiality were strictly maintained throughout the research process.
Results
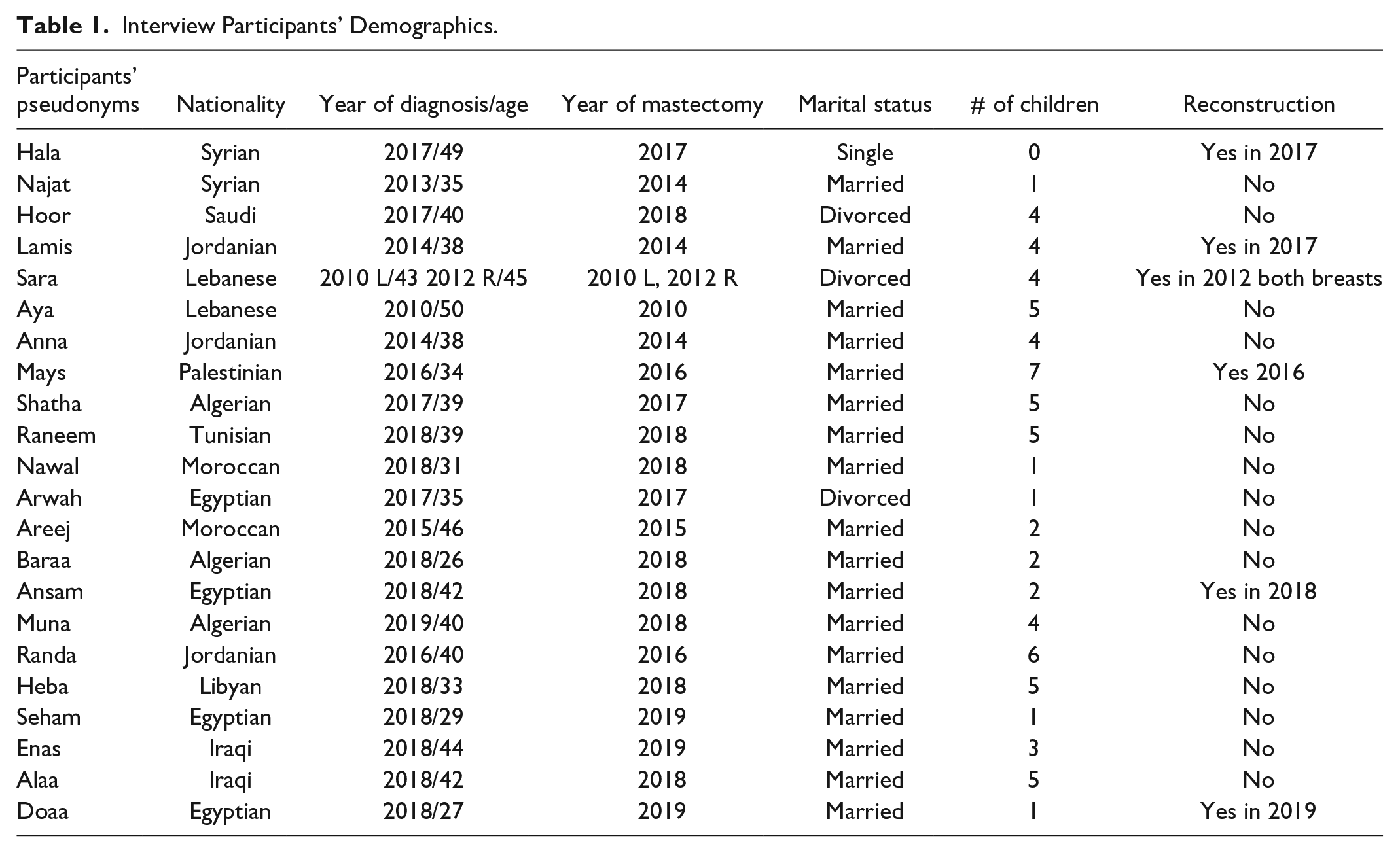
Twenty-two participants agreed to be interviewed, with interview durations ranging from 60 to 75 min. The demographic details of the participants are summarized in Table 1.
Interview Participants’ Demographics.
From the data, three main themes emerged regarding participants’ experiences of having a mastectomy: Losing My Femininity, Feeling Ashamed and Embarrassed, and Decreasing Sexual Relationships.
Losing My Femininity: “I Lost My Femininity in That Surgery”
Participants consistently expressed that physical appearance played a central role in their sense of femininity. Following mastectomy, many felt they had lost an essential part of their identity as women, which triggered deep emotional grief. Areej, for example, conveyed a profound sense of loss and incompleteness, fearing that society would forever see her as inadequate:
A painful feeling in my soul; a woman’s femininity is part of her being. It represents great pain when she loses part of her femininity, especially for a married woman who loves her husband, and her husband loves her. There is a disease in the soul that does not heal with time. (Areej)
Similarly, Enas also reported feeling as though she had lost her femininity, and experienced low self-esteem and perceived herself to be physically incomplete. She emphasized that the mastectomy scar served as a painful daily reminder of the diagnoses and surgery:
It [missing a breast] makes me feel like I am not a woman anymore . . . reminds me about the diagnosis and surgery pain and reminds me that I lost my femininity in that surgery. (Enas)
Participants in this study conveyed that they felt incomplete and imperfect after their mastectomies. This was exacerbated for some who also experienced hair loss because of medical treatments, as they considered their hair as a distinguishing feminine characteristic. Losing both their breast and their hair contributed to a loss of identity as a woman and negatively affected their confidence:
I just felt lacking self-confidence, as a woman, loss of her breast means I lost part of my identification as a woman . . . I have very nice hair, and I lost it as well, so my shape as a woman decreased, and you know, hair for Arab women is a part of their femininity. (Seham)
This statement illustrates the centrality of physical appearance to her sense of identity and self-worth, and how the physical changes associated with breast cancer treatment can deeply disrupt not only body image but also social and emotional well-being, particularly for younger women navigating cultural expectations around femininity and beauty.
Shatha revealed the mastectomy not only had an impact on her identity as a woman, but it also had a negative impact on her identity as a mother, especially as this meant she had to stop breastfeeding her youngest son:
I feel the difference, I lost an important part of my body, and an important part of my children, especially since my youngest son is only three years old [at the time of the interview]. (Shatha)
This theme underscores how the loss of a breast profoundly affected the women’s sense of identity, leaving many feeling less feminine and incomplete. The scarring and alterations in body shape resulting from the mastectomy contributed to feelings of embarrassment, shame, and a diminished connection to their bodies.
Feeling Ashamed and Embarrassed: “I Can’t Stand in Front of a Mirror and Look at Myself”
The women’s stories highlighted how breast cancer treatment, including mastectomy, scarring, and hair loss, deeply affected their body image. Many avoided looking at themselves in the mirror or showing their bodies to their partners. Enas shared her emotional struggle,
I can’t stand in front of a mirror and look at myself, just your question made me cry . . . of course, I was affected because I have a deficiency in my body. (Enas)
This sense of embarrassment carried over into their intimate relationships, with several participants describing how they concealed their bodies, fearing they would no longer be seen as attractive. Heba, for example, recalled how her husband had once admired her physical appearance. After her mastectomy, however, she feared he would no longer view her the same way. As a result, she began avoiding exposing her chest to him. She expressed a profound sense of loss, describing how her life had drastically changed after the surgery and how she mourned the life she once knew:
I feel [psychological] pain and feel that there is something I miss . . . my life with my husband and children is not the same as before; I became ashamed of myself and embarrassed to show my chest to my husband because I lost the breast and the wound shape. I did not show my chest to him, not even once after the operation. (Heba)
Some participants’ stories revealed that their partners perpetuated their embarrassment. Sara conveyed that her partner was proud of her appearance and liked to show her off publicly. She divulged that after losing her breast and her hair, she feared that her partner would no longer see her as physically and sexually attractive and would reject her. Sara shared one such instance in the following excerpt:
One day I drove him to work, and I had lost my hair and was wearing a scarf. He did not like it and told me to stop him at the corner, and I said are you shy [embarrassed] of me. He said yes, and that hurt me. (Sara)
Anna’s experience stood in contrast to many others, as her husband’s reassurance made her feel beautiful despite the physical changes. While most participants concealed their scars, Anna felt confident revealing hers, supported by her husband’s calm acceptance:
I was ashamed of the shape of my chest, but my husband insisted that I show the chest area, and then it became normal because I have been ashamed to expose my breast to him, but he reassured me and told me that I am still attractive. (Anna)
Despite the expectation that reconstructive surgery would restore the appearance of their breasts, some participants were dissatisfied with the results. Sara, for example, shared her struggle with accepting her reconstructed body, yet over time, she began to find peace with her new appearance:
It took me a very long time before I could stand with my cuts. It was not very pleasant . . . the reconstructive can never make it again as it used to be. You will never look again as you used to be . . ., but this feeling left me after six years. So, the trauma is over. It did not directly leave me, but I could see a living girl. (Sara)
This theme highlights the deep shame and embarrassment participants experienced after their mastectomies. Many women concealed their bodies, even from their partners, and felt further isolated when their partners reacted with discomfort or avoidance. These responses often strained sexual relationships and heightened emotional distress.
Deteriorating Sexual Relationships
Participants shared that their sexual quality of life significantly declined following their mastectomies. Many viewed their breasts as central to their sexuality. Ansam, for example, expressed that the loss of her breast directly affected her self-esteem, leading to a decrease in sexual desire. She also noted the exacerbating effects of hormonal therapy:
The effect was psychological rather than physical. I had a feeling of lack of sexual desire . . . Firstly, because I lose my breast and that affects my confidence, and secondly because of hormonal therapy side effects. (Ansam)
Areej compared her sex life before and after the mastectomy, describing a sense of distance from her husband. After the surgery, she felt as if her breasts no longer mattered to him, leading to a loss of intimacy:
No, my husband did not see my chest after the operation, not even one time, and he did not ask for it or even give a hint about it as if we dispensed with that area even though it excited him and was interested in it, but after the operation as if it did not exist . . . we dispensed with foreplay before sexual intercourse, as touching the breasts, but now that sexual intercourse is fast, and I feel its loss of intimacy during it because I did not reveal them completely in front of my husband. After all, he is a polite man. What will he see? It has become distorted and hindered. (Areej)
For many participants, the physical and emotional toll of cancer treatment, including feeling weak or unattractive, led to disinterest in sexual intimacy. For example, Heba shared that she could not engage in sexual intimacy due to her negative feelings about her appearance, particularly the loss of her hair and breast:
My sexual desire decreased, and I did not like sexual relations . . . of course, it never affected my husband, but I was affected a lot, so I can no longer tolerate sexual relations. (Heba)
In some cases, partners’ reactions worsened participants’ sense of embarrassment, deepening the lack of sexual desire. Shatha, for example, explained how her husband’s avoidance of her surgical site made her feel even more isolated:
Our relationship was affected so much. It has been more than a year and a half since the operation took place, and he did not see the place of the operation yet . . . I never refused the relationship, but I did not feel the desire for my husband to make any sexual relationship with me. I bought a lot of clothes suitable for this issue, and I was always ready for the relationship. But my husband’s needs for the relationship were decreased, and I am afraid to ask him about his change, if his answer hurts my feelings. (Shatha)
For many participants, regardless of their husbands’ understanding or sympathy toward the physical and emotional impacts of breast cancer, they continued to engage in sexual relations out of a sense of duty. They felt it was necessary to maintain their marriage and avoid the risk of their husband’s seeking separation or divorce, which is permitted in Arabic culture. As a result, some women engaged in sexual intercourse even when they lacked desire:
I was bearing the feeling of pain in order not to spoil the relationship between me and my husband . . . I was telling him, and he was asking not to have sexual intercourse and that will not affect our relationship, but I refused because he has no fault.
This theme underscores how breast cancer and its treatments led to a significant decline in sexual desire. Participants’ deteriorating sexual health was influenced by various factors, including the physical side effects of medications, body image perceptions, and concerns about how they appeared to their partners.
Discussion
The internalized emotional and cognitive responses of participants in this study can be understood through a critical feminist and social constructivist lens, which examines how societal structures shape individual experiences. In patriarchal societies like the Arab world, the female breast holds symbolic value, linked to fertility, motherhood, nurturing, and sexual appeal (Drew, 2020; Tullio-Pow et al., 2020). For participants, the loss of a breast due to mastectomy was not just a physical change but a profound rupture in identity, representing a loss of femininity, attractiveness, and self-worth (Sukartini & Permata Sari, 2021).
These internalized meanings are reinforced by patriarchal beauty standards that prioritize physical appearance and equate a woman’s value with sexual desirability, often validated through male approval (Rudman & Glick, 2021; Sledge, 2023). In this context, participants expressed deep feelings of shame, self-consciousness, and inadequacy. Many avoided mirrors and refrained from revealing their bodies to their partners, fearing they were no longer sexually or emotionally desirable. This internalized objectification links a woman’s self-esteem to physical conformity, leaving those who deviate, such as post-mastectomy patients, feeling alienated, incomplete, and less feminine (Lalhriatpuii, 2022).
Participants described how visible changes to their bodies, such as scars, breast asymmetry, and hair loss, negatively affected their sexual identity and confidence. This aligns with previous research showing that women who highly value body image are more vulnerable to psychosocial distress after breast cancer treatment (Oers & Schlebusch, 2020). In Arab society, where femininity is narrowly defined, many women reported feeling incomplete, leading to a loss of self-confidence and a perceived inability to satisfy their partners. These findings support Maleki et al. (2021), who noted that women often see themselves as sexually inadequate post-mastectomy, exacerbating emotional distress.
The responses of intimate partners also played a critical role in shaping women’s post-mastectomy self-image. Participants with supportive spouses reported greater emotional security and openness to intimacy. Partner affirmations helped ease body image concerns and promote healing, aligning with research showing that validation enhances resilience (Hasan et al., 2023; Sledge, 2023). Conversely, when partners were distant, women experienced emotional withdrawal and increased dissatisfaction.
Participants reported a decline in sexual desire and function due to both physical and emotional changes. Hormonal therapies caused vaginal dryness, fatigue, and discomfort, making sex painful (Mikić, 2022). Emotional distress, such as grief and loss of sexual identity, was equally impactful. Many mourned their pre-cancer sexual selves and expressed disappointment that reconstruction did not restore sensation or emotional wholeness (Grande, 2022; Lindau et al., 2023).
Participants’ experiences were shaped by patriarchal norms around sexuality and marriage. In Arab culture, women’s sexual roles are often defined by duty rather than mutual pleasure (Alinejad Mofrad et al., 2021; Durães Rocha et al., 2016). Many engaged in sex out of obligation, fearing divorce or social stigma (Ghabra, 2015). As a result, women’s sexual well-being was often sacrificed for marital preservation and spousal satisfaction, reinforcing gender imbalances. This dynamic has serious consequences, as sex without desire can lead to vaginal injury, infection, and psychological distress, including depression and anxiety (Gallagher et al., 2010; Nair et al., 2018). These findings underscore the need for culturally sensitive interventions that prioritize women’s bodily autonomy and emotional well-being.
The cultural taboo surrounding discussions of sex further compounded these challenges, limiting support and healing. Research links this silence to increased mental health issues and lower sexual satisfaction (Paraskeva et al., 2019). These findings emphasize the need for interventions that promote sexual autonomy, open communication, and gender-aware health care models that involve partners and prioritize inclusive sexual health education.
Strengths and Limitations
A key strength of this study was the use of a storytelling approach. Within the context of patriarchal Arabic culture, this method provided a safe space for women to share their breast cancer (BC) experiences, empowering them to voice their needs in health care decision-making. For many, it was the first time they had openly discussed their struggles, making the process cathartic (Alomair et al., 2021).
However, a limitation lies in the study’s purely qualitative design, which may introduce subjectivity. While qualitative research yields rich, in-depth insights, it lacks the statistical Generalizability of quantitative methods, which can provide broader, population-level conclusions when applied with rigor (Denscombe, 2017).
Conclusion
This study highlights the profound impact of breast cancer and mastectomy on women’s sexual health and overall well-being within a patriarchal cultural context. The loss of a breast was often experienced as a loss of femininity, leading to diminished self-confidence and emotional distress. Many participants felt obligated to engage in sexual activity despite pain or lack of desire, fearing harm to their relationships.
Such dynamics, rooted in cultural expectations, pose significant health risks, including reduced quality of life and increased emotional strain. These findings underscore the need for early identification of sexual health concerns and the development of culturally sensitive, gender-responsive health care interventions to support women’s recovery and well-being.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.