
Abstract
Introduction
Indigenous Peoples living in remote regions of northern Quebec, Canada, experience significant disparities in adverse birth outcomes compared with non-Indigenous populations, including premature birth, stillbirth, and neonatal mortality (Luo et al., 2012; Simonet et al., 2010; Simonet et al., 2012). These disparities are exacerbated by longstanding inequities in social determinants of health for Indigenous Peoples including lack of housing, high unemployment rates, lower educational attainment, food insecurity, and limited local health services (Inuit Tapiriit Kanatami, 2015; Loppie Reading & Wien, 2009). Without sufficient access to local birthing services, Indigenous Peoples in northern Quebec are frequently transferred to southern urban hospitals for childbirth, a practice known as maternal evacuation. A recent scoping review on Indigenous maternal evacuation in Canada outlines negative health and social impacts on Indigenous families and communities (Silver et al., 2022). Maternal evacuation can cause significant distress for pregnant women and their families (Kornelsen & Grzybowski, 2005; Vang et al., 2018), often related to separation from their families and culturally incongruent and discriminatory care in southern hospitals (Archibald et al., 1996; Brown et al., 2011; Guse, 1982; Struthers et al., 2014). In northern Quebec, maternal evacuation affects Inuit and Cree of Eeyou Istchee, who make up the largest proportion of the region’s inhabitants (see Figure 1). This article describes the design, implementation, and preliminary evaluation of cultural safety health interventions by Inuit and Cree of Eeyou Istchee stakeholders and their southern non-Indigenous perinatal service providers to support families in the context of evacuation.
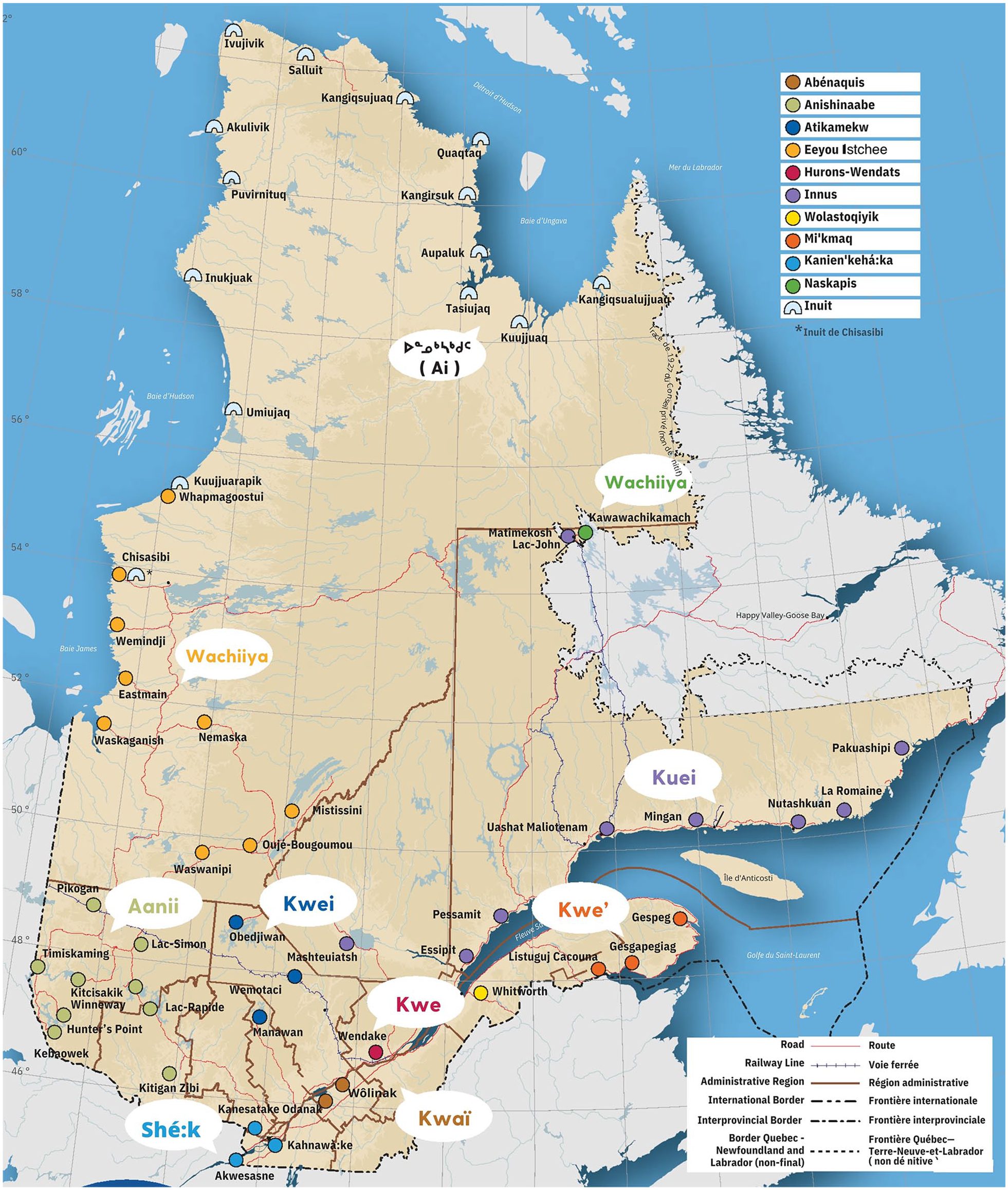
Map of Inuit and Cree Nation of Eeyou-Istchee communities. Printed with permission from Centre universitaire de santé McGill et Secrétariat aux relations avec les Premières Nations et les Inuit, avril 2023, Montréal, Québec, Canada.
Recognized by the Constitution Act (1982) as Indigenous Peoples of Canada, Inuit and Cree of Eeyou Istchee receive publicly funded universal health care coverage through a patchwork of federal, provincial, and territorial health policies (Lavoie, 2013). Nunavik, the Inuit territory in Northern Quebec, has a population of approximately 13,000 inhabitants spread across 14 communities solely accessible by air and sea (Statistics Canada, 2019). The Nunavik Regional Health Board (NRHB) provides local health services free of charge, along with transportation, food, and accommodation for individuals needing out-of-region medical treatment. Pregnant Inuit on the Hudson coast are served by the Inuulitsivik Health Centre, a local Level I hospital in Puvirnituq, and three Inuit maternities (midwifery-run birthing centers) in Salluit, Puvirnituq, and Inukjuak (Van Wagner et al., 2012). The maternities oversee care for people with medically low risk or uncomplicated pregnancies. Inuit living in communities on the Ungava coast travel several hundreds of kilometers by plane to Kuujjuaq for childbirth at the Tulattavik Ungava Health Centre, a Level I hospital and maternity. According to the most recent NRHB report, Inuit maternal evacuation rates range from 14–30% (ZM Vang, personal communication, April 2019).
In partnership with the Government of Quebec, the Cree Board of Health and Social Services of James Bay (CBHSSJB) provides publicly funded health care to the nine communities of the Cree Nation of Eeyou Istchee (hereafter Cree), accounting for 18,000 people (Grand Council of the Crees, 2023). Midwifery services are available in Chisasibi, Wemindji, and Whapmagoostui along with a midwifery-run birthing center in Chisasibi. The CBHSSJB runs a Level I hospital in Chisasibi and liaises with a Level I hospital in Chibougamau and a level II center in Val d’Or (K. Wou, personal communication December 2023). Recent anecdotal reports suggest that most pregnant Cree must leave their communities for birth (M. Corman-François, personal communication January 2024).
Inuit and Cree requiring specialized obstetric care are routinely transferred hundreds of kilometers to a university-affiliated tertiary care center in southern Quebec (hereafter referred to as ‘the hospital’). Approximately 400 such transfers occur every year, accounting for 10% of all hospital births (J. Pepin, personal communication, April 2022). Evacuees are housed in publicly funded local accommodation facilities run by their respective regional health authorities to await childbirth. Recent research on the experiences of Inuit and Cree cites numerous stressors for families and advocates for culturally safer and adapted services in the context of maternal evacuation (Vang et al., 2018).
Evidence indicates that Inuit and Cree face several important stressors in the context of maternal evacuation. Primary among them is having limited family support when transferred to southern Quebec for childbirth. Long distances, unpredictable weather, limited government funding for accompanying family members, high travel costs, and evacuations lasting weeks to months are among the many barriers to family presence and support (Silver et al., 2023; Vang et al., 2018). Standard hospital visitation policies (maximum two persons) are a further obstacle to family presence and the practice of Inuit and Cree perinatal traditions (Silver et al., 2022; Silver et al., 2023). This contrasts sharply with the collective experience of childbirth in the communities, where family and community members play important social roles in intergenerational transmission of traditional knowledges and rituals during childbirth (Silver et al., 2022).
Research suggests that evacuee Indigenous families have limited access to traditional country foods in southern Quebec, frequently relying on fast food or institutional food of poor quality (Silver et al., 2023). Central to Inuit and Cree health, country foods such as caribou, arctic char, and berries are regarded as especially important for perinatal wellness (Silver et al., 2022; Silver et al., 2023). A limited supply of country foods is available at the local accommodation centers, usually transported to Montreal by the families themselves, or other community members traveling to Montreal for medical care. Larger quantities of traditional country foods are donated by northern Indigenous organizations depending on seasonal hunting and harvests.
Considering this context, a hospital-based interdisciplinary working group of perinatal nurses and physicians (referred to as “we” in the remaining pages) set out to enhance the cultural safety of health services for Inuit and Cree evacuee families. This article describes our process of co-designing culturally safe interventions over a year-long project with Inuit and Cree stakeholders from relationship building through to implementation and preliminary evaluation of the interventions.
Methods
Theoretical Framework
Developed by Maori nurses in New Zealand, cultural safety seeks to address power dynamics and cultural considerations embedded in encounters between medical providers and those they care for (Papps & Ramsden, 1996). Culturally safe care for Indigenous Peoples must also take into consideration historical and sociopolitical realities and address the adverse impacts that colonialism and intergenerational trauma have on Indigenous People’s health (Brascoupé & Waters, 2009). Two theoretical frameworks, Andersson’s (2018) participatory research (PR) framework and Joyce’s Principle, guided our project to enhance cultural safety.
Moving beyond participation in research, Andersson’s framework conceptualizes PR as “systematic co-creation of new knowledge by equitable partnerships between researchers and those affected by the issue under study, or those who will benefit from or act on its results” (Andersson 2018, p. 155). It proposes stakeholder engagement in every step of the research and increases their ownership and active use of evidence and innovation. The resulting collaboration aligns fact-finding with the context and needs of stakeholders, ideally initiating solutions as part of the engaged research. The framework offers concrete guidance for the operationalization of Joyce’s Principle. Joyce’s Principle was written in memory of Joyce Echaquan, an Atikamekw First Nation woman who died in 2020 in a hospital in southern Quebec due to medical negligence and racism (Kirkup & Ha, 2020). The Principle outlines numerous steps healthcare providers and institutions must undertake to ensure culturally safe health services. First among them is the active participation of Indigenous Peoples in designing services that are grounded in their traditional knowledge systems (Council of the Atikamekw, 2020). Together with Andersson’s participatory framework, Joyce’s Principle informed the design, implementation, and evaluation of culturally safe interventions in the context of Indigenous maternal evacuation for childbirth. Our project received research ethics approval from McGill University Faculty of Medicine IRB, the Research Institute of the McGill University Health Centre REB, and Inuulitsivik Health Centre.
Project Design & Participants
The work described in this article is the second phase of a long-term participatory study on culturally safe Indigenous birth. In Phase 1 of the long-term study, the lead author (HS) and an Inuk researcher (ST) engaged Inuit evacuees and their non-Indigenous southern medical providers in visioning culturally safe birth in the context of evacuation using participatory fuzzy cognitive mapping (FCM). A visual display of people’s causal knowledge on a subject (see Andersson & Silver, 2019 for a detailed description of the method), FCM generated 17 recommendations for supporting culturally safe birth, reported separately (Silver et al., 2023).
After member-checking these recommendations with participants, HS drafted a plain language report summarizing participant visions and priority recommendations for culturally safe birth. A working group member with experience in Cree communities (MCF) then validated the relevance of the recommendations through semi-structured interviews with Cree families and their perinatal care providers. In total, we consulted 14 Inuit and Cree participants and 26 Indigenous and non-Indigenous perinatal providers (physicians, nurses, midwives, and community health workers) between April 2021 and March 2022. Purposive sampling in partnership with local medical providers facilitated our recruitment of Indigenous participants.
In Phase 2, we selected four areas of intervention to support culturally safe birth in the context of Indigenous maternal evacuation. These interventions were based on the highest-priority recommendations identified by both Indigenous families and their medical providers through the FCM in Phase 1. All interventions took place at the hospital. They included: (1) developing and testing an Indigenous-led perinatal cultural safety training program for hospital staff, (2) increasing family presence and support in childbirth, (3) facilitating access to traditional country foods, and (4) promoting Inuit and Cree perinatal traditions in the context of maternal evacuation. Following Joyce’s Principle, we recruited and funded two patient partners, Inuk mother, Cree mother, perinatal worker with lived experience of maternal evacuation, to collaborate on the project along with Inuit and Cree medical providers. Researchers from the participatory research lab at McGill University (CIET-PRAM), based in Montreal, Quebec, provided methodological support for developing our impact assessment tools described below.
Outcome Measures & Analysis
Staff Questionnaire
To assess the impact of the Indigenous-led perinatal cultural safety training program on medical providers, we used a seven-item online self-administered pre- and post-intervention questionnaire (Appendix 1). The questionnaire used a modified theory of planned behavior, which assumes that knowledge changes behavior through a results chain, or series of intermediate steps (Andersson et al., 2005). This theory expands on the widely known knowledge-attitude-practice model (KAP) (Bentler & Speckart, 1979) to explain how people’s knowledge shapes their actions. Specifically, the questionnaire measured changes in medical providers’
An independent researcher not associated with the hospital working group calculated probabilistic transitive closure using CIETmap to determine the net influence of each item in the CASCADA results chain according to direct influences and indirect “walks” (Andersson et al., 2017). We converted pre- and post-questionnaire scores into odds ratios, normalized on the interval [-1,1] (Andersson et al., 2017; Andersson et al., 2005). We calculated the net probabilistic transitive closure—the cumulative probability of given knowledge resulting in the anticipated action—by summing the weights of the influences across all arcs in the CASCADA chain in the range [-6,6].
Family Questionnaire
As cultural safety is not measured in the extent of a provider’s knowledge or skill, but by a patient’s feeling of safety and respect in a clinical encounter (Kirmayer, 2012), Inuit and Cree family perspectives and perceptions are essential indicators for impact assessment. A family experience questionnaire, co-designed with our patient partners and CIET-PRAM researchers, will capture Inuit and Cree families’ perceptions of the interventions (Appendix 2). Guided by our patient partners, we adapted the standard hospital survey for patient satisfaction to capture families’ experiences of the four interventions. Our approach was an iterative one, with a preliminary set of questions reviewed and modified by our patient partners. Offered electronically via tablet, the questionnaire will be administered by a member of the working group who is not involved in direct patient care. A series of close-ended questions assess whether the planned interventions are implemented by staff. Likert-type and open-ended questions investigate the degree to which patients and their families feel respected and safe during their hospital stay. On the advice of our patient partners, future storytelling and sharing circle activities will supplement the questionnaire data. Lastly, the data from families and staff will be regularly collected and reviewed by the working group over 12 months following the launch of our interventions. The findings will facilitate the adjustment of our interventions on an as-needed basis, which we will report on separately in a future publication.
Results
Informed by participatory principles of stakeholder-led health service redesign, our project results describe both the process and outcomes of the cultural safety interventions (Andersson, 2018). In the following section, we illustrate the implementation and partial assessment of the four interventions to support culturally safe birth for Cree and Inuit evacuees.
Intervention 1: Developing and Testing an Indigenous-Led Cultural Safety Training Program for Perinatal Staff
Inuit, Cree, and non-Indigenous midwives led the development of the perinatal cultural safety training program for hospital staff. Trust and mutual respect were core values. Beginning with online introductory meetings, the working group and Indigenous stakeholders got to know one another on personal and professional levels. Mutually agreed upon learning objectives lay the foundation for the training program, followed by regular meetings for program development. Below we describe the implementation and partial assessment of the training program.
In online presentations and in-person workshops, the training program addressed concepts of cultural safety, with specific implications and practical applications of culturally safe perinatal care for Inuit and Cree. Staff attended two online Grand Rounds presentations: (1) an introductory presentation on Inuit health, the realities of northern living and the current healthcare system in Nunavik led by the Nunavik liaison midwife, and (2) a presentation on Informed Choice versus Informed Consent by an Cree midwife and a patient partner. Next, a weeklong series of in-person workshops with Inuit midwives strengthened staff knowledge and proficiency in caring for Inuit evacuee families. The workshops began with an overview of Inuit history and culture (including intergenerational trauma and colonialism, and contemporary realities and challenges facing Inuit), followed by a deeper examination of Inuit perinatal traditions and methods of supporting families in the context of evacuation. Many perinatal staff and all nursing staff of the birth center attended, along with staff from the local Inuit accommodation center.
Figure 2 shows the impact of the training in transitive closure of CASCADA from pre- and post-intervention staff questionnaires, with green arcs representing positive influences and red arcs negative influences of each intermediate outcome on all others. Thicker lines indicate stronger influences. The cumulative net influence across the CASCADA sequence increased from 4.70 to 5.58 out of a possible maximum value of 6, showing a post-intervention increased influence of the Knowledge on Action. Pre-intervention, there was a negative cumulative influence of Subjective norms on Agency (-0.21): respondents did not feel able to act on what they knew about cultural safety. After the intervention, the results chain changed notably at the point of Agency, indicating this was a key impact of the intervention. (See Appendix 2 for complete CASCADA cumulative weights). A 1-hour video presentation recorded by the midwives captured the knowledge for future staff.
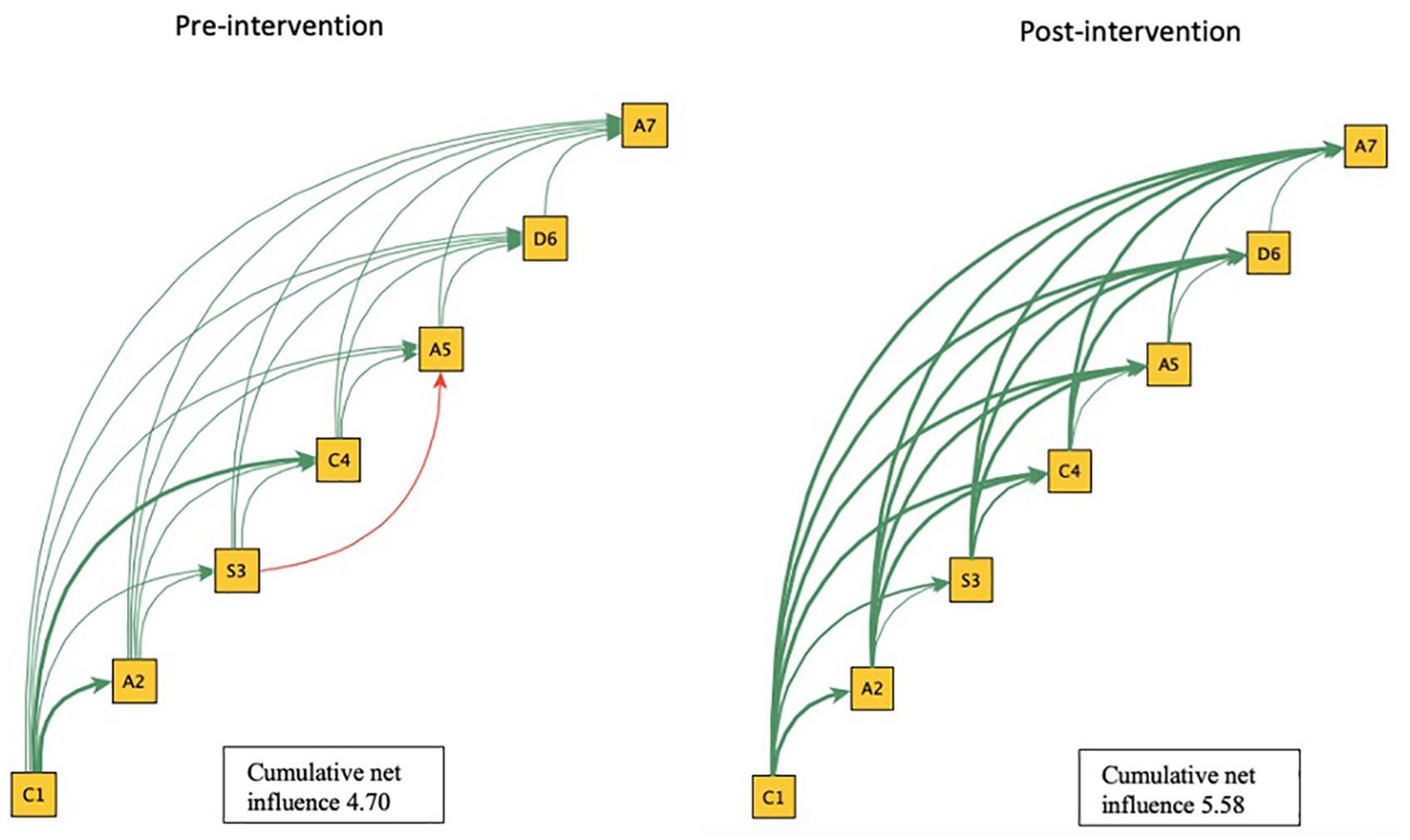
Probabilistic transitive closure of the CASCADA results chain pre-and post-intervention.
Intervention 2: Increasing Family Presence and Support During Childbirth
Inuit and Cree have limited family support when transferred to southern Quebec for childbirth. Cree and Inuit midwives guided the development of an expanded visitor policy in the birthing center, allowing up to four visitors (previously limited to two persons). Since our objective was to be a family-centered birth center, we strove for a culturally transformative approach, as opposed to mere policy change. This required a focus on staff skill-building in communicating with families, as well as their knowledge of Inuit and Cree communities.
To facilitate the implementation of the visitor policy, an information booklet for staff outlined basic information about Inuit and Cree communities, their perinatal customs, and basic Cree and Inuktitut phrases. Along with a detailed explanation of the new visitor policy, a communication guide provided prompts for staff to navigate common challenging situations such as medical emergencies, invasive clinical procedures, and safety measures. In collaboration with our patient partners, we developed a companion booklet for evacuee families outlining the visitor policy including information about the hospital units, designated family spaces, and infection prevention measures, as well as a photo catalogue of cultural items available to families for decorating their rooms during their admission (see details below).
Intervention 3: Access to Traditional Country Foods
As explained previously, lack of access to traditional or country foods is a significant concern for Inuit and Cree evacuees. To support family access at the hospital, we installed a country food fridge and freezer on the postpartum unit to facilitate storage and onsite preparation. The family informational booklet welcomes families to a seasonal supply of traditional broths and stews, Chisasibi and Labrador teas, and bannock on order from the hospital cafeteria. In partnership with the Inuit and Cree accommodation centers and a local Inuit organization, we established a service corridor for country food transportation to the hospital to facilitate continued access for families.
Intervention 4: Supporting Inuit and Cree Perinatal Traditions
Access to Inuit and Cree perinatal traditions and cultural items rounded off our interventions for culturally safer care at the hospital. Our patient partners led the selection of a series of artworks by Inuit and Cree artists including paintings, prints, and seal pelts for families to decorate their hospital rooms. Essential oil diffusers and smudging sprays provide families with familiar scents from home during labor, while beading kits offer respite for those experiencing lengthy hospital stays. Explanations of key perinatal items such as the Inuit Amauti and Immuti and the Cree Waaspsuyan (traditional infant wraps and carriers) were included in the staff informational booklet. A detailed guide for facilitating patients’ access to their placenta was included at the recommendation of our patient partners, along with information on culturally adapted mental health services and Inuktitut and Cree interpreter services. The booklet also contains resources for families on accessing complementary care within the hospital (such as spiritual care services), at their respective health authorities, and in the greater Montreal area.
Discussion
The purpose of this project was to implement co-designed cultural safety interventions in the context of maternal evacuation in collaboration with Inuit and Cree stakeholders. The group implemented four cultural safety interventions and a third-party evaluation examined the impact of the Indigenous-led perinatal cultural safety training. The ongoing project will evaluate Cree and Inuit satisfaction with the interventions and their impact on maternal-infant health outcomes and publish those results separately. In the meantime, anecdotal evidence from debriefings with hospital staff suggest rapid uptake and positive impacts of the other three interventions.
The independent impact assessment of the Inuit midwifery workshop showed an important increase in participant sense of agency after the training; this released the pre-training “blockage” in the CASCADA at Agency, the notion the respondent had the ability to change behavior, informing our reflection on the nature of the training and how it affects participants. The increased cumulative positive influence across the CASCADA partial order indicates a positive effect of training on the influence of Knowledge about cultural safety on Actions that derive from it. As the National Collaborating Centre for Aboriginal Health points out, cultural safety training for medical providers does not necessarily result in culturally safe care (Baba, 2013). Assessing a training’s impact on providers’ knowledge and actions, however, is a first critical step. Our results reinforce the work of Pimentel et al. (2021), which found CASCADA to be a useful and robust tool for assessing the impact of cultural safety educational programs on medical providers’ knowledge and actions.
As critics of cultural safety point out, there is limited evidence of the concrete application of cultural safety interventions in health care (Yeung, 2016). Our project offers an example of operationalizing co-designed cultural safety interventions in the context of Indigenous maternal evacuation to a tertiary hospital. Furthermore, by continuously engaging Indigenous stakeholders over the course of the project, we believe our work offers a concrete and reproducible example of implementing Joyce’s Principle in an acute care setting. Our Indigenous-led perinatal cultural safety training outlines the steps for creating a clinically tailored curriculum of cultural safety training based on mutually identified knowledge needs. It is the first step in our response to Joyce’s Principle’s call for “the recognition and respect of Indigenous people’s traditional and living knowledge in all aspects of health” (Council of the Atikamekw, 2020, p. 10). Our family-centered visitor policy offers a roadmap for maximizing family presence and support in other acute-care settings. This, along with facilitated access to country foods and traditional perinatal practices are some of the concrete ways in which we aim to secure the rights of Inuit and Cree to “enjoy the best possible physical, mental, emotional and spiritual health,” as outlined in Joyce’s Principle (Council of the Atikamekw, 2020, p. 10).
Limitations
We recognize that our work, motivated by service improvement rather than research objectives, has several important limitations. Although our consultations with Inuit and Cree families and providers took place over many months, we understand the emerging information as only a snapshot of how those families saw their needs at that point in time. Informative and motivating as they were, the small number of families we were able to engage limits generalizability to all Inuit of Nunavik and Cree of Eeyou-Istchee. We are currently addressing this limitation through continued assessment of Indigenous family experiences and our ongoing modification of cultural safety interventions on an as-needed basis. Finally, our work focuses on Inuit and Cree of Eeyou-Istchee perspectives and does not offer comparisons with other rural and remote Indigenous communities who experience maternal evacuation. While our project is specific in its scope and context, our process of relationship building with Indigenous communities and patient partners has wider relevance across healthcare settings seeking to enhance cultural safety and implement Joyce’s Principle.
Conclusion
Indigenous maternal evacuation for childbirth in Northern Quebec is associated with numerous stressors and adverse outcomes. Culturally safe and adapted services are critical to supporting Indigenous families and reducing the harms associated with evacuation. A participatory research framework guided by Joyce’s Principle has the potential to enhance the cultural safety of health services in the context of Indigenous childbirth evacuation through the engagement of Indigenous stakeholders in co-design and implementation of interventions.
Supplemental Material
sj-docx-1-tcn-10.1177_10436596241292042 – Supplemental material for Co-designing Culturally Safe Indigenous Birth in High-Risk Obstetrics: Implementing Joyce’s Principle with Inuit and Cree Families and Their Medical Providers
Supplemental material, sj-docx-1-tcn-10.1177_10436596241292042 for Co-designing Culturally Safe Indigenous Birth in High-Risk Obstetrics: Implementing Joyce’s Principle with Inuit and Cree Families and Their Medical Providers by Hilah Silver, Mischa Corman-François, Sophia Kapellas, Paasa Lemire, Jennifer Pepin, Ivan Sarmiento and Neil Andersson in Journal of Transcultural Nursing
Footnotes
Acknowledgements
We are deeply grateful to our collaborators for their guidance, wisdom, and dedication to the communities they serve: Elizabeth Bobbish, Jasmine Chatelaine, Brenda Epoo, Dr. Darlene Kitty, Samantha Leclerc, Aileen Moorhouse, Margaret Tarqiapik Ningiuruvik, Leah Walkty, and Louisa Whiteley Tukkiapik. Nakurmiik! Miigwetch! Sophie Tukulak collaborated with HS to facilitate cognitive mapping sessions. Andrés Rojas Cárdenas contributed to the implementation of the pre- and post-training staff questionnaires.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Herta Vodstrcil estate and the MUHC Foundation through the MUHC Innovation in Nursing Award and a Canadian Institutes of Health Research Project Grant (no. 426071).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.