
Abstract
Introduction:
Since 2009, nurses have relocated to Japan from Indonesia, the Philippines, and Vietnam under the auspices of the Economic Partnership Agreement (EPA). We asked why some migrant nurses remain in Japan whereas others leave.
Method:
We applied the methodology of Constructivist Grounded Theory. All participants were internationally educated nurses (IENs) currently or formerly working in Japan after passing the National Nursing Examination.
Results:
Difficulty in mastering the Japanese language was established as one of the main themes. Initial coding elicited two explanatory sub-categories: lack of confidence in communication and effects of language difficulty on workplace relationships. One explains how practical experience in the workplace affected nurses’ confidence in communication. The other explains how levels of Japanese language attainment shaped relationships with colleagues.
Discussion:
These findings suggest a need to regulate the working conditions of foreign nurses, and a need for training schemes to optimize IEN retention.
Keywords
Introduction
Nursing shortages in many countries have shaped patterns of health-worker migration (World Health Organization [WHO], 2022). Countries with high per capita income, such as Canada, the United Kingdom, and the United States, attract a large number of internationally educated nurses (IENs) from developing countries (Walton-Roberts, 2020). Factors contributing to their growing need for nurses include an aging society, the emergence of new diseases, changes in the prevalence and distribution of chronic diseases, and modifications to healthcare systems as medical technology develops. The supply of nurses has not kept up with these demands, largely because of a shortage of training opportunities, declining numbers of new graduates all over the world, and labor shortages due to staff turnover in the nursing profession. A shortfall of 10 million health workers has been projected by 2030, mostly in low- and lower-middle-income countries (WHO, 2022).
In recent years, there has been an increase in the number of foreign workers, including IENs, in Japan. After doubling since 2015, the total has now reached a record high of over 1.7 million, or about 1.4% of the total population (Ministry of Health, Labour and Welfare of Japan [MHLW], 2021). Foreign residents have given various reasons for relocation: studying, acquiring skills for their future careers, and sending remittances back home (Immigration Services Agency, 2021). Following rapid social change such as the aging of the population, problems have arisen as a result of the proportionate decline in the workforce and the limited potential for replacing lost workers with advanced technologies.
As in many other countries, the shortage of nurses in Japan is becoming increasingly serious. Attributable mainly to the high attrition rate among new entrants to the profession, the shortfall is estimated to reach at least 55,000 by 2025 (MHLW, 2019). Thus, both the recruitment of nurses and the encouragement of those recruits to remain in post are important for filling vacancies.
Since the 1990s, changes in both the international economic environment and national development strategies have accelerated the introduction of broad economic relations between Economic Partnership Agreement (EPA) signatories. When Japan implemented the EPA in 2002 to facilitate free trade across national borders, this was the first time that a program had been established to enable IENs to live and work in Japan. In terms of the movement of IENs, Indonesia, the Philippines, and Vietnam were co-signatories with Japan. EPA nurse candidates from Indonesia were first accepted in 2008, those from the Philippines in 2009, and those from Vietnam in 2014 (Ministry of Foreign Affairs of Japan [MOFA], 2014). As of 2023, other countries were not eligible to send nurses. The report found that nurses joined the EPA program to obtain the Japanese national nursing qualification so as to work in Japan, improve their nursing knowledge and skills, and earn money to send to family members in their home countries (Japan International Corporation of Welfare Services [JICWELS], 2023b).
To take part in the program, an EPA nurse candidate needs to be qualified as a nurse in their home country, have work experience, and demonstrate Japanese language skills. Irrespective of nationality, a nurse candidate must pass the Japanese National Nursing Examination (NNE) to become a registered nurse in Japan. Table 1 shows the proportions by nationality of successful EPA nursing applicants who subsequently passed the NNE (MHLW, 2023). From 2008 to 2019, over 1,400 EPA nursing candidates were accepted. They were allowed to take the NNE a maximum of three times in the 3 years following their arrival in Japan, but only a minority of candidates passed the examination in any 1 year (Table 1). The total number of Indonesian, Filipino, or Vietnamese IENs in Japan since the start of the EPA program in 2008 was 648 (MHLW, 2023).
Number of Successful EPA Nursing Applicants.

Source. (MHLW, 2023).
Note. There are no official data on aggregate on the total numbers of foreign nurses taking the NNE as opposed to foreign nurses from EPA countries.
However, the MHLW does not release official data concerning how many continue to work in Japan. Taking these numbers into account with the current EPA program, therefore, one can reasonably assume only one in three EPA nurse candidates was permitted to live and work as a nurse in Japan. This prompted the question of whether IENs themselves viewed the NNE as posing a major difficulty for their careers. As the current EPA program implies (Table 1), the low pass rate for EPA nurse candidates reflects the setting of the language threshold for IENs at the same level as for local Japanese nurse candidates. This means that IENs are expected to reach a native level of Japanese language proficiency and familiarity with medical terminology.
Language problems have been highlighted as among the most challenging difficulties during and after the EPA nurse candidacy period (Asai, 2018). These difficulties occur in communications with colleagues and with both patients and respective patients’ families. Although IENs can acquire basic Japanese language competence by taking part in the EPA program, most find it difficult to learn Japanese (Abuliezi et al., 2020). The program cannot give nurse candidates the level of communicative skill seen in Japanese sociocultural writing, with mastery of grammar and the conventions of usage in different social contexts.
The Japanese writing system presents EPA nurse candidates with particular challenges. Unlike Tagalog, which is the national language of the Philippines, and modern Vietnamese and modern Indonesian, all three of which use the Latin alphabet, Japanese has a unique and complex writing system which amalgamates two syllabic scripts (hiragana and katakana) with a more difficult logographic script of Chinese origin (kanji). The question has arisen whether or not IENs experience Japanese language problems after passing the NNE. This study investigates how fully qualified IENs’ levels of language proficiency affect their self-confidence and interpersonal relationships.
Method
The research is part of a doctoral study called “Exploring decisions as to whether to remain or to leave made by Indonesian, Filipino and Vietnamese registered nurses relocating to Japan under the EPA.” A qualitative method was adopted, based on Charmaz’s (2014) Constructivist Grounded Theory (CGT). This article addresses Japanese language acquisition, insofar as these findings permit a context-sensitive study of the influences facing IENs’ self-confidence and interpersonal relationships in Japan.
Inclusion and Exclusion Criteria
Participants in this study were Indonesian, Filipino, and Vietnamese IENs who passed the NNE EPA program. All had worked (or were currently working) as IENs in Japan since the program was inaugurated. All participants had formally agreed to take part in the study and were given their preferred choice of interview method (in person or online). The sole exclusions were those who were still candidates in the EPA program, that is, those who had not yet taken or who had taken but not yet passed the NNE.
Participant Recruitment Process
Ethical approval was first obtained from the School Research Ethics Panel under the terms of Anglia Ruskin University’s Research Ethics Policy (No. NM-SREP-19-006). Although we contacted the managers of 55 healthcare establishments employing IENs, they were preoccupied with handling the COVID-19 outbreak and unable to respond. Accordingly, we used social networking systems to circulate recruitment materials for the study. This resulted in the recruitment of 18 IENs. “Saturation” signals that data collection and analysis end when no additional data can be found to permit the analyst to refine category properties (Glaser & Strauss, 1967). After meeting the saturation criterion of Charmaz’s (2014) CGT in the course of the 18 interviews, one of the authors conducted two further interviews, bringing the final total to 20.
All participants consented to participate in the study and opted to be interviewed online. Each interview lasts between 60 and 90 minutes. All interviews were conducted in Japanese, as this was the only mutually comprehensible language between the interviewees and the interviewer. All interviews were audio-recorded and translated into English by the interviewer. While care was taken to minimize inaccuracy, it cannot be claimed that the transcripts are as nuanced as the informants intended.
Participant Demographics
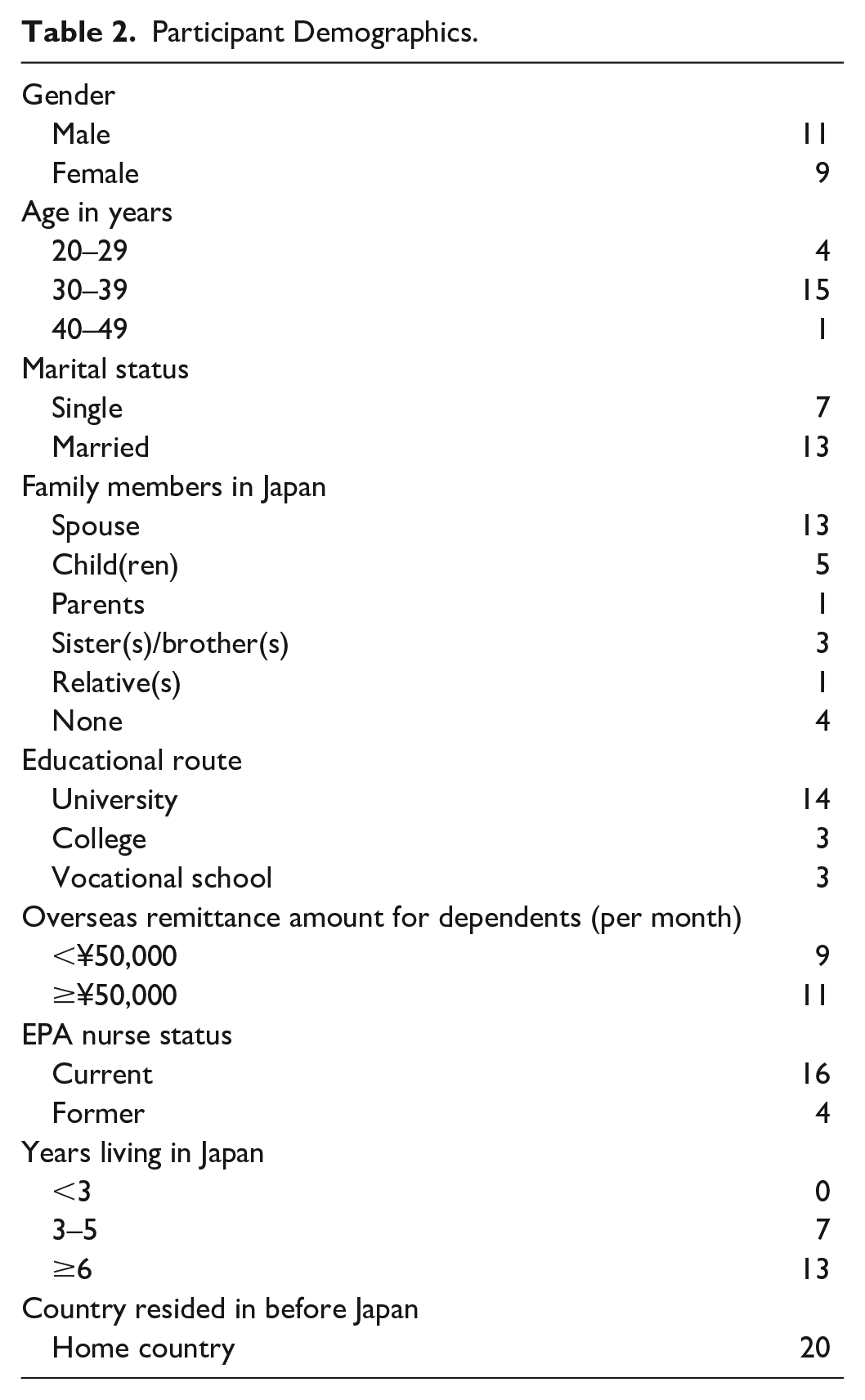
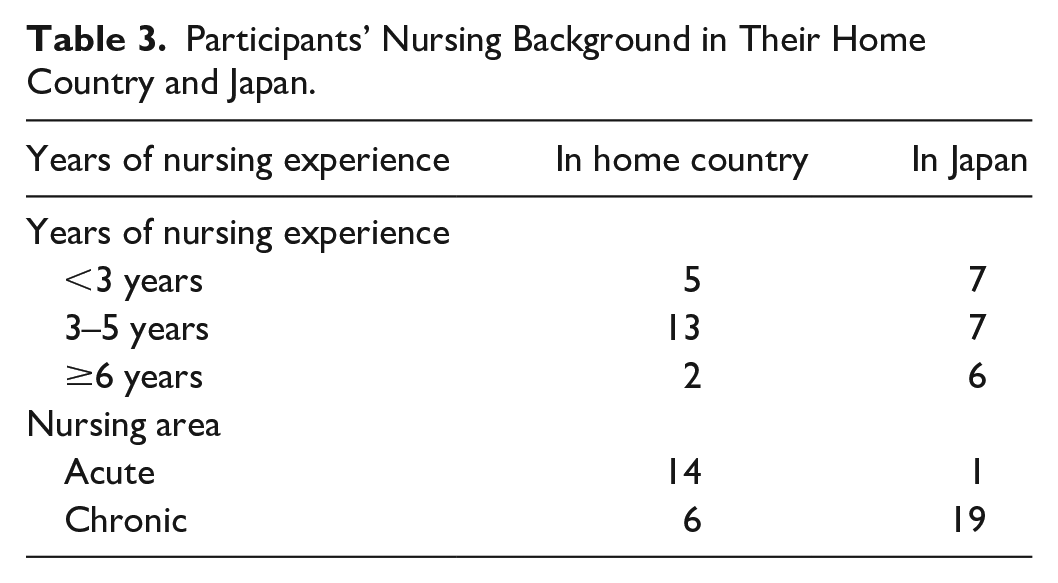
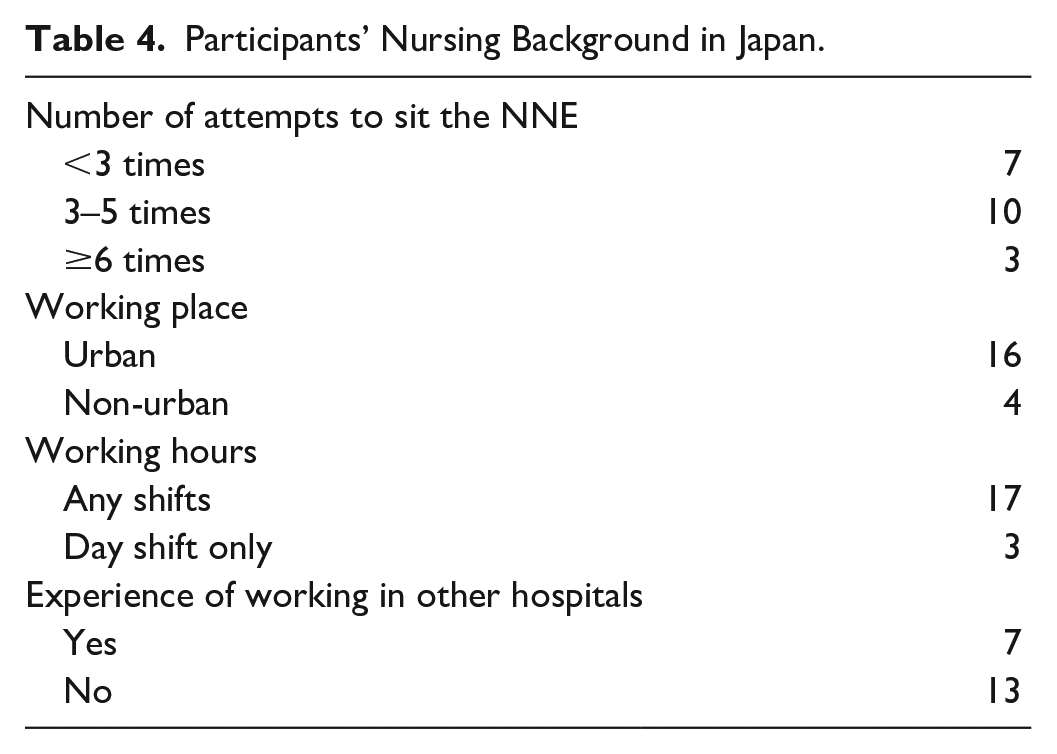
The participants were of Indonesian, Filipino, and Vietnamese nationalities (11 males and 9 females). Some trends can be discerned from the demographics: IENs were likely to have joined the EPA program in their 30s, to be married, to have a spouse or other family member already living in Japan, to send remittances to their home country, to hold a university degree, and to intend to remain at work in Japan for a long while (Table 2). They tended to sit the NNE more than three times, work shifts in urban areas, have more than 3 years of nursing experience, both in their home country and in Japan, and work at the health establishment where they had completed their training as EPA nurse candidates. While for many of the IENs, much of their previous experience back home had been on “acute” wards, their current work in Japan was mainly on “chronic” wards (Tables 3 and 4).
Participant Demographics.
Participants’ Nursing Background in Their Home Country and Japan.
Participants’ Nursing Background in Japan.
Data Analysis
The data collection process began in November 2019 and ended in August 2020. The sampling method had been purposive and theoretical, insofar as the interview responses were analyzed and revised each time that an interview had been concluded, and the process of revision continued until theoretical saturation had been achieved. Three main types of grounded theory coding procedures were used, namely initial, focused, and theoretical (Charmaz, 2014). In the initial coding, IENs’ views were explored. During the focused coding, the extracted initial codes were categorized (as sub-categories). At the theoretical coding stage, an abstract category with enriched explanatory power emerged as the main category which shows the difficulty for IENs to master the Japanese language (Figures 1 and 2). The analysis was undertaken with the qualitative data analysis software NVivo, in which the data and codes were stored in a stable format. The findings reported here form only part of a more extensive doctoral thesis.
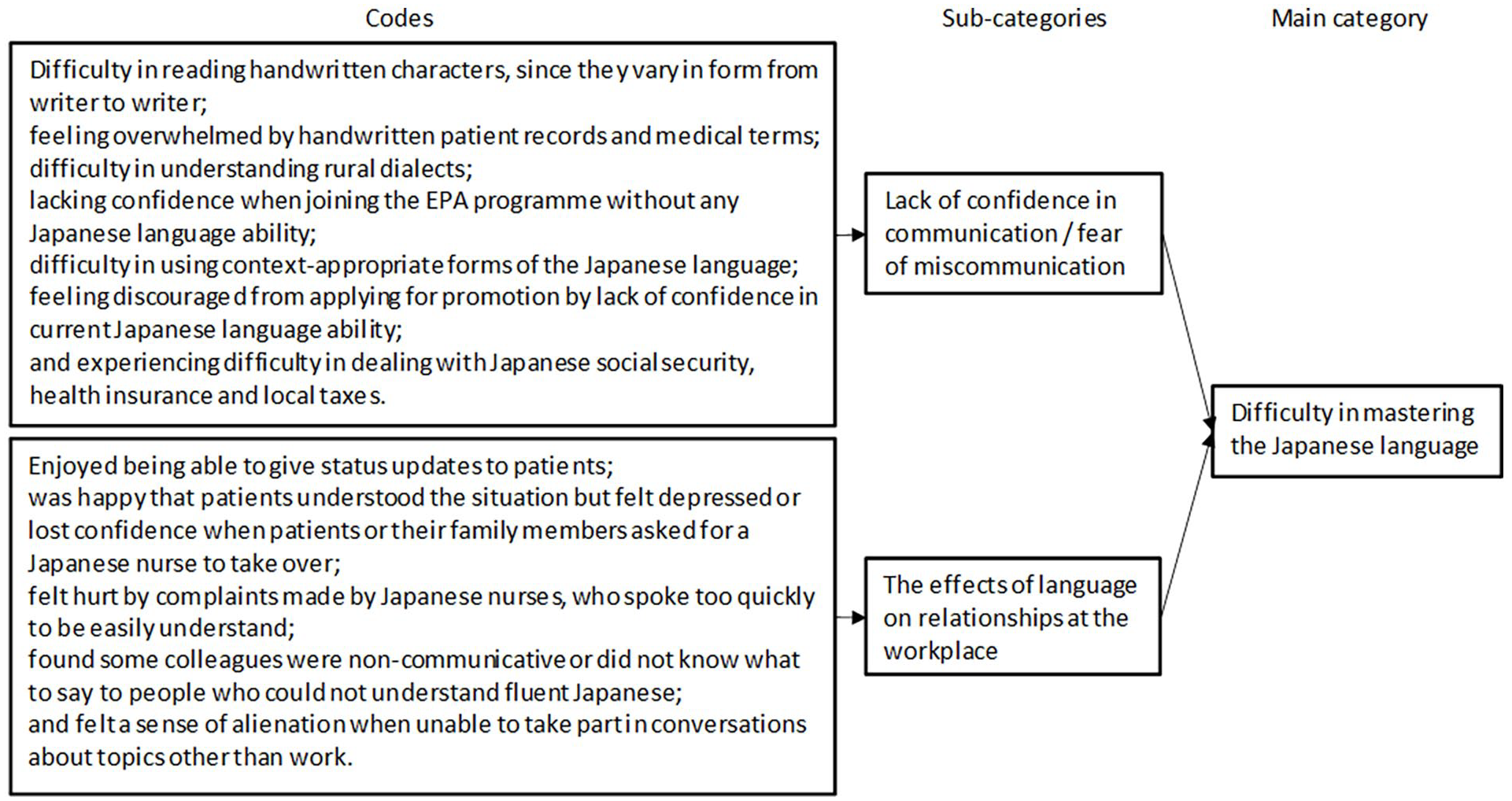
Data Structure and Summary of Codes, Sub-categories, and Main Category.
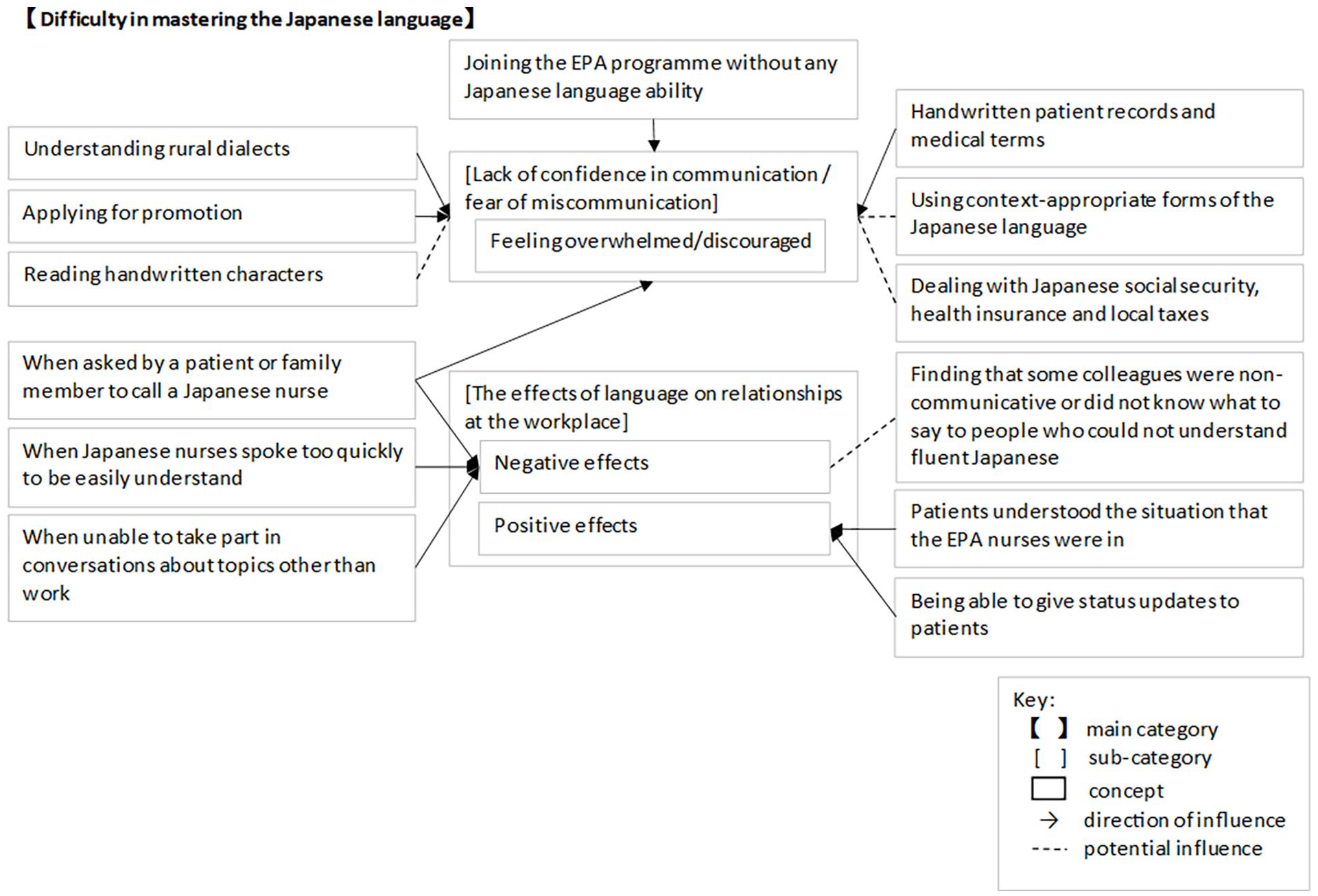
The Concept Map Shows Inter-relationships for Difficulty in Mastering the Japanese Language.
Rigor
To evaluate the quality of the emerging substantive grounded theory, Charmaz’s (2014) criteria of credibility, originality, resonance, and usefulness were applied. Credibility was achieved mainly by obtaining rich data through online interviews. Each interview was translated into English and fully transcribed as soon as it had been concluded.
The transcript was then analyzed thematically using NVivo, which helped with data organization and visualization before the subsequent interview took place. To establish credibility, extensive and constant comparisons were made between concepts, sub-categories, and main categories. These were analyzed strictly on the basis of the data, to mitigate the effects of the researcher’s preconceptions. Originality in the conclusions was sought through the researcher’s positionality as a Japanese national with experience of working at healthcare establishments in Japan, Australia, and the United Kingdom. In addition, the academic literature was re-examined to determine whether the analyses yielded a new conceptual account of the data. Resonance was achieved by including among the interviewees both current and former IENs, who were recruited to reduce survivorship bias that could occur if only current IENs had been interviewed. The emerging theory contributes to current EPA program policy in general, and specifically to training at care establishments that accept IENs, thereby meeting the criterion of usefulness.
Results
The IENs reported that they had continued to experience difficulties with the Japanese language even after passing the NNE, both in their work and in their everyday lives. “Difficulty for IENs to master the Japanese language” therefore emerged as a main category, which includes the following two sub-categories that emerged during the coding process (Figures 1 and 2).
Lack of Confidence in Communication / Fear of Miscommunication
Individual differences in Japanese writing can pose problems for IENs. The difficulties that they encounter in understanding medical terminology are compounded when they have to read handwritten nursing records: Handwritten characters vary from writer to writer and are harder to read than electronic characters. (IEN 8)
Unlike doctors in the Anglophone world, Japanese doctors may write in multiple languages; although they write mainly in Japanese, they also use loanwords from English or German. By contrast, Japanese nurses are unfamiliar with foreign languages in the course of their work, as nursing records are written exclusively in Japanese. However, record-writing is not required of EPA nurse candidates and so, like their Japanese colleagues, the IENs experience difficulty in deciphering the doctors’ handwritten notes: We had a lot of handwritten records and many medical terms I didn’t understand. In particular, reading the doctor’s handwriting was difficult for me (IEN 15)
In terms of listening and speaking, IENs are confused by the difference between what they learn in the lecture room and how Japanese is spoken outside. Even as they gain experience, IENs speak of their Japanese language difficulties with Japanese language dialects. In healthcare settings, they feel anxious when their communication is inadequate, and this can also lead to patient frustration. Miscommunication cannot be avoided until IENs become accustomed to speaking everyday Japanese with confidence: I find it difficult to understand Japanese rural dialects. For this reason, there have often been misunderstandings. (IEN 13)
Although the IENs were attracted to the EPA program having learned about it, they anticipated difficulty in attaining a high enough level of Japanese language fluency in the 3 years it takes to pass the NNE. For EPA nurse candidates whose native language is not Japanese, it proves a challenge to acquire sufficient Japanese language skills in such a short time, and this makes prospective candidates less confident about joining the program: I thought it would be impossible for me because I couldn’t speak Japanese. So, at first, I wasn’t confident about joining the EPA program. (IEN 15)
However, the experience of working and living in Japan built up their Japanese language skills and gave them a degree of confidence. In Japan, communicating with inappropriate use of the language causes anxiety or difficulties with relationships. Some of the IENs spoke of a need to master the vocabulary for particular situations, such as resuscitation, which can be especially fraught and require a high degree of linguistic sensitivity. Failure to use accurate Japanese in moments of crisis can cause serious misunderstandings between IENs and their colleagues: In the nursing home where I currently work, we need to consider whether a resident whose condition is worsening needs to be resuscitated or not. This work is very difficult because it is necessary to contact the care worker, the resident’s family doctor, and the resident’s family in advance, and to understand them accurately in Japanese. (IEN 10)
Whether they are native Japanese or EPA participants, as the IENs gain experience they have opportunities to take on the more senior role of charge nurse. Colleagues then expect them to perform more responsible roles with a proficiency equal to that of their Japanese colleagues. However, some of the IENs in the study were concerned about their lack of confidence in speaking Japanese when talking with other health professionals, or with patients’ or residents’ family members. In this case, lack of confidence creates a career barrier. For example, IENs who have been offered internal promotion to more senior positions have refused it, as they anticipated that greater responsibilities would require communication skills that they did not possess: As a nurse, I was on track to become a chief in the future at the workplace where I currently work in Japan. However, I am a foreigner, and although my expectations have been raised by the success of my friend, I refused promotion because I am not confident in my ability to establish a relationship with members of the client’s family at my current Japanese language level. (IEN 10)
IENs had spoken of other situations involving language difficulties during their NNE preparation, beginning with information about the health system: I felt it difficult because the topics of social security and health insurance were different from those in my country. There are no compulsory questions
1
in my country’s nursing exam. (IEN 4)
Later, as they pursued their careers in Japan, they encountered difficulties in finding a way through bureaucratic procedures. These difficulties occurred, for example, when they changed their workplace or their home address. As one informant admitted, I still find it difficult to cope with health insurance and local taxes. (IEN 17)
When EPA nurse candidates have passed the NNE and resumed work as fully qualified nurses, their involvement with the EPA program comes to an end. However, some of the IENs in the study continued to experience difficulties while living and working in Japan and called for assistance after qualifying: I would also like to see ongoing support for IENs as part of the EPA program. For example, skill enhancement training, learning how to write records, and how to deal with the patients’ families, so that we can feel secure in our jobs. (IEN 10)
Overall, the acquisition of Japanese language skills is an unavoidable challenge for those who join the EPA program. During the candidacy period, the focus was preparing for the NNE in Japanese, which is also taken by Japanese nursing students. After IENs have passed the examination, they need to become more proficient in Japanese as they have more opportunities to discuss with the family members of hospital patients or care home residents and with other health professionals. They also needed to familiarize themselves with regional dialects. Although they encountered difficulties in communication, practical experience led to an increase in confidence. Subject to individual differences, their level of Japanese language skills influenced interprofessional relationships.
The Effects of Language on Interpersonal Relationships in the Workplace
Working in another country requires people to reach a certain level of foreign language proficiency, and the attainment of professional qualifications does not always mean that IENs have confidence in their communicative abilities. IENs who had passed the NNE and started work reported that they were not good at taking down general information from new patients entering the ward, as this also requires listening and speaking skills that the NNE did not assess. In other words, the NNE was not a fully valid test of language competence on the ward. This is because, before they passed the NNE, they had not had enough time to practice listening and speaking while they were EPA nurse candidates. However, some of the IENs established warm relationships with patients and felt professional satisfaction when patients cared about them: Since we have many patients who are hospitalised for a long time, they became friends. It was fun to be able to give status updates to my patients. I’m glad when the patients care about me and talk to me. (IEN 7)
As in all other countries, the Japanese people have their opinions of foreigners. Some take an interest in and try to understand their foreign visitors. The Japanese patients who tried to understand their situation and showed concern for them helped the IENs to feel that theirs was a worthwhile profession. Nevertheless, patients did not show understanding or concern unless they trusted their nurses: I also find the job of a nurse rewarding when I have a good relationship with the patient. In particular, I am happy that patients understand that I am a foreigner and show concern for my own well-being. (IEN 18)
Not all IENs have good relationships with their patients. Colleagues and hospital patients, care home residents, or family members expect the IENs to communicate clearly to avoid medically related incidents in healthcare settings. Communications of this kind require a higher level of language skill than that required in informal everyday interactions. Some IENs experienced unpleasant situations with patients or their family members who expected health professionals to be able to speak fluent Japanese. If patients’ expectations were disappointed, they could ask for an IEN to be replaced by a Japanese colleague. Those experiences dented the self-confidence of the IENs. Without nurse–patient interactions, the IENs had no chance of enhancing their trust: When a patient knows that I cannot speak Japanese very well, they sometimes ask me to fetch a Japanese nurse. [How do you feel when that happens?] I sometimes feel depressed or I lose confidence in myself. (IEN 5)
Hostile remarks from hospital patients, care home residents, or family members were also prompted by the IENs’ non-Japanese appearance. The IENs concluded that replacements were made if they did not seem “Japanese.” This was a negative experience but one which could occur if they did not speak Japanese very well: I feel a little disappointed when the patient’s family asks for me to be replaced by a Japanese nurse if they think I cannot communicate well because I don’t look Japanese. (IEN 9)
Unpleasant interactions like this were not limited to dealings with patients. They also involved dealings with co-workers, who could strike IENs as unsympathetic, especially during busy periods. These perceptions of hostility led to mistrust, which might impair future interprofessional relationships: You can immediately tell what you want to say in your mother tongue. However, I’m a foreigner, so I cannot understand what my colleagues are saying when we are busy and they speak quickly. At times, this might be a cause for dissatisfaction and complaint on the part of Japanese nurses. (IEN 6)
Many Japanese people are unaware that their healthcare establishments employ IENs. As most Japanese health professionals expect to communicate only in Japanese, they might be unwilling to consider communication in any other language. For this reason, Japanese health professionals might not be sure how to work with colleagues from other countries and do not even attempt to communicate, which would allow no opportunity to build interprofessional relationships: If some colleagues think that I cannot understand anything in Japanese, they might simply decide not to talk to me. I think some people don’t even know what to say. (IEN 20)
Although an everyday level of language proficiency can be sufficient for the workplace, some IENs try to advance their Japanese language competence above that level. One unfortunate consequence of linguistic barriers for IENs is a sense of alienation from colleagues at work when they are unable to take part in conversations about non-work-related topics. These conversations are nevertheless expected, as they further interprofessional relationships. If they are unable to join in, the IENs feel unhappy and inadequate: I feel a sense of alienation when I cannot enter into conversations about topics other than the work when doctors are speaking with nurses. It might be that I don’t understand even if I do speak. (IEN 20)
Some of the IENs had nevertheless succeeded in establishing interprofessional relationships at the workplace, even while others had come to believe that their own Japanese skills were not good enough for that purpose. For the latter group, awareness of language challenges or of being expected to have difficulty in communicating had a negative impact on their relationships with other people.
Discussion
The study found that even after the IENs had passed the NNE they had encountered Japanese language difficulties while living and working in Japan. We found that IENs accordingly sought opportunities to advance their Japanese language skills, especially their communicative competence in social contexts. It was not in dispute that greater fluency in Japanese was essential for risk reduction and care quality enhancement.
Difficulties Resulting From Lack of Opportunity to Learn the Japanese Language
Previous studies have documented ways in which language barriers impact the relationship between nurses and patients (Gerchow et al., 2021), and this was also found in this study. The study also noted the effects on IENs and their colleagues, and on patients’ families, since some of the IENs had difficulty in writing and speaking correctly in terms of medical terminology. Unlike their Japanese colleagues, some IENs in this study anticipated difficulty in explaining their tasks in Japanese, especially when they were keeping nursing records. These are still sometimes written by hand and are essential for exchanging information between the multiple shifts of the working day. IENs’ difficulties in using nursing records have not been clarified by recent research. However, this study found that these difficulties were non-trivial. Since these records are important for keeping track of patient whereabouts and for evaluating nursing care, the IENs have to deal with much more paperwork in Japan than is the case in their home countries. Electronic health records can enhance collaboration between healthcare professionals (Vos et al., 2020), and nurses in this study recognized the advantage of maintaining nursing records electronically.
As had previously been found in studies of EPA nurse candidates, the IENs needed to master not a generic language but a variety of specific forms of Japanese language, such as medical terminology in the workplace, or bureaucratic terminology in everyday life. They also needed to become familiar with the local dialects used by patients or their families, and the special characteristics of the oral and written languages.
Japanese language difficulties will beset any IENs. EPA nurse candidates have access to Japanese language support under the EPA program, but once they pass the NNE there is no more Japanese language support. This study found that IENs continued to encounter language difficulties while living and working in Japan.
Once they became a qualified nurse in Japan, they still needed to acquire advanced Japanese language skills. Without those skills, they lacked confidence in communicating, and this impacted their interpersonal relationships. Accordingly, as part of the EPA program, it is recommended that ongoing Japanese language support be offered by healthcare establishments employing IENs so that they can reach proficiency in Japanese at a level permitting them to carry out their professional duties. This support must anticipate all situations likely to be experienced by IENs while living in Japan. In addition, the workplaces of IENs need to offer support and advice to understand the Japanese bureaucratic procedures.
Consequences of IENs’ Need for Greater Language Proficiency
Limited language proficiency negatively affects levels of satisfaction between healthcare professionals and service recipients, and has implications for patient safety (Al Shamsi et al., 2020). When nurses in South Korea spoke out, their willingness to communicate was influenced by the positive or negative consequences of doing so (Lee et al., 2023). In this study, individuals were reluctant to speak out when they felt isolated from colleagues. However, healthcare managers can create a more diverse and better-integrated workforce while ensuring that patient safety remains at the forefront of their efforts (Kamau et al., 2022). In maintaining the safety of patients or persons in need of care, communication skills play a key role. Thus, to maintain the quality of nursing care, language skills are an essential requirement.
Many countries of destination require IENs to pass national examinations. Host countries such as the United Kingdom, Australia, and the United States hold adaptation courses and language proficiency examinations. However, this method of recruitment leads to inconsistent outcomes, such as differences in the quality of nursing depending on the policies in force in the host country. In the United Kingdom, since the early 21st century, English language examinations have been part of the test of competence required of IENs. To supplement the test, Gillin and Smith (2021) recommended that changes in its content and effects should be evaluated with regard to the quality of support offered to IENs by NHS Trusts in the United Kingdom. Such an evaluation would also be helpful in Japan, where the difference between the language used in the NNE and the language used in everyday nursing confused the IENs in this study.
A further cause of anxiety that some of them mentioned was a need to conform to expectations of the politeness level of speech appropriate to diverse situations and individuals. The IENs added that leadership roles increased the need to liaise with other health professionals. If a patient’s situation and instructions were not accurately understood and reported, there was a risk of medical error. Thus, IENs recognized that they had to continue to work toward a higher level of Japanese language proficiency that was appropriate to these healthcare settings.
In Japan, the acceptance of non-native speakers as EPA nurse candidates under the EPA program necessarily entails a need for language training. When prospective EPA nurse candidates join the program, their Japanese language competence is assessed against a strict standard (JICWELS, 2023a). Without proficiency, they cannot be accepted by healthcare establishments to begin their first work experience in Japan. Since EPA nurse candidates were first accepted in Japan, research has been undertaken into their Japanese language acquisition, specifically in relation to the NNE (Hirano et al., 2020; Vilog et al., 2020). Japanese language training is provided for EPA nurse candidates under the EPA program, both before and after they start work. In the future, ongoing language support for newly qualified nurses wanting to progress to a higher level of Japanese language skills would enhance confidence in communication, leading to improvement in interprofessional relationships. Participants in this study reported that as soon as EPA candidates qualify and start work their colleagues expect them to be fully professional in discharging their nursing duties. Nevertheless, it is unreasonable to ignore their status as second-language speakers of Japanese and to expect them right away to have the same communication skills as Japanese nurses. Japanese colleagues need to support IENs who are being encouraged to develop their language skills on the job. It is necessary for the native Japanese in the team to engage in dialogue, to determine what allowances are possible and what the IENs should seek to achieve.
Communicative Competence in Social Contexts
Although IENs attain basic language competence during preparation for the NNE, they need extensive knowledge of Japanese culture. Moreover, some of the IENs reported that people living in rural areas would use forms of the language differing markedly from standard Japanese. The use of dialect intensified their anxieties to the extent that they hesitated to accept more senior roles and responsibilities. The finding of this study that IENs experience language difficulties, both at work and in their everyday lives, is illuminated by Bachman’s (1990) theory of the “communicative language ability,” which proposes ways in which abilities demonstrate how different individuals perform in sociocultural settings. The variability of nurses’ performance on the ward can be explained, in part, by individual differences in their communicative language ability. Some of those IENs had encountered situations in which they required a more advanced Japanese language competence, and they realized that they would have to continue learning Japanese after their nursing registration. To sum up, to pass the NNE and undertake their professional duties, IENs need to display “communicative language ability” according to the situations in which they are placed. The attainment of “communicative language ability” is an essential goal. Accordingly, ongoing language support in the workplace is required for IENs until they have become familiar with Japanese medical terms. This support should be broadly contextualized within the host country’s customs and culture. Thus, while further training is required, it needs to be focused on communicative competence, to establish a culture of safety-consciousness.
Limitations
All IENs taking part in the study were nurses coming to Japan from Indonesia, the Philippines, and Vietnam under the auspices of the EPA program. It is not known whether IENs coming from countries outside the EPA program have different experiences in Japan. Healthcare staff working with IENs, patients/residents, and their family members were not invited to share their own perspectives on IENs. Nevertheless, further improvements to the training given at Japanese healthcare establishments should be implemented only after careful consideration of third-party perspectives.
Conclusion
Many countries including Japan have become increasingly reliant on the employment of IENs to meet healthcare demands. This study found that EPA can experience difficulties while living and working in Japan. Mastery of the Japanese language must continue to be addressed, even after they have passed the NNE, but in different and more demanding contexts. The language barrier depresses their self-confidence, both at work and in their interpersonal relationships. From this study, it appears important to provide opportunities for IENs to advance to a higher level of Japanese language skill in the context of specific situations relevant to their work settings, and to help them become more confident in using the Japanese language in their interpersonal relationships. However, the study found that some Japanese nurses were unwilling to compromise by making their language more accessible to their EPA colleagues. With this in mind, it is important for healthcare establishments to encourage Japanese staff to understand the need to support and help the IENs, whose mother tongue is not Japanese so that they can communicate clearly to patients, care home residents, and their family members.
Footnotes
Acknowledgements
The authors express their deepest gratitude to the EPA nurses who took part in this study, to the managers of their healthcare establishments, and to Dr Micah Auerback being a proofreader.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.