
Abstract
Introduction:
This study examines the subjective experiences of Turkish students who work in immigrant health facilities providing nursing care to people of different cultures. Nurses are often encountered by immigrants in these centers. Although qualitative research on nurses’ experiences assisting immigrants has been often cited in the literature, the literature on nursing students’ experiences is limited.
Methodology:
The study has a descriptive qualitative design. Data were collected using a face-to-face, in-depth, and semistructured interview form. The data were evaluated using a content analysis method.
Results:
The study yielded four themes: (a) inability to control emotions, (b) barriers to care involvement, (c) benefits of intercultural care, and (d) recommendations.
Discussion:
Learning intercultural care is critical in these years of increased immigration. Understanding nursing students’ experiences is essential for improving the quality of intercultural care.
Introduction
Humans have been forced to leave their birthplaces by harsh conditions since the beginning of time, giving rise to the ideas of “immigration” and “immigrant” (Waldinger, 2015). The most fundamental definition of migration is a shift of a person’s place of belonging, which results in a change in physical space and the meaning and value of both the individual and the society (Gamlen, 2019). Climate changes, drought, increasing population, and insufficient agricultural lands have been the primary reasons for human migration throughout history; however, these reasons have been succeeded by more recent causes, such as war/civil war, natural disasters, violence, poor living conditions, and oppressive political policies (Racimo et al., 2020).
The public upheavals in Tunisia in 2010 triggered a chain of events known as “the Arab Spring,” which affected many countries directly and indirectly (Kargin, 2018). Syria is one of the most affected countries by this process. Although public upheavals in several Arab countries have resulted in regime or administrative changes, no change or transformation has happened in Syria. In response to the protests, the Syrian government’s oppression and punitive actions resulted in hundreds of thousands of civilian deaths and millions more fleeing the country (Tumen, 2016). Approximately 585,000 people died in Syria over the course of a 10-year period. In addition, 6.6 million people became internal migrants, and 5.6 million people fled the country to become refugees (Stubblefield & Joireman, 2019).
Syria’s tyranny produced the most refugees, followed by Afghanistan, the Lake Chad Basin, South Sudan, and Somalia. Turkey officially hosts the most Syrian refugees, at 3.8 million as of 2021 (International Organization for Migration, 2023). This sudden influx of immigrants brought many political, cultural, economic, and sociological problems to Turkey. Conditions such as malnutrition, poor shelter and hygiene, infectious diseases, trauma, a lack of social support, and difficulties accessing medical services threatened immigrants’ health (Özkan, 2019).
The WHO framework agreement established in 1949 explicitly stated that health services are a fundamental human right and should be provided equitably (United Nations General Assembly, 1949). To this end, health care provided to immigrants should be regarded as a human right, and each country should make plans to meet the WHO agreement’s requirements. However, the unexpected and rapid increase in immigration challenged local resources and disrupted local health care services. To address these problems, the European Union and Turkey launched the “Health Project” in 2016 to provide vital health care services to Syrian refugees (Küçük, 2020). To this end, Turkey established centers throughout the country where immigrants congregate to provide primary and mental health care services. Turkey has 181 migrant health centers in 29 provinces as of 2022 (“Sıhhat Project,” n.d.). Nurses are the health workers who commonly interact with immigrant individuals while obtaining health care services in these centers; at the same time, nurses are the workforce necessary to protect and improve the health of immigrants.
Nursing is primarily a cultural phenomenon. Holistic nursing care requires understanding the patient’s cultural values, beliefs, and behaviors. In the 1950s, Peplau (1952) first introduced the concept of culture in nursing. Then, with Leininger’s (1996) “Transcultural Nursing Model,” nursing care for people of different cultures became more popular. In 1969, the International Nurses Association started to use the concept of culture in nursing. The Transcultural Nursing Organization was founded in 1974 (Pektekin, 2000). With the impact of the globalizing world, the nursing profession has recognized the necessity and responsibility of providing individual-centered care to the whole society and ethnic groups in today’s settings (Jeffreys, 2000).
To provide effective and patient-centered nursing care, nurses must be attentive to the needs of people from different cultures and structure their services accordingly. Nursing programs should provide theoretical and clinical practices to prepare students to become aware of their patient’s values, beliefs, and lifestyles (Akgül-Gündoğdu & Selçuk-Tosun, 2022; Backlund & Olausson, 2021; Kuru Alici & Öztürk Çopur, 2023). Studies conducted with students come to the forefront in structuring the education curriculum. However, although there are studies in the literature examining nurses’ care experiences for individuals from different cultures (Hussam & Alnjadat, 2022; Sevinç, 2018), it was found that studies conducted with nursing students were primarily investigated using the quantitative method in the fields of cultural competence and effectiveness (Tosun, 2021; Üzar-Özçetin et al., 2020). No study has examined students’ experiences providing long-term nursing care to immigrants.
It is a basic requirement of patient-centered nursing care that nurses take cultural differences into consideration in the structuring of services provided to individuals or groups from different cultures. The education that nurses receive during their student years has a great share in nurses having this perspective. In this respect, understanding nursing students' experiences of providing long-term care to immigrants from different cultures can help fill the gaps in the literature and improve the nursing school curriculum. This study will help to train nurses equipped to meet the needs of different cultural groups in society.
Method
Research Design
This study was conducted using a descriptive qualitative design. This type of study is used when an event or phenomenon is characterized explicitly without intuition and is concerned with the nature of the phenomenon rather than how or why something occurs (Sandelowski, 2010). This study was conducted with students who work in immigrant health centers. The study’s inclusion criteria include a third-year student at the Faculty of Nursing who completed the Diseases and Nursing Care 3 course internship at immigrant health centers for 1 month and volunteered to participate in the research. The exclusion criteria were one absence, which is consistent with the internship limit, in practices in migrant health centers and previous experience with transcultural care in their previous practice.
Data Collection
Between June and July 2022, data were collected face-to-face using an in-depth interview method and a semistructured interview form, and all interviews were recorded on a voice recorder. There were open-ended questions in the semistructured interview form to understand the students’ experiences throughout their program at the immigrant health center, which was their first contact with intercultural care (Table 1). The first and second authors, research assistants at the same nursing faculty, conducted all interviews in Turkish. The questions were selected after two pilot interviews assessing their clarity and competency. The pilot interviews were not used in the study. The participants were informed about the purpose of the research and the audio recording, and the time and place of the interviews were scheduled with those who consented to be interviewed. The first and second authors, who participated in the data collection and coding, know each other from previous nursing practices with the students that study sample students, which is a helpful factor in the data collection interviews.
Semi-Structured Interview Outline.
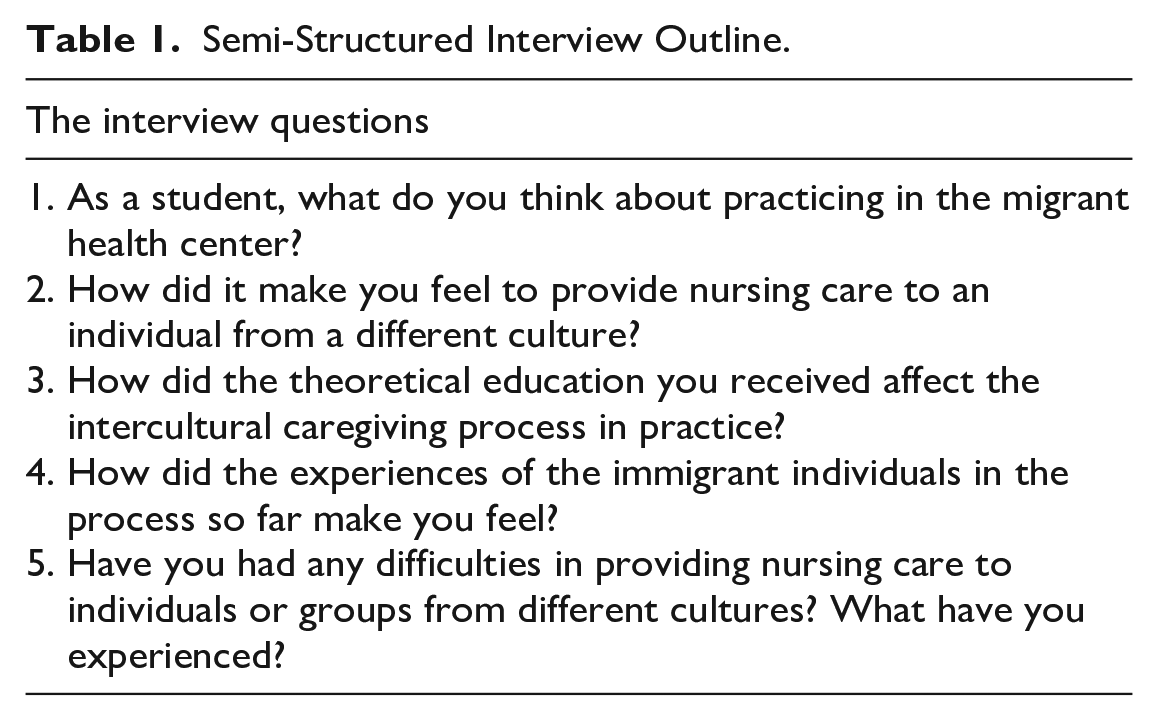
The interviews were conducted in a well-lit, interruption-free room in the Faculty of Nursing. The interviews lasted a minimum of 23 min and a maximum of 37 min, with no one else in the room but the researcher and the student. The interviews proceeded until the data became saturated, which began to repeat, and no new information was forthcoming. In 2022, migrant health centers were used as an application area in the Faculty of Nursing’s practical courses for the first time. The study population in this context comprised 23 students who applied for the Diseases and Nursing Care 3 course at the migrant health center. The study included 23 students who worked at an immigrant health center. However, two students were excluded because they had previous experience with intercultural care in their previous practice, albeit short term (one and two practice days, respectively). The total study sample included 21 individuals, and each participant was interviewed once.
Data Analysis
With doctoral-level training and qualitative research experience, the first and second authors independently examined the interview data using a content analysis method. The study was guided by the steps outlined by Erlingsson and Brysiewicz (2017). All interviews were transcribed verbatim before data analysis. The interviews were listened to and read repeatedly to characterize the nature of the experience.
The language was divided into meaningful small units in the first phase, staying true to the nature of the experience. Preserving the primary/essential meaning was very crucial at this point. The researchers then constructed a code list of meaningful units, and their code lists were compared. The analysis continues using the acceptable code list in the following phases. Categories were produced during the analysis’ category generation stage by bringing together and grouping comparable and dissimilar codes. The meaning of the categories was used to name them. Then, two or more categories were combined to form themes that described the experience. Theme development is a super synthesis step. All the researchers met to discuss the topics, and four themes that explained the phenomena were agreed upon. MAXQDA program was used to store, code, and organize the data.
Ethical Considerations
Written consent was obtained from the institution and the non-interventional Research Ethics Committee (22-6T/37). Before the interview, the students were briefed about the research, and their written and verbal agreement was collected. Furthermore, they were informed that data anonymity would be ensured by using codes to identify them in the transcripts, data analysis and study report and that all information they provided would be kept confidential.
Trustworthiness
To guarantee the correctness of the data, four main methods were used in the study: credibility, transferability, consistency, and confirmability (Colorafi & Evans, 2016; Houghton et al., 2013). All of the researchers had received training in qualitative research and had prior experience with this method. In addition, the researchers had experience working in intercultural care and immigrant mental health. The study included students from various backgrounds in the sample, and interviews were conducted until no new information was obtained. The same two researchers conducted interviews using the semistructured interview form. On the code list agreed upon by the two researchers, data analysis was performed independently of each other. Examples of students’ remarks were provided as direct quotations under each subject (Colorafi & Evans, 2016; Houghton et al., 2013). To enhance the study’s credibility at the end of the interviews, the participant’s interviews were summarized, and confirmation was asked of them. Following data collection, Kappa analysis was used to assess the dependability levels of the themes among the coders. The coherence value between the coders in this study was 0.92, indicating an acceptable level of concordance (Campbell et al., 2013).
Results
This section provides the participants’ sociodemographic characteristics and qualitative findings.
Demographic Characteristics of Participants
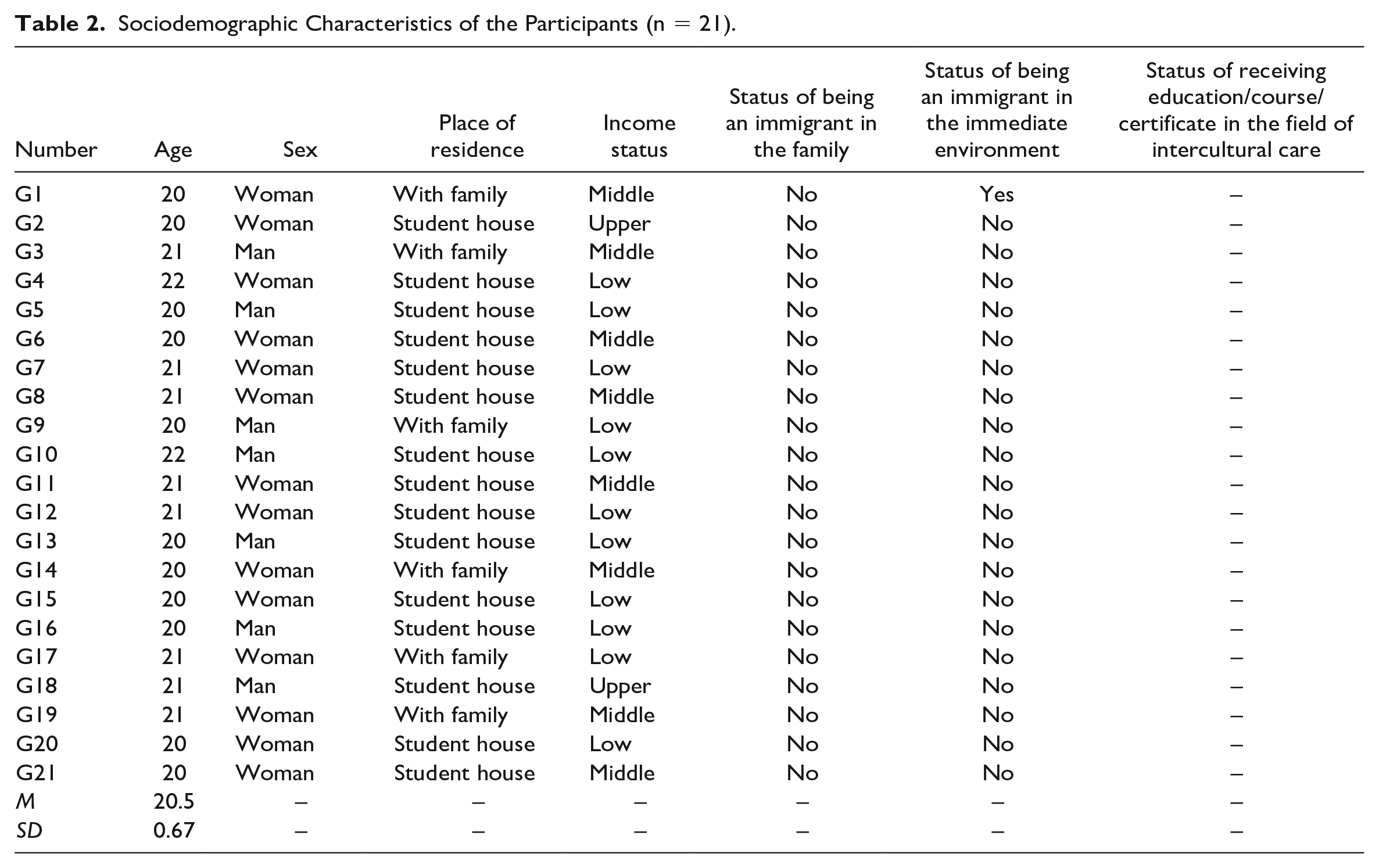
Table 2 shows the sociodemographic characteristics of the students who worked in immigrant health centers.
Sociodemographic Characteristics of the Participants (n = 21).
Qualitative Findings
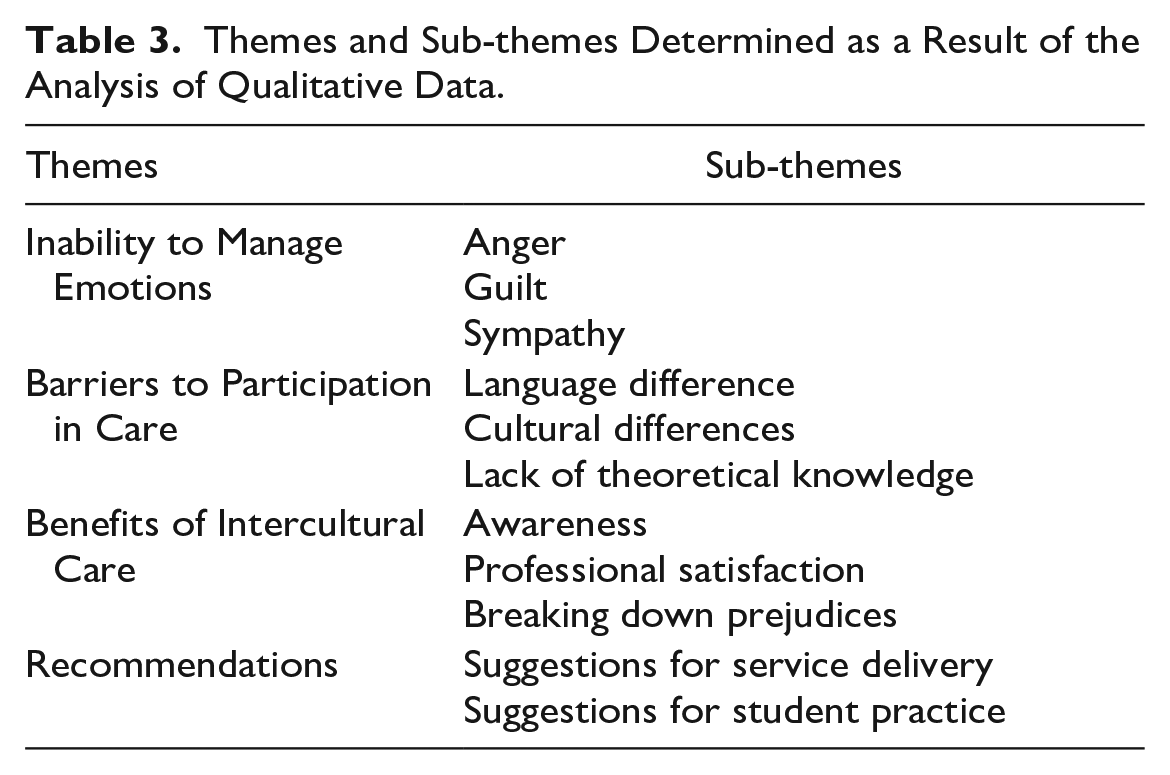
The study found four themes that described nursing students’ experiences throughout the immigrant health center program: (a) incapacity to control emotions, (b) barriers to care involvement, (c) benefits of intercultural care, and (d) recommendations (Table 3).
Themes and Sub-themes Determined as a Result of the Analysis of Qualitative Data.
Theme 1: Inability to Control Emotions
Students expressed difficulty controlling some of their emotions when providing intercultural care in immigrant health centers, particularly anger, guilt, and sympathy.
Anger
While delivering treatment to people of all ethnicities at the immigrant health center, the students expressed their displeasure that immigrants received better care than local inhabitants in the host country: I am not sure why they moved here to avoid the battle. I understand women and children a little bit but not the others. How may a person flee his home and country? Regardless of the outcome, I would not leave my own country. (Participant 7)
Another student expressed anger, saying, It is frustrating that they come here and have possibilities that we do not have. While I was attempting to arrange an appointment for my father, he offered me a range of 1 to 2 months later, but immigrants may be evaluated comfortably here. (Participant 3)
Guilt
As the students were engaged in their intercultural care, they expressed regret for their hostility toward the immigrants: Recently, I saw a lot of harsh comments against immigrants on social media. I was dismayed when I learned that the internship lists were complete and that I would apply to the immigration center, even though I did not want to. However, when I heard their life stories, I was very embarrassed; I blamed myself for being the person I was. I could not get over this feeling for a few weeks. (Participant 10)
Sympathy
While providing care in the immigrant health center, the students felt sympathy for the immigrants because of the difficulties the immigrants had experienced: There were people my age there. It is unavoidable that people absorb it. For example, people my age were expecting their fourth child . . .. When I encountered such situations, I cried until I got home after practice. (Participant 1)
Theme 2: Barriers to Care Involvement
According to the students, language problems, cultural differences, and the lack of theoretical knowledge were challenged in properly treating immigrants in the immigrant health center.
Language Differences
The students stated that they could not offer sufficient treatment to immigrants because they did not know the language the immigrants spoke; they attempted to understand the patients through body language: I realize that nursing care is universal, but the person before me attempted to explain something I did not understand. In such cases, I had no idea what to do. Thank goodness my Arabic friend was there to assist me. We sometimes tried to communicate with signals and body language, but we generally could not understand each other. (Participant 12)
Cultural Differences
During their intercultural care experience, the students stated that the cultural differences of immigrants prevented them from giving proper care: Some female patients would not even let a man draw their blood. Of course, I understand that this is not personal; it is part of their culture. However, how can I provide effective treatment in such circumstances? (Participant 5)
Lack of Theoretical Knowledge
The students found that their theoretical knowledge (from their training) was insufficient for the problems of dealing with immigrants at the health center: When a Turkish person is ill, I can instantly decide what to say and how to communicate with the patient but not with those here. Let me tell you something: I have no idea what to do when I give information. For example, I had no idea how to approach the issue. I had no idea how to establish a conversation with people from other cultures or what to look for upon meeting them. That is when I realized how inadequate my theoretical knowledge was . . . . (Participant 1)
Theme 3: Benefits of Intercultural Care
Students stated that their experience caring for immigrants in the immigrant health center increased their awareness and professional satisfaction and helped them overcome prejudices toward immigrants.
Awareness
Nursing students stated that they got an appreciation of immigrants’ hardship and assistance needs: As I listened to their stories and watched their experiences, I recognized that what they went through was quite painful. They are distant from their own country and trying to adapt to a different culture; such things are complicated. Even attempting to understand them made them pleased when we contacted them. It would be great if we could help them out more. (Participant 7)
Professional Satisfaction
The students said that having more opportunities to engage in professional procedures, such as taking blood, injections, and transfer of information transmission, boosted their professional satisfaction: At the migrant health center, I performed several interventional operations, such as bloodletting, vascular access, injections, and immunizations. Because we lack experience, Turkish patients do not allow us to perform such things. However, the employees supported us here, and the immigrants allowed us to do so. (Participant 20)
Dissolving Prejudices
The students stated that they had preconceptions toward immigrants before giving treatment in an immigrant health center but that their prejudices diminished after providing care to the immigrants.
You hear reports on social media or elsewhere about immigrants starting fights, stealing, and annoying people. When people observe such things, they are bound to acquire prejudices toward immigration. However, after I started practicing here, my ideas changed. In other words, among the immigrants, some fight and steal. However, some individuals misbehave in every community. When I observed the struggles of immigrants here and the smiles on their faces after caring for them, everything changed for me. (Participant 19)
Theme 4: Recommendations
Following their program at the migrant health center, the students discussed the centers’ service delivery and their recommendations for using student nurses:
Service Delivery
Students discussed migrant health centers for improving the services they give to immigrants: Immigrant health centers are newly built, and all the vehicles are new.” What do they do at home, for example, and where do they live? They should investigate. Home visits are often discussed in the classes, but I have not seen anyone go throughout my internship. Furthermore, studies should be conducted to inform immigrants of the practices here. (Participant 6)
Student Practice
The students discussed their ideas for improving future student practice at immigrant health centers: Caring for individuals from different cultures was a great experience for me. However, at the immigrant health center, I sometimes felt inadequate. In this case, it would be preferable if someone I could rely on was constantly present. Okay, our teacher came to the center where we practiced occasionally, but it would be nice if she came more often. (Participant 21)
Discussion
The students claimed that they experienced intense anger when giving the immigrants health services and nursing care, a significant obstacle to delivering quality nursing care. Students believe that immigrants did not fight for their home country and posed a risk regarding access to limited resources, particularly shelter. This anger toward immigrants worldwide comes from students and is common among all population segments. The unexpected and rapid increase in the number of refugees, in particular, has caused problems in meeting basic needs, such as health, education, and transportation (Baranowski et al., 2018). Furthermore, the supply chain has been and continues to be interrupted due to the pandemic, and economic indicators have suffered (Buheji et al., 2020). Some students felt terrible about their preconceptions and unfavorable perceptions after having time condition encounters with the immigrants. The students’ negative beliefs and views may vanish due to their contact with the immigrant for the same reasons that drive their rage. Although this circumstance demonstrates a beneficial advantage of the program, traumatic events and the immigrants’ experiences negatively affected students and sometimes made it difficult for them to maintain a professional attitude.
Students would understandably experience difficulties caring for individuals from different cultures who do not speak the students’ language. To mitigate the language problem, Arab-speaking students were equally distributed across the groups during the student rotations; however, the language problem persisted. Different studies conducted with health care professionals (physicians and nurses) who provide service to immigrants and immigrants who are service recipients found a similar experience of language and cultural differences impeding health service delivery (Çavuşoğlu et al., 2018; Doğan et al., 2017; Sevinç, 2018; Tuzcu & Bahar, 2015). To avoid this difficulty, several nations have recruited expert interpreters; otherwise, similar to the center where our study was conducted, health care services are delivered by immigrants to immigrants by employing immigrant health professionals (Berbel, 2020; Motsaanaka et al., 2020). However, according to student statements, the difficulties in delivering health services due to language and cultural differences continue. When the students’ statements are examined, it is discovered that there is theoretical weakness in establishing and maintaining therapeutic interactions, developing effective communication methods, dealing with ethical problems, and performing data collection interviews. These are the areas where theoretical knowledge would be most beneficial for patient–nurse interactions with people from different cultures, rather than medical terminology and understanding of the diagnostic and treatment process. Similarly, it was found in another study on cultural sensitivity in Greek nursing students that the nursing education curriculum needs to teach more theoretical knowledge on providing care to people from different cultures (Kotrotsiou et al., 2020).
Students typically said that they had previous experience with immigrants in social settings and that immigrants were mainly in the minority in the settings they were in. However, when the students practiced at the immigrant health center, they felt alone, helpless, and confused, particularly at the start of the program. Students get an understanding of immigration challenges, such as anxiety about the future, decreased social status, loss of family and social support, language problems, cultural adaptation and adaptation difficulties, efforts to adapt to a new culture, and perceived discrimination via theoretical education. When students learn about these negative experiences through direct transmission from immigrants, they benefit from long-term mutual interactions that increase their awareness. Relevant literature emphasizes the benefits of contacting people from different cultures to increase cultural awareness (Yilmaz et al., 2017). Our study went beyond understanding cultural awareness to emphasize some of the psychosocial problems that immigrants experience.
Because immigrants have been in Turkey for many years and have a population of 4 million (International Organization for Migration, 2023), their social environments have formed students’ cultural awareness even before they start the practice. Although it is acknowledged that the negative attitudes and prejudices toward immigrants continue, providing health services to and interacting with immigrants at the immigrant health center has increased the student’s professional satisfaction and helped dissolve prejudices. The positive feedback from the immigrants significantly contributed to the students’ professional satisfaction because they often received negative feedback from Turkish patients due to their student status. This increased the students’ internal motivation and encouraged them to feel valuable while providing a relevant program for the immigrant community. Other studies with nursing students had similar results (Backlund & Olausson, 2021; Kuru Alici & Öztürk Çopur, 2023).
Migrant health centers are primary health care delivery organizations that provide health promotion, preventive health services, diagnosis, treatment, and rehabilitation services in one place. According to the students, there was less emphasis on preventive health services and more emphasis on diagnosis and treatment. The students also criticized health services that were always limited to taking place at a medical facility; they believed that home visits would be a more effective way to provide services because they could see the patients in their homes.
This situation contradicts understanding optimal health and transitioning from a biomedical to a biopsychosocial model. However, immigrant health centers are a relatively new entity that tries to provide services with limited personnel; thus, access to home care may be a step for the future. The student experience in the immigrant health program was the focus of the second subtheme for improvement. Students generally agree that the practices at the immigrant health center should be carried on for the next generation of students. However, they thought that they required more support from their instructors at the immigration health service center. They believed that doing so would help them solve some of the problems they had faced during the program (communication problems, a lack of theoretical knowledge, and adapting to the environment). This recommendation applies to students in the immigrant health center and those in other clinical units. Previous studies found that students’ feedback encouraged teaching staff to spend more time in program centers (Altundal et al., 2022; Öner & Karabudak, 2021).
Implications for Nursing Education
Nursing students provide nursing care to people from different cultures in their clinical practice, despite their low resources. Due to the importance of said students’ cultural values, gaining awareness and competency for different cultures in these practices might be challenging. In this respect, implementing practices at institutions where immigrants receive services can be crucial in improving awareness. In addition to the theoretical education provided to students as part of the standard curriculum, supportive activities, such as courses, seminars, and case studies on topics such as intercultural care, communication with immigrants, and ethics, can be developed. Therefore, students may put their conceptual knowledge to the test while caring for people from different cultures. Planning these practices early in their education will provide more opportunities for faculty to intervene in areas where students have difficulty or feel lacking in intercultural care in the future.
At the same time, students expressed concerns regarding in-home visits, which are vital in providing and planning health services for immigrants in general. Hence, it is recommended that a section for home visits be included in the appropriate course curriculum and that students’ home visits be accompanied by a staff appointed by the immigrant health center or the school. Finally, it is believed that providing students with mentors who can be role models and provide consultancy in areas where students may encounter challenges, such as communicating (i.e., immigrant health centers), is necessary for these practices. Considering the positive results of mentoring programs in nursing education in previous studies, it is plausible to conclude that the mentoring program in transcultural care can be effective in nursing education (Bulut et al., 2010; Huybrecht et al., 2011; Sawatzky & Enns, 2009). Thus, it will directly contribute to training nurses with high cultural sensitivity in globalizing conditions and indirectly improve nursing care quality.
Conclusion
After migration, immigrants and native-born people of the host country face cultural, political, economic, and sociological issues. To improve health services after migration, education provided during the student period is important in providing effective and high-quality nursing services when mutual relations are challenging. In this study of Turkish nursing students’ experiences providing long-term care to immigrants, students struggled to manage their emotions at the start of the program due to cultural differences; however, there was a significant improvement in nursing services later in the program, such as empathy, professional satisfaction, a decrease in prejudices, and an understanding of the importance of preventive health services. In this regard, the educational institution should provide opportunities for nursing students to interact with immigrants starting during their studentship. This will train nurses who act on equality principles, have a high cultural sensitivity and awareness, and provide service regardless of a patient’s ethnic origin and background.
Footnotes
Author Contributions
The authors’ statement of contribution rate is as follows: Conceptualization: A.T., E.Ü.; Project administration: A.T.; Supervision: A.D.; Data curation: E.Ü.; Formal Analysis: A.T., A.D.; Resources: E.Ü.; Writing—original draft: A.D., A.T.; Writing—review and editing: E.Ü., A.D.; Funding acquisition: A.T.
Data Availability Statement
We affirm that the methods used in the data analyses are suitably applied to their data within their study design and context, and the statistical findings have been implemented and interpreted correctly.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.