
Abstract
Introduction:
Limited research on experiences of women, who constitute a double vulnerable group in both women and refugee status, regarding sexual and reproductive health. The purpose of this study is to examine the knowledge, beliefs, and cultural practices of Afghan women living in Türkiye regarding sexual and reproductive health.
Method:
This descriptive phenomenological study was conducted with 18 Afghan refugee women. In-depth, semi-structured interviews were conducted to collect data.
Results:
Four themes emerged from interviews: cultural practices and beliefs related to pregnancy and postpartum, use of contraceptive methods, gender-based violence, and access to health services.
Conclusions:
Afghan women have different cultural practices regarding prenatal, pregnancy, and postpartum and lack of knowledge about sexual and reproductive health. Considering individual differences in sexual and reproductive health, providing sensitive, supportive, and informative services is recommended.
Introduction
Globally, by the end of 2021, 89.3 million people were forcibly displaced due to conflict, violence, fear of persecution, and human rights violations, and around 27.1 million were refugees (United Nations High Commissioner for Refugees [UNHCR], 2021). Türkiye hosts the largest number of refugees in the world and 4 million people under temporary protection and international protection in Türkiye. Afghanistan has the second-highest number of international protection applicants in Türkiye, with 133.062 Afghans under international protection status (UNHCR, 2022). Currently, Afghans constitute one of the largest refugee populations worldwide, with 120,000 Afghans having fled the country after the collapse of the Afghan government and the Taliban takeover in August 2021 (UNHCR, 2021). As of July 2023, UNHCR (2023) estimates that 5.2 million Afghan citizens were refugees and asylum seekers in neighboring countries. Attention to the specific needs of Afghan refugees is therefore critical.
Afghanistan was one of the countries with the highest maternal mortality in 2017 (World Health Organization [WHO], 2017). Maternal and infant mortality is projected to increase by 50% (from 638 to 963 deaths per 100,000 live births) by 2025 in the absence of comprehensive intervention. This increase translates into a woman dying every 2 hr from childbirth or pregnancy complications in Afghanistan (WHO, 2022).
Pregnancy and childbirth complications are the leading cause of death and disability among women of childbearing age in developing countries. Seventy-five percent of these deaths are due to severe bleeding, infection, high blood pressure, complications from childbirth, and unsafe abortions (WHO, 2023). In addition to pregnancy and childbirth complications, the causes of maternal mortality in Afghanistan include very low rates of women receiving antenatal care, women’s lack of or limited access to basic health services, poverty, unequal access to resources, low status, low education level and cultural factors (Ackerson & Zielinski, 2017; Neyazi et al., 2022; WHO, 2022).
Although migration to Türkiye changes the status of Afghan women, low education level, unequal access to resources, differentiation in health service delivery, language barriers, and cultural factors affect Afghan women’s sexual and reproductive health (UNHCR, 2021; Yağmur & Aytekin, 2018). For these reasons, it has been reported that women in the minority group have less and later access to maternity care services compared to the local population, are less likely to give birth in health facilities compared to the local population, and are more likely to experience perinatal and intrapartum complications. There are significant differences between the maternity care women expect and receive (Huang et al., 2018; Raleigh et al., 2010; Toh & Shorey, 2023; Yağmur & Aytekin, 2018). Indeed, even when health services are accessible, it is stated that women do not utilize these services, which may be related to women’s cultural beliefs, knowledge, and attitudes (Engmann et al., 2013; Withers et al., 2018). Although the reasons for the underutilization of health services are many and complex, sociocultural barriers to accessing health services and information need to be overcome to prevent maternal mortality and morbidity (WHO, 2018). As a result of reproductive health and sexual health being shaped by sociocultural values, pregnancy and postpartum processes are also highly influenced by cultural values and beliefs. In fact, pregnancy and the postpartum period involve deeply rooted health practices and beliefs (Engmann et al., 2013).
Culture is an integrated model of learned beliefs and behaviors that can be shared across groups. It includes ideas, communication styles, ways of interacting, views about roles and relationships, values, practices, and traditions. Improving cultural competence in health professionals, institutions, and agencies working with refugees is important to improve the health of refugees (Matlin et al., 2018). It is reported that women and their families express higher levels of satisfaction and have higher rates of health service utilization when all women, regardless of country of origin, are provided with respectful and culturally competent services (Ackerson & Zielinski, 2017; Culhane-Pera et al., 2015). Systematic reviews emphasize the need to illuminate local contexts, cultural beliefs, and social experiences to understand people’s preferences for maternity and family planning services (Gabrysch & Campbell, 2009; Say & Raine, 2007).
Sexual and reproductive health is an important global health priority addressed by Sustainable Development Goals 3, 5, and 10. To achieve these priorities and leave no one behind, it is imperative to address the sexual and reproductive health needs of refugees and migrants (United Nations, 2015; WHO, 2017). Context-specific research from different geographical regions is needed to develop maternity policies and emergency practices targeting minorities and to ensure a holistic view of women’s needs and how they are well supported (Toh & Shorey, 2023). The existing literature emphasizes the need for studies that represent the experiences and needs of women, who constitute a double vulnerable group in both women and refugee status, regarding sexual and reproductive health. Therefore, the purpose of this study is to examine the knowledge, beliefs, and cultural practices of Afghan women living in Türkiye regarding sexual and reproductive health.
Method
This study was designed as a phenomenological study. Phenomenological designs are a powerful research strategy for exploring challenging issues for health professionals (Neubauer et al., 2019). Phenomenology aims to describe the essence of a phenomenon by exploring it from the perspective of those who experience it, in terms of what the meaning of the experience is and how it is experienced (Teherani et al., 2015). In the reporting process of this study, the COREQ (CONsolidated criteria for REporting Qualitative research) guidelines (Tong et al., 2007).
Sample and Setting
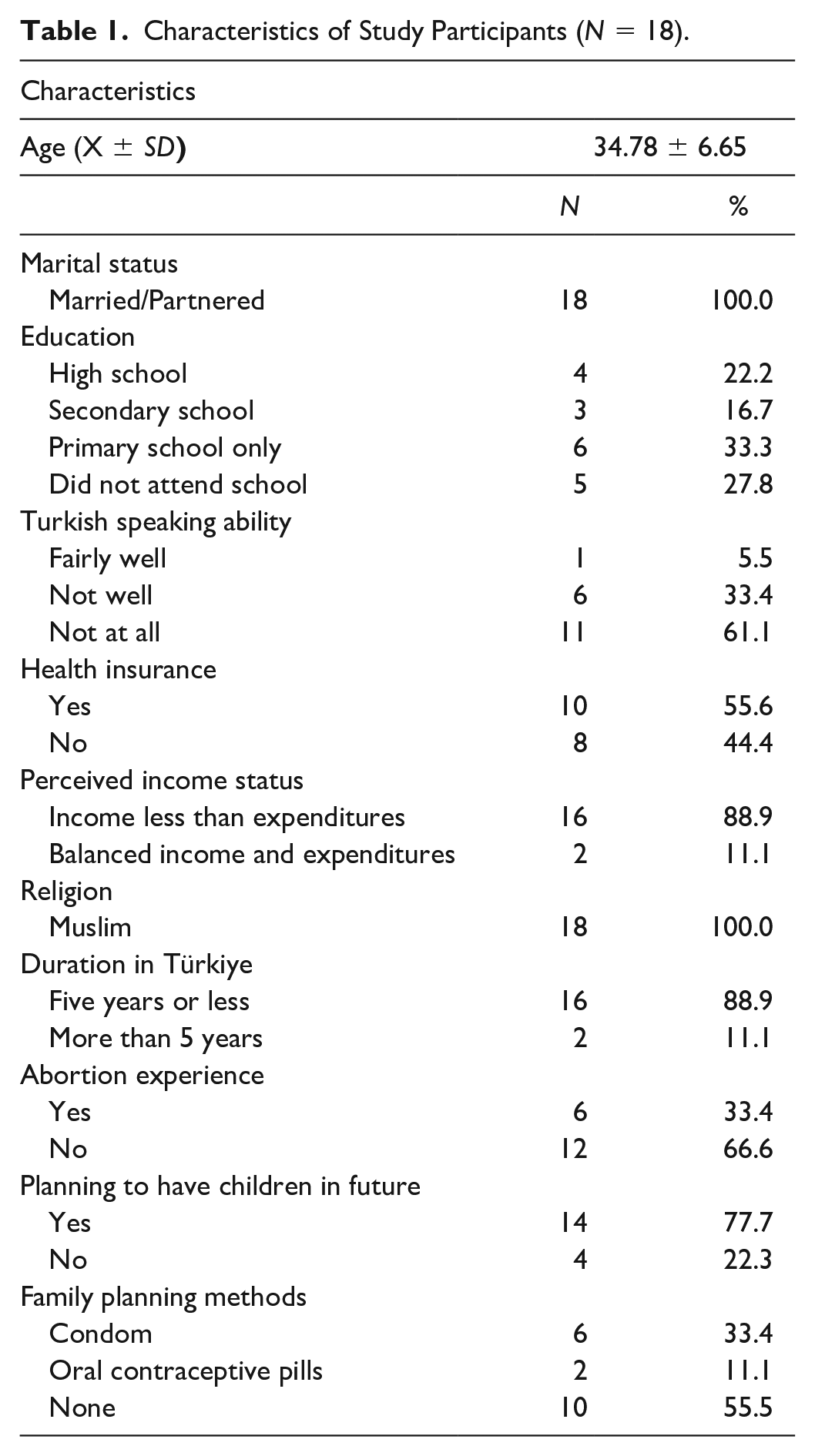
The sample of the study consisted of Afghan refugee women registered with the Refugee Support Association of Türkiye, determined by purposive sampling method. The inclusion criteria were (1) being an Afghan refugee woman, (2) having a history of pregnancy and childbirth, and (3) volunteering to participate in the interviews. The researcher’s field experience, conceptual framework, and existing literature guided the initial sample selection for the study. Data analysis started with the first data collected and guided the initial analysis results into the sampling process (Gibbs et al., 2007). Sample diversity was assured by purposely selecting participants in maximum variation to provide a broader understanding of the phenomenon under study (Graneheim & Lundman, 2004). Eighteen Afghan refugee women participated in the study, and their ages ranged between 27 and 45 years, with a mean age of 34.78 ± 6.65 years. Sociodemographic data are shown in Table 1.
Characteristics of Study Participants (N = 18).
Data Collection
Data were collected between September and November 2022. Afghan refugee women who previously received counseling services from the association that met the inclusion criteria were called by the second researcher. Afghan refugee women who met the criteria and were willing to take part study were invited to participate in the research. After explaining the purpose and method of the study, an interview appointment was arranged with those willing to participate at a mutually appropriate time and date.
Data were collected through a semi-structured form. The form consisted of two parts: the first part included sociodemographic data and the second part consisted of semi-structured questions about the participants’ knowledge, beliefs, cultural practices, and experiences related to the sexual and reproductive health of Afghan refugee women.
Afghan refugee women who participated in the study participated in the interviews in a quiet room in the association, with the support of a sworn translator, and the interviews were conducted through the Zoom Meeting program and recorded. Before the interviews began, the interpreter was informed about the study process, and a pilot study was conducted. The interviews lasted an average of 40 min (35–45) and were then transcribed verbatim by the 2nd researcher for analysis after every meeting. No repeat interviews were conducted. Data collection was continued until no further new relevant information can be identified, data saturation was achieved in the 18th interview and the study’s sample size was determined. (Saunders et al., 2018). None of the participants recruited dropped out of the initial interviews.
Semi-structured interviews were conducted by the principal investigator (PI), a female Ph.D. graduate in public health nursing with experience in qualitative research and working as an Associate Professor in Nursing Faculty in different cities with participants. The second researcher of the study is a male nurse with experience in the field of refugees who works as a health educator in the Refuge Support Association, has certificates, especially in women’s health education, and works with male and female refugees in the field within the scope of this subject, and is a graduate student in public health. The interpreter who did the translations in the study was a woman with a bachelor’s degree who can speak and write both Turkish and Farsi, has a degree in interpreting, and has experience working in the Refuge Support Association.
Data Analysis
The latent content analysis was chosen for analysis and interpreting the meaning of the data (Graneheim et al., 2017; Graneheim & Lundman, 2004). In latent content analysis, the researchers try to describe the relationship aspect and involve an interpretation of the underlying meaning of the text (Graneheim et al., 2017; Kleinheksel et al., 2020). Based on the aim of the study, data analysis and meaning units were started as soon as the first interview was completed. The researchers individually and separately read the data from each interview form repeatedly from start to finish to obtain the meaning of the whole and to become familiar with the meanings within the interview. The meaning units were identified by the research team through re-reading the transcribed material several times and discussing the groupings and the findings. Colored pencils were used to examine how well the texts and inferences were aligned with the meaning units. The researchers focused on the meaning units, identified themes and subthemes, compared the themes and subthemes created by the researchers, and discussed them until a consensus was reached. In the final stage, comparisons were made between the compilation, individual interviews, and subthemes, and all subthemes were reorganized to better identify similarities and differences. All the data was then synthesized so that a single analysis emerged, and the themes were common to the interviewees (Lindgren et al., 2020).
For each theme, the researcher provided quotes from different participants to add transparency and credibility to the findings and interpretation of the data. During transcription, a pseudonym was assigned to each participant to guarantee confidentiality (Graneheim et al., 2017). To establish transferability, participants with varied backgrounds were included, including variation in age and education. The reliability of the study was intensified by the research team by re-reading the transcribed material several times and discussing the groupings and the findings (Graneheim & Lundman, 2004).
Ethical Consent
This study was approved by the Ethics Committee of a Public University (No. 2022/11). The researcher explained the purpose of the study, the confidentiality of the data, the voluntary nature of participation, and their freedom to discontinue the interview or withdraw from the study at any time without reason. The interviews were audio-recorded, and verbal and written consent was obtained from each participant before audio-recording the interviews. Transcribed data were saved to Google Drive™ and stored on software password-protected laptops for 5 years by the second author.
Results
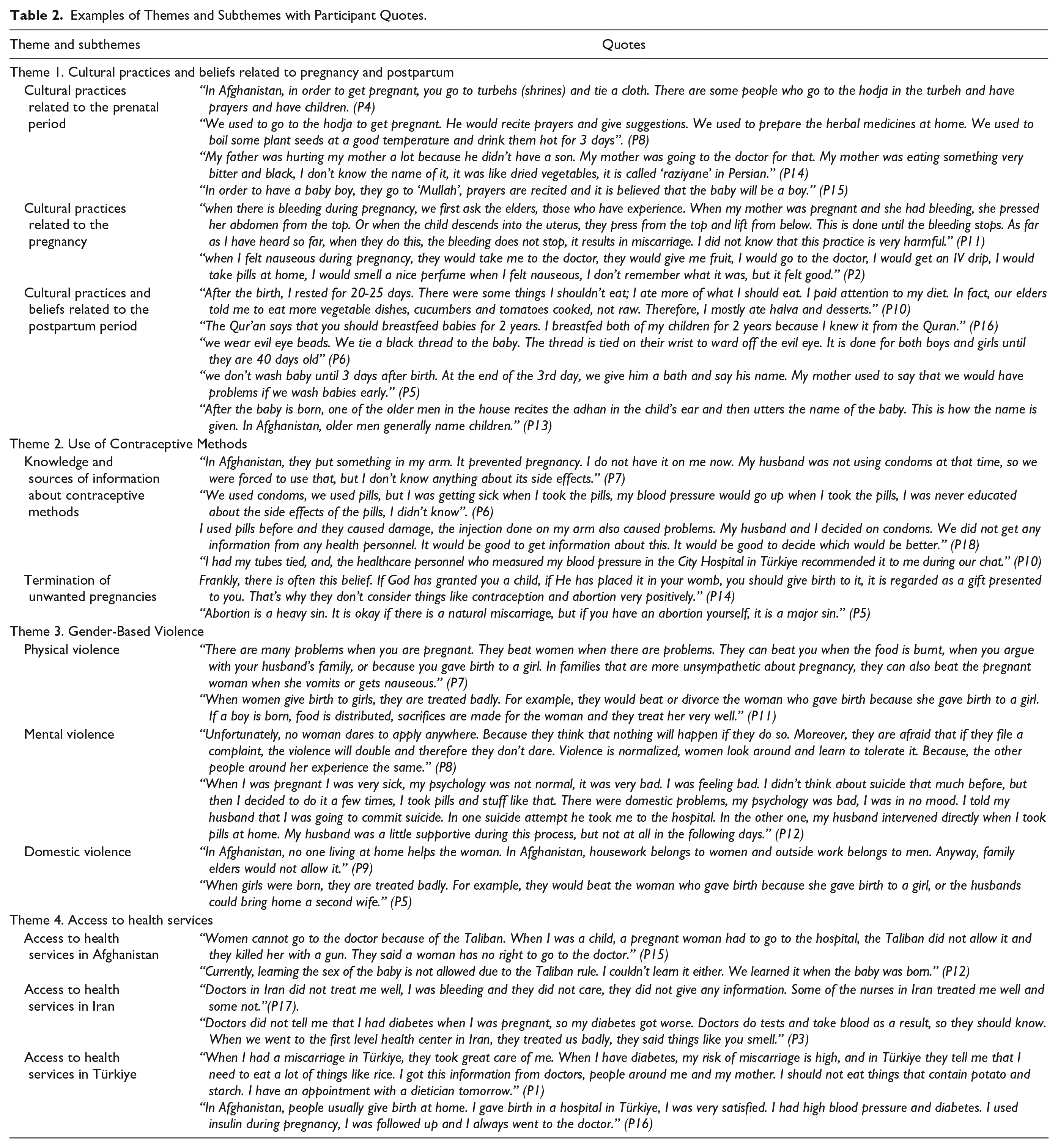
Four themes and subthemes related to each theme were formed from the data of the study conducted with Afghan women. Examples of themes and subthemes with participant quotes are presented in Table 2. The themes of cultural practices and beliefs related to pregnancy and postpartum, contraceptive method use, based-gender violence, and access to health services, and subthemes related to each theme are given in Figure 1.
Examples of Themes and Subthemes with Participant Quotes.
Representation of the Themes and Subthemes.
Theme 1. Cultural Practices and Beliefs Related to Pregnancy and Postpartum
In this theme, the cultural practices of Afghan women regarding the pre-pregnancy, pregnancy, and postpartum periods were included. Women’s experiences are presented in three subthemes as cultural practices related to the prenatal period, cultural practices related to the pregnancy and cultural practices related to the postpartum period.
Cultural Practices Related to the Prenatal Period
In the prenatal period, women resort to different ways to conceive and have a male baby. One of the cultural practices that Afghan women frequently use to conceive is to ask the hodja (Muslim clergyman) in the shrines to recite prayers. It is quite common that the prayers recited by the hodja and herbal prescriptions given by the hodja are prepared and consumed by women at home. In Afghanistan, the gender of the male child is very important, so there are practices that women do before pregnancy to have a male child. In food-related practices, it was found that Afghan women characterize food as hot and cold according to their culture, regardless of the temperature of consumption, and they think that hot foods are effective for giving birth to a male child.
Cultural Practices Related to the Pregnancy
The cultural practices and beliefs of Afghan women regarding their experiences after pregnancy are given under this theme. It is stated that in solving the problems faced by Afghan women during pregnancy, family elders are often consulted first or health institutions are rarely consulted.
Cultural Practices and Beliefs Related to the Postpartum Period
There are different cultural practices for the mother and the baby in Afghanistan after childbirth. Practices learned from family elders shape the mother’s postpartum care process such as feeding and resting. It was also found that women’s beliefs shape their behaviors toward feeding the baby. In Afghanistan, the belief that newborn babies can be touched by the evil eye is quite high. Women stated that they wear evil eye beads, have evil eye prayers read, burn incense, and perform herbal practices to prevent the evil eye on the baby. Among the practices regarding the care process, after the baby is born, it is seen that there are traditional practices regarding the baby’s naming ceremony and care. Mothers stated that they swaddled their babies, that the shower time was determined by the elders, and that kohl should be applied to the baby’s eyes after the baby was born.
Theme 2. Use of Contraceptive Methods
The theme on contraceptive use among Afghan refugee women has two subthemes: knowledge about contraceptive methods sources of information and termination of unwanted pregnancies.
Knowledge and Sources of Information About Contraceptive Methods
Almost all women don’t know what contraceptive methods are, their purpose of use, how they, are used, or what their side effects are. Women did not receive structured training from health personnel in Afghanistan and Türkiye, and their first point of contact for method use was their family or circle of friends.
Termination of Unwanted Pregnancies
It was stated that women’s religious beliefs are an effective decision mechanism. The baby is a gift; it is a sin for women to have an abortion unless there is a health problem. Women do not have the right to terminate unwanted pregnancies, and they may be considered murderers. Women try to terminate unwanted pregnancies with their own methods.
Theme 3. Gender-Based Violence
Afghan women stated that they were subjected to physical, mental, and domestic violence during pregnancy because they were women.
Physical Violence
Afghan women stated that they were subjected to physical violence in case of disruptions in the execution of household chores due to problems encountered during pregnancy or in the presence of pregnancy symptoms.
Mental Violence
Women experienced mental health problems during pregnancy, were not supported by their husbands or family members, had to accept the violence, and that they had no support mechanisms to break the cycle of violence.
Domestic Violence
Women are subjected to domestic violence and it is reported that violence is perpetrated by family members or elders.
Theme 4. Access to Health Services
The women participating in the study expressed their access to health services related to sexual and reproductive health in Afghanistan, Iran, and Türkiye.
Access to Health Services in Afghanistan
The restrictive policies of the Taliban government, the country’s perspective toward women, and the limited availability of free health services prevent women from accessing health services related to sexual and reproductive health.
Access to Health Services in Iran
Some of the Afghan women, who had lived in Iran before coming to Türkiye, stated that they generally experienced problems in accessing health services in Iran too, due to health service personnel (such as prejudice, trust issues, unethical behaviors, xenophobia) and health service fees (paid access due to lack of health insurance or lack of identification).
Access to Health Services in Türkiye
It was found that Afghan women in Türkiye generally have access to health services, are followed up before and especially during and after delivery, and are mostly satisfied with the services provided.
Discussion
The purpose of this study is to examine the knowledge, beliefs, and cultural practices of Afghan women living in Türkiye regarding sexual and reproductive health. Afghan women stated that to get pregnant or to have a baby of the male gender, prayers are recited from the hodjas in the turbehs, herbal medicines are prescribed by the hodjas, and they consume foods in the “hot” group in their diets.
Although the classification of foods as hot and cold is an old practice among Afghans, it is thought that in this classification, which is still in use, foods are classified as hot and cold according to the amount of heat they produce as a result of their metabolic activities in the body. Accordingly, hot foods generally include foods with high calories and made with flour, while cold foods are foods with high water content such as vegetables, fruits, and green tea (Metro South Health, 2016). In a different study, Afghan women reported that pregnancy is seen as an indicator of reproductive system functioning, while a similar social perspective attributed to pregnancy is seen in low- and middle-income countries (Shafiei et al., 2012). A Sudanese woman stated that not getting pregnant immediately after marriage can be a big problem, while Iraqi women stated that pregnancy is seen as a test for them and they are expected to have children immediately after marriage (Ngum Chi Watts et al., 2015; Shafiei et al., 2012).
The study emphasizes the importance of Afghan women not only getting pregnant but also bringing a male child into the world. Families with no or few male children are perceived as weak and stigmatized, and women are often accused of being “effeminate” and seen as a burden on the family (Lalthlamuanpuii, 2020). When the Afghan family structure is examined, we come across a social structure in which women are responsible for producing male children in a male-centered structure (Sindhu, 2018). Similarly, in patriarchal societies, a key component of the value placed on boys is the role they can play in the economic productivity of the household. As an important finding of our study, it was reported that parents do not care about child gender after migration to Türkiye. Similarly, Afghan women who migrated to Australia reported that their husbands did not care about the gender of their children, suggesting that their strong preference for male children was relaxed to some extent after the migration (Hamidi et al., 2021). This shows that the culture of the new society and its view of gender inequality can change the perspective of migrant families on gender inequality.
Afghanistan is one of the countries where Intimate partner violence (IPV) is most common (WHO, 2021). In this study, Afghan women were subjected to physical, emotional, and domestic violence by their husbands and other family members because they could not conceive, because of the symptoms they experienced during pregnancy, or because they gave birth to a girl child. In another study, one out of every two Afghan women had been subjected to physical, emotional, and IPV in the last year (Dadras et al., 2022). Gender inequality, a patriarchal society, ongoing civil conflict, early marriage, poverty, and low literacy explain the high levels of violence against women in many resource-poor countries (Qamar et al., 2022). In addition, it has been reported that IPV+ women have less access to contraceptives and more unmet family planning needs than IPV− women (Akbary et al., 2022; Dadras et al., 2022; Ibrahimi & Steinberg, 2022). This may be explained by the fact that abused women are more likely to engage in risk-taking behaviors in general, whether by choice or coercion (Stubbs & Szoeke, 2022).
In Afghanistan, knowledge about contraceptive methods among married and non-pregnant women is inadequate and utilization rates are quite low. In this study, it was found that among migrant Afghan women, knowledge on sexual and reproductive health was insufficient, women needed information on this subject and the means of access to information were internet sources and information they received from their relatives/relatives who they thought were experienced. Similarly, women reported that they directly use the internet and Google for information on maternal and infant health (Rostamzadeh et al., 2022). Poverty, low education level, and young age are influencing factors (Rasooly et al., 2015). The low education level and young age of the women in the study may have affected the results of the study.
In the study, Afghan women either terminate unwanted or unplanned pregnancies or give birth as a gift from God. Women reported that abdominal compression, heavy housework, jumping from heights, and consuming herbal medicines were commonly used as methods to terminate unwanted pregnancies in their communities. Similarly, Ethiopian women use traditional practices to terminate unwanted pregnancies, including abdominal massage, the use of herbs, and heavy physical exercise (Solomon & Tesfaye, 2022). There are studies showing that abdominal massages performed by non-specialists can cause fetal and maternal morbidity and mortality (Amadi et al., 2022; Banul & Halu, 2020). It is seen that the religious beliefs and attitudes of all participating Muslim Afghan women who wanted to continue pregnancy influenced this decision. Afghan women reported that the baby was sent by God and that it was a sin to terminate the pregnancy against their will. According to studies, Muslims are more likely to have unintended pregnancies than Christians, while other studies have suggested that Christians (Catholics and other Christians) are more likely to have unintended childbearing than Muslims (Alene et al., 2020; Bain et al., 2020; Oyediran et al., 2020).
In this study, women reported limited utilization of health services related to sexual and reproductive health, but they were more satisfied with the care and resources provided by maternity services in Türkiye compared to health services in Afghanistan. While most women stated that they found the care provided by staff and maternity services in Türkiye to be better than in Afghanistan and Iran, interview findings indicated that interactions with staff were critically important in Afghan women’s experiences of maternity care. Even if the women did not speak the same language as the health personnel, positive gestures and facial expressions of the health personnel were found to affect the level of satisfaction. Although access to health services in the country of immigration is more accessible than in the country of origin, women were found not to receive services. Structural factors such as distance or financial constraints constitute barriers for Asian women to access health services related to pregnancy, childbirth, and the postpartum period, while traditional beliefs and practices related to pregnancy and childbirth also have a negative impact on access to health services (Withers et al., 2018). A different study found that the use of interpreters in the provision of obstetric health services is low, thus jeopardizing the exchange of important information. It is supported by studies that Afghan women have difficulties communicating with health professionals and that there is not enough quantity and quality of interpreters (Riggs et al., 2020).
Conclusion
In this study, it was determined that Afghan women have different cultural practices regarding prenatal, pregnancy, and postpartum and lack of knowledge about sexual and reproductive health. It is important for health care providers to be aware of Afghan women’s cultural practices regarding sexual and reproductive health and to provide culturally based health care services. Afghan women’s access to sexual and reproductive health services needs to be supported. Considering individual differences in sexual and reproductive health, providing sensitive, supportive, and informative services is recommended. It can be achieved by planning home visits or visits to health facilities before, during, and after delivery, considering language barriers, and allocating enough time to allow women and their partners to ask questions and receive adequate information and explanations. More supportive, respectful, and compassionate care by health care providers will likely increase women’s satisfaction with their care experiences. Moreover, interventions to improve health literacy of Afghan women’s might include offering, sexual and reproductive health education in mother tongues and using written-visual teaching materials. It is also recommended that women’s use of the internet as a means of accessing information should be informed about access to accurate information and useful websites, in addition to increasing the number of reliable sources of information for the public in Persian.
Limitation
The study focused on refugees from Afghanistan in one region of Türkiye. The fact that the women who agreed to participate in the study were clients who were already receiving various psychosocial and financial support from the existing association, the proximity of the association to the Provincial Migration Management building, and the participants’ fear of deportation may have contributed to their inability to provide unbiased data. Fear of being unable to access those services provided by the associations may have contributed to their inability to provide unbiased data. However, the association has a right-based approach and safe space policies. Although it is difficult to assess the generalizability of the results, it shows that many of the problems identified are also applicable to other communities at the national and international levels. Moreover, since the birth experience of Afghan women occurs not only in Turkey but also in different countries such as Iran and Afghanistan, it should be considered when interpreting the results.
Footnotes
Acknowledgements
The authors would like to thank the Afghan women who shared their knowledge and experiences during the interviews. Moreover, the authors thank the Refugee Support Association for the support, and the Embassy of France in Ankara.
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Embassy of France in Ankara provided financial support for the conduct of this research but did not provide any support in the writing of the article. Participants were provided €7 for participation for the purpose of preventing potential economic difficulties that can be caused because of absence at the workplace and the transportation fees.