
Abstract
Introduction:
Staff shortages and retention are the major challenges in residential aged care facilities (RACFs). This study aimed to explore migrant care workers’ perceptions of job demands, their coping strategies, and employment intentions to leave or stay in the sector.
Methods:
Using a descriptive qualitative research design, semi-structured interviews were conducted with n = 20, RACF migrant care workers from Filipino, Indian, and Nigerian backgrounds in Perth, Western Australia, from April to December 2019. Data were thematically analyzed.
Results:
Motivating factors included the availability of care work in RACFs, and positive cultural norms associated with caring for older family members. Participants experienced a combination of resettlement and workplace challenges specifically, limited support network, communication challenges, and racial discrimination.
Relevance to Practice:
Work challenges that are compounded by post-migration stressors should be recognized and addressed in the design and implementation of the aged care workforce reforms to attract and retain migrant care workers.
Introduction
Recruiting and retaining care workers in the aged care sector has been a challenge in high-income countries, and this will intensify as the demand for care increases with the population aging (Wilson et al., 2020). By 2066, the global population of people aged 65 and above will be around 10 million (Wilson et al., 2020). Concomitant with population aging, there will be chronic age-related conditions resulting in multiple medical conditions that require reliance on formal or informal support services (Roe et al., 2020). Both of these factors placed unprecedented demands on residential aged care facilities (RACFs; Roe et al., 2020).
RACFs provide significant long-term care for older people when other care services, such as outpatient hospital care and community and home-based care services, are no longer sufficient (Roe et al., 2020). Admission into a RACF is often associated with factors such as exacerbated illness or burn-out of family carers, rapid progression of challenging behaviors associated with dementia, safety issues, inappropriate accommodation, or an increase in the severity of dementia (Roe et al., 2020). These issues also render aged care workers’ duties in RACFs psychologically and physically demanding (Oppert et al., 2018), regardless of their cultural backgrounds. In addition, working in aged care is often socially perceived as low-status work and is associated with low job satisfaction and limited career development opportunities (Oppert et al., 2018). These negative factors often contribute to low workforce retention in RACFs.
With the declining availability of family members and other informal carers and the shortages of skilled personnel in aged care, many aged care employers utilize newly arrived migrants to help meet current and future care demands (Charlesworth & Isherwood, 2021). Similar to other high-income countries like the United Kingdom that rely on migrant care workers in their aged care sector (Turnpenny & Hussein, 2022), the Australian aged care sector is one of the most ethnically diverse with 35% of the RACF direct care workforce identifying as being from a culturally diverse background (Australian Government Department of Health, 2021). The discourse on the migrant workforce in the aged care sector focuses mainly on recruitment as a strategy to address labor shortages and does not focus on the needs of the migrant aged care workforce. Presently, a large proportion of migrant aged care workers working in high-income countries are from the Philippines (Mavromaras et al., 2017). India also has well-established patterns of supplying care workers to high-income countries (Mavromaras et al., 2017). In Australia, between 2011 and 2016, there was a substantial influx of migrant care workers from South Asia (333% increase) and sub-Saharan Africa (145%; Negin et al., 2016).
In 2020, the Australian Aged Care Workforce Census also reported that the majority of staff from culturally diverse backgrounds are personal care assistants (PCAs; 72%), followed by nursing and allied health staff (24% and 4%, respectively; Australian Government Department of Health, 2021).
It is well documented in the literature that migrant aged care workers are significantly disadvantaged (Charlesworth & Isherwood, 2021). They are more likely to work overtime, have limited control in choosing their shifts, and may engage in a higher number of night shifts compared with their native-born co-workers’ projection (Overgaard et al., 2022). Migrant care workers on temporary work visas are especially vulnerable as their employment is crucial to their residence in the host country (Charlesworth & Isherwood, 2021). In addition, migrant workers may experience psychological and cultural changes as a result of their continuous exposure to a second culture, a process known as acculturation (Doucerain, 2019). Acculturation is defined as a process of cultural and psychological changes that occur as a result of contact between two or more cultural groups and their members (Doucerain, 2019). These psychological changes can lead to stress known as “acculturation stress” in some migrants (Doucerain, 2019). Acculturation stress affects migrant care workers’ well-being (Doucerain, 2019) and may negatively affect their capacity to provide quality care to residents.
An Aged Care Workforce Strategy Taskforce established by the Australian Government recommended that policymakers should examine and respond to the different factors affecting the employment retention of specific cohorts of employees, including workers from culturally diverse backgrounds (Commonwealth of Australia, 2018). Given the need to expand the workforce in the aged care sector to meet the demands of an increasingly multicultural aging population (Wilson et al., 2020), it is essential to explore migrant care workers’ challenges in adapting to cross-cultural care practices in their settlement countries. Such findings would help the aged care sector to better understand the strategies needed to mitigate issues associated with staff shortage. This study aimed to explore migrant care workers’ perceptions of job demands in RACFs, their coping strategies, and employment intentions to leave or stay in the sector. The key research questions were as follows:
Method
Design
This research is part of a large mixed-methods sequential study exploring the psychosocial well-being and working conditions of migrant workers caring for older people in Australian RACFs, including those living with dementia. The descriptive qualitative study comprising semi-structured interviews was conducted between April and December 2019.
Study Setting
The study was conducted in Perth in Western Australia. Perth comprises approximately 79% of the Western Australian population and 8.58% of Australia’s overall population. Perth is Australia’s fourth-largest city in population size (Australian Bureau of Statistics, 2021).
Participants
Following Howe (2009), a migrant care worker was defined as an individual “born outside the country in which they are employed in frontline care work” (Howe, 2009, p. 6). Given their dominance in the aged care sector, migrant workers from Indian, Filipino, and Nigerian backgrounds were targeted for recruitment. The selection criteria were limited to participants who were migrant care workers, aged 18 and above, and first-generation migrants from the three nations mentioned above. Care workers who were second- or third-generation migrants (Australian-born individuals with at least one parent or grandparent born overseas) were excluded from the study.
Recruitment
Study participants were recruited from RACFs, ethnic groups, and multicultural support service organizations across Perth metropolitan areas. Advertisements were distributed via emails and social media, including Facebook, WhatsApp mobile apps, and LinkedIn. Participants were also recruited through the researchers’ networks. A purposive sampling technique was used to achieve maximum diversity by age, gender, locality, level of education, and job title.
Data Collection
Semi-structured interviews were conducted by the first author (B.A.), who is a Nigerian migrant to Australia and an experienced qualitative researcher. Information sheets were provided, and participants were encouraged to ask questions relating to their participation and to sign the consent form. Participants who requested to be interviewed via the phone were sent the information and consent form prior to the phone interviews, and verbal consent was provided by participants over the phone on the day of the interview. Face-to-face interviews were conducted at their workplace facility or a convenient place suggested by the participants. The duration of the interviews was between 30 and 45 min, and all participants consented to their interviews being audiotaped. Figure 1 lists the topics and questions asked during the interview. Care was taken by the interviewer to check the participant’s understanding of the questions and to rephrase or clarify as needed. Participants were given a token $20 gift card at the end of the interview to acknowledge their time. All interviews were professionally transcribed verbatim for analysis.
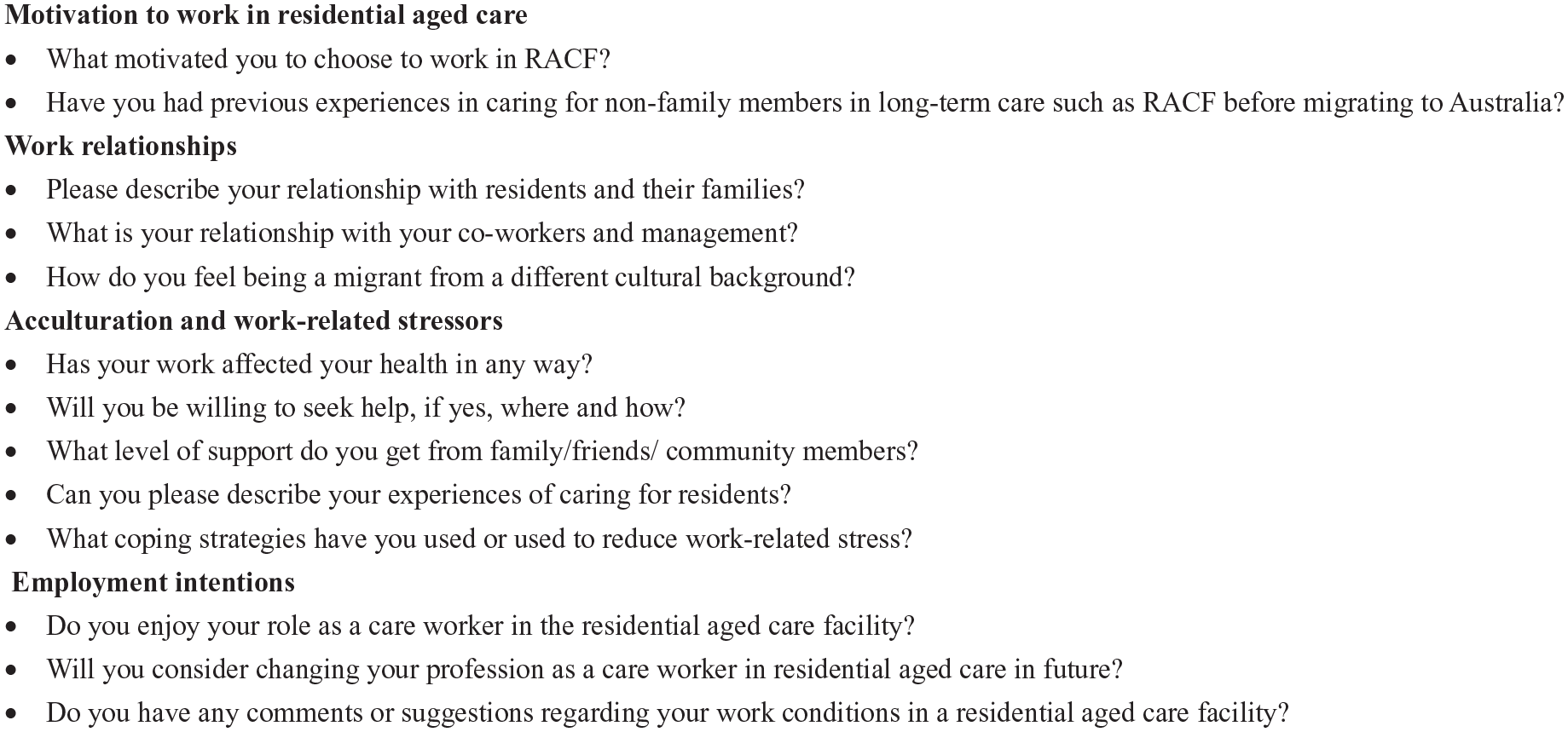
Interview Questions.
Ethical Considerations
This study was approved by the Curtin University Human Research Ethics Committee (HRE 2017-0863). Prior to giving consent, participants were informed that participation in the study was voluntary and of their rights to privacy, confidentiality, and the right to withdraw from the study at any time. All study materials including transcripts and other documents related to the participants were coded with an identification number to protect identities and ensure confidentiality.
Data Analysis
The qualitative data were analyzed using the essential steps outlined by Braun and Clarke (2006). The first author carried out data familiarization at the initial stage; preliminary codes were generated with the aid of NVivo version 12 software. Preliminary codes were developed and synthesized into categories and then expanded into themes. The third and fourth authors independently reviewed several transcripts and checked the accuracy of the coding categories. Theme development was informed by areas of commonality using keywords, phrases, and sentences. Using constant comparison, the researcher revised codes, examined the negative and positive findings, and connected codes together to explain themes (Vaismoradi et al., 2016). Constant comparison was applied to examine similarities and differences in perceptions between the three population groups. An iteration process involving a discussion between the first author and the other two authors resolved discrepancies that emerged during the phases of thematic analysis.
To improve the rigor of the study, the trustworthiness of the data collection, analysis, and interpretation process was enhanced through a peer debriefing strategy by having the transcripts assessed by the other two authors to verify the consistency of the results and accuracy of interpretation (Creswell & Miller, 2000). The content of the reflective notes was discussed with other chief investigators to clarify personal assumptions that might affect data collection and interpretations. The Standards for Reporting Qualitative Research (SRQR) was also used to improve the transparency of all aspects of reporting. The SRQR is an improved reporting tool for a broader range of qualitative studies (Dossett et al., 2021). The study findings were interpreted, and the authors’ decisions were clearly outlined in the “Discussion” section.
Results
A total of 20 migrant care workers employed in RACFs participated in this study. Fifteen were women and five were men. Nine were Nigerians, six and five were from Indian and Filipino backgrounds, respectively. Participants ranged in age from 25 to 45 years with an average of 32.2 years. The majority were PCAs, and more than three quarters (85%) had lived in Australia between 6 and 10 years. Table 1 summarizes the characteristics of the study participants.
Sociodemographic Characteristics of Qualitative Study Participants According to Nationality (n = 20).
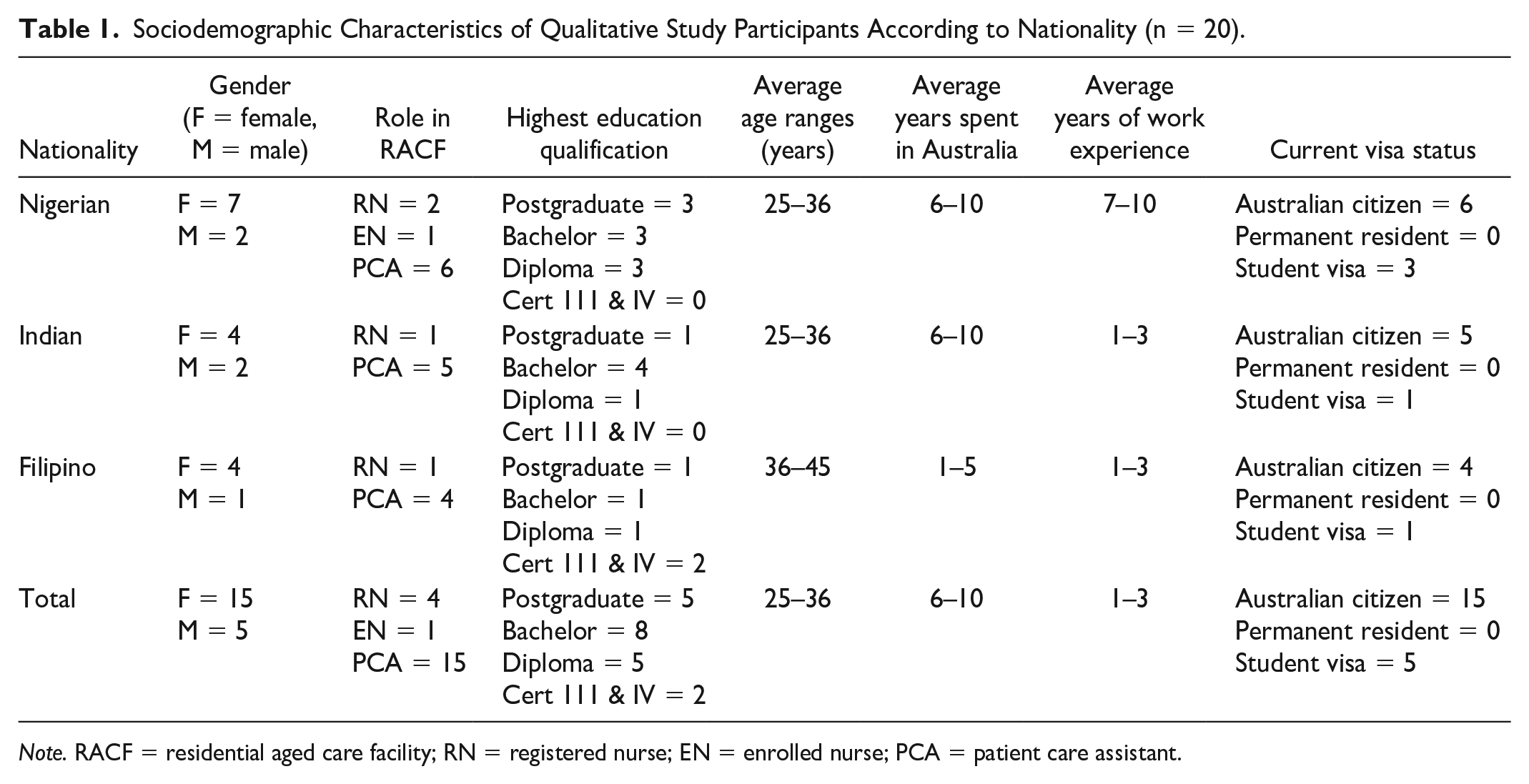
Note. RACF = residential aged care facility; RN = registered nurse; EN = enrolled nurse; PCA = patient care assistant.
An analysis of the interview data revealed a number of themes relating to care workers’ perceptions of working in RACFs as a migrant. These include motivation to work in RACFs, work-related stressors and resettlement challenges, and coping strategies deployed to mitigate these stressors. These themes also explain the high levels of acculturation stress and intentions to leave or reasons for having left employment in residential aged care.
Motivation to Work in RACF
Cultural Norms and Compassion
Some participants’ cultural values influenced their decisions and motivation to work in RACF. Drawing on their cultural values, our participants perceived residents as similar to their grandparents. Twelve participants, mostly women, indicated that they loved caring for their grandparents in their countries of birth, and their compassion for caring for older people influenced their decision to work in RACF. Some participants reported that they were caring for children with special needs in their countries of origin, and it was instinctive for them to look for a job in the health and social care sector.
My grandma stayed at my house, so I used to take care of her with my siblings. I love her very much. I love her so much, so that is what I have transferred to the residents here. (Female Nigerian PCA) I had the experience of taking care of human beings, so when I came here actually, I wanted to do Child Care, I think the first training that came to my mind was to do Aged Care. (Female Indian PCA)
Availability
The availability of caring roles in RACFs and the opportunity to train as a PCA within a short duration also motivated some participants to work in RACFs. Some migrants will inevitably experience challenges such as unemployment during their adaptation and integration into their settlement country (Overgaard et al., 2022). Two participants, a skilled worker and a professional in the finance sector in their countries of birth, identified unemployment as a challenge when they first arrived in Australia. They explained their difficulties in securing employment in their professions because of their lack of work experience in Australia. Both participants decided to work in RACF because it was work they could more readily secure. “Well, at first that was my gateway to come here. So let me just be honest with you that was the available work” (male Filipino RN).
Some participants were overseas-qualified nurses working in Australian RACFs in lower-skilled roles (e.g., PCAs) because their overseas qualifications were not recognized and they were unable to practise in Australia. “I do not have my registration as a nurse, so I cannot work as a nurse, this [being a PCA] is the closest thing” (female Filipino PCA).
These participants found care work in RACFs as a useful stepping-stone to gaining practical knowledge and experience in the Australian health and aged care system before obtaining formal registration in the country. For some participants, working in a RACF was a starting point for their future employment goals in the Australian health care sector, such as working as a nurse in a hospital. “It’s also helpful to me because it’s a good training ground in terms of culture and the healthcare system. I get familiar with things that I need to know before I become a nurse” (female Indian, PCA).
Stressors
Work-Related Stressors
Stressors such as resettlement and acculturation stressors were specific to migrant care workers. These stressors hampered their ability to efficiently perform their roles in RACFs. One such stressor identified by most participants was difficulty communicating with residents and co-workers. Residents’ and non-migrant care workers’ accents, colloquial language, and slang were reported to impede effective communication for most participants. Some participants explained that some residents also complained about their (workers) accents and difficulty understanding them, which eroded their self-confidence in communicating effectively with residents and non-migrant staff. Racist comments by residents generally took the form of verbal abuse toward migrant care workers.
I was trying to explain the plans for the day to a resident and I was trying my best to speak louder, but the resident was showing an unpleasant attitude. Another carer came in to intervene and he [resident] said, “Because of her bloody accent, I could not hear what she was saying. I was affected. I do not have the choice to choose my accent, this is who I am.” (Female Nigerian PCA)
Communication difficulties were more profound in newly arrived migrant care workers. Most participants were able to overcome these challenges with a longer duration in their occupational roles. For instance, participants who had worked for more than 2 years in RACFs expressed more confidence and the ability to communicate effectively with residents and staff.
At the start, it was like the language was a problem. It was like a barrier . . . The first year was a little bit difficult to understand the language or the accent here, but once you settle here, you know the jargon they use. (Female Indian RN)
Participants who experienced negative attitudes from residents, especially those with challenging behavioral symptoms, tended to ascribe the residents’ negative attitudes to their medical condition. They recognized that having a good knowledge of residents’ medical conditions assisted them to establish a meaningful relationship with the older person.
It can get very challenging if they start getting aggressive. But, well, the first few months I was affected. I really felt bad for them, as I understood their condition better because they don’t know, they don’t recognise their children or their husbands, and it’s like a prison. They’re locked in that body. (Female Filipino PCA)
Another stressor that affected care provision was a lack of familiarity with workplace routines. Routine care provision for residents, such as preparing a cup of tea and placing the right towels for the resident’s needs, was initially challenging for one participant. As explained by this participant, the adjustment to the caring role in Australian RACFs was shaped by cultural differences between her country of birth and Australia rather than her skillset (or lack thereof).
It’s like from birth they are used to their afternoon tea. I did not even know how to make white tea. Well, the first difficulty that I had was differentiating between dinner, afternoon tea, and morning tea. I felt really stupid at first, and I did not know the difference between a bathmat, a face towel, and a face wash. Because they all looked like towels to me. (Female Filipino PCA)
Working with residents with challenging behaviors, especially those with dementia, was another stressor identified by participants. As noted earlier, the majority of participants had no previous dementia care experience. Working in RACFs was a foreign concept before they arrived in Australia. In addition, their knowledge of dementia and the associated physical and physiological symptoms was limited before their arrival. Most participants described their initial experiences of caring for residents with challenging behavior as being confronting and disturbing.
I was on the dementia wing; I was just sitting alone doing my documentation on the laptop. A resident just came out. I do not know where he found the knife, probably in the kitchen. He ran towards me. I thought he was going to hurt me and there was no exit . . . he did not hurt me. I realised that he came to the kitchen to get a knife and then went back to his room. I was scared to go back to work the next day. (Male Indian PCA)
The regulatory requirements of the aged care quality and safety measures were described as cumbersome by two participants who were clinical nurses in leadership positions. These participants expressed the challenges associated with adapting to emerging policies and regulations associated with aged care practices.
If you are an RN on the floor, it doesn’t really bother you that much. But when you are in middle and upper management, it is different. There are big changes to the policies and big changes in the way you work and deal with the residents and their families. Aged care is an ever-evolving trade. I mean a policy or mandate may come out this week and then the following week, another mandate will come out as well. It’s hard to keep up with these challenges. (Male Filipino RN)
Discrimination was one of the key themes described by the majority of participants. However, discriminatory treatment varied across ethnicity, with migrant care workers from Nigerian backgrounds experiencing discrimination more frequently. Most Nigerian participants (seven out of eight) reported having experienced discrimination and racism from residents, families, or work colleagues and attributed the racist treatments to their skin color and accent.
Everything happens to Africans, by the time you wonder who these things happen to, you find out it’s Africans, why is it only the Africans? (Female Nigerian PCA)
However, discriminatory treatment was not limited to migrant care workers from African backgrounds. Participants from Asian backgrounds also reported discrimination and prejudice in their workplaces.
You can’t really erase cultural prejudice or discrimination. It’s still there, but it’s not as blunt. Sometimes it can be offensive, especially when your colleagues say that the company prefers Asians, and they should give the jobs back to the white people. (Female Filipino PCA)
Acculturation Stress
Participants mentioned some non-work stressors such as the lack of support from their social network and the inability to balance work and family life because of limited support from families and friends. Participants who were students on temporary visas reported additional stressors of not being eligible to access subsidized health treatment (Medicare) and other benefits in Australia.
Being an immigrant and not yet a permanent resident, it is very difficult. When I was in the hospital, one of the major things that made me weep was how do I clear my hospital bill? . . . A happy person will deliver more quality care, somebody that got so many things going on in his or her mind would have a limit to what they can deliver. (Female Nigerian PCA)
Coping Strategies and Psychosocial Well-Being
Several coping strategies were adopted by participants to alleviate their work-related stressors. Ignoring the stressors was the most common coping strategy that participants used to manage stressors, particularly when engaging with residents with negative attitudes or challenging behaviors associated with dementia. “Part of the coping strategy I have used in the past and most of the time was to ignore and move on” (male Nigerian PCA).
Other participants who have family members working in a similar role in a RACF supported each other. “My husband also works in aged care, so every night when I come home, we sort of debrief each other” (female Filipino PCA).
All participants described their roles in RACFs as physically and psychologically challenging. Strategies used to relieve stress at work and after work included meditation and spiritual practices.
Mostly here we have a Tai Chi session where we invite the staff or anyone to join. (Female Indian RN) I believe in Jesus Christ, and I think that he gives us the power to overcome things. (Male Filipino RN)
Employment Intentions
Enablers to Staff Retention in RACFs
Despite the work-related challenges that participants experienced, nearly two-thirds (12 out of 20) indicated their intentions to continue their employment in RACFs. Being part of a family-friendly workplace and flexibility with working hours were driving factors for participants to continue working in the sector. Women with children described the shift work arrangements in RACF as compatible with meeting their family responsibilities. The shift work arrangements also provided opportunities for some to complete their studies, particularly those on student visas.
The aged care sector is family-friendly and because I have a family . . . Yes. It is very easy to talk to people to arrange your shift. (Female Filipino PCA)
Adequate organization support is another factor driving the retention of migrant care workers. A participant who had worked for 14 years in one RACF described her prior intention to train as a registered nurse and work in the hospital setting. She was unable to complete university assignments as a result of her limited computer skills. However, the barrier to progressing her career did not affect her intention to continue working in RACFs. She described support from the organization and good working conditions, including mutual respect and support among team members, as the main reason to continue working in the RAC sector.
If you can see me as an African working in one place for 14 years, it means the management is taking care of not only their residents but even their workers. (Female Nigerian PCA)
Perceived Barriers to the Retention of Aged Care Staff
Compassion for the caring needs of older adults and a desire to help others had initially motivated one participant to work in RACF. However, she worked for only 8 months and left because of tension and perceived racially motivated treatment from non-migrant workers, as well as disloyalty from some migrant care workers from different cultural backgrounds, which affected her general and mental health.
I love to work and look after older people, and I did not have a problem with the residents. I am always patient and tolerant and I know they (residents) need care . . . What I hated was colleagues talking behind me. I was constantly having heartache and couldn’t sleep well, even after work. I had to quit? If I had stayed there, I would go mad. (Female Filipino PCA)
Another factor that contributed to leaving or intending to leave the sector was a perception of poor quality of care for residents. Organizational resources such as low staffing levels were seen as negatively affecting residents’ quality of care. Three participants perceived residents’ level of care as being inadequate. They described care as frequently rushed with minimal time for interaction and communication with the residents. For these three participants, their decisions for leaving the aged care sector were influenced by a sense of social justice.
I cannot handle the way the residents are treated. It’s not the workers’ fault; they have been told by the managers to rush their duties and finish at a specific time . . . The RACF is too money-oriented. For me, not treating someone right is wrong. I cannot work in that environment I had to leave. (Female Nigerian PCA)
Five participants, all of whom were pursuing nursing qualifications at university, intended to leave the residential aged care workforce. They provided reasons, including a perceived lack of career options. RACF tasks were also described as repetitive.“I love to work in an acute care environment. I want to learn new things. That’s why I’m going to work in the hospital as well, so I can get to know about more things” (female Indian PCA).
Two out of the three participants had already resigned from their full-time positions in RACF to work in the disability sector. The participants described greater career fulfillment working in the disability sector, due to a reduced workload, which enabled an opportunity to engage meaningfully with the care recipients. The majority of participants (14 out of 20) expressed good personal relationships with the management and will continue to work in this setting. However, this might not be sufficient for some participants, as they perceived the quality of care provision as being compromised by the high workload that often deters good relationships between care workers and residents.
Discussion
Engaging with migrant care workers and addressing their challenges are important to attract and retain a high-quality aged care workforce. This current study reveals three key findings: (a) positive impacts of migrant care workers’ cultural norms that value care of older people in relation to their roles in RACFs; (b) migrant care workers’ coping strategies to work-related and resettlement stressors; and (c) critical facilitators and barriers to the attraction and retention of RACF migrant care workers.
Our participants’ cultural norms and values influenced their perceptions and attitudes toward care delivery, including their decisions to continue their jobs in RACF. Care workers from culturally diverse backgrounds often perceive care provision for older adults as family and community responsibility (Nguyen et al., 2022). Drawing on their cultural values, our participants associated the residents with their grandparents and provided them with respect and affectionate care. Harnessing cultural norms of respect and care for older people means that migrant care workers may have a lot to offer older adults (Torres & Lindblom, 2020). Thus, despite the negative aspects of care work, many migrants perceive care work as meaningful (Gao et al., 2015) and made active decisions to seek employment in aged care.
Language and communication skills are integral to migrants’ acculturation process (Doucerain et al., 2015), and communication difficulties can create tension in workplace relationships (Overgaard et al., 2022) with co-workers and residents. For instance, difficulties in comprehending regional accents, colloquial language, and slang used by co-workers and residents from the dominant culture can result in migrant care workers being vulnerable to discrimination and racial comments projection (Overgaard et al., 2022). Our findings also reveal that communication difficulties were particularly challenging for newly arrived migrant care workers. Communication difficulties may also create a barrier to migrant care workers’ ability to form social networks with members of the host country (Doucerain et al., 2015), including with non-migrant colleagues at their workplace, which could negatively affect their well-being and sense of social inclusion.
Participants from Nigerian backgrounds experienced more work-related stressors in the form of racial discrimination from their colleagues and residents compared with participants from Filipino and Indian backgrounds. These findings concur with previous studies (Adebayo et al., 2021; Olasunkanmi-Alimi et al., 2021). However, while communication barriers among migrant care workers can be addressed through language support programs (Ngocha-Chaderopa & Boon, 2016), the issue of racism is more challenging to address as the diversity in the workforce is reflected in terms of the size, employee composition and roles, industrial relations, and the culture of the organization—factors that may make it more challenging for some organizations to implement anti-racism policies (Ngocha-Chaderopa & Boon, 2016). Nevertheless, it is the responsibility of the management to provide a safe and inclusive workplace for all employees (Ngocha-Chaderopa & Boon, 2016).
Our participants used various coping strategies to manage these stressors. Coping is referred to as the cognitive and behavioral efforts that are constantly changing to manage specific external and/or internal demands that are appraised as exceeding the resources of the person (Folkman & Lazarus, 1984). Coping strategies can be problem-focused or emotion-focused (Folkman & Lazarus, 1984). Problem-focused coping includes problem-solving activities and seeking information, while emotion-focused coping includes seeking others’ company and cognitive activities such as the denial of facts to distort the real situation or being unreasonably optimistic (Folkman & Lazarus, 1984). Participants in this study expressed emotional-focused strategies such as avoidance, meditation, and debriefing with family members. There is no established evidence to suggest the best coping strategies; however, a study shows that problem-focused coping strategies are related positively to job satisfaction and negatively to poor health conditions when dealing with workplace stress.
Our participants recognized that continuous engagement and trust between them and the residents is essential in establishing a mutual and affective relationship. However, RACFs are often established to provide health and social support for residents on a lucrative basis, and staff are trained to provide physical care within a limited time frame, which often does not allow sufficient time to attend to residents’ personal and emotional support needs (Gao et al., 2015). This suggests that the organization’s policies, funding, and appropriate staffing levels are essential for quality care to be provided in RACFs.
Stressors such as high workload, low remuneration and lack of career projection (Overgaard et al., 2022), complex regulatory care requirements, deprivation of personal time, deteriorating health, aggressive behaviors, and violence from residents are some challenges faced by aged care workers, and not only migrant care workers (Chen et al., 2020). Our study adds to the literature that the complexity of resettlement challenges, including communication difficulties, the lack of familiarity with the host culture, and social support, can negatively affect migrant care workers’ ability to perform their roles effectively in the aged care sector. Addressing these challenges is crucial to retaining a quality migrant care workforce and enhancing the effective performance of their roles in this emotionally challenging work environment (Oppert et al., 2018). It is recognized that workforce retention challenges are complex, and strategies to enhance job satisfaction and address workplace retention have been described as multi-factorial (Oppert et al., 2018). However, strategies to enhance job satisfaction could improve staff shortages (Oppert et al., 2018), as highly engaged and enabled employees are more likely to provide better service to care recipients, contribute to improved business performance, and remain with their organizations (Commonwealth of Australia, 2018).
Policy and Practice Implications
This study highlights the intersection of resettlement challenges with other work stressors that are specific to migrant care workers. This study recommends that aged care management should provide education on stress reduction in the workplace, implement and action anti-racist policies, and offer programs such as language support services to facilitate problem-focused coping strategies among care workers from migrant backgrounds. Empowering them to utilize both emotional and problem-focused coping strategies such as utilizing the strategies from stress education seminars, discussing concerns with supervisors, and creating culturally safe workplace environments could alleviate work-related stressors and enhance migrant care workers’ job satisfaction.
Our findings identified some groups of migrant care workers such as international students and new arrivals as likely to be highly disadvantaged compared with other migrant care workers. RACF management could provide mentoring support for newly arrived migrant care workers with limited work experience to build their confidence in performing their roles efficiently. Workplace health promotion programs such as general health checks, mental health promotion, and provision of health information would be of great benefit to migrant care workers, especially those on temporary visas, for example, student visas that cannot afford preventive health care services.
Strengths and Limitations
A strength of this study was the participation and contribution of migrant care workers in aged care research. A diverse sample of migrant care workers was recruited to enrich the understanding of their employment experiences and possible strategies to address barriers affecting migrant care workers’ retention in RACFs. A limitation of this study is that these findings might not reflect the perceptions of the whole migrant care workforce, including those from other culturally diverse backgrounds. In addition, the study was conducted in one location and only among those working in RACFs. Those in different locations and working in community aged care may provide a different set of experiences. Finally, these data were collected pre-COVID-19 crisis and its devastating impact on aged care in Australia. It is likely that if the study were replicated during or post-pandemic, the results would be different. Future research with a diversified sample, including from regional and rural areas, incorporating community aged care workers, and post-COVID-19 is required.
Conclusion
Meaningful employment outcomes are essential to individuals’ economic security, general well-being, and sense of identity. The current study contributes to the literature by expanding knowledge of migrant care workers’ employment experience in high-income RACFs. Aged care management and government policy can enhance migrant care workers’ positive work experience by considering their resettlement challenges when creating workplace reforms to enhance their job satisfaction and retention in the aged care sector.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Researcher B.A. was supported to undertake this research study by the Australian Government Research Training Program Scholarship.
Compliance With Ethical Standards
The study was approved by the Curtin University Human Research Ethics Committee (HRE 2017-0863).