
Abstract
Introduction
With the global aging process intensified, the demand for end-of-life care has surged, especially in China. However, its development is restricted. Understanding the life and death attitude among the elderly and its formation process, and clarifying their needs, are so important to promote social popularization of end-of-life care.
Methodology
This qualitative study included 20 elderly residents in Nan and Shuangbei Communities, Chongqing City, People’s Republic of China. Data were collected through semistructured in-depth individual interviews and processed by thematic analysis method.
Results
Three themes and eight subthemes were identified: Characteristics of formation process (passive thinking, closed and single), life-and-death attitude (cherish and enjoy life, quality of life priority, let death take its course) and expectations of end-of-life care (preferences, basic needs, good death).
Discussion
Life-and-death attitude and end-of-life care expectations of the elderly support the development and delivery of end-of-life care. Furthermore, the individual-family-hospital linkage discussion channel needs to be further explored.
Introduction
Global aging process is rapidly intensifying, the number of chronic diseases and cancer patients is increasing, and the rigid demand for palliative and hospice care has surged, especially in China. According to the World Health Organization (WHO) report, the number of people aged 60 and older in the world is as high as 1 billion in 2019, and this number will double by 2050 (WHO, 2018). Not only that, chronic diseases have become the world’s largest culprit of health issues. In 2019, 74% of the population’s deaths were caused by chronic diseases (WHO, 2020), and the elderly were the most susceptible population. Nearly 30 million patients worldwide are in urgent need of hospice palliative care, of which 69% are older than 60 years old (Stephen & Maria, 2014).
In China, seniors aged 60 and older made up 18.1% of the total population by 2019 (National Bureau of Statistics of China, 2020). More than 180 million elderly people suffer from chronic diseases, and there are about 40 million disabled or partially disabled elderly people (National Health Commission of China, 2019). Along with the age growth, concomitant diseases and general weakness of the elderly not only endanger the health and life quality of themselves but also bring huge psychological and economic burden to each family (Sharp et al., 2013). However, the hospice care service coverage has reached only 1% of the population in mainland China (Yang & Liu, 2019). The development of end-of-life care cannot be delayed.
People in southwestern China are still passively accepting end-of-life care. The lack of full acceptance of end-of-life care is not only limited to the obstacles of hospice palliative care resources but also stemed from the conflict between the values of traditional social culture and hospice palliative care, which directly leads to the slow development since its introduction into China in the 1980s. In Chinese traditional culture, the emphasis on life and the lack of research on the ontological nature of death have resulted in people’s fear of death, thus avoiding talking about death, and leading to people’s lack of a rational understanding of death (Hsu et al., 2009). Such as Confucian culture, Confucius said: “life even unknown, how about afterlife,” when being asked for afterlife by his students. These words, compounded of human’s instinctive fear of death, represented Chinese social consensus on the avoidance about death, which led to the neglect of end-of-life care relevant institutions and often empty beds (Lv & Zhang, 2015). In addition, some Chinese attributed the law of life and death to fate, as reflected from the words “life and death are preordained” in The Analects of Confucius. It seems that Chinese people are more tendentious to reduce their end-of-life considerations and arrangements.
The study on the end-of-life care of the elderly is significant and necessary. Most existing researches have the following characteristics. First, the research objects are mostly concentrated in patients with a certain disease such as cancer, Alzheimer’s disease and so on (Boyd et al., 2019) or their care groups (Barlund et al., 2021), while few studies have been conducted on the relatively healthy elderly. Second, the research contents are mostly to explore the nursing mode (Fuoto & Turner, 2019) or preference for dying places (Johnston et al., 2020; Schou-Andersen et al., 2016), and there is a lack of research that combines the expectations of end-of-life care with life-and-death attitudes. Third, these researches are mostly conducted in countries with relatively mature development of palliative and hospice care, while less research has been conducted in low- and middle-income countries or regions with the greatest demand for end-of-life care.
Not only for China but also for all the countries facing the challenge of an aging population, it is a priority to understand the life-and-death attitudes and care expectations of the elderly. The findings of this study will provide a basis for the development of end-of-life care, which is beneficial for the whole world, especially for countries influenced by Confucian culture or countries with Chinese immigrants.
Method
Study Design
The research was designed as a qualitative study using semistructured in-depth interviews. This study was conducted from October 10 to November 30, 2020. The elderly from two different communities (Nan Community and Shuangbei Community) in Chongqing city, People’s Republic of China China, were selected by purposive sampling for the interview. This research focused on understanding the attitudes of the elderly toward life and death, their own experiences and related expectations. The thematic analysis method was used for data analysis.
Participants
The purpose sampling method was adopted to recruit elderly people from the Nan Community and Shuangbei Community to conduct interviews. Inclusion criteria were as follows: (1) aged 65 years and older, (2) able to understand the survey contents and express their thoughts, (3) voluntary participation. Exclusion criteria were as follows: (1) those with mental illness or confusion, (2) those with a major illness that makes them unable to cooperate, and (3) those who have been involved in a similar investigation, (4) other factors that were not suitable for participation were excluded.
Data Collection
In order to investigate the real attitudes and expectations of the elderly about life and death, this study formed the final interview outline through literature review, expert review, research group discussions, and preinterview revisions (Table 1). Face-to-face in-depth interviews were conducted around the interview outline. The two researchers explained the purpose, content, and significance of this interview to the elderly who were accompanied by the staff of the community health service center. After the interviewee has signed the written informed consent form, the interview was conducted in a room where it is familiar to the elderly, quiet, and not easy to be disturbed (such as the interview room of a community health service center or their homes) to ensure that the interviewees relaxed.
Semistructured Interview Outline.
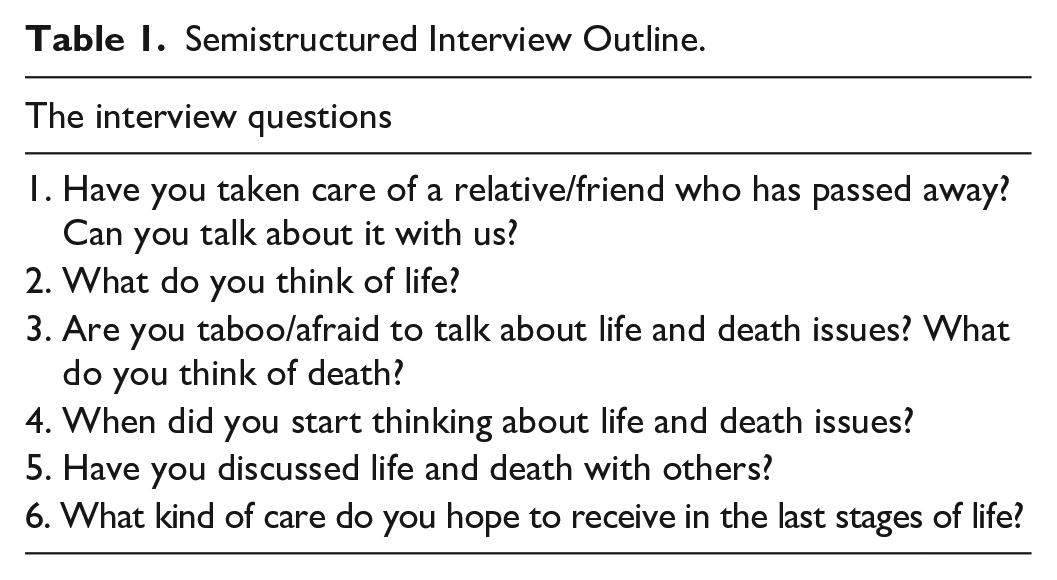
During the interview, the order of questions was adjusted according to the specific situation. Interview methods such as rhetorical questioning, elaboration, and clarification were used to clarify the views of the interviewees while inducing and suggesting were avoided. The whole interview was recorded, including not only the conversation but the nonverbal behaviors, expressions, and tones of voice of the interviewees. According to the principle of information saturation, when there was no new information about the interview topic and questions during the interview referred to the model of data saturation (Saunders et al., 2018), we did two repeated interviews to ensure saturation and determined the sample size. The length of a single interview of this study is 30mins to 80mins depending on the actual situation during the interview.
Data Analysis
Within 48 hours after the interview, the interviewers jointly converted the verbal and nonverbal recording contents into text materials. After checking the transcripts with the interviewees, thematic analysis method was adopted (Kiger & Varpio, 2020): (1) Familiarization: two researchers read through the transcripts to get familiar with the whole contents; (2) Coding: The transcripts were separately coded by both the interviewer and the recorder; (3) Generating themes: researchers created codes, identified features among them, and started coming up with themes. In order to fully reflect the research contents, subthemes were formed under each theme; (4) Reviewing themes: To reanalyze the subthemes and themes as useful and accurate representations of the data; (5) Defining and naming themes: Themes represented the transcripts and clearly expressed our meaning. A succinct and easily understandable name for each theme was developed; (6) Writing up: Analysis of the data were written.
Ethical Consideration
This study was approved by the Ethics Committee of University (2020-01302). Before the start of the formal interview, the researcher explained the purpose, significance, and precautions of the research. The content of the interview was clarified, and the interview was recorded. After obtaining the informed consent (written) of the interviewee, the interviewer started the interview formally. If the interviewees feel uncomfortable, they can terminate and withdraw from the interview at any time. The research process completely follows voluntary principle and confidentiality principle. The interview data is only used for scientific research. The subsequent analysis of the interview data uses codes to achieve the purpose of anonymity and protect the personal information of the research subjects.
Trustworthiness
To ensure the trustworthiness of the research, researchers, research processes and results were focused to improve credibility, transferability, dependability and confirmability. The two investigators have received qualitative research system training in university with experiences of interviewing. And an early familiarity with the participants before the interview was developed to gain an adequate understanding of the situation and to establish a relationship of trust. The interviewed elderly were encouraged to be open and all the nonverbal information were recorded during the interview. The themes were thoroughly discussed between researchers, the supervisor, and peer scrutiny of this study before the final determination, to guarantee the trustworthiness (Shenton, 2004).
Results
Participants
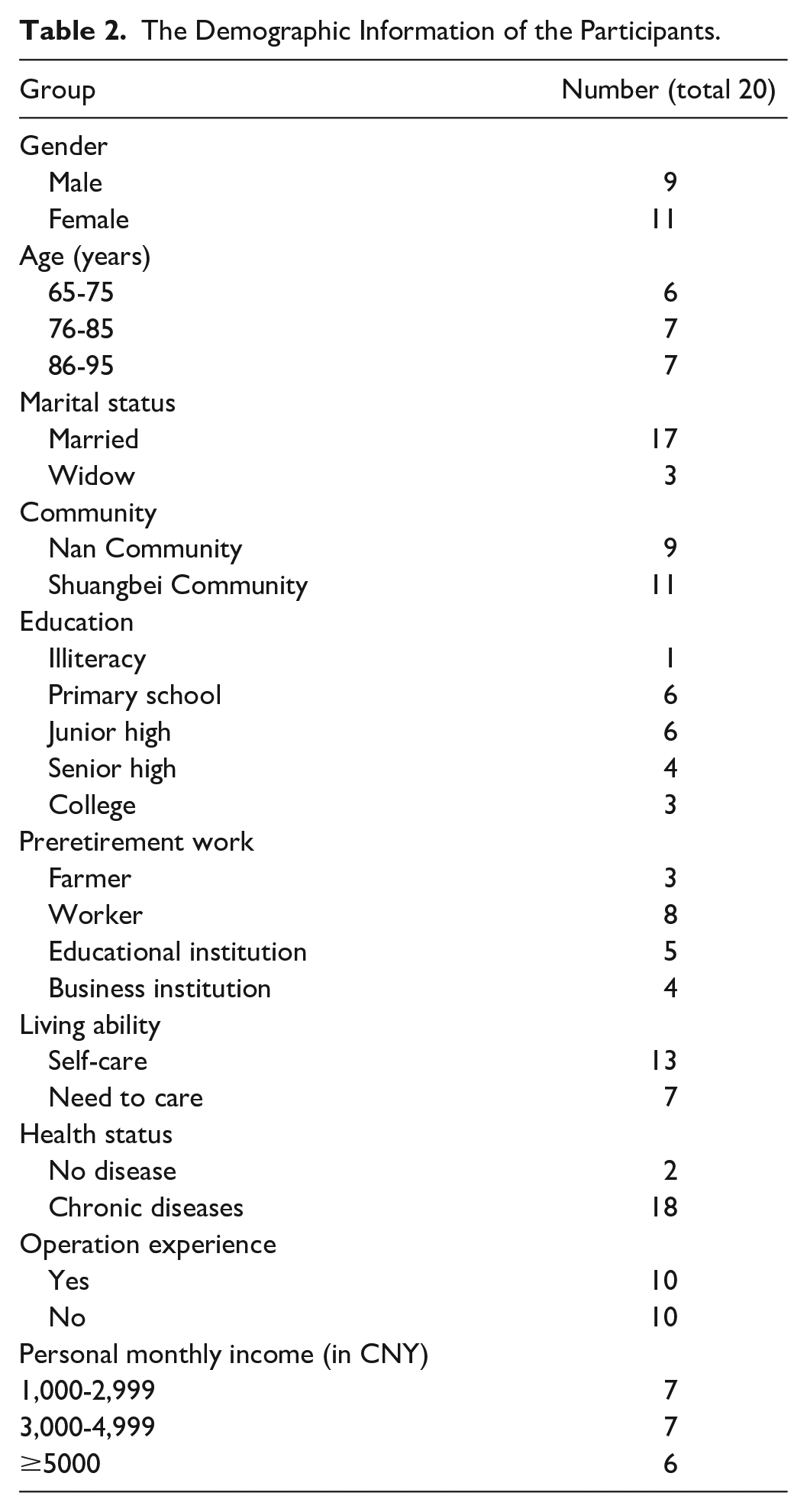
In this study, 20 elderly people were interviewed. Demographic information is shown in Table 2.
The Demographic Information of the Participants.
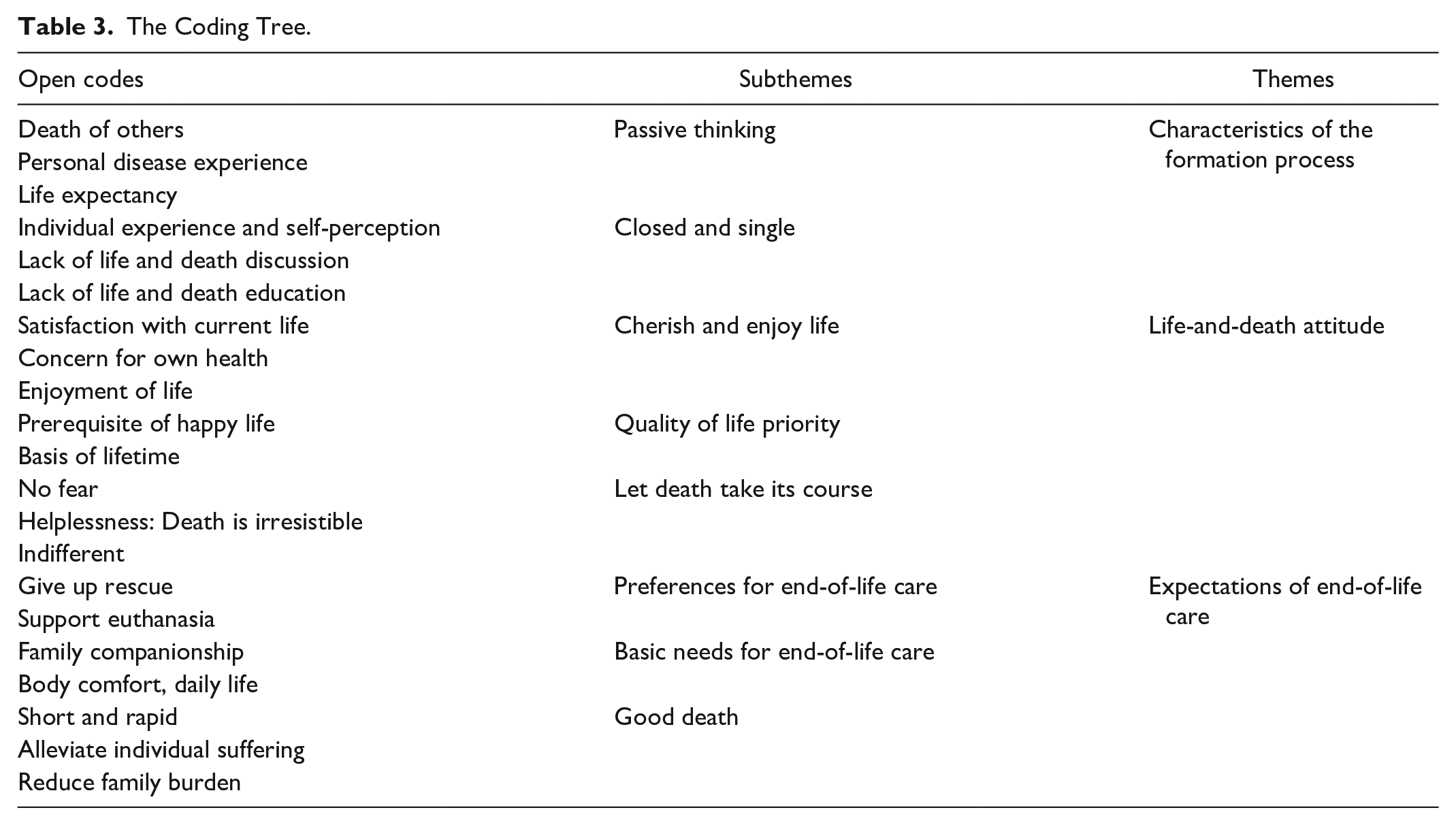
This research identified three themes and eight subthemes about the life-and-death attitude of the elderly: Characteristics of the formation process (passive thinking, closed and single), life-and-death attitude (cherish and enjoy life, quality of life priority, let death take its course) and expectations of end-of-life care (preferences for end-of-life care, basic needs for end-of-life care, good death). The details are shown in Table 3.
The Coding Tree.
Theme 1: Characteristics of the Formation Process
Subtheme 1.1: Passive Thinking
People do not usually think about how to improve the quality of death like how to improve their living standards but in some cases, the objective reality pushes them to consider death. First, the experience of other people’s death brings psychological stimulation to the elderly, which invisibly guides and strengthens the elderly’s thinking about life and death; second, many elder people may start thinking about death with the deterioration of their physical conditions accompanied by increasing incidence of health issues. During the interview, the elderly often mentioned “feeling that they have reached their age,” indicating that they have aroused thoughts about death.
P6: I have seen it, too. I have experienced it and suffered from it even when I was sick. When I was in hospital, I couldn’t hold my breath. It was like dying. It doesn’t matter if you have experienced these. I am not afraid, only uncomfortable.
Subtheme 1.2: Closed and Single
In China, people rarely talk about life-and-death and believe that talking about death will bring bad luck. The children hardly talk about this topic with their elderly parents as they fear that it will produce negative emotions to their parents. There are few in-depth discussions about life and death. Almost all elderly people formed the concept of life and death through their own experience and perception without relevant education, meaning that the whole process is closed and single.
P1: No one talks to me, no one discusses with me, anyway, I’m not afraid, I’m bold, . . . my (adult children) are still young, they don’t talk about death at all. What’s the point of an old woman like me talking to them about life and death? P20: My son will question me, “why do you say about those things (about life-and-death)?” Let’s talk about it when time comes.
Theme 2: Life-and-Death Attitude
Subtheme 2.1: Cherish and Enjoy Life
The elderly reflect their cherishment of life from three aspects: satisfaction with their current life, concern for their own health, and enjoyment of life. They have gone through a period of extreme poverty and witnessed the development of China, thus they cherish the hard-won happy life. In addition, the elderly have a deep understanding of the impermanence and fragility of life with the experiences of the death of their relatives and friends. Therefore, the elderly cherish life and pay attention to their own health.
P5: I feel that life is too short. Nothing matters. I must keep my body healthy and be happy throughout the day. There are enough food and money in my life. I don’t buy famous brands. Just keep clothes clean and warm. My requirements are not high.
Subtheme 2.2: Quality of Life Priority
Most elderly people believe that the quality of life is more important compared with the length of life. Quality of life is the prerequisite of happiness in life, and it is also the basis of lifetime. It is the most ideal state to combine the quality of life and the length of life together. However, for the elderly, their physical functions are gradually weakening.
P2: The quality of life is more important. If you live a good life, you can live longer. If you don’t pay attention to the quality of your life, it’s vain to live a long time. People are eager to live longer, but when they are older, they still have to take care of themselves. They walk and move on their own. If they collapse in bed, it is troublesome because they can’t take care of themselves. It will bring burdens to their children.
Subtheme 2.3: Let Death Take Its Course
Death is an indispensable part of the life cycle, and avoiding death is a normal psychological response. When talking this topic with the elderly, their first reaction is not fear but to let death take its course. With the increase of life experience, the acceptance of death is higher. However, it also reveals a sense of helplessness and indifference to death. Compared with cherishing life, the emotion of facing death is more complicated.
P2: First, we must be optimistic. If we want to go out and play, just go and enjoy it. Anyway, if Hades wants your life, you have no choice but to go. I think my mentality is very good. P4: It doesn’t matter, it’s not fear, just letting it be. When the time comes, people who should go still have to go.
Theme 3: Expectations of End-of-Life Care
Subtheme 3.1: Preferences for End-of-Life Care
During the interview, the preference for hospice care mainly was reflected in the choice of giving up end-of-life rescue. Most elderly people think that the rescue is vain and painful, and even if the rescue is successful, their quality of life would hardly get better, and the remaining life expectancy is very limited. This is consistent with “quality of life priority.” Based on the considerations of quality of life and survival time, the elderly prefer to give up rescue at the end of life and are more willing to support euthanasia, which is not allowed in China.
P10: There is no euthanasia now, and in my opinion, euthanasia can be done. When people can’t be saved and no consciousness, it’s best to euthanize. Now euthanasia is not advocated and is not allowed. Anyway, you will die sooner or later. It would be meaningless and boring if you had to be intubated to survive. People are dead as soon as the tubes are pulled out.
Subtheme 3.2: Basic Needs for End-of-Life Care
Compared with the holistic care model including physical, emotional, spiritual, social, and informational supportive care provided by the hospice care team, the elderly are more likely to receive home care, and family members are mainly responsible for the basic and dietary care. Most of them tend to restrict themselves from expressing their demands for end-of-life care, by which they believe would reduce the financial pressure of their family. Therefore, the need of end-of-life care for most of the elderly remains in the daily-life company.
P2: I don’t think I need a lot of care. If I can’t take care of myself when I lie on the bed, my children will take care of me. . . . If my children don’t have time, then I can only go to nursing homes, but I always feel that that’s not good, and my children are also worried about me.
Subtheme 3.3: Good Death
The elderly’s understanding of good death is still in the basic physiological aspects. Just as the elderly are passively closed in thinking about life and death, their understanding of good death is also restricted by their own cognition and financial condition. Other aspects such as psychology, spiritual beliefs, and social and humanistic care were not mentioned. According to their descriptions, the most prominent characteristic of a good death is short and rapid, which incorporates expectations of reducing individual suffering and the burden on others.
P8: We all think that it is best to die during sleep. In people’s mind, the uncomfortable process of dying is very short through sleeping. People who die while sleeping are not uncomfortable, and may end in an instant. The degree of discomfort is less. My father was rescued, but it was uncomfortable to live one more day.
Discussion
As far as we know, few studies have researched on attitudes toward life and death and the needs of end-of-life care based on the elderly in southwestern China. The economy in the western region of China is relatively worse than that in the eastern coastal region. Chongqing, where this study is located, is the only municipality in southwestern China, and there are elderly people with various cultural levels and income levels. Therefore, analyzing the characteristics and formation process of life-and-death attitudes and deeply exploring the expectations for the end-of-life care are the necessary foundation to promote the popularization and development of hospice palliative care.
In this study, the attitude of the elderly in Chongqing to life-and-death is different from the idea of wish to die among the elderly in the Netherlands (van Wijngaarden et al., 2015) as they put more emphasis on cherishing life and accepting death. In fact, the elderly rarely discuss life-and-death or dying issues in their daily lives. On the one hand, they are influenced by traditional Chinese culture (Cheng et al., 2019), in which it is unlucky to talk about death, and it may bring bad luck to death prematurely. On the other hand, the elderly lack the knowledge about life-and-death and end-of-life care while they pay more attention to current life. They have great expectations for modern medical technology and believe that they will not face death in a short period of time. Even if the elderly are willing to discuss relevant issues with their children, the children will avoid or refuse. Talking about death is a taboo not only in China but also in most countries around the world (Nyatanga, 2018).
Attitudes toward life-and-death among the elderly interviewed are formed from embedded events, lacking appropriate education and decent discussion. The United States has passed the “Patient Self Determination Act: 1990,” laying a foundation and opportunity for talking about death and formulating end-of-life care plans. The Conscious Dying Institute in the United States has also provided social support for the promotion of death and end-of-life care (Rosa & Estes 2016). In the United Kingdom, the peer education programs for the elderly, life planning workshops, and compassion communities (Seymour et al., 2013) have also created a good social environment for the elderly to talk about life and death. The Groundswell Project (Williams, 2018) established in Australia in 2009 has also made great efforts to promote life and death discussion. In contrast, social activities about life-and-death discussion have not yet been launched and the promotion of end-of-life care needs to be improved in southwestern China. As a result, life-and-death attitudes of the elderly are mostly formed in embedded events, including death experience of others, life expectancy, and illness stimulation. Death-related experiences can truly help reduce anxiety of death and shape individuals’ life goals and values (Barberia et al., 2018). However, the elderly developed their life-and-death attitudes by themselves and they seldom communicate with their families and other stakeholders. This leads to differences between caregivers and the elderly in the end-of-life care preference, which does not fully reflect the individual’s willingness (Chan et al., 2018). The life-and-death attitude can provide a reference for advance care planning about palliative care, thereby improving the quality of death (Fan et al., 2019).
Moreover, in the process of expressing their dying needs, the elderly are more sensitive to the burden they would cause, and they consider more for their family members to avoid dragging down their children. This may be related to the altruistic motives of aging (Borrat-Besson et al., 2020). Even so, based on traditional Chinese culture and the social reality of the southwestern region, it is a manifestation of filial piety and a moral obligation for adult children to support elderly parents, and it is also a psychological comfort for both the elderly and their adult children. The elderly take into account the work and life pressures in modern society, and they do not want to be a burden to their adult children. But due to the decline in living abilities and insufficiency or lack of financial resources, parents needs to be supported by their children in both practical and economic aspects. As a result, adult children have become the key decision makers in choosing the mode of end-of-life care for the elderly. So, when popularizing hospice palliative care, family members are also an important group that cannot be ignored (Zhai et al., 2020).
Breaking the barriers to life-and-death discussions and moving forward the discussion window of end-of-life care is the key to the popularization and development of hospice care. This study found that most of the elderly have formed hospice care expectations based on their experience. However, as the current development of hospice care in southwestern China is very limited, the “holistic care” the elderly could get access to remains in physical comfort and family companionship. They do not form an advance directive, lacking the prerequisites for a good death (Hopkins et al., 2020). Therefore, discussing the expectation of end-of-life care with the elderly beforehand is the key measure to improve the quality of death and reduce the burden on family members. Not only can the actual needs of the elderly be clarified but also shared decision making can be carried out to promote the formulation of advance care planning. Thereby, the quality of life of the elderly at the end of life can be improved and the psychological pressure and grief of family members will be reduced (Abba et al., 2019).
The development of end-of-life care not only is limited to the problems in the practice of medical institutions but also requires attention to the cultural philosophy questioning of life and death in hospice care. The cultural philosophy viewpoints, value orientations, moral ethics, and cultural customs are the foundations for the promotion and improvement of hospice care. It reflects the process of human beings’ self-awareness and the social environment, and it is also a natural need raised with the improvement of social material civilization and spiritual civilization. Therefore, it should be based on the cultural environment to better satisfy individual knowledge needs, to ensure the rights of decision making and to improve the quality of life and death of the elderly.
In this study, the life-and-death attitudes of the elderly in southwestern China and their end-of-life care needs are in accordance with the Chinese culture. And it shows that there are certain commonalities among the elderly in regard of life-and-death and dying care. Therefore, targeted communication strategies and care models developed under the social and cultural backgrounds may have greater significance for reference and promotion to deal with aging.
Limitations, Implications for Practice, and Research
Although this study includes as many interviewees as possible with different education levels and income levels, it is undeniable that based on the voluntary principle of the interviewees, the elderly in this interview may be more open to life-and-death issues. Those who fear to talk about this topic may not participate in the research. But we can drive the surrounding groups to know more about life-and-death by the positive elderly individuals in the future. As for implications for practice, the findings suggest that nurses should pay more attention to life-and-death education for the elderly and their family members to break the barrier of facing the reality and reconstruct an appropriate cognition of life and death. When community nurses conduct health education about end-of-life care, they can reduce the negative feelings about death of the elderly through gradual desensitization to form a death buffer stage in society (Otani et al., 2017), so that the elderly groups can really open their hearts to discuss death, face death, and make the advance care planning. Then the elderly can have more chances to achieve their end-of-life care expectations. As nurses in charge of end-of-life care, we should focus on the needs and preferences of the elderly, improve the documentation on giving up rescue, reduce the pain and increase the frequency and time of family companionship, in order to achieve “Good Death,” which is expected by the elderly.
Conclusion
The quality improvement of end-of-life care for the elderly has become an international priority. However, most of the elderly’s dying planning is still relatively rough, and their thinking about death is also in a passive and closed state, which is not conducive to the implementation of hospice care. Starting from exploring life-and-death attitudes of the elderly, how to form an individual-family-hospital linkage life-and-death discussion channel needs to be further explored. Moreover, the discussion window about life-and-death should be moved forward in order to achieve the improvement of end-of-life care and quality of death for the elderly.
Footnotes
Acknowledgements
Thanks to Jinyu Huang for language editing of the article. Thanks for the funding.
Authors Contribution
Study conception and design: Jing Tan, Yu Luo
Data collection: Lei Lei, Quanxi Gan, Chunyan Gu
Data analysis and interpretation: Lei Lei, Quanxi Gan, Chunyan Gu
Drafting of the article: Lei Lei
Critical revision of the article: Yu Luo
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the National Social Science Fund of China (Grant No.19XRK001).