
Abstract
Introduction:
New immigrants underutilize health care because of multiple barriers. Although culturally competent health care improves access, it is typically assessed by providers, not newcomers whose perceptions matter most.
Methodology:
Surveys that included measures of cultural competence and health-related quality of life (QOL) were completed by 117 new immigrants in Windsor, Ontario, Canada. A series of stepwise linear regression analyses were conducted to identify independent predictors of QOL and its four domains: physical health, psychological, social relationships, and environment.
Results:
Our adjusted results suggest that experiences of discrimination was negatively associated with overall QOL (β = −.313; p < .001) and its psychological (β = −.318; p < .001), social (β = −.177; p = .048), and environmental (β = −.408; p < .001) domains.
Discussion:
Discrimination negatively influences new immigrant QOL. Provider cultural competency training should emphasize the influence of provider discrimination on immigrant health and explore learners’ values and biases.
Introduction
Canada is known for its welcoming immigration policies. Each year, about 250,000 people make Canada their new home (Subedi & Rosenberg, 2014). In 2011, immigration accounted for two thirds of the country’s population growth (Gushulak et al., 2011), and immigrants represented approximately 20% of the total population (Dean & Wilson, 2010; Statistics Canada, 2013). Recent projections suggest that immigrants will continue to make up an increasing proportion of the Canadian population, and that by 2025, immigrants will become the single source of population growth in Canada (Dean & Wilson, 2010). Immigration and population growth of this size has important implications for health care providers and for the Canadian health care system (Gushulak et al., 2011).
A recent report suggests that Canada’s foreign-born immigrant population experience poorer health outcomes relative to the Canadian-born population (Public Health Agency of Canada & Pan-Canadian Public Health Network, 2018). At time of entry into Canada, the majority of new immigrants have fewer chronic conditions and disabilities, and better functional health than their Canadian-born counterparts (Dean & Wilson, 2010; Setia et al., 2011). Within 5 to 10 years of settlement in Canada, many new immigrants experience declines in health, reaching levels that are equal to or worse than those born in Canada (Dean & Wilson, 2010; Newbold, 2009). This foreign-born health advantage is known as the “healthy immigrant effect” (HIE), and it has also been observed among immigrants in other developed countries such as the United States, Australia, and the United Kingdom (Dean & Wilson, 2010; Subedi & Rosenberg, 2014).
Although various hypotheses have been proposed to understand the HIE, the health transition of new Canadian immigrants remains poorly understood (De Maio & Kemp, 2010; Subedi & Rosenberg, 2014). The phenomenon is multifaceted; immigrant health is affected by numerous factors, including (a) integration into their new place of residence; (b) social determinants of health such as socioeconomic status, social support networks, education, employment, and culture; and (c) the accessibility and responsiveness of health care providers and systems to their unique health needs (Dean & Wilson, 2010; Gushulak et al., 2011; Subedi & Rosenberg, 2014). With regard to the latter factor, many new immigrants underutilize health care resources and face multiple barriers in accessing appropriate health care services (Wang, 2014; Wang & Hu, 2013). Inability to communicate in either of the official languages, unease or distrust of the health care system, and a lack of culturally competent care are some of the barriers faced by new immigrants (Newbold, 2009; Subedi & Rosenberg, 2014).
In response to the surge of immigration, there is a greater need for health care providers and the care system to provide culturally competent care (Kolapo, 2017). Health care cultural competence refers to the ability of health systems to provide care to patients with diverse values, beliefs and behaviors, and to tailor the delivery of health care services to meet patients’ sociocultural and linguistic needs (American Hospital Association, 2020). A culturally competent system is one that recognizes the importance of culture in assessment of cross-cultural interactions, is attentive toward the dynamics that result from cultural differences, and that adapts services to meet the culturally unique needs of individuals and groups (Betancourt et al., 2003). A consumer or patient-centered approach to the delivery of health care is vital to providing culturally competent care (Agency for Healthcare Research and Quality [AHRQ], 2012; American Hospital Association, 2020). When implemented correctly, culturally competent health care can improve health care access and quality and reduce health disparities in immigrant populations (Health Research & Educational Trust, 2013; Smith, 2013).
Nevertheless, cultural competence has come under scrutiny over the past decade. Research has largely assessed health care providers’ own perceptions of cultural competence and therefore offering biased judgments of self-perceived knowledge, skills, and attitudes (Kirmayer, 2012). This has slowed the development of patient-centered strategies aimed at improving the delivery of high-quality care (Stern et al., 2012). Understanding patients’ perceptions of cultural competence is essential to improving engagement in health care services and health outcomes. The purpose of this study was to explore new immigrant perceptions of health care provider cultural competence, and the impact of these perceptions on new immigrant health-related quality of life (QOL).
Method
Study Design
We conducted a descriptive cross-sectional survey design using a convenience sample of 117 new immigrants in the city of Windsor, a midsize city with a population of 300,000 in southwestern Ontario, Canada. With over 100 minority languages spoken, and foreign-born citizens representing 27% of its population, Windsor is one of the most culturally diverse cities in Canada (City of Windsor, 2020). Individuals were eligible to participate in this study if they had immigrated to Canada within 5 years and were 18 years or older. The minimum sample required for the study was 81 participants, assuming a modest effect size (f 2 = .10), 80% power, and a two tailed alpha of .05 (Faul et al., 2007). Study participants were recruited from two local organizations that serve new immigrants in the city. The study received ethics clearance from the University of Windsor’s Research Ethics Board.
Variable Definitions and Instrumentation
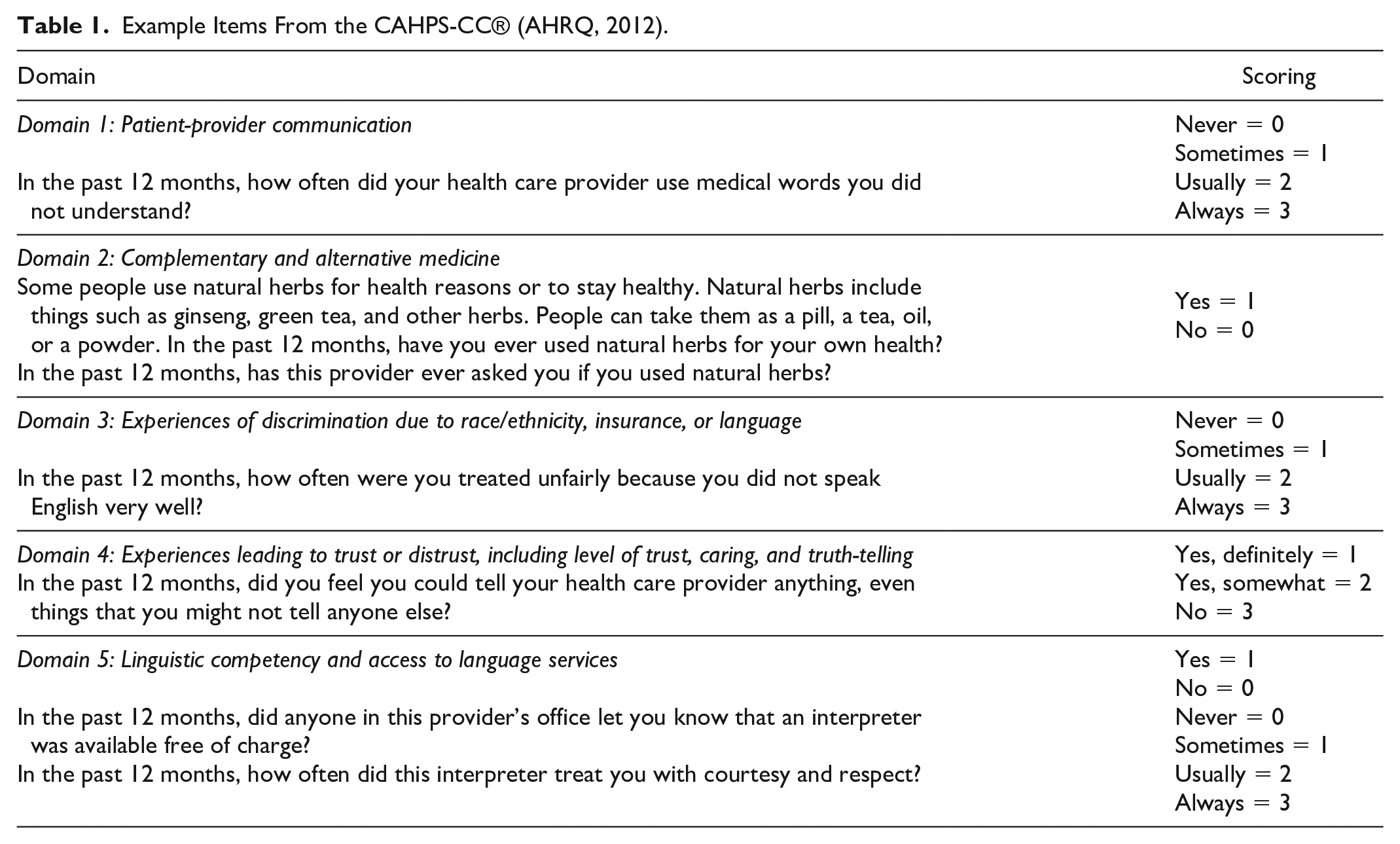
While there are various definitions of cultural competence, we conceptually defined the term as the “ongoing capacity of health care systems, organizations, and professionals to provide diverse patient populations with high-quality care that is safe, patient and family centered, evidence based, and equitable” (National Quality Forum, 2008, p. 2). In this study, health care provider cultural competence was measured using the Consumer Assessment of Healthcare Providers and Systems Cultural Competency (CAHPS-CC®) item set (AHRQ, 2012). Developed by the AHRQ, the CAHPS-CC® is a 34-item supplement to the CAHPS Clinician and Group Survey that is used to assess culturally competent care from the patient’s perspective. The CAHPS-CC® item set addresses five domains: (a) patient-provider communication; (b) complementary and alternative medicine; (c) experiences of discrimination due to race/ethnicity, insurance, or language; (d) experiences leading to trust or distrust, including level of trust, caring, and truth-telling; and (e) linguistic competency and access to language services (AHRQ, 2012).
The CAHPS-CC® is noted to be a valid and reliable scale for assessing culturally competent care from the patient perspective (Stern et al., 2012; Weech-Maldonado et al., 2012). Weech-Maldonado et al. (2012) confirmed the internal consistency of the original seven-factor CAHPS-CC® scale using Cronbach alphas, as well as its validity using exploratory and confirmatory factor analysis, multitrait scaling analysis, and regression analysis. Its internal consistency and validity were confirmed in Stern et al.’s (2012) study of 600 patients from primary care safety-net clinics in the United States. The scale was designed to target specific areas for quality improvement. Its domains have various levels of measurement; therefore, an overall composite score cannot be calculated. In this study, we calculated domain scores by totaling its item scores and generating average scores. Example items are provided in Table 1.
Example Items From the CAHPS-CC® (AHRQ, 2012).
The World Health Organization (WHO) defines QOL as “an individual’s perception of their position in life in the context of the culture and value systems in which they live, and in relation to their goals, expectations, standards and concerns” (Skevington et al., 2004). The WHOQOL-BREF is a 26-item person-centered, multilingual instrument that is used to subjectively assess well-being (WHOQOL Group, 1998). It includes sociodemographic and health status questions and produces scores for four QOL domains: (a) physical health, (b) psychological, (c) social relationships, and (d) environment (Skevington et al., 2004; WHOQOL Group, 1998). The WHOQOL-BREF arose from a decade of developmental research in 23 countries (Skevington et al., 2004), and it has been determined to have good test–retest reliability, as well as discriminant and content validity (WHOQOL Group, 1998). Although the WHO (1998) suggests that all four domains should be taken into consideration when evaluating QOL, an average score of all four WHOQOL-BREF domains was computed in this study as an exploratory measure of overall QOL. In this study, the Cronbach’s alpha for the overall instrument was .89.
Data Collection Procedures
Data were collected in October 2017 at two organizations that provide services to new immigrants. The principal researcher (AZ) explained the study to those who were interested. After consenting, participants were given a survey package that included a demographic questionnaire, the CAHPS-CC®, and the WHOQOL-BREF. Volunteer translators were available for those who required such services. Once completed, the survey packages were sealed by participants and placed into an onsite locked survey box. Completion of the survey averaged 20 to 25 minutes, and all those who participated received a $5.00 gift card as a token of gratitude for their participation.
Data Analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) Version 22 software. Before proceeding with data analysis, we screened the database for missing data, outliers, and normality. Of the 149 survey packages that were completed, 32 cases were deleted for either not meeting the inclusion criteria of living in Canada for less than 5 years (n = 14) or having more than 20% missing data on the outcome measure (n = 18). This yielded a final sample of 117 participants. Descriptive statistics were performed to summarize the sample characteristics. We then used univariate statistical procedures (Pearson moment correlation and one-way analysis of variance) to examine the crude association that the outcomes (i.e., overall health-related QOL and each of its four domains) had with the demographic and cultural competence variables. Stepwise linear regression analysis was then used to determine the independent predictors of overall health-related QOL and its domains of physical health, psychological, social relationships, and environment. To achieve a parsimonious model, only variables with significant associations at a liberal alpha ≤.25 were entered into the linear regression analyses (Hosmer & Lemeshow, 2001). Statistical inference was established using a two-tailed alpha of .05 and/or 95% confidence interval.
Results
Sample Characteristics
Participants were immigrants from 31 countries. Fifteen different languages were spoken, and all participants were enrolled in English language classes. Almost half of participants were from Syria (n = 30; 25.6%) and Iraq (n = 29; 24.8%). Mean age and length of time living in Canada were 40 years and 2 years, respectfully. The majority of the sample was female (n = 95, 81.2%), and 84.6% of participants reported being married or in a common law relationship (n = 99). However, 65% of respondents had dependent children at home (n = 76), and 78.7% reported a household income of less than $35,000 (n = 92). In terms of education, 36.8% of respondents had a high school diploma or less (n = 43), 10.3% had a college diploma (n = 12), 45.2% had a university degree (n = 53), and 7.7% had a postgraduate university degree (n = 9). Three quarters of the participants (n = 88) were unemployed (Table 2).
Demographics.
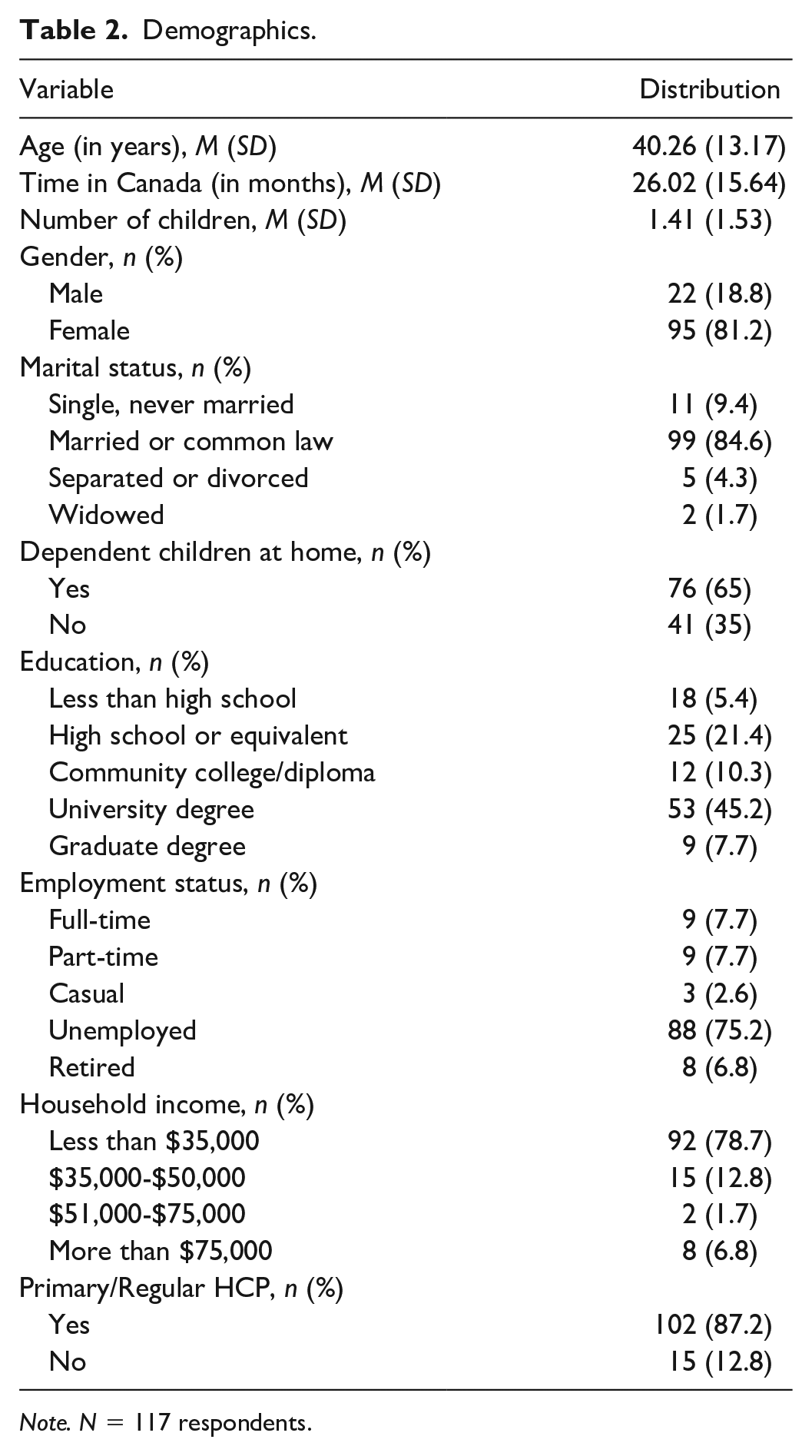
Note. N = 117 respondents.
Unadjusted Univariate Analyses
We explored the unadjusted association that each of the study variables had with the study outcomes. These results suggested that only age (r = −.184; p = .047) and number of children (r = −.285; p = .002) were associated with physical health. Experiences of discrimination (F = 11.059; p = .001), patient–provider communication (r = .230; p = .013), trust, caring and truth-telling (r = .213; p = .021), age (r = −.189; p = .041), and marital status (F = 4.279; p = .041) were associated with psychological health. Only age was associated with social relationships (r = −.278; p = .002). Experiences of discrimination (F = 29.211; p < .001), patient–provider communication (r = .276; p = .003), interpreter use (F = 7.092; p = .009), trust, caring, and truth-telling (r = .232; p = .012), overall trust in health care provider (F = 5.321; p = .023), dependent children at home (F = 3.964; p = .049), and number of children (r = −.224; p = .015) were all associated with the environment domain. Finally, experiences of discrimination (F = 13.776; p < .001), patient-provider communication (r = .214; p = .021), age (r = −.247; p = .007) and number of children (r = −.216; p = .020) were associated with overall health-related QOL.
Multivariate Adjusted Analyses
Table 3 highlights the independent predictors of overall QOL and its domains, with experiences of discrimination being the most influential individual predictor of new immigrant QOL. Experiences of discrimination (β = −.313; p < .001), higher level of education (β = −.327; p < .001) and having more children (β = −.261; p = .003) had negative associations with overall health-related QOL. While trust in the primary health care provider (β = .192; p = .030) had a positive association with physical health, having more children (β= −.279; p = .002) and increasing age (β = −.197; p = .026) were negatively associated with new immigrant physical health. Experiencing discrimination (β = −.318; p < .001) and having higher education (β= −.262; p = .003) had negative associations with the psychological domain of QOL among participants. With regard to social relationships, experiences of discrimination (β = −.177; p = .048) and increased age (β = −.281; p = .002) were negatively associated with the social relationship domain. Finally, while interpreter use (β = .200; p = .013) positively predicted environmental health, experiences of discrimination (β = −.408; p < .001) were negatively associated with the environmental domain of QOL.
Health-Related QOL: Linear Regression Analyses.
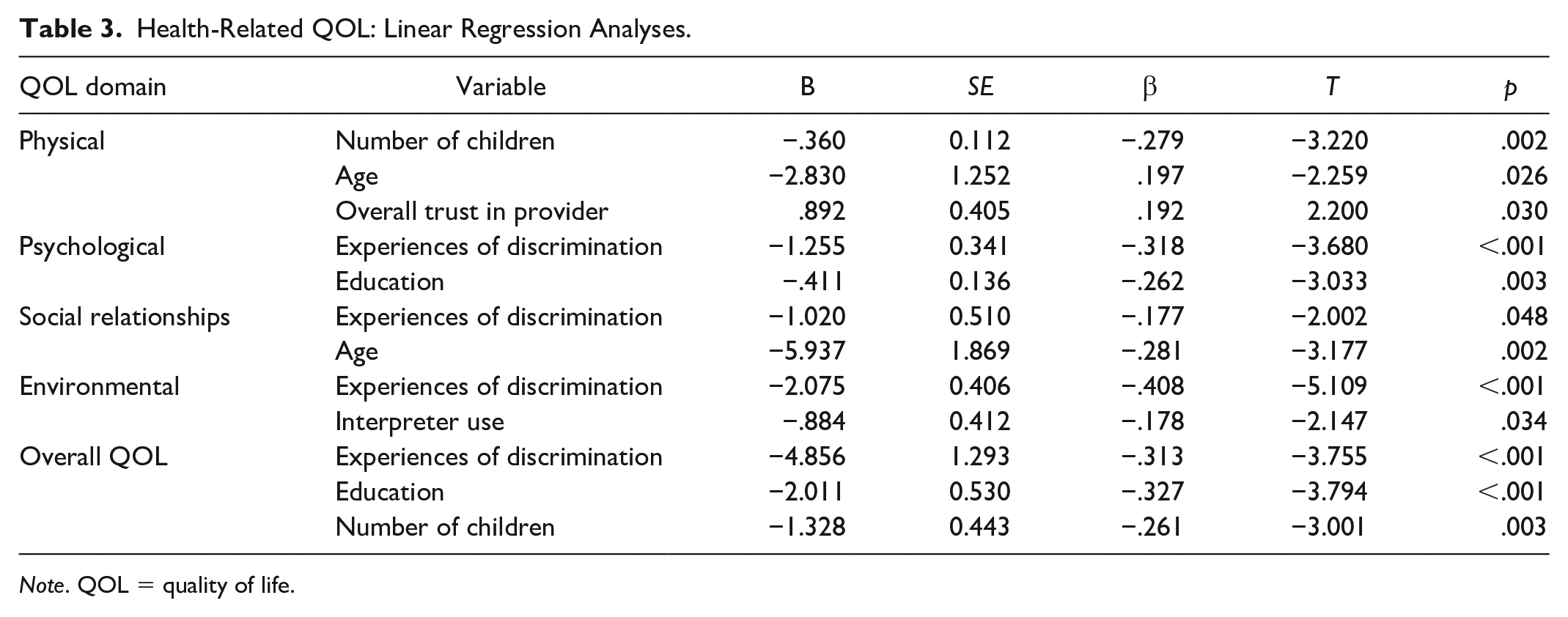
Note. QOL = quality of life.
Discussion
The results of this study provide new and surprising insights about the relationships between cultural competence, discrimination, and health-related QOL. Our findings suggest that experiences of discrimination, interpreter use, and overall trust in primary care provider are independently associated with the overall health-related QOL among new immigrants. This study validates the negative influence of discrimination on new immigrant psychological, social, environmental, and overall QOL, and it is the first Canadian study to do so from a patient perspective. Interestingly, there was no association between discrimination on the physical health of new immigrants.
Discrimination
According to the 2019 Wellesley Institute report on the Prevalence and Predictors of Everyday Discrimination in Canada (Hyman et al., 2019), recent foreign-born Canadian immigrants have a 31% lower odds of reporting discrimination experiences as compared with people born in Canada. In this study, only 12.8% of participants (n = 15) reported experiencing unfair treatment at their health care providers’ offices because of their race or ethnicity, type of health insurance or lack of health insurance; however, 44.5% reported discrimination in the form of unfair treatment due to language barrier. Although the overall prevalence of perceived discrimination among study participants appears to be relatively low, this is not entirely uncommon. According to Edge and Newbold (2013), experiences of racial discrimination are often underreported when explicitly asked in surveys. These questions may be confusing to respondents who often struggle to identify the root cause of their discriminatory treatment (Edge & Newbold, 2013). Nonetheless, our findings suggest that the experience of such discrimination is significantly associated with participants’ evaluations of their psychological, social, environmental, and overall QOL. This finding is consistent with literature reporting that discrimination or unfair treatment are related to poor self-reported health status and QOL among visible minorities and immigrant populations (De Maio & Kemp, 2010; Edge & Newbold, 2013; Gee & Ponce, 2010).
In this study, we found that experiencing discrimination had a significant impact on the psychosocial determinants of health, but not physical health. There is a large body of evidence that reports the relationship between perceived discrimination on physical health problems including hypertension (Dolezsar et al., 2014), cardiovascular disease and inflammation (Stepanikova et al., 2017) and related factors, such as poor sleep (Slopen et al., 2016), obesity (Bernardo et al., 2017), and alcohol use (Gilbert & Zemore, 2016). Discrimination has also been linked with decreased health care seeking behaviors and adherence to medical recommendations among those who experience it (Williams et al., 2019).
The effects of perceived discrimination on psychological health are also widely supported in the literature, with adverse mental health outcomes including anxiety, depression, anger, psychological distress, and others (Williams et al., 2019). Research suggests that the relationship between discrimination and mental health may be stronger among nonrecent immigrants as compared with recent immigrants (Hyman, 2009). Therefore, it is possible that the mental strain associated with discrimination takes longer to negatively influence the physical health of new immigrants. Furthermore, all participants in this study would have had access to a local immigrant health clinic whose services include health assessments and physical examinations, referrals to primary care providers, and health education (Erie St. Clair Victoria Order of Nurses, 2020). This may be a factor in explaining the lack of association between perceived discrimination on the physical health of new immigrants in this study.
Interpreter Use
Our findings indicate that interpreter use is an independent predictor of environmental QOL with 41.9% of respondents reporting a need for interpreter services at their provider’s office. This finding is not surprising as the use of interpreters has been shown to improve the quality of care for limited English proficient patients (Karliner et al., 2007) and enhance patient access to primary care and preventive services among individuals with limited English proficiency (Jacobs et al., 2004). The unavailability of interpreters or failure to use interpreters has been noted as one of the most significant barriers to accessing health care services among immigrants and newcomers (Kirmayer et al., 2011).
In this study, 60.7% of respondents indicated that they use friends or family member as interpreters when communicating with their health care providers (n = 71). Trained interpreters are recommended over family or friends as research suggests that trained interpreters have a positive impact on safe, quality of care as opposed to the use of untrained interpreters (Paradise et al., 2019). This is because trained interpreters may better promote appropriate screening and treatment, and their involvement is associated with reductions in communication, diagnostic, and medical errors, avoidance of drug interactions, and increased medication adherence (Brach & Fraserirector, 2000; Karliner et al., 2007). Studies further suggest that patients with limited English proficiency who use professional interpreters have increased health care-seeking behavior, more visits to their primary care provider, and are more likely to receive preventive health care services (Brach & Fraserirector, 2000; Flores, 2005; Jacobs et al., 2004). We strongly advocate for organizational investments in trained interpreters. This singular intervention has great potential to improve QOL among new immigrants and reduce health disparities because it expands patient choice and access to high-quality health care providers (Brach & Fraserirector, 2000)
Trust in Provider
This study findings support the notion that the more trust participants had in their health care providers, the better they rated their physical health. The majority of study respondents reported high levels of trust in their health care providers. Overall, 90% of respondents could trust their health care providers with their medical care (n = 106) and 68% felt they could tell their health care provider anything (n = 80). This finding is promising given research that reports low levels of trust among immigrant and ethnic minority patients toward their health care providers (Hillen et al., 2018). The high levels of trust among participants in this study may also be attributed to Canada’s welcoming immigration policies, its valuing of multiculturalism, and supportive local community resources for new immigrants. It may also reflect racial, ethnic, and language concordance between the health care providers and participants.
Trust in the health care provider is important because it facilitates disclosure of relevant health information and allows for more accurate and timely diagnoses (Müller et al., 2014). Studies have found that patients’ trust in their health care providers is associated with better self-reported health, higher levels of patient satisfaction, improved continuity of care, and adherence to medical advice and pharmacological regimens (Müller et al., 2014; Suurmond et al., 2011; Traylor et al., 2010).
Other Factors
Despite high levels of education, many respondents experienced low-income, and very few were employed. Our findings contradict literature demonstrating a positive association between level of education and health (Leu et al., 2008). Unfortunately, many well-educated newcomers experience almost no returns to their university education, and they often find themselves unemployed or with low earnings despite having an advanced degree or diploma (Picot, 2008). Unemployment or underemployment can occur because of difficulty obtaining professional accreditation with foreign degrees, limited language skills, and reluctance of employers to hire people with little or no Canadian education or work experience (Dharssi, 2016; Picot, 2008). Sustained funding for programs that support the employment of newcomers based on their education and skills is essential to reducing employment disparities among new immigrants, while also contributing to a strong Canadian economy and skilled workforce.
Number of children was found to negatively impact both physical health and overall QOL. Although we could not uncover any known studies that specifically explore the link between number of children and health-related QOL among immigrants, the literature does offer some insights about how number of children, well-being, and happiness may be connected at a global level (MaRgolis & MyRskylä, 2011; Pappas, 2011). According to scholars, having more children lowers marital satisfaction, increases housework, and strains the psychological health of parents, especially among young couples (MaRgolis & MyRskylä, 2011; Pappas, 2011). While the financial and emotional costs of raising children are greater when children are young (MaRgolis & MyRskylä, 2011), feelings of unhappiness may fade as larger families bring joy to parents in later years (Pappas, 2011).
Implications for Education, Practice, and Research
Education
Changing attitudes, behaviors, and practices among health care providers to better address cultural competence is necessary in order to build trust, eliminate discrimination, and therefore improve the QOL of Canada’s increasingly diverse patient population. Engaging learners in discussions about the negative impact of provider discrimination on new immigrant health may promote cultural humility, a lifelong skill that is foundational to nursing practice (Hughes et al., 2020). Attitudinal and behavioral change is more likely to occur when content is strategically integrated in health sciences curricula and tied to learner values (Biles, 2020). Training for health professionals should begin with clarifying and recognizing personal and systematic biases. It should provide learning opportunities to model tolerance and respect, foster trust, safety and a welcoming environment, and to demonstrate responsibility for combating discrimination in health care settings (Ihara, 2004; Shaya & Gbarayor, 2006) and within interprofessional teams (Pecukonis et al., 2008). While cultural competence training can reduce racism among learners (Lewis & Steinert, 2020), curriculum design and delivery is extremely complex (Biles, 2020). Learning activities must not perpetuate stereotyping (Betancourt et al., 2005), and training cannot be simply dropped into a curriculum; quality cultural competency training must be strategically embedded and should involve active and intentional debriefing (Biles, 2020).
Practice
Because experiences of discrimination can be a major driver of health inequities in newcomer populations (De Maio & Kemp, 2010), recognizing racism as a determinant of immigrant health is the first step toward reducing these inequities and disparities (Hyman, 2009). This can be done by increasing provider organizational awareness of discrimination and its impact on health, access to care, and quality of care. Doing so can promote open and honest dialogue about the effect of discrimination (Hyman, 2009; Ihara, 2004). The American Hospital Association, in collaboration with others, published a guideline for supporting health care organizations to become culturally competent (Health Research & Educational Trust, 2013). Specific actions steps include enhancing patient access to language, cultural support, and appropriate education materials, ongoing staff education in cultural competence, improving ethnic and racial diversity in leadership, and measuring/tracking satisfaction and health care disparities data (Health Research & Educational Trust, 2013). We believe that trust-building should be a primary intention of each of these action steps. Establishing trust with immigrant patients is imperative because it creates more open and genuine patient–provider interactions (Hillen et al., 2018). When patients trust their health care providers, they can become knowledgeable and empowered partners in their care, and motivated to succeed in improving and maintaining their health (Becker & Roblin, 2008). Trust enables a better understanding of immigrant perspectives, and it drives the potential to enhance QOL, reduce health disparities, and inform the advancement of relevant programs in the health sector (Stewart et al., 2006). Further to these steps, organizations should seek to recruit and retain health care staff who reflect the diversity of Canadian society, and who understand the ethnic and cultural backgrounds of the population they serve (Hyman, 2009; Ngo-Metzger et al., 2007).
Research
Although this study offers new insights on relationships between cultural competence, discrimination, and health-related QOL, current knowledge remains inconclusive. There is a need to further develop and validate scales that measure cultural competence and perceived discrimination. Inadequate measurement of these concepts could underestimate or overestimate its true rate and health effects (Williams & Mohammed, 2009). More research is also needed to explore the effects of low health literacy and limited English proficiency on patient–provider communication and interactions, and to better understand the root causes of distrust in health care providers (Ngo-Metzger et al., 2006). While some scholars are placing greater emphasis on concepts of cultural safety (Kirmayer, 2012) and cultural humility (Hughes et al., 2020; Yeager & Bauer-Wu, 2013), others challenge the need to delineate these related concepts (Greene-Moton & Minkler, 2020). Regardless, reliable measures of cultural safety and cultural humility are lacking, as are instruments that measure cultural competence from the patient perspective. Future research should continue to include newcomers in meaningful ways in the research design and process so that recommendations can be translated into changes that reflect and honor their voices (Pollock et al., 2011).
Limitations
Our findings reflect the perceptions of a largely female sample from two countries of origin—Iraq and Syria. The cross-sectional study design of our study did not allow for longitudinal exploration of immigrant experiences of health care provider cultural competence and QOL. Therefore, we were unable to examine the widely accepted phenomenon of the HIE among the study population. Recruitment was limited to those who those who attended two organizations that serve local immigrants. Thus, it is possible that immigrants who attended these organizations had more social support, which may have positively influenced their health-related QOL and protected them from negative relational experiences, including discrimination. Our results may not be generalizable to other countries, especially those that have less welcoming attitudes toward immigrants. Furthermore, given the self-report nature of our study, social desirability, and response bias could not be ruled out. The CAHPS-CC® tool currently lacked in-depth instructions for analyzing data, and it is not available in languages other than English. Also, the tool was limited in its ability to provide an overall cultural competence score that encompassed all five domains.
Conclusions
This is the first known Canadian study exploring the impact of patient perceptions of health care provider cultural competence on health-related QOL among immigrants. Three variables related to cultural competence were found to be significantly associated with health-related QOL in our study: experiences of discrimination, interpreter use, and overall trust in health care provider. Age, education, and number of children were also associated with health-related QOL. A better understanding of new immigrants’ perspectives has the potential to enhance QOL, reduce health disparities, and promote healthy and successful integration of immigrants and their families into Canadian society. All health care providers should seek to understand how cultural competence is perceived by new immigrants and seek to provide care that is nondiscriminatory, linguistically accessible, and that fosters patient–provider communication (AHRQ, 2012). Organizations that provide health care to newcomers should take action to implement culturally competent health care practices and policies that eliminate disparities and promote equitable care (Health Research & Educational Trust, 2013).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding from the University of Windsor to support this research and its publication.