
Abstract
Keywords
Introduction
The World Health Organization predicts a shortage of health care workers, specifically nurses in western European countries (Gottlieb, 2016; WHO, 2017). The demand for international nurses in the Netherlands is driven by three major factors: population growth, the ageing population, and shortage of local health care staff. It is estimated that the number of people in the Netherlands will increase to 18.4 million inhabitants by 2060 (Central Bureau for Statistics Netherlands [CBS], 2018; Merçay, Dumont, & Lafortune, 2016; Organisation for Economic Cooperation and Development [OECD], 2019). Currently, there are 3.2 million aging citizens (people older than 65 years) living in the Netherlands and the number of people aged 80 years will be doubled by 2025 (CBS, 2018). In the Netherlands, the health care staff shortage had already reached 120,000 unfulfilled jobs in 2018, combined with the predicted shortage of 470,000 health care providers, more nurses will be needed (Both-Nwabuwe, Dijkstra, Klink, & Beersma, 2018; CBS, 2018; Marć, Bartosiewicz, Burzyńska, Chmiel, & Januszewicz, 2019).
In 2015, 34,344 immigrants from Syria, Eritrea, Iraq, Libya, and Afghanistan settled in the Netherlands (CBS, 2018; United Nations High Commissioner for Refugees [UNHCR], n.d.; Willekens, Massey, Raymer, & Beauchemin, 2016). Among these there were professionals who obtained a bachelor’s degree in nursing in their country of origin. These nurses might get new starts by working in Dutch nursing health care centers. Although nursing practices share similarities globally, there are local differences, as nursing is socially, culturally, and politically constructed. Variations in nursing practice along with difficulties with communication, discrimination, and skill underutilization pose a challenge for successful workforce integration (Moyce, Lash, & de Leon Siantz, 2016). In this study, we used the definition of “workplace integration of internationally educated nurses” as formulated by Ramji and Etowa (2018, p. 15): The interaction between international educated nurses and the established nurses is a two-way reciprocal process where both groups adjust their professional practice to each other. The purpose of this study was to examine social processes affecting workforce integration of first-generation immigrant health care professionals (HCPs) in aging citizens in a Dutch health institution in the Netherlands.
Processes of Workforce Integration
Since 2000, the Netherlands have recruited overseas immigrant nurses. It is widely recognized that first-generation nurses’ adaption to a new work environment in a new country is a key factor affecting workforce integration. New nurses experience multiple challenges in dealing with cultural differences, intercultural communication, and conflict resolution in their host country (Kingma, 2018; Spijkerman, Benschop, & Bücker, 2018). Several studies on the settlement of first-generation immigrants in the Netherlands found that access to the labor market was difficult and job placements often failed based on biases toward international educated nurses. Their overseas diplomas from the Global South, their knowledge and skills were often not recognized in the Global North. They were more seen as professionals who had deficiencies and needed retraining, than people who could add value (Ramji & Etowa, 2018). Besides, first-generation immigrant nurses were expected to expend significant effort in adapting into the new health care institutions, while little was demanded from established nurses (Muller, Beckers, & Pijpers, 2017).
Other studies found that when job placement succeeded, the newly arrived immigrants faced huge problems at the workplace, due to prejudices based on age, religion, or ethnic origin, and discrimination. Cultural clashes with colleagues were widely reported. The host colleagues had not been able to bridge the gap between different work cultures either (Buttigieg, Agius, Pace, & Cassar, 2018; Maltby, de Vries-Erich, & Lund, 2016; Putturaj & Prashanth, 2017; Steinmann, 2019; Wachter & Fleischmann, 2018). Intercultural understanding, egalitarianism principles, and positive interactions between immigrant nurses and established nurses are factors which influence positive workforce integration. However, studies show that these conditions are difficult to achieve due to the existence of ethnocentrism and racial discrimination in the health care sector (Al Maqbali, 2015; Aurilio, 2017; Eijberts & Roggeband, 2016).
There is an argument that established HCPs can learn from immigrant nurses to reorganize their practices in the best interest of their patients. Increasing diversity in health organizations not only leads to a better use of talent but also to more creativity and an increase in the problem-solving ability of teams (Hunt, Layton, & Prince, 2015). However, this is not in accordance with experiences in the Dutch health care sector thus far. Scholars like Muller et al. (2017) argued that established nurses disqualified the work of their immigrant colleagues. In their studies, the established staff assessed the complaints of the immigrants about discrimination as overemotional and their different ways of working as unprofessional (Muller et al., 2017).
While research to date confirms the problems immigrants face, there is still little insight into the social processes affecting the workforce integration of first-generation immigrant HCPs in the Netherlands. To fill this gap, we conducted research into the everyday care practices in a Dutch nursing home for the ageing citizens that just had recruited 10 newly arrived immigrant nurses. The research question was: which social processes occur in the interaction between first-generation immigrant health care professionals and established nurses in a Dutch nursing home in the Netherlands?
Method
Design
In this study, we used ethnographic methods. Ethnography gives insight not only into what people think but also into what they actually say and do in a particular situation (Ingold, 2014). The context in which the experiences take place is taken into account, which helps to understand what is going on in everyday life (Bergman & Lindgren, 2018; Hammersley, 2018; McDonald & Simpson, 2014). To ensure validity, we combined different methods: participant observation (shadowing), semistructured interviews, and focus groups. With this triangulation, different kind of data were compared and this provided a more solid basis for checking interpretations and added depth to the description of the meanings involved in the setting at the nursing home (Hammersley, 2018).
Setting and Sample
This study was conducted in a rural health care institution for the ageing citizens in the Netherlands. The institution provided care to psychogeriatric, medical, and terminal residents. Because of a shortage of staff, the heath care institution started a project where they employed 10 first-generation immigrant nurses.
Data Collection
We first asked the executive board and managers of the wards if we could monitor their project with our research. After informed consent, selection was done by a purposive sample of nurses; selection criteria included first-generation immigrant nurses and the established nurses (with whom they worked with) at the nursing home. Oral and written information was given by the researchers to the immigrants during one of their first training programs and to the established nurses by email. Informed consent forms, letters with information, and a response paper for agreement were distributed. The researchers contacted the participants who were willing to participate by email, phone, or WhatsApp to decide on days and times for shadowing, interviews, and focus groups. All participants were free to withdraw from the study at any time. The data collection was conducted by two researchers, both anthropologists with a background in nursing, over a 4-month period. The researchers shadowed three immigrant nurses for 2 days a week for a total of 105 hours on different workdays and during evening shifts, at staff meetings, and during breaks. This enabled us to craft thick descriptions of the interactions and informal conversations between all participants (Leeds-Hurwitz, 2015). In-depth, semistructured interviews were held with eight participants, four immigrant HCPs and four established HCPs. The interviews took place in the nursing home and lasted between 45 and 75 minutes. The researcher audio-recorded and transcribed the interviews verbatim. Each interview opened with a narrative eliciting question: “Could you tell me something about the workforce integration?” Two focus groups took place on a voluntary basis within the nursing home, one with eight immigrants, and one with six established HCPs. We invited all 10 immigrants and all 10 established nurses for the focus groups. Four established nurses were not able to attend the focus group because of other commitments. One immigrant nurse was sick that day and one immigrant nurse refused to attend. On the basis of our observations on the wards and the outcomes of the individual interviews, we discussed three topics: their views about the similarities and differences between established HCPs and first-generation immigrants; their ideas about whether and if so, how (mutual) learning and adaptation was taking place; and finally, what they considered to be the major challenges and barriers in the process of workforce integration. The focus groups lasted between 90 to 120 minutes. They occurred in a meeting room at the nursing home and were audio-recorded and transcribed verbatim.
Data Analysis
Inspired by a postpositivist grounded theory coding approach, we analyzed data using Atlas.ti (Charmaz & Belgrave, 2018; Denzin, 2019). First, the ethnographic fieldnotes and transcripts were read and re-read to develop familiarity with the data (Evans, Huising, & Silbey, 2016). Following this approach, frequently occurring observations were open coded (Charmaz & Belgrave, 2018; Denzin, 2019) attaching a label to each part. Second, axial coding (Charmaz & Belgrave, 2018; McCann & Polacsek, 2019) took place: to find similarities and differences, codes were compared with earlier data coding. The codes were merged, grouped, and labeled. Finally, to generate more abstract core concepts and categories, selective coding (Charmaz & Belgrave, 2018; McCann & Polacsek, 2019) took place. With this combination of inductive and deductive analysis, we hoped to gain a deeper understanding of the social processes affecting the workforce integration. Saturation of information occurred after moving back and forth between sampling, data collection, and analysis. Thus, we could make use of Elias and Scotson’s (1965/1994) notions of “outsiders” and “established” to understand the social processes at work when newcomers arrive in a long-standing community, while the notion of “resentment,” as developed by various sociologists (Cramer, 2016; Hochschild, 2016), helped to shed more light on the anger and resistance we observed among many established HCPs. Observations and interview quotes that underpinned the results and analyses were first checked within the research team. Then the main findings were presented to the participants (member check) to check the validity. The reactions of the participants indicated that our findings were consistent with their experiences and views.
Results
Ten immigrant HCPs from East African countries and 10 Dutch established health care professionals participated in this study. The immigrant nurses (five men and five women between 20 and 40 years old) had temporary resident permits (for 5 years). Their foreign diplomas did not meet the criteria for acceptance to work according to the Dutch information center for credential evaluation. So, the health care institution provided the new arrivals a Dutch (re-)vocational qualification retraining program into nursing (HCP Level 3) and Dutch language lessons (B2). This program lasted 18 months. The work experience in their home countries varied from 1 to 5 years. Oral and written information was given by management to the established staff about the arrival of the new employees before the immigrants started with their retraining and work. A meet and greet was arranged by management preparing both groups for this experience and a voluntary buddy network was set up, which meant that each new employee was being coached by a native buddy. The immigrants participated in the retraining program and simultaneously worked in the medical wards at the nursing home. Their tasks were in accordance with nursing Level 3 in the six-level classification of the Dutch Qualifications Framework (DQF; Table 1). The 10 established HCPs were all native Dutch women between the ages of 18 and 68 years. They worked in the wards at Levels 2 to 3 (DQF). Their years of employment and work experience varied from 6 to 15 years. The majority of the established employees were born and raised in the village where the nursing home was located. They had formed a community (Gemeinschaft) with a high degree of internal cohesion, especially through church memberships and family ties. At the time of this research, the nursing home had no experiences with immigrant or non-native Dutch staff, nor was there any diversity policy. Working with new colleagues from different ethnic, linguistic, and professional backgrounds caused considerable commotion among both groups.
Nursing Care Staff in the Netherlands.
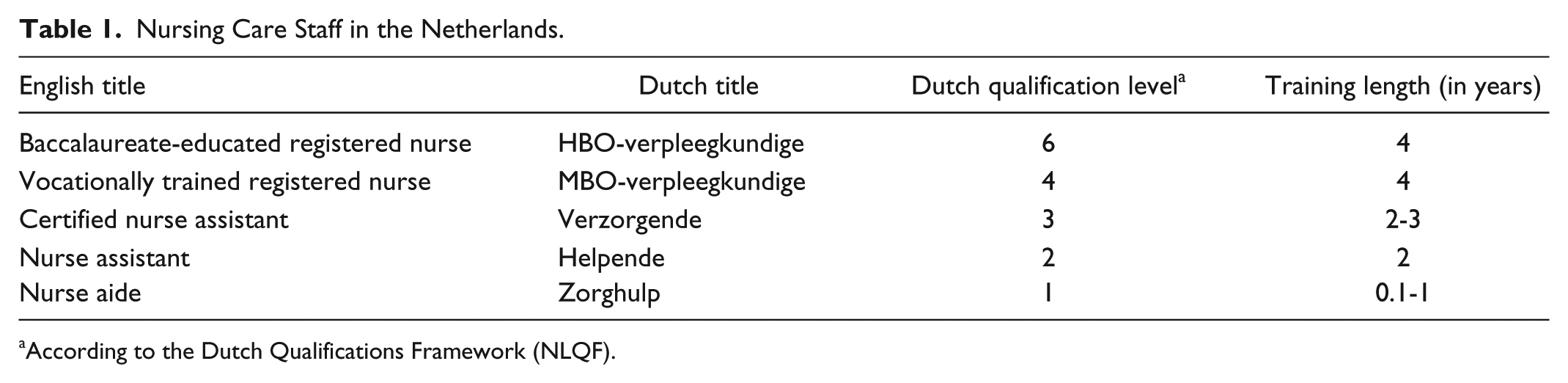
According to the Dutch Qualifications Framework (NLQF).
Norms of Professionalism
During the shadowing, the interviews, and the focus groups, we found in the interactions of both groups of professionals’ mutual themes that reflected and revealed their norms of professionalism. Some established HCPs doubted the professional capabilities of the immigrants and presented their own standards of professionalism as the only norm. Some even argued that caring practices in non-Western countries were inferior to those in Western countries. Thus, after asking one of the immigrant nurses whether she knew how to insert a catheter, the established nurse immediately responded by saying that there were probably no hygiene standards in her primitive country. These presumptions about supposedly insufficient professionalism had a negative impact on the relationship between the established HCPs and the immigrant professionals. They contributed to a sense of alienation and created tensions and conflicts between the two groups. For example, during lunch breaks the groups usually sat at separate tables and did not speak or pay attention to each other: The established colleagues enter the staffroom, laughing out loud and chatting to each other. They are talking about the fair the church is organizing this weekend. The immigrant nurse is sitting at the long white table in the middle of the canteen staffroom. The established nurses take a seat at another table, paying no attention to him. The immigrant nurse remains seated, looks at his iPhone, does not say anything.
Simultaneously, the immigrants found that their Dutch colleagues did not always meet their standards of professional care. Their criticisms were related to three issues. First, one of the immigrant nurses believed that his Dutch colleagues were not supportive when residents refused his care. He was sure that if the host nurses were more supportive and positive about him being new, that the residents would not have had any problems with him providing care and would not have had refused his care. Second, they were critical of the allocation of workload and doubted whether the established HCPs divided the workload in a fair way. One immigrant nurse felt his Dutch colleagues blamed him for having a slow tempo at work, but he stated that they themselves were guilty of having a lazy pace and were burning their time. Third, the immigrants were critical of the standards of hygiene in the nursing home. They were surprised about the lack of hygiene as there was no protective equipment, like gloves for hand and shoe covers in the department with a risk of contaminating the residents. One immigrant nurse said that she was anxious to discuss these concerns and to be critical of their Dutch peers as she was afraid that they would not recognize her knowledge and skills. Some of the established HCPs related their own professional status to their many years of work experience in the Dutch nursing home. She stated that they themselves were not racists, but that because they had been working there for years the immigrants had to behave as professional like themselves.
Resentment toward the “Elite”
Not only was the familiar environment of the established group disrupted by the immigrants, they were also angry with the management who had made this happen. Many established HCPs believed that management paid a lot of attention to the immigrants while at the same time their own hard work was ignored. One of them complained that the managers were never present in the wards, did not even know their names, and treated them as less than human. This pain of not mattering intensified feelings of resentment of the established HCPs toward the immigrants which surfaced in their behavior. One team on the medical ward started to write down all instances of what they considered to be “bad” or “unprofessional” behavior of their immigrant colleague. This diary was then sent to their manager, resulting in the transferal of the immigrant nurse to another ward. Although some scholars (Hutchinson & Jackson, 2015; Ybema & Horvers, 2017) find that such forms of resistance merely create an “imaginary sense of power,” in this case it seems that the strategy of Dutch nurses served as an effective “weapon of the weak” (Colburn, 2016; Ginzberg, 2017; Scott, 2008). Bitter indignation and frustration also appeared in remarks made by some of the younger established nurses. Management offering the immigrant nurses opportunities for education they themselves were deprived of. They viewed themselves as “sideliners” in the workforce. They felt disadvantaged, not appreciated, and not respected. Gossip was an everyday form of resistance for the established HCPs to protect their professional norms, beliefs, and relationships. In the focus group some of them suggested that caring professionals should behave in a certain way: They needed to be motived, interested, and extrovert, they should be able to say no and to take initiative. Two established nurses said that they worked in a very good professional team and they did not want “bad apples,” because these were like a virus to their team. The immigrants were quite aware that their Dutch colleagues were gossiping about them. To them, this behavior was another example of the lack of professionalism of their new colleagues. One of the immigrant nurses said that the Dutch nurses should behave according to the etiquettes of the ward. Mistakes should be regarded as a private matter, and gossip should not be allowed. The immigrants had been full and active nursing professionals in their home countries, but felt that this was not recognized by their Dutch colleagues nor by management. They blamed management for not taking the lead and not facilitating communication between the established HCPs and themselves. They felt that management were supposed to do something about the established nurses who did not accept the newcomers. This intensified their pain of not mattering.
The immigrants found the Dutch language very difficult. During breaks, they struggled understanding their Dutch colleagues. Besides, the Dutch colleagues chattered about things the newcomer was not involved in, and they felt that their Dutch colleagues would find their Dutch language not good enough. This was one reason why one of the immigrant nurses often kept quiet and did not engage in conversations, as one of them explained in an interview. Besides, he found it strange that one of the Dutch workers interpreted his silence as a lack of interest and that one of his Dutch colleagues had even reported this to management. However, one of the established nurses said in an interview that she wanted to relieve the newcomers by not talking to them during breaks, because she realized that the Dutch language was so difficult for them. One of the immigrant nurses on the other hand, interpreted the fact that her Dutch colleagues were not talking to her as a sign of disinterest. She also complained about this to management: The nurses sometimes didn’t even look at me! They just walk away like . . . I am not there . . . Maybe if they talk to me, be nice—but no, they only talk together. I went to the team leader and manager and asked, “Why aren’t the nurses talking to me?”
The immigrant nurse did not receive a follow-up on her report, she concluded that the ward manager was not interested either. For her, being ignored added insult to injury, and meant that some of the established professionals were simply being racist.
Discussion
This study examined the social processes taking place in a Dutch nursing home when immigrant nurses were recruited and started working on the wards. In this study of workforce integration, we applied a sociological approach to understand what was going on in daily practice. Our study revealed that the recruitment of immigrant nurses generated consequences on the workplace that management had neither foreseen nor intended. Different norms of professionalism, language difficulties, and unspoken expectations were misinterpreted as signs of disinterest by both groups.
Our findings showed similarities with results from other studies (Cramer, 2016; Hensmans & van Bommel, 2019; Hochschild, 2016). These studies showed that in various Western countries many citizens in rural villages distrust national and local government as well as urban liberal elites. They feel disadvantaged and not receiving what they deserve. They perceive themselves as the “good citizens” who are “waiting in line,” while various outsiders are cutting the line and moving ahead of them. They see these “line cutters” as a threat, not only to their social standing but also to the stability of their culture. This makes them feel jealous, causing resentment and a fear of becoming “strangers in their own land” (Hochschild, 2016). The remarks and behavior of the Dutch HCPs showed that they too felt left behind and pushed back in line.
The established-outsiders framework of Elias and Scotson is very helpful in showing how social processes work when a group of newcomers arrives and how “strangers” are perceived in local established communities. Elias and Scotson’s first outlined their theory in 1965. They had studied the tense relations between an established group and a group of outsiders that did not differ from the established group in any other way. They observed how certain mechanisms occur which reinforce the divisions between the groups and constitute “imagined” communities of “we” and “they” that are not based on racial, ethnic, class, or gender differences (Elias & Scotson, 1965). In 1974, Elias further elaborated the theory of established-outsider relations. He demonstrated that this theory could be applied to the group dynamics between other groups in society, for example, working and middle class, different ethnic groups, colonized and colonizers, men and women, parents and children, and so on. In 1990 and 1994, Elias substantially discussed his ideas in relation to the changing dynamics of race and racism in the United States. In his introduction to this last edition, Elias pointed out that structural inequalities are based on power relations between groups and the degree of internal cohesion and communal control of one group to integrate into other groups. So, as Elias has claimed, the focus needs to be on the relationship between two groups within an established and outsiders figuration, where a dominant group excludes members of the other group. According to Elias, prejudice is a product of groups within a particular figuration of power dynamics and not of individual persons who are prejudiced about other individuals, based on their different race (Elias, 1994/2002 [1990]). The theory of Elias has implications for the microanalysis of group dynamics and social patterns between groups within local communities. It demonstrates the significance of looking beyond individuality when analyzing group processes and their dynamics in societies. So, in each society, where a group of newcomers arrive in an established community, we can expect similar social patterns and power dynamics to occur.
However, this approach has three drawbacks. The first drawback is that this approach may simultaneously enforce the construction of otherness in these social processes (Clarke, 2018; Thomas, 2016). Because the unintended consequence of this approach is the framing of people into categories, it can easily lead to perceiving groups as static entities that determine the way individual members think and act. We should always realize that boundaries between people are socially and historically situated constructions that nevertheless can have very real performative effects (Krebbekx, Spronk, & M’charek, 2017; Verkaaik, 2010).
The second drawback is that according to Elias theory, prejudice is a product of groups within a particular figuration and not of individual persons who are prejudiced about other individuals. However, in our study we did find that individual prejudice was often related to negative traits of otherness, as in premises of exclusion and discrimination. This is in line with other studies that show that racism, sexism, and xenophobia do occur and exist in Western institutions (Blanchet Garneau, Browne, & Varcoe, 2018; Essed & Muhr, 2018). Many scholars address racism in nursing institutions in European countries. They argue that stereotypes and categories cannot be ignored and are often internalized because of power differences, resistance, and institutional racism (Hilario, Browne, & McFadden, 2018; Reimer-Kirkham et al., 2016).
The third drawback is that Elias and Scotson’s figuration, in its exclusive focus on local communities, cannot sufficiently account for the institutional dynamics of workforce integration. In our study, we focused on social processes in a specific setting, that is, the workforce integration of non-Western first-generation immigrant nursing professionals in a Western health care institution. We found that the established-outsider figuration can serve as a tool to understand social processes taking place between more and less powerful groups and the ways in which a dominant discourse acts as a source of privilege. However, the results in our study also showed that the Dutch established HCPs and the newcomers both had internalized their own norms of professionalism. Elias and Scotson’s figuration theory does not give much room to professionally hybrid identities. For example, the immigrant professionals learned to navigate between, and mix elements from, two work cultures, that is, the professional culture of their “buddy” nurse on the one hand, and the professional culture of nursing in their home country on the other hand. Thus, institutions need to carefully monitor and understand the social processes that occur when newcomers arrive, but they should also have a keen eye for the underlying systematic inequalities that serve as barriers for achieving an egalitarian workplace.
Conclusion
This article aimed to answer the question of which social processes are affecting the workforce integration of first-generation immigrants in a Dutch nursing home. Our study identified various social processes like the imposing standards of norms, gossip, the use of “weapons of the weak,” mutual suspicions of indifference, and appealing to collective images of “us” versus “them.” These processes supported and reinforced divisions in the nursing home which affected workforce integration. Besides, the established and immigrants HCPs both referred to norms of professionalism to distinguish themselves in a positive way from the other group. Both groups experienced ongoing tensions, irritations, and frustrations in daily practice on the work floor. Many of these feelings were triggered, or at least aggravated by a sense that management had no idea of their problems. Hence, although members of both groups conceived the “others” as the source of their discomfort, they shared this pain that their difficult predicament did not seem to matter to management.
Implication for Practice
Our study highlights the need to pay more attention to the lack of respect and recognition of the contribution of HCPs in nursing homes. We recommend that management of health care institution provide and facilitate guidance to promote and foster good work relations, power equity, and respectful treatment for not only the newcomers, but for all HCPs. The findings in our study confirm the outcomes of previous studies that argue that adequate support of management is important to make workforce integration a truly two-way process (Buttigieg et al., 2018; Kuokkanen et al., 2016; Ramji & Etowa, 2018). In light of our results, two directions for future research can be identified. First, more research is needed to analyze the role of management in facilitating and supporting mutual workforce integration within health care institutions. A more in-depth analysis of “the weapons of the weak” might give a deeper insight into the emotions of the established professionals, like their anger with management directed at the immigrants. Second, we might also investigate how other (inter)national health care organizations address mutual workforce integration and how they take up potential challenges of institutional change.
Footnotes
Acknowledgements
We are grateful to the immigrant nurses, the Dutch health care providers, the residents, and staff members of the health institution for the aging citizens for their willingness to participate in this research. All work is collective, I would like to thank Prof. Dr. Ria Reis and Dr. Baukje Prins for their support and guidance during this research. I thank Fatima El Bouk, Julie Lehmann, Magdeline Aagard & Roukayya Oueslati, for their comments on earlier drafts of this article and their support.
Author’s Note
This study was approved by The Medical Ethical Review Committee of the Leiden University Medical Center (code P 16.087).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Dutch Organization for Scientific Research (NWO) (023.008.044/1105).