
Abstract
To date, coagulation tests are unable to reflect in vivo coagulation status in the same system, including platelet function, fibrin clot formation, and whole blood flow. The Total Thrombus Analysis System (T-TAS), which is a microfluidic assay that simulates conditions in vivo, measures whole blood flow at defined shear rates under conditions designed to assess platelet function (PL-chip) or coagulation and fibrin clot formation (AR-chip). The T-TAS records occlusion start time, occlusion time, and area under the curve. We evaluated this test in healthy control dogs. We also investigated the effect in vivo of acetylsalicylic acid (ASA), and the effect in vitro of an anticoagulation drug (dalteparin; low-molecular-weight heparin; LMWH). The CV of the AUC of both chips was good (CVs of 6.45% [PL] and 1.57% [AR]). The inhibition of platelet function by ASA was evident in the right-shift in the PL test pressure curve. The right-shift in the AR test pressure curves showed that the administration of LMWH inhibited both platelets and the coagulation cascade. The T-TAS may be useful in the evaluation of canine blood coagulation.
Blood coagulation is a complicated process, incorporating 3 separate systems: platelets are involved in primary hemostasis, coagulation factors are involved in secondary hemostasis, and those 2 steps are followed by fibrinolysis in tertiary hemostasis. There has been an increasing focus on blood coagulation systems in veterinary medicine.2,4,9,10,15,16 Patients with hemostatic disorders (e.g., congenital bleeding diseases such as von Willebrand disease, hepatic failure, and disseminated intravascular coagulation) have a tendency to bleed. On the other hand, patients with thrombotic disorders (e.g., immune-mediated diseases, such as immune-mediated hemolytic anemia; hypoproteinemias, such as protein-losing enteritis or protein-losing nephropathy; and Cushing syndrome) exhibit excessive clot formation.
According to the Virchow triad, the stasis of blood flow, vascular wall injury, and coagulable state each influence blood coagulation. However, almost all current blood coagulation tests address only the coagulable state. For dogs, few tests can measure both primary hemostasis (based on platelets) and secondary hemostasis (based on coagulation factors).1,2,4 None of the existing tests assess blood flow, which is one of the most important factors in blood coagulation. Thus, the existing tests do not permit the complete evaluation of canine blood coagulation. The Total Thrombus Analysis System (T-TAS; Fujimori Kogyo), which was developed based on the Virchow triad, mimics damaged blood vessels and uses microfluidic chips with collagen applied on the microducts and is performed under flow conditions using microfluids. Hence, the T-TAS assesses blood coagulation status under closer to in vivo conditions than do conventional coagulation tests.5,6,19 The use of the T-TAS has been reported in human congenital bleeding diseases (e.g., von Willebrand disease and congenital diseases that result in abnormal platelets, such as Glanzmann disease)3,11–13 and in the evaluation of some antiplatelet and anticoagulant drugs.7,14,20 The T-TAS has also been used in the evaluation of a canine bleeding disorder 8 and in a canine model of atrial fibrillation.17,18 However, the T-TAS has not been evaluated in detail in healthy dogs nor used to test the ability of the analyzer to detect inhibition with in vivo or in vitro drugs in dogs.
The T-TAS employs 2 microfluidic chips: one is a platelet chip (PL chip), which can evaluate platelet function; the other is an atheroma chip (AR chip), which can evaluate coagulation and fibrin clot formation and is also affected by platelet function. These chips permit the testing of the primary and secondary coagulation systems, respectively. The chips employ microducts that are coated with collagen (PL chip) or collagen and thromboplastin (AR chip); the microducts imitate the injured vascular wall. Injection of whole blood into the microduct at certain shear rates (12 µL/min for PL; 10 µL/min for AR) induces the formation of a thrombus. The T-TAS tests the pressure within the microduct during thrombus formation by video recording (Fig. 1A). We evaluated the T-TAS assessment of clotting of blood from healthy control dogs, and also assessed the in vivo effect of acetylsalicylic acid (ASA), a nonsteroidal anti-inflammatory drug that inhibits platelet aggregation, and the in vitro effect of an anticoagulation drug, dalteparin sodium (low-molecular-weight heparin [LMWH]).
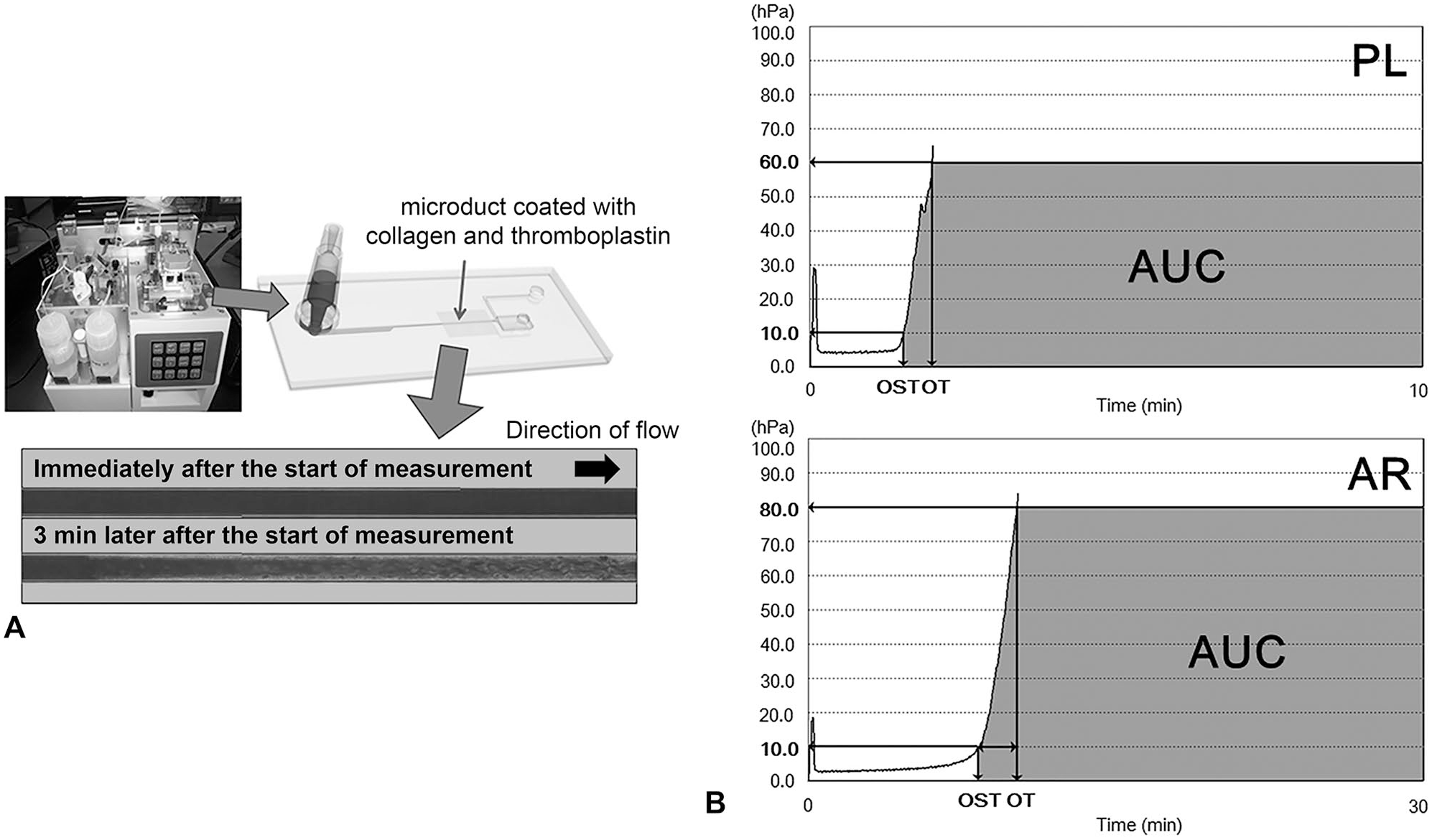
Principles of the Total Thrombus Analysis System (T-TAS).
We collected whole blood from 7 healthy control dogs (2 Labrador Retrievers, 3 Beagles, 2 mixed breeds; 1 male, 2 castrated males, 4 spayed females; ages 1–10 y [median: 2 y, mean: 4.3 y]). This study was conducted in accordance with the Ethical Code of Animal Experiment of Kagoshima University (Approval VM17021). The control dogs were clinically healthy and had normal complete blood counts (CBCs). The dogs were not under treatment with any drugs. All blood samples were collected from a jugular vein using a 23-ga needle and 2.5-mL syringe (Terumo) and were tested within 3 h. For the PL chip, we collected whole blood with hirudin (1.5% final concentration) as the anticoagulant; 350 µL of hirudin blood was loaded onto a collagen-coated PL chip at a flow rate of 12 µL/min. For the AR chip, we collected whole blood with citrate (3.13% final concentration) and danaparoid (0.5 IU/mL final concentration) as the anticoagulants. In mice and dogs, it is necessary to add danaparoid, the main component of which is heparan sulfate, which exists endogenously in the bloodstream, as an anticoagulant because citric acid alone can create a very small clot in the microducts and affect the formation of a thrombus. The citrate–danaparoid blood (480 µL) was combined with 20 µL of corn trypsin inhibitor (CaCTI), and the resulting mixture was loaded onto a collagen- and thromboplastin-coated AR chip at a flow rate of 10 µL/min. T-TAS parameters included occlusion start time (OST), occlusion time (OT), and area under the pressure curve (AUC; Fig. 1B and 1C). We defined OST as the time at which the pressure reached 10 kPa, and the OT as the time to reach 60 kPa (PL chip) or 80 kPa (AR chip). The measurement was completed when the sample reached OT, or (in the absence of occlusion) an assay endpoint of 10 min (PL chip) or 30 min (AR chip). The AUC was calculated for the interval from the OST through the end of the assay (10 min for PL; 30 min for AR).
In the group of 7 healthy control dogs, the means ± SDs of OST, OT, and AUC for the PL chip were 2.26 ± 0.81 s, 4.73 ± 1.21 s, and 407 ± 54, respectively; the values for the AR chip were 5.02 ± 1.83 s, 6.04 ± 2.14 s, and 1955 ± 54, respectively. We measured the same samples from each healthy control dog twice and calculated the CV of these parameters to confirm the differences between individuals. The CVs for the PL and AR chips were: OST, 10.9% and 10.0%; OT, 15.4% and 7.6%; and AUC, 6.4% and 1.6%, respectively.
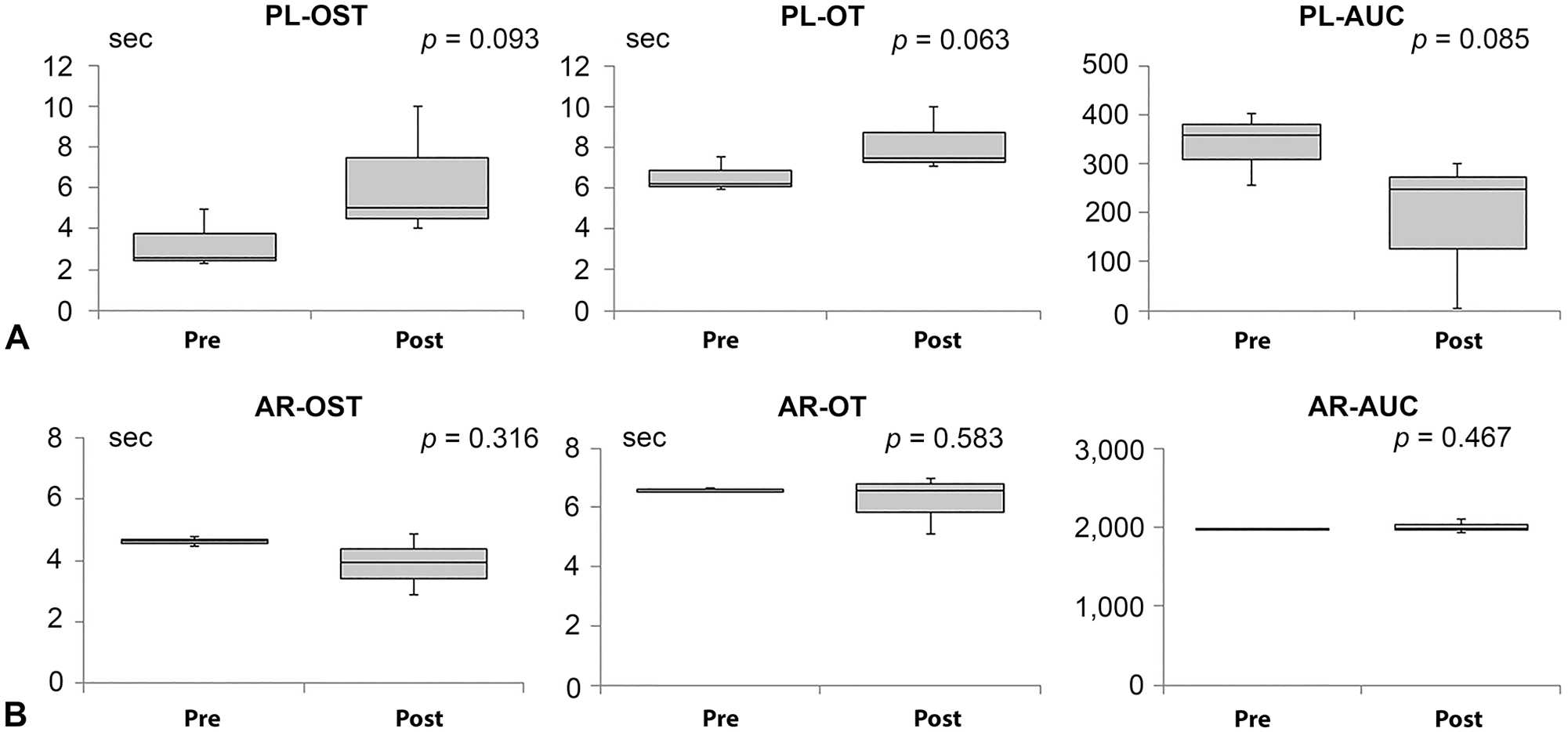
We measured the effect of ASA (sulfate salt; Bufferin combination tablet A81; Eisai) to assess whether the PL chip could detect platelet inhibition. We administered ASA (0.5 mg/kg, q24h, PO) to 3 healthy Beagles and collected blood after 2 d of administration; the blood was assessed using both AR and PL chips. Compared to control (pre-treatment) specimens, samples from animals treated with ASA exhibited right-shifts in the waveforms of PL parameters. In contrast, the waveforms of AR parameters were essentially unchanged. The right-shift of the waveform in the PL test indicates delayed occlusion as a result of suppression of platelet aggregation (Fig. 2A). We compared pre- and post-dose parameter values by 2-tailed paired t-tests using an alpha of 0.05. For PL parameters, pre- and post-dose values did not differ significantly for each parameter, but all alphas of PL parameters were <0.1; PL-OST (p = 0.093), PL-OT (p = 0.063), and PL-AUC (p = 0.085); AR-OST (p = 0.316), AR-OT (p = 0.583), and AR-AUC (p = 0.467; Fig. 3). These observations suggested that the T-TAS may be able to evaluate changes resulting from in vivo inhibition of platelet function alone, as expected after administration of ASA.
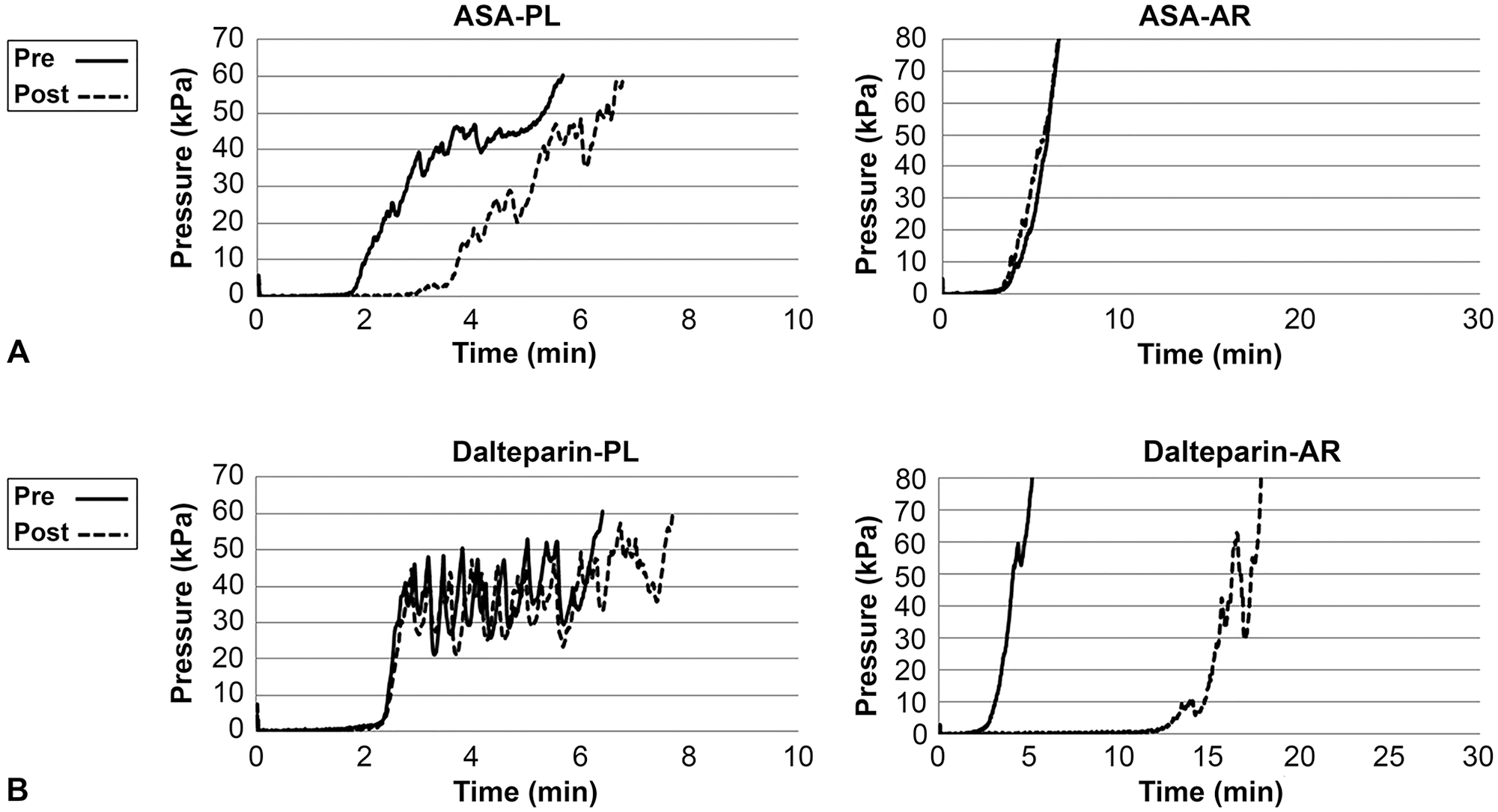
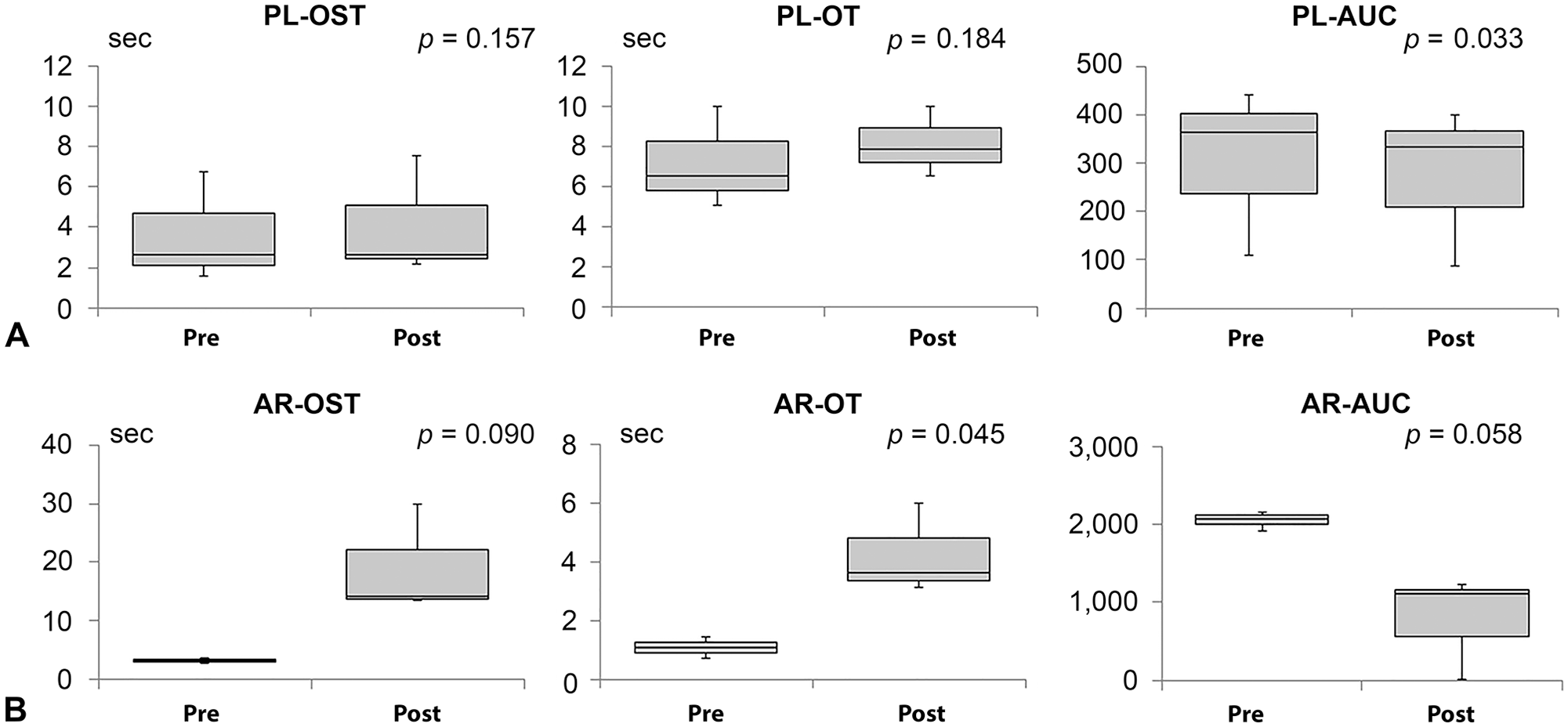
We next measured the in vitro effect of LMWH to determine whether the AR chip could detect selective changes in secondary hemostasis (i.e., in coagulation and fibrin clot formation). We collected whole blood from 3 healthy control dogs, added dalteparin sodium (5,000 IU/5 mL; Fragmin; Pfizer) at 2.0 IU/mL, and tested the samples on both AR and PL chips at 10 min after the addition of dalteparin. Compared to control samples, whole blood treated with dalteparin exhibited right-shifts in the waveforms of AR parameters. In contrast, the waveforms of PL parameters were essentially unchanged upon treatment. The right-shift of the waveform in the AR test indicates delayed occlusion as a result of suppression of coagulation (Fig. 2B). We compared pre- and post-dose parameter values by 2-tailed paired t-tests using an alpha of 0.05. For AR parameters, there was a significant difference between pre- and post-dose values only in AR-OT (p = 0.045). But alphas of other parameters, including AR-OST (p = 0.090) and AR-AUC (p = 0.058), were <0.1. Conversely, pre- and post-dose did not differ significantly for 2 of the 3 PL parameters, yielding p = 0.157 (PL-OST) and p = 0.184 (PL-OT), although a significant difference was seen for PL-AUC (p = 0.033; Fig. 4). These observations suggested that the T-TAS may be able to evaluate changes resulting from in vitro inhibition of coagulation and fibrin clot function alone, as expected after administration of dalteparin. However, it is possible that platelets were influenced by dalteparin, given the observed significant change in PL-AUC when comparing pre- and post-administration values.
The blood of all dogs tested exhibited occlusion within the defined time limit (PL, 10 min; AR, 30 min), yielding precise AUCs, with relatively low variances. Notably, AUCs were relatively stable among the parameters, with CVs of AUCs of <10% for both PL and AR chips. These results suggested that the T-TAS could be used to provide measurements of canine blood coagulation, given that the AUC measures the total process of coagulation: from start of occlusion to finished occlusion in the microduct. In both drug effect experiments, we proposed that the T-TAS may be able to show a tendency of ASA to suppress platelet function and of LMH to suppress coagulation and fibrin clot formation. However, we found no significant differences in our in vivo ASA study. This may be because of the variability in the data after ASA administration, and given the small sample size, we could not exclude type II error in our assay. Regarding our LMWH test, although the PL-OT and PL-OST did not differ significantly pre- and post-LMWH addition, PL-AUC was significantly altered. PL-OST is dependent on the onset of platelet thrombus formation; PL-AUC may reflect the overall stability of the platelet thrombus, which may be affected by the fibrin clot. 6 Therefore, we speculated that a LMWH affected PL-AUC only. Our results indicated that the T-TAS may be of use in evaluating the effects of antiplatelet and anticoagulant drugs in dog blood, as has been shown with human blood.7,14,20
There are some limitations to our study. Specifically, we measured baseline parameters in only 7 healthy control dogs, and the effects of anticoagulation drugs in only 3 dogs. We could not exclude type II error in our assay; increased sample size is needed in future studies. Additionally, the evaluation of a LMWH was performed only in vitro.
Footnotes
Acknowledgements
We thank Ms. Ayako Masuda for her excellent technical assistance with T-TAS measurement. The methods and initial evaluation in this study was presented at the 2017 American College of Veterinary Internal Medicine meeting, and the abstract is available at Iwanaga T, et al. J Vet Intern Med 2017;31:1301.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI (16K08054, 17H03926, and 20K21375) and by the Kurosumi Medical Foundation.