
Abstract
A 4-mo-old French bulldog was presented with acute onset pain and reluctance to move. A tubular structure arising in the dorsal thoracic midline and extending from a cutaneous orifice into deeper tissues was palpated on physical examination. Computed tomography with sinography revealed a dermoid sinus associated with spina bifida at the level of T3-T4. On surgical exploration, the dermoid sinus was found to communicate with the dura. Histology confirmed the diagnosis and classification as a type VI dermoid sinus. The pain response and hyperesthesia were suspected to be the result of tethered cord syndrome. Complete resolution of clinical signs was appreciated post-surgery, with the patient still free of clinical signs 3 mo later.
Dermoid sinus is defined as a congenital malformation resulting from failed separation of the neural tube from the skin ectoderm. 28 The result is typically a tubular sac that is lined with hair follicles, sweat glands, and sebaceous glands, extending from the dorsal midline to underlying tissues. 28 Six different types have been described, depending on the ventral extent of the tubular sac (Fig. 1),17,28 with type VI reported only rarely. 17 According to this classification, the open sinus tract reaches downward to the level of the supraspinous ligament (I), subcutaneous tissue (III), or dura mater (IV); in types II and VI, the patent sinus extends to the level of the muscle and supraspinous ligament, respectively, then continues as a solid fibrous cord to the ligament (II) or dura (VI). Type V is cyst-like, with no connection to the skin surface.
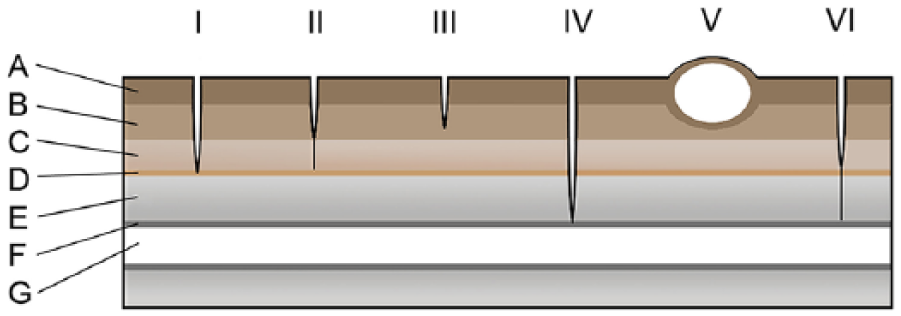
Schematic representation of the 6 different types of dermoid sinus (modified from reference 17). A = skin; B = subcutaneous tissue; C = muscle; D = supraspinous ligament; E = bone; F = dura mater; G = spinal cord.
The condition has been well documented in the Rhodesian Ridgeback,18,19 with autosomal dominant mutations involving 3 fibroblast growth factor genes identified as the cause of their characteristic dorsal ridge that also predisposes to dermoid sinus malformations. 16 Dermoid sinuses have also been reported in a variety of other canine breeds, including Boxer, 26 Shih-Tzu, 8 Boerboel, 22 Great Pyrenees dog, 6 Yorkshire Terrier, 13 Chow Chow, 4 Siberian Husky, 9 English Springer Spaniel, 24 Golden Retriever, 10 Chinese Crested dog, 17 Swedish Vallhund, 17 Victorian Bulldog, 20 Dachshund, 3 Labrador Retriever, 2 and a Labrador Retriever × Poodle. 2
Several reports have documented the presence of a dermoid sinus in association with various skeletal conditions, including hemivertebra,5,13 vertebral3,8,13 and thoracic limb malformations, 3 and spina bifida8,17,20 in dogs, and vertebral malformations 29 and spina bifida in cats. 17 A dermoid sinus–like lesion has also been documented with the presence of a myelomeningocele in a dog. 23 We describe herein a case of type VI dermoid sinus in association with spina bifida, in a French bulldog, with the principal clinical sign of back pain, suspected to be the result of tethered cord syndrome (TCS).
A 4-mo-old intact male French Bulldog was presented to New Zealand’s Massey University Veterinary Teaching Hospital because of acute onset of pain and reluctance to move. The owner reported progressive ataxia and reluctance to climb stairs, over the few weeks preceding presentation. Marked hyperesthesia was noted on attempts at evaluating for spinal hyperpathia, particularly in the cervicothoracic region. Serial neurologic examinations revealed no consistently repeatable deficits apart from the hyperesthesia of the dorsal epaxial muscles and paraspinal region. Under general anesthesia, a tubular structure, extending from an opening in the skin into the deeper subcutaneous tissue was palpated over the cranial thoracic spine. In addition, an opening at the skin surface was noted following clipping over the area, raising suspicion of a dermoid sinus. Computed tomography (CT) with sinography revealed a dermoid sinus associated with spina bifida at the level of T3-T4, believed to be type III based on imaging findings (Fig. 2). Variable degrees of spina bifida and spinous process malformation were also identified at T2 and T6.

Computed tomography with sinography of a type VI dermoid sinus, bone-window, thoracic spine, in a French bulldog.
The sinus was observed to communicate with the dura at T3-T4, after performing a dorsal laminectomy and expanding the bone defect around the sinus with a pneumatic bur. Sharp dissection was used to resect the sinus from the dura (Fig. 3). Hair was visualized inside the sinus following its removal.
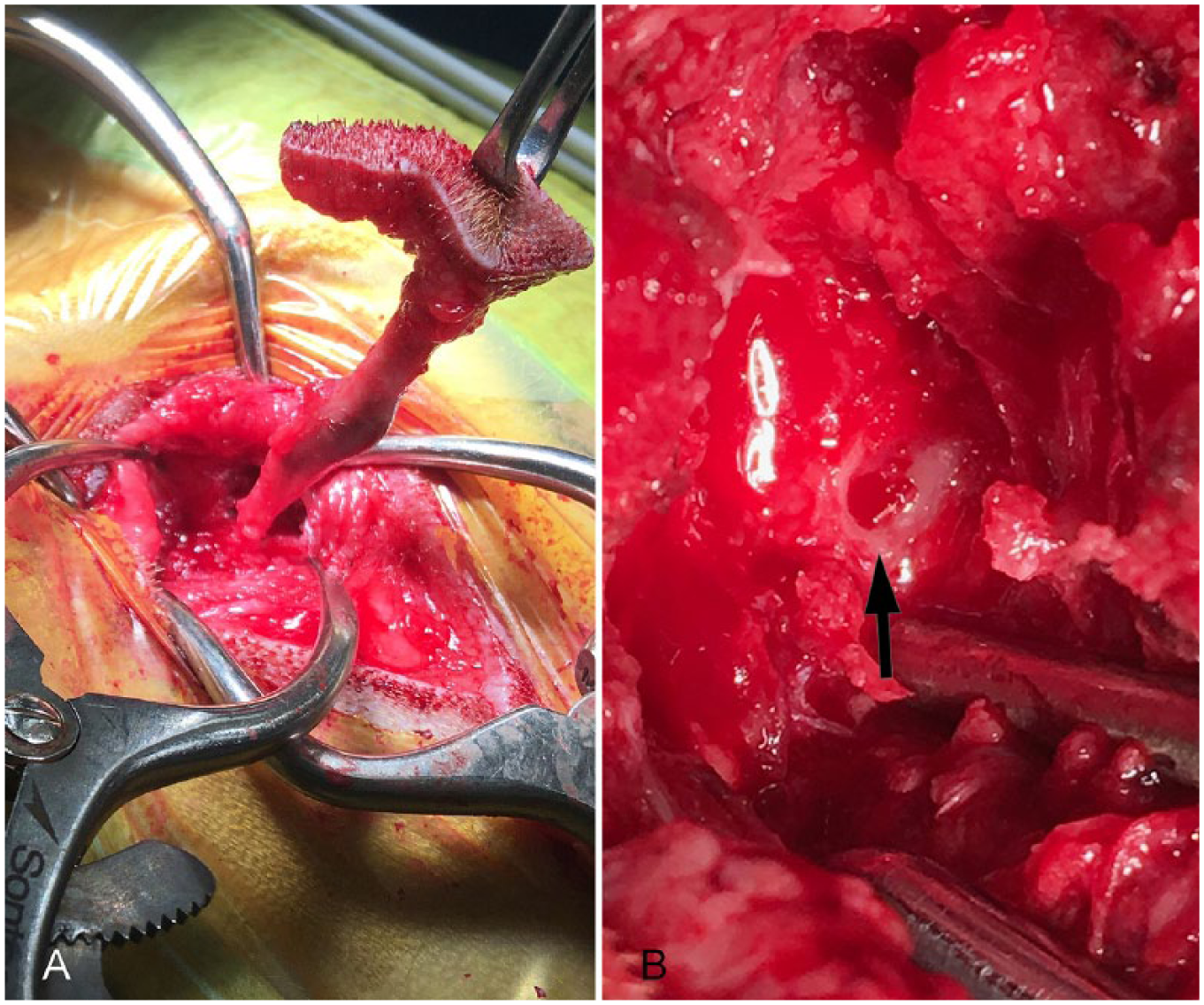
Type VI dermoid sinus with spina bifida at T3-T4 in a French bulldog at the time of surgery.
Histology demonstrated a thin-walled tubule lined by keratinizing stratified squamous epithelium, with a prominent stratum granulosum (Fig. 4). Within the lumen, ample amounts of lamellar keratinaceous debris and hair fragments were present. Thick concentric layers of collagen were present around the tubule wall. Several well-developed folliculosebaceous units, consisting of hair follicles, sebaceous glands, and apocrine glands, radiated away from the tubule wall. Proximally, the cyst opened to the skin, whereas distally, it transitioned into a thick band of fibrous connective tissue that inserted into woven bone and contained occasional folliculosebaceous units. The superficial skin included 2 separate foci of infiltration and obliteration of hair follicles by large numbers of neutrophils and lesser numbers of histiocytes, lymphocytes, and plasma cells. Such findings were consistent with a type VI dermoid sinus, along with mild, chronic folliculitis and furunculosis. The patient had complete resolution of clinical signs post-surgery and remains pain-free 3 mo later.
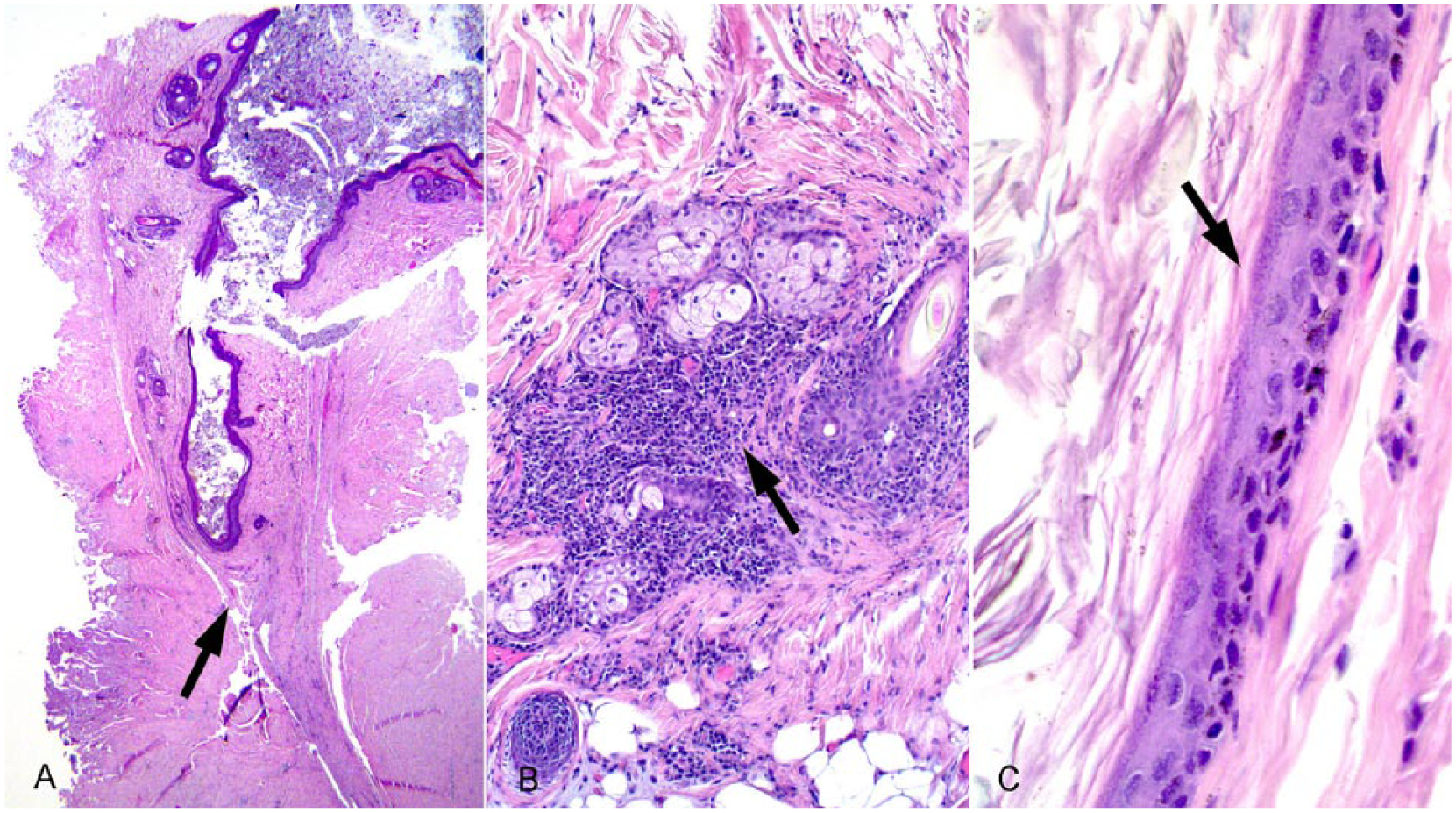
Histology of a type VI dermoid sinus with spina bifida at T3-T4 in a French bulldog.
Spina bifida is defined as failure of the vertebral arch(es) to close over the spinal cord. 28 This failure is further classified into either occulta (closed) or aperta, based on the amount of neural tissue involvement. 28 Spina bifida occulta has no neural tissue involved, whereas spina bifida aperta is either associated with a meningocele or meningomyelocele. 28 With no neural tissue involved, the spina bifida in our case is subclassified as occulta. Neural tube defects can occur in various combinations; however, concurrent spina bifida and dermoid sinus in dogs has been reported only rarely.17,20
The most commonly reported clinical signs in cases of dermoid sinus, prompting further investigation, are typically neurologic abnormalities ranging from abnormal motor function to paraparesis. 19 Pain and/or hyperesthesia have been described only rarely as part of the clinical presentation in dogs with a dermoid sinus.13,26 Potential causes include spinal cord compression 13 and meningomyelitis secondary to infection of the dermoid sinus. 26 In our case, we propose that the pain response and hyperesthesia were secondary to TCS, given the resolution of clinical signs post-surgery. TCS is defined as excessive stretching and tension on neural tissues, as a result of abnormal attachments to the vertebrae or skin. 28 This syndrome has been described only rarely in dogs.7,12,14,21,27 To our knowledge, TCS has not been reported in association with a dermoid sinus in a dog. It has, however, been commonly identified in human cases of dermal sinus, with one case series reporting an incidence as high as 79%. 1 Typically TCS results in progressive worsening of neurologic deficits, including pelvic limb paresis and various degrees of fecal and urinary incontinence accompanying skeletal growth. 28 Diagnosis is based on one or more of the following: advanced imaging findings demonstrating traction or elevation of the dura,7,14 visualization at time of surgery, 12 or improvement or resolution of neurologic deficits post-surgery. 27 The marked clinical improvement found in our dog after surgical intervention is concordant with outcomes in humans after surgical correction of TCS in association with spinal cord defects.11,15 In these human cases, surgery often results in better cord mobility and symptomatic improvement, including resolution of upper motor neuron deficits and enhanced urinary bladder function.11,15
Various imaging modalities have been utilized in an attempt to determine the ventral extent of dermoid sinuses, including radiography or CT with sinography, and more recently the use of magnetic resonance imaging (MRI). In our case, CT with sinography failed to correctly define the ventral extent of the sinus, likely because hair and adnexal tissue filled the deeper extent of the sinus, which prevented complete filling with contrast. Unfortunately, even with advanced imaging modalities such as MRI, the true extent is often underestimated.17,25 Our case, along with the rare reports of dermoid sinus in association with spina bifida,17,20 suggests that such association should prompt suspicion of communication with the dura, despite imaging findings. In addition, pain and/or hyperesthesia may be part of the clinical presentation of such dogs, potentially secondary to TCS, given the communication with the dura. Appropriate surgical management is necessary to prevent long-term neurologic deficits.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.