
Abstract
Between January 1, 2013 and December 31, 2015, findings of a New York State Gaming Commission–Cornell University postmortem examination program were utilized in a multi-disciplinary mortality review process to review 129 racing fatalities at Thoroughbred racetracks operated by the New York Racing Association (NYRA). Musculoskeletal fractures comprised 79% of the fatalities; cardiopulmonary conditions accounted for 12% of the fatalities. Other causes of death included gastrointestinal (3%), respiratory (5%), and central nervous system (2%) conditions. Fetlock failure represented 50% of the musculoskeletal fatalities. The general distribution of these findings was very similar to that reported by the California Animal Health and Food Safety Laboratory System during the same period. These findings, used in conjunction with a comprehensive mortality review process and regulatory reform, have contributed to a significant reduction of the incidence of Thoroughbred racing fatalities at NYRA racetracks during the period of this review.
Introduction
Thoroughbred horse racing is a glamorous and exciting sport that is rich in tradition, and it is practiced by many cultures worldwide. Nevertheless, Thoroughbred racing in North America is an industry in crisis, confronted by changing population demographics, an aging fan base, and direct competition with alternative wagering platforms and entertainment options (Singer D, Lamb M. Driving sustainable growth for Thoroughbred racing and breeding: findings and recommendations. The Jockey Club Roundtable. 2011. https://goo.gl/PVp4j5). Thoroughbred horse racing is inherently dangerous, given that races are conducted with horses and riders maneuvering in close proximity at speeds of up to 60 km/h (38 mi/h). Equine racing fatalities represent a tragic personal loss for horse owners, trainers, and caretakers, and a public relations nightmare for the industry. For these reasons and the obvious equine welfare considerations, risk management and reduction of equine fatalities are top priorities.
The New York State Gaming Commission–Cornell University (NYSGC-CU) postmortem examination program was created as a recommendation of the New York Task Force on Racehorse Health and Safety in the fall of 2012 following an investigation of a cluster of fatalities that occurred during the Aqueduct winter 2011–2012 meet (https://goo.gl/ItHNLk). The postmortem examination protocols used at Cornell University were modeled after those of the postmortem examination program of the California Horse Racing Board (CHRB), operated by the California Animal Health and Food Safety Laboratory System (CAHFS) at the University of California, Davis.
The goal of the NYSGC-CU postmortem examination program is to document pathologic findings in horses that die or are euthanized while training or racing at New York racetracks and to use this information to 1) direct tactical epidemiologic research intended to identify horses at increased risk of injury, 2) provide individual feedback to horsepersons and veterinarians caring for the injured horses through a mortality review process, 3) provide evidence-based recommendations to the NYSGC for rulemaking intended to reduce injury of horses and riders and generally enhance equine welfare, and 4) develop continuing education programs for trainers and veterinarians in order to minimize equine fatalities in the future. The objective of our study was to summarize the findings of the NYSGC-CU postmortem examination program during a 3-y period (2013–2015) and to investigate the use of this information by a multi-disciplinary mortality review board to reduce the incidence of equine fatalities at racetracks operated by the New York Racing Association (NYRA).
Materials and methods
Horses (n = 129) that experienced racing, training, or non-exercise fatalities at NYRA racetracks between January 1, 2013 and December 31, 2015 were transported to The Animal Health Diagnostic Center (AHDC) at Cornell University (Ithaca, NY) for postmortem examination. Autopsies were performed, and samples of major internal organs, including a routine set of samples and any grossly abnormal tissue were obtained for histologic analysis. Laboratory tests and cultures were performed as indicated in all cases of infectious disease. The reporting of clinical history and diagnostic findings for all organ systems provided a broad context for the definitive cause of injury or death. Subsequent to the gross examination of the carcass and visceral organs, detailed dissection of the affected and contralateral limb was performed with emphasis on identifying pre-existing musculoskeletal lesions that may have contributed to the injury.
Coincident with the above postmortem examination, interviews were conducted with trainers, jockeys, and attending veterinarians of the fatally injured horses by NYSGC investigators. Veterinary treatment records and the results of diagnostic imaging obtained within 60 d of the incident event were reviewed. The NYSGC Equine Steroid Administration Log was examined to determine if intra-articular corticosteroid injections were administered within 60 d of the incident. Exercise history of the injured horse from the first official workout to the incident event was reviewed and analyzed. Gaps in training were investigated. Both categorical and continuous data from the exercise history were used to determine what, if any, risk factors were present at the time of the incident. High-definition video recordings of the incident races were reviewed with input from the track stewards and a retired Thoroughbred jockey in cases where jockey performance may have contributed to the incident. Drug testing results from the New York State Drug Testing and Research Program were reviewed. Weather conditions, racing surface moisture content, and track maintenance procedures at the time of the incident event were also reviewed. The NYRA Equine Safety Review Board (ESRB) convened to discuss the findings of the investigation. Follow-up interviews with trainers and other stakeholders were conducted as necessary to address questions or concerns discovered during the course of the investigation. Subsequent to reaching a consensus on the findings of the investigation, the chair of the ESRB discussed the findings with the trainer and made recommendations, where appropriate, to help avoid future injuries. These meetings are intended to serve as a teaching opportunity to help trainers, veterinarians, and other stakeholders prevent equine fatalities in the future. No punitive action was taken, except in cases that involved discovery of a violation of NYSGC regulations, NYRA house rules, or a significant animal welfare concern.
In order to determine the impact of this program upon racing fatality rates, the incidence rate of racing fatalities was compared for a 3-y period before and after the postmortem examination and mortality review program was put in place. The cumulative incidence of racing fatalities at NYRA tracks from 2010 to 2012 was compared to the 3-y period immediately following implementation of this program (2013–2015). The cumulative incidence of racing fatalities for both periods was computed as the total number of racing fatalities during the respective period out of the total number of race starts during the same period. The significance of difference between the 2 incidences was compared using the t-test at p ≤ 0.05. The analysis was performed using Statistix9 (Analytical Software, Tallahassee, FL).
Results
Thoroughbred racehorses (n = 129) that died or were euthanized at NYRA racetracks between January 1, 2013 and December 31, 2015 were presented to the Cornell University AHDC for postmortem examination. There were 25 submissions in 2013, 49 submissions in 2014, and 55 submissions in 2015. Autopsy, histology, and detailed limb dissection were performed in all 129 cases. Laboratory tests and cultures were performed as indicated in all cases of infectious disease. The distribution of submissions per month is shown in Figure 1. The median age of the horses submitted for postmortem examination was 4 y, with a range of 2–12 y (Fig. 2). In this study population, there were 42 intact males, 50 intact females, and 37 geldings (Fig. 3).
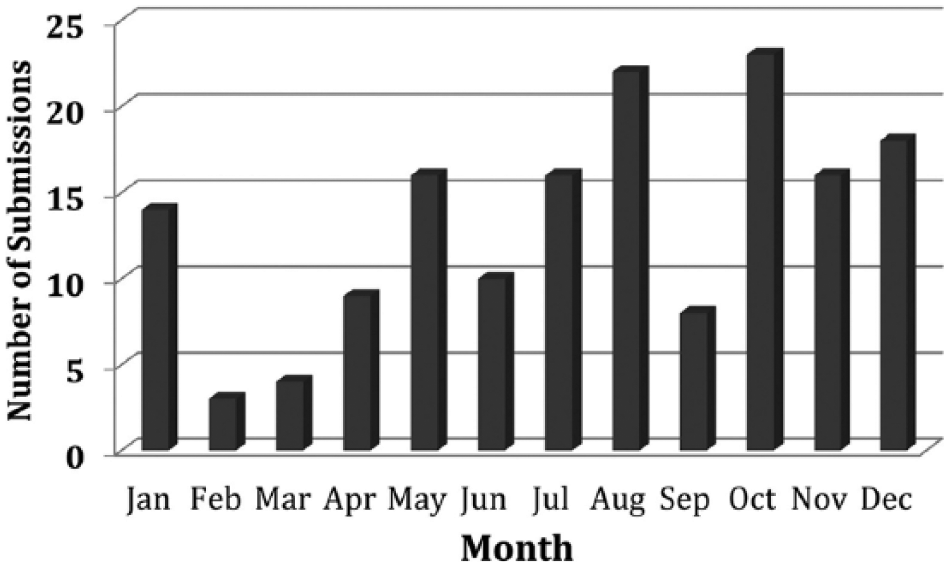
Number of New York Racing Association submissions to the New York State Gaming Commission–Cornell University postmortem examination program between 2013 and 2015 sorted by month.
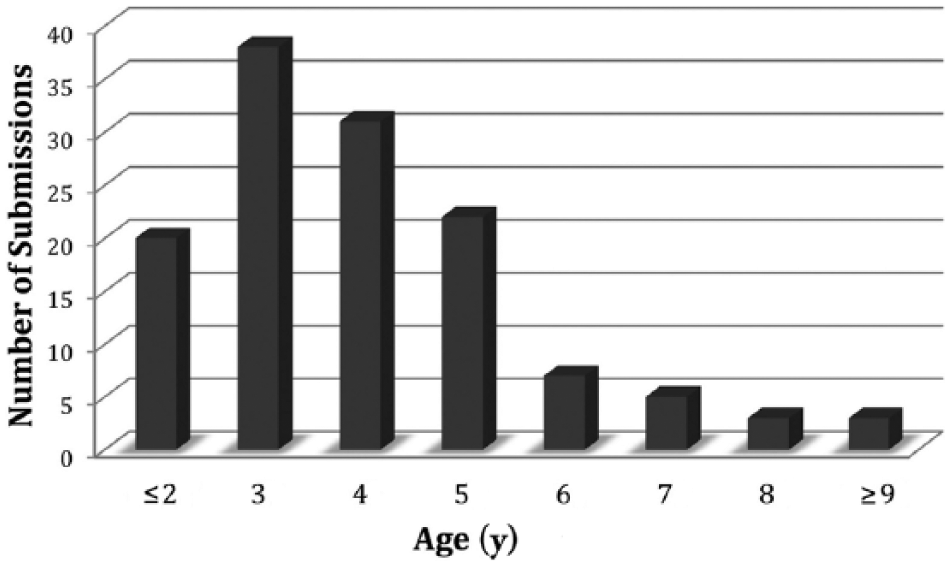
Number of New York Racing Association submissions to the New York State Gaming Commission–Cornell University postmortem examination program between 2013 and 2015 sorted by age.
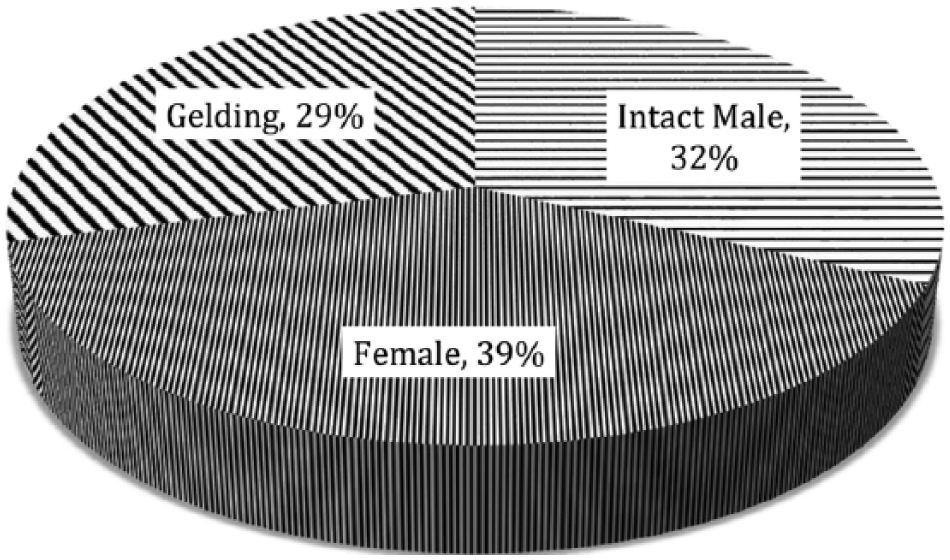
Number of New York Racing Association submissions to the New York State Gaming Commission–Cornell University postmortem examination program between 2013 and 2015 sorted by sex.
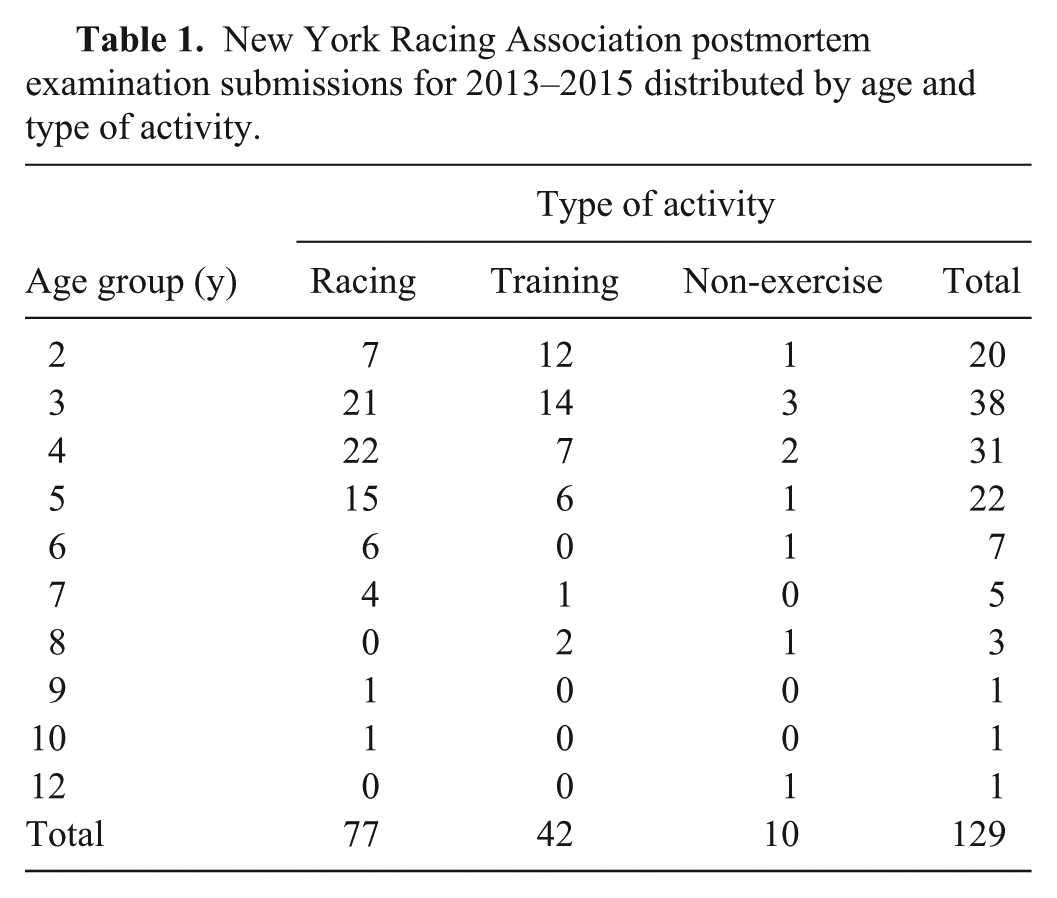
Seventy-seven horses were injured while racing; 42 horses were injured while training; 10 horses died during non-exercise activities (Table 1). Musculoskeletal injuries accounted for 102 fatalities (79%). Sixteen fatalities (12%) involved the cardiovascular system. Other causes of death included 4 gastrointestinal (3%), 6 respiratory (5%), and 2 central nervous system (2%) fatalities (Table 2). One horse had a combination of a cardiovascular system (sudden death) and a musculoskeletal injury (lateral condylar fracture). In this case, the cardiovascular event was determined to be the actual cause of death.
New York Racing Association postmortem examination submissions for 2013–2015 distributed by age and type of activity.
Distribution of fatalities at New York Racing Association racetracks for 2013–2015 by primary organ system as the proximate cause of death or euthanasia.*
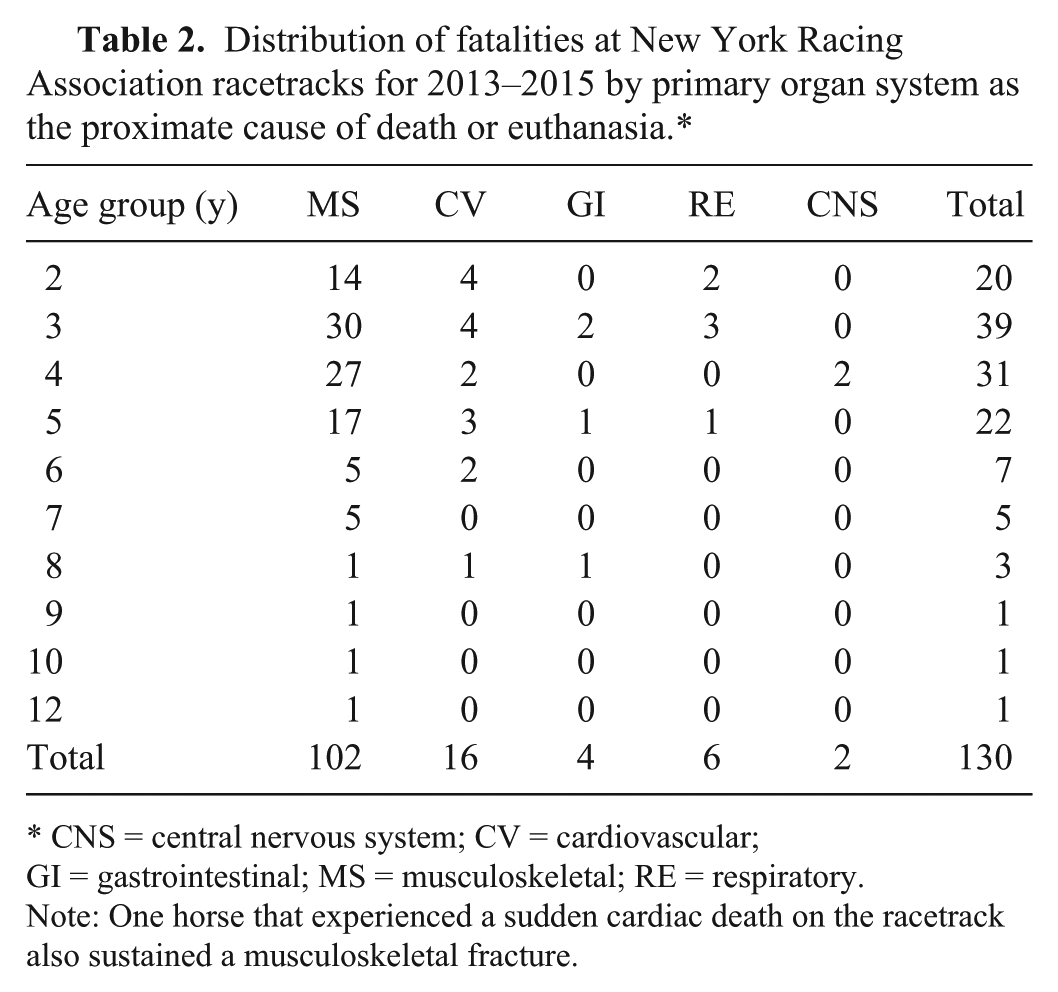
CNS = central nervous system; CV = cardiovascular; GI = gastrointestinal; MS = musculoskeletal; RE = respiratory. Note: One horse that experienced a sudden cardiac death on the racetrack also sustained a musculoskeletal fracture.
Cardiovascular fatalities included major vessel rupture, coronary or myocardial abnormalities, and suspected cardiac arrhythmias believed to have contributed to sudden death on the racetrack. Gastrointestinal fatalities included inflammatory conditions of the bowel, strangulation of small intestine and the large colon, and epiploic foramen entrapment. Respiratory conditions included a postoperative laryngeal infection and exercise-induced pulmonary hemorrhage. Central nervous system conditions included equine protozoal myeloencephalopathy.
A total of 108 fatal musculoskeletal injuries (FMSI) occurred in 102 horses (Table 3). The most common FMSI in this group of Thoroughbred horses included condylar fractures of the third metacarpal bone, diaphyseal fractures of the third metacarpal bone, proximal sesamoid bone fractures, carpal fractures, and humeral fractures (Table 4). In addition to the fractures, there were 3 fatal musculoskeletal injuries that involved the distal sesamoidean ligaments, and 1 horse experienced a rupture of the superficial digital flexor tendon.
Distribution of fatal musculoskeletal injuries at New York Racing Association racetracks for 2013–2015 by age and location.*
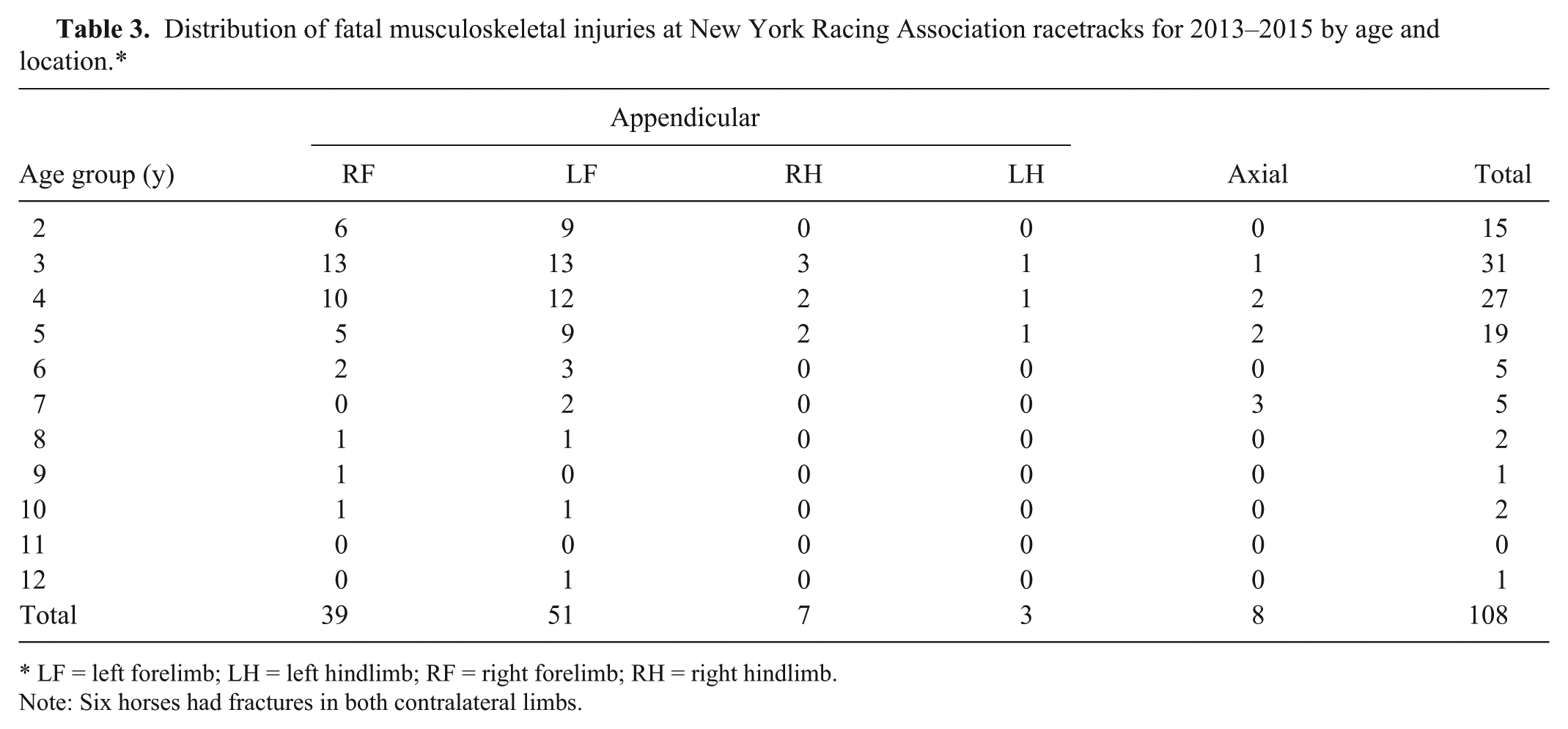
LF = left forelimb; LH = left hindlimb; RF = right forelimb; RH = right hindlimb. Note: Six horses had fractures in both contralateral limbs.
Distribution of the fatal musculoskeletal injury types at New York Racing Association racetracks for 2013–2015 by age.*
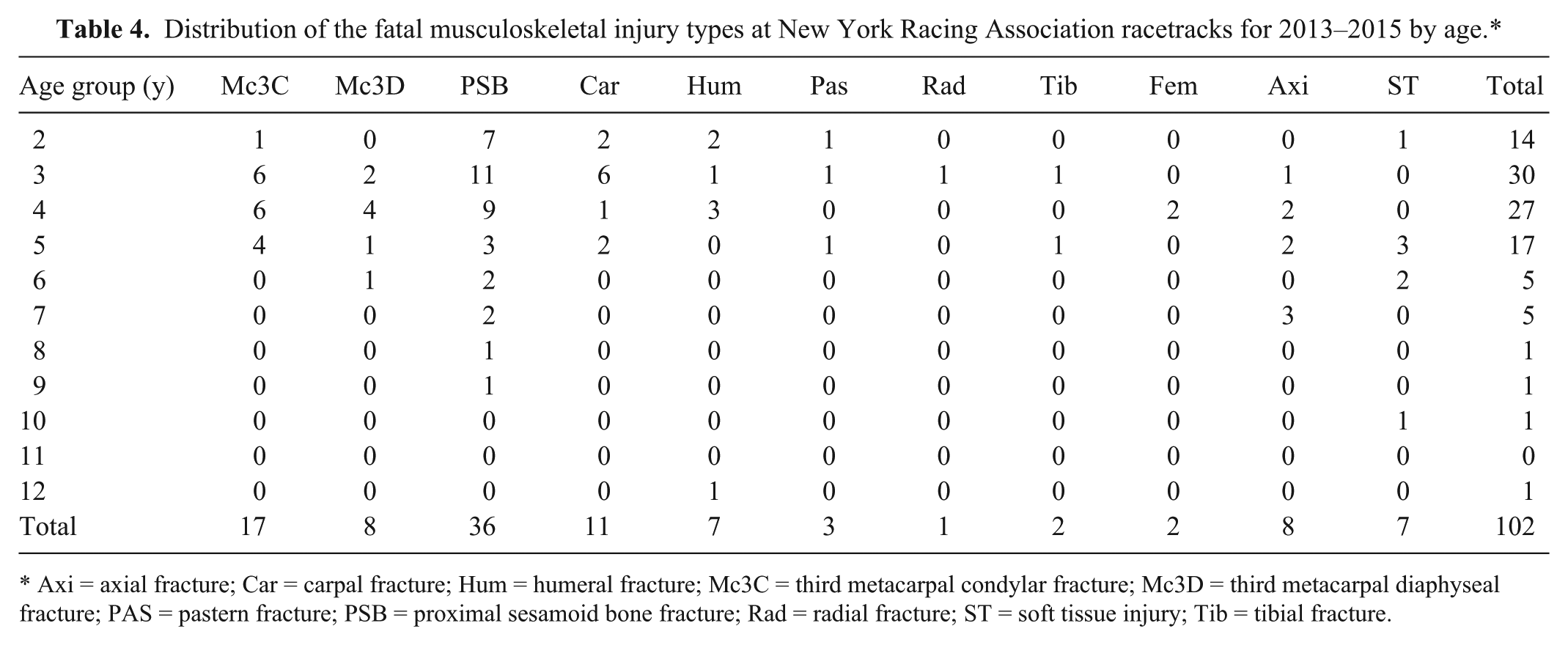
Axi = axial fracture; Car = carpal fracture; Hum = humeral fracture; Mc3C = third metacarpal condylar fracture; Mc3D = third metacarpal diaphyseal fracture; PAS = pastern fracture; PSB = proximal sesamoid bone fracture; Rad = radial fracture; ST = soft tissue injury; Tib = tibial fracture.
Advanced subchondral bone sclerosis or necrosis and articular cartilage scoring were common pre-existing findings associated with fractures of the carpus, metacarpus, proximal sesamoid bones, and the first phalanx. In the 94 horses with fatal appendicular fractures, 76 horses (80%) had pre-existing cartilage injury (scoring, fibrillation, ulceration), and 56 horses (59%) had subchondral bone sclerosis or necrosis. Subchondral bone sclerosis and cartilage injury was often found in both the fractured limb and the contralateral limb. Examples of pre-existing subchondral bone sclerosis and/or necrosis are illustrated in Figures 4–9. Examples of pre-existing cartilage damage are illustrated in Figures 10–12.
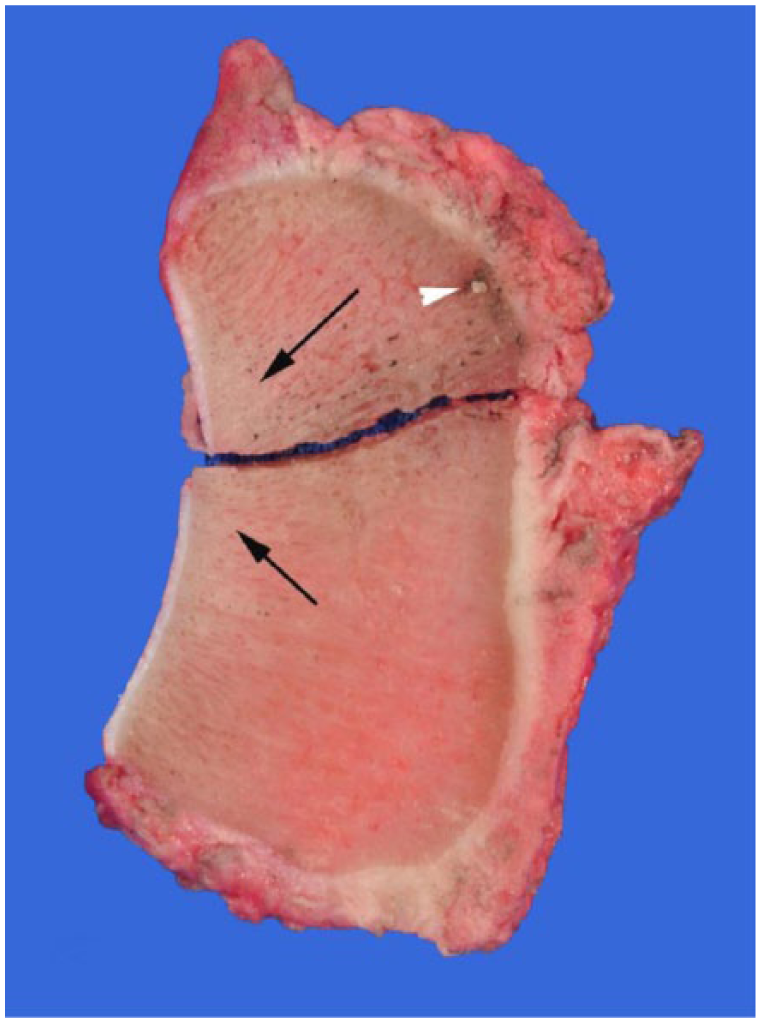
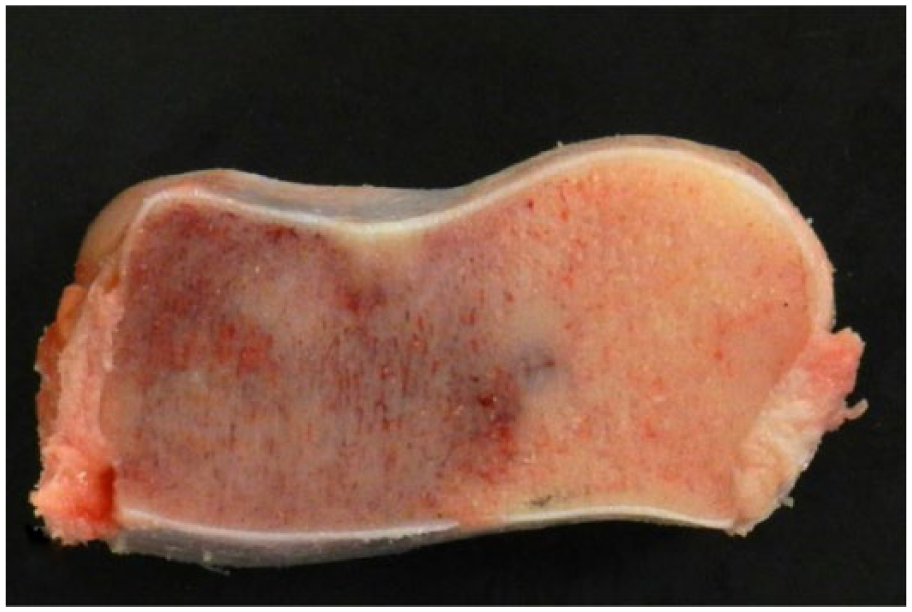
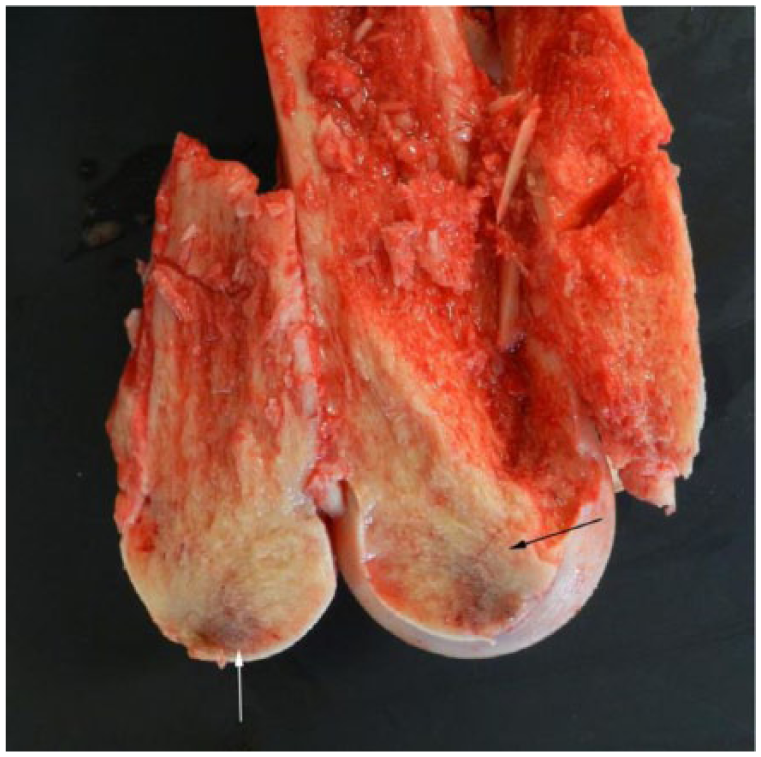
Sagittal section of a proximal sesamoid bone with an apical fracture. Note the generalized increased bone density in this specimen. The fracture line is located at the junction of advanced bone sclerosis (black arrows) and a localized area of subchondral bone necrosis (white arrowhead).
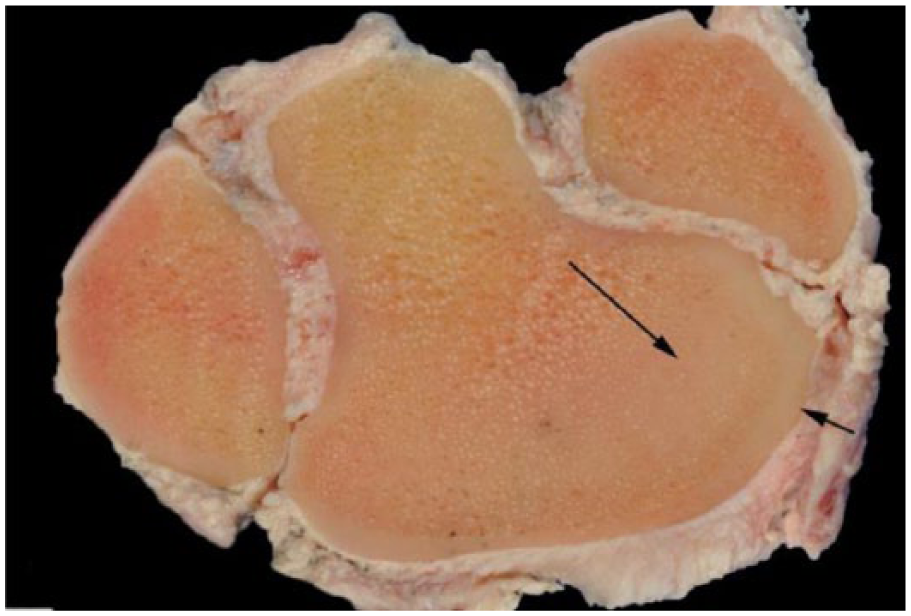
Transverse section of the second, third, and fourth carpal bones. Note the generalized increase in bone density, which is especially pronounced in the subchondral bone of the radial facet of the third carpal bone (arrows).
Transverse section of the second, third, and fourth carpal bones with an area of bone necrosis surrounded by an area of severe sclerosis in the radial facet of the third carpal bone.
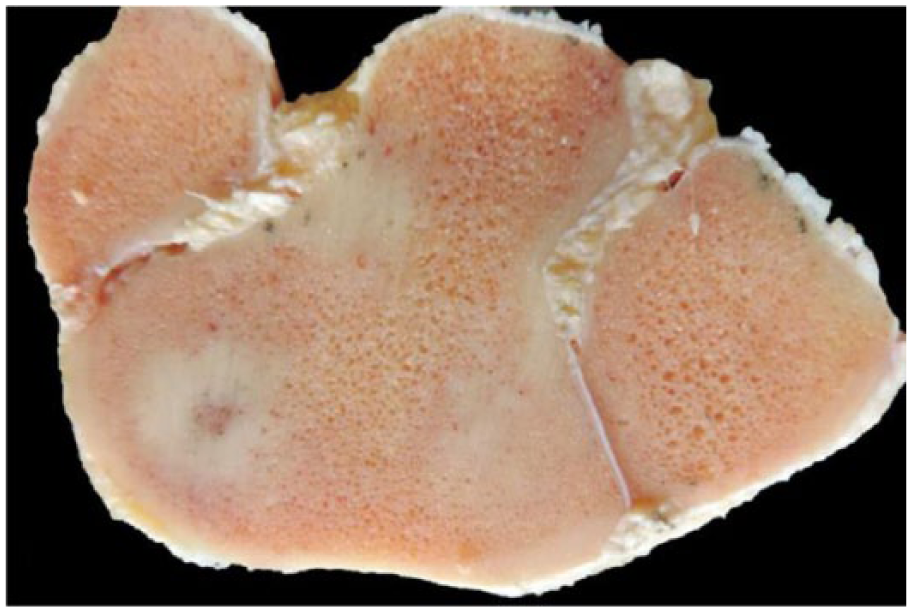
Sagittal section of the third carpal bone with advanced subchondral bone sclerosis and necrosis in the dorsal aspect of the bone.
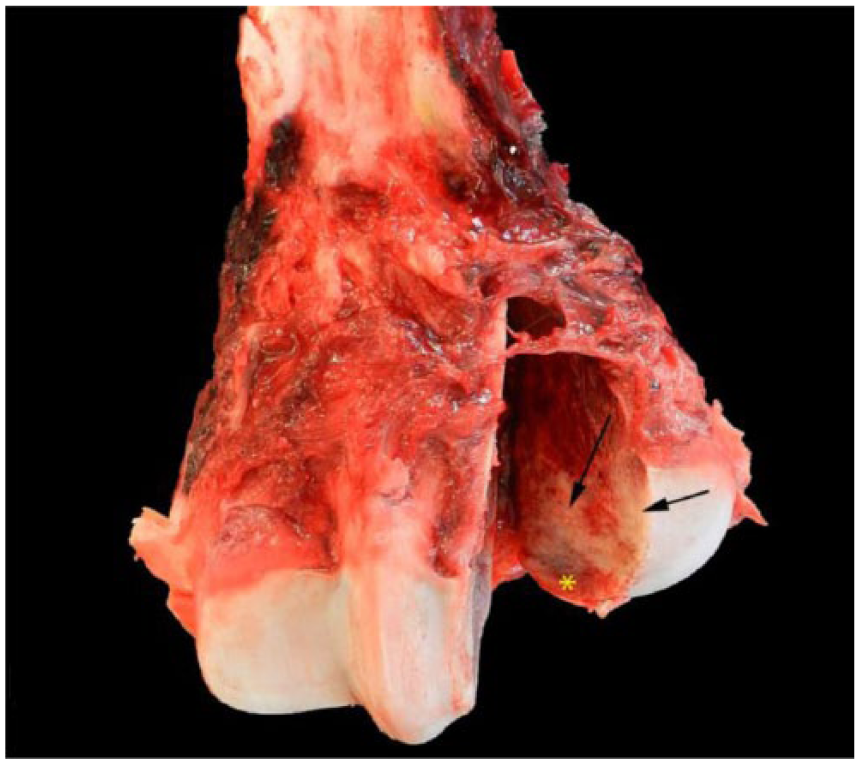
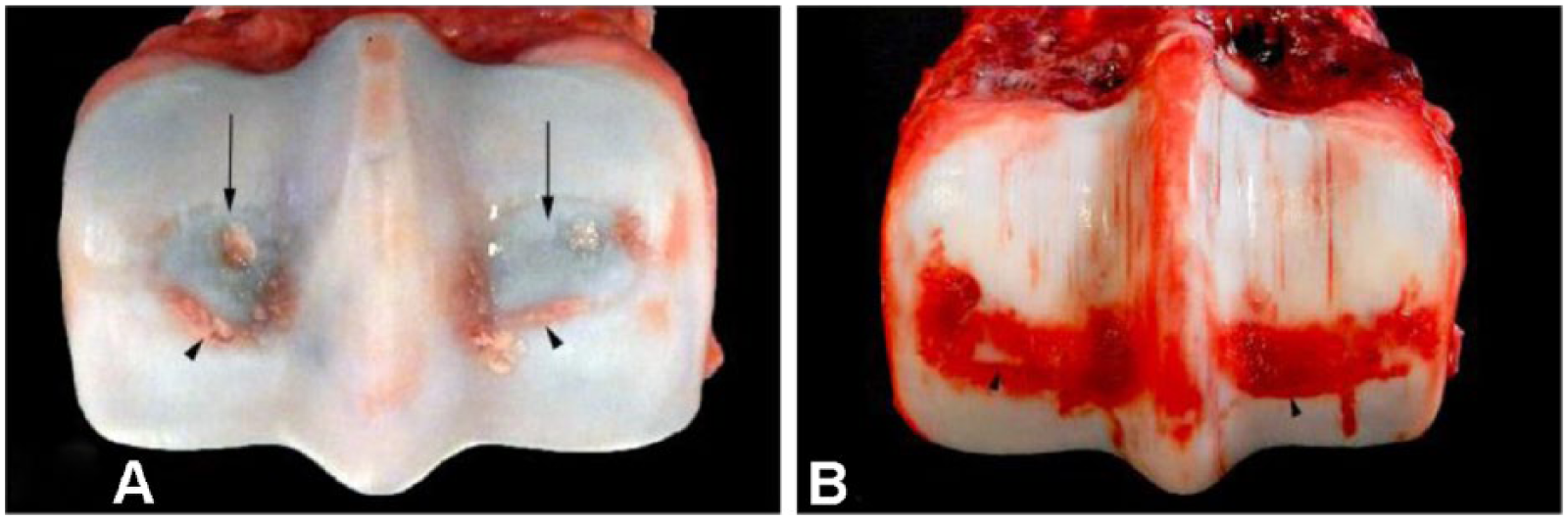
Lateral condylar fracture at the base of the midsagittal ridge of the third metacarpal bone. Note that the fracture line propagated through an area of subchondral bone necrosis (asterisk) and sclerosis (arrows).
Fractured surface of a lateral condyle of the third metatarsal bone revealing advanced subchondral bone sclerosis (black arrow) and necrosis (white arrow).
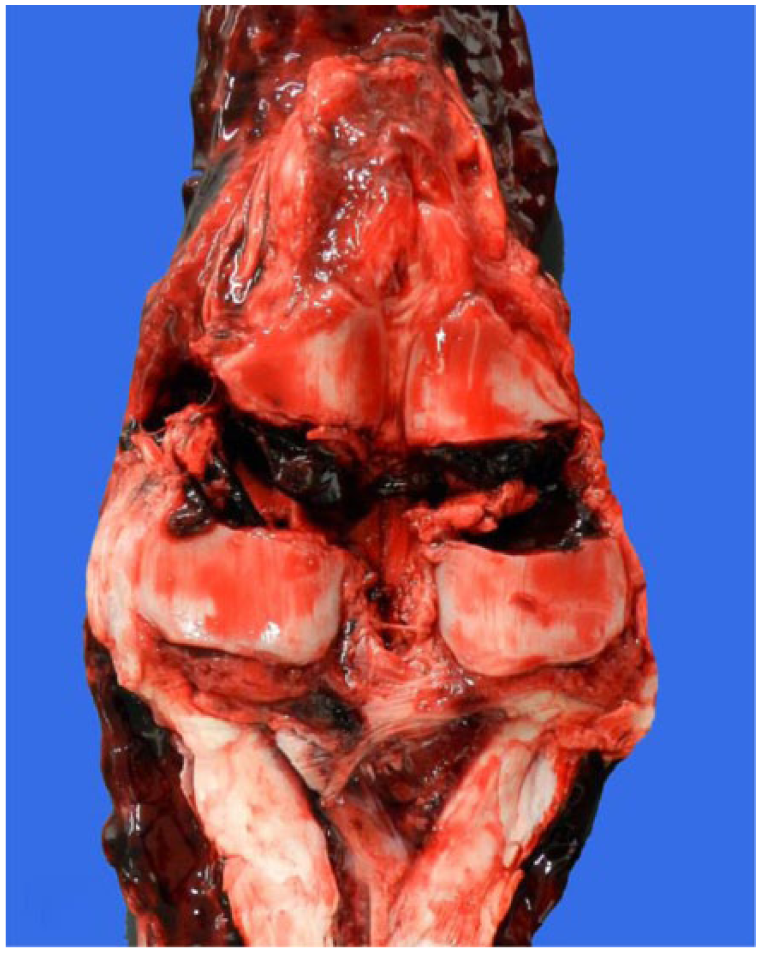
Biaxial mid-body fracture of the proximal sesamoid bones. Note the presence of extensive cartilage ulceration and score lines on the articular surfaces of both proximal sesamoid bones and disruption of the intersesamoidean ligament.

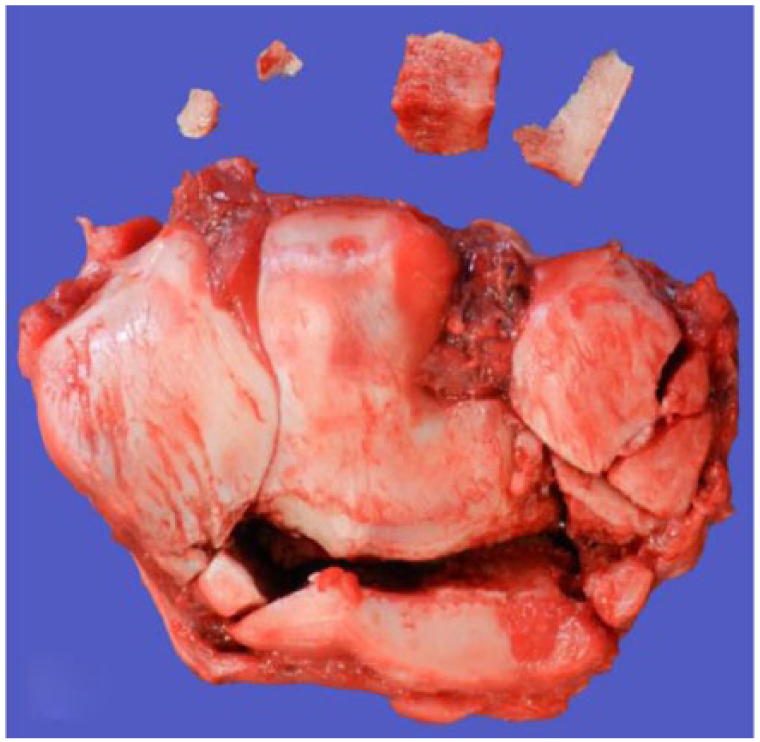
Biaxial proximal sesamoid bone fracture with severe comminution of the base of the medial proximal sesamoid bone. The presence of a sagittal fracture line dividing the base of one of the proximal sesamoid bones was a common finding in cases of biaxial proximal sesamoid bone fracture. Note the presence of score lines in the articular cartilage of the sesamoid bones.
Distal articular surfaces of the left.
The first phalanx was fractured in 3 horses. Although pastern fractures were relatively uncommon, they were often extensively comminuted and found in conjunction with condylar fractures of the third metacarpal bone and/or proximal sesamoid bone. This combination of injuries results in instability of the fetlock joint (e.g., Fig. 13). It was not uncommon to find multiple fractures at the time of postmortem examination, not all of which were identified at the time of triage at the racetrack.

Comminuted compound fractures of the third metacarpal bone and/or the first phalanx frequently result in fetlock joint instability (fetlock failure).
There were 7 humeral fractures in this group of horses. Humeral stress fractures were most often seen in younger (2- to 4-y-old) horses, with the catastrophic fracture line propagating through a pre-existing area of callus on the surface of the bone (Fig. 14). The humeral fracture that occurred in the 12-y-old horse occurred as a direct result of a fall on the steeplechase course.

Humeral stress fracture that propagated through an area of bony callus in the caudal and proximal shaft of the bone just distal to the humeral head (arrow).
Secondary diagnostic findings of horses submitted for postmortem examination that were felt to be significant, but unrelated to the primary cause of death, commonly included exercise-induced pulmonary hemorrhage and gastric ulceration. Pre-existing secondary musculoskeletal findings in this group of racehorses included subchondral bone sclerosis, cartilage erosion, ulceration and fibrillation (Fig. 15), osteophytes, chip fractures, joint capsule fibrosis, and traumatic disruption of ligaments and tendons.
Comminuted slab fracture of the radial and intermediate facets of the third carpal bone and a comminuted fracture of the second carpal bone. Note the presence of extensive cartilage damage on the articular surfaces of these bones.
During the period of study, there were 21 episodes of sudden death of horses at NYRA racetracks. These incidents were not uniformly distributed within the 3-y period: 2013 (n = 3); 2014 (n = 11); 2015 (n = 7). In 5 cases of sudden death, exercise-induced pulmonary hemorrhage was found to a degree sufficient to be implicated as the likely cause of death of the horse. In 2 cases, there were ruptures of major blood vessels (1 cranial mesenteric artery and 1 left pulmonary artery). In one case, there was evidence of moderate coronary arteriosclerosis and myocarditis with involvement of the His bundle, which may have precipitated rhythm disturbances. In another case, there was an anomalous coronary artery in conjunction with locally extensive areas of focal ventricular myocardial degeneration, fibrosis, and repair, suggestive of a previous ischemic event. In 12 cases, there were no abnormal findings of the heart or lungs, leading to an open diagnosis.
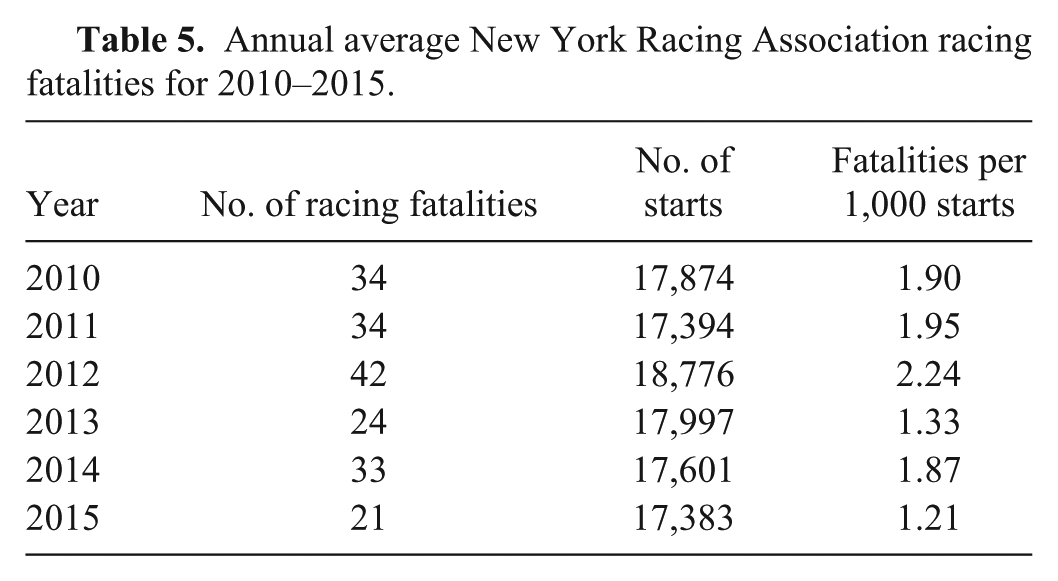
The average NYRA racing fatality rate for 2010–2012 was 2.04 per 1,000 starts (Table 5). This time period includes the 3 y leading up to the creation of the NYSGC-CU Postmortem Examination Program and the NYRA ESRB. The average NYRA racing fatality rate for the subsequent 3 y, 2013–2015, was 1.47 per 1,000 starts (Table 5), which is a 28% decrease compared to 2010–2012. Horses that raced in the 3-y period following implementation of the NYSGC-CU program and ESRB review process were at decreased risk of fatality compared to horses that raced in the 3-y period immediately prior to implementation of this program (p < 0.03).
Annual average New York Racing Association racing fatalities for 2010–2015.
Discussion
For many years, the California postmortem examination program reported the presence of pre-existing bone lesions in Thoroughbred horses that experience catastrophic injuries.1,2,7,9,10 Similar findings were reported by researchers in the United Kingdom. 6 The NYSGC-CU postmortem examination program findings support these observations. The presence of subchondral bone sclerosis and necrosis in the third carpal bones, the distal aspect of the third metacarpal bones, and the proximal sesamoid bones likely plays an important role in the pathophysiology of catastrophic injury of these structures. Conveying this information to veterinarians and trainers is an important first step to increase awareness of the risk related to training horses with such bone lesions. However, our ability to identify horses at increased risk of injury is often confounded by the absence of clinical signs associated with early stages of this process, the absence of specific and sensitive diagnostic aids (e.g., bone markers), and the cost and relative lack of convenience and/or availability of advanced diagnostic imaging that can detect these changes (e.g., CT and MRI in particular). Additionally, there is a need for longitudinal studies to define “normal” bone modeling and remodeling in the bones of Thoroughbred horses in the formative stages of active race training. Although it is abundantly clear that bone remodeling is an essential process in the construction of a healthy skeleton able to withstand the stress of race training, the detection of maladaptive bone remodeling, particularly in its early stages, remains a challenge.
The fact that in some cases more than one fracture was identified during the postmortem examination, some of which were not diagnosed at the time of examination at the racetrack, is not surprising and has been reported in other studies. 8 This observation reflects the obvious differences between a clinical and a postmortem examination, as well as the fact that horses with open catastrophic fractures of the distal extremity have such a poor prognosis for treatment that many of these horses were euthanized without benefit of a radiographic examination.
Exercise-induced pulmonary hemorrhage (EIPH) is a common finding in racehorses, but is rarely believed to be a cause of sudden death. The American College of Veterinary Internal Medicine consensus statement points out that there is only low-quality evidence of an association between EIPH and sudden death of Thoroughbred horses. 4 The authors in one large multicenter study imply that only cases of chronic pulmonary hemorrhage with findings of hemosiderophages and pulmonary fibrosis should be considered as likely causes of sudden death in Thoroughbred racehorses. 5 However, another study found that repeated blood instillation into the airway of the horse does not cause pulmonary fibrosis, drawing into question the association between fibrosis and EIPH. 11 Further, an additional study found only acute hemorrhage into alveoli, bronchi, interstitium, and subpleural spaces in one-third of horses that died with EIPH. This subset of horses had no evidence of fibrosis or inflammation. 3
No pulmonary fibrosis was found in any of the 5 cases in which the cause of death was attributed to EIPH in our study, but one horse did have significant numbers of alveolar macrophages with hemosiderin, compatible with prior episodes of pulmonary hemorrhage. In one case, acute centrilobular coagulative necrosis in the liver, compatible with rapid development of severe hypoxia associated with pulmonary hemorrhage, was identified on histopathology. Assigning EIPH as the cause of death in these horses was based in part on ruling out competing causes of death. There was no evidence of competing causes of death in any of these horses. In addition, the degree of pulmonary hemorrhage was thought to be sufficient in volume and extent (20–75% of the pulmonary parenchyma) to significantly impair alveolar gas exchange, making EIPH the cause of death, to a reasonable degree of medical certainty. The fact that there remains uncertainty in such cases reflects the current state of the art in diagnostic pathology when dealing with a pathophysiologic mechanism that is poorly understood.
Of the 21 cases of sudden death in our study, gross or histologic abnormalities were present in 9 (43% of the cases). This finding was similar to that of a much larger previous multicenter study in which pathologists were able to identify a definitive cause of death in 53% of cases. 5
The findings of the NYSGC-CU postmortem examination program have been used at NYRA racetracks to create a paradigm shift among horsepersons from the long-held belief that “a bad step” is the inevitable cause of FMSI to a realization that FMSI is a multi-factorial event that involves both risk and protective factors, many of which are “modifiable.” The significant sustained decrease in the number of racing fatalities at NYRA racetracks following the implementation of a comprehensive safety program based in part on postmortem examination findings provides strong evidence that racing fatalities are subject to intervention.
An analysis of the 16% decrease in the 2014–2015 national racing fatality rate in North America was able to account for only 35% of the 16% decrease by modification of specific numerical risk factors, such as increasing the number of horses racing at 2 y of age and decreasing the relative number of sprint claiming races at a distance of ≤7 furlongs (Parkin TDH. Equine Injury Database—Can we explain the significant drop in risk in 2015? Welfare & Safety of the Racehorse Summit VII. 2016; https://goo.gl/yrVCcq). It is likely that some portion of the reduction of FMSI can be accounted for by the introduction of protective factors. For example, amendment of claiming rules to permit voiding of claims in the event of a FMSI or severe lameness immediately following a race increases the responsibility of horse trainers for equine safety and welfare. Without such rules in place, the responsibility of the trainer for the welfare of a horse in a claiming race ends when the starting gate opens. Because a number of the recommendations of the New York Task Force on Racehorse Health and Safety were put in place in conjunction with the NYSGC-CU postmortem examination program and the mortality review process, it is not possible to attribute total success to any one intervention. Nevertheless, integration of the postmortem examination findings into a multi-disciplinary mortality review process, used in conjunction with innovative regulations by the NYSGC, a continuing education program for horse trainers, and related research efforts, has contributed to the overall sustained reduction of racing fatalities between 2013 and 2015 at NYRA racetracks.
In order to investigate the possibility of regional differences in the postmortem examination findings among racing jurisdictions, we compared the NYRA postmortem examination findings from 2013–2015 with the Thoroughbred findings of the CAHFS Postmortem Examination Program annual reports for the fiscal years 2012–2013, 2013–2014, and 2014–2015 (Table 6). The average number of Thoroughbred submissions per month for NYRA racetracks was 13.3, whereas that of California racetracks was 41.5. The reason for this discrepancy can be explained in part by the fact that during this period California Thoroughbred racetracks averaged 29,651 starts per year whereas NYRA racetracks averaged 27,397 starts per year. Additionally, the Thoroughbred data reported in the CHRB Annual Reports during this period included submissions from all California Thoroughbred racetracks, whereas this review included only submissions from New York racetracks operated by NYRA. Submissions from Finger Lakes racetrack in New York were not included in this study given a lack of consistency of data collection and mortality review procedures at that racetrack during this period of study. Finally, the number of submissions in the first year of the NYSGC-CU postmortem examination program was approximately half of the number of submissions in the subsequent 2 y given organizational and logistical challenges faced by participating NYRA racetracks as well as organizational challenges associated with creating a novel and evolving collaborative program between the NYSGC and Cornell University to perform the postmortem examinations during the first year of the program. There was also some degree of variation in the mean number of month-to-month submissions at both New York and California racetracks during this 3-y period. This may be explained by seasonal variation in the horse populations, the number of races run, and the number of horses in active training at multiple tracks at the same time during peak racing periods.
Comparison of the frequency of Thoroughbred musculoskeletal injuries as a percent of total submissions from California Thoroughbred and New York Racing Association racetracks (2013–2015).*
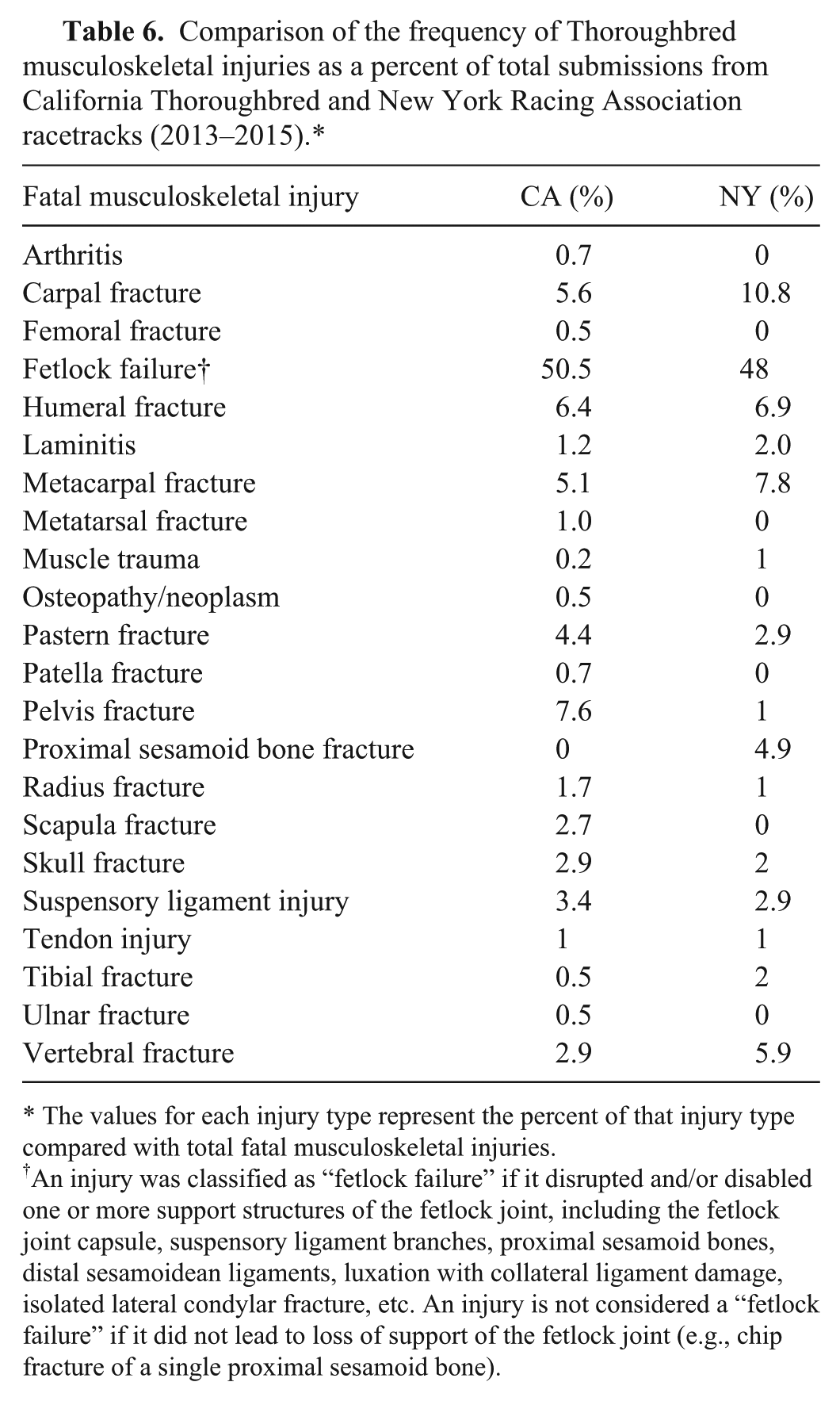
The values for each injury type represent the percent of that injury type compared with total fatal musculoskeletal injuries.
An injury was classified as “fetlock failure” if it disrupted and/or disabled one or more support structures of the fetlock joint, including the fetlock joint capsule, suspensory ligament branches, proximal sesamoid bones, distal sesamoidean ligaments, luxation with collateral ligament damage, isolated lateral condylar fracture, etc. An injury is not considered a “fetlock failure” if it did not lead to loss of support of the fetlock joint (e.g., chip fracture of a single proximal sesamoid bone).
All Thoroughbred races in New York are conducted on either dirt or turf surfaces. No NYRA races were conducted on synthetic surfaces during the period of study. NYRA submissions for autopsy examinations in 2013–2015 included 80 FMSI that occurred while horses were exercising on dirt surfaces and 22 FMSI that occurred while horses were exercising on turf. The relative proportion of FMSI on dirt and turf surfaces was similar between NYRA and California racetracks (Table 7). Data obtained from The Jockey Club Equine Injury Database during the 2013–2015 period, indicated that the North American fatality rate on turf was 1.44 per 1,000 starts whereas that on dirt was 1.98 per 1,000 starts. This information, combined with the fact that during this 3-y period there were 689,131 Thoroughbred races run on dirt surfaces in North America and only 157,387 Thoroughbred races run on turf, helps to explain the relative difference in the number of fatalities reported for each surface in our review.
Distribution of musculoskeletal fatalities in Thoroughbred racehorses at California and New York Racing Association (NYRA) racetracks for 2013–2015 by racing surface.*
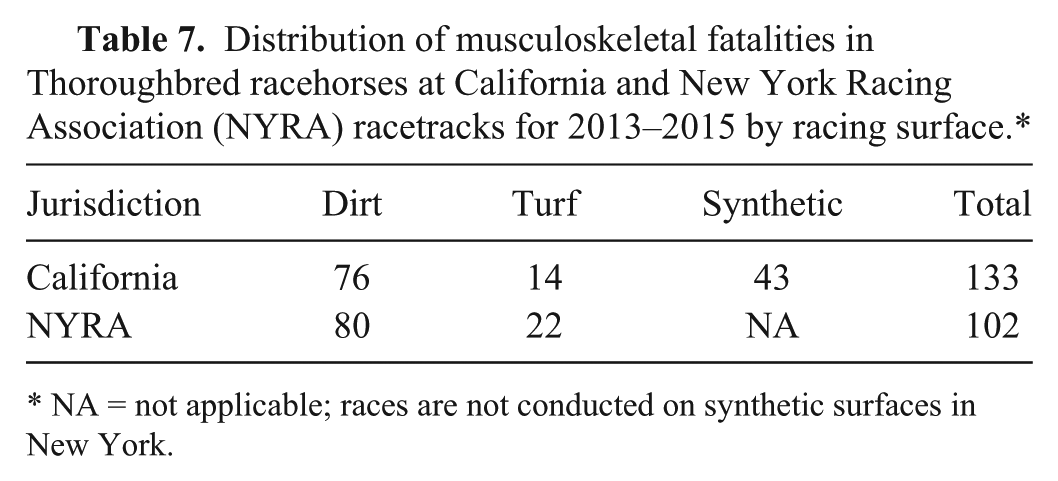
NA = not applicable; races are not conducted on synthetic surfaces in New York.
The age of horses submitted for postmortem examination was slightly different between NYRA and California racetracks. At California racetracks, 3- and 4-y-old horses made up 57% of total submissions, whereas at NYRA racetracks, 3- and 4-y-old horses comprised 53% of the total submissions. At NYRA racetracks, the range of 3-, 4-, and 5-y-old horses accounted for 71% of submissions, whereas the same age group at California racetracks accounted for 59% of submissions. It is likely that these numbers reflect the relative number of available starters and race conditions offered in the respective jurisdictions.
The sex distribution of horses submitted for postmortem examinations from NYRA and California racetracks were similar. Females comprised 39% of submissions from NYRA racetracks and 41% of submissions from California racetracks. Males comprised 62% of submissions from NYRA racetracks and 59% of submissions from California racetracks. However, intact males represented 32% of submissions from NYRA racetracks and 20% of submissions from California racetracks; geldings comprised 29% of submissions from NYRA racetracks and 39% of submissions from California racetracks. Intact male horses have been found to be at increased risk for fatal musculoskeletal injury. 1 At both NYRA and California racetracks, the number of female submissions was greater than the number of intact male submissions. However, comparative data were not available to account for the actual numbers of intact males and females racing in either jurisdiction during this period.
There were some variations in the activity during which the fatalities occurred between NYRA and California racetracks. At NYRA racetracks, racing fatalities represented 60% of total fatalities, training fatalities represented 33% of total fatalities, and non-exercise fatalities represented 8% of total fatalities. At California racetracks racing fatalities represented 40% of total fatalities, training fatalities represented 34% of total fatalities, and non-exercise fatalities represented 26% of total fatalities. The majority of racetrack equine fatalities occurred during exercise in both jurisdictions, with the raw number of racing fatalities being higher than the number of training fatalities during this period.
The location of appendicular fractures was also similar between NYRA and California racetracks. In both jurisdictions, there was little difference between contralateral fore- and hindlimbs (LF-RF and LH-RH), but forelimb fractures were much more common than hindlimb fractures in both jurisdictions. There also was a great deal of similarity in the distribution of types of FMSI between California and New York. Injuries were classified as “fetlock failure” if one or more support structures of the fetlock joint were disrupted or disabled. Although “fetlock failure” accounted for the highest percentage of fatal musculoskeletal injuries at both NYRA (48%) and California (50.5%) racetracks, the percent of carpal fractures at NYRA racetracks (10.8% of FMSI) was nearly twice that at California racetracks (5.6% of FMSI). The percent of pelvic fractures at California racetracks (7.6% of FMSI) was more than 7 times that of NYRA racetracks (1% of FMSI). Finally, the percent of proximal sesamoid bone fractures at NYRA racetracks (4.9% of FMSI) was more than 5 times that of California racetracks (0% of FMSI). The reason for these differences cannot be answered with the data provided herein, but with a significant portion of the California races contested on synthetic surfaces during this period (no synthetic surfaces are present at NYRA racetracks), further investigation of this observation has merit.
Given the fact that there are regional differences among racing jurisdictions in terms of weather and environmental conditions, track design, composition and maintenance procedures, as well as scheduling, horse populations, and other factors, it is reasonable to expect that there may be some regional variation in racing injuries. This was the case in this 2013–2015 review of NYRA and California FMSI. However, with few exceptions, the high degree of correlation of the pathologic findings in both the NYRA and California reports for 2013–2015 suggests that similar patterns of injury and pre-existing bone lesions are likely to be present in other racing jurisdictions in North America and that similar interventions such as a mortality review program that brings evidence-based recommendations to horse trainers and other racing stakeholders may help to reduce equine fatal musculoskeletal injury in those jurisdictions as well.
An opportunity exists for the collaboration of multiple racing jurisdictions to institute similar postmortem examination programs teamed with mortality review boards. This will standardize the collection of data and increase the power of the individual anatomic pathology databases as well as increase the number of racing stakeholders impacted by the process of increased accountability. Additionally, multiple academic institutions can contribute to the continuing education of veterinarians and trainers at the racetrack to increase the knowledge base in order to help stakeholders make evidence-based decisions regarding the care and training of racehorses. Finally, collaborative research efforts will be more efficient in setting priorities and addressing the most critical factors that contribute to racing injuries.
Footnotes
Acknowledgements
We thank the veterinary pathologists and staff of the Cornell University Department of Biomedical Sciences, and faculty in the Department of Population Medicine and Diagnostic Sciences and the Animal Health Diagnostic Center; members of the New York Equine Safety Review Board (Dr. Anthony Verderosa, NYRA Chief Examining Veterinarian and his staff; Mr. Glen Kozak, Vice President of Facilities and Racing Surfaces; and Mr. Hugh Gallagher, NYRA Safety Steward), and The Jockey Club–InCompass solutions software.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Provided by the Henry M. Zweig Memorial Equine Research Fund.