
Abstract
The delta total nucleated cells (ΔTNC) measurement with the Sysmex XT-2000iV (Sysmex Europe, Norderstedt, Germany) has high diagnostic accuracy on effusions in feline infectious peritonitis (FIP) cases, but the test can be performed only on fresh samples. We evaluated whether supernatants from effusions retain the ability to induce cell clumping and assessed the diagnostic accuracy of this modified ΔTNC method. Effusions were collected from FIP cats (n = 19) and from cats with other diseases (n = 15). ΔTNC was measured on fresh samples and on frozen–thawed supernatants after the addition of feline blood at 1:10 dilution. Diagnostic accuracy was assessed at the cutoffs of suggestive of FIP (ΔTNC = 1.7) and consistent with FIP (ΔTNC = 3.4). The influence of the protein content, number of added cells, and magnitude of dilution were also investigated. Specificity and positive predictive value were 100% for both the methods. Sensitivity and negative predictive value were higher for the modified ΔTNC (84.2% and 83.3%, respectively, at the cutoff of 1.7; 78.9% and 78.9%, respectively, at the cutoff of 3.4) than for the ΔTNC on fresh samples (78.6% and 81.3%, respectively, at the cutoff of 1.7; 57.1% and 68.4%, respectively, at the cutoff of 3.4). Protein content, total cell count of the added blood, and magnitude of dilutions did not influence the results. Supernatants of frozen effusions from FIP cats retain the ability to induce cell clumping, thus the modified ΔTNC measurement is a reliable tool to diagnose FIP on samples that cannot be analyzed immediately.
Feline infectious peritonitis (FIP) is a disease of felids caused by a mutated feline coronavirus and by an inadequate immune response of infected cats. 10 Diagnosing FIP in vivo can be challenging, especially in dry forms, because of the lack of confirmatory tests. 8 Serum protein electrophoresis and α1-acid glycoprotein may be useful,7,9 as well as, in wet forms, macroscopic and cytologic analyses of the effusions, 12 which show a high protein content with a low albumin:globulin ratio.1,6 The measurement in effusions of the delta total nucleated cells (ΔTNC) with the Sysmex XT-2000iV has been shown to have high accuracy for diagnosing FIP.6,11
The Sysmex XT-2000iV is a laser-based analyzer widely employed in veterinary laboratories, which counts leukocytes in the WBC-DIFF channel (where cell populations are differentiated based on nucleic acid content and cytoplasmic complexity) and in the WBC-BASO channel (where an acidic reagent causes shrinkage of all nucleated cells). 14 The delta WBC (ΔWBC, the ratio between the WBC-DIFF and WBC-BASO counts) is close to 1.0 in samples from healthy animals. 3
In FIP effusions, given the presence of high molecular weight proteins, the acidic reagent of the WBC-BASO channel induces the formation of clumps, which entrap cells as it occurs in the Rivalta test.4,5,13 Consequently, the WBC-BASO count is low, and the ΔTNC count, which corresponds to the ΔWBC in effusions that contain nucleated cells other than leukocytes, is high. ΔTNC >1.7 is suggestive of FIP; values >3.4 are diagnostic for FIP. 6 However, ΔTNC can be measured only on fresh samples, because storage may alter cellular structure, leading to inaccurate cell counts and consequently inaccurate ΔTNC values. Therefore, effusions with a low WBC-DIFF count may be falsely negative, despite high protein content.
Our hypothesis was that, when blood cells are added to frozen–thawed FIP supernatants, the WBC-BASO channel will give very low counts because of clumping of cells induced by high molecular weight proteins, whereas the WBC-DIFF count reflects the actual number of cells, leading to a high ΔTNC. We evaluated whether cell-free supernatants from FIP effusions retain the ability to clump cells after the addition of cells obtained from blood samples, and assessed the diagnostic value of this modified method for evaluating the ΔTNC.
We analyzed 34 effusions from cats with FIP (n = 19) or other diseases (n = 15). The samples had been collected for diagnostic purposes by referring veterinarians according to standard veterinary procedures. Therefore, according to the regulations of our institution, a formal approval of the Institutional Ethical Committee was not required.
The diagnosis of FIP was based on postmortem findings in 18 of 19 FIP cats and on histology of biopsy samples in 1 of 19 cats. FIP was excluded based on postmortem findings in 5 of 15 cats without FIP. These 5 cats had pleuropericardial chronic fibrosis (cat 20), pleural undifferentiated pleomorphic sarcoma (cat 21), abdominal hemangiosarcoma (cat 24), undifferentiated liver neoplasia (cat 27), and acute leukemia (cat 33). In 4 of 15 cats without FIP, a diagnosis of neoplasia was obtained through cytology (cats 22 and 23) and confirmed through histology (cats 30 and 34). In the remaining 6 of 15 cats without FIP, the following diagnoses were obtained in vivo: cats 25 and 29 were diagnosed with cardiomyopathy, and cat 32 with pancreatitis; all responded appropriately to treatment; cats 26, 28, and 31 were diagnosed with chylothorax through cytology and diagnostic imaging.
Twenty-seven samples were collected in EDTA tubes and analyzed within 12–18 h. First, the ΔTNC was measured, then the effusions were centrifuged (3,000 × g, 5 min); the supernatants were transferred to other tubes and frozen at −20°C (~1−8 wk). Seven samples (1, 10, 16, 18, 19, 28, 29) were centrifuged by the referring veterinarians, and the supernatants were sent to our laboratory where the supernatants were immediately frozen.
In order to evaluate its ability to induce cell clumping, 20 μL of fresh feline blood (ΔWBC of 1.00 ± 0.15; mean ± standard deviation), obtained from the routine caseload of our laboratory, were added to 180 μL of thawed supernatants to obtain a dilution of 1:10. Specifically, 15 different blood samples were used (WBC counts: 5.11−154 × 109 WBC/L). Each blood sample was used to spike 1–4 effusions (Table 1). After gentle mixing, the samples were analyzed with the Sysmex XT-2000iV. a WBC-DIFF and WBC-BASO counts and ΔTNC were recorded. The samples were classified as positive or negative using a ΔTNC of 1.7 and a ΔTNC of 3.4 as cutoff thresholds. Using both the cutoffs and based on the final diagnosis (FIP vs. non-FIP), the numbers of true-positive, true-negative, false-positive, or false-negative results were counted. Specificity, sensitivity, positive predictive value (PPV), and negative predictive value (NPV), were then calculated. 2
White blood cell (WBC) counts of the 15 blood samples added to the effusions of the 34 cats included in the current study.
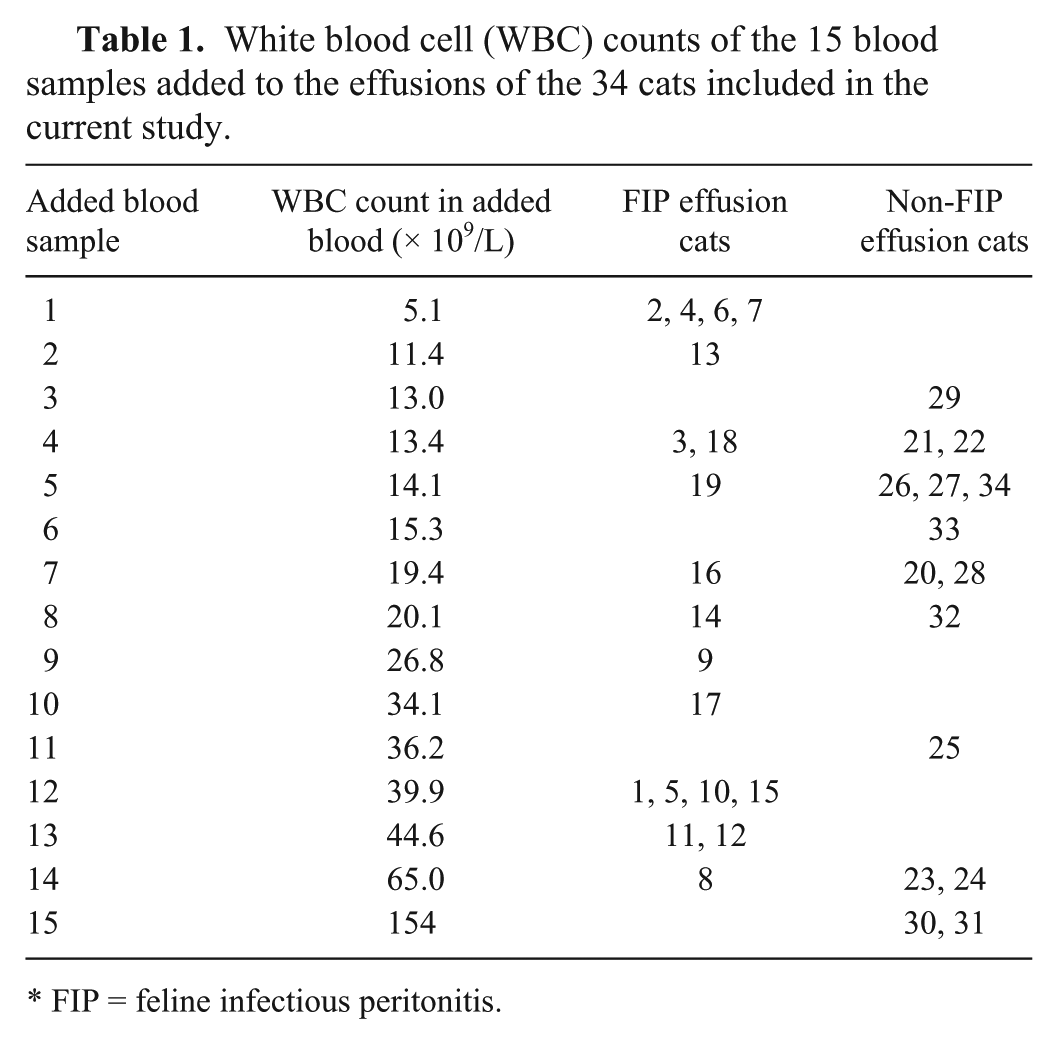
FIP = feline infectious peritonitis.
Except for 1 case, in which the WBC-DIFF count recorded in the effusions added with blood was 24.6% compared with the WBC count in blood, the WBC-DIFF in the effusion was close to 10% compared with blood, as expected using the 1:10 dilution (10.9 ± 1.2 in the whole caseload; 11.1 ± 1.2 in FIP effusions; 10.8 ± 1.2 in non-FIP effusions). Thus, the addition of blood did not generate a matrix effect that interfered with the cell counts. In 12 of 27 cases that were analyzed with both methods (cats 2–4, 6, 7, 13, 15, 17, 21, 31, 32, 34), the modified ΔTNC was lower than the original (Fig. 1). In 8 of these cases, the WBC-DIFF count was lower than in the case of the fresh sample. Conversely, in 6 of 27 cases (cats 5, 9, 11, 12, 14, 26), the modified ΔTNC was higher than the original, and in 3 of these cases the WBC-DIFF count was higher than that of the fresh sample. In 9 of 27 cases (cats 8, 20, 22–25, 27, 30, 33), 8 of which belonged to the non-FIP group, the modified ΔTNC remained unchanged compared with the original ΔTNC (<10% variation compared with the original ΔTNC), despite the WBC-DIFF count being higher in 6 of these cases than in the fresh sample. Therefore, the modified method induced variations of the ΔTNC in approximately two-thirds of samples (16 of 27 cases).
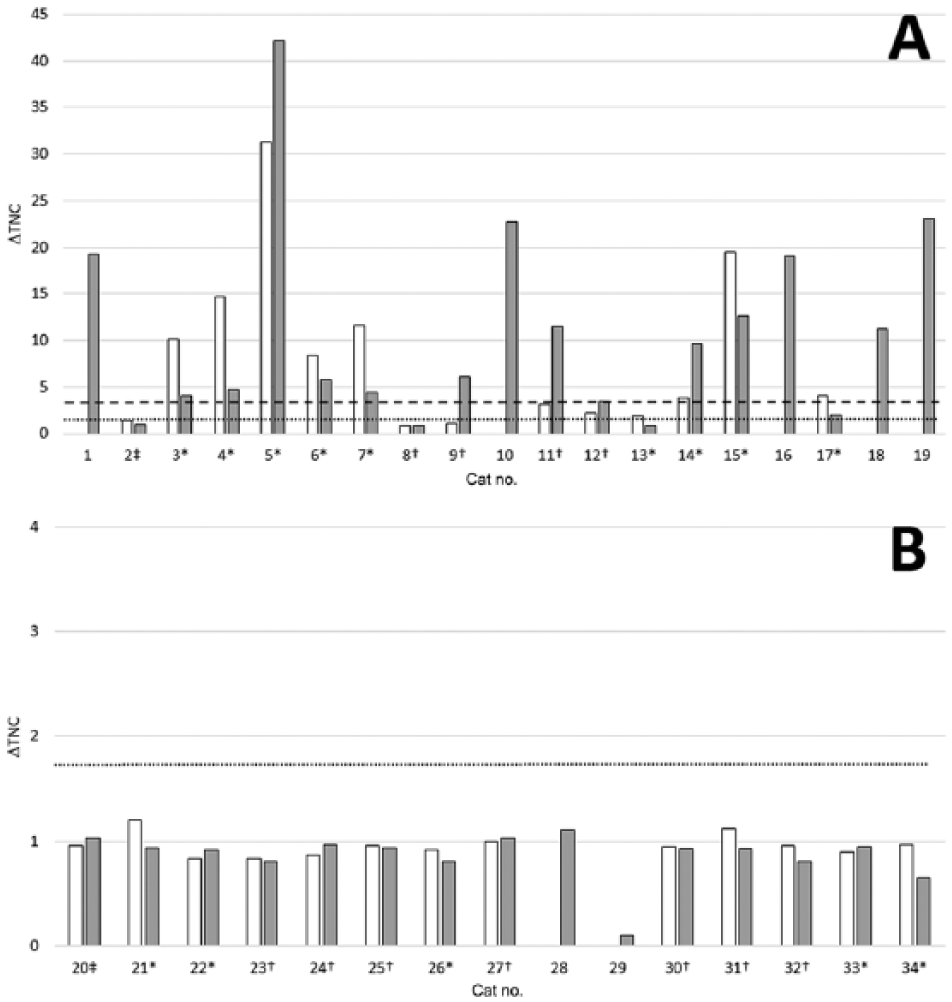
Results of the delta total nucleated cells (ΔTNC) on fresh effusions with the original method (white bars) and on frozen–thawed supernatants using the modified method (gray bars) in cats with feline infectious peritonitis (FIP;
Results obtained with the 2 methods were compared using a Wilcoxon signed rank test, and no significant differences were recorded, suggesting that frozen supernatants provide results similar to fresh samples (Fig. 2). Moreover, the increase or decrease of the ΔTNC does not seem to be proportional to the values of the WBC-DIFF counts recorded after mixing blood with supernatants; in approximately one-third of samples, the ΔTNC did not change, despite a marked difference between the WBC-DIFF count of fresh samples and the WBC-DIFF count recorded after mixing blood with the supernatants. This suggests that the final WBC-DIFF count obtained after dilution does not directly influence the ΔTNC. The design of our study does not allow determination of the number of WBCs needed in a feline blood sample to optimize the test. However, the fact that effusions sampled with the same blood sample often had different ΔTNC (e.g., as shown in Table 1 and Fig. 1 in the 4 samples with 13.4 × 109 WBC/L added, corresponding to ~1.3 × 109 WBC/L after 1:10 dilution, the ΔTNC were 0.92 and 0.94 in the non-FIP effusions and 4.10 and 11.30 in the FIP effusions), supports the hypothesis that the ΔTNC is influenced by the type of effusion rather than by the cell count of the added blood. However, it is possible that blood samples with leukopenia, not included in our study, lead to a WBC-DIFF count in the effusion so low as to hamper the possibility of having, in FIP cats, a ΔTNC sufficiently high to support a clinical diagnosis of FIP. Hence, the use of leukopenic blood samples to spike frozen effusions cannot be recommended based on our results.
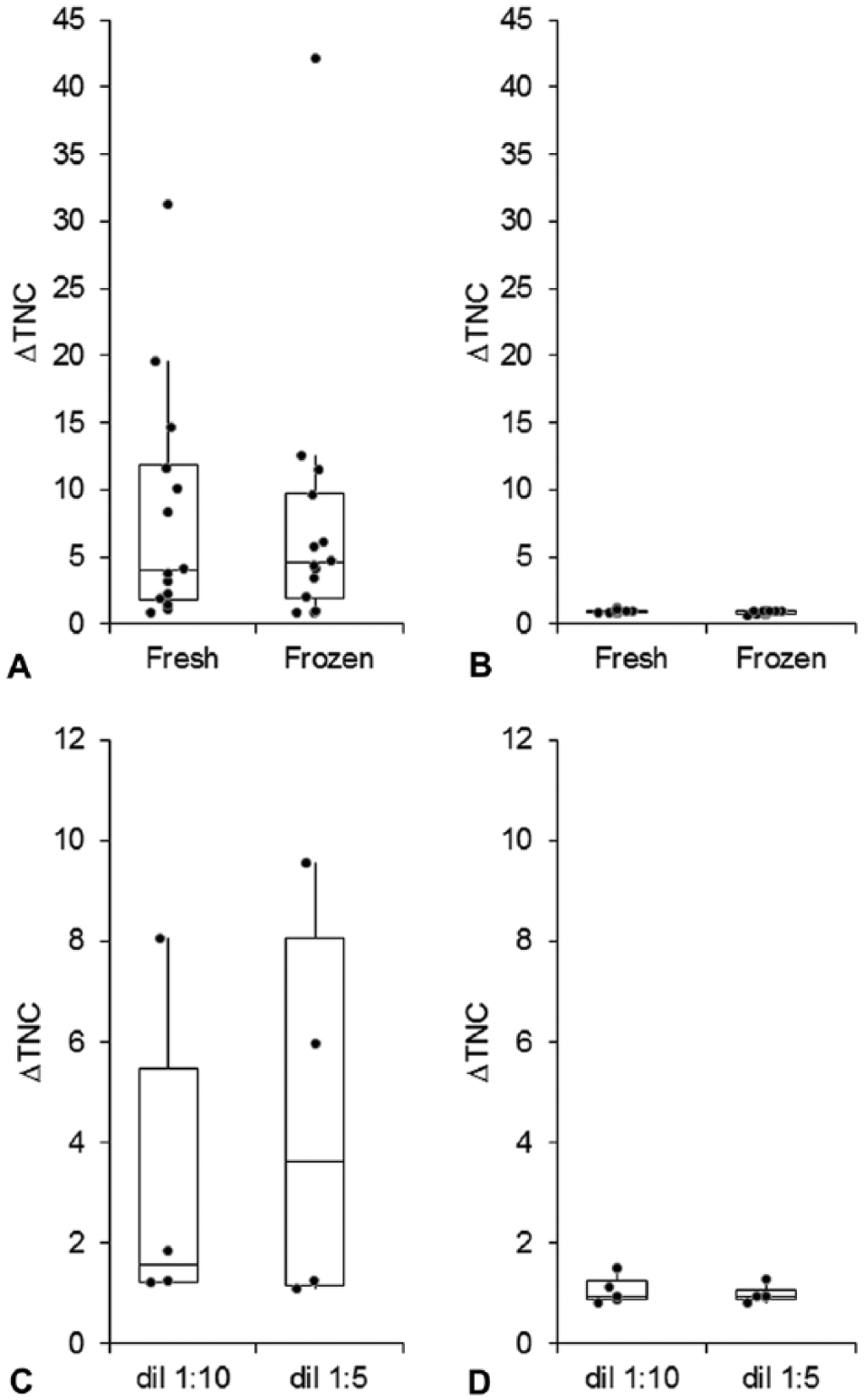
Comparison of results obtained from fresh effusions processed with the original method (
In order to assess the effect of dilution, 9 samples (4 from cats with FIP and 5 from cats without FIP) were tested using 2 dilutions of blood: 1:10 as described above, and 1:5 (i.e., 40 μL of blood in 160 μL of supernatant). Also in this case, no significant differences were found with the 2 dilutions either in the FIP group or in the non-FIP group, and the classification of samples as consistent or not consistent with FIP did not change at the 1:5 dilution compared with the 1:10 dilution. The 4 FIP effusions were also analyzed using a 1:2 dilution (100 µL of blood in 100 µL of supernatant) and, even though no significant differences or changes in the classification of samples were found in this comparison, the ΔTNC decreased in all 4 cases (data not shown). These data suggest that when the supernatant:blood ratio is low, the amount of fibrin (and other inflammatory proteins) is too low to induce cell clumping given the dilution of proteins responsible for WBC clumping. Therefore, these additional experiments demonstrated that the 1:5 and 1:10 dilution provide similar results, and, in our opinion, the 1:10 dilution should be preferred to facilitate the calculation of volumes.
In order to understand if the protein content of the effusion may affect the results, the concentration of total proteins in supernatants was determined using the biuret method on an automated spectrophotometer. b The total protein of the effusion did not influence the ΔTNC value with either the original or the modified method. Samples with low or high protein content had comparable ΔTNC values either in FIP cats or in cats without FIP (data not shown), suggesting that it is not the overall amount of protein that is responsible for the increased ΔTNC, but rather the presence of a particular protein pattern.
Using the 1:10 dilution, independently of the differences in ΔTNC values between fresh and frozen–thawed samples, all the effusions from cats without FIP had a ΔTNC <1.7 using both methods. Conversely, on fresh effusions from cats with FIP, 4 of 14 samples (cats 2, 8, 9, 17) had a ΔTNC <1.7, 3 of 14 samples (cats 11–13) had a ΔTNC of 1.7–3.4, and 7 of 14 samples (cats 3–7, 14, 15) had a ΔTNC consistent with FIP (>3.4). Using the modified technique, 2 of 4 “false-negatives” (ΔTNC <1.7; cats 2, 8) remained falsely negative, 1 of 4 (cat 17) increased to values suggestive of FIP (ΔTNC of 1.7–3.4), and 1 of 4 (cat 9) resulted as positive (ΔTNC >3.4). Only 1 true-positive sample based on the fresh sample (cat 13; which, however, had a ΔTNC of 1.89, close to the lowest cutoff of 1.7) resulted as a false-negative (ΔTNC <1.7) using the modified technique. The 2 other samples that on fresh effusions had a ΔTNC of 1.7–3.4 (cats 11, 12) resulted as positive (ΔTNC >3.4) using the modified technique. Therefore, in cats with FIP, using the modified technique, 3 of 19 samples (cats 2, 8, 13) had a ΔTNC <1.7, 1 of 19 (cat 17) has a ΔTNC of 1.7–3.4, and all the other samples had a ΔTNC >3.4.
Hence, both methods, independently of the cutoff, show absolute specificity and PPV (100.0%). The sensitivity and NPV of the modified method (84.2% and 83.3% at the cutoff of 1.7; 78.9% and 78.9% at the cutoff of 3.4) were higher than that of the original method (78.6% and 81.3% at the cutoff of 1.7; 57.1% and 68.4% at the cutoff of 3.4). Thus, the diagnostic interpretation of ΔTNC using the cutoffs that, in the previous study, 6 were considered suggestive of FIP (ΔTNC >1.7) or consistent with FIP (ΔTNC >3.4) indicates that the modified method minimally affects the classification of samples as “FIP” or “non-FIP,” independently of the ΔTNC value obtained from fresh samples.
Three samples from cats with FIP had a low ΔTNC count either with the original method or with the modified technique (in one case the ΔTNC remained low also when blood with higher WBC-DIFF counts was added). This was already noted in the previous study, 7 and suggests that this “false negativity” depends on intrinsic properties of the effusions, not investigated in this study (i.e., low concentration of high-molecular-weight proteins), which do not allow the formation of cell clumps. Therefore, if the ΔTNC is negative using both methods, FIP must be confirmed using tests other than the ΔTNC.
The results of our study demonstrated that the modified ΔTNC is an alternative, reliable tool to diagnose effusive FIP in those cases where cytology of the effusion or other biochemical tests on the supernatants cannot be performed immediately after sampling. This method can be performed on frozen supernatants, thus allowing retrospective analyses of stored fluids. Supernatants from FIP effusions, likely because of their protein pattern, retain the ability to clump cells derived from blood samples, whereas the non-FIP effusions do not. Therefore, it may be best to centrifuge effusions that cannot be analyzed immediately, and to remove and send the supernatant to the laboratory. Future studies focused on determining the minimum number of WBCs needed to obtain a positive result may further improve the performance of this alternative method.
Footnotes
Authors’ contributions
A Stranieri contributed to conception and design of the study, and drafted the manuscript. S Paltrinieri and A Giordano contributed to design of the study. All authors contributed to acquisition, analysis, and interpretation of data; critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
a.
Sysmex Europe, Norderstedt, Germany.
b.
Cobas Mira, Roche, Basel, Switzerland.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.