
Abstract
A 2-year-old female Yorkshire Terrier dog presented with neurological deficits. Magnetic resonance imaging revealed an 8 mm in diameter mass centered left of midline arising from the quadrigeminal cistern, with a fatty or proteinaceous content. A further fat signal intensity focus was present in the tip of the temporal horn of the right lateral ventricle, in keeping with a “floating” fat embolus within the cerebrospinal fluid. A ruptured dermoid cyst was diagnosed. Within the frontal lobe on both sides were ill-defined and extensive high T2 signal areas, with mass effect within the white matter, and asymmetrical contrast enhancement following intravenous injection of gadolinium. Postmortem gross and histological examination confirmed the mass in the quadrigeminal cistern to be a dermoid cyst. In addition, severe multifocal necrotizing granulomatous leukoencephalomyelitis was found in the corona radiata and spinal cord. The relationship between these 2 pathologies is discussed.
A 2-year-old female Yorkshire Terrier dog was presented with acute onset weakness in all 4 limbs. Clinical examination revealed the animal was bright and alert but unable to stand. Neurological examination revealed reduced proprioception in the hindlimbs and no proprioception or weight-bearing reflexes in the forelimbs.
Magnetic resonance imaging (MRI) revealed an 8 mm in diameter mass centered left of midline arising from the quadrigeminal cistern (Fig. 1a). The mass was of moderately high T1 signal, which is indicative of fatty or proteinaceous content, and was displaced to the left by a cerebrospinal fluid (CSF) signal intensity structure, probably an encysted mesencephalic aqueduct. Associated with the mass were 2 very high T1 signal intensity nodules with chemical shift artifact on T2, indicating lipid. A further fat signal intensity focus was present in the tip of the temporal horn of the right lateral ventricle, in keeping with a “floating” fat embolus within the CSF (Fig. 1b, 1c). The findings were considered diagnostic of a ruptured dermoid cyst. There was marked ventricular hydrocephalus with moderate third ventricular enlargement, with preserved cerebral sulci. Within the frontal lobe on both sides were ill-defined and extensive high T2 signal areas, with mass effect within the white matter (Fig. 1d), and asymmetrical contrast enhancement following intravenous injection of gadolinium.
Due to the poor prognosis, the owners elected euthanasia and a postmortem examination was carried out. The brain and spinal cord appeared unremarkable when intact; however, when sectioned, a 1 cm in diameter spherical cystic structure containing abundant hair, soft, brown material (sebum), and white flakes resembling keratin was found in the quadrigeminal cistern. The structure displaced the rostral colliculus in a rostrodorsal direction (Fig. 2a). In addition, bilateral, poorly delineated, focal areas of the internal capsule white matter were soft and discolored brown (Fig. 2b).
Microscopic analysis of the cyst in the quadrigeminal cistern revealed that it was lined by 1–3 layers of well-differentiated keratinized squamous epithelial cells (Fig. 3). The lumen of the cyst contained numerous cross sections of hair follicles, abundant eosinophilic, amorphous, fragmentary material (keratin), and a small amount of proteinaceous fluid admixed with inflammatory cells (neutrophils and fewer lymphocytes). External to the epithelial cells was a layer of tissue resembling dermis, which contained hair follicles, sebaceous glands, mildly ectatic apocrine glands, adipose tissue, and moderate numbers of lymphocytes. There was moderate perivascular cuffing (lymphocytes and macrophages) and gliosis of the neuropil adjacent to the cyst. The histological findings were consistent with a diagnosis of dermoid cyst.
Within the left and right cerebral hemispheres, there was a bilateral regionally extensive area of severe granulomatous inflammation and malacia of the white matter of the corona radiata and the dorsal margin of the internal capsule. The inflammation was characterized by marked perivascular cuffs of macrophages and lymphocytes, and infiltration of lymphocytes, macrophages, gitter cells, and occasional gemistocytic astrocytes within the white matter (Fig. 4). There were numerous swollen and fragmented axons (spheroids) and vacuoles (axonal drop out). No lesions were noted in the gray matter of the cerebral cortex, and no lesions were noted in the cerebellum or the brain stem. Sections of spinal cord at C2, T2, and L2 were examined. At the level of the second cervical vertebrae, there was severe, regionally extensive inflammation and degeneration of the white matter in the dorsal funiculus, with prominent perivascular cuffs, diffuse macrophages, gitter cells, spheroids, and empty axonal sheaths. Lymphocytes, plasma cells, and macrophages were the main inflammatory cells present in the perivascular cuffs. At the level of the second thoracic vertebrae, the changes in the spinal cord were similar but more extensive, being present in both dorsal and ventral funiculi. A section of spinal cord from the lumbar region was unremarkable. Gram, Ziehl–Neelsen, and Grocott stains of the brain and spinal cord did not reveal any microorganisms.
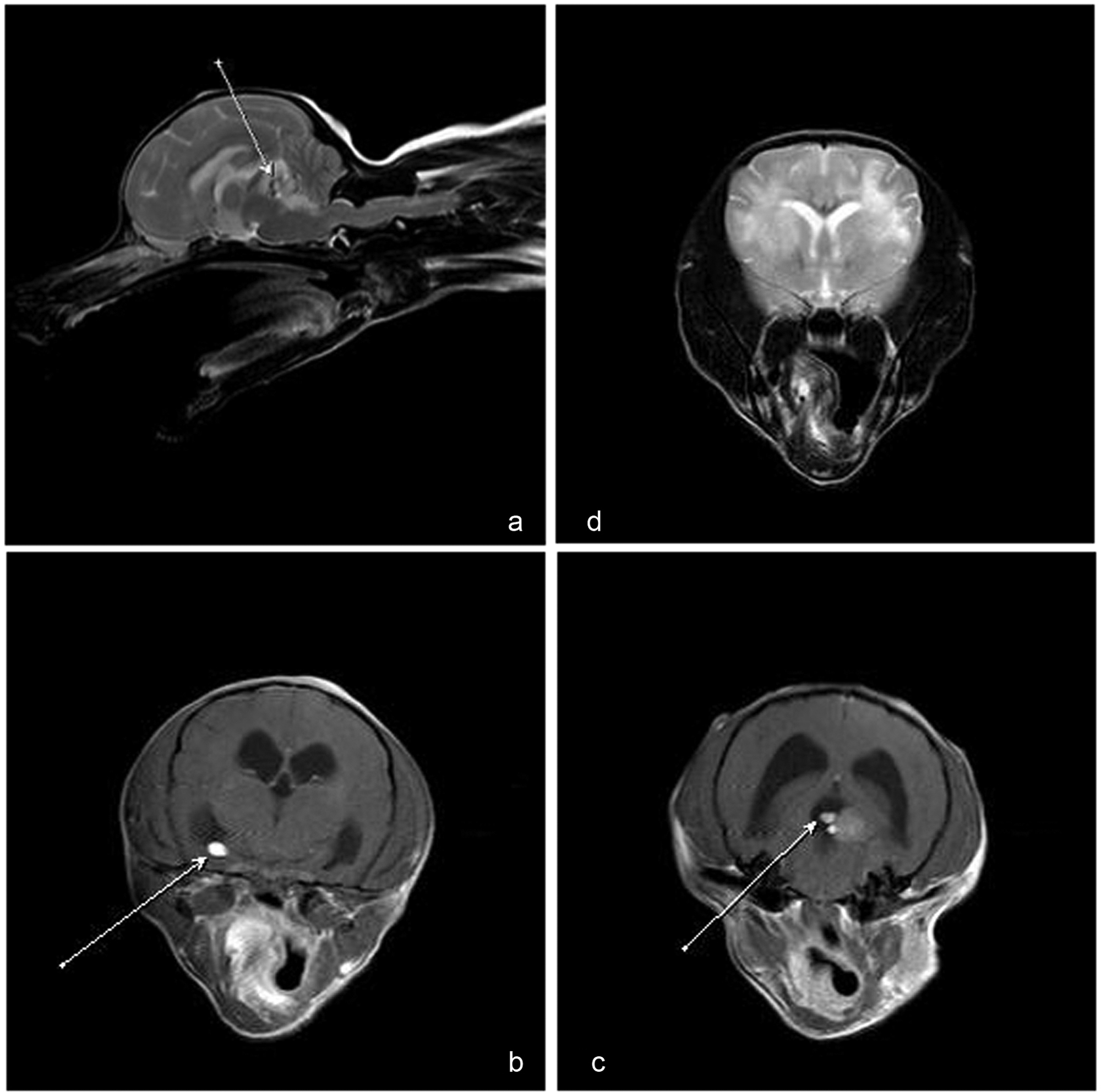
Magnetic resonance imaging; Yorkshire Terrier dog.

Yorkshire Terrier dog.
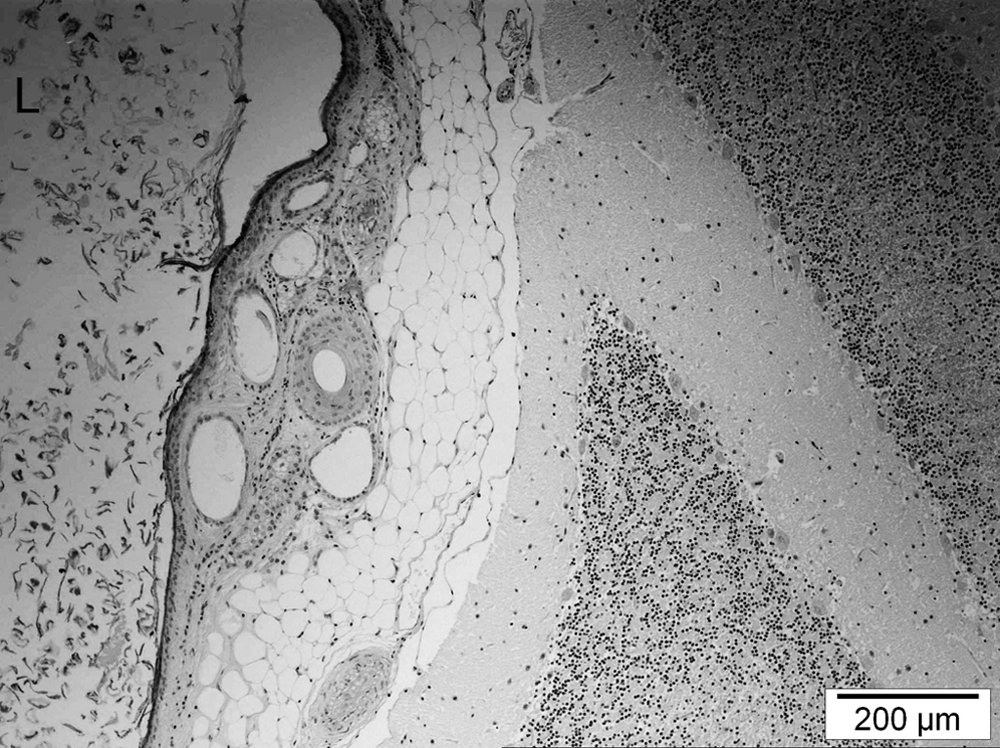
Yorkshire Terrier dog. Histological image of cerebellum (right) abutting the wall of the dermoid cyst (left). The lumen (L) of the dermoid cyst contained keratin flakes. Bar = 200 µm.
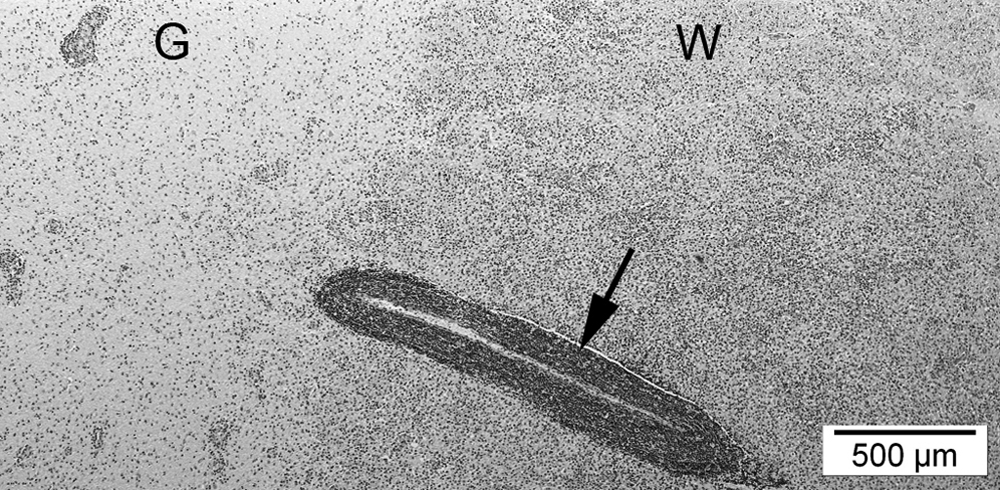
Yorkshire Terrier dog. Histological image at the junction of white (W) and gray (G) matter in the brain, demonstrating the granulomatous leukoencephalitis with prominent perivascular cuffing (arrow). Bar = 500 µm.
In summary, 2 pathologies were found in the central nervous system of the dog in the current study: 1) a dermoid cyst within the quadrigeminal cistern and 2) severe multifocal necrotizing granulomatous leukoencephalomyelitis. Dermoid cysts are benign developmental lesions caused by a defect in epidermal closure, which leaves islands of multipotent ectoderm in abnormal locations such as within the central nervous system. 3 The cysts are usually found along the midline and may communicate with the skin surface via a sinus pore (this was not a feature of the dermoid cyst reported herein). Dermoid cysts may be asymptomatic unless they enlarge sufficiently to cause local compressive effects or rupture and release keratin and cholesterol breakdown products resulting in chemical meningitis or ventriculitis and occasionally cerebral vasospasm and ischemia.1,8 Despite this list of sequelae, numerous cases of ruptured intracranial dermoid cysts in human beings have been asymptomatic. 1 Dermoid sinuses and cysts are most common in Rhodesian Ridgeback dogs,7,10 although a dermoid sinus associated with malformed vertebrae T6 and T7 has been reported previously in a Yorkshire Terrier. 2
In the present case, the fat within the temporal horn of the lateral ventricle seen on MRI indicated rupture of the cyst. The severe, multifocal, granulomatous leukoencephalomyelitis was considered either a reaction to the rupture of the dermoid cyst or due to an unrelated pathological process. To the authors’ knowledge, rupture of a dermoid cyst has not previously been reported to cause granulomatous leukoencephalomyelitis. A dermoid cyst can cause granulomatous meningitis if ruptured into the arachnoid space or ependymitis of the ventricles, with infiltration of small inflammatory cells if ruptured into the ventricles. 5 Rupture has also been associated with cerebral vasospasm and transient cerebral ischemia, possibly due to the irritating effects of the lipid component of the dermoid cyst on the blood vessels. 1 In the case reported herein, features of meningitis, ventriculitis, or ischemia were not present, suggesting that the presence of the dermoid cyst contents in the ventricular system may have been asymptomatic. An unrelated pathological process was considered as the cause of the severe granulomatous inflammation; differential diagnoses included fungal or bacterial infections, granulomatous meningoencephalomyelitis (GME), necrotizing encephalitis of the Yorkshire Terrier (NEYT), 4 or necrotizing leukoencephalitis. 9 The negative findings of the Gram, Ziehl–Neelsen, and Grocott stains rendered fungal and bacterial infections unlikely, while the distribution of the inflammatory lesions in the rostral white matter of the brain and spinal cord are not characteristic of GME and NEYT. The histopathological features identified in the brain were most consistent with necrotizing leukoencephalitis, an idiopathic disease reported in various toy breeds of dog. 9
Whilst the concurrent ruptured dermoid cyst and multifocal necrotizing granulomatous leukoencephalomyelitis may have been coincidental in the dog in the current study, there has been a case report of an arachnoid cyst in the quadrigeminal space of a 2-year-old Yorkshire Terrier associated with necrotizing encephalitis, 6 raising the possibility that space-occupying lesions within the quadrigeminal space may predispose to a necrotizing inflammation of the central nervous system in toy breed dogs.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr. Donald Collie for his assistance with the interpretation of the MRI of this case.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.