
Abstract
A 6-month-old, intact, male Weimaraner dog presented to the veterinary teaching hospital for bilateral mucopurulent ocular and nasal discharge that began at approximately 10 weeks of age. A computed tomography scan showed an expansile soft-tissue mass involving both frontal sinuses, the ethmoid regions, and nasal cavities with lysis of the maxillary turbinates and hyperostosis of the walls of the frontal sinus. The dog was euthanized after complications during a trephination and biopsy procedure. At necropsy, a large, tan, papillary, gelatinous mass filled the entire nasal cavity and frontal sinus. The mass was composed of large fronds of loose fibrovascular stroma covered by a single layer of pseudostratified, columnar, ciliated epithelium and intermixed goblet cells. The cells occasionally formed glandular structures that were continuous with the surface epithelium. The mass was diagnosed as a respiratory epithelial adenomatoid hamartoma based on the morphologic appearance.
Hamartomas are defined as excess or abnormal growth of normal cells or tissue native to the organ in which they occur, likely as a result of aberrant differentiation. 8 Hamartomas may involve 1 or more cellular elements and are presumed to involve either errors during fetal growth or postnatal disturbance of immature tissue. 4 In animals, vascular, 8,9,11 rectal, 5 cranial nerve, 11 meningeal, 7 muscle, 8 melanocyte, 8 bile duct, 13 ovarian interstitial cell, 6 cutaneous adnexal, 8 mesenchymal, 2 pulmonary microcytic, 14 hypothalamic, 3 and fibroepithelial 12 hamartomas have been reported. However, no nasal or frontal sinus hamartomas have been reported in animals. In humans, the classification of nasal hamartomas includes vascular, chondromesenchymal, rhabdomyomatous, mesenchymal, fibro-osseous, and respiratory epithelial. 1
A 6-month-old, intact, male Weimaraner dog presented to the Veterinary Teaching Hospital at the Virginia-Maryland Regional College of Veterinary Medicine (Blacksburg, VA) with bilateral mucopurulent ocular and nasal discharge of approximately 5 months' duration. The dog had been treated previously with antibiotics with no response. Rhinoscopy at another veterinary referral center showed nasal turbinate loss but no fungal plaques. A computed tomographic scan of the head at the Veterinary Teaching Hospital showed a heterogeneously enhancing, expansile soft-tissue mass occupying both nasal cavities, the ethmoid region, and the frontal sinuses (Fig. 1). The nasal septum was deviated laterally, and there was bilateral lysis of the maxillary turbinates. The walls of the frontal sinus were thickened, irregular, and heterogenous. Based on the computed tomography findings, fibrous dysplasia or fungal rhinosinusitis was suspected. The dog was anesthetized for frontal sinuses trephination to collect samples of the mass for biopsy. The dog was euthanized after a prolonged anesthetic recovery and the development of neurologic signs consistent with caudal transtentorial herniation.
On gross examination, moderate amounts of tan, suppurative nasal and ocular exudate were present bilaterally. The left eyeball was deviated laterally. The nasal cavity was completely occluded by a light red to tan, soft, gelatinous mass that replaced the turbinates and extended into the frontal sinuses. Impression smears of the mass revealed large numbers of neutrophils and normal respiratory epithelium. Fungal and bacterial cultures failed to identify a causative agent. Histologically, the mass was composed of large fronds of loose fibrovascular stroma covered by a single layer of pseudostratified, columnar, ciliated epithelium (Fig. 2). Moderate numbers of goblet cells were interspersed among the columnar epithelial cells. Individual cells were uniformly sized and lacked cellular atypia, pleomorphism, or mitotic activity (Fig. 3). The epithelial cells occasionally formed invaginations into the supporting stroma that were continuous with the surface epithelium or formed glands or ducts (Fig. 2). The glands contained abundant mucinous material. The centers of the fronds were occasionally mineralized or were composed of residual bony trabeculae. In some sections of the mass, the stroma was infiltrated by large numbers of lymphocytes, plasma cells, macrophages, and neutrophils; the epithelium was focally eroded. Based on the histologic appearance, the age of the dog, and the extent of nasal and frontal sinus involvement, a diagnosis of respiratory epithelial adenomatoid hamartoma (REAH) was made.
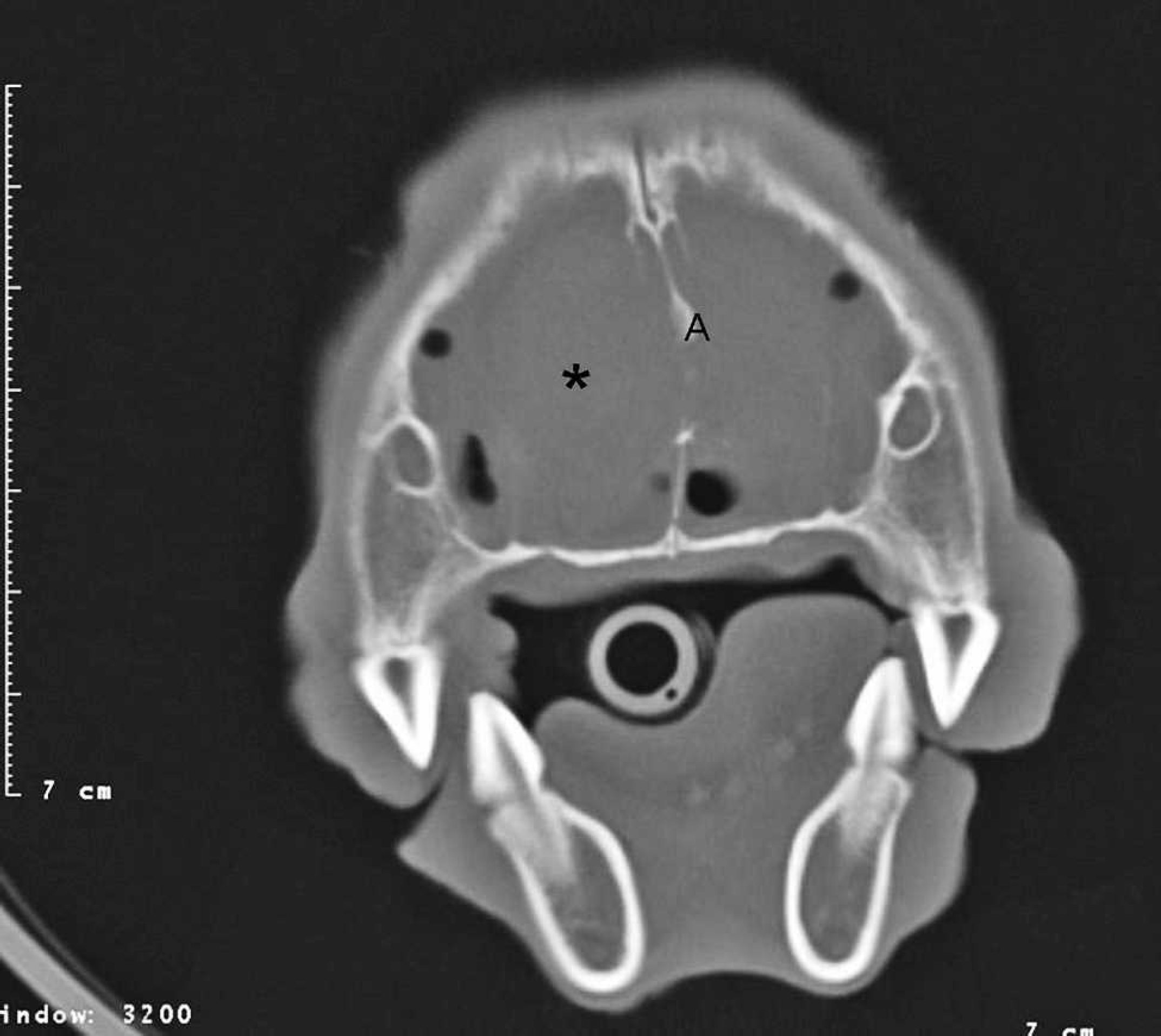
Computed tomographic image of the head through the nasal cavity and frontal sinuses. A heterogeneous soft-tissue mass occupies both nasal cavities and the frontal sinuses (*). The nasal septum is lytic and deviated laterally (A).
The criteria for the diagnosis of REAH in humans are 1) that the glandular component consists of respiratory epithelium that is continuous with the surface epithelium and 2) that the polypoid growth is the result of respiratory epithelial adenomatoid proliferation. 1 The feature that differentiates these masses from inflammatory sinonasal polyps is the extensive glandular proliferation. 1 There is some speculation that chronic rhinosinusitis may induce REAH, because nasal polyposis occasionally occurs in conjunction with REAH. 4 However, whether the sinusitis or the REAH develops first has not been established.
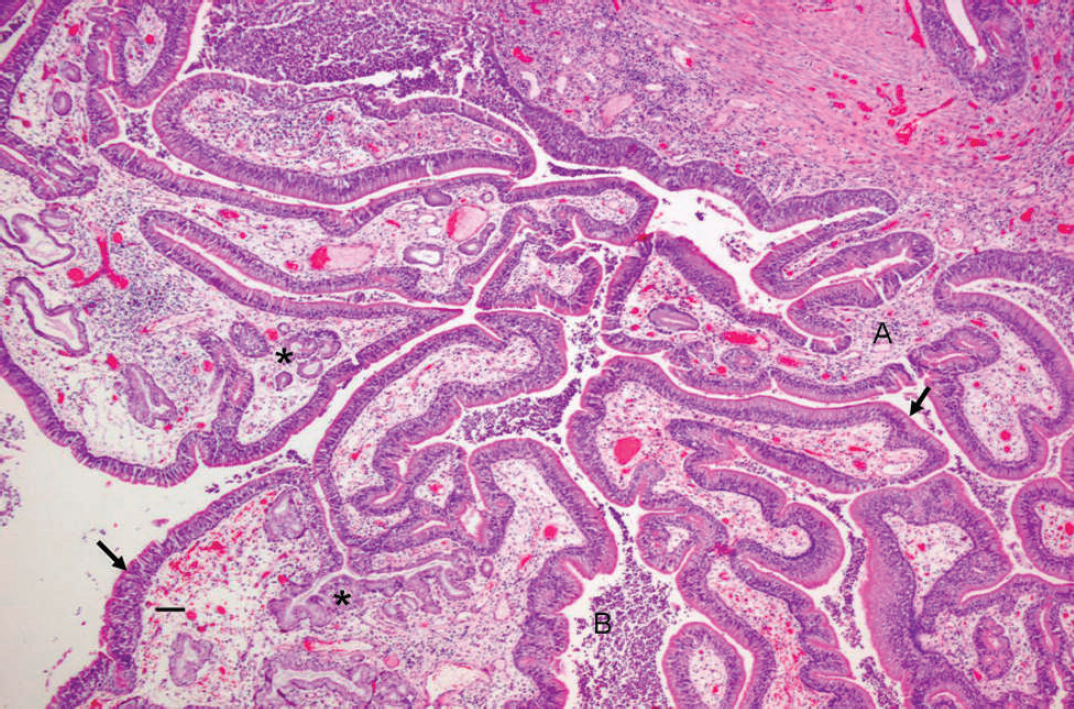
Large fronds of loose fibrovascular stroma (A) are covered by a single layer of pseudostratified, columnar, ciliated epithelium (arrows) and interspersed goblet cells. The epithelial cells occasionally form invaginations into the supporting stroma that are continuous with the surface epithelium or form glands or ducts (*). Large numbers of neutrophils are in the lumen (B). Hematoxylin and eosin. 40 × magnification. Bar = 50 μm.
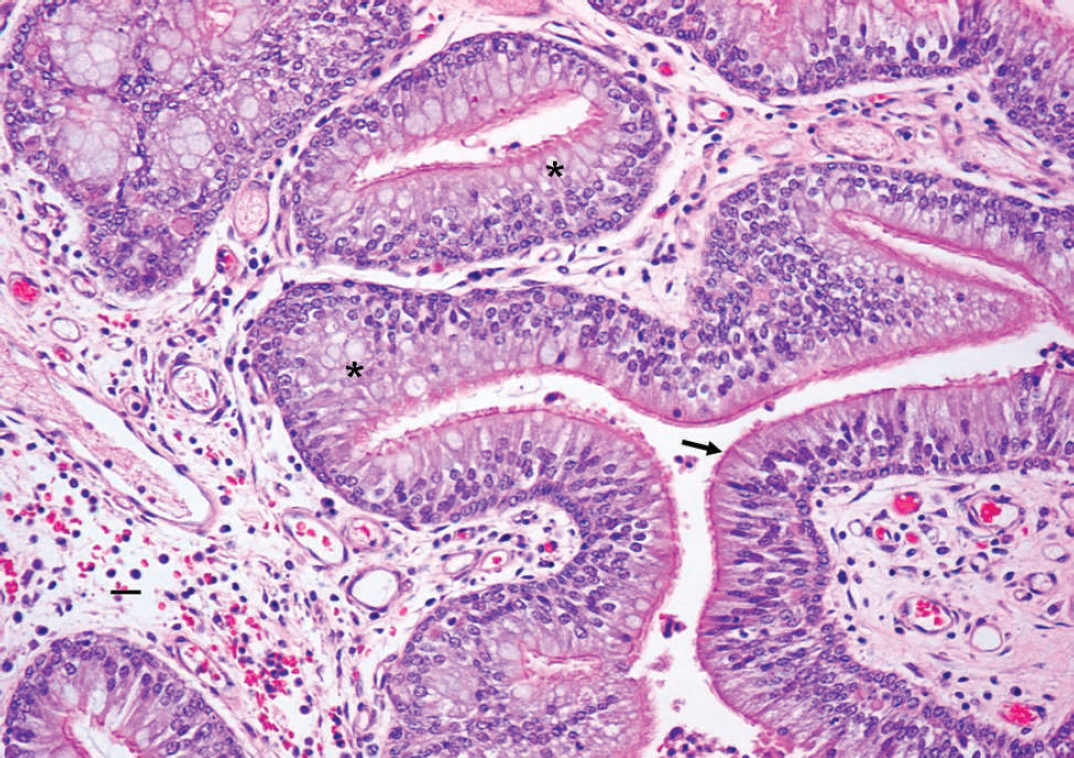
Higher magnification of the uniform layer of pseudostratified, columnar, ciliated epithelium (arrow) and goblet cells (*). The cells are uniformly sized, and there is no cellular atypia, pleomorphism, or mitotic activity. Hematoxylin and eosin. 200 × magnification. Bar = 25 μm.
Rhinosinusitis may potentially develop as a result of abnormal bacterial clearance in the nasal and sinus cavities because of the space-occupying mass and turbinate loss. Although conservative surgical excision of REAH in humans is considered curative, 1 distinguishing hamartomas from inverted papilloma or adenocarcinoma is important to prevent more aggressive surgical approaches. 10 Histologically, the mass in the dog in the current study had criteria for the diagnosis of REAH. The inflammatory infiltrates were considered secondary and were most likely a result of decreased bacterial clearance due to the extensive turbinate loss. Although complete surgical excision may not have been possible in the present case due to the close association with the cribriform plate, debulking followed by radiation therapy may have been at least partially successful in reducing the size of the mass and clearing secondary infections. Unfortunately, complications due to frontal sinus trephination resulted in cerebellar herniation, and the dog was euthanized.