
Abstract
Background
Patients’ access to psychiatric care is partially limited by the number of psychiatric providers. To address this gap in care, there has been an increase in advanced practice providers (APPs) providing psychiatric care.
Method
We discuss our institution’s experience with the integration of APPs into our outpatient psychiatry clinic. We describe our motivations, the problems we faced, and the changes we made to address them. In addition, we describe the current practice model of APPs in our practice, and the impact of having APPs in our practice.
Results
Our institution has added 17 APPs to our pool of clinicians. We increased the number of patients we see annually from 3163 unique patients in 2015 to 11667 unique patients in 2023. In 2023, APPs saw 6362 of these unique patients. In addition, the average wait time for a new appointment dropped from over 12 weeks in 2015 to 2 weeks in 2023.
Conclusion
APPs have been valuable in addressing the growing demand for psychiatric services at our institution. Our described current model can serve as a reference for the integration of APPs into an outpatient psychiatric clinic.
Keywords
Introduction
Patients’ access to psychiatric care is a long-standing yet urgent challenge for healthcare institutions. The need is great, but resources are often limited by availability of clinicians and inadequate payor sources. Creating effective and efficient models of care is a practical and ethical problem with several potential solutions. One such solution available relatively quickly is the integration of advanced practice providers (APPs) into psychiatric teams. The complexities of psychiatric care demand this assimilation be thoughtful, but incorporating APPs can be a valid way to increase patient’s access to quality care. In this paper, we will share our institution’s experience with bringing APPs into our practice. We will describe our motivations, the problems we faced, and the changes we made to address them. In addition, we will describe the impact of having APPs in our practice. Our research has been approved by the University of Texas Southwestern Institutional Review Board as non-regulated research. We hope our current model can provide guidance to institutions interested in improving patient access with APPs. We also hope to begin a conversation about how best to improve ongoing APP training to help ensure the highest quality care.
APPs refers to 2 categories of clinicians: Physician Assistants (PAs) and Nurse Practitioners (NPs). PA graduate school training is around 2.5 years full-time, including preclinical didactics and clinical rotations. There is some formal psychiatric training, with the certifying body of PA schools requiring behavioral and mental health in the didactic curriculum and supervised clinical experience. 1 NPs enter graduate training after receiving their RN degree. NP training is around 2 years full-time. NPs trainees typically arrange their own clinical rotations, and there are an increasing number of online NP training programs. 2 NP trainees decide on their specialty focus before their training starts, so they can obtain a wider foundational base in psychiatry by the end of the training. This stands in contrast with PAs that are trained using the medical models. This model sets up PA trainees to have more general medical knowledge, but less foundational knowledge in a specific specialty like Psychiatry. NPs, though, may have differing types and amounts of nursing experience prior to their further training. Recently, there are 1-year post-graduate training opportunities for APPs in specific specialties, like psychiatry. 3
By contrast, medical school is typically 4 years. In addition, psychiatric training requires a post-graduate residency. Adult psychiatry residency require 48 to 60 months of supervised clinical hours, and child psychiatrists require even further training. 4
Legal restrictions for APPs also varies between states. Many states mandate that APPs have protocols approved by a medical director to ensure structured patient care plans tailored to their training, but an increasing number – currently 26 states – have adopted a full practice authority for APPs. 5 In Texas, where we practice, APPs do not have full practice authority, and are required to have a prescriptive authority agreement with a physician through the medical board. 6 There are no formal requirements for ongoing supervision in Texas.
The Beginnings of APP Integration into UTSW
In 2010, our clinic was facing a large demand for psychiatric services that we could not provide with the MDs we had available. Our waitlist had over 100 patients on it, and we could not estimate when any of them might be seen. This number soon became almost meaningless, as we felt we could do nothing about it. But as soon as we appreciated that this number represented actual people waiting for care, the ethical imperative to improve access became acute. Let me give an example.
A psychologist in our group asked me (Dr Larry Thornton) to see a patient on the waitlist. The patient was getting increasingly depressed, and the psychologist was worried. I evaluated the patient over lunch, started escitalopram, and a month later he was well on his way to remission. Although most of our work is rarely so straight forward as this, sometimes it is, and I became haunted by the thought of people unable to get care “who just needed Lexapro.” So, when our Vice Chair for Clinical Services developed a plan to grow our clinic using a mix of MDs and APPs, I was eager. I wanted to get care to as many people as effectively as possible.
Initially, we brought on 3 NPs as they were easier to find and hire quickly than academic psychiatrists. Our first 3 APP hires were experienced NPs who had already worked independently for some years and came with excellent recommendations. Since none of us had worked with APPs before, our first concern was to establish trust between the NPs and their supervising MDs. Our major questions were could the NPs develop an alliance with patients, formulate a solid differential diagnosis, and develop and monitor a reasonable treatment plan. To answer these questions, we had the new APPs shadow their supervising MD for 2 weeks; the MD sat in on at least one evaluation by the NP. The MD and APP then met weekly for an hour to review cases, and the MD reviewed all the NPs charts for the first weeks to assess documentation practices and clinical reasoning. We also made it clear to the new APPs that they could reach out to their supervisor at any time for consultation. We wanted to create a culture of consultation without fearing that asking questions would call into question their competency. We made it clear that the MDs in the practice regularly sought input, including formal second opinions, from their colleagues on challenging cases.
Because our first hires were so experienced, we rapidly gained trust in them. Of particular importance in developing trust were the quality and frequency of their questions. Good questions can show a good understanding of the case, demonstrate the questioner’s extent of knowledge, and provide a reassuring realization of limitations and comfort seeking help. These features were essential for developing trust between the supervisor and the APP.
As our need for access was so high and our current physician’s practices were already full, our first APPs immediately began seeing new evaluation. We did a slow ramp up of the number of new evaluation seen, maximizing to 4-5 new evaluations each day. Since our APPs were experienced, they managed this early period well and soon developed a typical panel of patients. As soon as they had trouble getting follow-ups scheduled within 4 weeks, we lowered their new visits to 2 daily.
We found during this early period that some of the APP’s cases were too complex and challenging to be addressed in supervision. For these cases, the supervising MD would be scheduled to see the patient themselves, typically for 30 minutes. Some of these cases were one time visits, others were taken by the MDs into their practices, while some stayed primarily with the APP, but were seen periodically by the MD. This co-management of patients would become a template for our later practice.
Current Practice Model for APPS at UTSW
Training Model
As our clinic grew, we added new APP positions, but we had more difficulty finding experienced clinicians than we had imagined. We decided to hire recently graduated APPs that impressed us as intelligent, hardworking, and likely to develop into good clinicians. We favored NPs with longer experience as RNs and were fortunate to find two APPs with psychotherapy training, but we often hired those with the personal characteristics we thought were worth taking a chance on.
We found, not surprisingly, that this lack of experience as front-line clinicians led to some problems. The most common were underdiagnosing significant depression as adjustment disorder, not increasing antidepressant doses quickly enough, and not being able to give patients a sense of confidence in the care they were receiving. One marker was a high rate of requests to either see an MD or to change clinicians. Satisfaction scores were substantially lower for the less experienced APPs than for most of our MDs. This led to our current training model for APPs at UTSW.
Onboarding Training That Advance Practice Providers (APPs) Receive at the University of Texas Southwestern (UTSW) Psychiatry Clinic

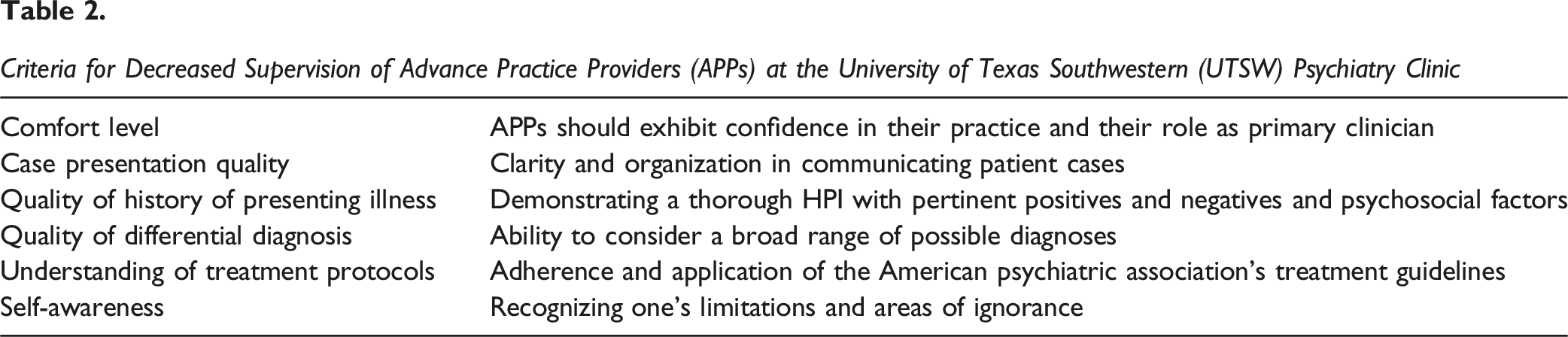
Criteria for Decreased Supervision of Advance Practice Providers (APPs) at the University of Texas Southwestern (UTSW) Psychiatry Clinic
Structure of Continued Learning of Advance Practice Providers (APPs) at the University of Texas Southwestern (UTSW) Psychiatry Clinic

Current Model of Practice
Triaging patients who might be better suited an APP vs an MD has been a challenge. We initially assigned cases to APPs and MDs by diagnosis, but ultimately decided that this was not a good predictor of complexity. We therefore rely on weekly supervision and a culture of second opinions to address more challenging cases.
Currently, we do route all ADHD referrals solely to our APPs. For the remainder of our non-specialty referrals, we have two broad categories, General Psych A includes depression, anxiety, PTSD, grief, and adjustment disorder. These are routed to all providers in clinic. General Psych B includes bipolar disorder and psychotic disorders. These are routed to all MDs and a select number of APPs who have been judged by their supervisors to be ready for such cases. Typically, these APPs have been with us at least 1 year, but this can vary based on level of prior experience and their demonstrable ability.
We considered having MDs see all the new patients, but the MDs wanted to maintain enough time to develop long-standing relationships with their patients, and the APPs wanted to improve their evaluations skills. Still, we do encourage the MDs to develop a collaborative team model with the APPs so the MDs can maintain enough time to utilize their typically more advanced diagnostic skills.
We maintain a structured system of oversight for APPs. We require newly hired APPs to meet with their supervising MDs one hour weekly for a minimum of one year. Weekly supervision can continue as long as the MD finds it necessary. Some newer APPs have continued weekly supervision for 4 years now. The minimum frequency for supervision is monthly. The UTSW Healthcare system requires at least 10% of the APPs cases be reviewed. While APPs cannot staff every patient case with a medical provider, they are encouraged to seek guidance and collaboration whenever necessary, allowing for flexibility based on individual confidence and case complexity. As APPs develop, they are clearly able to evaluate and manage patients of high complexity with great skill. They have provided high quality care to the full spectrum of patients, including initiating Clozapine, MAOIs, and referring for ECT.
We have recently begun quarterly meetings for the MDs supervising APPs to discuss challenges and share strategies. This has been especially helpful for the junior faculty who have had less experience supervising residents.
As our team of APPs has grown, we have designated a lead APP who is their voice in the administrative structure of the clinic. The lead APP helps with education, problem solving, recruiting, and performance appraisals.
Impact of APPs in the UTSW Psychiatry Clinic
Our model of APPs in the UTSW psychiatry clinic has led to major improvements. Our data assessment for the impact of APPs in the UTSW psychiatry was approved by the UTSW IRB as non-regulated research. We have been able to add 17 APPs to our pool of clinicians. This has helped us increase the number of patients we see annually from 3163 unique patients in 2015 to 11667 unique patients in 2023. In 2023, APPs saw 6362 of these unique patients. In addition, our average wait time for a new appointment dropped from over 12 weeks in 2015 to 2 weeks in 2023. We have also developed an urgent-care function in our clinic using APPs which allows us to see crisis patients or urgent new evaluations within a day or so.
Patient satisfaction with APPs is now high, with Press Gainey Scores comparable to our MDs. We understand there are limitations with the Press Gainey Score, but it is notable that average scores for the last 4 years are comparable between Physicians and APPs (2021: 95.20 (MD) to 93.44 (APP), 2022: 96.10 (MD) 91.89 (APP), 2023: 92.04 (MD) vs APP (92.53). Since implementing our new training and practice model, fewer patients request to change from APPs to Physicians. This phenomenon could also be explained with the cultural shift as APPs are more well known in our society. We have also found that if the MD has a strong collaborative relationship with the APP and genuinely feels that they are a team, patient acceptance and satisfaction is high.
Our APPs report appreciation for the amount of supervision we provide. A few have said they have stayed with us because they know they are becoming better clinicians. Others have said they became more deeply aware of the role of psychotherapy in medication-management practice. Most of our APPs are becoming increasingly adept at listening in a therapeutic way.
Future Directions
As the UTSW Psychiatric Clinic looks to the future with APPs, we plan for a strategic shift towards a competency-based framework. This approach will emphasize the development of specific, essential competencies for psychiatric care, ensuring that APPs are proficient in both theory and practice. APPs tend to have minimal psychotherapy training in their education. We are incorporating more formal education in psychotherapy fundamentals, and we plan to have more ongoing attending-observed evaluations and appointments, with an emphasis on improving interviewing and alliance-building skills.
We are also creating more designated slots for APPs to get MD consultations. We have found that AAPs learn much from these formal second opinions. As mentioned before, we want to create a culture where second opinion, consultations, and shared patient care is valued and promoted. We are currently looking at developing an algorithm which will prompt all clinicians in our clinic to consider a consultation when their patient is not improving.
From a hiring perspective, we value APP applicants who demonstrate enthusiasm for learning. We also look for evidence that they are flexible and able to adapt to new situations. We place importance of teamwork and growth, with an eagerness to ask questions and comfort in recognizing their limitations. These are skills we also value in our physicians. In addition, we have come to value APPs who are fellowship trained. We have seen a marked difference in readiness to practice with APPs with fellowship training. They demonstrate more sophisticated clinical reasoning and a stronger ability to conceptualize cases.
Conclusion
We describe a model at UTSW of integrating APPs into an outpatient psychiatry clinic. While there have been challenges with the incorporation of APPs into the clinic, we have established a robust onboard training, supervision and continual learning requirements for our APPs. APPs have been valuable in addressing the growing demand for psychiatric services at our institution.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors list above certify that they have NO affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.