
Abstract
Background
Habit reversal training (HRT) is an efficacious intervention for individuals with tic disorders that can be delivered both in-person and via telehealth. Despite noted effectiveness, no known studies have directly compared provider perceptions of these modalities of HRT delivery.
Methods
Professionals providing HRT for individuals with tic disorders (n = 136) completed an online survey to assess perceptions of telehealth-delivered HRT compared to in-person services.
Results
Providers reported lower feasibility of telehealth relative to in-person HRT for patients younger than 8 years old but greater feasibility of telehealth for patients 13-17 years old and 18-65 years old. Telehealth HRT was perceived to be more feasible for patients with less severe tic presentations. Providers reported greater feasibility in an in-person environment compared to telehealth for addressing therapeutic factors, individual patient differences, and characteristics of the patients’ tics. Lastly, providers reported that all aspects of HRT are more feasible to implement in-person compared to telehealth settings.
Conclusion
Findings suggest there are a variety of clinical factors that providers believe could impact HRT treatment, which should be considered when determining whether an in-person or telehealth treatment model is best fit for individuals with tic disorders.
Introduction
Tics, or rapid, non-rhythmic movements or vocalizations, are the hallmark feature of a class of childhood onset neurological conditions called persistent (chronic) tic disorders (PTDs). 1 Motor and vocal tics can be categorized as simple or complex, with simple tics as typically brief, purposeless movements (eg, eye blink, head jerk) or sounds (eg, sniff, grunt), and complex tics as more purposeful behaviors that may consist of a coordinated action of multiple muscle groups (eg, tapping, jerking an arm then head) or words/phrases. 2 Under the umbrella term of tic disorders, three primary diagnosable conditions exist, including: Tourette’s disorder (TD), persistent motor or vocal tic disorder, and provisional tic disorder. These three conditions are differentiated by the duration and type of tics (ie, motor and/or vocal) present. TD involves the presence of multiple motor and one or more vocal tics for at least 1 year, while individuals with persistent motor or vocal tic disorders have a single or multiple motor or vocal tics, but not both, present for at least 1 year. Provisional tic disorder includes individuals with motor and/or vocal tics present for less than 1 year.
Tic disorders impact approximately 1% of youth 3 and are more prevalent in males (4:1 male to female prevalence ratio), 4 with tic onset usually appearing between the ages of 5 and 7.2,4 Premonitory urges, which are uncomfortable physical sensations such as an itch or tension, occur prior to tics in approximately 90% of individuals with tic disorders. 5 These sensations are typically localized to body parts directly involved in the tic but may also be generalized across the entire body. Most individuals report that tics alleviate the uncomfortable physical sensation, which leads to the negative reinforcement of the behavior.6,7 Additionally, academic, social, and familial impairment are common in those with tics,8,9 and between 78% and 90% of individuals also experience comorbid conditions,10,11 with attention-deficit hyperactivity disorder (ADHD), obsessive-compulsive disorder (OCD), and anxiety disorders being the most common.2,10
Treatment guidelines suggest psychotherapeutic interventions as a first-line option for tic disorders. 12 Randomized controlled trials (RCTs) have demonstrated that habit reversal training (HRT) leads to significant reductions in tics and is more effective than supportive psychotherapy at reducing tic severity and tic-related impairment.13,14 In treatment, HRT is applied to each of the patient’s tics and consists of awareness training, competing response training, and social support. Awareness training is implemented to help patients recognize discrete instances of their target tics. Clinicians guide the development of a detailed description of the tic and use prompts and praise to help patients detect the target tic and tic warning signs (eg, premonitory urge). In competing response training, patients are taught to engage in a different behavioral response that is incompatible or inconsistent with the tic (eg, gently pressing shoulders downward for a shoulder shrug tic) when they feel the urge to perform their target tic or after target tic occurrence. Finally, social support training involves teaching a support person (eg, parent or spouse) to praise patients for correctly engaging in their competing responses and prompt the use of competing responses if they are not performed correctly. 15
Comprehensive behavioral intervention for tics (CBIT) is an effective behavioral intervention for tics and includes HRT as the primary treatment component, along with functional assessment/functional interventions, relaxation training, and a motivational reward program. 15 Additional RCTs with larger sample sizes built upon early HRT findings and demonstrated that CBIT is more effective than supportive psychotherapy at reducing tic severity and tic-related impairment in youth and adults with tic disorders.16,17 Behavior therapy for tics delivered via telehealth has also shown preliminary efficacy in several studies.18-21 Himle et al 18 randomized 20 children with tic disorders to CBIT delivered in-person or via telehealth. Results showed that youth in both conditions experienced significant reductions in tic severity and tic-related impairment, with no differences between groups. Similar findings were demonstrated in a study that compared in-person to telehealth behavior therapy (either HRT or exposure and response prevention (ERP) for tics), with results showing improvements in tic severity scores in both conditions and no differences between groups. 21 Additionally, Ricketts et al 20 found that children provided telehealth CBIT demonstrated better treatment outcomes than children in a wait-list control (WLC) group, while Inoue et al 19 showed that telehealth group CBIT led to improvements in tic severity. Although preliminary evidence for telehealth HRT and CBIT is promising, existing research has been limited to small sample sizes, with the exclusion of complex cases that may be seen in an open clinic setting (eg, tic severity and comorbid ADHD severity exclusion criteria).
Indeed, CBIT/HRT are the first-line psychotherapeutics for tic disorders, with growing evidence supporting effective telehealth delivery.18-22 This is consistent with broader literature, where telehealth psychotherapies can be effective for addressing concerns across the continuum of psychopathology.23-25 Despite noted effectiveness, telehealth and in-person psychotherapies may not be analogous, as telehealth services may present unique problems that are not present during in-person services.24,26 Prior research notes limited field of view,27,28 concerns of technology literacy, 29 difficulty concurrently engaging family members alongside patients, 30 and difficulties with visual and physical assessments of symptoms 31 as relevant factors that can adversely impact telehealth treatment delivery. These concerns may be further compounded in pediatric populations, where providers report greater levels of preparation and creativity necessary to adequately engage and deliver therapeutic interventions in a telehealth environment.32-34 Although telehealth services can be effective, little research has examined factors that may impact the delivery and effectiveness of telehealth interventions. As stated by Batastini and colleagues, 24 it remains unknown “what works for whom and under what circumstances.” Our group has independently posed a similar question, “when and for whom are telehealth services appropriate?”
Considering these questions, we have initiated work examining provider perceptions of both telehealth and in-person therapies across different psychopathologies. From this research, we provide evidence that providers report greater ability to identify and address factors that adversely impact the course of treatment in an in-person compared to telehealth environment, and that providers identify telehealth services as less feasible relative to in-person when working with younger and more severe presentations.35,36 Collectively, this suggests there may be circumstances and/or patient characteristics where telehealth services are suboptimal relative to in-person services, although this has not yet been examined in tic disorders.
These concerns may be particularly relevant to tic disorders, where access to appropriate care has been limited.37,38 This is further corroborated by both children and parents of children with tic disorders reporting difficulty accessing treatments and concerns their health care providers are generally unaware of these conditions and appropriate treatment options. 39 Telehealth delivery of HRT poses the opportunity to mitigate difficulties accessing care; however, it must be considered if it is a viable option for all presentations, as the expansion of telehealth does not appear to be slowing anytime soon. Although limitations may be present with telehealth, the rapid expansion of available services may offer many benefits that are not afforded with in-person services.34,40 This includes increased access to care, more convenient and cost-effective treatment options, improved appointment flexibility, reduced travel and wait times for patients, decreases in patient stress, and increases in overall patient satisfaction.41-43 Additionally, telehealth services have been shown to be beneficial for providers themselves by increasing scheduling flexibility, reducing the number of cancellations, and reducing provider burden overall, while also allowing providers a unique insight into the everyday lives of their patients to provide more effective care.43,44 Although these benefits cannot be overstated, it must be considered whether telehealth services are appropriate in all circumstances, and what considerations are warranted when treating those with tic disorders. These considerations are particularly timely and important to consider in the wake of the COVID-19 pandemic, as telehealth behavior therapy has become increasingly popular and appears to be here to stay.
The present study examined provider perceptions of in-person vs telehealth delivery of HRT for individuals with tic disorders. Since HRT is present in both traditional behavioral treatments, and newer treatments (ie, CBIT), we assessed provider perceptions of HRT to be more inclusive. The survey assessed the perceived feasibility of delivering HRT for patients at different age ranges and levels of tic severity. Another aim of the study was to examine provider perceived ability to identify and address therapeutic factors (eg, use of competing responses) and patient individual differences (eg, treatment motivation) that may impact in-person and telehealth delivery of HRT. The survey also assessed provider perceived feasibility of implementing in-person and telehealth HRT based on characteristics of patients’ tics (eg, simple vs complex motor tic), as well as perceived feasibility of implementing different components of HRT in-person and via telehealth. We hypothesized that (a) providers would report greater feasibility for in-person compared to telehealth HRT for patients under the age of 13; (b) providers would report greater feasibility for in-person compared to telehealth HRT for higher vs lower levels of tic severity; (c) providers would report greater ability to identify and address therapeutic factors that may impact treatment in an in-person environment compared to telehealth; (d) providers would report greater feasibility of implementing HRT in an in-person environment relative to telehealth for patient individual differences that may impact treatment; (e) providers would report greater feasibility to implement different components of HRT in-person compared to telehealth.
Methods
Participants
Participants consisted of a variety of mental health providers with diverse clinical backgrounds and experiences who are currently providing HRT for adults and/or children/adolescents with tic disorders. Eligible participants included those: (1) between the ages of 18-88 years old, (2) fluent in English, and (3) reported history of treating individuals with tic disorders with HRT based interventions. Participants who completed less than 50% of the survey items were excluded from the analyses.
Materials
A brief survey assessing experiences using HRT to treat individuals with tic disorders in both in-person and telehealth settings was administered to all participants. The present survey was adapted and modified from a survey used previously to investigate clinicians’ perceptions of telehealth vs in-person ERP for individuals with OCD. 35 External expert HRT clinicians unaffiliated with the project independently reviewed the survey and provided feedback on each item before the questionnaire was finalized and distributed. In addition to basic demographic information, providers were asked to provide information regarding their clinical background and current occupation title (eg, psychologist, psychiatrist, psychotherapist, occupational therapist, neurologist, etc.), level of clinical training (eg, clinician or student/trainee), and the number of years they have practiced as a mental health professional. Providers were then asked a series of questions pertaining to their perceptions of telehealth compared to in-person HRT as a feasible and effective method of treating individuals with tic disorders.
Providers were first asked to rate the feasibility of implementing telehealth compared to in-person HRT services when treating individuals with tic disorders based on the consideration of age. Participants provided their responses for the following age groups on a scale from 1 (much less feasible) to 5 (much more feasible): < 8 years old; 8-to-12 years old; 13-to-17 years old; 18-to-65 years old; and > 65 years old. Providers were then asked to rate the feasibility of telehealth compared to in-person HRT for individuals with differing levels of tic severity. Responses were provided for the following categories of severity level on a scale from 1 (much less feasible) to 5 (much more feasible): mild symptoms, moderate to marked symptoms, and severe to extremely severe symptoms.
Next, each provider was asked to provide feedback, based on their own experiences, regarding their perceived ability to identify and address various therapeutic factors that may impact treatment for both telehealth and in-person delivered HRT. Participants responded to the prompt, “As a provider, I am able to identify and address the following…” for both in-person and telehealth scenarios and responses were collected for the following factors: upper body tics, lower body tics, elicit feedback from patients about the use of competing responses and functional intervention techniques, tic-contingent consequences, intense premonitory urges, non-verbal communication, and difficulties delivering/patient understanding of psychoeducational materials. Responses were collected on a scale from 1 (strongly disagree) to 5 (strongly agree). Providers were then instructed to rate the feasibility of telehealth compared to in-person HRT for individuals with tic disorders based on individual patient differences that may impact the effectiveness of HRT delivery. Responses were recorded on a 1 (much less feasible) to 5 (much more feasible) scale and collected for the following patient characteristics: awareness of tics, treatment motivation, anxiety sensitivity, cognitive ability, family support. Additionally, providers were asked to rate the effectiveness of implementing telehealth vs in-person HRT based on characteristics of the patient’s tics that may impact the delivery of HRT. Responses were recorded on a 1 (very ineffective) to 5 (very effective) scale and collected for the following tic characteristics: simple motor tics, complex motor tics, simple vocal tics, and complex vocal tics.
Finally, participants rated their perceived feasibility of implementing different components of HRT including awareness training, competing response training, social support, and functional assessment/interventions in telehealth vs in-person environments. Responses were recorded on the same 1 (very unfeasible) to 5 (very feasible) scale.
Procedures
Participants were recruited through public email listservs from mental health-related organizations, including the Tourette Association of America, the International OCD Foundation, and the Anxiety and Depression Association of America, and snowball recruiting methods that targeted individuals with known expertise in treating tics. Data were collected from January 2023 to March 2023. After enrolling in the study, participants were given a brief description of the study purpose in relation to past research and asked to complete the virtual survey included. The survey was generated using Qualtrics Software and an anonymous link was provided. Completion of the survey was entirely voluntary, and all participants consented to participate by opening and completing the survey. Providers not currently or with little experience providing HRT to individuals with tic disorders were asked not to complete the survey but encouraged to share with others who meet the eligibility requirements. The survey was estimated to take approximately 20 minutes to complete, and no compensation was provided. This study was reviewed and approved by the Institutional Review Board at Baylor College of Medicine.
Data Analysis Plan
First, data were examined to assess normality. To investigate the perceived feasibility of delivering in-person vs telehealth HRT for different patient age-ranges, an omnibus repeated-measures analysis of variance (ANOVA) was conducted with age as the independent variable, which included five different age-ranges, and provider feasibility ratings as the dependent variable. Given the number of comparisons, post-hoc deviations contrasts (ie, mean feasibility rating for each age group compared to the mean of the other age groups except for the reference group) were used, with P < .001 as the significance value to reduce the risk of type-1 error.
To assess the provider perceived feasibility of delivering in-person vs telehealth HRT for different levels of tic severity, an omnibus repeated-measures ANOVA was conducted with the three levels of tic severity as the independent variable and provider feasibility ratings as the dependent variable. Post-hoc paired-sample t-tests were conducted, with P < .001 used as the significance value to reduce the risk of type-1 error.
To examine provider perceived ability to identify and address therapeutic factors that may impact treatment, perceived feasibility of implementing in-person and telehealth HRT based on patient individual differences, perceived effectiveness of implementing in-person and telehealth HRT based on characteristics of patient tics, and perceived feasibility of implementing components of HRT, four separate series of paired-samples t-tests were conducted. To account for multiple comparisons, a conservative P < .001 was chosen.
Results
Participant Characteristics
Demographic Information of the Study Sample (n = 136)
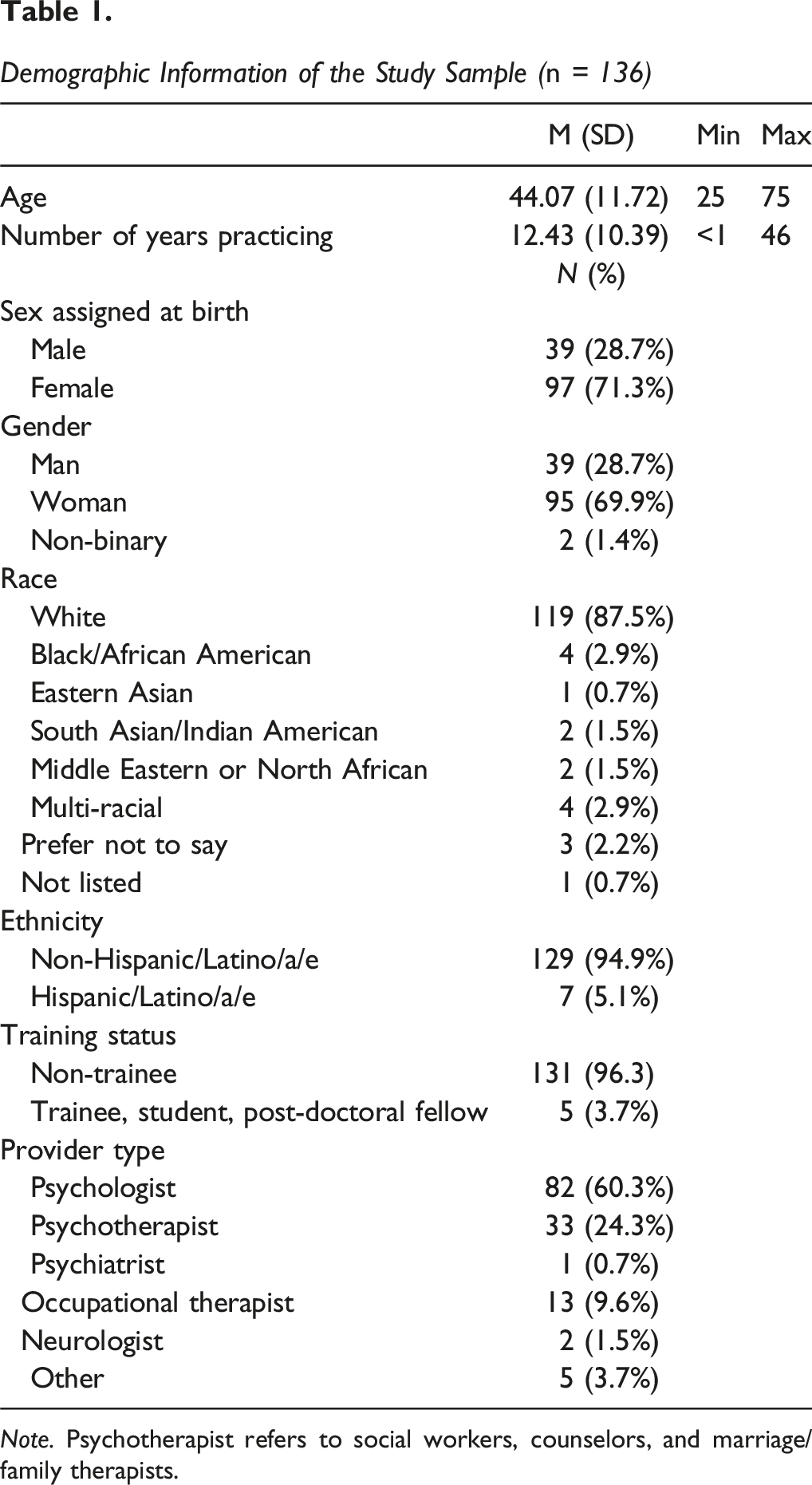
Note. Psychotherapist refers to social workers, counselors, and marriage/family therapists.
Factors Associated with Perceived Feasibility of Telehealth HRT
Age
To examine the perceived feasibility of delivering in-person vs telehealth HRT for different patient age ranges, a repeated measures ANOVA was conducted with self-reported feasibility ratings for each age-range as the dependent variable. Mauchly’s test showed a violation of sphericity (χ2 (9) = 131.40, P < .001), so degrees of freedom were corrected using Greenhouse-Geisser estimates of sphericity (ε = .69). Results showed a main effect of age (F (2.76, 62.70) = 111.28, P < .001, ηp2 = .473), which indicates that providers believe telehealth delivery of HRT relative to in-person is differentially feasible across different patient age groups.
Deviation contrasts were used to reduce the number of post-hoc tests needed to explain the main effect, with each age-range being compared to the grand mean of the other age-ranges. Provider-reported feasibility ratings for each age-range were as follows: Less than 8 years old (M = 1.77, SD = .85), 8-to-12 years old (M = 2.54, SD = .94), 13- to-17 years old (M = 3.11, SD = .81), 18-to-65 years old (M = 3.25, SD = .82), and greater than 65 years old (M = 2.85, SD = .96). Telehealth HRT was rated as less feasible than in-person HRT compared to the mean of all the other groups for children younger than 8 years old, t(124) = −15.82, P < .001. Age ranges in which telehealth HRT was rated as more feasible than in-person HRT compared to the mean of all the other groups included: 13-to-17 years old, t(124) = 11.42, P < .001; and 18-to-65 years old, t(124) = 12.09, P < .001. Finally, age ranges in which there were no significant difference between groups included: 8-to-12 years old, t(124) = −3.36, P = 001; and greater than 65 years old, t(124) = 2.48, P = .014 (See Figure 1). Self-Reported Feasibility Ratings for Delivering HRT via Telehealth Relative to In-Person for Different Age-Groups (1 – “much less feasible”; 5 – “much more feasible”). Error-Bars Reflect Standard Error of the Mean. ***P < .001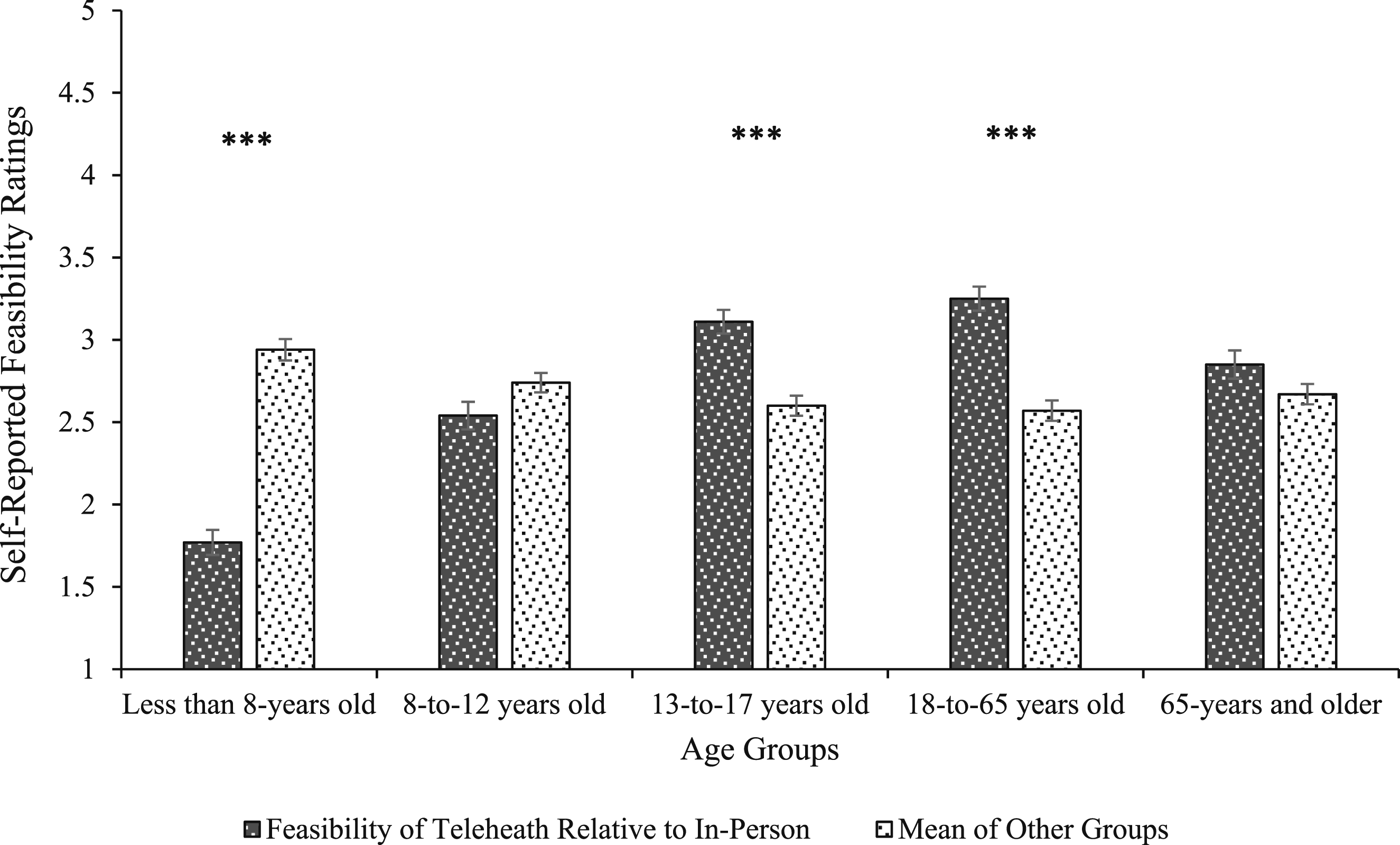
Tic severity
To examine the perceived feasibility of delivering HRT for patients with different levels of tic severity, a repeated measures ANOVA was conducted with self-reported feasibility ratings for each severity-range as the dependent variable. Mauchly’s test showed a violation of sphericity (χ2 (2) = 57.97, P < .001), so degrees of freedom were corrected using Greenhouse-Geisser estimates of sphericity (ε = .74). Results showed a main effect of severity (F (1.48, 199.83) = 73.79, P < .001, ηp2 = .353), which suggests that providers believe telehealth delivery of HRT relative to in-person is differentially feasible across tic severity levels.
Planned contrasts were used to examine the perceived feasibility for in-person relative to telehealth HRT for the following tic severity ranges: mild (M = 3.10, SD = .74); moderate-to-marked (M = 2.81, SD = .83); severe-to-extremely severe (M = 2.40, SD = .88). Results demonstrated greater feasibility for telehealth HRT for mild compared to moderate-to-marked (t(135) = 5.62, P < .001, d = .48); mild compared to severe-to-extremely severe (t(135) = 9.63, P < .001, d = .83), and moderate-to-marked compared to severe-to-extremely severe (t(135) = 9.04, P < .001, d = .78; Figure 2). Self-Reported Feasibility Ratings for Delivering HRT via Telehealth Relative to In-Person Across Different Levels of Tic Symptom Severity (1 – “much less feasible”; 5 – “much more feasible”). Error-Bars Reflect Standard Error of the Mean. ***P < .001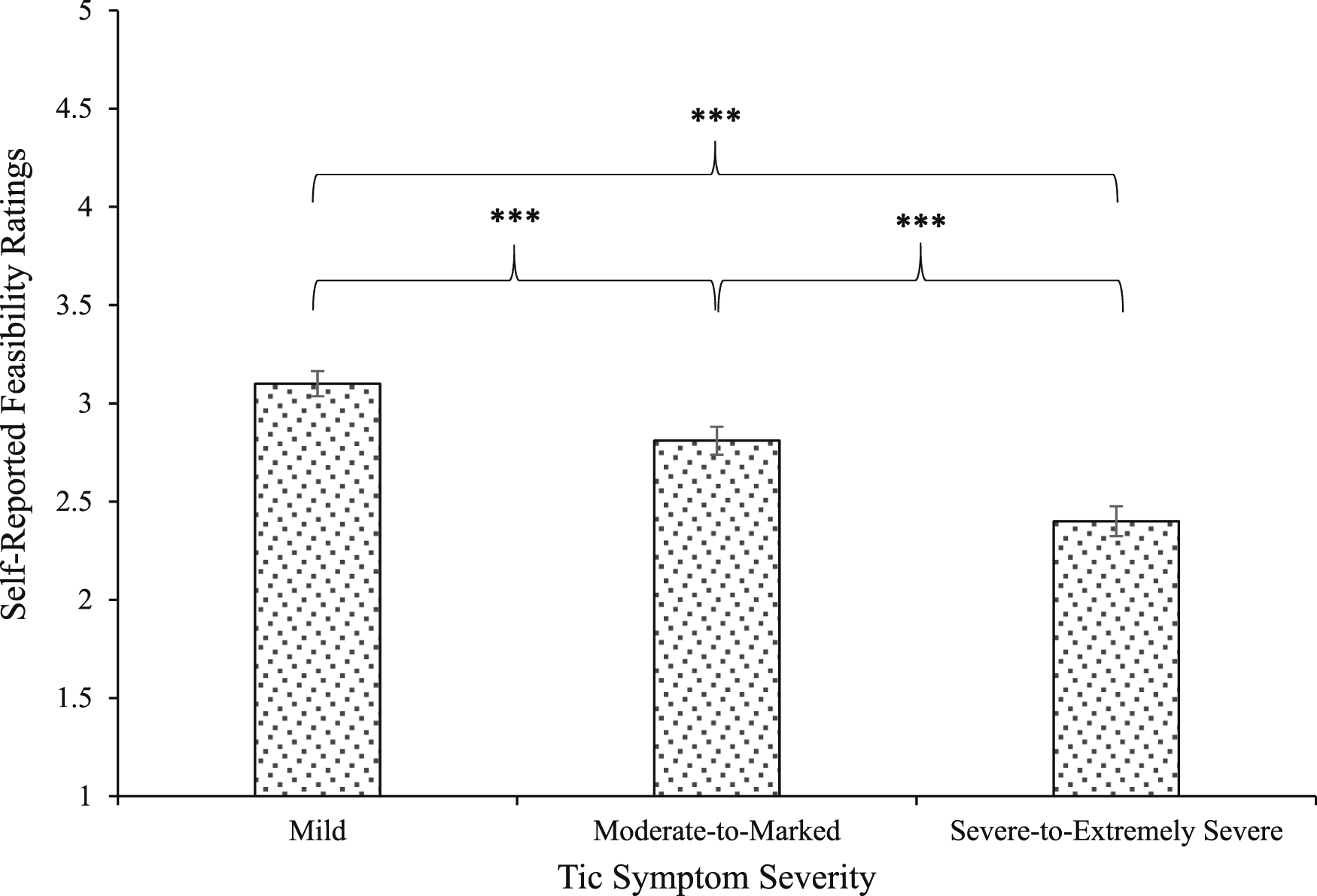
Therapeutic factors
Provider Ability to Identify and Address Therapeutic Factors That May Impact the Effectiveness of HRT in an In-Person vs Telehealth Environment
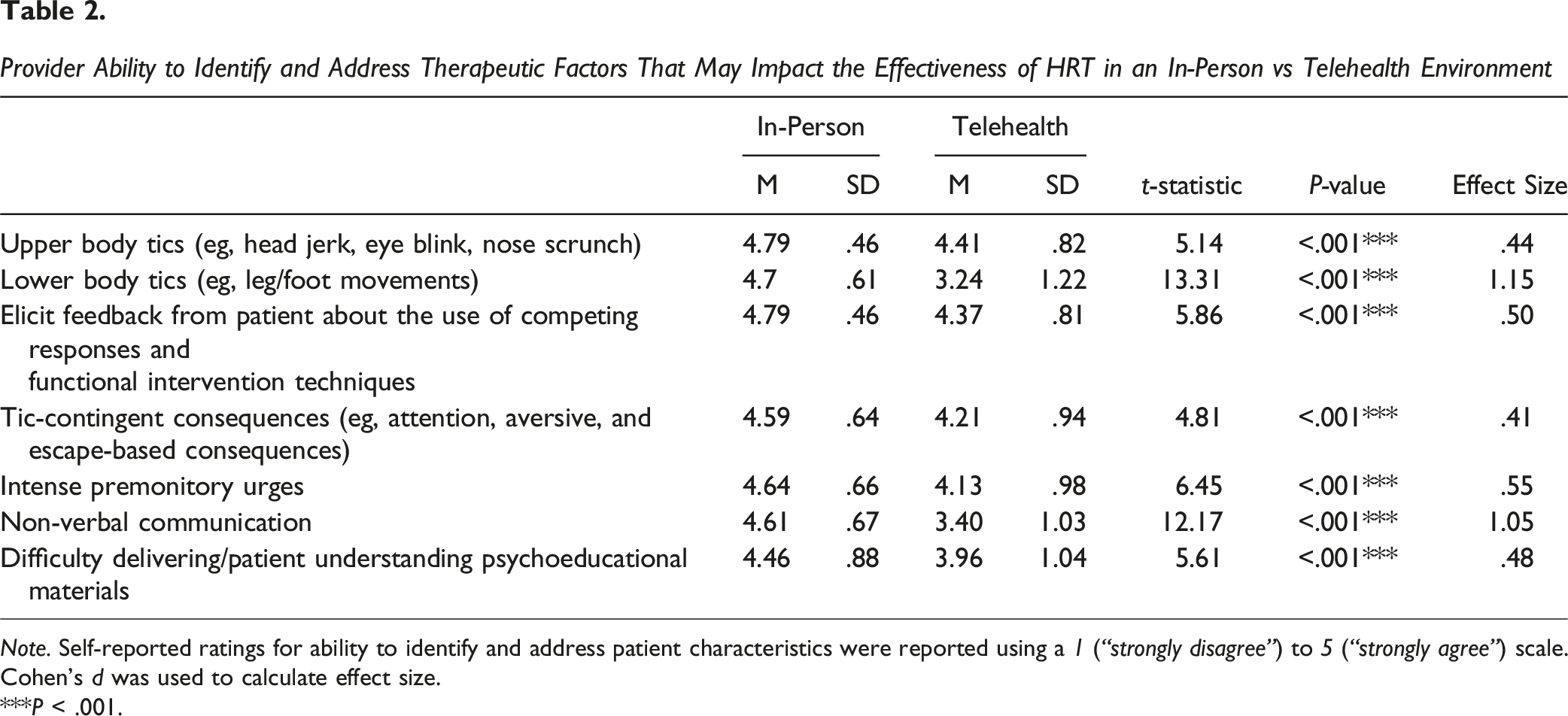
Note. Self-reported ratings for ability to identify and address patient characteristics were reported using a 1 (“strongly disagree”) to 5 (“strongly agree”) scale. Cohen’s d was used to calculate effect size.
***P < .001.
Perceived Feasibility of Implementing Telehealth Relative to In-Person HRT for Individual Patient Differences That May Impact HRT Delivery
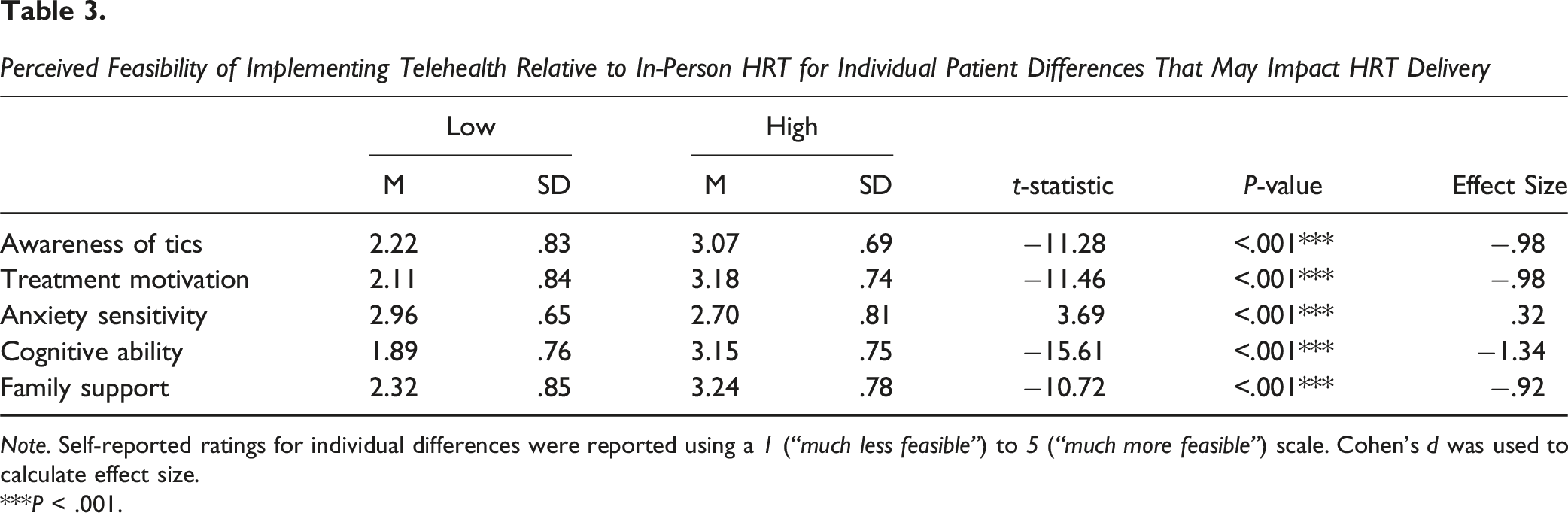
Note. Self-reported ratings for individual differences were reported using a 1 (“much less feasible”) to 5 (“much more feasible”) scale. Cohen’s d was used to calculate effect size.
***P < .001.
Perceived Effectiveness of Implementing In-Person vs Telehealth HRT Based on Characteristics of the Patients’ Tics
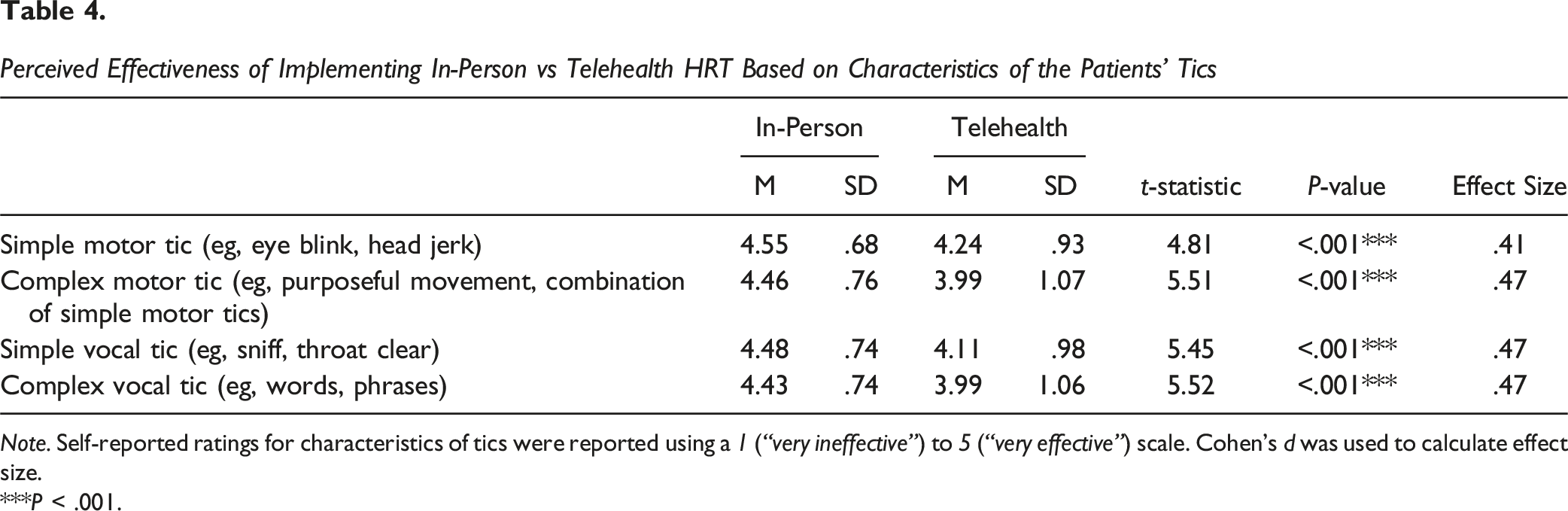
Note. Self-reported ratings for characteristics of tics were reported using a 1 (“very ineffective”) to 5 (“very effective”) scale. Cohen’s d was used to calculate effect size.
***P < .001.
Perceived Feasibility of Implementing Different Components of HRT for Tics In-Person vs Telehealth
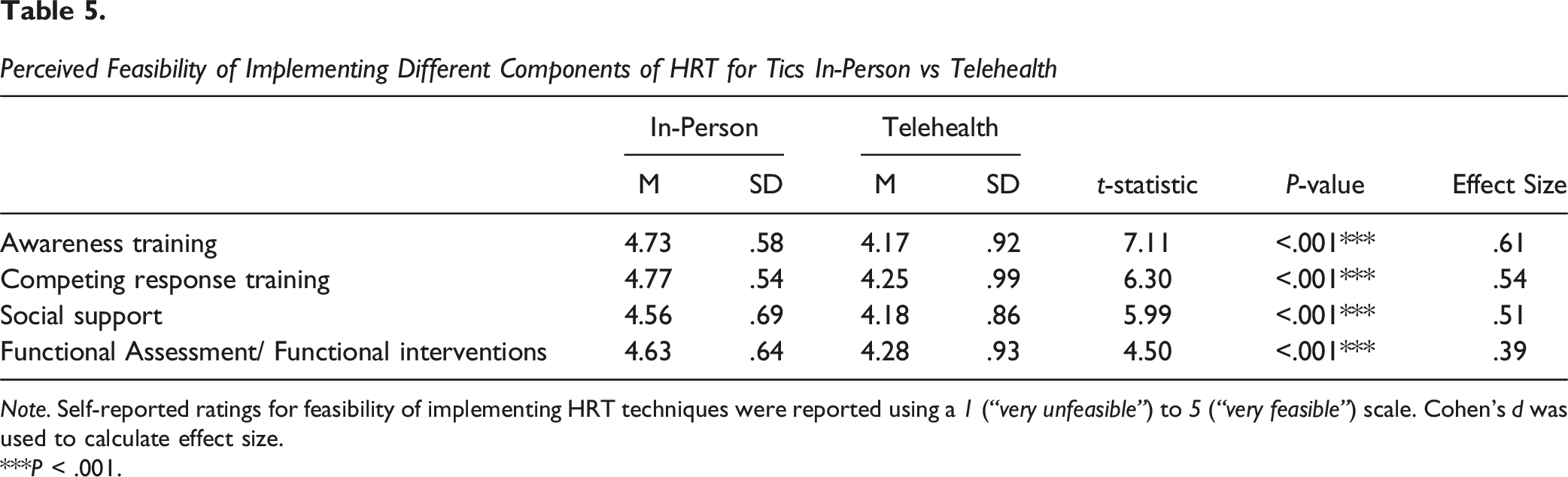
Note. Self-reported ratings for feasibility of implementing HRT techniques were reported using a 1 (“very unfeasible”) to 5 (“very feasible”) scale. Cohen’s d was used to calculate effect size.
***P < .001.
Discussion
In the present study, providers reported perceived feasibility and effectiveness of in-person and telehealth delivery of HRT for tics, as well as patient and environmental factors that may impact treatment feasibility. Compared to the combined mean of the other age ranges, providers reported lower feasibility for telehealth relative to in-person HRT for patients younger than 8 years old, and higher feasibility for telehealth HRT for patients 13-to-17 years old and 18-to-65 years old. There were no differences between groups for 8-to-12-year-olds and patients older than 65. Providers also indicated that telehealth HRT was more feasible for patients with lower levels of tic severity. Further, providers reported greater ability to identify and address therapeutic factors that could impact the delivery of HRT in an in-person environment relative to telehealth. These factors included upper body tics, lower body tics, feedback from patients about the use of competing responses and functional interventions, tic-contingent consequences, intense premonitory urges, non-verbal communication, and delivery of psychoeducational material.
For patient individual differences that may impact HRT delivery, providers reported greater feasibility of implementing in-person vs telehealth HRT for low compared to high cognitive ability, low compared to high treatment motivation, low compared to high awareness of tics, low compared to high family support, and high compared to low anxiety sensitivity. Providers also indicated that in-person compared to telehealth HRT was more effective for simple and complex motor and vocal tics. Providers reported that implementing all components of treatment (ie, functional interventions, awareness training, competing response training, social support) was more feasible in an in-person environment compared to telehealth. Although overall feasibility and effectiveness ratings were high regardless of treatment modality or item assessed, results suggest that when deciding between these treatment modalities, providers should consider several clinical factors (eg, age, tic severity, types of tics).
Despite the fact that there is preliminary support for delivering behavioral treatments for tics (ie, HRT, CBIT) via telehealth,18-21 and there is increasing acceptance and adoption of telehealth behavior therapy in the wake of the COVID-19 pandemic, 45 the present findings suggest there are several therapeutic and patient variables in which in-person treatment may be more feasible and effective. One clinical factor that should be considered is patient age. Providers indicated lower feasibility for telehealth relative to in-person HRT for patients younger than 8 years old, which is consistent with studies examining providers perceptions of treatment for OCD and BFRBs.35,36 Past studies have demonstrated difficulties with building rapport and engaging younger children over video, which may explain the perceived decrease in feasibility.32,34 Further, treatment for tics via telehealth has not been assessed for children younger than 8 years old. Bennett et al 46 demonstrated that an in-person family-based adaptation of CBIT led to significant decreases in tic severity for children 5-8 years old. The treatment used an activity called “The Opposite Game” as a developmentally appropriate way to teach HRT techniques, which may be less feasible to implement via telehealth. Unexpectedly, providers reported no difference in the feasibility of delivering HRT for tics in-person or via telehealth with patients between the ages of 8 and 12. Compared to OCD and BFRBs, tic disorders have an earlier age of onset, as tics typically begin around age 6 and peak in severity at age 10, while mean age of onset of OCD and BFRB symptoms is approximately 10 years old. 2 Thus, tic providers may be more comfortable providing treatment to younger children, which may carry over to treating younger children via telehealth.
Additionally, tic severity is another variable that should be considered when determining the feasibility of treatment via telehealth, as providers reported that telehealth treatment may be less feasible for patients with greater symptom severity. Providers also reported that it was more difficult to identify and address intense premonitory urges, tic-contingent consequences, and patient feedback about the use of competing responses and functional interventions in a telehealth compared to in-person environment. These therapeutic factors tend to be more relevant in patients with greater tic severity, so if clinicians struggle to address them via telehealth, it may lead to more difficulties in delivering telehealth HRT. Therefore, in-person HRT may be more beneficial for patients with greater tic severity; however, future research is needed to determine if these perceptions match empirical data.
There are also several results, with large effect sizes, that suggest provider ability to identify and address tics is more difficult via telehealth. For instance, providers reported that it was significantly more difficult to identify and address lower body tics (eg, leg/foot movements) via telehealth relative to in-person treatment. Providers also reported more difficulty addressing non-verbal communication of tics via telehealth compared to in-person. These results suggest that clinicians may struggle to see certain tics when treatment is provided via telehealth. Indeed, in a systematic review, Connolly et al 31 found that it is more difficult for health care providers to conduct physical and visual examinations of symptoms in telehealth settings. This is particularly relevant for tics, as clinicians may struggle to implement awareness and competing response training via telehealth for discrete tics (eg, stomach tense) or tics that are not visible in typical telehealth set ups (eg, lower body tics). It may also be more difficult to hear certain vocal tics (eg, sniff, grunt) over a video call. Providers visually examine patients’ tics to assist with awareness training and develop a competing response that is physically incompatible with the first movement of the tic. Therefore, it may be more difficult to engage in awareness training and develop an effective competing response via telehealth if the provider’s ability to hear or see the first motion of the tic is decreased. This may be one variable that led providers to report that all components of HRT (ie, awareness training, competing response training, social support) were less feasible over telehealth and that HRT is less effective for all types of tics (ie, simple and complex motor and vocal tics) over telehealth relative to in-person. However, future research is needed to determine if all these factors truly impact the effectiveness of telehealth HRT for tics.
The current study has several limitations. First, the study only examines provider perceptions of in-person vs telehealth HRT, with no direct comparison of treatment outcomes between the two modalities. This is a clear critical area of future research given the recent widespread adoption of telehealth. Although studies have shown preliminary support for telehealth HRT for tics, future research, with larger sample sizes, is needed to determine if certain patient characteristics, such as age-group and tic severity, impact telehealth HRT treatment outcomes. Second, patient perspectives were not evaluated in this study. Future studies could complement the provider perspectives by including patient views of in-person vs telehealth delivery of treatment. Additionally, although providers reported greater effectiveness and feasibility of in-person HRT relative to telehealth, results showed that overall feasibility and effectiveness ratings were high regardless of the treatment modality or item assessed. This indicates that providers believe that both treatment modalities are viable options; however, in-person treatment may still be more optimal for patients with certain clinical factors. Finally, the cross-sectional design of the study is another limitation, as provider ability to deliver telehealth treatment may improve as graduate programs, workshops, and conferences continue to provide additional resources and train providers in telehealth interventions. Patients may also become more comfortable with treatment via telehealth, as they become more familiar with virtual platforms in different facets of life, such as at school and work.
Conclusions
HRT is a first-line treatment for tic disorders, with growing support for the delivery of treatment via telehealth.18-22 In the present study, HRT providers reported several factors that may make the implementation of HRT via telehealth more difficult than in-person treatment for tics. They indicated that telehealth HRT is less feasible for patients under 8 years old and patients with greater tic severity compared to in-person HRT. Providers also found it more difficult to identify and address various patient and treatment factors and less feasible to implement components of HRT over video. These findings are similar to provider perceptions of treatment for BFRBs 36 and OCD. 35 Results do not indicate that in-person HRT is more effective than telehealth HRT, but they suggest that providers should consider the suitability of telehealth HRT for tics depending on patient and treatment factors. To improve treatment for patients with tics, future research should continue to investigate when and for whom telehealth services are appropriate.
Footnotes
Funding
Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under Award Number P50HD103555 for use of the Clinical and Translational Core facilities. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. W.K.G receives a consulting fee from Biohaven, and royalties from Proem, LLC and OCDscales, LLC., and funding from NIH, IOCDF, and McNair Foundation. E.A.S. reports receiving research funding to his institution from the Ream Foundation, International OCD Foundation, and NIH. He was a consultant for Brainsway and Biohaven Pharmaceuticals in the past 12 months. He owns stock less than $5000 in Proem. He receives book royalties from Elsevier, Wiley, Oxford, American Psychological Association, Guildford, Springer, Routledge, and Jessica Kingsley. A.G.G. receives research support from the Misophonia Research Fund and Texas Higher Education Coordinating Board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.