
Abstract
Objective
The Australian Institute of Health and Welfare regularly reports on specialised mental health facilities. Data are available from 1992 to 2022 on public mental health hospital and residential mental health service beds, as well as supported housing and staffing of specialised mental healthcare facilities. We provide a clinical commentary on these reports, reflecting upon the implications for psychiatric practice and patient care.
Conclusions
There are overall trends in public specialised mental health bed numbers. There were substantial declines in public mental health beds that slowed around 2000 and subsequently plateaued in 2015–16 in most jurisdictions with two exceptions, South Australia and the ACT. By contrast, residential mental health service beds increased from 1999 onwards, though since 2015 there have been declines for the ACT, Victoria and Tasmania. For supported housing, most states and territories showed declines in the reported levels since 2002, although there were increases in the Northern Territory, South Australia and Western Australia. From 2009 supported housing rates were relatively stable, with declines in all states and territories from 2015 onwards.
Deinstitutionalisation has significantly shaped mental healthcare delivery in Australia. Its goals were to reduce unnecessary admissions to hospitals, ensure patients were prepared for community living upon discharge, and connect them with community mental health services. 1 This shift was evident in Queensland – used as a proxy model for other states – through two major phases of inpatient reductions. 1 From 1953 to 1963, the ‘opening the back door’ phase focused on discharging patients to community accommodation with psychosocial supports. 1 From 1963 onwards, the ‘closing the back door’ phase aimed to avoid certification and admission, while private hospitals began to emerge – a trend that continues to the present time (see Figure 1 in ref. 1). 1 Crucially, the success or failure of such deinstitutionalisation has relied upon Australian state and territory governments creating a comprehensive system of stepped care and supported housing to replace mental hospital beds, and enable rehabilitation.
Current difficulties in accessing emergency mental healthcare may therefore be due to a shortage of stepped care and public sector specialist beds, as well as residential care and community psychosocial care. 2 Patients experience long waits in busy emergency departments, and brief hospital stays, and/or are discharged to under-resourced community mental health services. 2 There are also exit block issues due to the shortage of supported accommodation. We therefore compare trends in specialised mental healthcare facilities across states and territories during the later second stage of deinstitutionalisation 1 from the early 1990s to when the most recent data are available, in 2022.
The Australian Institute of Health and Welfare (AIHW) regularly publishes data on specialised mental health facilities. We accessed these in September 2024 3 to investigate long-term trends in numbers of public specialised mental health hospital beds, residential mental health service beds and supported housing.
These data are drawn from the National Mental Health Establishments Database, including data from 1992 to 1993, the earliest data collection for that database. 3 ‘The scope of the [database] is all specialised mental health services managed or funded, partially or fully, by state or territory health authorities. Specialised mental health services are those with the primary function of providing treatment, rehabilitation or community health support targeted towards people with a mental disorder or psychiatric disability’. 3 These services provide for those most in need, that is primarily those with severe mental illness, 4 including people with schizophrenia, bipolar disorder and major depressive disorder. 2
To allow for changes in population over long periods, we focused on the rate per 100,000 of population. The data, covering the different timeframes supplied by the AIHW, are displayed in Figures 1–3, reproduced from the AIHW website ‘Spotlight’ Figure 2 on the cited webpage.
3
Public mental health hospital beds. Residential mental health service beds. Supported housing.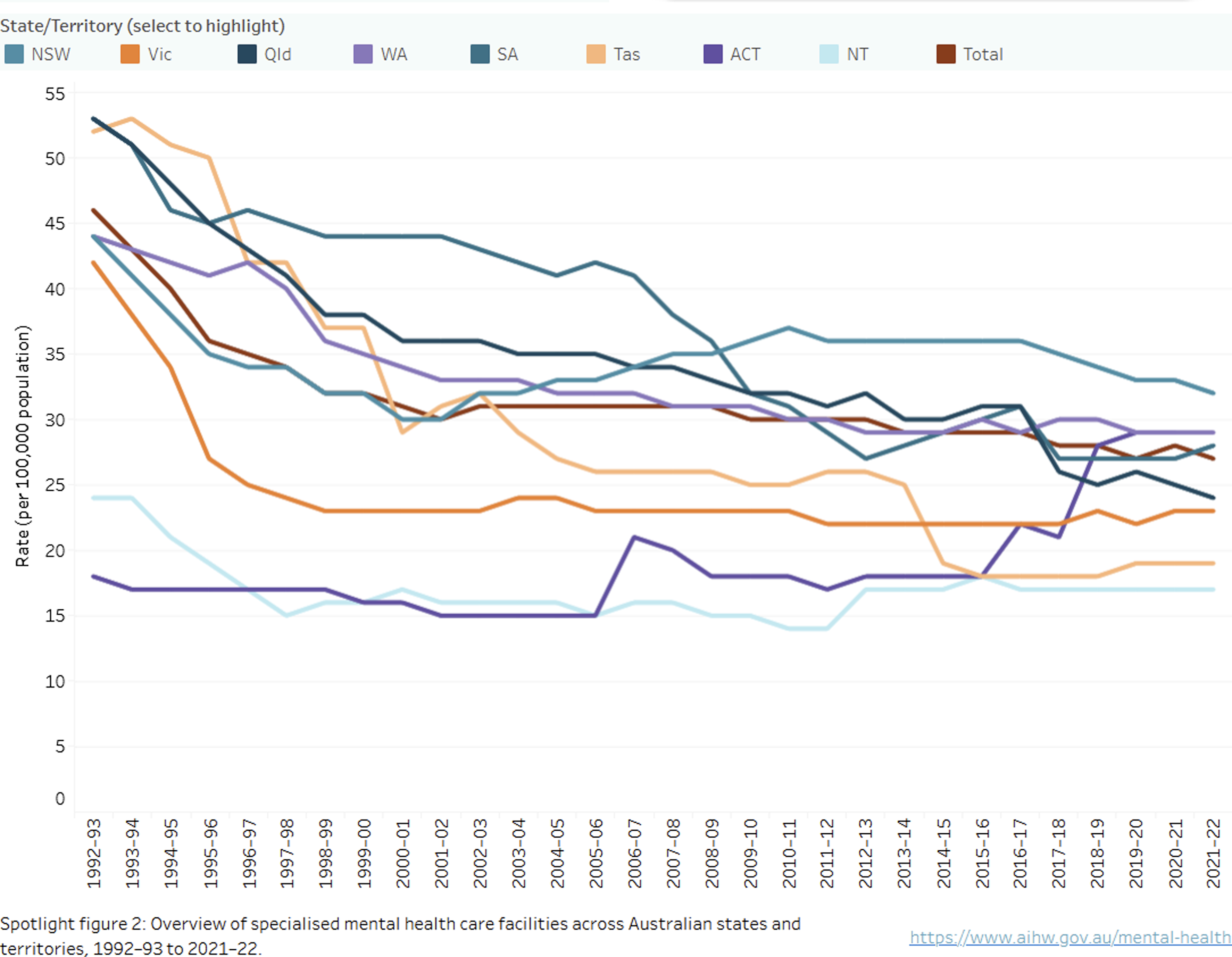
We hypothesised that there may be at least a partial inter-relationship between these three service delivery components. For instance, those needing acute specialised mental healthcare will likely require, in extremis, public mental health beds. They will receive emergency care and be discharged from hospital. For those with a need for step-down care, residential mental health service beds will be required, or alternatively, for lesser illness severity, supported housing. Those with either the best social supports, or the least symptoms, will return home. All three components provide both mental healthcare and accommodation. However, there are other determinants of care outcomes, such as access to (and willingness to engage with) GP and community mental healthcare, that are not measured in the facility dataset.
In this context, relative changes in any of these three components may induce increased demand in others, for example, a decline in hospital beds may increase the need for both residential mental health and supported accommodation beds. We consider the reported data in this light.
Public mental health hospital beds (Figure 1)
The levels of public mental hospital beds ranged from a low of under 20 per 100,000 population in the ACT to just under 55 per 100,000 in South Australia, in 1992–1993. Thereafter, there were substantial declines that slowed around 2000 and plateaued in 2015–16 in most jurisdictions with two exceptions. South Australia continued to decline while, conversely, there was an increase in beds in the ACT. The other states and territories either plateaued or showed small fluctuations in bed numbers from 2015 to 2016. Comparisons with international benchmarks are challenging due to different models of care, definition of bed types and governance. 4
The consequences of plateaus and reductions in bed numbers were demonstrated by a 2014 bed crisis in South Australia with ramping, emergency department access block, and incarceration of those with severe mental illness. 5 These problems were relieved with an increase in bed numbers decompressing the demand. 5 Also these plateaus and small fluctuations were likely to induce demand in residential mental health beds and supported accommodation.
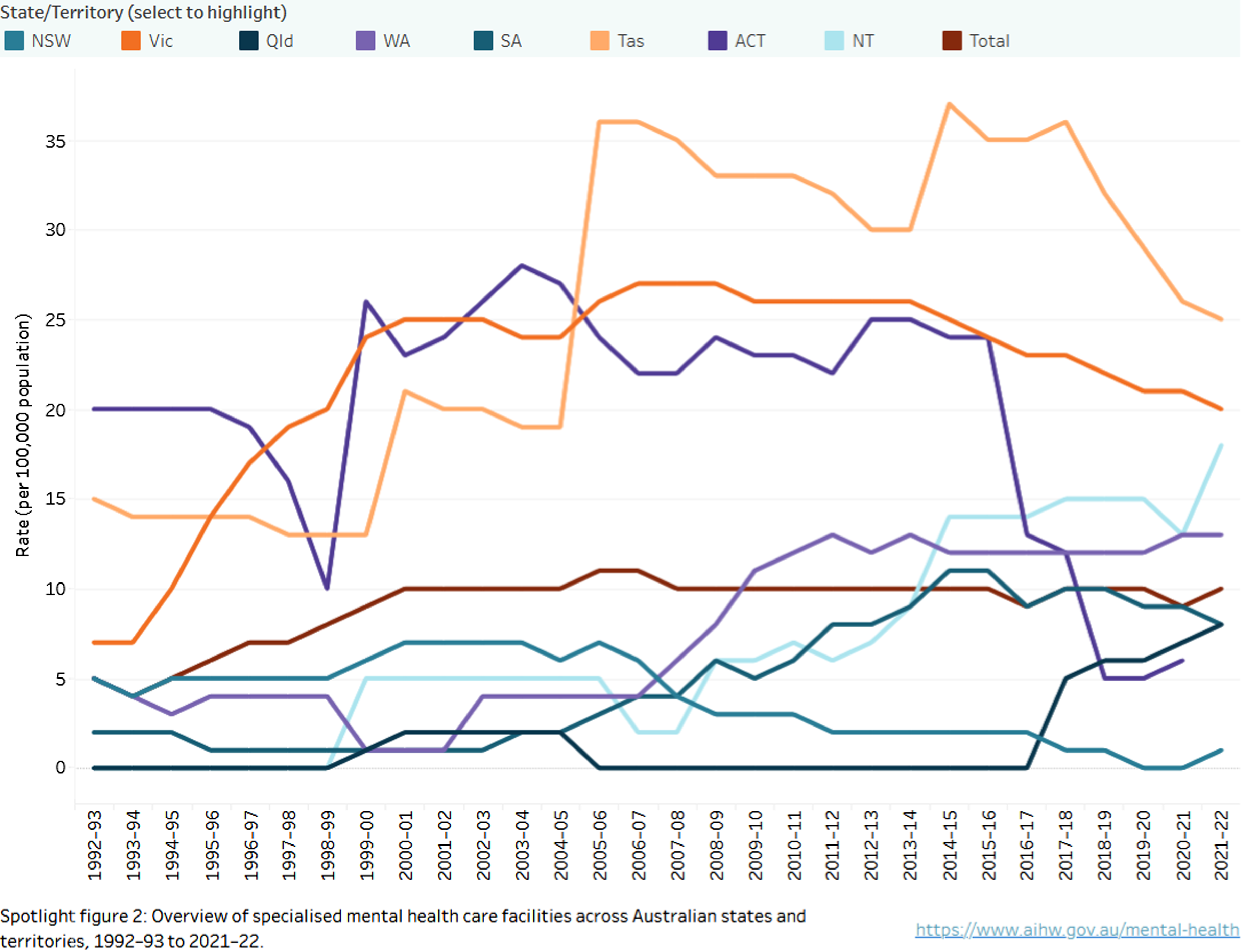
Residential mental health service beds (Figure 2)
At the same time as declining or stagnant bed numbers, there was an increase in residential mental health service beds from the late 1990s in most states and territories although this was followed by a decline in most jurisdictions from 2004 to 2005. The exception was that both Tasmania and the ACT showed marked increases, along with Victoria from 1998 to 1999 through to 2015–16. In the subsequent 2 years there was an apparent decline in numbers although this may have been explained by a reclassification of some beds as falling under the National Disability Insurance Scheme (NDIS). As a result they were out of scope for reporting to the Mental Health Establishments (MHE) Database. 3
Notwithstanding the impact of reclassification due to the NDIS, the relative increases in residential mental health beds should ensure that more patients receive step-down care on discharge from acute hospital beds. However, length of occupancy may be a particularly relevant factor, for if some more severely ill patients occupy these residential beds long-term, there may still be limited capacity for discharge from hospital to residential care. Therefore, data on length of stay in residential mental health beds would be useful, and could be complemented by the data from the National Mental Health Performance Framework on acute hospital length of stay, as in previous research. 6 It would be useful for AIHW to collect separate data for 24-h residential beds that provide patients with about 2 weeks length of stay post-acute phase as distinct from 24-h residential beds that provide several months of accommodation. 7
By international benchmarks, the rate per 100,000 of residential mental health beds remains somewhat low, as do the overall specialised public hospital beds.4,8 The relatively low-resourcing of these capacities will then flow on to increase demand in supported housing.
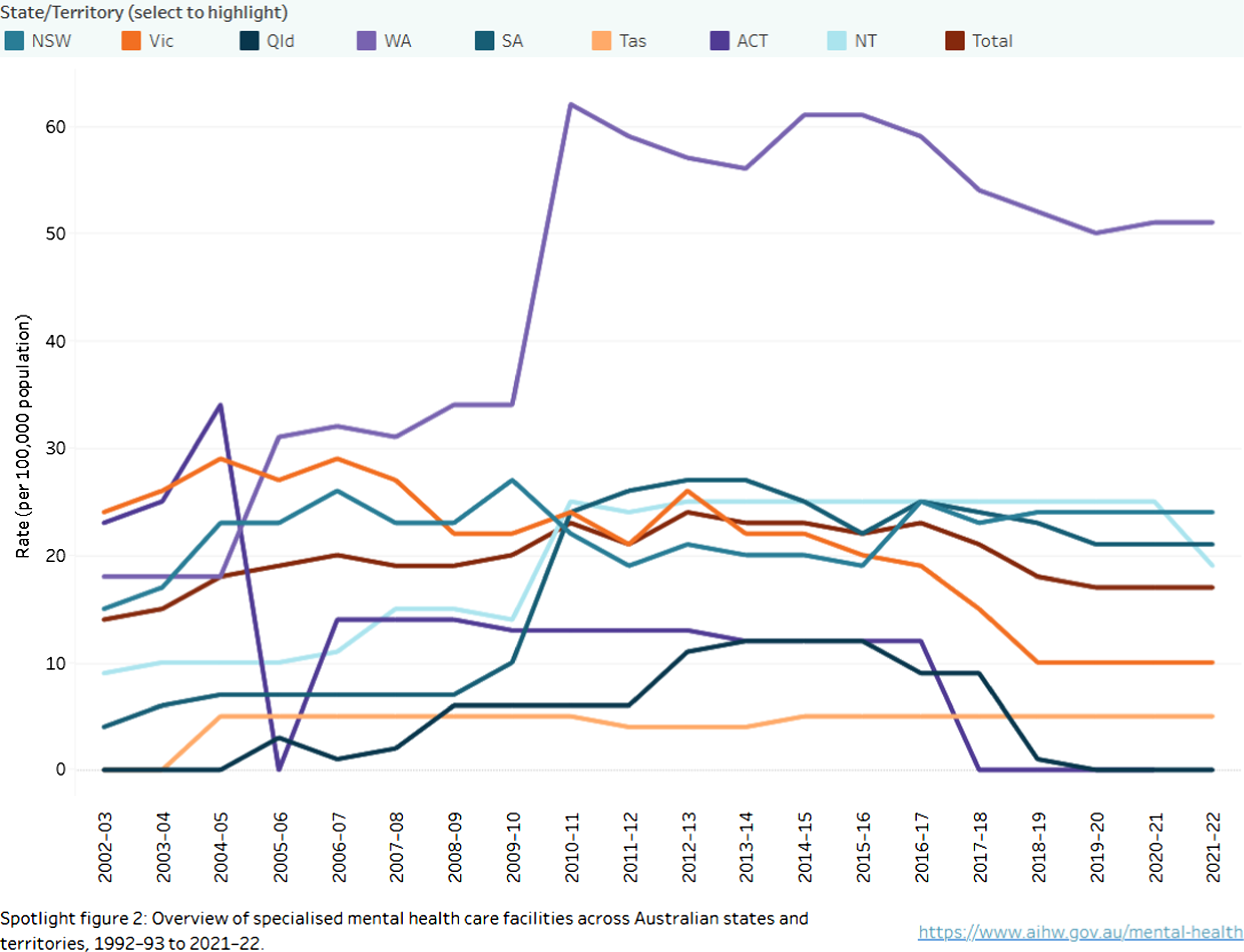
Supported housing (Figure 3)
Overall, across most states and territories supported housing levels remained steady, until a decline from 2015 to 2016, which, based on the AIHW explanation for Figure 2, may also have resulted from changes in funding due to the NDIS. It is notable that Western Australia has consistently the highest levels of supported housing, approaching 60 per 100,000 since a marked increase in 2009–2010, though there has also been a decline since 2015–2016, perhaps again due to the NDIS changes.
Relative declines in supported housing are concerning in that this may detract from support to help patients discharged from acute care to stabilise and improve their mental health. ‘Homeless’ people who are ‘couch-surfing’ or who are living on the street may be more difficult to provide housing for, unless there is assertive community mental healthcare follow-up, 9 which in turn is challenging due to their itinerant living conditions. A recent systematic review found that supported housing was of limited overall efficacy in improving health in the general homeless population (i.e. not those previously identified as mentally ill), and mainly improved anxiety and depressive symptoms. 10 Another systematic review on mental illness and homeless indicates that specific psychosocial interventions are necessary to improve outcomes, such as provision of skills training, assertive community mental healthcare and specific housing support. 11
Discussion
These data on state and territory mental health facilities give some insight into trends in the delivery of healthcare in Australia; especially during the later phase of deinstitutionalisation that aimed to avoid unnecessary admissions. 1 The key framing consideration is that the components of bed infrastructure that provide the base of hospital care for unavoidable admissions are to a lesser or greater degree interdependent. However, bed types are not fully interchangeable and deficits in acute, non-acute or residential beds might increase waiting times for admission throughout the system. The relative stasis or decline of hospital bed numbers may be inadequate for unavoidable severe mental illness patient needs, depending on lengths of stay and the effectiveness of hospital treatment. 2 Lesser capacity then is likely to result in a less resilient system of care, especially if there are surges of demand. A possible result of these generally stagnant levels might be increased demand for residential mental health beds or supported accommodation.
However, while the overall increases in specialised residential mental health beds are reassuring, they appear low by international standards and there may be challenges in smaller states and territories where there is limited capacity. In addition, the general decline in supported housing stock, except in Western Australia, raises the spectre of homelessness, particularly amongst the most severely ill. Further study is needed into whether this is a true decline or due to cost-shifting from states and territories to the NDIS.
Limitations
Statistical indicators such as these offer limited information without an understanding of how mental health services are provided in Australia, which includes the models of care, infrastructure and staffing. For instance, these data do not cover community mental healthcare, primary care, supported housing, carer and family support and access to disability support/welfare. We have also not been able to provide a trend diagnostic breakdown, which may reveal changing diagnostic-related bed utilisation and supported accommodation requirements. There are also those with severe mental illness who receive care in the private sector, such as through private hospitals and these data are not represented in the AIHW reporting we comment upon. The ACT did not report some data for 2021–2022.
A future broader systemic view of mental health service provision and psychosocial care could be achieved through the further development of research-based models using other databases and modelling, such as the Medicare Benefits Schedule. These models could be considered in the context of the National Mental Health Service Planning Framework, although this tool is not currently publicly available.
Conclusions
Sixty years of deinstitutionalisation in Australia have resulted in, unwelcome consequences for patients with a systemic reliance on short acute admissions and varying access to non-acute rehabilitation and supported residential care in states and territories. 2 Potential recommendations include improved planning of services focused on patient care journeys, that encompass hospital beds, residential mental health beds, supported accommodation, workforce, as well as adequacy of primary and community healthcare in states and territories. This includes not just ensuring adequate capacity, but also an optimisation of communication and operational cohesion between these components. Further research is also needed into the capacity of private sector services to complement the assessments of public sector service capacity in states and territories. Finally, quality of care, as assessed by key performance indicators, in the National Mental Health Performance Framework (NMHPF) is also essential to interpret if capacity is effective or not. And if there is commensurate sufficiency in community mental healthcare, there should be limited hospital readmissions; this could be explored in the NMHPF data which should be made public to judge the relative performance of state and territory systems.
Footnotes
Ethical considerations
No ethics approval or consent was required as this paper does not involve research with humans or animals.
Author contributions
All authors have satisfied: Substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: JCLL, SA, TB, SK and PAM are all members of the journal editorial team – they were not involved in editorial handling or peer review of this paper. This paper was independently peer-reviewed.