
Abstract
Objective
To examine the risks and benefits associated with tapering and ceasing antipsychotic medication after treatment for psychotic illness.
Method
Narrative synthesis of major guidelines and meta-analyses, landmark trials and recent randomised controlled trials (RCTs).
Results
(1) Maintenance is consistently protective against relapse and associated harms in the first 1 to 2 years of illness. (2) Some evidence suggests long-term functional benefits from reduction in dose or medication discontinuation, but findings are inconsistent and of low certainty. (3) Relapse after abrupt cessation is common, often within 3 months, possibly due to dopaminergic super-sensitivity. (4) Hyperbolic tapering, with slow and progressively smaller dose reductions, may reduce withdrawal effects and relapse risk. Clinical features associated with safer tapering included sustained remission, insight, absence of substance use, strong social support and access to rapid review.
Conclusion
Deprescribing is not universally safe, but a structured, gradual and reversible approach is consistent with ethical and patient-centred treatment, and in a small proportion of patients is not followed by relapse. Clinicians should emphasise shared decision-making, hyperbolic tapering and robust relapse-prevention strategies.
Introduction
The recent Coronial inquest into the Sydney shopping-centre stabbing by a man who had tapered and ceased antipsychotic medication under supervision, and had then been lost to follow-up, highlighted the risks of stopping treatment and the need for reliable, evidence-based deprescribing advice. 1 Although catastrophic outcomes are rare, with homicide of strangers by people with schizophrenia estimated to be around 1 per 14 million people per year, 2 the Coroner’s findings highlighted the need for structured tapering and dependable follow-up whenever deprescribing is considered.
Antipsychotic medications that act by blocking dopamine receptors remain the cornerstone of schizophrenia treatment, reducing acute symptoms and halving relapse risk in the years after onset. 3 However, long-term exposure can have significant negative effects, including metabolic syndrome, cardiovascular disease, tardive dyskinesia, emotional blunting, subjective dysphoria and possible structural brain changes. 4 Many patients, especially younger or more recently diagnosed patients, ask if they can reduce or stop medication, and without clear advice may abruptly do so, heightening relapse risk. Another important group is those who do not recognise they have been unwell and disagree with the need for treatment. Both groups illustrate the clinician’s dilemma: respecting autonomy and minimising long-term harms while preventing relapse.
This dilemma raises the questions of who can safely reduce and cease antipsychotic medication, and how tapering should be conducted. This Clinical Update reviews current guidelines, recent trials, biological evidence and ethical considerations to provide practical advice for prescribers. Although a narrative review is suitable for integrating guideline recommendations and heterogeneous data, it lacks the reproducible search strategy and quantitative synthesis of more structured review methods.
With regard to the terminology used in this paper, remission generally refers to sustained low levels of positive symptoms, while relapse denotes the re-emergence of positive symptoms requiring intervention. These constructs capture only part of schizophrenia symptomatology, as negative, cognitive and functional domains are not included. Recovery describes broader symptomatic and functional improvement compatible with living independently and social participation. Tapering refers to a planned, stepwise reduction in dose. Dose reduction denotes lowering the maintenance dose without intending cessation. Deprescribing refers to clinician-guided reduction or cessation. Discontinuation refers to complete cessation, whether planned or unplanned.
Long-term prognosis and recovery
Kraepelin’s view of schizophrenia as an inevitably deteriorating condition was modified by Bleuler, who recognised the heterogeneity of psychotic disorders and their long-term outcomes. Long-term outcome data is mostly derived from cohorts diagnosed with schizophrenia rather than heterogeneous first-episode psychosis samples. Reported outcomes and recovery rates in FEP vary and have been influenced by diagnostic evolution, and cautious antipsychotic reduction may help clarify the trajectory of illness after an initial psychotic episode.
A systematic review of outcomes after 20 years reported that about a quarter (24%) recovered, a third (36%) had good or better outcomes and nearly two-thirds (60%) had moderate or better outcomes; 40% had a poor outcome
5
(Figure 1). The outcome categories are hierarchical rather than mutually exclusive, which is why the percentages exceed 100% when summed (e.g. ‘good or better’ includes those who also meet criteria for ‘recovery’). These findings came from naturalistic studies, in which most participants received antipsychotic treatment, although exposure varied. Because higher attrition was linked to more favourable outcomes, the authors conducted a worst-case sensitivity analysis assuming all dropouts had poor outcomes. Under this assumption, recovery fell to 13%, good or better outcomes to 22% and moderate or better outcomes to 38%, while 62% were classified as having a poor outcome. Long-term outcomes in schizophrenia over more than 20 years Data shown for the main analysis and an attrition-adjusted (worst-case) analysis. Dark grey = main analysis; light grey = attrition-adjusted (worst case). Percentages represent the proportion of individuals achieving each outcome category. Data derived from Molstrøm et al. (2022).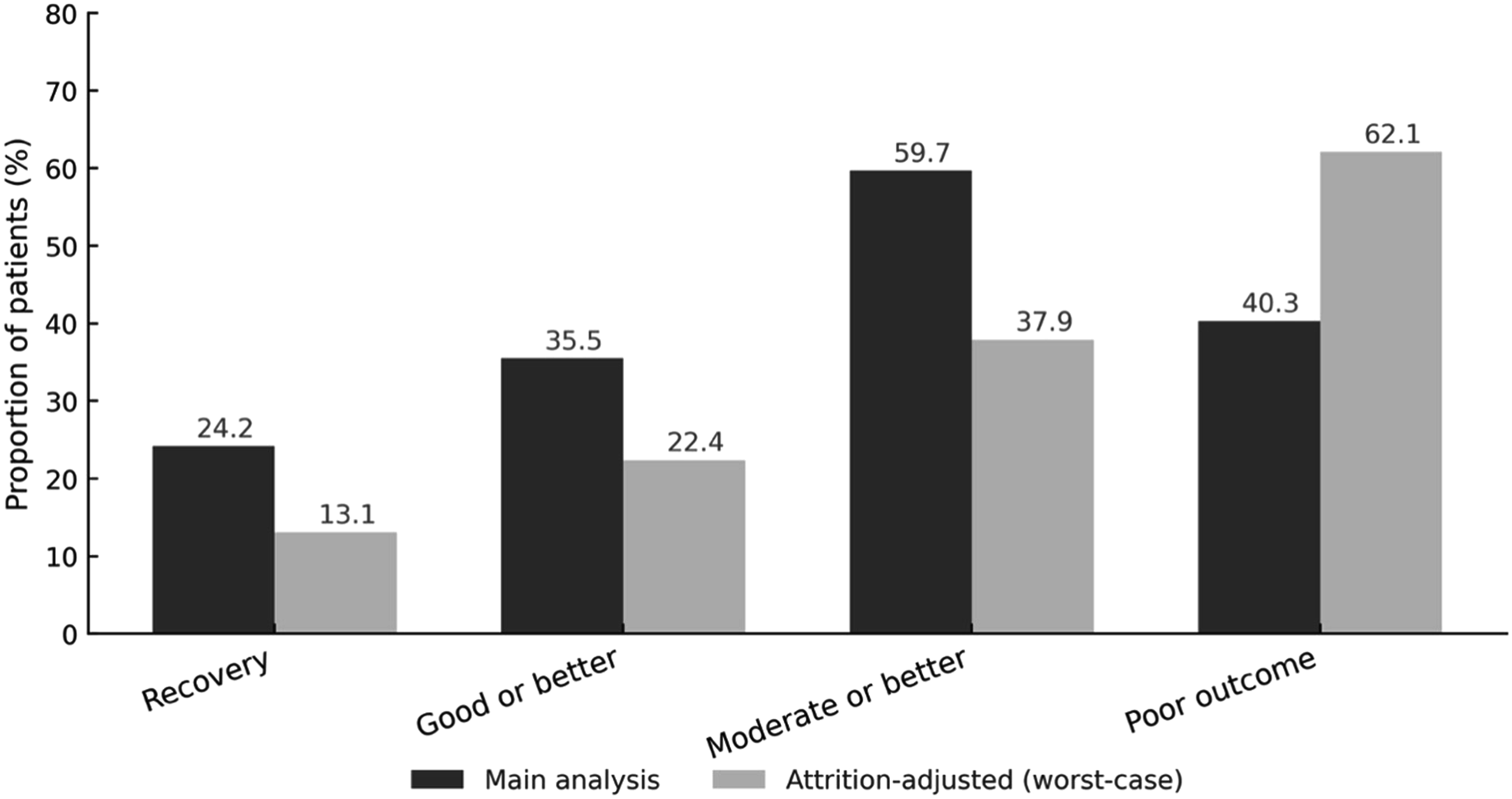
Time-dependent effects of antipsychotic medication discontinuation
A 2023 meta-analysis of 35 studies of patients followed up for up to 15 years found no overall difference in social function or quality of life between discontinuation and maintenance. 6 Time-dependent analyses suggested that while maintenance was superior in the first 2 years, discontinuation was associated with significantly better social function at both medium-term (2–5 years) and long-term (>5 years). Relapse risk, however, was consistently higher in those who stopped medication. Interpretation of these apparent long-term benefits is limited by the obvious bias that less severely unwell patients were the ones who were able to stop treatment, and the overall quality of evidence was rated as very low.
Existing guidelines
Guidelines for the treatment of schizophrenia emphasise the maintenance of antipsychotic medication during early remission. The 2014 National Institute for Health and Clinical Excellence (NICE CG178) noted the high likelihood of relapse but recommends that if tapering is to be attempted, the dose should be reduced gradually and patients monitored for at least 2 years after cessation. 7 The American Psychiatric Association (APA) guidelines from 2020 strongly favour maintenance but allow individualised deprescribing where adverse effects are severe, or motivation is high and supports are in place. 8 The Maudsley Prescribing Guidelines endorse cautious tapering and cessation of antipsychotic medication as ‘good practice’ but suggest at least 6 months’ remission before tapering in first-episode cases and 12 months in multi-episode illness. 9 The RANZCP guidelines from 2016 recommended that antipsychotic reduction only be considered after sustained recovery and conducted under medical supervision. 10
All the current guidelines agree that if deprescribing is to be attempted, taper should be slow, closely monitored and reversible.
Controlled trials of antipsychotic discontinuation
The Hong Kong trial by Hui and colleagues of first-episode psychosis (FEP) patients randomised to maintenance or discontinuation soon after remission found that at 10 years, 39% of the discontinuation group had poor clinical outcomes (persistent psychosis, treatment resistance or suicide) compared with 21% of those maintained on treatment. 11 Only 16% remained positive-symptom free, similar to recovery rates in meta-analysis, 5 indicating that sustained drug-free maintenance is possible but uncommon. Predictors of successful discontinuation included being male, shorter duration of untreated psychosis, better social function, non-schizophrenia diagnoses and fewer relapses. 12
In the Netherlands, Wunderink randomised remitted FEP patients after 6 months of treatment to maintenance or guided dose-reduction/discontinuation. At 2 years, relapse was higher in the reduction arm (43% vs 21%). 13 However, at 7 years the reduction group had twice the rate of functional recovery (40% vs 18%), defined by functional rather than symptomatic remission. 14 Critics noted unequal diagnostic distribution, high attrition, the conflation of dose reduction and discontinuation, and that most participants received some antipsychotic exposure over time. 10
Several large RCTs in the past decade have attempted to address limitations of the Hui and Wunderink studies, using structured tapering, relapse-prevention strategies and broader outcome measures. The UK RADAR trial is the largest tapering study in chronic or recurrent psychotic disorders, predominantly established schizophrenia (SCZ). Of 4157 screened, 253 were enrolled (126 guided reduction; 127 maintenance). The reduction group followed gradual, individualised tapers over 12–18 months. At 24 months there was no difference in symptoms, social function, employment or quality of life, but relapse was more common (severe 25% vs 13%; any relapse 41% vs 22%), and side-effects were modestly lower. Overall, among patients with more than one psychotic episode, slow dose reduction increased relapse risk over 2 years without functional gain. 15
The Danish multicentre TAILOR trial allocated early psychosis (FEP) patients in remission for at least 3 months to maintenance or a slow taper. The primary outcome was sustained remission without antipsychotic medication at 1 year. Of 225 screened, 29 were enrolled due to strict eligibility and low willingness to participate. Relapse rates were similar (14% taper vs 20% maintenance) with few adverse events, but low recruitment meant the trial was only able to demonstrate that slow tapering is feasible and acceptable in highly selected FEP patients. 16
The Taiwanese GARMED trial evaluated a structured clinician-guided reduction algorithm in 97 adults with schizophrenia-spectrum psychosis (SCZ), with 76 randomised and 21 in naturalistic maintenance. Over 2 years, relapse rates did not differ between guided reduction and maintenance, and about three-quarters remained well on lower doses. One-third achieved substantial reductions (nearly 60%), with clinical and quality-of-life improvements. 17
The HAMLETT study in the Netherlands recruited 347 FEP patients from 24 centres who had achieved remission after 3–6 months’ treatment, randomised to guided dose reduction within 12 months or at least 1 year of maintenance. 18 The primary outcome was World Health Organization Disability Assessment Schedule (WHO-DAS) function at 4 years. There was no difference in WHO-DAS scores, but the reduction arm showed higher relapse risk in the first year (OR 2.84, 95% CI: 1.08–7.66), lower quality of life, but better researcher-rated global assessment of functioning (GAF) from year three. A further analysis of 227 participants who tapered found that antipsychotic D2 receptor affinity, not tapering speed, predicted relapse: 46% relapsed within 18 months, and users of high-affinity D2 antagonists had roughly twice the relapse risk and shorter time to relapse than those on low-affinity antagonists or partial agonists. 19 These findings suggest antipsychotic pharmacodynamics play a greater role than tapering rate in determining relapse after first-episode remission.
Key trials of antipsychotic dose reduction and discontinuation.

Abbreviations: FEP: first-episode psychosis; WHO-DAS 2.0: World Health Organization Disability Assessment Schedule 2.0.
Mechanisms of functional benefit
Several mechanisms may explain functional improvement with lower antipsychotic exposure. Excessive dopamine D2 receptor blockade (beyond 65–70% occupancy) has been associated with reduced affective range and dysphoria, whereas doses that keep receptor occupancy within a therapeutic window might reduce these adverse effects. Because dopamine signalling is also critical for cognitive flexibility, attention and learning, maintaining adequate rather than excessive receptor occupancy can help preserve cognitive performance. In addition, mesolimbic dopamine activity underpins motivation and goal-directed behaviour, so avoiding unnecessary blockade may improve drive and social engagement. 20
Neurobiology of antipsychotic medication tapering
Chronic blockade of D2 and D3 receptors can result in receptor super-sensitivity, and PET and clinical data support increased dopaminergic responsivity after long-term treatment. 21 Abrupt cessation can precipitate withdrawal-related psychosis that may be hard to distinguish from illness relapse, which might have the effect of inflating ‘relapse’ rates in discontinuation arms of some trials, compared to those of more recent studies that emphasise slow, patient-specific tapering of doses with close monitoring of the effect of dose reductions.
Dose–receptor occupancy follows a hyperbolic curve, especially for antipsychotic medications with high affinity for dopamine receptors, so that proportional dose reductions do not necessarily translate into equal physiological changes. 20 Proportional reductions (10–25% of the current dose every 8–12 weeks) could better approximate the hyperbolic-dose occupancy relationship, and at very low doses lower receptor occupancy, reductions should slow further, with the option to pause or increase doses if symptoms re-emerge.
Features associated with safer antipsychotic tapering
Features thought to favour safer tapering include sustained remission for over a year, few prior relapses, good premorbid function, preserved insight, adherence, absence of substance use, strong family support and access to rapid clinical review (Box 1 and 2).12,22 These features are derived from observational analyses and post hoc subgroup findings, largely in first-episode samples, and should be regarded as signals rather than validated predictors of safe antipsychotic reduction. A diagnosis of established schizophrenia, particularly with a relapsing course, is associated with poorer outcomes following dose reduction or discontinuation compared with FEP populations.5,11,14,15 As such, findings from FEP studies should not be extrapolated without careful consideration to people with established schizophrenia. No scoring tool or checklist reliably identifies ‘good candidates’, and existing studies are heterogeneous in cohort type, definitions of remission and follow-up duration (Box 3).
23
Clinical vignette. Practical tapering pathway. Ethical, legal and service considerations in antipsychotic discontinuation.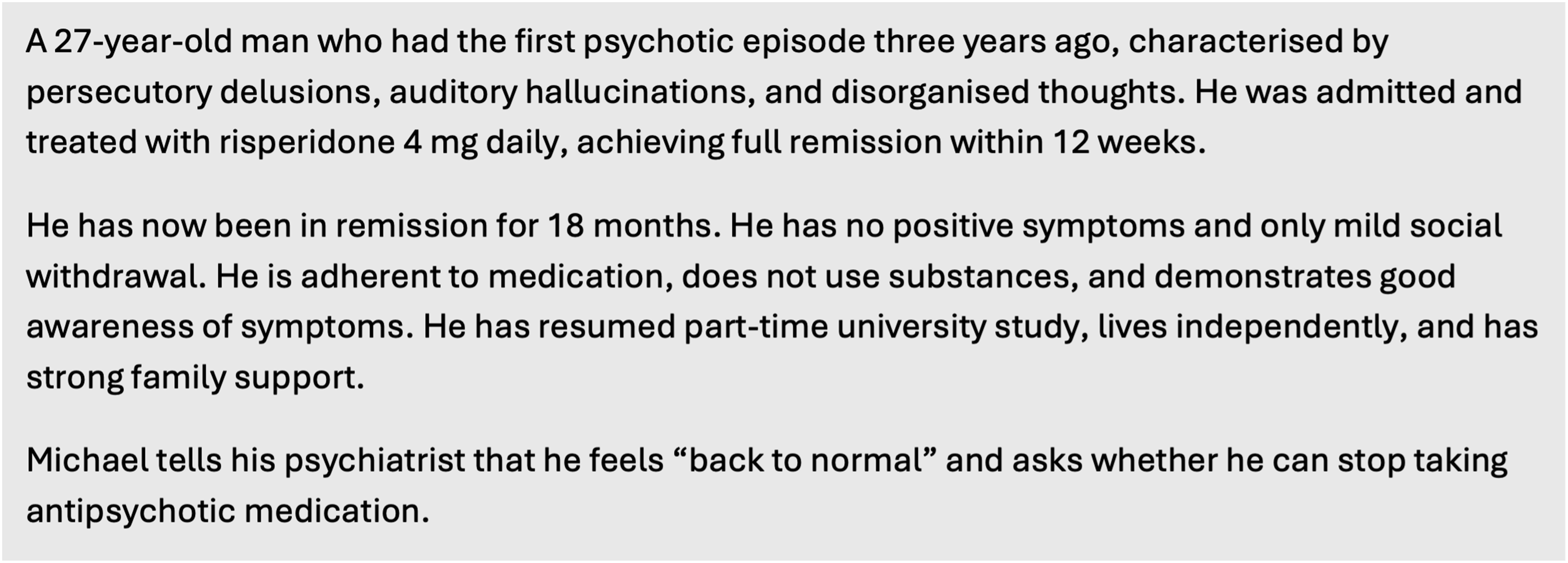


Conclusion
The risk of relapse in the short term is consistently elevated, and evidence for long-term functional benefits from withdrawing antipsychotic medication is limited and inconclusive. However, there are clear advantages in reduced side effects and improved quality of life, and the natural course of schizophrenia is that a proportion of people who are diagnosed with the condition achieve sustained recovery without treatment. Some early relapse might be due to dopamine receptor sensitivity. Given the high risk of relapse, a cautious, proportionate and reversible approach to tapering, supported by close monitoring and relapse-prevention strategies, is recommended.
Footnotes
Ethical considerations
This study is a narrative synthesis of previously published literature. Ethical approval was not required as no primary data were collected and no identifiable patient information was used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.