
Abstract
In September 2025, I accepted an invitation to speak at Professor Gordon Parker’s Festschrift. This paper reflects on some of the topics I expounded upon in my presentation. When executed properly, debating involves skilful and erudite critique, for which Gordon’s marvellous mind is innately suited. Therefore, in this paper, I argue that this seemingly innate ability has contributed to his success in argumentation as well as his penchant for entertaining academic discourse. To illustrate this, I retrace an ongoing debate that he and I have had over the past two decades that concerns the validity of subtyping bipolar disorder. Gordon is the quintessential academic gladiator as he never cowers and seldom crows. Consequently, his contributions to the field of mood disorders have been phenomenal and time and again he has proven that he is a true champion. Hence, it is a pleasure to celebrate him and his achievements.
Where to begin, but from Gordon’s Gin, A story so bold you’ll blush and grin, But when all is said and all has been done, You’ll be mighty glad coz you’ll have had fun, So please dear reader, read on below, Raise the curtains, begin the show … ‘…if you can’t annoy somebody, there’s little point in writing…’ Kingsley Amis (1922-1995).
Apéritif: or ‘a pair of teef’?
At Gordon’s Festschrift in September of 2025, pretending not to be familiar with the purpose of the occasion, I jested that Gordon had asked me to attend his ‘celebratory function’ because he regarded me an essential accoutrement to his fetish. Although clearly a joke, there was a grain of truth in this remark – albeit tangential – in that, over the years his appetite for the publication of papers and books as well as the research that has relentlessly fed this ‘habit’ has been a form of intellectual gratification for Gordon that is no doubt at least in some ways on par with his other desires. 1
Gordon’s port-folio
As anyone who knows Gordon would already know, his collective works include countless scientific publications, textbooks, seminars and presentations, as well as more accessible material for the lay public. Surprisingly and somewhat less well-known is the fact that Gordon has also published fictional works, again including books but also plays that have graced the stage, and on top of this he is also a dab hand at impromptu speaking, which again anyone in the know, knows only too well, requires both courage and skill. Consequently, appraising the entirety of his scholarly accomplishments is beyond the scope of an aperçu such as this, and so I have focused on his debating skills and in particular his proclivity for argumentation. To my mind, this is perhaps the most important of Gordon’s many literary skills, but it is also important because it is a form of ‘cerebral calisthenics’ that is sadly on the decline, particularly in psychiatry, where arguably (no pun intended) it is needed most. However, before delving into the specifics of one of the many debates he has partaken in, it is necessary to understand the terms involved in the business of disputation.
Shaken, not stirred
In essence, argumentation is the sum of the various activities and practices that entail the exchange and communication of arguments. Informally, this is often referred to as debate or discourse and ‘an argument’ refers straightforwardly to a structured statement in which some components referred to as ‘the premises’ offer support to another part of the same statement namely, ‘the conclusion’. This holds for both written and spoken arguments, where essentially one is asserting a proposition in favour of a particular outcome and the basic concept is that the person arguing a point is attempting to prove their particular point of view.
When arguing against Gordon, one is immediately at a disadvantage. This is because Gordon’s marvellous mental apparatus is engineered, nay, fine-tuned for intellectual jousting and consequently, oftentimes his mind machinates or muses mellifluously – seemingly spontaneously and without sweating so to speak. On top of this, when preparing for a debate his whole demeanour begins to embody the spirit of an argument. Indeed, even in day-to-day interactions with Gordon, I would often observe that while engaged in routine tasks he would be actively exercising his telencephalon – wrestling with a problem which often involved trying to prove something. Surprisingly, the result of such intense ‘gyral grappling’ and ‘frontal frotteurism’ would usually be the genesis of a splendid idea. In my view, such cerebration to develop arguments and the process of argumentation are critical, especially in our speciality of psychiatry where disagreement and uncertainty permeate every aspect of its practice.
Philosophically, argumentation can be thought of as a process of dialogue and through the exchange of reasons and ideas there is a sharpening of collective understanding as clarification is sought. It entails an openness to and acceptance of learning from each other, and the process provides a critical mechanism to understand our experience and the world around us. Over the years I have known Gordon, this is one of the things that have impressed me most. In this collective and occasionally collaborative quest for the truth, Gordon has time and again shown his innate ability to see things differently, and it is this unique mindset that has been the basis of much of the intellectual parrying and repartee between him and others over the years. With respect to our interactions, I realised early on that like myself, Gordon not only liked the English language and playing with words, but that he also enjoyed creating new ideas. For example, many of the titles of his papers skew the spelling or meaning of words or exploit their sounds, such as ‘ADDing up?’, a comment on the increase in prevalence of attention-deficit disorder (ADD), 1 and ‘Journeying with a bipolar disorder: The quest plot’, an article born of Gordon’s ability for conceptual amalgamation on the prescience that sometimes occurs in mania and drives behaviour in bipolar disorder 2 ; this penchant for wordsmithing was also reflected in our exchanges over the years when debating both in conferences and in the pages of international journals, for instance, ‘Bipolar II disorder: once missed, now dismissed, time to resist’. 3
Often in arguments, people will retort by stating that ‘this is just semantics’, suggesting that by being technical about the meaning of a word or phrase, the person is missing the point. But semantics do matter. Indeed, without meaning, words are useless and so trying to ascertain the meaning of words, phrases, ideas and concepts, I would argue, is the very substance and life blood of psychiatry. This clearly manifests in Gordon’s work. For instance, he was never satisfied with the DSM classification of major depressive disorder, a checklist descriptor that lacks specificity. He often referred to it disparagingly as a ‘shopping list’, meaning that it had no rhyme or reason. To my mind, his criticisms of DSM depression are wholly correct and many of the problems with diagnosis and the treatment of depression stem from a simple failure to describe the clinical entity accurately in the first place. His definition of melancholia and the separation of melancholia from the many nonspecific descriptions of clinical depression have value. 4 Nevertheless, the division of depression into melancholia and the somewhat maladroit term, non-melancholic depression, led to this approach being applied to bipolar disorder, and while I wholeheartedly agreed with Gordon when he was fighting valiantly as a medieval knight against new world ideology for recognition of heterogeneity in the field of depression, I could no longer in good conscience serve as his armiger when the fight manoeuvred to the ills within the bipolar hills. It is here, when embarking on the emotional cartography of the Himalayas of mood, that we parted ways and our debate truly began.
Approaching the lectern, to begin my talk as part of Gordon’s Festschrift, celebrating his achievements as Herr Parker, né Gordon, ‘the professor who professeth too much’, I experienced a flashback to a simpler time, 40 years ago when as a medical student at Manchester University I was called upon by the late Professor David Goldberg, later Sir, in his introductory lecture to the clinical psychiatry module to answer a question. In my response, I quoted from his book and David was delighted, and that first impression lasted and resulted in valuable mentorship throughout my subsequent training and career. A decade or so later, my first encounter with Gordon was similar, in that we immediately bonded over a self-referent joke as I gifted him a bottle of ‘Gordon’s London Dry Gin’, having recently arrived from the capital of England a few days earlier to take up a lecturer role in the Department of Psychiatry of which Gordon was the Head and undeniably the ‘supreme god emperor’.
Beginnings are important, and so I began my talk at Gordon’s Festschrift with a tongue-in-cheek quip to emphasise that while it is necessary to celebrate Gordon’s exceptional academic achievements, it is equally important to acknowledge that unlike many in psychiatry he is exceptional because he is a fully rounded person, on top of which he has a robust sense of humour. Indeed, it is partly because of his ability to laugh at matters and my tendency to jest that we have been able to debate and argue and at times robustly, and yet still maintain a dialogue and a meaningful relationship.
On the rocks
Like Gordon, I have learnt that one should take any and every opportunity to espouse one’s views especially if they contribute to an ongoing colloquy, and hence why even a Festschrift is fair game provided any criticism is offset by cajolery and the overall effect is that one fares well but not at the expense of one’s oppugner. A key controversy that remains unsettled to this day – an unsettling fact for a settler such as myself – is the question of whether bipolar disorder can be subtyped into bipolar I and bipolar II (see Figure 1). (A). The debate within the Australian and New Zealand Journal of Psychiatry (ANZJP) Volume 55 Issue 6 regarding the status of Bipolar II9,10. (B). Reproduced from the debate in Figure 1A: Comparisons between proposed models for the classification of bipolar disorder. The schematic illustrates the different criteria used by DSM-5 (left), those proposed by Parker (centre) and those proposed by Malhi (right) to define bipolar disorders. Each model uses different criteria to inform classification, with DSM-5 relying on duration and Parker employing symptoms to subtype bipolar disorder, and Malhi utilising severity as a dimensional proxy. DSM-5 uses minimum duration criteria to specify bipolar II (4 days of manic symptoms) and bipolar I (7 days of manic symptoms), but it also includes a category of hypomania with insufficient symptoms (with the addition of a major depressive episode), and short-duration cyclothymia, which entails subsyndromal mood symptoms over multiple episodes. Parker’s proposal, which focuses on symptoms, loosely maintains the minimum of 4 days duration criterion for hypomania as outlined in DSM, but relies more specifically on the presence of psychosis of any duration to delineate bipolar I from bipolar II. Finally, Malhi uses the three domains of Activity (green), Cognition (blue) and Emotion (red), which constitute the ACE model to identify symptoms and gauge their severity (modelled dimensionally) and to define the presence of mania or mixed episodes; this model also accommodates mixed features and subsyndromal symptoms. In addition, psychotic symptoms are depicted in a separate domain that runs alongside manic symptoms. These can feature at any time and at any level of impairment/change in functioning and are not necessarily a defining feature of the disorder per se. Broadly speaking, the longer symptoms last the greater the impairment and change in functioning they are likely to cause; however, this is a loose association as opposed to a tight correlation, and hence, the three measures are represented along the x-axes separately.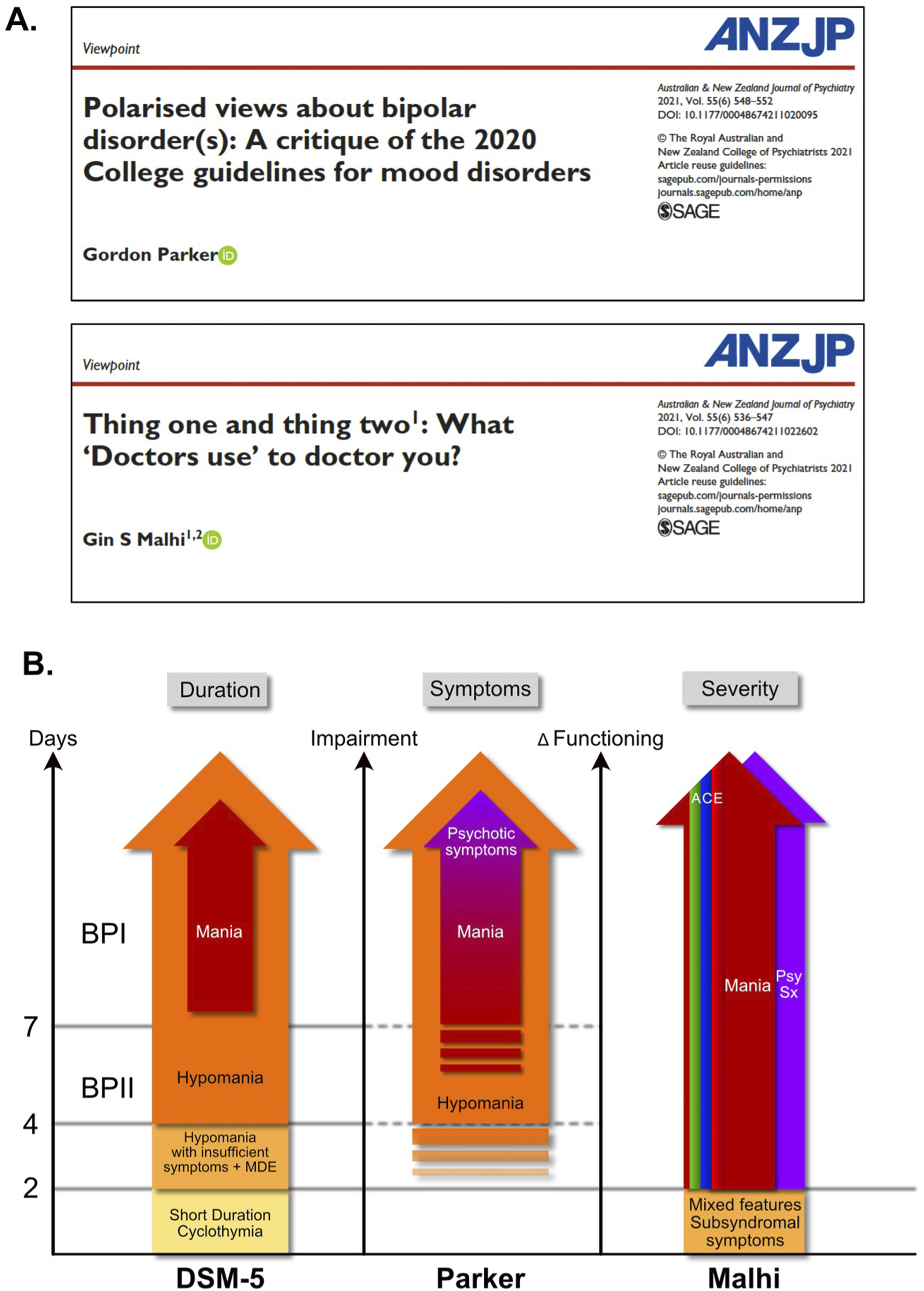
Gordon’s view, which I politely refer to as the ‘bifurcatory perspective’, is that there are two types of bipolar disorder, one defined by manic symptoms and psychosis, and the other by a lesser degree of mania and the absence of psychotic symptoms. Gordon himself did not approve of the use of ‘hospitalisation’ to differentiate the subtypes, possibly one of the most absurd criteria in DSM-5, and that’s quite an achievement given that the manual also contains the mythical disruptive mood dysregulation disorder (DMDD) 5 – a diagnosis so remarkably preposterous that it warrants an interrobang.
Ironically, my opposition to bipolar II was twofold. First, there is no evidence for what Gordon himself often described as ‘a break’, or ‘a step’ in the continuum of illness severity, be it based on the number of symptoms, functional impairment or some other biomarker or parameter that coincides with the illusory line drawn between bipolar I and II by DSM-5. In other words, there is no evidence for any distinction, and this is the basis for my second objection to the bifurcation of bipolarity, as these purported subtypes lack treatment specificity and virtually all the same treatments are used for both bipolar I and II. In practice, the diagnosis of bipolar II has caused immense confusion because lesser degrees of severity of bipolar disorder necessarily appear similar to traits of personality dysfunction and aspects of substance misuse, and nowadays the multifarious forms of unclear diagnostic designations such as ADHD. In other words, while I understand why David Dunner 6 and others wanted to further define and refine the diagnosis of bipolar disorder, the division they created has not found any firm footing, and in my view given what we know now, it never will, and this is problematic because it cannot provide diagnostic precision or meaningfully inform management.
I first shared my concerns about bipolar II disorder with Gordon when he asked me to write a chapter in his book on its neurobiology. 7 When, after extensive research, I concluded that there was little to no pathophysiological evidence to support a biological basis for the subtype, he included my chapter but did so reluctantly. Further, when a few years later the book was being updated for its second edition, I learnt that I had not been invited to contribute, and so when the book was finally published, I alluded to this curious oversight in a lecture that I gave where Gordon was in attendance. Then, when preparing for the third edition of the same text, maybe out of contrition or simply because he wanted to be inclusive, he invited me to write a commentary 8 ; perhaps he thought I had changed my mind. However, once again I articulated my doubts and put forward my objections both about the validity of the construct and the potential risks therein; suffice to say, Gordon was not amused.9,10
Brandy-shing blandishments
In amongst this bookish back and forth, Gordon and I also had a more scholastic discussion in the pages of the Australian and New Zealand Journal of Psychiatry (ANZJP), a journal that both he and I have managed as editors-in-chief. Our Viewpoints9,10 captured our respective arguments and were published together (see Figure 1(A)), and regardless of which side of the debate you fall, I recommend reading both of them as they provide an insight into the complexity of delineating the ontology of psychiatric conditions. In addition, I also recommend digesting Gordon’s Bryson-esque rebuttal in which, true to form, he tried to have an easy win, arguing that given the journal is called Bipolar Disorders, ‘to demonstrate congruence, consistency of view and rationality, then Gin (as Editor of “Bipolar Disorders”) should immediately rename this journal, while as President of the “International Society for Bipolar Disorders” he should also bring singular status to its naming’. Gordon’s cunning came as no surprise as he had previously used humour to sway opinion when he quoted the lauded French painter Georges Braque who said that ‘two ideas are always needed: one to kill the other’. Suffice to say his plurality argument that there are more than one kind of disorder, that is, I and II, because they are referred to as bipolar disorders carried little weight, and as I stated in my article quoting Harper Lee (author of To Kill a Mockingbird), ‘there’s just one kind of folks. Folks’. To my mind, ‘bipolar disorders’ refers to the many individuals who are sadly affected by the illness and it is not plural because there are more than one kind of disorder.
Last orders
There is no way of doing justice to this or any of the arguments that Gordon has ever mounted, but it is important to once again iterate that not everyone is capable of seeing beyond the dispute itself as he always has. And that despite the many exchanges and ongoing scientific disagreements, I have never felt anything other than respect and admiration for Gordon, and though I do not always agree with his viewpoint, I am always prepared to stand next to him and share the view as we point to different events on the horizon – fleeting glimmering concepts – beyond which lies the enormous abyss into which we cannot as yet see. What is evident however, and palpably so, is the indelible impact that Gordon has made on the field – on par with many of the leading figures in psychiatry, and the lasting impression he has made on individuals through mentorship and support – not to mention the many patients that have benefitted from his wisdom. I for one will forever be in his debt, and though I will likely continue to disagree with him on aspects of mood disorders, I cannot help but find that we agree on most things, and that mostly he is most agreeable.
Footnotes
Acknowledgments
The views presented in this manuscript are solely those of the author (GSM) and do not reflect the views of any organization or institution or any committee that GSM serves on. No AI software has been used in the preparation of this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
G.S.M. serves as an Advisor to the Editor-in-Chief of Australasian Psychiatry. He did not take part in the assessment of this article. He is also the Editor-in-Chief of The British Journal of Psychiatry and the College Editor for the Royal College of Psychiatrists and has previously served as the Editor-in-Chief of the Australian and New Zealand Journal of Psychiatry. He currently receives funding from Wellcome (UK) for GALENOS, and is the lead researcher on an investigator-initiated study (PoET) that is supported by Janssen-Cilag. In the past he has received grant funding or research support from the American Foundation for Suicide Prevention, the National Health and Medical Research Council, Australian Rotary Health, NSW Health, Ramsay Research and Teaching Fund, and The North Foundation, as well as the University of Sydney and National Taiwan University as part of an Ignition Grant. In the past he has also received grant funding from AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier; and has on occasion been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier.