
Abstract
Recent tragic deaths alleged to have arisen from the unauthorised departures of involuntarily detained individuals at Cumberland hospital highlight weaknesses in mental health service provision in New South Wales and beyond. These events occur in the context of the mass resignation of psychiatrists over quality and safety of public mental healthcare in NSW. Overall resourcing of health professionals and infrastructure remains parlous. New South Wales has dropped to the lowest expenditure per capita on public mental health services, according to the AIHW, and needs to invest considerably more to reach the national average and remedy fundamental systemic weaknesses. There remains a need for systemic reform to provide integrated hospital and community care, as well as supported accommodation and welfare for people with severe mental illness.
The recent failure of a patient to return from leave from Cumberland Hospital, in NSW, on Sunday 22 February 2026, may itself seem quotidian. 1 However, it occurs in the context of the alleged stabbing of three people, and subsequent death of two, by another individual who had absconded from Cumberland 10 days previously. 2 A third patient who had absconded earlier in the same month was allegedly involved in a fatal car accident, in which two people died. 1 Although Cumberland Hospital has provided specialised care for people with severe mental illness (SMI) for many decades, these episodes raise concerns over the current human capital and infrastructure for public mental healthcare and the State’s ability to organise major reforms.
These events occur against the background of the mass resignation of public mental health sector psychiatrists in early 2025, 3 even though some have since returned following a temporary 1-year pay award. Yet, as these recent episodes demonstrate, access to psychiatric expertise is only part of the solution to decades of under-resourcing and policy-making neglect. 4
A recent ABC report quotes Dr Anuradha Kataria, who had resigned from Cumberland after 23 years, observing: ‘We’re taking the highest-risk patients and clumping them together in a small space with not a lot to do, very limited resources to look after them’. 5 In the same report, NSW Nurses and Midwives Association’s Cumberland branch delegate, Teaghanne Sarina, stated: ‘We’ve been requesting extra resources, extra pay, extra people on the floor’, and ‘We would be better able to manage, better able to behaviourally de-escalate’. 5 The lack of security staff to support nurses and other health workers has also been reported by the ABC, with more frequent absconding, once every 1333 days, from Cumberland than the average of once every 4348 days for all NSW public mental health facilities. 5 In the same ABC report on Cumberland Hospital, there is an anonymised personal account by a patient’s sister who stated: ‘They’re very good at masking their symptoms … I don’t believe a 2-week admission is enough to actually observe somebody’. And ‘It’s a terrible place to be in. I would fight black and blue to get her out of that place’. 5
Such observations exemplify some of the ongoing impacts of inadequate staffing and lack of bed capacity on the quality of care, leading to shorter admissions and less personalised care. Even before the pandemic, the suboptimal working conditions of public mental health services were evident. 6 A recent national survey of psychiatrists highlighted that working conditions had actually worsened in both public and private sectors due to widespread burnout as a result of workforce shortages and increasing workload. 7
These recent critical incidents and the under-resourcing context in which they occur are the legacy of decades of neglect. However, they also reflect wider factors in society, such as rising methamphetamine use and associated crime that is driving an influx of patients to mental health wards who are diverted by the lower courts in NSW. 8 This is not a trend that should be criticised, as flooding jails with such individuals who need mental health care would be a terrible outcome. However, it is abundantly clear that mental health units are buckling under the pressure of rising admissions of individuals who are at times extremely difficult to manage, with a dearth of resourcing of security staff. 5
Constant pricing data for 2023–2024 from the AIHW show that per capita, NSW expends the least on state-funded mental health services (Figure 1).
9
NSW needs to re-join the rest of the country by reaching at least the Australian average on per capita investment. State and Territory constant price expenditure per capita on Mental Health Services from 2014–2015 to 2023–2024. Notes. Constant prices are adjusted for inflation. There was no reported data for the Australian Capital Territory from 2020–2021 to 2023–2024. Based on Australian Institute of Health and Welfare material from: https://www.aihw.gov.au/mental-health/topic-areas/facilities-resources/expenditure.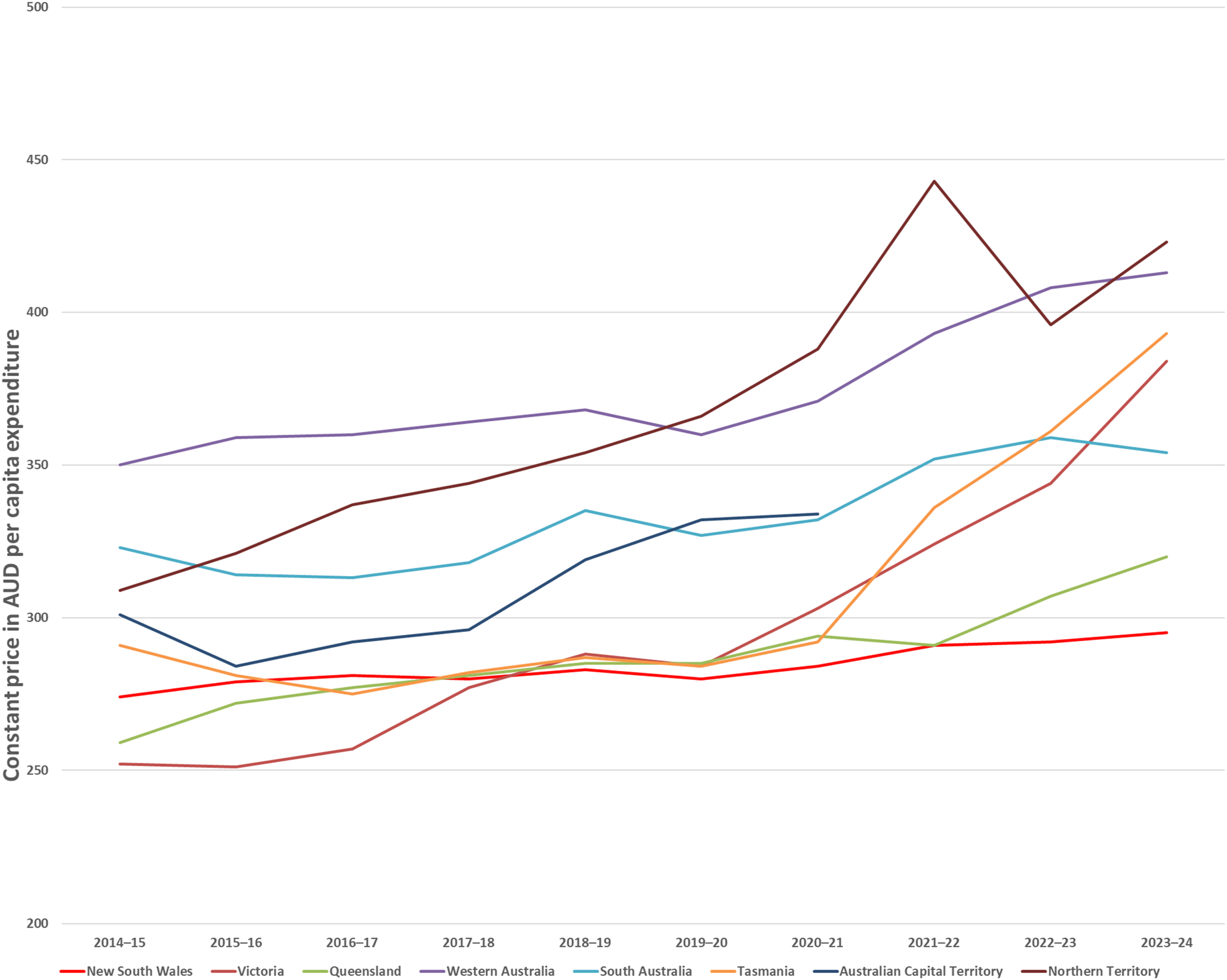
Systemic reform and resourcing are necessary for repair to provide safe and effective public mental health services to avert further incidents arising from shortfalls in the care of people with SMI. 10 It is also necessary to examine and address the downstream drivers of rising admissions to mental health wards amid dire funding for services such as drug and alcohol rehabilitation. There are three main immediate areas of reform needed: health professional, infrastructure and adaptive system redesign. The central focus of reform should be to provide integrated public mental healthcare that supports the entire patient journey, but also encompasses infrastructure for long-term supported care and living in the community. This is underpinned by comprehensive community mental healthcare services that outreach to provide short- and long-term care to those with severe mental illness, for day-to-day support and crisis.
Community mental healthcare must not be delivered in isolation, but, instead, link patients to their general practitioner, broader social services, supported accommodation, drug and alcohol rehabilitation services and longer-term housing. The closer integration of these community services can facilitate the transition to acute mental health hospital when needed in emergent circumstances, and support of transfer to community healthcare upon discharge, including supported accommodation as needed.
This requires a renewed focus on people with SMI including substantial investment and ongoing funding in the provision of staffing, hospital and related infrastructure, as well as social support and housing, as outlined in a white paper from the Australian National University and The Australian in 2024. 11
Yet, despite substantial media reporting and ongoing critical incidents beyond Cumberland Hospital such as at Bondi Junction, 12 there remains a lack of effective political will and action, even following the mass resignations of psychiatrists from the NSW public mental health system over quality of care and safety concerns. 13
The concern over a lack of action has continued into 2026 with further unrest at Concord Hospital over the lack of senior medical, nursing and allied health staffing, as quoted by The Australian: ‘My view is that the resignations of the psychiatrists actually was part of a systemic problem throughout NSW Health – it could have been any specialty body’, ‘Concord was the epicentre of the psychiatry resignations. But there has been no inquiry. Nothing has changed’. 14
Unless the systemic failings of state-provided public healthcare, especially mental healthcare, are addressed with determined action – more lives may be lost. Political responses to date have characterised by denial, 15 victimisation of those who raise issues and what appear to be efforts to suppress raising of concerns on quality and safety in public healthcare.16,17
The incidents at Cumberland are indicators of broader systemic challenges within public health services–challenges for which evidence-based solutions exist, but for which sufficient political commitment has yet to materialise. Public reporting, supported by an independent press, can enable a greater visibility of these issues. To generate the political impetus required for reform, transparent communication through the media and collective advocacy by healthcare professionals, such as those at Concord and Cumberland Hospitals, remain critical for improving patient outcomes, community safety and preventing further system deterioration.
Footnotes
Author contributions
All authors have made substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics and consent
No ethics approval or consent was required as this paper does not involve research with humans or animals.
Conflict of Interest
Commissioned editorial. This paper reflects the views of the authors, not the journal or any other organisation that the authors are affiliated with.
CRediT taxonomy
Jeffrey C.L. Looi: conceptualisation, investigation, methodology, project administration, writing – original draft and writing – reviewing & editing.
Stephen Allison: conceptualisation and writing – reviewing and editing.
Tarun Bastiampillai: conceptualisation and writing – reviewing and editing.
Steve Kisely: conceptualisation and writing – reviewing and editing.
Natasha Robinson: conceptualisation and writing – reviewing and editing.
Stephen Robson: conceptualisation and writing – reviewing and editing.