
Abstract
Background
Medical schools are essential in promoting psychiatry as an appealing career, especially amid workforce shortages and prevailing negative perceptions that deter interest in the field. Research suggests that increasing mentorship opportunities and access to enrichment programs and electives can significantly improve attitudes towards psychiatry, encouraging more to consider it as a career path.
Objective
To reflect on an Australian medical student’s experience in the Perspectives of Psychiatry Program for International Learners (PoPPIL) at Johns Hopkins University School of Medicine, demonstrating how the program, based on its structured multi-perspective framework, serves as an example of an enrichment activity that aligns with these recommendations.
Conclusion
The PoPPIL serves as a compelling model for integrating enrichment activities and mentorship within psychiatric education. Participants engage in discourse-driven learning, encouraging reflection on diagnostic formulations and explication of inherent reasoning processes. By establishing its foundations on an adaptable, conceptually sound framework, the PoPPIL aims to facilitate the development of psychiatrists who are holistic and integrative in their daily practice. Integrating educational opportunities such as these into Australia’s psychiatric curricula may prove advantageous for future generations.
Keywords
Medical schools are essential in promoting psychiatry as an appealing and relevant career choice, 1 especially amid workforce shortages 2 and persistent negative perceptions1,3,4 that deter interest from this field. Research has shown that developing strategies to increase high-quality teaching, positive clinical experiences and access to enrichment activities can significantly improve medical students’ attitudes towards psychiatry, encouraging some to consider it as a career path.3,5,6 Therefore as the field evolves, so must the methods used to educate future clinicians, requiring an integrated revised psychiatric curriculum that is clinically relevant 7 and scientifically rigorous8–10 whilst expanding access to specialised programs and mentorship.3,5,6 This paper reflects on an Australian medical student’s experience in the Perspectives of Psychiatry Program for International Learners (PoPPIL), an example of a program that facilitates enrichment activities and quality mentorship. 11
Program overview
McHugh and Slavney argue that the heart of effective psychiatric education is a strong conceptually sound structure that provides a coherent framework for both teaching and learning. 10 Without this, students may struggle to connect different pieces of knowledge, resulting in confusion and an incomplete understanding of psychiatric practice. 12 This led them to develop the Perspectives of Psychiatry (PoP) which has underpinned psychiatric education at Johns Hopkins University School of Medicine since the 1980s. The PoP provides a structured and nuanced framework for diagnostic formulation, explicating what is implicit in contemporary psychiatric practice whilst promoting interdisciplinary collaboration and research.13,14
Following this, the Perspectives of Psychiatry Program for International Learners (PoPPIL) 11 was established in 2024 to provide undergraduate and graduate learners from varying national and cultural contexts the opportunity to experience the practical application of the PoP framework and has hosted learners from Europe, Australia and South America since its launch. 11 During the month-long program, participants will grasp an understanding of the PoP framework in different contexts including adult inpatient units, subspeciality outpatient clinics, consult-liaison attachments whilst joining in lectures and case-based tutorials known as ‘service rounds’. Supplemental online curricula and resources are also accessible for all PoPPIL participants with optional scholarship and mentorship opportunities available for select learners.
The Perspectives of Psychiatry (PoP)
The PoP incorporates four primary perspectives – disease, dimensional, behaviour and life story
13
– each offering a different lens to view psychiatric disorders. These are derived from the four proposed fundamental, interactive and functional features of the mind that represent the compositional attributes structuring conscious psychological life Figure 1. Components, disorders and treatments (CDT) of the Perspectives.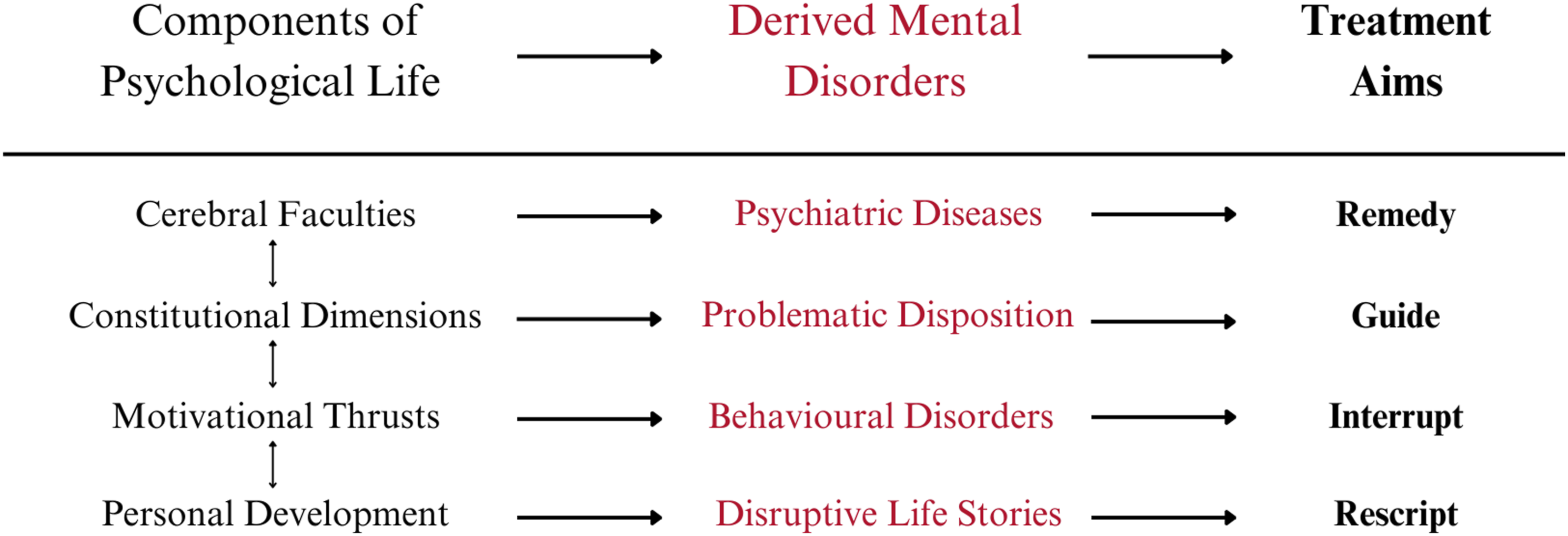
The ‘Disease’ perspective describes how neurobiological pathologies can disrupt intrinsic features (e.g. consciousness, memory, language, cognition and affect), resulting in the reported and observable symptomology in a patient. 13 When all three elements of the conceptual triad are elucidated, treatments based on a causal link between aetiology, brain pathology and clinical syndromes become possible. An example of this is dementia, a global cognitive decline in the absence of delirium, usually due to the loss of brain tissue as a result of various aetiologies (e.g. Alzheimer’s disease or traumatic brain injury).
The ‘Dimensional’ perspective considers how one’s self-defining features (e.g. intelligence, temperament and maturity) predispose them to developing distress in certain situations. 13 When these aspects of an individual are leveraged successfully, it can result in successes in life that may not be previously believed possible. 15 Consequently, treatment consists of helping the patient recognise and accept who they are and their predispositions, whilst subsequently guiding them to adapt by noticing, anticipating, managing and avoiding (if appropriate) circumstances that provoke distress. 13
The ‘Behavioural’ perspective describes how classical and operant conditioning of innate physiological drives, acquired drives and overvalued ideas can lead to psychiatric conditions such as anorexia nervosa, sexual paraphilias, substance use disorders and conversion disorders. 13 Treatment begins with interrupting the maladaptive behaviour whilst systematically limiting exposure to rewards, punishments, or influences that may encourage the pathological behaviour. 16
The ‘Life Story’ perspective focuses on the extrinsic and experiential features of the mind (e.g. childhood development, significant life events, social networks, education and culture) that generate distress, resulting in grief, demoralisation or post-traumatic stress disorders. Stories don’t necessarily discover the truth but propose one that is fitting with the significance and implications of an individual’s emotions. Thus, treatment is achieved through rescripting a patient’s personal narrative to one that is more beneficial whilst enabling self-determination and the ability to regain control of their life and future.13,15,17 Figure 2. The four Perspectives of Psychiatry.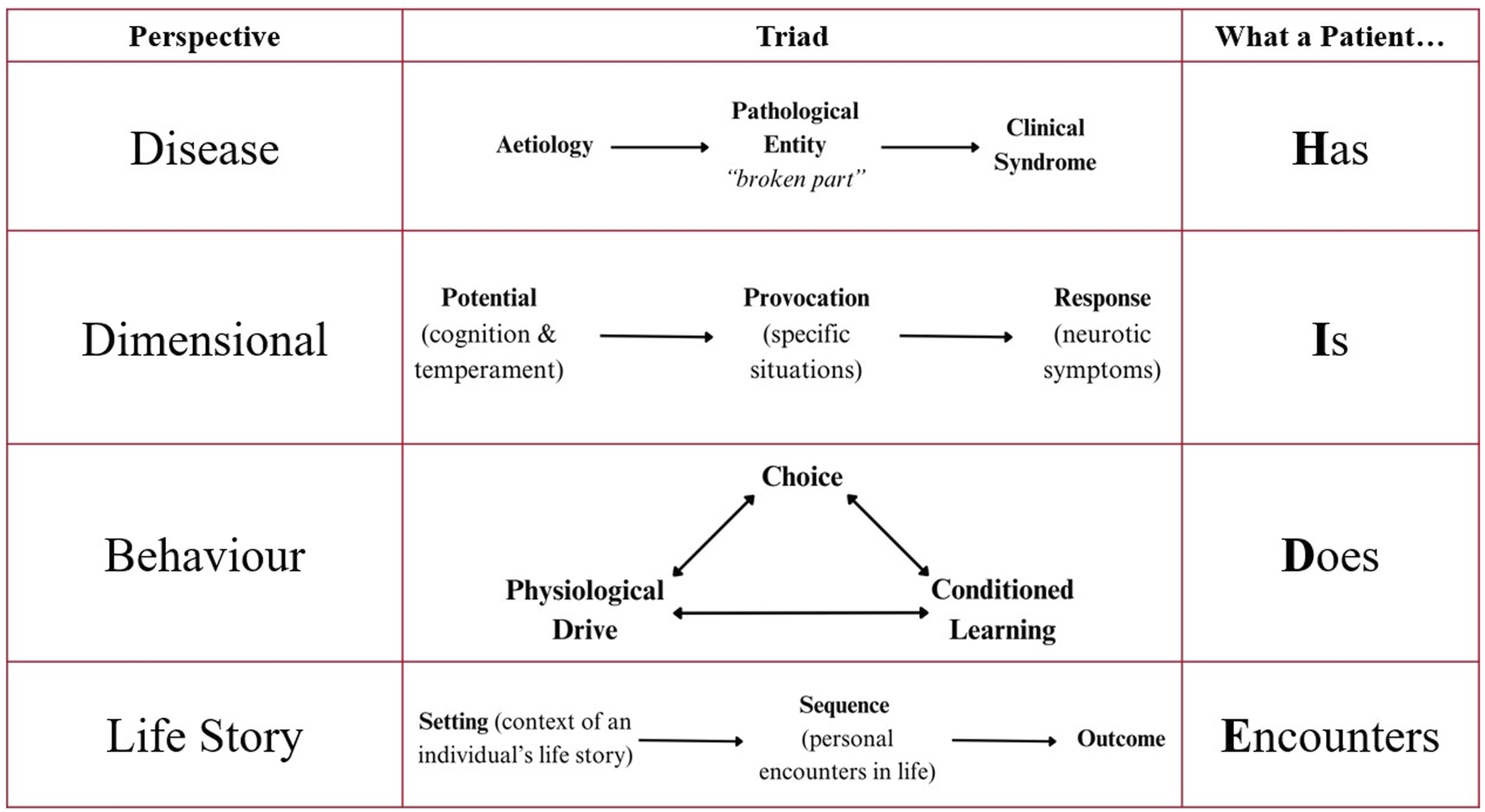
Together, this framework provides a standardised, structured, efficient, integrated and comprehensive system to diagnostic formulation which enables learners to develop a coherent and nuanced understanding of psychiatric disorders. In my experience, although the four perspectives can be intermingled in formulating a clinical presentation, each depends on distinct explanatory pathways. Any perspective can be chosen to explain a patient’s presentation but once a choice is made, it always presents a set of demands that extend from the patient to a defence of the choice itself. I found that once these implicit distinctions were made more explicit, I could then clarify my presumptions and formulation so that everyone, especially patients and their families, can be placed on more equal ground. This empowers them to ask questions about my underlying assumptions, thought processes and treatment plans, enabling them to contribute more discerningly in their own recovery.15,18
It also encourages the holistic consideration of a patient which promotes the creation of management plans that not only address their psychiatric symptoms but also their social needs and personal goals. 16 I believe in Australia, this would further improve the integration of mental health care plans into effective collaboration with services such as Centrelink, NDIS, Departments of Housing and Child Protection and skilled multidisciplinary teams including GPs, social workers, psychologists and occupational therapists.
Ingredients to recipes
Prior to participating in the PoPPIL, my exposure to psychiatric education was primarily based on the Diagnostic and Statistical Manual of Mental Disorders (DSM) which, whilst valuable and efficient for its diagnostic and clinical administrative utility, often felt transactional, rigid, reductionist and disconnected from the lived experiences of patients. Formulation models such as the ‘five P’s (presenting, precipitating, predisposing, perpetuating and prognosis)’, ‘biopsychosocial-cultural/spiritual’ and various psychological models, offered me valuable ‘ingredients’ for understanding patients but failed to provide me a clear and cohesive methodology – ‘recipes’ – to integrate these elements with patients’ diagnoses. 18 As defined by the RANZCP, 19 formulations are a set of explanatory hypotheses or speculations that should ideally be amenable to refutation and refinement.18,20 However, I often struggled to see a standardised and explicable approach to formulation and the rationale behind certain treatment plans was rarely elucidated. The PoP, however, held value in providing me the ‘recipe’ for a standardised and explicable approach to formulation. This is aptly summarised by Forbes: ‘It is advantageous for the profession and our patients to ask why we do what we do in our day-to-day work. The reply that it has always been done that way doesn’t suffice’. 20
Educational environment
The discourse-driven teaching methods used to convey knowledge and foster critical thinking further enhanced this inquisitorial approach to clinical practice. The PoPPIL encouraged reflective practice through weekly service rounds where we were able to engage in critical discussions about patients’ diagnostic formulations, treatment plans and the ethical dilemmas presented by each case. I (learner) presented my understanding of the patient’s presentation whist the consultant (instructor) provided constructive criticism. The reflective approach helped me develop and justify my diagnostic formulations and management plans which helped me build confidence, learn from mistakes, develop analytical skills, consider alternative perspectives and have my preconceived notions challenged by colleagues. The collaborative learning environment also allowed for new ideas and viewpoints to be shared whilst concurrently being tested, scrutinised and sometimes rejected. 21 I believe that one of the strengths of the PoPPIL is its commitment to the importance of academic freedom of thought, most widely known through the Chicago Principles: ‘Education should not be intended to make people comfortable, it is meant to make them think. Universities should be expected to provide the conditions within which hard thought, and therefore strong disagreement, independent judgment, and the questioning of stubborn assumptions, can flourish in an environment of the greatest freedom’. 22
Personal challenges
Consistent with this view of the academic journey, the PoPPIL experience was not without its challenges. One of the most significant challenges was realising that psychiatric diagnosis and formulation is not encompassed by the assertion that ‘the patient’s symptoms match up with this DSM diagnosis’. This required a shift in mindset and a willingness, albeit difficult, to realise that an uncritical acceptance of the purely descriptive epistemology of the DSM can overpathologise normal human experiences. 23
Another challenge was the learning curve in understanding the PoP as it required extensive foundational knowledge in other areas such as neurobiology, personality and temperament, and the ability to accept the uncertainty and ambiguity that encapsulates the field. These implications derive from the mind–brain problem, 24 a fundamental obstruction which McHugh and Slavney propose can be circumvented by the PoP by ‘differentiating patient groups according to the nature of their disorders with implications for treatment’. 13
Looking forward
Due to the subjective nature of this reflection, the comparison of the PoPPIL to undergraduate medical education is limited by my experience and may not be reflective of all programs in Australia and New Zealand. Consequently, there is a potential for my views to be modified and influenced by further training and experiences. Whether or not increased participation in these enrichment programs achieves the desired result of increased workforce recruitment and improved perceptions of psychiatry will need to be further explored. Future studies comparing the PoP diagnostic formulation framework to current practices may also be advantageous in strengthening formulation competence and confidence in students and trainees. 18 I speculate that by grounding psychiatric practice in a coherent framework that can be explicated and challenged, the field can potentially be put on a more positive foundation with other medical and surgical specialties.
Conclusion
Overall, the PoPPIL at Johns Hopkins serves as a practical example of a program that facilitates enrichment activities and quality mentorship in an educational environment that is clinically relevant and scientifically rigorous.9–11,15 The focus on critical discussions, discourse-driven collaborative learning, and conceptual clarity cultivated a deeper professional identity and enhanced my critical thinking skills, enabling me to engage with the complexities of psychiatry in a more productive manner whilst improving my perceptions of the field. 25 Since returning, it has helped affirm my future career in psychiatry whilst the opportunity to present and share my experience has stimulated numerous conversations, with various colleagues positively acknowledging that the PoP framework ‘just makes sense’.
Footnotes
Acknowledgements
The author thanks Paul R. McHugh, MD, for his inspiration, encouragement, teachings and historical review. The author would like to further thank Drs. McHugh, Chisolm and Roy for reviewing an earlier draft of this manuscript and for their ongoing encouragement and guidance in his early career; all are affiliated with Johns Hopkins University School of Medicine, Baltimore, Maryland, USA. The author would also like to thank A. Professor Amos and Dr Clarke for their review of an initial draft and ongoing advisership – both are affiliated with RANZCP.
Author contributions
The author has contributed to this paper and has verified the content.
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Allen J Huang received an Australian Government OS-HELP loan for the purposes of funding his elective through The University of Adelaide Medical School Dean’s Elective.